
Abstract
Study Design
Prospective Cohort Study.
Objective
This prospective observational study aimed to compare differences in the incidence of Cutibacterium acnes isolation in intervertebral discs from patients undergoing surgery for degenerative vs non-degenerative spinal pathology, and to assess differences in Modic changes and Pfirrmann grades between culture-positive and culture-negative discs.
Methods
Intervertebral disc tissue was obtained from patients undergoing discectomy or interbody fusion for degenerative pathology, or from traumatic or oncological indications without degenerative pathology. Samples were cultured for Cutibacterium acnes. MRI scans were assessed for Modic changes and Pfirrmann grades.
Results
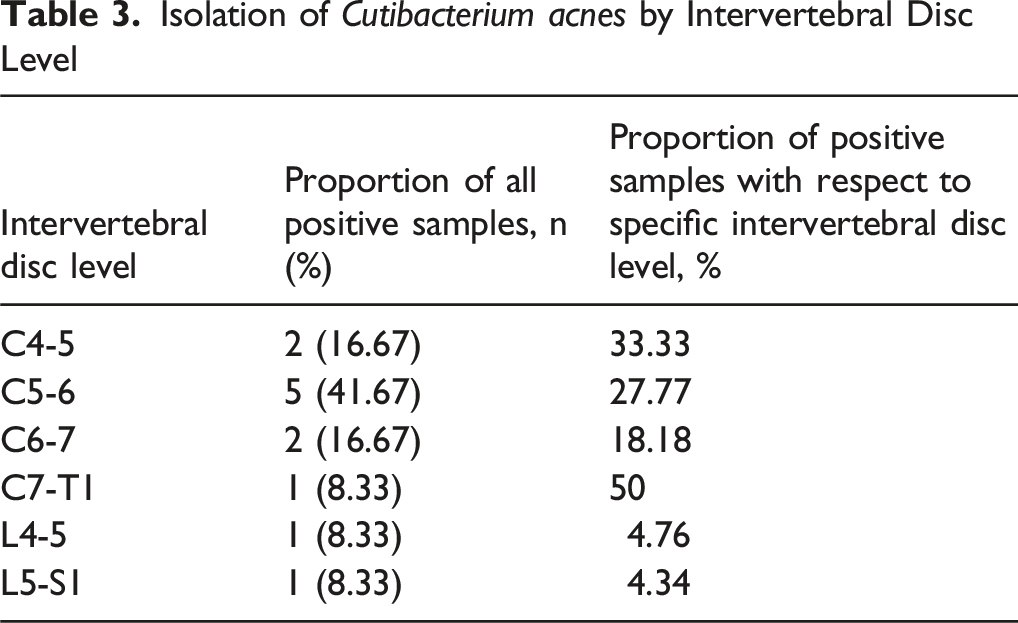
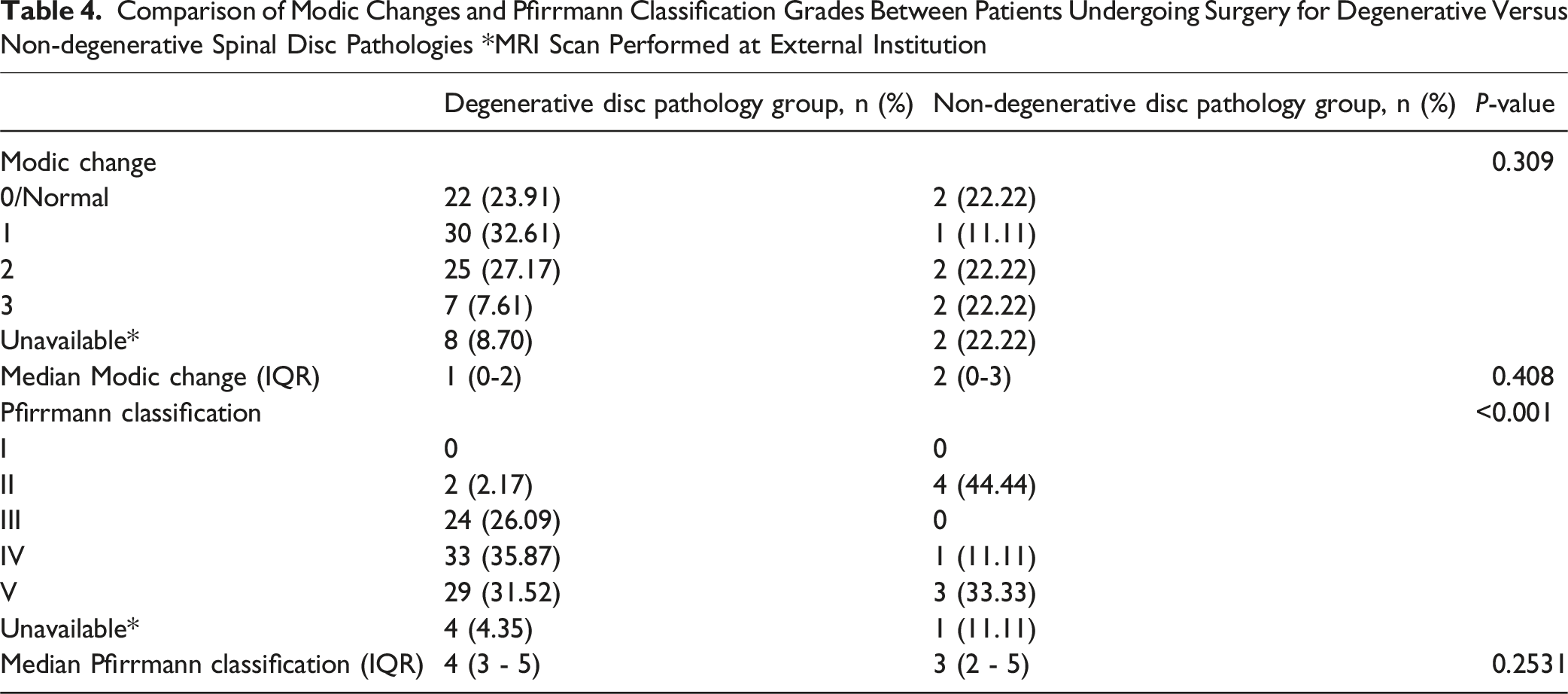
There were 92 samples (91.1%) collected from 60 patients with degenerative pathology, while nine samples were obtained from seven patients with non-degenerative pathology. Cutibacterium acnes was cultured in 10/92 (10.87%) degenerative and 2/9 (22.22%) non-degenerative samples (P = 0.338). Samples from the cervical spine had a significantly higher incidence of Cutibacterium acnes culture (25.71% vs 4.76, P = 0.002). No significant differences were observed in Modic changes and Pfirrmann grades between culture-positive and culture-negative samples in either group. Higher Pfirrmann grades were observed in the degenerative pathology patient group (P < 0.001).
Conclusion
The lack of significant differences in Cutibacterium acnes isolation between patient groups suggests that the presence of Cutibacterium acnes cultured from disc tissues is likely from contamination. This finding adds to the growing body of work examining the role of Cutibacterium acnes in degenerative disc disease, although the study is underpowered to draw firm conclusions. Further investigation involving larger patient groups is needed to build on these preliminary observations.
Keywords
Introduction
Degenerative disc disease (DDD) is a progressive spinal condition characterised by structural degeneration of the intervertebral discs. In symptomatic cases, this degeneration can manifest as localised or radiating pain, sensory disturbances, limb weakness, and impaired mobility. 1 Multiple risk factors contribute to the development of DDD including advancing age, mechanical stress, genetic predisposition, nutritional deficiencies, and lifestyle factors such as smoking and obesity.2-6 Chronic inflammation is also thought to play a role in disc degeneration, and an increasingly studied and proposed contributor to this inflammation is a low-grade bacterial infection within the disc by Cutibacterium acnes, which is an anaerobic gram-positive rod-shaped skin commensal.7,8 Many studies utilising microbiological culture and polymerase chain reaction methods have confirmed detection of Cutibacterium acnes in intervertebral disc specimens from patients suffering from a range of spinal conditions including low back pain, sciatica, disc herniation, and disc degeneration.9-12 These findings suggest that Cutibacterium acnes can colonise intervertebral discs without causing an acute infection leading to discitis, however instead inducing chronic low-grade inflammation.13,14 It has been hypothesised that Cutibacterium acnes gains access to the disc through various routes including haematogenous spread, iatrogenic introduction during surgery or injections, or local extension from adjacent tissues. It is believed that infiltration of the nucleus pulposus by Cutibacterium acnes occurs via microfissures in the annulus fibrosus and vertebral endplates, which is aided by the avascular nature of the intervertebral disc. These theories are supported by prior research that have shown that intervertebral discs that are culture-positive for microorganisms are more likely to exhibit new Modic changes, consistent with an inflammatory response to low-grade infection within the disc. 15 Furthermore, intervertebral discs are an immune-privileged site that are isolated from normal immune surveillance, potentially allowing bacteria to persist and promote inflammation. 16
However, there are also several completed studies that have failed to culture Cutibacterium acnes in patients who underwent surgery for DDD and other spinal pathology, suggesting their presence could be due to contamination.17-20 Further complicating the matter is that other studies have found that the cultured Cutibacterium acnes represents strains that are distinct from those commonly found on skin. 21 Also, Cutibacterium acnes is occasionally the sole organism cultured from disc specimens rather than part of a polymicrobial culture, suggesting its identification is likely to be due to contamination. 9 Thus, the potential role of Cutibacterium acnes in the pathogenesis of DDD remains an area of active investigation. There is a paucity of studies that have evaluated the presence of Modic and Pfirrmann changes in patients who underwent spinal surgery with culture-positive Cutibacterium acnes isolated from disc specimens. Additionally, even fewer studies have compared the incidence of Cutibacterium acnes isolation between patients who underwent surgery for degenerative vs non-degenerative spinal conditions. Addressing this gap in the literature provides further insights into the clinical significance of Cutibacterium acnes and its potential role in disc degeneration.
This study aimed to compare: i. the incidence of Cutibacterium acnes isolated from intervertebral tissue samples in patients undergoing surgery for degenerative vs non-degenerative spinal pathology ii. the presence and type of Modic changes and Pfirrmann grading between intervertebral discs that were culture-positive and culture-negative for Cutibacterium acnes iii. the presence and type of Modic changes and Pfirrmann grading in culture-positive vs culture-negative intervertebral discs among patients undergoing surgery for degenerative compared to non-degenerative spinal pathology
Methods
Study Design and Eligibility Criteria
This was a single-centre, prospective observational study conducted at a tertiary referral center between October 2019 and September 2020. Inclusion criteria were patients undergoing spinal surgery involving discectomy or interbody fusion at any vertebral level, provided the indication was not infective. Patients with disc degeneration undergoing surgery for conditions including disc herniation, spinal canal stenosis, scoliosis, or spondylolisthesis were compared to those undergoing surgery for traumatic or oncological indications, in whom there was no evidence of disc degeneration on magnetic resonance imaging (MRI) as assessed using the Pfirrmann classification. Based on this criteria, patients were categorised into two groups according to whether surgery was performed for degenerative or non-degenerative spinal pathology. Patient eligibility and group allocation was confirmed by a combination of clinical assessment and imaging analysis. The study was approved by the Research Subjects Review Board at our institution.
Assessment of Modic Changes and Pfirrmann Grading System
MRI is routinely performed pre-operatively at our institution. The imaging protocol included T1-and T2-weighted sequences in the sagittal, coronal, and axial planes, as well as short tau inversion recovery (STIR) sequences. These images were analysed to assess the grading of Modic changes at the superior and inferior vertebral endplates, and Pfirrmann classification for each intervertebral disc that was operated on. This radiological assessment was performed by the senior author and two research fellows.22-24 The following epidemiological and clinical data were collected from hospital records: age, sex, race, and surgical indication. Written informed consent was obtained from all participants.
Collection of Intervertebral Disc Tissue Specimens and Microbiological Culture
The surgical site was prepped and draped using standard sterile technique. Perioperative antibiotics were administered to the patient prior to skin incision, in accordance with institutional protocol. During the surgery, samples of intervertebral disc tissue were obtained during the disc removal stage and were collected into sterile collection tubes. In cases involving multilevel surgery, separate specimens were collected at each operated level. Tissue specimens were handled using sterile techniques to minimise the risk of contamination and were subsequently transferred to the department of microbiology at the University of Rochester School of Medicine and Dentistry for culturing for Cutibacterium acnes. Tissue samples were initially homogenised and then inoculated onto three anaerobic agar media including Wilkins-Chalgren agar, Columbia blood agar, and LB (Luria-Bertani) agar. The plates were incubated at 37°C under strict anaerobic conditions. Cultures were monitored for 14 days to accommodate the slow-growing nature of Cutibacterium acnes. Suspected colonies were identified based on their characteristic morphology and confirmed by Gram staining.
Statistical Analysis
Categorical variables are summarised as frequencies and percentages, and analysed using Chi-squared or Fisher’s exact tests. Odds ratios (OR) are also presented for comparisons involving categorical values. Parametric data were reported using mean and standard deviation, and analysed using two-sided unpaired t-tests. Non-parametric data was reported as median and interquartile range (IQR), and analysed using independent samples Mann–Whitney U test. Depending on the specific comparison, the unit of analysis was either the participant or the individual intervertebral level. 95% confidence intervals are presented, and statistical significance was set at P < .05. Analyses were performed using Stata software (version 18.0, StataCorp LLC, College Station, Texas, USA, 1985-2023).
Results
Patient Characteristics
There were a total of 101 intervertebral disc samples among 67 patients (34 female and 33 male) who underwent surgery. Of these, 92 samples (91.1%) were obtained from 60 patients who underwent surgery for degenerative spinal disc pathology, while the remaining nine samples were collected from seven patients who underwent surgery for non-degenerative spinal disc pathology.
The median age at the time of surgery was 60 years (IQR 59-72) in the degenerative spinal pathology patient group and 52 years (IQR 38.5-61) in the non-degenerative spinal pathology patient group (P = .118). Most participants were White (n = 59; 88.06%), with the remainder comprising five Black (7.46%), one Asian (1.49%), and two Hispanic/Latino (2.99%) participants. There were no significant differences in racial distribution between patient groups (P = .980).
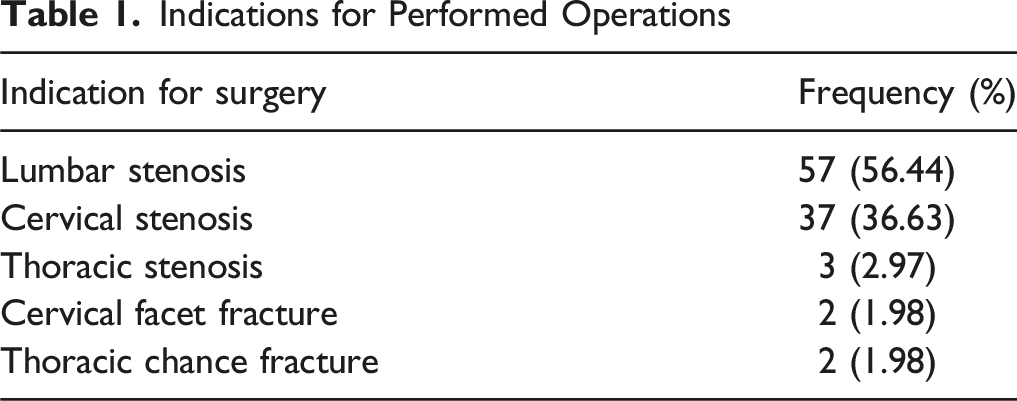
Indications for Performed Operations
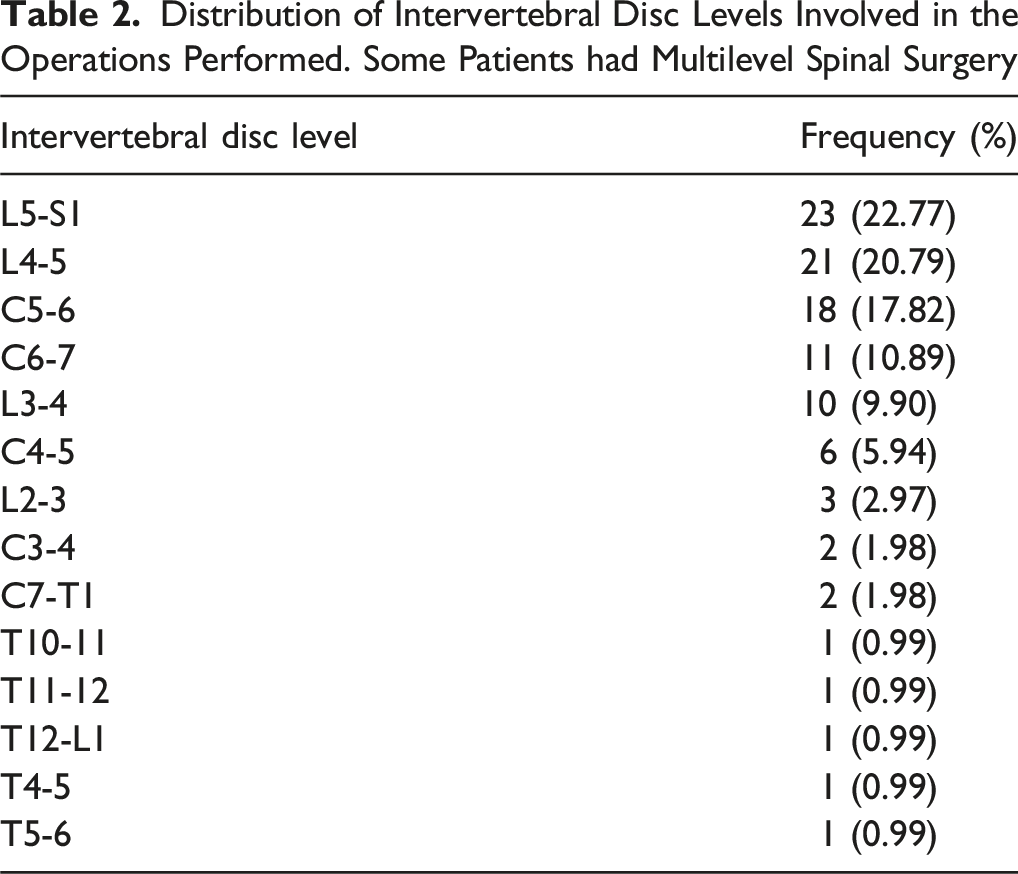
Distribution of Intervertebral Disc Levels Involved in the Operations Performed. Some Patients had Multilevel Spinal Surgery
Cutibacterium acnes Microbiological Culture
Isolation of Cutibacterium acnes by Intervertebral Disc Level
Modic Changes and Pfirrmann Classification Grades
Comparison of Modic Changes and Pfirrmann Classification Grades Between Patients Undergoing Surgery for Degenerative Versus Non-degenerative Spinal Disc Pathologies *MRI Scan Performed at External Institution
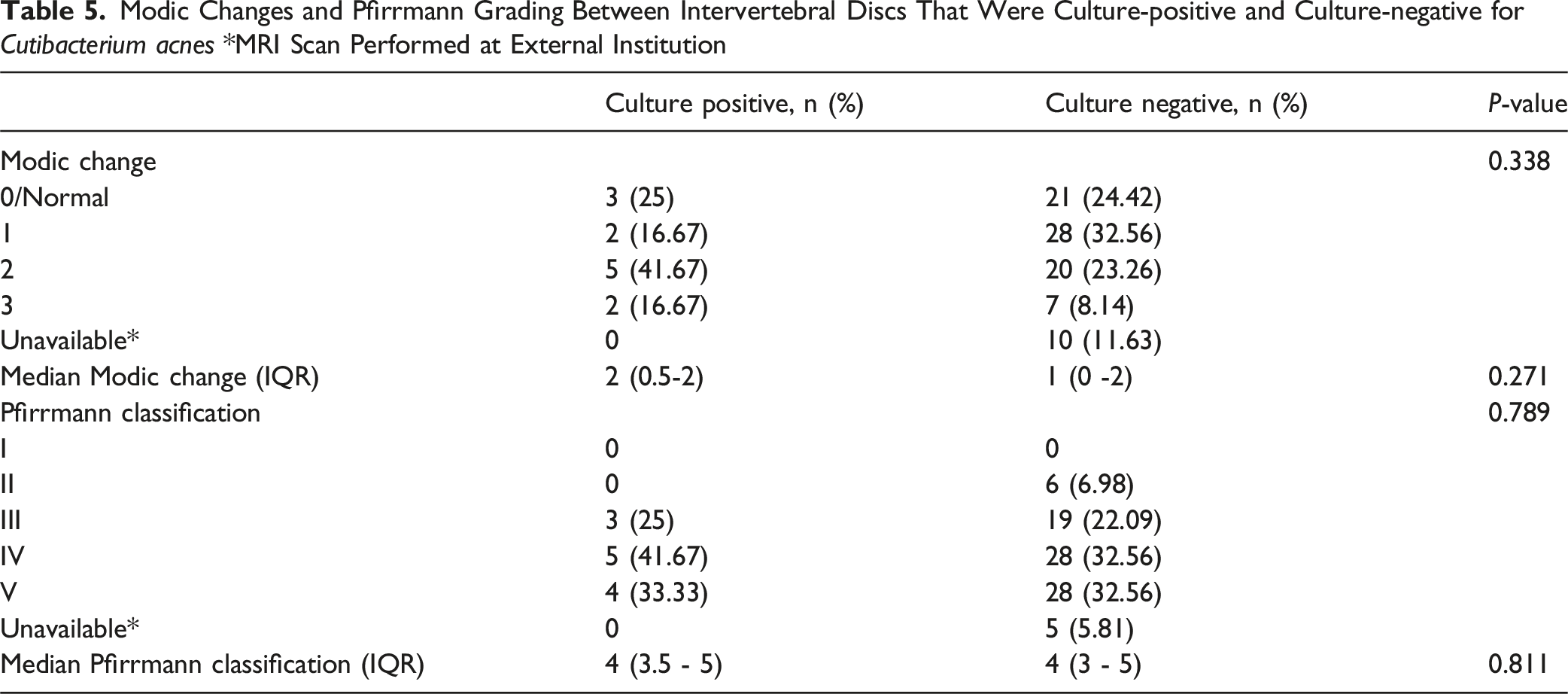
Modic Changes and Pfirrmann Grading Between Intervertebral Discs That Were Culture-positive and Culture-negative for Cutibacterium acnes *MRI Scan Performed at External Institution
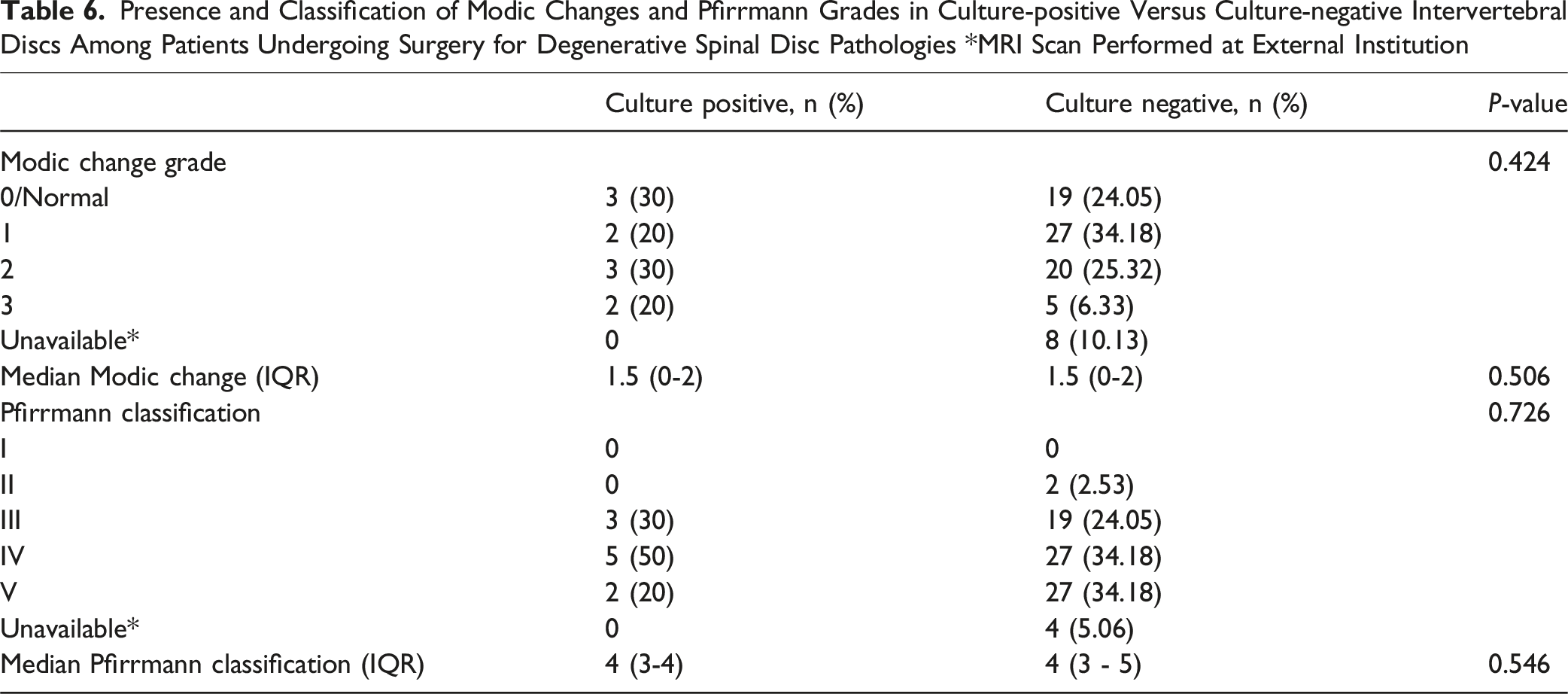
Presence and Classification of Modic Changes and Pfirrmann Grades in Culture-positive Versus Culture-negative Intervertebral Discs Among Patients Undergoing Surgery for Degenerative Spinal Disc Pathologies *MRI Scan Performed at External Institution
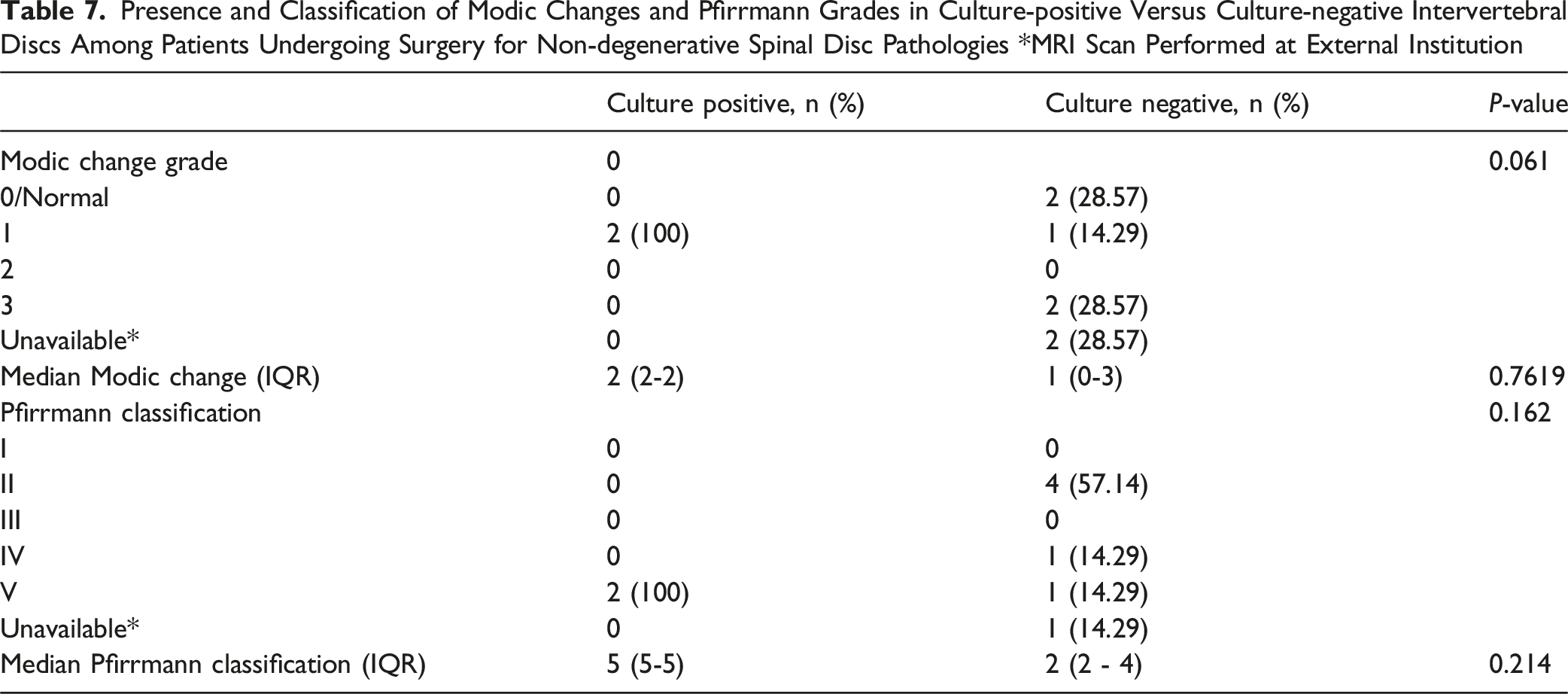
Presence and Classification of Modic Changes and Pfirrmann Grades in Culture-positive Versus Culture-negative Intervertebral Discs Among Patients Undergoing Surgery for Non-degenerative Spinal Disc Pathologies *MRI Scan Performed at External Institution
Discussion
Our study found that Cutibacterium acnes was cultured from a minority of intervertebral disc samples, with no significant difference in its detection between patients with degenerative and non-degenerative spinal pathology. Samples taken from operations involving the cervical spine had a relatively higher incidence of positive cultures of Cutibacterium acnes compared to other regions of the spine. Furthermore, there was no differences between Cutibacterium acnes culture status and Modic changes and Pfirrmann grading. This finding persisted when the degenerative and non-degenerative patient groups were analysed separately. As expected, Pfirrmann grades were significantly higher in the degenerative spinal pathology groups, supporting the internal validity of our study’s methods. However, there were no significant differences in Modic changes between the two patient groups. Collectively, these findings suggest that the presence of Cutibacterium acnes in disc cultures is more likely due to contamination rather than a true pathogenic role in degenerative disc disease.
The existing literature on this topic is conflicting, with some studies supporting our findings. Schmid et al. assessed 30 intervertebral disc samples from patients presenting with disc degeneration or herniation and reported a similar proportion of positive samples of Cutibacterium acnes (10%). 25 In another study, only two of 54 patients (3.7%) who underwent surgery for lumbar disc herniation were found to have grown Cutibacterium acnes from disc fragments. However, a higher proportion of patients (18.5%) had Cutibacterium acnes detected in samples taken from surrounding tissues including the ligamentum flavum and muscle, or even from the laminar flow machine in the laboratory, raising concerns regarding the cause of growth being contamination. 26 With respect to Modic changes, Rigal et al. evaluated MRI scans and microbiological cultures of 385 samples from 313 patients undergoing lumbar spine fusion or disc arthroplasty for chronic low back pain, and found no correlation between bacterial growth and disc degeneration. 27 Notably, all procedures in their study were performed using an anterior rather than posterior approach, which involves surgical access through an area with lower Cutibacterium acnes colonisation and may explain the very low number of culture positive (0.52%). Consistent with our findings regarding Modic changes, other studies have also reported no association between Modic changes and growth of Cutibacterium acnes or other bacteria.11,28 These findings support our study’s conclusion that Cutibacterium acnes cultured from disc tissue samples is most likely due to contamination. The relatively higher incidence of Cutibacterium acnes isolation in cervical spine samples may be attributed to regional variation in the density of sebaceous glands on the body, which create a favourable environment for Cutibacterium acnes colonisation, with the upper back and neck containing some of the highest gland densities. 29 This suggests that the risk of contamination risk may correlate with local sebaceous gland density.
The strengths of our study include the evaluation of multiple outcomes, including the presence of Cutibacterium acnes, Modic changes, and Pfirrmann grades, using data obtained from clinical, microbiological, and radiological assessments. This multidimensional approach enabled a comprehensive evaluation of whether bacterial isolation correlates with the severity of disc degeneration or MRI indicators of inflammation. In contrast to most previous studies that limited their analysis to a specific region of the spine and focussed solely on patients with type 1 Modic changes, our study encompassed all spinal levels and evaluated Modic types 1, 2, and 3. Moreover, while prior studies focussed solely on patients with degenerative spinal pathology, we also included individuals with non-degenerative conditions, such as those with acute fractures and malignancy. This approach enabled a direct comparison between the two groups to better explore whether Cutibacterium acnes has a pathogenic role in degenerative disc disease. This constitutes a more rigorous methodological approach that improved the validity of the study’s findings and addressed one of the biggest limitations in prior literature on this topic. To minimise the risk of false-negative cultures, disc samples were inoculated onto three different types of culture media and incubated for 14 days to allow sufficient time for Cutibacterium acnes to grow.
However, there are also limitations to this study. Patients undergoing surgery for non-degenerative spinal pathology are less common than those with degenerative conditions, resulting in a smaller sample size in the non-degenerative pathology patient group. This has implications on statistical power and generalisability of the observed findings. Recruitment was further affected by the COVID-19 pandemic, which contributed to the reduced number of participants in this cohort. The radiological assessment of Modic changes and Pfirrmann grades is open to subjectivity. Furthermore, this was performed by three reviewers who were not blinded, each of whom reviewed different scans, which precluded assessment of inter-rater reliability and may have introduced bias. The use of more sensitive detection methods, such as polymerase chain reaction (PCR), might have provided additional insights into our findings. However, these techniques could also have confounded interpretation, as PCR detects both viable and non-viable Cutibacterium acnes. This may lead to false-positive results that overestimate the organism’s true presence within disc tissue and obscure its relevance in the context of our research. In contrast, standard culture methods are less prone to these limitations, since they identify only viable organisms capable of growth. Lastly, the study focussed exclusively on Cutibacterium acnes only and did not evaluate the growth of other micro-organisms or explore potential correlations between pre-operative clinical outcomes and growth of Cutibacterium acnes.
This study found no significant differences in the incidence of Cutibacterium acnes isolation between degenerative and non-degenerative groups, or between culture-positive and culture-negative discs in relation to Modic changes or Pfirrmann grades. This potentially suggests that the isolation of Cutibacterium acnes from disc samples may more likely reflect contamination rather than true infection. These findings add to the growing body of evidence that challenges the hypothesis that Cutibacterium acnes plays a pathogenic role in the development of degenerative disc disease. Given the limitations of this study, particularly the small sample size of patients undergoing surgery for non-degenerative disc pathology, this study’s findings should be interpreted cautiously, and confirmation in larger studies is needed. Nonetheless, this study represents a valuable stepping stone, offering further evidence that does not support an association between Cutibacterium acnes and degenerative disc disease, and encourages research exploring alternative explanations and mechanisms contributing to this pathology.
Footnotes
Acknowledgements
URMC Department of Orthopaedics Clinical Coordinators and Research Staff.
Ethical Consideration
No informed consent was required. IRB approved through the University of Rochester Medical Center (URMC) Institutional Review Board (STUDY00000577)
Author Contributions
Authors S.G, A.M, E.M contributed to curation and supervision of the study. Authors M.F, L.B, N.M, A.P, P.G, M.B completed data collection/analysis and manuscript formulation. Authors M.F, L.B, N.M, A.P, P.G, K.Y, J.J, M.E supported editing and submission of the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Goldstein Award at the University of Rochester School of Medicine and Dentistry.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Addisu Mesfin following conflict of interest: Grants from Nuvasive, OREF grant, Depuy speaking fees, Globus consulting. The remaining co-authors have no conflict of interest to declare.
Data Availability Statement
Data is available upon reasonable request to the corresponding author.