
Abstract
Study Design
Retrospective cohort study.
Objective
To compare the association of vertebroplasty and hook fixation at the uppermost instrumented vertebra (UIV) with proximal junctional failure (PJF) after long-segment fusion for degenerative sagittal imbalance (DSI).
Methods
A total of 139 patients with DSI who underwent posterior fusion from T9/T10 to the pelvis between 2016 and 2022 were retrospectively reviewed. Patients were categorized into three groups according to proximal junctional strategy: vertebroplasty (n = 21), hook fixation (n = 47), and control (n = 71). The primary outcome was PJF incidence; secondary outcomes included proximal junctional kyphosis (PJK), distal junctional failure, rod breakage, and changes in global sagittal alignment. Multivariate logistic regression was performed to identify independent factors associated with PJF.
Results
The overall incidence of PJF was significantly lower in the intervention group (vertebroplasty or hook) than in controls (5.9% vs 21.1%, P = 0.009). Within the intervention subgroups, hook fixation showed a lower PJF rate (4.3%) than vertebroplasty (9.5%), although the difference was not statistically significant (P = 0.544). Multivariate analysis demonstrated that hook fixation was independently associated with reduced PJF (OR 0.04, P = 0.015). The incidence of PJK did not differ significantly among groups (P = 0.640).
Conclusions
In this retrospective cohort, hook fixation was associated with a lower incidence of PJF, whereas vertebroplasty did not reach statistical significance. These findings suggest that proximal junctional strategies may influence PJF. Prospective randomized controlled trials are needed to confirm these findings and define optimal prophylactic strategies.
Keywords
Introduction
Degenerative sagittal imbalance (DSI) is a progressive spinal deformity that predominantly affects elderly patients, leading to a forward-stooped posture and compensatory changes that impair spinal alignment and lower extremity function. This misalignment often causes significant pain, fatigue, and reduced mobility, substantially diminishing quality of life.1,2 Although conservative management, including physical therapy, may help alleviate symptoms, surgical intervention becomes necessary in advanced cases where daily functioning is compromised. 3
Long spinal fusion is a commonly employed surgical technique for DSI to restore sagittal balance and stabilize the spine. However, complications such as proximal junctional kyphosis (PJK) and proximal junctional failure (PJF) are common postoperative challenges.4,5 PJK is defined as a proximal junctional sagittal Cobb angle of ≥10° measured between the inferior endplate of the uppermost instrumented vertebra (UIV) and the superior endplate of the vertebra two levels above (UIV+2), with a postoperative increase of at least 10° compared to the preoperative measurement.6,7 While many cases of PJK are asymptomatic, progression to PJF—a more severe entity involving structural instability, vertebral fracture, or instrumentation failure—can result in substantial morbidity and frequently necessitates revision surgery due to pain, neurological compromise, or deformity progression.8-10
Among these complications, PJF is particularly consequential, as it not only undermines the goals of surgical realignment but also carries significant clinical and economic burdens. Preventing PJF is therefore a primary consideration in optimizing the outcomes of long-segment fusion for DSI, especially in elderly and medically vulnerable patients. 11 Several patient-related factors—including advanced age, female sex, high body mass index (BMI), and low bone mineral density—have been associated with increased PJF risk. Similarly, radiographic parameters such as increased sagittal vertical axis (SVA) and pelvic incidence-lumbar lordosis mismatch (PI-LL) are predictive of junctional failure.4,9,11-13 Recent studies indicate that restoring the T4–L1 pelvic angle (PA) mismatch to normative ranges reduces the risk of PJF-related mechanical complications in patients with DSI undergoing long-segment posterior spinal fusion.14,15
In addition, surgical factors, such as construct rigidity and excessive sagittal correction, may amplify mechanical stress at the proximal junction, further contributing to PJF risk. 16
To mitigate these risks, adjunctive techniques such as vertebroplasty (VP) and hook fixation at the UIV have been proposed as strategies to reinforce the proximal junction and reduce the likelihood of failure.17-22 Although both techniques are hypothesized to lower the incidence of PJK and PJF, their relative efficacy, particularly in preventing the more severe complication of PJF, remains incompletely understood. Given the substantial clinical consequences of PJF, clarifying the preventive role of VP and hook in this context is of paramount importance. This study aims to address this gap by evaluating whether vertebroplasty and hook fixation reduce the incidence of PJF in a retrospective cohort of patients with DSI undergoing long fusion.
Methods
Study Design and Participants
This retrospective cohort study included 139 patients diagnosed with DSI who underwent long spinal fusion extending from T9 or T10 to the pelvis at our institution between 2016 and 2022. All patients had a minimum postoperative follow-up of two years. The study was approved by the Institutional Review Board of Asan Medical Center (IRB number: S2024-0479-0002), and the requirement for informed consent was waived due to the retrospective nature of the study.
Surgical intervention was indicated for patients with severe sagittal malalignment—defined as a sagittal vertical axis (SVA) > 50 mm and a pelvic incidence-lumbar lordosis (PI-LL) mismatch >10° on standing radiographs—that resulted in significant functional impairment, chronic back pain, and reduced quality of life.
Eligible participants were categorized into three groups based on the proximal junctional intervention received: a vertebroplasty group (n = 21), a hook group (n = 47), and a control group (n = 71) with no proximal intervention. Inclusion criteria comprised patients aged over 60 years with a diagnosis of DSI requiring long fusion and meeting the above radiographic criteria for severe sagittal imbalance. Patients with prior spinal surgery involving the proximal junction, active infection, or malignancy affecting the spine were excluded from the study.
Surgical Procedure
Interbody fusion was performed from L2 to S1 using an anterior surgical approach. In cases where vascular anatomy (common iliac vessels) precluded safe anterior cage placement at L5-S1, a staged posterior lumbar interbody fusion was added following completion of the anterior procedure. After repositioning the patient to a prone position, all patients underwent posterior spinal fusion from the thoracic spine (T9 or T10) to the pelvis for sagittal alignment correction. Fusion constructs included segmental pedicle screw fixation at each vertebral level, with final fixation to the pelvis using pelvic fixation techniques to enhance distal construct stability. Intraoperative sagittal realignment was achieved through segmental Ponte osteotomies combined with corrective rod contouring, with careful adjustment to achieve balanced global alignment without overcorrection. All constructs utilized 6.0-mm cobalt–chrome alloy rods. Four-rod configurations were predominantly employed in both intervention groups to improve construct durability. Prior to 2019, no additional proximal interventions, such as vertebroplasty or hook application, were performed (Figure 1). Beginning in 2019, either vertebroplasty or hook fixation was selectively implemented at the UIV (T9 or T10) to enhance proximal stability and potentially reduce the risk of PJK and PJF. Hook fixation consisted of bilateral placement of transverse process hooks at the UIV instead of pedicle screws, aiming to create a “soft landing” effect and modulate proximal construct stiffness. The choice between vertebroplasty and hook fixation evolved over time, reflecting surgeon preference and evolving biomechanical considerations rather than a strictly predefined protocol. Vertebroplasty was primarily used to reinforce osteoporotic vertebrae, whereas hook fixation was selected to reduce stress concentration at the proximal junction through dynamic stiffness modulation. Representative case of long-segment posterior fusion without proximal junctional intervention (control group) A 70-year-old female patient presented with degenerative sagittal imbalance. Preoperative whole-spine radiographs (Panels A and B) demonstrate marked sagittal malalignment. The patient underwent spinopelvic fixation from T10 to the pelvis. Postoperative whole-spine radiographs (Panels C and D) show restoration of lumbar lordosis and improved global sagittal alignment
Variables and Measurements
Clinical variables included age, sex, BMI, comorbidities (diabetes mellitus [DM], hypertension [HTN], malignancy), osteoporosis, and the number of rods used during surgery. Additionally, clinical outcomes were assessed using the Visual Analog Scale (VAS) for back pain, which was recorded preoperatively and at 2 years postoperatively to evaluate pain improvement. Radiographic parameters were assessed using standardized standing anteroposterior and lateral whole-spine radiographs obtained preoperatively and postoperatively prior to discharge. Parameters included pelvic incidence (PI), pelvic tilt (PT), lumbar lordosis (LL), thoracic kyphosis (TK), PI–LL mismatch, and C7 SVA..23,24 All radiographic measurements were performed twice by a single blinded orthopedic surgeon, with the mean value used for analysis. Postoperative complications were analyzed with respect to the occurrence of PJK, PJF, distal junctional failure, and rod breakage. These complications were defined as follows: PJK was defined as an angle at least 10° greater than the baseline when measuring the lower endplate of the UIV and the upper endplate of two supra-adjacent vertebrae (UIV + 2). 12 PJF was defined as any symptomatic PJK that necessitated revision surgery due to vertebral fracture, implant pullout, or significant kyphotic collapse. 25 Distal failure included structural failure at the distal end of the fusion construct.
Statistical Analysis
For continuous variables with a normal distribution, comparisons among the three groups (vertebroplasty, hook, and control) were performed using one-way analysis of variance (ANOVA). For non-normally distributed variables, the Kruskal–Wallis test was applied. Categorical variables were analyzed using the chi-square test or Fisher’s exact test, as appropriate.
To identify independent risk factors for PJF, multivariate logistic regression analysis was performed. Variables included in the model were age, sex, follow-up period, BMI, presence of osteoporosis, number of rods, whether hook or vertebroplasty was performed at the UIV, and preoperative and postoperative radiographic parameters (PI, PT, LL, TK, PI–LL mismatch, C7 SVA, T4 PA, L4 PA, and T4-L1 PA mismatch). Odds ratios (ORs) with corresponding 95% confidence intervals (CIs) were calculated. Variables with P < 0.1 were retained in the final model, and variables with P < 0.05 were considered statistically significant.
Intra-observer reliability for the measurement of global sagittal alignment parameters (PI, PT, LL, TK, SVA, T4 PA and L1 PA) was assessed using intraclass correlation coefficients (ICC), yielding values of 0.915 (PI), 0.923 (PT), 0.934 (LL), 0.853 (TK), 0.846 (C7 SVA), 0.852 (T4 PA), and 0.872 (L1 PA) for preoperative measurements, and 0.921 (PI), 0.931 (PT), 0.932 (LL), 0.860 (TK), 0.855 (C7 SVA), 0.857 (T4 PA), and 0.864 (L1 PA) for postoperative measurements, indicating excellent reliability throughout the study.
Preoperative and postoperative clinical outcomes (VAS for back pain) within each group were compared using the paired t-test. Differences in clinical outcomes between groups were assessed using one-way analysis of variance (ANOVA).
All statistical analyses were conducted using SPSS software version 21.0 (IBM Corp., Armonk, NY, USA) for descriptive statistics and univariate analyses, and Statsmodels in Python for multivariate logistic regression. A P-value of less than 0.05 was considered statistically significant.
Results
Primary Outcome: Proximal Junctional Failure
Patient Characteristics and surgical Outcomes Across vertebroplasty, hook, and Control Groups

Values are expressed as n/n, n (%), or mean ± standard deviation. P-values for categorical variables were calculated using the chi-square test or Fisher’s exact test, and for continuous variables using one-way analysis of variance (ANOVA) or the Kruskal–Wallis test, depending on data distribution.
BMI, body mass index; DM, diabetes mellitus; HTN, hypertension; PJK, proximal junctional kyphosis; PJF, proximal junctional failure. *P-value <0.05.

Incidence rates of proximal junctional failure (PJF) and proximal junctional kyphosis (PJK) among vertebroplasty (VP), hook fixation, and control groups. PJF showed a significant difference among the three groups (P = 0.044), with the lowest rate observed in the hook group (4.3%) and the highest in the control group (21.1%). In contrast, PJK did not differ significantly across groups
Multivariate Logistic Regression Analysis for Risk Factors of proximal Junctional Failure

The following variables were included in the multivariate logistic regression model: age, sex, follow-up period, BMI, osteoporosis, number of rods, type of instrumentation at the UIV, and preoperative and postoperative radiographic parameters (PI, PT, LL, TK, PI-LL mismatch, C7 SVA, T4 PA, L1 PA, and T4-L1 PA mismatch). Backward stepwise selection was used, and variables with P < 0.1 were retained in the final model.
Odds ratios (OR) with corresponding 95% confidence intervals (CI) were calculated by exponentiating the logistic regression coefficients. Variables with P < 0.1 were retained in the final model, and variables with P < 0.05 were considered statistically significant. An OR <1 indicates a protective effect, while OR >1 indicates increased risk.
UIV, uppermost instrumented vertebra; OR, odds ratio; CI, confidence interval; PI, pelvic incidence; PT, pelvic tilt; LL, lumbar lordosis; TK, thoracic kyphosis; PI-LL, pelvic incidence-lumbar lordosis mismatch; C7 SVA, C7 sagittal vertical axis; PA, pelvic angle; *P < 0.05.

Forest plot of risk factors for proximal junctional failure (PJF) Forest plot illustrating the results of multivariate logistic regression analysis for risk factors of PJF. The chart displays the odds ratios (OR) and 95% confidence intervals (CI) for variables retained in the final model. Hook fixation at the uppermost instrumented vertebra (UIV) was identified as a significant protective factor against PJF (OR 0.04, P = 0.015). Vertebroplasty also demonstrated a trend towards a protective effect (OR 0.08, P = 0.053), though it did not reach statistical significance. Error bars represent 95% CIs. The x-axis is presented on a logarithmic scale. An OR <1 indicates a protective effect, while an OR >1 indicates an increased risk. *P < 0.05
Secondary Outcomes: Proximal Junctional Kyphosis and Mechanical Complications
There was no significant difference in the incidence of PJK among the three groups. PJK occurred in 19.0% (4/21) of patients in the vertebroplasty group, 29.8% (14/47) of patients in the hook group, and 29.6% (21/71) of patients in the control group (P = 0.640) (Figure 4) (Table 1). Representative case of proximal junctional kyphosis following long-segment posterior fixation with hook instrumentation. A 72-year-old female patient underwent spinopelvic fixation with hook instrumentation at the UIV. Proximal junctional kyphosis developed at the 6-month follow-up; however, additional surgery was not performed due to mild symptoms. Panel A shows the preoperative radiograph, Panel B the immediate postoperative radiograph, and Panel C the 6-month postoperative radiograph. Panel D is a magnified view of the yellow box in Panel C, demonstrating the measurement of the proximal junctional angle (between yellow lines), which was 20°
Regarding distal junctional failure, no significant differences were observed across groups. Distal failure was noted in 4.8% (1/21) of patients in the vertebroplasty group, 6.4% (3/47) in the hook group, and 7.0% (5/71) in the control group (P = 0.932) (Table 1).
In contrast, the incidence of rod breakage differed significantly among groups (P = 0.026). The control group demonstrated a significantly higher rate of rod breakage at 23.9% (17/71), compared to 8.5% (4/47) in the hook group and 4.8% (1/21) in the vertebroplasty group (Table 1).
Clinical Outcomes: VAS for Back Pain
Comparison of Preoperative and 2-Year Postoperative Back Pain VAS Scores Among the Vertebroplasty, Hook, and Control Groups

Values are expressed as mean ± standard deviation. P-value.
VAS, Visual Analog Scale. *P-value <0.05.
* for between-group comparison (One-way ANOVA). P-value
** for within-group comparison (Preoperative vs Postoperative) using paired t-test.
Radiographic Outcomes: Global Sagittal Alignment
Preoperative and postoperative radiographic Sagittal Alignment parameters
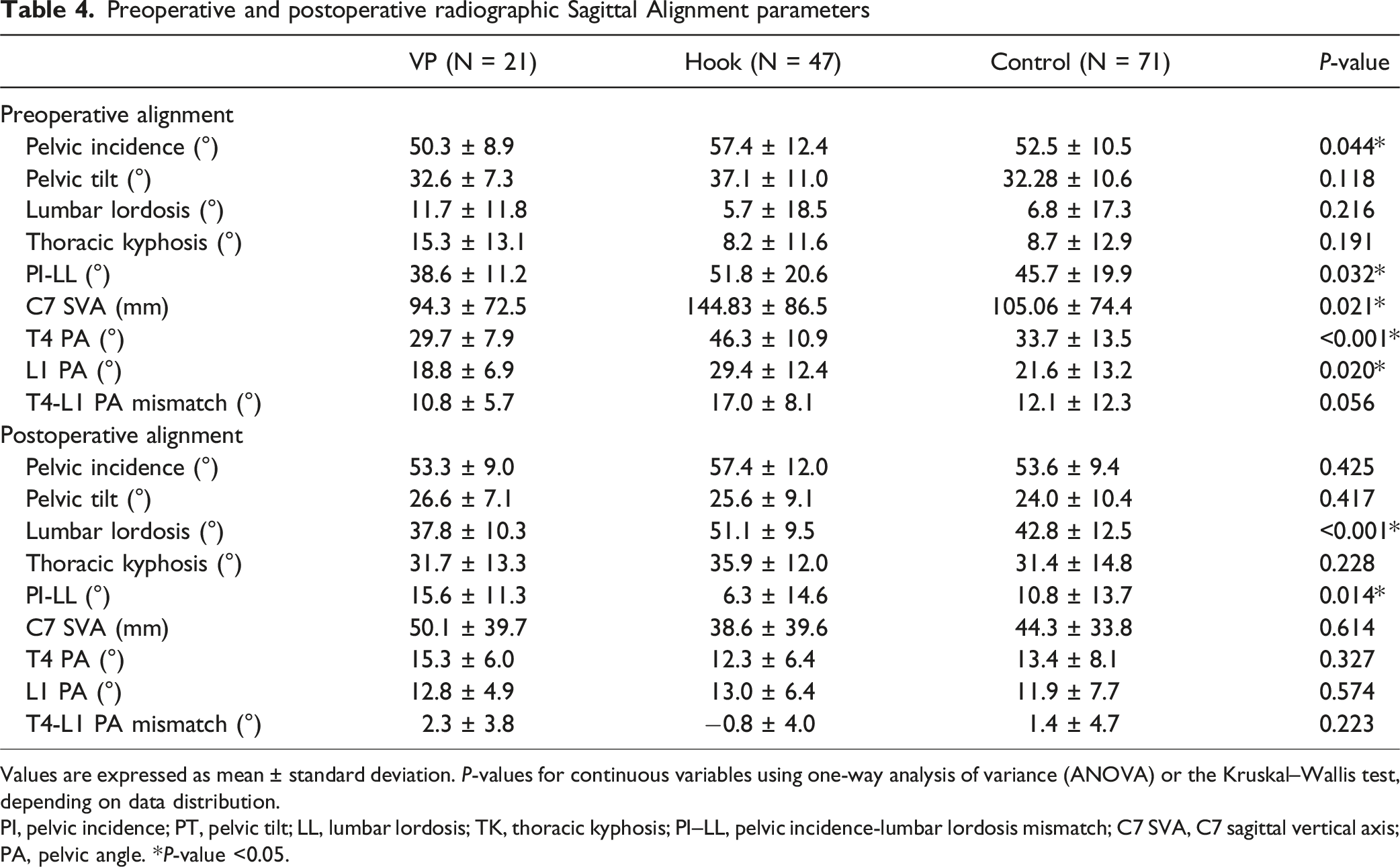
Values are expressed as mean ± standard deviation. P-values for continuous variables using one-way analysis of variance (ANOVA) or the Kruskal–Wallis test, depending on data distribution.
PI, pelvic incidence; PT, pelvic tilt; LL, lumbar lordosis; TK, thoracic kyphosis; PI–LL, pelvic incidence-lumbar lordosis mismatch; C7 SVA, C7 sagittal vertical axis; PA, pelvic angle. *P-value <0.05.
All groups demonstrated significant postoperative improvements in global sagittal alignment. Lumbar lordosis was significantly greater in the hook group (51.06° ± 9.49°) compared to the vertebroplasty (37.77° ± 10.34°) and control groups (42.81° ± 12.53°; P < 0.001). The hook group also demonstrated a significantly lower PI–LL mismatch (6.32° ± 14.56°) compared to the control group (10.78° ± 13.69°) and vertebroplasty group (15.57° ± 11.26°; P = 0.014). No significant differences were observed among the groups in postoperative PI, PT, TK, C7 SVA, T4 PA, L1 PA, or T4-L1 PA mismatch (all P > 0.05) (Table 4).
Discussion
Our findings demonstrated that hook fixation at the UIV was independently associated with a significant reduction in the risk of PJF, whereas vertebroplasty did not show a statistically significant protective effect. Neither technique appeared to influence the incidence of PJK.
The protective role of hook fixation likely derives from its biomechanical advantage of reducing the abrupt stiffness transition at the proximal junction, thereby allowing a more gradual load transfer and decreasing stress concentration at adjacent segments.26-28 In contrast, vertebroplasty, although capable of reinforcing vertebral body strength and resisting compression-related failure, did not consistently translate into a measurable reduction in PJF risk in our analysis. The lack of significance (P = 0.053) suggests that its preventive effect may be limited.17,29,30
Four-rod configurations were used in all vertebroplasty cases (21/21, 100%) and the majority of hook fixation cases (44/47, 93.6%), whereas the control group received variable configurations (2-rod, 3-rod, or 4-rod) based on technical feasibility of rod placement and surgeon preference. Interestingly, within the Control group, 4-rod constructs showed a numerically higher PJF rate (23.5%) compared to 2-3 rod constructs (16.2%), although this difference was not statistically significant. These findings suggest that increasing construct rigidity with additional rods alone does not prevent PJF; rather, adjunctive proximal interventions, such as vertebroplasty or hook fixation, appear to be crucial for mitigating the risk of proximal junctional failure.
Notably, the hook group exhibited higher preoperative C7 SVA and lower BMD than the control group, indicating more severe sagittal imbalance and compromised bone quality. Despite these elevated baseline risk factors, the hook group demonstrated a substantially lower incidence of PJF. Although causal inference cannot be definitively established, this finding may suggest a potential association between hook fixation and reduced PJF risk, even in patients with greater deformity severity and osteoporosis. However, the more favorable postoperative alignment observed in the hook group should also be considered as a contributing factor to the reduced incidence of PJF.
Taken together, these results underscore the importance of optimizing proximal junction mechanics in long-segment fusion for DSI. While vertebroplasty may provide benefits in selected patients with severe osteoporosis, hook fixation appears to offer more robust biomechanical protection and may exert a greater influence on long-term outcomes by mitigating junctional stress and preserving adjacent segment motion. Future prospective studies with larger sample sizes are warranted to validate these findings and refine patient-specific strategies for proximal stabilization.
In our study, neither hook fixation nor vertebroplasty significantly reduced the incidence of PJK, supporting the growing consensus that such interventions may have limited utility in PJK prevention. Several prior studies have similarly reported mixed findings regarding the potential of hook fixation or vertebroplasty to mitigate PJK risk. For instance, Matsumura et al. 31 compared hook constructs with pedicle screws at the UIV in 39 patients and found that PJK occurred in 17.6% of the hook group vs 27.3% of the pedicle screw group; however, this difference was not statistically significant. Interestingly, Tsutsui et al. 32 reported an even higher incidence of PJK in the hook group (25.7%) compared to the pedicle screw group (8.0%) in their retrospective series, suggesting that in some cases, hook fixation may paradoxically contribute to PJK development. Similarly, the efficacy of prophylactic vertebroplasty in preventing PJK remains inconclusive. A systematic review by Rahmani et al. 30 , analyzing eight studies comprising 685 patients, highlighted conflicting results regarding the impact of vertebroplasty on PJK incidence, with the authors ultimately concluding that evidence is “inconclusive and conflicting.” Moreover, a prospective 5-year cohort study by Raman et al. 29 found that although vertebroplasty may contribute to early reduction of PJF, it did not significantly reduce long-term PJK rates, with 28.2% of patients developing PJK during follow-up. Taken together, these findings underscore the current lack of high-quality, definitive evidence supporting either hook fixation or vertebroplasty as standalone preventive strategies for PJK. Our present results are consistent with this perspective, reinforcing the notion that structural augmentation at the UIV alone may be insufficient to mitigate the multifactorial risk of PJK. Comprehensive approaches—addressing factors such as alignment correction, paraspinal muscle preservation, and patient-specific risk profiles—are likely required to more effectively reduce PJK incidence in long-segment constructs.
Interestingly, several factors previously identified as predictors of PJF—including demographic variables such as sex and BMI, as well as key sagittal alignment parameters (PI–LL mismatch, C7 SVA and T4-L1 PA mismatch)—did not emerge as significant risk factors in our multivariate analysis.8,9,11,12,14,15,25,33 These findings suggest that while such parameters have been associated with PJF risk in prior studies, they may not consistently predict outcomes across different patient populations or surgical contexts. Taken together, these results highlight that the prevention of PJF likely depends not only on patient factors or global alignment targets, but also on the biomechanical optimization of the proximal junction through thoughtful selection of UIV instrumentation. Our findings highlight the importance of incorporating hook fixation as a proximal stabilization strategy in surgical planning for long-segment constructs, particularly in elderly patients with DSI who are at increased risk of junctional failure.
Regarding clinical outcomes, corrective surgery resulted in meaningful pain relief across all groups, as reflected by the overall improvement in VAS back pain scores at 2-year follow-up. While the vertebroplasty group demonstrated numerical improvement that approached statistical significance (P = 0.058), statistical significance was not achieved, likely due to the relatively small sample size (n = 21). Importantly, there were no significant differences in postoperative VAS scores among the three groups (P = 0.269), indicating that the addition of proximal prophylactic strategies did not translate into superior back pain reduction compared with the control group at mid-term follow-up. These findings suggest that although interventions such as hook fixation may reduce the radiographic incidence of proximal junctional failure, their impact on general pain outcomes appears limited. This observation is consistent with prior literature indicating that clinical outcomes following adult spinal deformity surgery are multifactorial and influenced by a broad spectrum of biomechanical, neurological, and patient-specific factors.3,6,34 Given the relatively small number of patients in the intervention subgroups—particularly in the vertebroplasty cohort—further studies with larger sample sizes and adequately powered analyses are warranted to clarify whether subtle differences in clinical outcomes may emerge over longer follow-up periods or in specific patient subpopulations.
This study has several important limitations. First, the retrospective design and non-randomized allocation introduce a significant temporal allocation bias. As the control cohort was treated predominantly before 2019, whereas proximal junctional interventions were introduced thereafter, improvements in surgical technique, rod construct strategies, surgeon experience, and alignment principles over time may have independently contributed to the observed reduction in PJF.
Second, the relatively small size of the vertebroplasty cohort (n = 21) limits statistical power and increases the risk of type II error. Post-hoc power analysis demonstrated limited power to detect differences in PJF between groups; therefore, the absence of statistical significance should not be interpreted as evidence of equivalence. In addition, the relatively small number of PJF events (n = 19) raises the possibility of model overfitting in the multivariate logistic regression analysis. Given the number of variables included, the stability of the estimated odds ratios should be interpreted with caution, as sparse-data bias may have influenced the results.
Third, although key sagittal parameters were included in the multivariate analysis, composite alignment indices such as the Global Alignment and Proportion (GAP) score and cervical alignment parameters were not routinely assessed. Given the reciprocal relationship between cervical and thoracolumbar alignment in adult spinal deformity, omission of these measures may limit comprehensive evaluation of global sagittal balance.35,36
Fourth, quantitative assessment of paraspinal muscle quality, sarcopenia, and frailty was not available, representing a potential source of residual confounding.
Fifth, follow-up duration differed significantly among groups and was relatively shorter in the intervention cohorts. Among patients with more than 5 years of follow-up (n = 18), 17 were in the control group, with only one patient in the vertebroplasty group and none in the hook group. This imbalance limits assessment of long-term durability beyond 5 years in the intervention groups. Notably, among control patients with extended follow-up, rod fractures were observed in 12 patients (70.6%). These findings suggest that long-term mechanical failure remains a relevant concern; however, comparable long-term data are lacking for the intervention cohorts.
Finally, PJF was defined as symptomatic pathology requiring revision surgery. Consequently, the reported incidence reflects not only radiographic progression but also surgeon-mediated decision-making and individual thresholds for reoperation. In addition, the selection between hook fixation and vertebroplasty was based on surgeon discretion rather than a predefined treatment algorithm. These factors underscore the need for prospective studies with standardized allocation criteria and revision thresholds to more definitively establish the independent effect of proximal junctional prophylactic strategies.
Despite these limitations, this study offers important strengths. To our knowledge, it is among the few to directly compare vertebroplasty and hook fixation for PJF prevention in elderly DSI patients. Moreover, our findings provide valuable evidence supporting the critical role of proximal stabilization techniques in optimizing surgical outcomes—extending beyond radiographic correction alone.
Conclusion
In this retrospective cohort, hook fixation was associated with a lower incidence of PJF, while vertebroplasty showed a numerical trend toward reduction that did not reach statistical significance. These findings suggest that proximal augmentation strategies may influence PJF risk in patients undergoing long-segment fusion for degenerative sagittal imbalance. However, given the retrospective design, temporal allocation bias, limited number of outcome events, and relatively short follow-up in the intervention groups, these findings should be interpreted as exploratory and hypothesis-generating. Prospective studies with larger cohorts and longer follow-up are warranted to validate these observations and further clarify optimal strategies for PJF prevention.
Footnotes
Ethical Considerations
This retrospective study was approved by the Institutional Review Board of Asan Medical Center (IRB No. S2024-0479-0002)
Consent to Participate
The requirement for written informed consent was waived.
Author Contributions
(I) Concept and design: S.T.C, J.H.C; (II) Administrative support: J.H.C; (III) Provision of study materials or patients: S.T.C, J.H.C; (IV) Collection and assembly of data: S.T.C, J.H.C; (V) Data analysis and interpretation: S.T.C, J.H.C; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request