
Abstract
Study design
Prospective multicentric study.
Objective
Thoracolumbar fractures without neurologic deficit are challenging situations in terms of treatment decision making. We aimed to analyze the occurrence of adverse events (AEs) after surgical and nonsurgical treatment and its impact on functional outcomes.
Methods
198 patients from a prospective multicentric database were included. The occurrence of adverse events and treatment failure within 2 years of follow up were recorded. ODI was compared between patients with and without adverse events at six months, 1 year and 2 years follow up. Multivariable regression analysis was conducted to assess the association between post-treatment adverse events and ODI at 1-year follow-up.
Results
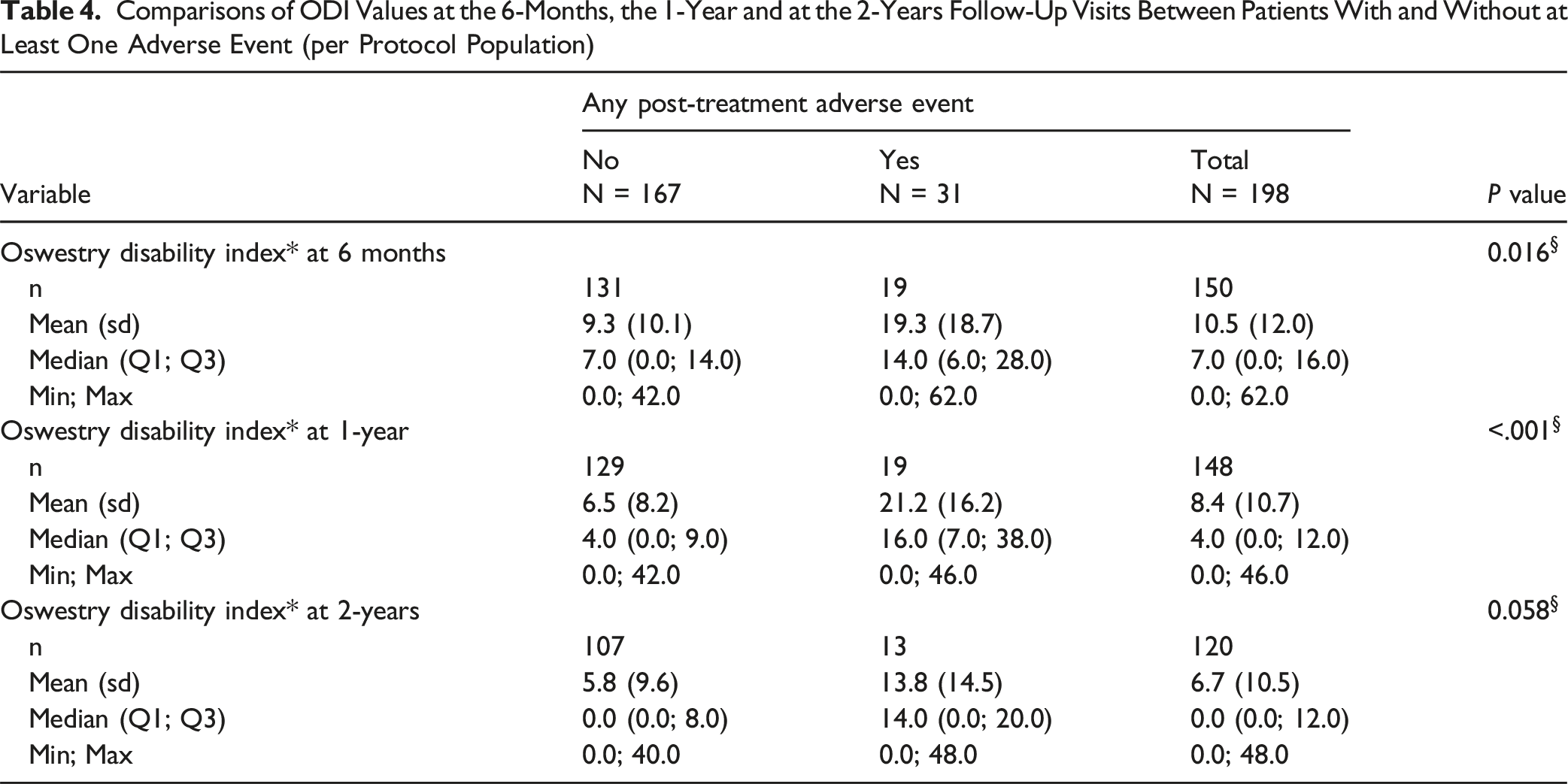
46 adverse events were recorded (23.2%). Higher categories of the Charlson Comorbidity Index (CCI) (P = 0.006), unemployment or retirement (P = 0.027), and current smoking (P = 0.008) were significantly associated with the occurrence of adverse events whereas no significant differences were observed in terms of treatment decision (conservative vs surgical). ODI values were significantly higher in patients with adverse events at the 6-month and 1-year follow-up visits without significant differences at 2 years follow up. Treatment failure was observed in only 5 patients.
Conclusion
We found association between the occurrence of AE and higher ODI at 6-months and one-year follow up. Additionally, a higher CCI and smoking status were associated with higher likelihood to develop adverse events in our cohort.
Introduction
Thoracolumbar burst fractures represent around 45% of major thoracolumbar spine injuries.1,2 The transition from a relative rigid thoracic spine to a mobile lumbar spine makes this region particularly affected due to axial and flexion forces. 3 This type of fractures can have significant impact on patient’s quality of life due to risk of progressive kyphosis or neurological compromise. Despite being a relatively common pathology, there is a lack of consensus on how to treat these injuries. Whereas some authors showed better functional outcomes after surgical treatment other findings suggested similar results in both surgical and non-surgical groups with higher rate of complications and costs in patients receiving surgical treatment.4,5
Adverse events (AEs) and treatment failure are deviations from the normal treatment evolution that can happen either after operative or non-operative treatment and are usually associated with higher hospital stay and costs. 6 Moreover, some studies showed poorer patient reported outcomes associated with the occurrence of AE 6 whereas other authors showed similar long-term outcomes and satisfaction in patients despite the occurrence of complications. 7 The impact of AEs in functional outcomes after thoracolumbar trauma has not been deeply analyzed.
This study aimed to assess whether patients who experienced at least one post-treatment AE or treatment failure had worse absolute ODI values at 6 months, 12 months, and 2 years compared to patients without adverse events. Additionally, we aimed to examine whether the treatment approach (operative vs nonoperative) affected the relationship between adverse events and ODI outcomes.
Methods
This is a sub analysis from a prospective observational study, the AO Spine TL A3/A4 study [Clinical Trials.gov Identifier NCT02827214], that was designed and conducted by the Knowledge Forum Trauma of the AO Spine, an expert driven research study working group supported by the non-profit AO Foundation. Informed consent was obtained in all patients. This study analyzed data gathered from a total of 14 sites across four continents. Study sites were located in the United States (4 sites), Canada (2 sites), the Netherlands (1 site), Spain (1 site), Switzerland (1 site), Romania (1 site), Greece (1 site), Egypt (1 site), India (1 site), and Australia (1 site). The study included patients between 18 and 65 years of age with an acute (<10 days from injury) traumatic fracture between T10 - L2 inclusive where the fracture met the criteria of an AO Type A3 or A4 burst fracture based on the judgement of the treating physician on a CT scan. 8 Patients with an A3 or A4 fracture with or without a suspected Posterior Ligamentous Complex (PLC) injury and a TLICS Score between 2-5 were also included. A detailed information of the patients included can be found in the original paper. 9
Comparisons were made between patients who experienced at least one post-treatment adverse event (AE) and between those who experienced treatment failure and those who did not. Adverse events (AE) were defined as any event due to medical or surgical management that leads to patient harm or require additional monitoring or treatment, 10 AE were recorded using the Spinal Adverse Events Severity System (SAVES-V2). 11 AE were registered up to two years of follow up. Surgical treatment failure was defined as necessity of an non-scheduled additional surgery after the primary surgical treatment whereas non-surgical treatment failure was defined as necessity of surgery after non-surgical treatment. Implant removal was not considered an adverse event or treatment failure as it was the standard of treatment in some participating centers.
The Spine AdVerse Events Severity (SAVES) system version 2 was used to record AEs. SAVES-V2 is a validated tool to capture AEs in spine surgery patients and is categorized into intra-operative and post-operative AE. AEs were reported by category at the patient level; multiple events of the same type were combined for each patient, thus counting each patient with at least one AE only once. In cases with multiple events, the most severe event within each category was reported. Event rates were calculated using the total population size as the denominator, irrespective of dropouts during the course of follow-up. This assumes that any adverse event would have been reported for study patients if they had occurred, even after initial lost to follow-up.
AEs were further categorized according by their seriousness at patient level. Serious AEs included those leading to death, resulting in a life-threatening illness or injury, in a permanent impairment of a body structure or function, in a medical or surgical intervention to prevent life-threatening, requiring in-patient hospitalization or prolongation of existing hospitalization.
AEs were also summarized by severity grade and time of occurrence at the AE level. Severity was graded from 1 (adverse event does not require treatment and has no adverse effect) to 5 (significant neural injury (i.e.: one or more grade deterioration in ASIA grade) or serious life or limb threatening event).
Statistical Analysis
Summary statistics were used to assess differences in demographics, treatment, and fracture classification at baseline between patients with and without at least one post-treatment adverse events and between those with and without treatment failure. Categorical variables were summarized using frequency and percentage for each category. Continuous variables were summarized using n, mean, standard deviation (SD), median, lower and upper values of the inter-quartile range, and minimum and maximum values. For BMI, a t-test was applied while for all other continuous variables, the Wilcoxon rank sum test was used due to non-normal distribution. Chi squared tests were used to evaluate differences in categorical variables while Fisher’s exact test was used if the expected cell count was less than five in one or more of the cells. Due to the relatively small number of patients with treatment failure, these analyses were repeated for patients with and without treatment failure, but without applying statistical tests as statistical power for detecting significant differences may have been limited.
We conducted a descriptive analysis to assess the association between the occurrence of at least one adverse events and ODI values at 6 months, 12 months, and 2 years, using the Wilcoxon rank sum test. This analysis was repeated within patients who received surgical and conservative treatments. Due to the small number of patients with a post-treatment adverse event and available ODI data at the different follow-up visits, especially in the conservatively treated group, no statistical tests were performed for this assessment acknowledging again that statistical power for detecting significant differences may have been limited. Similarly, due to the small number of patients with treatment failure, the same approach was applied for patients with and without treatment failure, with no stratification by treatment group. Finally, ODI values assessed prior the occurrence of an adverse event were not considered for the analyses. Finally, a multivariable robust regression analysis was conducted to assess the association between post-treatment adverse events and ODI at the 1-year follow-up, while considering potential outliers and leverage points. This approach was chosen to provide more reliable estimates by reducing the influence of data points that may disproportionately affect the model due to extreme values or unusual leverage. Based on the AIC and BIC criteria, the model was adjusted for ODI at discharge, sex, race, Charlson Comorbidity Index (CCI), injury impact type, posterior ligamentous complex, time from injury to treatment (days), and current smoking status.
Results
Baseline Characteristics
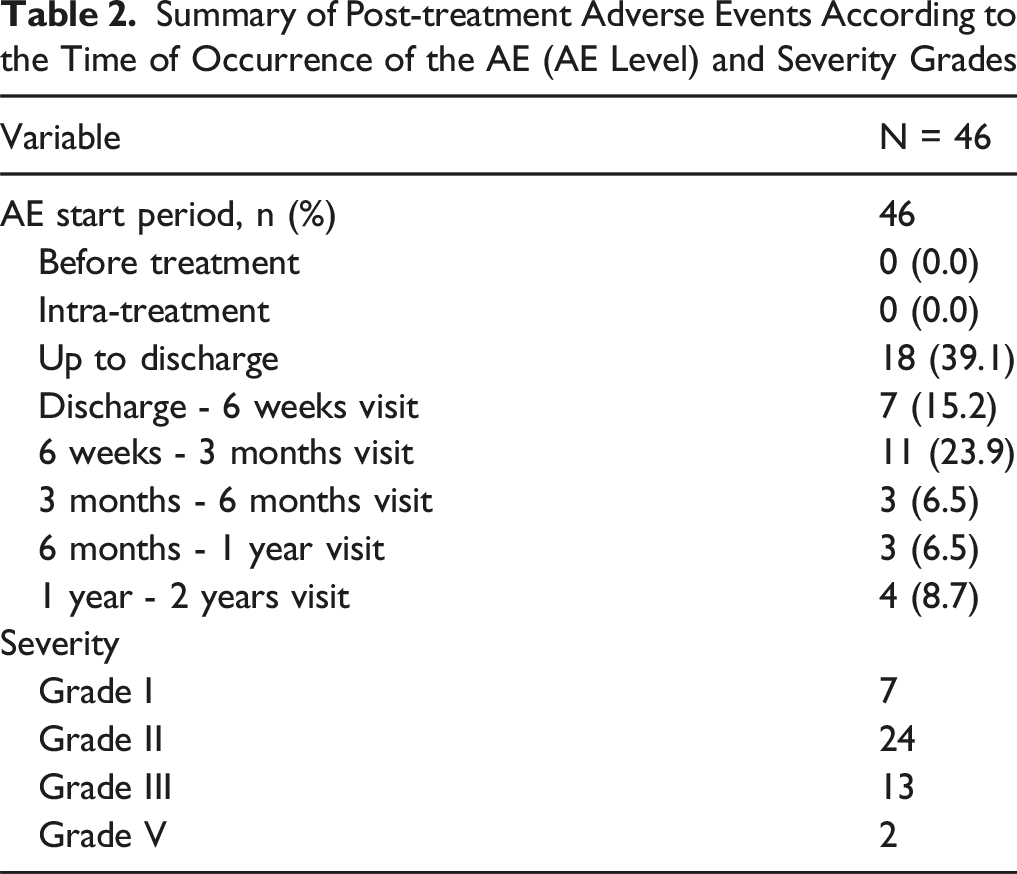
198 patients were finally included in the study. During the 2 years follow-up period, 31 patients suffered at least one post-treatment adverse event and the calculated risk of a patient developing at least one AE during the study period was 15.7% (95%-CI: 10.9%-21.5%). In total 46 adverse events were recorded. Of the AEs with a severity grade provided (n = 46), more than half (52%, 24/46) were considered minor non-invasive events that required treatment but had no long-term effects. The majority of AEs (54.1%) occurred up to discharge, while 21.7% occurred between 3 months and 2 years after treatment.
Summary of Post-treatment Adverse Events (Patient Level) N = 198

Summary of Post-treatment Adverse Events According to the Time of Occurrence of the AE (AE Level) and Severity Grades
Summary of Patient Characteristics by Patients With and Without a Post-treatment Adverse Event (per Protocol Population)
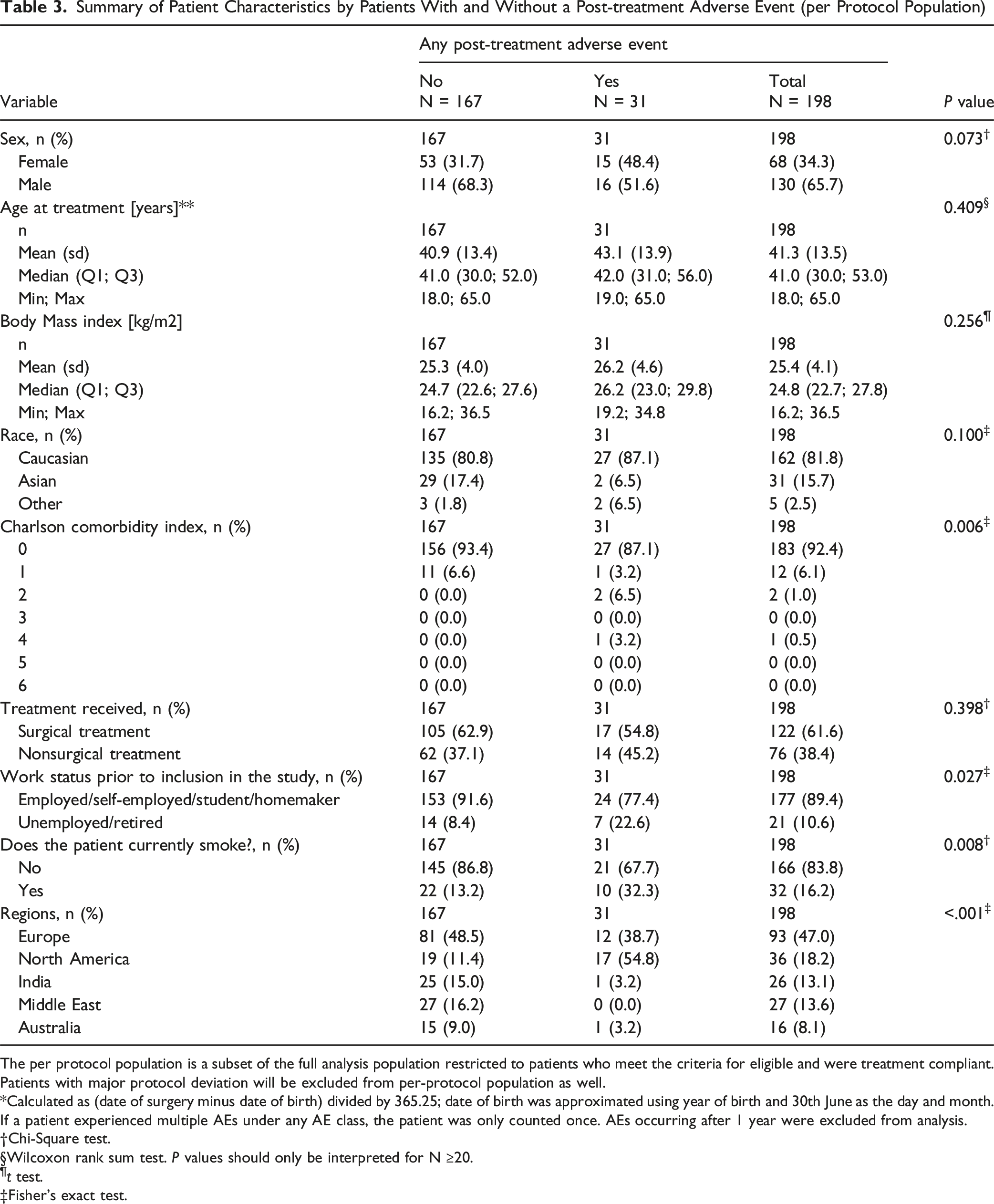
The per protocol population is a subset of the full analysis population restricted to patients who meet the criteria for eligible and were treatment compliant. Patients with major protocol deviation will be excluded from per-protocol population as well.
*Calculated as (date of surgery minus date of birth) divided by 365.25; date of birth was approximated using year of birth and 30th June as the day and month.
If a patient experienced multiple AEs under any AE class, the patient was only counted once. AEs occurring after 1 year were excluded from analysis.
†Chi-Square test.
§Wilcoxon rank sum test. P values should only be interpreted for N ≥20.
¶t test.
‡Fisher’s exact test.
17 adverse events (54.8%) were observed among patients treated surgically, while 14 adverse events (45.2%) occurred in those receiving conservative treatment (Table 3). Additionally, patients with at least one post-treatment adverse event had significantly shorter times from injury to treatment decision and to treatment initiation. No significant differences were observed in other injury characteristics and in terms of primary injury type, although patients with adverse events more often had L1 as their primary injury level.
Among the 198 patients, 5 experienced treatment failure, 3 cases in the non surgical group and 2 cases in the surgical group. Overall, these patients were more frequently male, smokers, and treated conservatively. The majority were from European centers. Treatment failure patients also had shorter times from injury to treatment decision and treatment initiation. Three of these patients had A4 fractures as their primary injury type, whereas those without treatment failure were more likely to have A3 fractures.
Adverse Events
Comparisons of ODI Values at the 6-Months, the 1-Year and at the 2-Years Follow-Up Visits Between Patients With and Without at Least One Adverse Event (per Protocol Population)
Finally, patients with treatment failure showed lower ODI values at the 6-months and the 2-years follow-up visit but higher ones at the one-year follow-up visit.
Discussion
Adverse events and treatment failures are unintentional situations that can occur during the treatment and follow up period of either conservative management or surgery in patients with thoracolumbar burst fractures. In our study, we found higher ODI values in patients with at least one post-treatment adverse events at the 6-month and 1-year follow-up visits, compared to those without such events. Interestingly, we found that over 90% of the patients without a post-treatment adverse event had ODI values of 20% or less at the 1-year follow-up, whereas only 52.6% of patients with at least one post-treatment adverse events achieved ODI values of 20% or less at this timepoint. Multiple prior patient acceptable symptom state (PASS) thresholds have been defined in the literature for ODI ranging from 5 to 25 in the spine literature while an ODI of 21 is the threshold value below which patients are considered able to cope with most activities of daily living based on the ODI’s intended interpretation. Analysis by treatment type suggested worse ODI values at the follow-up visits in both conservatively and surgically treated patients with at least one post-treatment adverse event than for patients with no adverse events. However, no significant differences were observed between conservative and surgical groups. It is worth noting that the statistically significant higher ODI might not results in clinical significant impairment, as previously mentioned, we observed an increased of 6 points in patients with AEs, while this could increase the disability, it might not imply worse clinical outcomes. Finally, the number of patients with adverse events who had available ODI values was small, thus limiting the ability to draw robust conclusions from this subgroup analysis.
Controversy in decision making in neurologically intact patients with thoracolumbar burst fractures is not only regarding clinical outcomes and functionality. Intraoperative and postoperative complications are also important metrics when considering these treatment options. The analysis of adverse events is an important metric that should be considered either in surgical or non-surgical management, these events can be associated with higher hospital length of stay, readmission, 12 increased healthcare cost and lower patient’s satisfaction. 6 Moreover, systematic reporting of negative outcomes such as adverse events and complications helps physicians and researchers to identify the prevalence and risk factors in order to improve efforts to decrease them, this is important considering the relative low rate of complications reporting in spine surgery.13,14
Comparative studies have found that the rate of complications is higher after surgical treatment, 15 in this regard, numerous complications have been reported such as postoperative infection, pseudoarthrosis, instrumentation failure and anesthetic related complications.16,17 Certain preoperative baseline patient factors have also been associated with higher risk of adverse events in the literature. Our study showed that higher CCI, smoking and unemployment or retirement were significantly associated witht the occurrence of adverse events. CCI is an effective preoperative risk stratification tool in spine surgery, 18 McGee et al found higher mortality in patients with higher CCI after cervical and thoracolumbar injuries. 19 Smoking is a known risk factor for postoperative complications such as pneumonia, 20 wound healing complications 21 and readmission. 22 Regarding employment status, literature suggest that unemployment status is associated with worse functional outcomes and disability after spine surgery. 23
Adowa et al analyzed 360 patients undergoing elective spine surgery, found longer hospital stay and higher readmission rate at 30 days in unemployed patients with no significant differences in terms of perioperative complications between employed and unemployed patients. 24
We have observed a significant geographical variation of AEs with higher report in North America, this finding could be associated with the differences of report of AEs and complications observed in the literature, in this regard, Camino-Willhuber et al. performed a systematic review of surgical outcomes in spine surgery, in this regard authors found a high rate of underreport of complications and heterogeneity when reporting negative outcomes. 13 While AEs were clearly defined in this study, variations on reporting outcomes across different regions could affect the generalization of our results. 12
Treatment failure after surgical or conservative management represent a negative result that is associated with higher costs, prolonged hospital length of stay and longer time of returning to normal daily activities. 12 Implant failure after surgical treatment has been reported in different series after short segment fixation. McLain et al reported a failure rate of 54% in 19 patients treated with SSF at six months 25 whereas Altay et al. reported no cases of implant failure after SSF. 26 Different factors have been described as predictors for treatment failure in thoracolumbar fractures such as lack of anterior support, loss of correction, implant breakage or pull out due to insufficient instrumentation. In our series, only 2 patients required unplanned surgery due to implant failure and progressive kyphosis in the surgical group. Even though different factors increase the risk of implant failure such as poor bone quality, lack of instrumentation at the index level, 27 SSF offers advantages over long fixation such as smaller incision and less implant with subsequent less operative time and is considered the preferred treatment of choice in thoracolumbar burst fractures. Regarding the impact of treatment failure on ODI, we observed lower ODI values at the 6-months and the 2-years follow-up visit but higher ones at the one-year follow-up visit. However, due to the very small sample size, these results regarding in this subgroup should be interpreted with caution. The limited statistical power may result in an inability to detect significant differences, and the potential for selection bias cannot be ruled out. As such, the findings in this subgroup should be considered preliminary and warrant further investigation in larger cohorts.
This study has some limitations, first the number of AE was relatively low and heterogenous to draw strong conclusions, on the other hand, we found association between ocurrence of AE and higher ODI in our cohort. Implant removal was not considered an AE due to the fact that it is recommended in some centres, but it could be an AE if implant removal was associated with pain or discomfort, to avoid mis interpretation we have not consider this event as an adverse event. Another limitation of this study is the lack of data regarding return to work, this finding could be helpful in expanding the discussion on this aspect and it’s relationship with AEs. Additionally, a low number of treatment failures preclude possible associations with certain type of patters (A3 vs A4) and the different surgical options.
Conclusion
Our study showed an association between the occurrence of AE and higher ODI at six months an one year of follow up, this trend appears to decrease at 2 years follow up without significant differences between groups. Subanalysis between conservative and surgical cohorts showed similar results. Additionally, a higher CCI and smoking status were associated with higher likelihood to develop AE in our cohort. Future studies should focus on the AEs analysis and their specific impact on functional outcomes.
Supplemental Material
Supplemental Material - Adverse Events and Treatment Failure in Patients With Thoracolumbar Burst Fractures Without Neurological Deficit: A Sub Analysis From Prospective Multicentric Study
Supplemental Material for Adverse Events and Treatment Failure in Patients With Thoracolumbar Burst Fractures Without Neurological Deficit: A Sub Analysis From Prospective Multicentric Study by Gaston Camino Willhuber, Charlotte Dandurand, Cumhur F Öner, Marcel Dvorak, Mohammad El-Skarkawi, Alexander R. Vaccaro, Eugen Cezar Popescu, Richard J. Bransford, Andrei Fernandes Joaquim, Harvinder Singh Chhabra, Ulrich Spiegel, Hauri Dimitri; Klaus John Schnake, Sebastian F. Bigdon, Jerome Paquet, William Lavelle, Miguel Hirschfeld, Spyros Pneumaticos, Gregory Schroeder, Lorin M. Benneker
Footnotes
Acknowledgments
We thank Olesja Hazenbiller, AO Foundation Senior Research Project Manager, for guiding and coodinating this study.
ORCID iDs
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Trauma &, a focused group of international Trauma experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through AO Network Clinical Research and the AO Innovation Translation Center, Clinical Evidence.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Authors from this study are members of the AO Spine Trauma and Infection Knowledge Forum.
Clinical Trial Registration
Patient demographics and all clinical and outcome data were taken from the observational, prospective multicenter cohort study comparing surgical vs nonsurgical treatment of TL burst fractures in neurological intact patients (An observational, multicenter cohort study comparing surgical vs nonsurgical treatment, ClinicalTrials.gov: NCT02827214). Each enrolling center obtained local approval from their local institutional review board.
Institutional Review Board Approval
Each enrolling center obtained local approval from their local institutional review board (UBC CREB NUMBER: H16-02527). Informed consent was obtained in all patients.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.