
Abstract
Study Design
Single-center retrospective comparative study.
Objective
While vitamin D (VD) levels are known to correlate with outcomes in lumbar degenerative disease (LDD), it remains unclear whether LDD is related to elevated risk of VD deficiency. This study aimed to compare the prevalence and epidemiological characters of VD deficiency between surgical LDD patients and health screening (HS) populations.
Methods
7300 HS participants and 1147 surgical LDD patients were included. All participants accepted serum VD test. In both HS participants and LDD patients, the epidemiological characteristics and influence factors of VD deficiency were analyzed. Propensity score matching was used to create a matched healthy control group, and the prevalence of VD deficiency was further compared.
Results
66.9% of HS participants and 42.9% of LDD patients were with VD deficiency. Age, sex, BMI and season were influence factors of VD deficiency in both groups. As age grows, the VD levels increase in young age and decrease in older age after the peak. Female, high BMI and Winter/Spring season were risk factors of VD deficiency. Compared with matched control group, LDD group exhibited statistically higher median VD levels than controls [median (interquartile range), 21.6 (16.3, 27.9) vs 19.3 (15.0, 25.3), P < 0.001]. However, the prevalence of VD deficiency was not significantly different between the matched groups.
Conclusion
LDD does not appear to be associated with an elevated risk of VD deficiency. Compared with the HS cohort, surgical LDD patients exhibit similar epidemiological patterns of VD levels, including an unusual biphasic relationship with age.
Keywords
Introduction
Lumbar degenerative diseases (LDD), one of the most prevalent musculoskeletal disorders, frequently coexists with osteoporosis, with reported prevalence rates of comorbid osteoporosis ranging from 31.3% to 74% in LDD patients.1-3 Vitamin D (VD), a steroid derivative, has been reported to have a wide range of physiological functions and played an important role in bone metabolism and the maintenance of skeletal health. 4 Consequently, the lack of VD could lead to bone loss and higher risk of osteoporosis in adults.5,6
Given the close correlation between VD and bone health, several studies explored and reported the associations between VD levels and the clinical outcomes of LDD.7-15 While this suggests a link between VD and LDD prognosis, it remains controversial whether individuals with LDD are more susceptible to concomitant VD deficiency. This question is complicated, as even in the general population, VD insufficiency demonstrates a high prevalence rate. A number of epidemiological studies of VD deficiency has been performed in different study populations.16-21 In a pooled analysis of 7.9 million participants, the prevalence of VD deficiency was reported to be 44.7%, indicating VD deficiency as a common disorder globally. 16 Therefore, this high background prevalence complicates any effort to determine the specific impact of LDD.
Furthermore, the prevalence of VD deficiency demonstrates marked heterogeneity across studies, 16 which is attributable to variations in study population demographics, geographic factors and local lifestyles etc. In LDD patients, similar variations have also been reported, the prevalence of VD deficiency varies ranging from 11.2% to 74.3%,8-14 and most previous studies merely included LDD patients without a comparable “normal” cohort. Considering such great differences of VD deficiency, existing studies could barely show if LDD patients presented different VD levels comparing to the general population. Therefore, to better understand the relationship between LDD and prevalence of VD deficiency, a well-designed comparable study between LDD patients and a matched healthy cohort is essential.
In this study, a large sample of health screening (HS) individuals and patients undergoing surgical treatment for LDD were included. The study analyzed the epidemiological characteristics of VD deficiency across different populations and compared its prevalence between the groups. This research is expected to provide updated insights into the epidemiology of VD deficiency in both HS and patient populations, and also to improve our understanding of the correlation between VD deficiency and LDD.
Materials and Methods
Study Design
This was single-center retrospective study performed in Beijing, China. Due to its retrospective nature, the informed consent was waived within the permission of the ethnics committee. The study was approved by the ethics committee of our hospital, and was conducted within the principles of the Declaration of Helsinki.
Participants
This study included both local HS participants and consecutive patients who underwent lumbar surgery for LDD in our center with the following criteria.
HS Participants
Inclusion criteria: (1) aged over 18; (2) with complete demographics and medical history needed in this study; (3) accepted HS in our medical center in 2024 with results of VD level testing; Exclusion criteria: (1) Presence or history of severe endocrine or metabolic diseases affecting VD metabolism (eg, parathyroid disorders, severe renal insufficiency); (2) History or current use of VD supplements or other drugs that may affect VD level; (3) history or presence of any diagnosed spinal diseases.
Patients
Inclusion criteria: (1) aged over 18; (2) with complete demographics and medical history needed in this study; (3) diagnosed as lumbar degenerative diseases accepted surgical treatment in our center from 2022 to 2024, with routinely preoperative VD level testing. Exclusion criteria: (1) Presence or history of severe endocrine or metabolic diseases affecting VD metabolism; (2) Patients who received relevant medications for osteoporosis or VD deficiency but lacked baseline VD data; (3) Patients who orally consumed VD supplements for health maintenance purposes but had not been previously diagnosed with bone metabolism disorders or VD deficiency; (4) with non-degenerative spinal diseases including tumor, tuberculosis, ankylosing spondylitis, severe fracture etc.
Baseline Data Collection
The baseline data of the participants were collected, including age, sex, body mass index (BMI), medical history and time of accepting VD testing in the HS system and in-patient system of the hospital. According to the city’s climate, the seasons were defined as following: spring (March to May), Summer (June to August), Autumn (September to November) and Winter (December to February).
VD Level Evaluation
All participants accepted the serum VD (25-hydroxyvitamin D) testing in our center. The test was performed using a fully automated Elecsys Vitamin D total chemiluminescence immunoassay analyzer (Roche Diagnostics GmbH, Pleasanton, CA, USA). Especially, for LDD patients who accepted VD supplementation therapy preoperatively, the initial serum VD before therapy was recorded. The VD deficiency was diagnosed as the following 22 : Severe Deficiency: VD ≤ 10 ng/mL; Mild Deficiency: 10 ng/mL <VD ≤ 20 ng/mL; VD Insufficiency: 20 ng/mL < VD ≤30 ng/mL; VD Sufficiency: VD > 30 ng/mL.
Statistical Analysis
Statistical analysis was performed using SPSS version 26.0 (SPSS Inc., Chicago, IL, USA) and R version 4.1.2. (R Foundation, Vienna, Austria, https://www.r-project.org). Due to the non-normal distribution of VD levels, the serum VD levels were shown in form of median (first quartile, third quartile), and other demographics statistics were shown as mean ± standard deviation with the 95% confidence intervals (CI) of mean value. Numerical statistics including age, BMI were compared between different subgroups using t-test or analysis of variance, and category statistics including sex, season were compared using Chi-square test. The serum VD levels were compared using Kruskal-Wallis test (among 3 or more subgroups) and Mann-Whitney U Test (between 2 subgroups). The median difference of VD was estimated using Hodges-Lehmann Estimator. The relationship between age, BMI and VD were analyzed using locally estimated scatterplot smoothing model, and multivariate linear regression was used to analyze the influence factors of VD levels. Propensity score matching (PSM) was used to match participant with 1:1 ratio from the patient group and the HS group using the nearest neighbor algorithm. Statistical significance was set at the level of P < 0.05.
Results
Demographics
The Demographic Data of the Cohort
BMI, body mass index; LDH, lumbar disc herniation; LSS, lumbar spinal stenosis; DLS, degenerative lumbar spondylolisthesis.
aIn form of mean ± SD [95% confidence interval of mean]
bWith statistically significant difference among different VD levels.
cIn form of median (first quartile, third quartile).
Baseline Data of HS Group and Patient Group With Different VD Levels
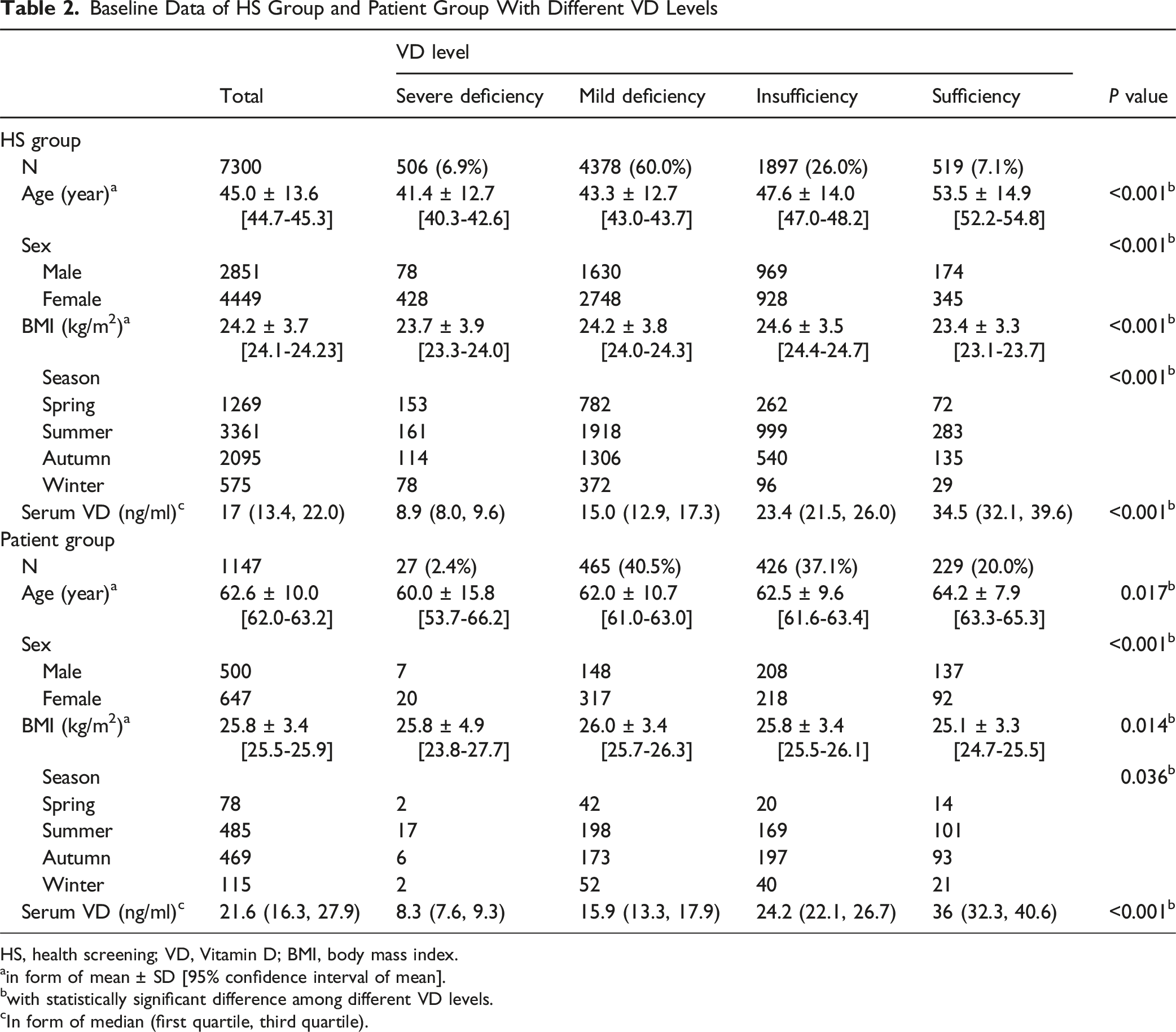
HS, health screening; VD, Vitamin D; BMI, body mass index.
ain form of mean ± SD [95% confidence interval of mean].
bwith statistically significant difference among different VD levels.
cIn form of median (first quartile, third quartile).
Potential Influence Factors of VD Deficiency
The potential influence factors of VD deficiency were compared among subgroups with different VD deficiency levels, as shown in Table 2. Generally, all of age, sex, BMI and season of examination were significantly different among different VD subgroups, no matter in HS group or patient group.
Relationship Between Age and Serum VD Levels
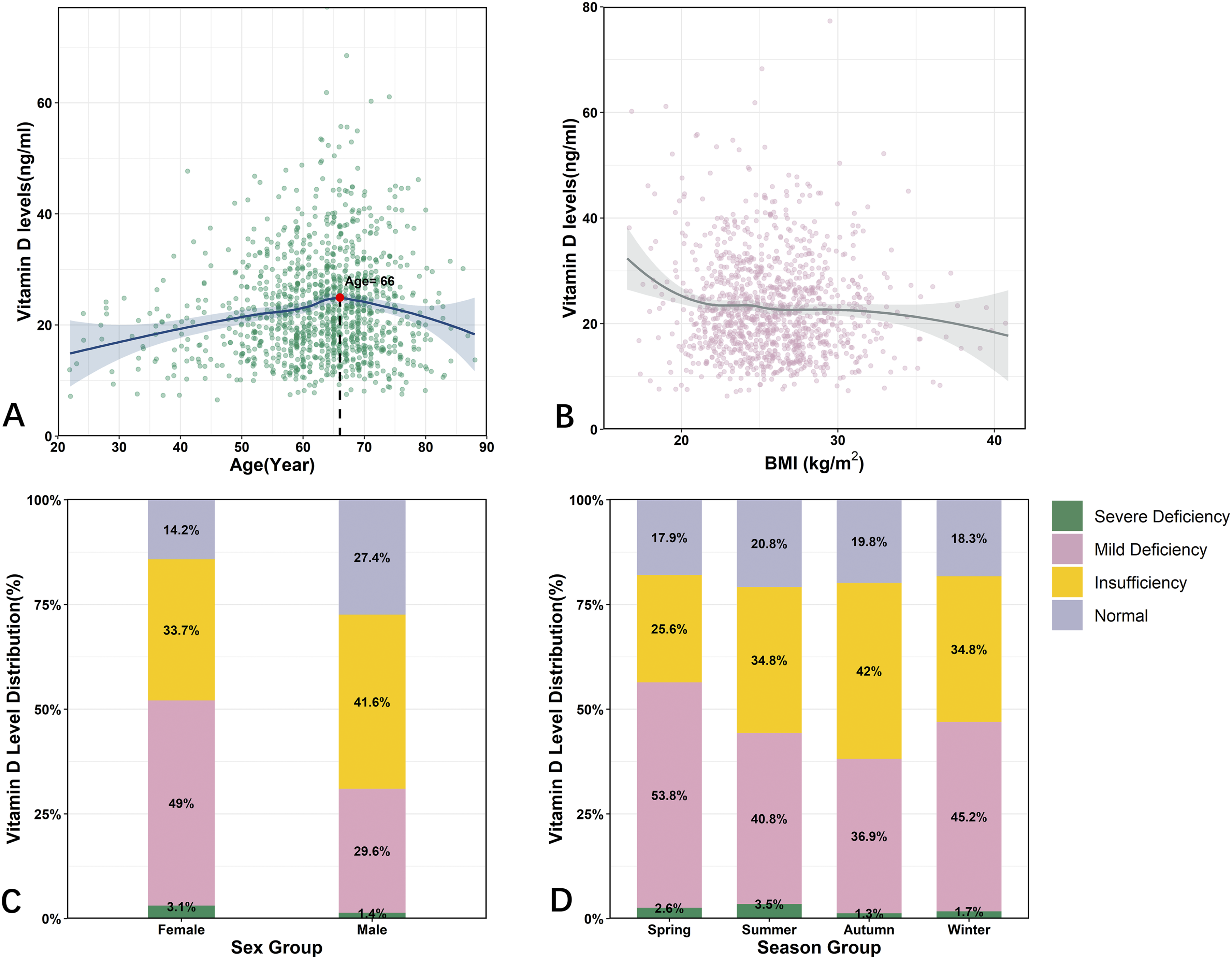
From normal VD group to severe VD deficiency group, the average age decreased with statistically significant difference in both HS group and patient group (P < 0.001). However, the relationship between age and serum VD levels was not monotonic. In HS group, the non-linear fitting model in Figure 1A showed that serum VD level increased as age grown initially, followed by a declining trend after the age of 72 years. Also, in patient group, a similar pattern was observed with VD levels peaking at 66 years (Figure 2A). The Epidemiological Characteristics of VD Levels in HS Population. (A) The Scatter Plots of VD and Age. The Non-linear Regression Model Presents a Biphasic Correlation With Peak Age at 72 Years. (B) The Scatter Plots of BMI and VD. (C) The Prevalence of Different VD Deficiency Levels Between Males and Females. (D) The Prevalence of Different VD Deficiency Levels in Different Season Groups The Epidemiological Characteristics of VD Levels in LDD Patients. (A) The Scatter Plots of VD and Age. The Non-linear Regression Model Presents a Biphasic Correlation With Peak Age at 66 Years. (B) The Scatter Plots of BMI and VD. (C) The Prevalence of Different VD Deficiency Levels Between Males and Females. (D) The Prevalence of Different VD Deficiency Levels in Different Season Groups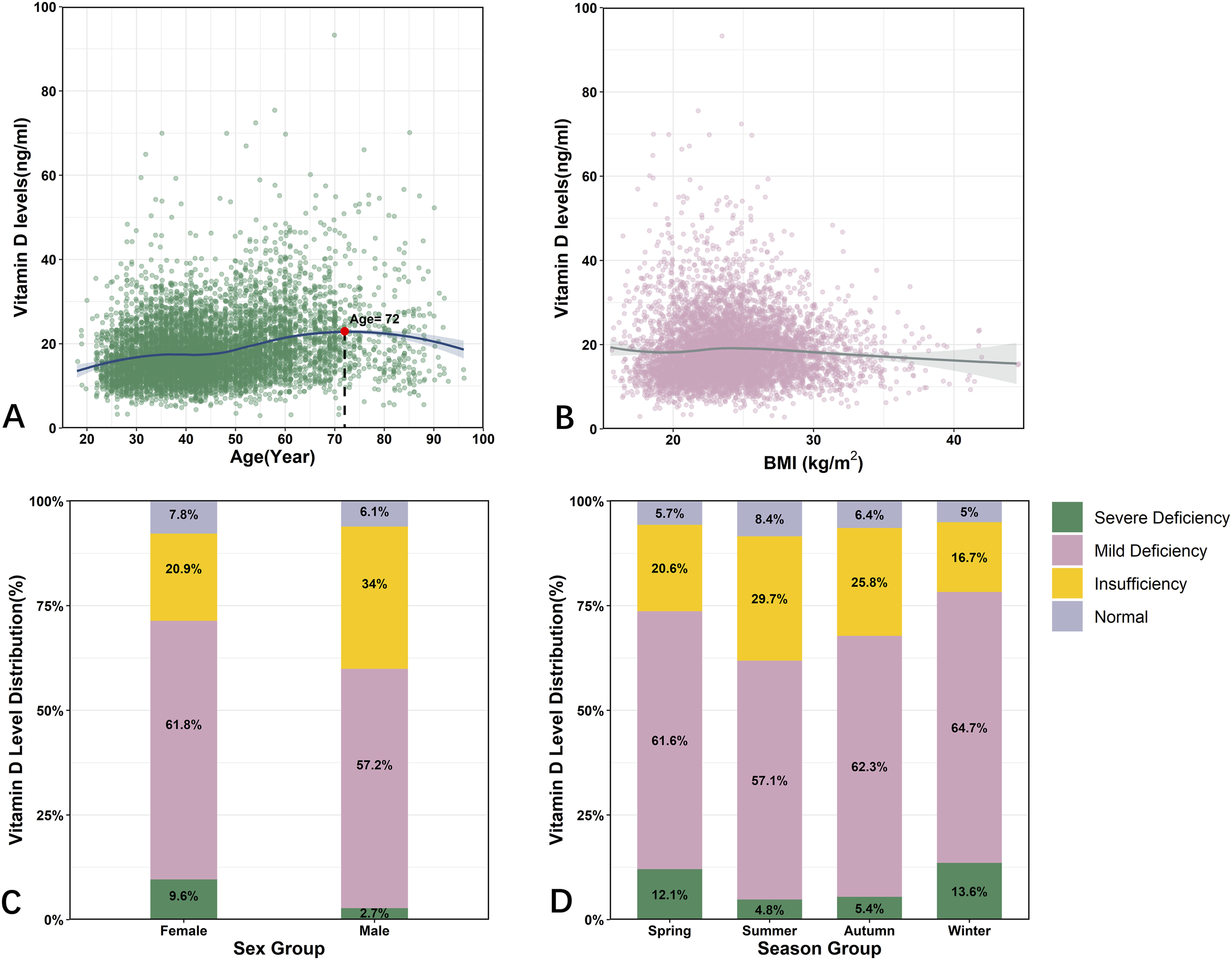
Relationship Between Sex and Serum VD Levels
There were significant differences in the prevalence of VD deficiency between males and females. In the HS group, females had a higher prevalence of both severe (9.6% vs 2.7%) and mild (61.8% vs 57.2%) VD deficiency compared to males. Conversely, VD insufficiency was less common in females (20.9% vs 34%), while the proportion of participants with normal VD levels was similar (7.8% in females vs 6.1% in males) (Figure 1C). In patients, although there were still higher prevalence of severe and mild VD deficiency and less VD insufficiency participants in females, the proportion of normal VD levels was significantly higher in males (27.4% vs 14.2%) (Figure 2C). Overall, males exhibited higher VD levels in both HS and patient groups, with this sex difference being more pronounced among patients.
BMI and Season Effect on VD Levels
Among the different VD deficiency groups, although statistically significance was observed in both HS (P < 0.001) and patient group (P = 0.014), the numerical differences were minimal (Table 2). Similarly, the variation in VD levels with BMI was relatively small, as illustrated in Figures 1B and 2B. Moreover, the distribution of VD deficiency subgroups was significantly different among different seasons in both HS (P < 0.001) and patient group (P = 0.036). Higher prevalence of severe and mild VD deficiency was observed in Spring and Winter in HS group, and there was a correspondingly higher prevalence of VD insufficiency and normal VD in Summer and Autumn (Figure 1D). In contrast, in the patient group, the proportions of normal VD and severe deficiency were similar, with a higher prevalence of mild VD deficiency and a lower prevalence of VD insufficiency in Spring and Winter (Figure 2D).
Multivariate Linear Regression Analysis of Potential Influence Factors
Multivariable Linear Analysis of Potential Influence Factors Affecting Serum Vitamin D Levels
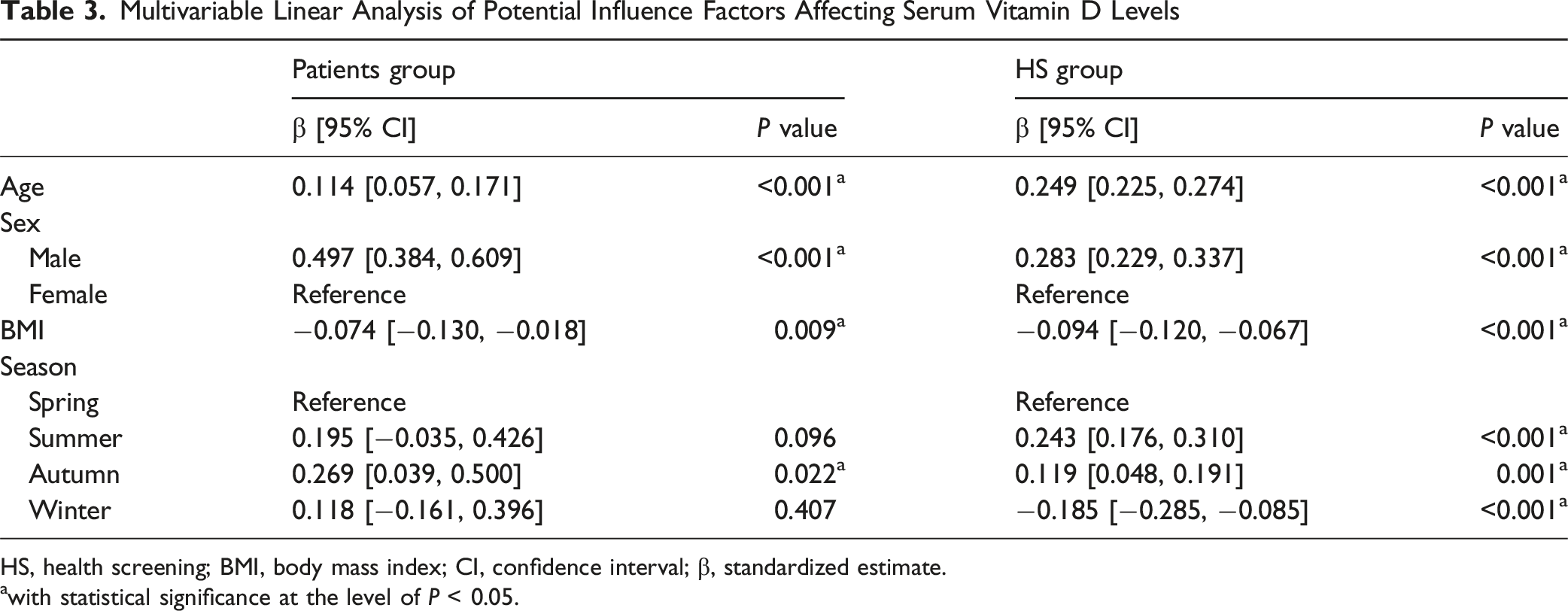
HS, health screening; BMI, body mass index; CI, confidence interval; β, standardized estimate.
awith statistical significance at the level of P < 0.05.
Variations in the Prevalence of VD Deficiency in Patients and HS Participants
To compare the prevalence of VD deficiency between patients and HS participants, a matched-control group were established within the HS participants based on age, sex, BMI and season. Finally, 1136 participants were 1:1 matched between patient group and HS group. Comparing the matched patient group and control group, no statistically significant differences were found in sex, age and season. Although BMI differed between the groups (mean difference 0.3[0, 0.6] kg/m2, P = 0.029), it was not considered clinically relevant due to its minimal numerical difference.
Comparison of Baseline Data and VD Levels Between Patient Group and Matched Control Group
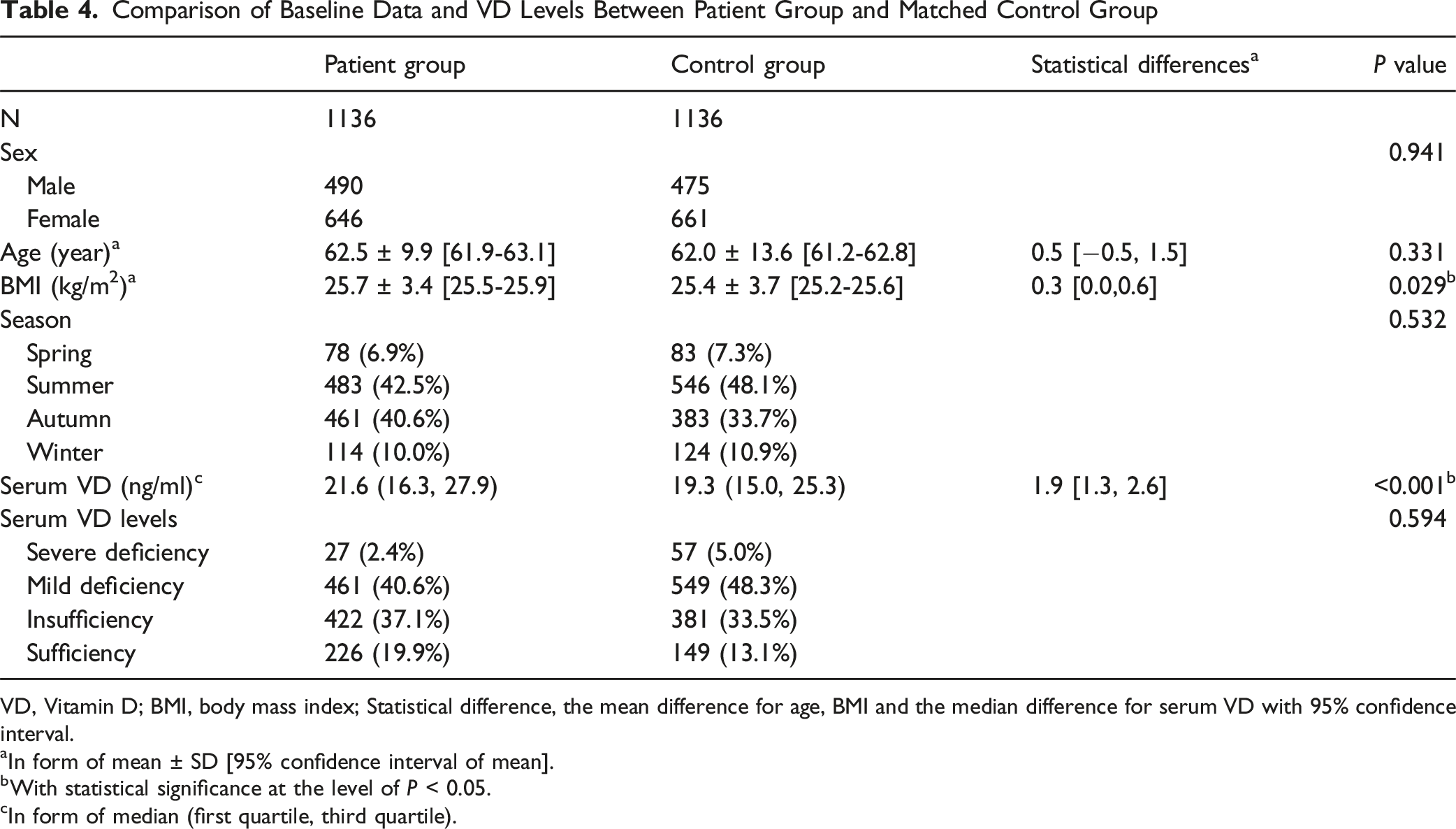
VD, Vitamin D; BMI, body mass index; Statistical difference, the mean difference for age, BMI and the median difference for serum VD with 95% confidence interval.
aIn form of mean ± SD [95% confidence interval of mean].
bWith statistical significance at the level of P < 0.05.
cIn form of median (first quartile, third quartile).
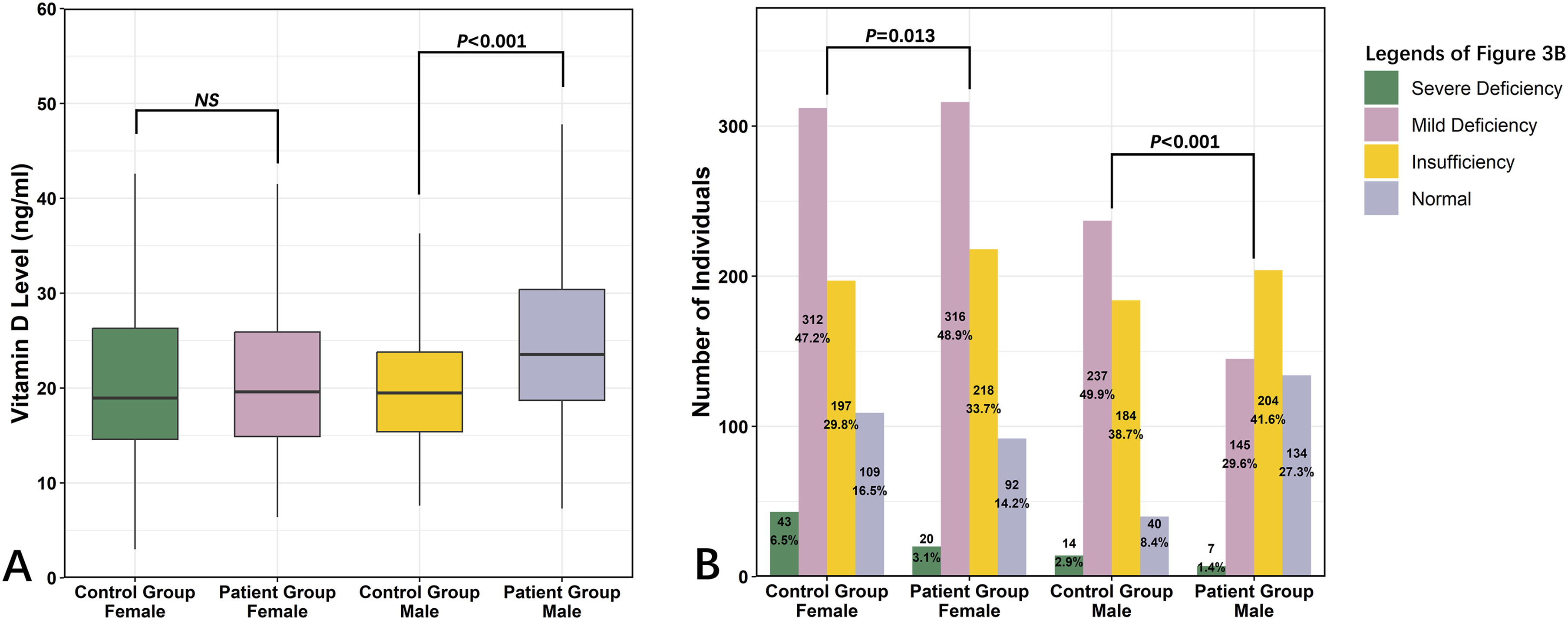
The Differences of VD Levels Between LDD Patients and Matched Control Group in Different Sex Group. (A) The Box Plot Showed the Comparison of Serum VD Levels in Different Sex Groups. There Were Significant Differences in Males Between Patients and Control Group, and No Statistical Difference was Found in Females. (B) The Prevalence of 4-Level VD Deficiency Gradings in Different Groups. Statistically Significant Differences Were Found Between Patients and Control Group in Both Males and Females
Discussion
While a high prevalence of VD deficiency and its clinical relevance were well-documented in LDD patients,7-15 VD deficiency is not exclusive to LDD patients but is also prevalent in the general population. Consequently, whether LDD patients exhibit a greater susceptibility to concomitant VD deficiency remains inconclusive, primarily due to the lack of comparative studies evaluating VD status between LDD patients and general populations. Furthermore, confounding factors such as age, sex, and seasonal variations significantly influence VD levels, necessitating large-scale studies to adjust for these variables and determine whether LDD itself constitutes an independent risk factor for VD deficiency.
In this study, we conducted the large-scale investigation and demonstrated that the prevalence of VD deficiency in LDD patients showed no significant difference compared to a demographically adjusted general population (adjusted for age, sex, BMI, and seasons). Notably, absolute VD levels in LDD patients were even marginally higher than those in controls. These findings suggest that LDD is not associated with an elevated risk of VD deficiency. Additionally, our analysis revealed consistent epidemiological patterns of VD status between LDD patients and healthy individuals. The effect of age, sex, BMI and seasons on VD levels was detailed evaluated. Especially, the relationship between VD status and age exhibits a non-linear association characterized by a biphasic pattern with a VD level increase during early adulthood followed by progressive decline in elderly life stages.
The relationship between age and VD was widely concerned and reported with controversial results. While several studies indicated a negative correlation,18,23 opposite conclusions were also drawn in both HS populations and LDD patients.11,24,25 In this study, the relationship between age and VD levels was biphasic in both HS group and LDD patients, with increase at young age and decline in old age (≥66 for patient cohort and ≥72 for HS cohort). Such biphasic patterns were consistent with the study of Ning et al in the same region. 26 The mechanism of such relationship was not clear yet with possible reasons including different sun exposure, physiological requirement, ability of VD synthesis etc. Critically, this observation suggests that the risk of VD deficiency does not simply increase linearly in the general population aged 18 to 65 years, while in elderly individuals aged above 65-70 years, the VD levels required special consideration. Given the association between VD levels and the prognosis of LDD,7,12-14 the necessity of VD supplementation in patients aged 65 and above should warrant particular attention.
Between different sexes, significant differences in VD levels were also demonstrated in the present study. In both patients group and HS group, males presented higher VD levels and lower prevalence of VD deficiency, which was consistent with previous studies in China.18,26-28 Moreover, such sexual difference was particularly pronounced in patients, with the prevalence of VD deficiency 52.1% in females compared to 31% in males. The reason of such variation could be mainly related to the lifestyle habits rather than physiological factors. This is supported by a previous comparison study which found that males presented higher VD levels in Chinese population, while the trend was reversed in the American population. 27 The differences in outdoor activities, physical labor, sunscreen use, and dietary habits may contribute to different levels of sun exposure between males and females in China, ultimately leading to the observed sex disparity.
The influence of BMI on VD levels has been relatively consistent across different studies.24,29-31 Overall, BMI is negatively correlated with VD levels, 29 aligning with the findings of this study. Moreover, Rafiq et al. 29 reported that the impact of BMI on VD levels became more pronounced as BMI increased. This also explains why the correlation between BMI and VD levels in this study was relatively weak, given that most participants had low to moderate BMI. The underlying mechanisms of the negative correlation between BMI and VD levels are multifaceted. One possible explanation is the increased storage of VD in adipose tissue, leading to lower circulating plasma VD levels32,33 Additionally, VD may play a regulatory role in fat metabolism, as a recent study suggested that VD deficiency and obesity mutually reinforce each other at the molecular level. 34 The findings of this study indicate that in LDD patients with a BMI over 30 kg/m2, the risk of serum VD deficiency is significantly higher and requires particular attention. However, whether VD supplementation can improve clinical outcomes in this specific subgroup remains to be further investigated.
Sunlight exposure plays a crucial role in the cutaneous synthesis of VD. Solar ultraviolet B radiation in skin converts 7-dehydrocholesterol to previtamin D3, which is subsequently metabolized in the liver to form 25-hydroxyvitamin D. 4 In the geographical region of this study, which has 4 distinct seasons, the seasonal variations of sunlight exposure significantly affected the VD levels of the residents. In this study, the prevalence of severe VD deficiency in HS participants was notably higher in Winter and Spring (12.1% to 13.6%), whereas it was around 5% in Summer and Autumn. Moreover, in the LDD patients, the seasonal effect was primarily reflected in the increased prevalence of mild VD deficiency during the colder months. These epidemiological characteristics suggested that reduced cutaneous synthesis of VD during autumn and winter significantly increased the prevalence of VD deficiency, highlighting the potential benefits of increasing the intake of VD-rich foods or oral VD supplementation during these seasons.
The prevalence of VD deficiency varies considerably across different studies,8-14,16-21 making direct comparisons between LDD patients and healthy populations challenging. In this study, both HS participants and LDD patients in our center were included, and an age, sex, BMI, and examination season matched control group of the LDD patients was established. While the control group exhibited a higher prevalence of severe and mild VD deficiency, no statistically significant differences were observed when compared to the patient group. This finding suggests that, overall, VD deficiency is not clearly associated with the prevalence of LDD. Further, when comparing VD levels separately by sex, we found that the observed difference in VD levels between LDD patients and HS participants was primarily derived from the male population. The reason of such heterogeneity between different sexes remains unclear. One possible explanation is that this sex-specific finding is attributable to lifestyle and occupational differences. The HS population may primarily consist of middle to high-income individuals engaged in non-manual occupations, leading to less outdoor activity and an increased risk of VD deficiency. In surgical LDD patients, the increased outdoor labor could contribute to the development of LDD, 35 while the greater time spent outdoors simultaneously leads to higher vitamin D levels. Influenced by traditional gender roles, a higher proportion of males may be engaged in outdoor physical work, and this disparity could be more pronounced in males. However, the reason of the phenomenon could be multifactorial, and future prospective study considering the occupation and sunlight exposure time would be helpful.
Although this study included relatively large sample size of HS and surgical LDD participants, several limitations should still be noted. Firstly, this study was performed in a single center with a homogenous Asian population. Considering the close relation between VD levels and sunlight strength, living habits and diet, the epidemiological characteristics could be different in other regions or ethnics. Secondly, as an explorative study, the present research included the general surgical LDD patients with different specific diagnosis. The non-surgical patients were not included, and the diagnosis, severity of the disease or the surgical procedures were not further differentiated. Considering the potential heterogeneity of LDD patients with different diagnosis, although our results could represent an overall trend, further research focusing on specific patient subgroups is still warranted to provide a more detailed understanding. Thirdly, as a retrospective study, this study could not include all potential confounding factors such as diet, time of outdoor activity, occupation and exercise habits, and a future well-designed prospective study would be valuable.
Conclusion
In conclusion, in both HS participants and surgical LDD patients, VD deficiency was a common disorder. Age, sex, BMI, and season were influence factors of VD levels, with age exhibiting a notable biphasic relationship. Compared to the HS cohort, LDD patients showed similar epidemiological patterns in VD levels. Generally, surgical LDD patients were not associated with an elevated risk of vitamin D deficiency. However, for patients with old age, female sex, obesity, and surgery in spring and winter, higher risk of VD deficiency should be noted.
Footnotes
Ethical Considerations
The study was conducted within the principles of the Declaration of Helsinki, and was approved by the ethics committee of our hospital (No. IRB00006761-M2023727).
Consent to Participate
Due to its retrospective nature, the informed consent was waived within the permission of the ethnics committee.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key Research and Development Program of China (grant no. 2023YFC3604400) and the National Natural Science Foundation of China (grant no. 82202779). The funders had no role in study design, data collection or analysis, decision to publish, or preparation of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.