
Abstract
Osteochondroma is the most common benign bone tumor; however, the natural history of the lesion is still poorly understood. Symptomatic osteochondromas are treated with excision, but more often the indications are mainly cosmetic or fear of malignant transformation. There are few reports of spontaneous regression of solitary osteochondroma suggesting several theories causing their regression. We present one such case of a solitary osteochondroma of the humerus in an adolescent male, where a traumatic event resulted in the spontaneous resolution of the lesion.
Introduction
Osteochondroma is the most common benign bone tumor accounting for 35% of all benign bone tumors and 8% of all bone tumors. 1 However, the exact incidence may be higher, as majority of these tumors are asymptomatic and never reported. The natural history of disease is poorly understood. These lesions are usually seen in children, and in majority of the cases, they stop growing at the time of skeletal maturity. 2–3 Symptomatic osteochondromas are treated with surgical excision, however sometimes the indication may be just cosmetic or the parents fear for the possible malignant transformation. But, surgery in itself is not without complications, with reported incidence as high as 12.5%. 4 Very rarely, these lesions are known to regress spontaneously which makes the surgery unnecessary and provide an evidence-based alternate option of observation in such patients for spontaneous resolution to occur. We report one such case of a spontaneous resolution of an osteochondroma after an episode of trauma in an adolescent male.
Case report
A 17-year-old male presented in the outpatient clinic with left arm bony swelling for last 2 years. The swelling was painful on deep palpation, however there was no rest or night pain. There was no history of trauma and presence of similar swellings in other parts of the body.
The past medical history and family history were unremarkable.
The physical examination showed a 1-cm bony hard swelling over the left upper arm which was continuous with the underlying bone. There was mild tenderness on deep palpation. Rest of the examination including the distal neurovascular examination was normal.
The investigations included radiograph of the left shoulder which showed a pedunculated bony lesion in the metaphyseal region of the proximal humerus suggestive of an osteochondroma (Figure 1). The lesion was further investigated with a computed tomography (CT) scan (Figure 2), which reported a tiny 6-mm bony excrescence at the anterolateral cortex of the left proximal humeral shaft with nonaggressive features most likely an osteochondroma. Based on clinicoradiological features, the provisional diagnosis of osteochondroma was made. The patient and the parents were explained the nature of the lesion and were given the options of both observation and excision biopsy. The parents chose to observe the lesion.
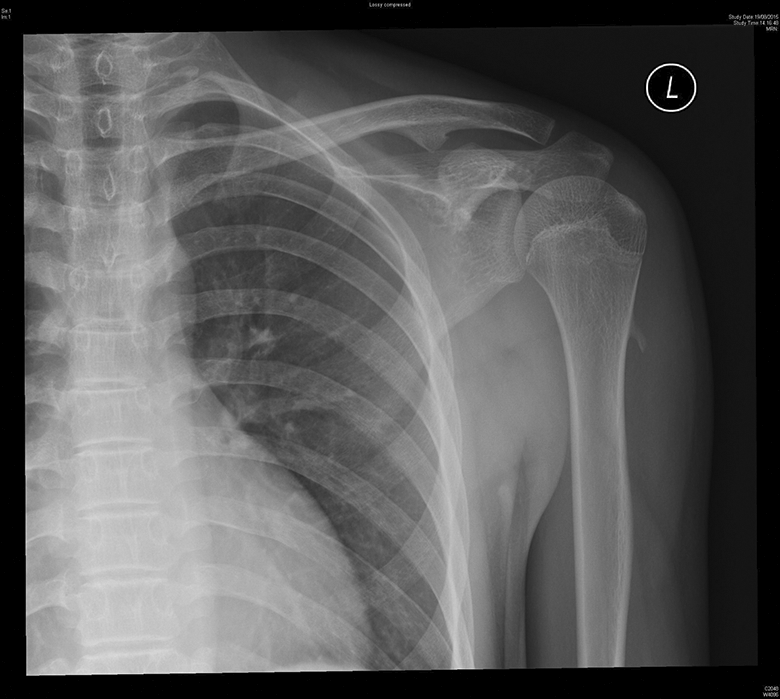
Initial radiograph at the time of first presentation showing the pedunculated osteochondroma at the proximal humerus.
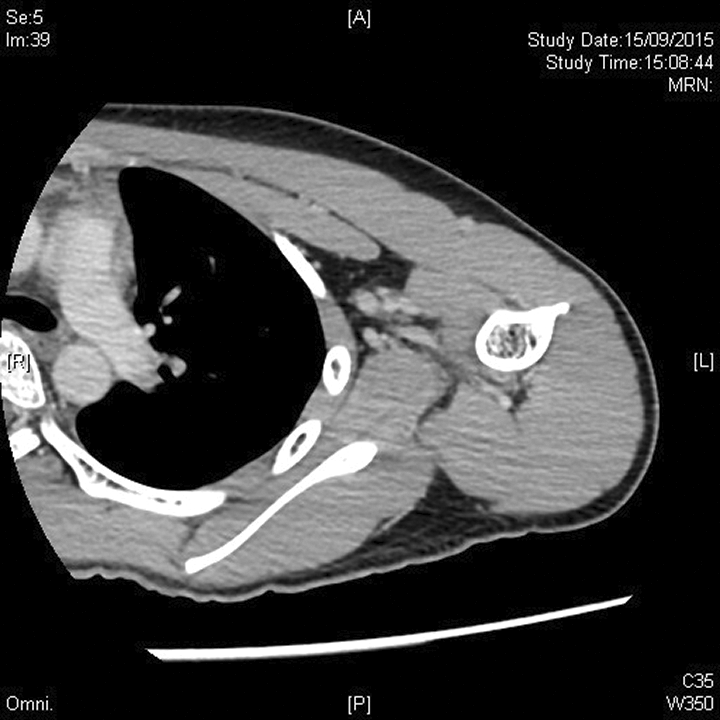
Axial CT image confirming the presence of osteochondroma. CT: computed tomography.
At 6-month follow-up, the patient gave the history of being hit at the site of lesion by his friend 3 months prior to the follow-up. There was significant pain which subsided in 2 days. Now, for the last 1 month, he was unable to palpate the bony lesion. On examination, the bony lesion was not palpable. The radiograph also showed no lesion (Figure 3). The patient was subsequently advised CT scan which confirmed the absence of the bony lesion (Figure 4). No detached bony fragment was seen in the soft tissues as well. At 1.5-year follow-up, the patient was asymptomatic and a repeat radiograph was also unremarkable (Figure 5).
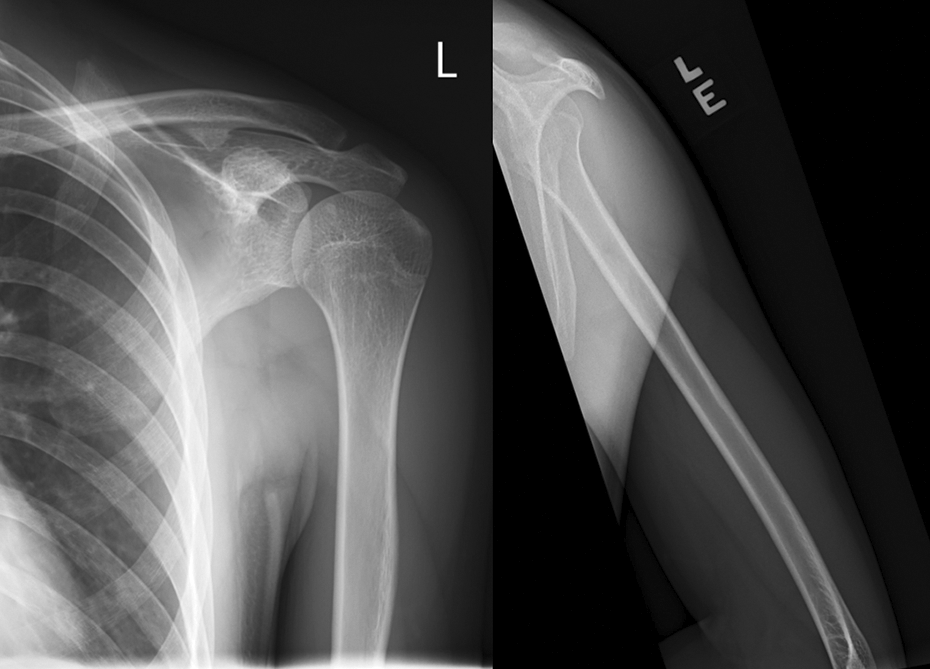
AP and lateral radiograph at 6 months showing the absence of osteochondroma. AP: antero-posterior.

Axial CT image confirming the absent osteochondroma at 6 months. CT: computed tomography.
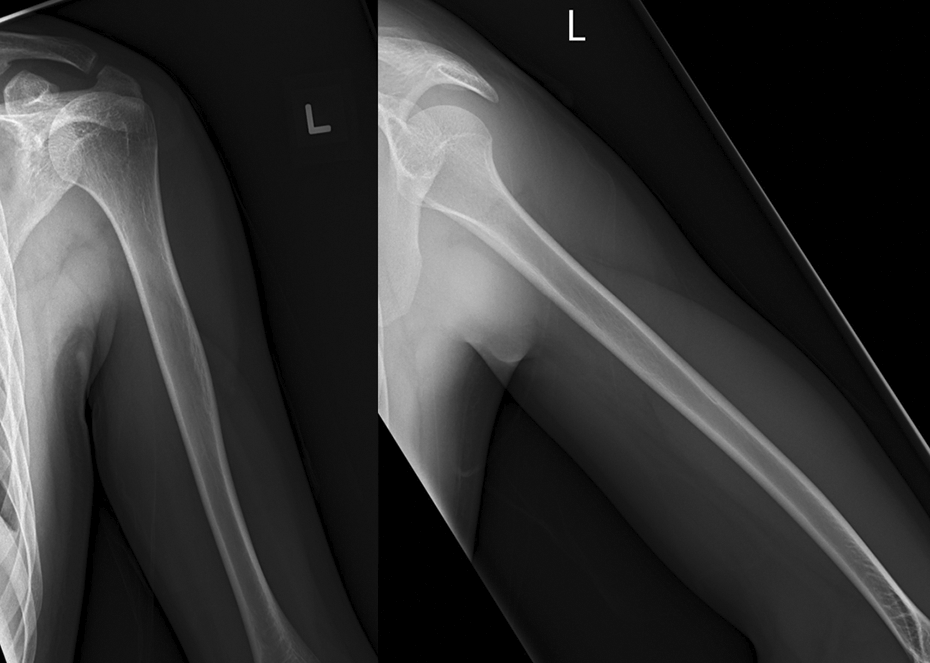
Follow-up radiograph at 1.5 years confirming the spontaneous resolution of osteochondroma.
Discussion
Spontaneous regression of a solitary osteochondroma is rare and till now there are only 27 cases, published mainly as case reports or small series. Although the first case of spontaneous regression of osteochondroma was described in 1835 by Hunter, the exact mechanism of regression of these tumors are still poorly understood.
Several theories have been put forward to explain the mechanism of regression in these cases. Paling 5 suggested that cessation of growth of tumor prior to skeletal maturation may result in the incorporation of the lesion into the host bone. Copeland 6 reported that the regression may follow a traumatic event such as fracture causing injury to the cartilaginous cap, disruption of vascular supply, or stimulating the reparative process in the adjacent bone. This may be the reason for regression of osteochondroma in our case, as there was a history of significant injury to the lesion which might have caused the growth arrest and subsequent resorption of the lesion. Spontaneous regression subsequent to the progressively enlarging pseudoaneurysm was reported by Choi et al., 7 while Song 8 found spontaneous regression of osteochondromatosis of radius and ulna after an ulnar lengthening procedure suggesting change in mechanical strain as the possible cause.
The computer-based literature search showed 27 other cases of solitary osteochondroma which regressed spontaneously (Table 1). 9 –12 The average age at diagnosis was 8.8 years with the range between 5 and 15 years. Our patient was the oldest with the age at the time of diagnosis being 17 years. A majority of the lesions were sessile accounting for 20 cases, while our case was a pedunculated osteochondroma. Most common location of these spontaneously regressing lesions was distal femur (11), followed by proximal humerus (8), proximal tibia (4), and one case each at distal tibia, distal ulna, distal radius, and proximal phalanx. The average time of regression of these lesions reported was 3 years, while our case showed an early resolution in just 6 months which may be caused by an episode of trauma. Some of the lesions showed an initial period of growth before regressing, 9 so caution should be exercised before excising all growing lesions.
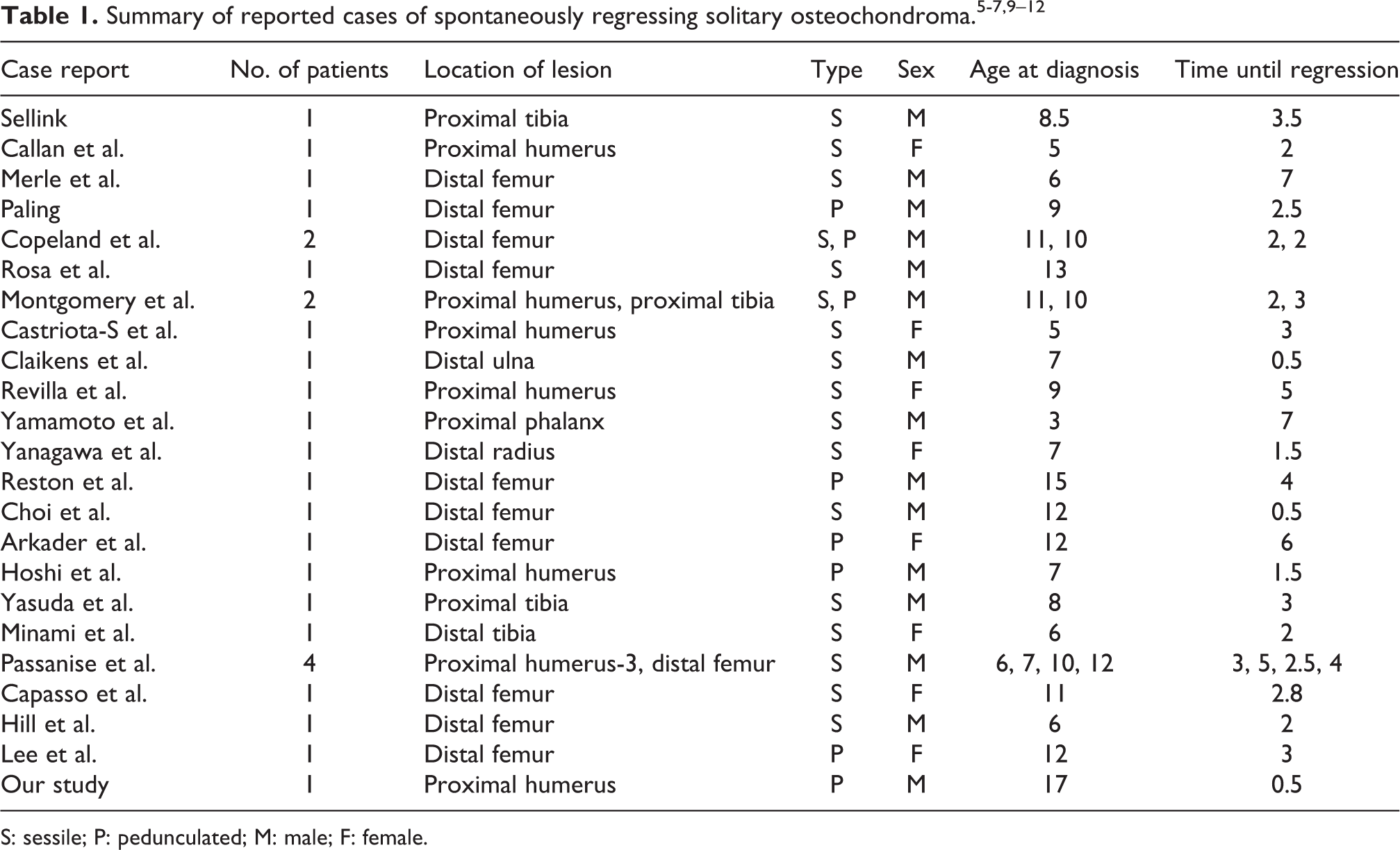
S: sessile; P: pedunculated; M: male; F: female.
This case report adds to the available evidence that the osteochondroma can actually resolve spontaneously, supporting one of the theories of trauma causing regression. Secondly, this case report would help treating physicians in discussing treatment option for these lesions and considering a conservative approach for asymptomatic patients, thereby reducing unnecessary surgery and its related complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.