
Abstract
Study Design
Meta-analysis-based calculation.
Objectives
Falls are the primary cause of vertebral fractures and spinal cord injuries (SCI). We aimed to analyze the burden and trends of vertebral fractures and SCI due to falls.
Methods
We extracted data on the incidence, prevalence, and years lived with disability (YLDs) of vertebral fractures and SCI due to falls in 21 regions and 204 countries. Estimated annual percentage changes and the Joinpoint regression analysis was used to assess time trends. And we used the Bayesian Age-Period-Cohort model to project the burden for the next 15 years. Then, We developed smoothed curve models and used Spearman’s correlation coefficient to analyze the relationship between the Socio-Demographic Index (SDI) and the burden. Finally, frontier analysis was applied to evaluate the effective differences.
Results
In 2021, there were 4.73 million new cases of vertebral fractures and 3.67 million prevalent cases, and SCI accounted for .3 million new cases and 6.94 million prevalent cases. Although age-standardized rates (ASRs) showed a declining trend, absolute case numbers increased by more than 50% since 1990. Middle-aged males and elderly females are more vulnerable. A positive correlation was found between SDI and ASRs (P < .001), with higher burdens in high SDI regions. Burdens continue to rise in low and middle SDI regions due to limited healthcare resources and development-related risks.
Conclusions
The global burden of vertebral fractures and SCI continues to grow. Prevention of falls and musculoskeletal degeneration is critical. Urgent action is needed to improve healthcare infrastructure and preventive measures.
Introduction
Vertebral fractures and spinal cord injuries (SCI) are significant public health challenges with significant long-term impacts on healthcare systems worldwide.1,2 These injuries often result in chronic pain, permanent disability, and reduced quality of life.3,4 Additionally, they impose a considerable socioeconomic burden through healthcare costs, productivity losses, and long-term care needs. 5 Although advances in healthcare have improved survival rates and rehabilitation outcomes, full recovery from severe vertebral fractures and SCI remains difficult, leaving many patients with lifelong sensory and motor impairments. 6 Falls are the primary cause of these injuries, especially among the elderly, contributing substantially to the global burden of disability.7,8 The percentage of traumatic vertebral fractures and SCI caused by falls increased from 38.4% and 51.6% in 1990 to 52.2% and 63.0% in 2021. 9
Previous studies on the epidemiology of spinal fractures and SCI have shown considerable variation in data. 2 This is particularly evident in developing countries (as defined by the International Monetary Fund), where the annual incidence of SCI ranges from 2.1 to 130.7 per million. 10 This heterogeneity largely stems from differences in data collection methods, case definitions, and socioeconomic structures across countries. 11 Accurate and up-to-date estimates of disease incidence and prevalence are essential for evidence-based healthcare planning and resource allocation. The Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2021 has developed systematic methods for detailed quantification of health loss by disease, age, sex, year, and geographical location. 9 GBD 2021 includes significant data additions, improvements, and methodological refinements, providing a comprehensive opportunity to assess disease incidence, prevalence, years lived with disability (YLDs), and trends over time.
In this study, we utilize data from GBD 2021 to estimate the global, regional, and national burden of vertebral fractures and SCI due to falls from 1990 to 2021. Our goal is to provide a deeper understanding of the age, sex, and socioeconomic distribution of these injuries, analyze trends over time, and explore the relationship between development status and disease burden. We aim to contribute to the existing body of knowledge on spinal injuries and highlight key disparities.
Materials and Methods
Data Source and Study Population
The GBD 2021 derived from repeated cross-sectional data from the Global Health Data Exchange covers the global burden of 371 diseases and injuries in 21 regions and 204 countries and territories from 1990 to 2021. 9 All data were identified through systematic reviews of published studies, searches of government and international organization websites, published reports, primary data sources (eg, demographic and health surveys), and datasets provided by GBD collaborators. 9 Most sources of data on falls come from hospital patient records, supplemented by some surveys, injury surveillance, and emergency department data. 1 Definitions in the supplementary materials. Bayesian meta-regression using DisMod-MR 2.1 was used to estimate incidence and prevalence by combining epidemiologic data. YLDs were calculated by multiplying cause-age-sex-location-year-specific prevalence of sequelae by their respective disability weights, for each disease and injury. The general methodology has been previously published.1,9 The data sources used in GBD 2021 are available online. 12
From GBD 2021, we extracted the number, rates, and age-standardized rates (ASRs) of incidence, prevalence, and YLDs for vertebral fractures and SCI due to falls globally, in 21 regions (from countries and territories that are geographically proximate and have similar epidemiological characteristics), and in all 204 countries and territories. The term rate was used to indicate the number of cases per 100 000 population. All the data have 95% uncertainty intervals (UI).
Statistical Analysis
Descriptive Analysis
We compared absolute number and ASR of incidence (ASIR), prevalence (ASPR), and YLDs and their 95% UI for vertebral fractures and SCI from 1990 to 2021. Subgroup analyses were stratified by Socio-demographic Index (SDI) quintiles, sex, and 20 age groups (<5 years to 95+ years, per 5 years).
Trend Analysis
We calculated the estimated annual percentage changes (EAPCs) in ASRs. When the EAPC and lower confidence interval (CI) limits are positive, the ASR tends to increase. Conversely, when the EAPC and upper CI limits were negative, ASR tended to decrease. 13 To further parse the phase trends over the period, we used the Joinpoint regression model to identify and quantify mutation points in the data, segmenting the data into different trend segments. The detailed methodology is described in the supplementary materials.
Predictive Analysis
Constructing and fitting Bayesian Age-Period-Cohort (BAPC) models to project ASIR, ASPR, and age-standardized YLDs rate for vertebral fractures and SCI over the next 15 years (2022-2036) using the BAPC and Integrated Nested Laplace Approximation (INLA) packages in R software. Compared to other prediction methods, BAPC exhibits better coverage and accuracy, as demonstrated in previous studies.14,15
Correlation and Frontier Analysis
We developed smoothed spline curve models to determine the relationship between SDI and ASRs of vertebral fractures and SCI in 21 regions from 1990 to 2021, and between SDI and ASRs of vertebral fractures and SCI in 204 countries and territories in 2021 with calculated expected values. Spearman’s correlation coefficient analysis was used to evaluate the correlation between SDI and ASRs. We further applied frontier analysis to produce a nonlinear boundary that implies a minimum achievable burden based on the state of development and shows the countries and territories with the best control of the disease burden.
All statistical analyses were conducted using Joinpoint (version 5.2.0) and R (version 4.3.1). Statistical significance was set at P < .05.
Ethics Statement
The GBD 2021 followed the Guidelines for Accurate and Transparent Health Estimates Reporting statement 16 and was performed by the Institute for Health Metrics and Evaluation (IHME) using anonymous data and public accessibility 12 ; therefore, no ethics approval and informed consent were required.
Patient and Public Involvement Statement
No patients or the general public were involved in the analysis.
Results
Global Burden and Trends of Vertebral Fractures
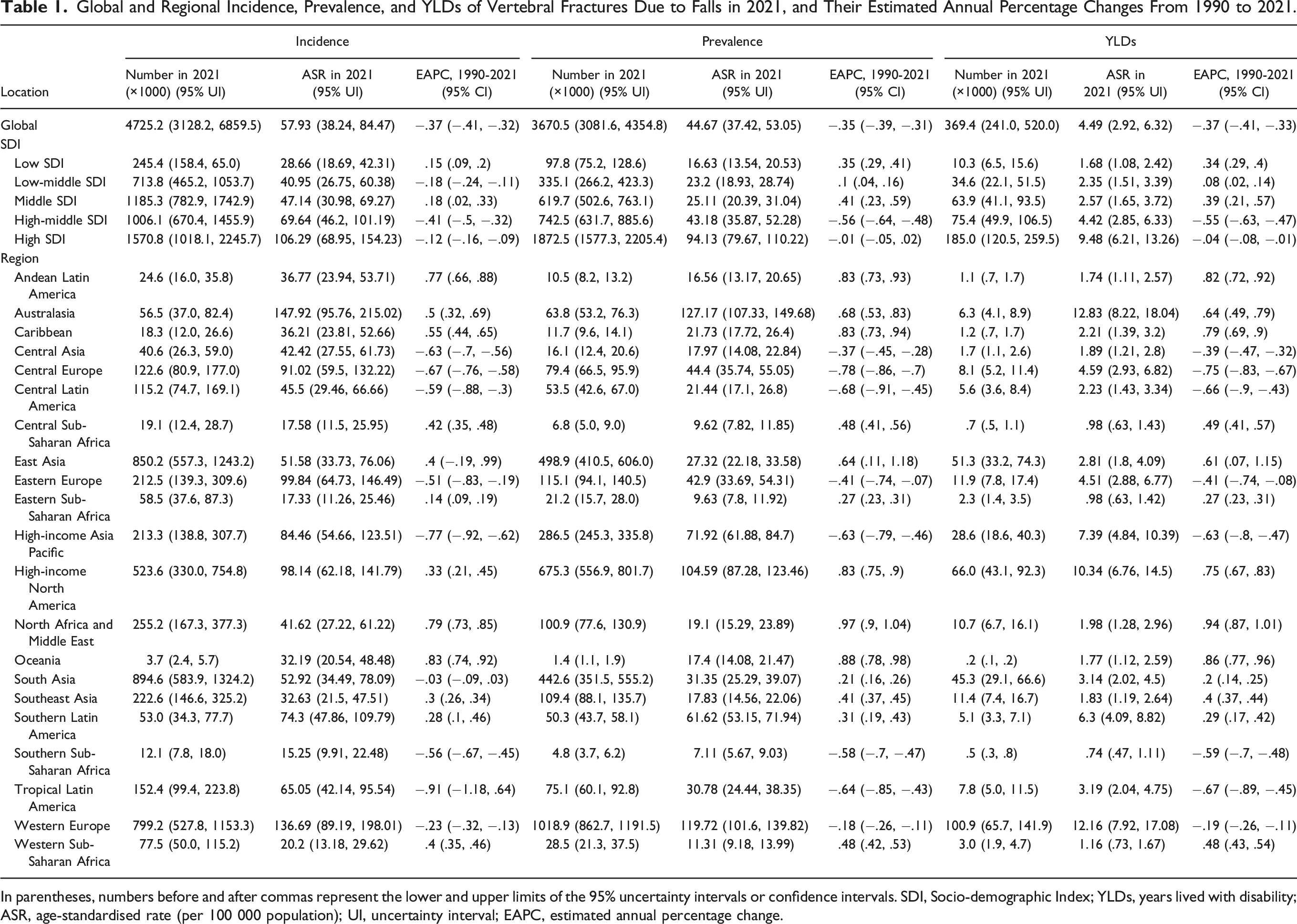
In 2021, the global absolute number of incidence, prevalence, and YLDs for vertebral fractures due to falls were 4 725 208 (95%UI: 3 128 249-6 859 512), 3 670 453 (95%UI: 3 081 600-4 354 780), and 369 432 (95%UI: 240 952-519 986), respectively, reflecting increases of 56.4%, 92.9%, and 89.0% since 1990. Global and regional burden data for 1990 are recorded in Table S1. The global ASRs of vertebral fractures showed a decreasing trend (EAPC: −.37, −.35, and −.37) from 1990 to 2021 (Figure 1A and Table 1). Further Joinpoint analysis (Figure S1 A–C and Table S2) showed the same trend in both male and female groups. The stage-wise trends of ASIR, ASPR, and age-standardized YLDs rate for vertebral fractures showed a significant pattern (P < .05), marked by an initial increase (1990-2000), a decrease (2000-2016), and a subsequent rise (2016-2021). The predicted ASIR, ASPR, and age-standardized YLDs rate of vertebral fractures are shown in Figure S2 A–C and Table S3. Globally, the ASIR, ASPR, and age-standardized YLDs rate of vertebral fractures were predicted to increase, with predicted values of 74.39, 72.35, and 6.87 respectively, by 2036. Bar chart & Line chart: Numbers and age-standardized rates (per 100 000) of incidence, prevalence, and YLDs of vertebral fractures and spinal cord injuries at the global level from 1990 to 2021. (A) Numbers and age-standardized rates of incidence, prevalence, and YLDs of vertebral fractures. (B) Numbers and agestandardized rates of incidence, prevalence, and YLDs of spinal cord injuries. Error bars indicate 95% uncertainty intervals. YLDs: Years lived with disability; ASIR: Age-standardised incidence rate; ASPR: Age-standardised prevalence rate. Global and Regional Incidence, Prevalence, and YLDs of Vertebral Fractures Due to Falls in 2021, and Their Estimated Annual Percentage Changes From 1990 to 2021. In parentheses, numbers before and after commas represent the lower and upper limits of the 95% uncertainty intervals or confidence intervals. SDI, Socio-demographic Index; YLDs, years lived with disability; ASR, age-standardised rate (per 100 000 population); UI, uncertainty interval; EAPC, estimated annual percentage change.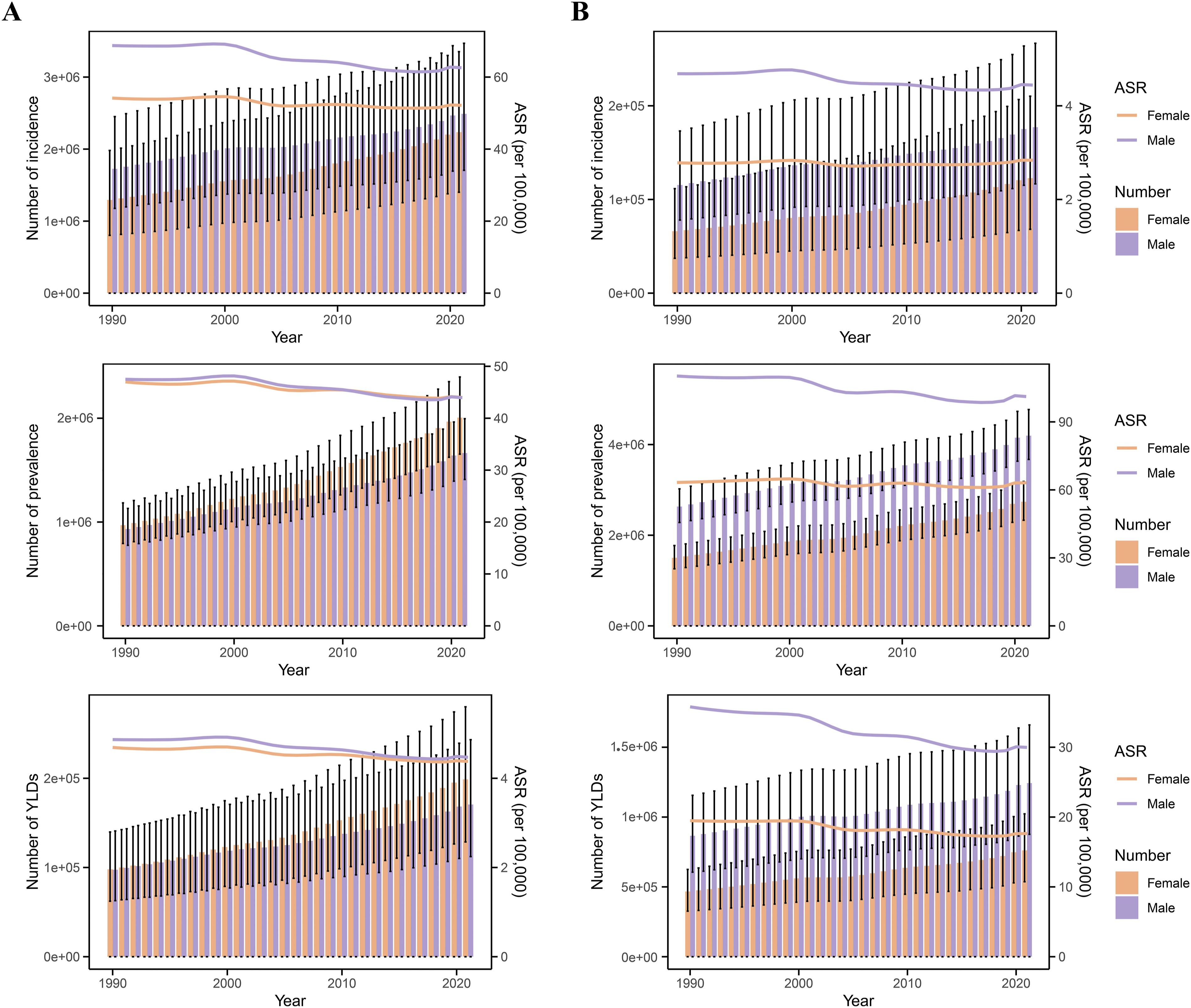
Subgroup analyses were performed by sex and age group. The trends of vertebral fractures were similar in males and females, with the absolute number of incidence, prevalence, and YLDs increasing each year from 1990 to 2021 (Figure 1A). In terms of number, the distribution of incidence in females tends to be more towards the elderly, while the distribution of crude incidence in males tends to be more towards the middle-aged. The age group with the highest incidence of vertebral fractures in males was 30-34 years and in females it was 80-84 years. The age group with the highest prevalence and YLDs in males was 70-74 years and in females it was 80-84 years (Figure S3 A–C). Males had higher rates of incidence, prevalence, and YLDs across all age groups than females. Rates of incidence, prevalence, and YLDs increase with age, especially after age 70, and the differences between males and females widen with age (Figure S4 A–C). In the 95+ years group, the rates of incidence, prevalence and YLDs in males amounted to 368.98 (95%UI: 213.74,575.5), 1513.19 (95%UI: 1220.9-1909.95), and 136.68 (95%UI: 85.39,193.46) and those in females reached 641.34 (95%UI: 339.55-1050.79), 2332.22 (95%UI: 1832.86-3031), and 207.84 (95%UI: 126.4-299.78) (Table S4).
Regionally, Australasia had the highest ASIR (147.92), ASPR (127.17), and age-standardized YLDs rate (12.83) for vertebral fractures among the 21 regions. Oceania, North Africa and Middle East, and Andean Latin America saw the largest increases in their burdens, while Tropical Latin America, Central Europe, and Central Latin America reduced their burdens the fastest (Table 1 and Figure 2A). Among 204 countries and territories (Figure 3 and Table S5), the Principality of Andorra had the highest ASIR (214.96), ASPR (199.63), and age-standardized YLDs rate (20.09) for vertebral fractures. Countries such as the Kingdom of Bhutan, the Socialist Republic of Viet Nam, the Kingdom of Cambodia, and the Republic of Turkey experienced the largest increases in burden, while countries such as the Republic of Armenia, the Republic of Latvia, and the Hungary experienced the largest decreases. Bar chart: Estimated annual percentage changes in age standardized rates of incidence, prevalence and YLDs for vertebral fractures and spinal cord injuries in 21 regions from 1990 to 2021. (A) Estimated annual percentage changes for vertebral fractures. (B) Estimated annual percentage changes for spinal cord injuries. EAPC: Estimated annual percentage change; ASIR: Age-standardised incidence rate; ASPR: Age-standardised prevalence rate; YLDs: Years lived with disability. Choropleth map: National age-standardized rates of incidence, prevalence, YLDs, and their estimated annual percentage changes of vertebral fractures in 2021. (A) National age-standardised incidence rates and their estimated annual percentage changes. (B) National age-standardised prevalence rates and their estimated annual percentage changes. (C) National age-standardized YLDs rates and their estimated annual percentage changes. YLDs: Years lived with disability; ASIR: Age-standardised incidence rate; ASPR: Age-standardised prevalence rate; EAPC: Estimated annual percentage change.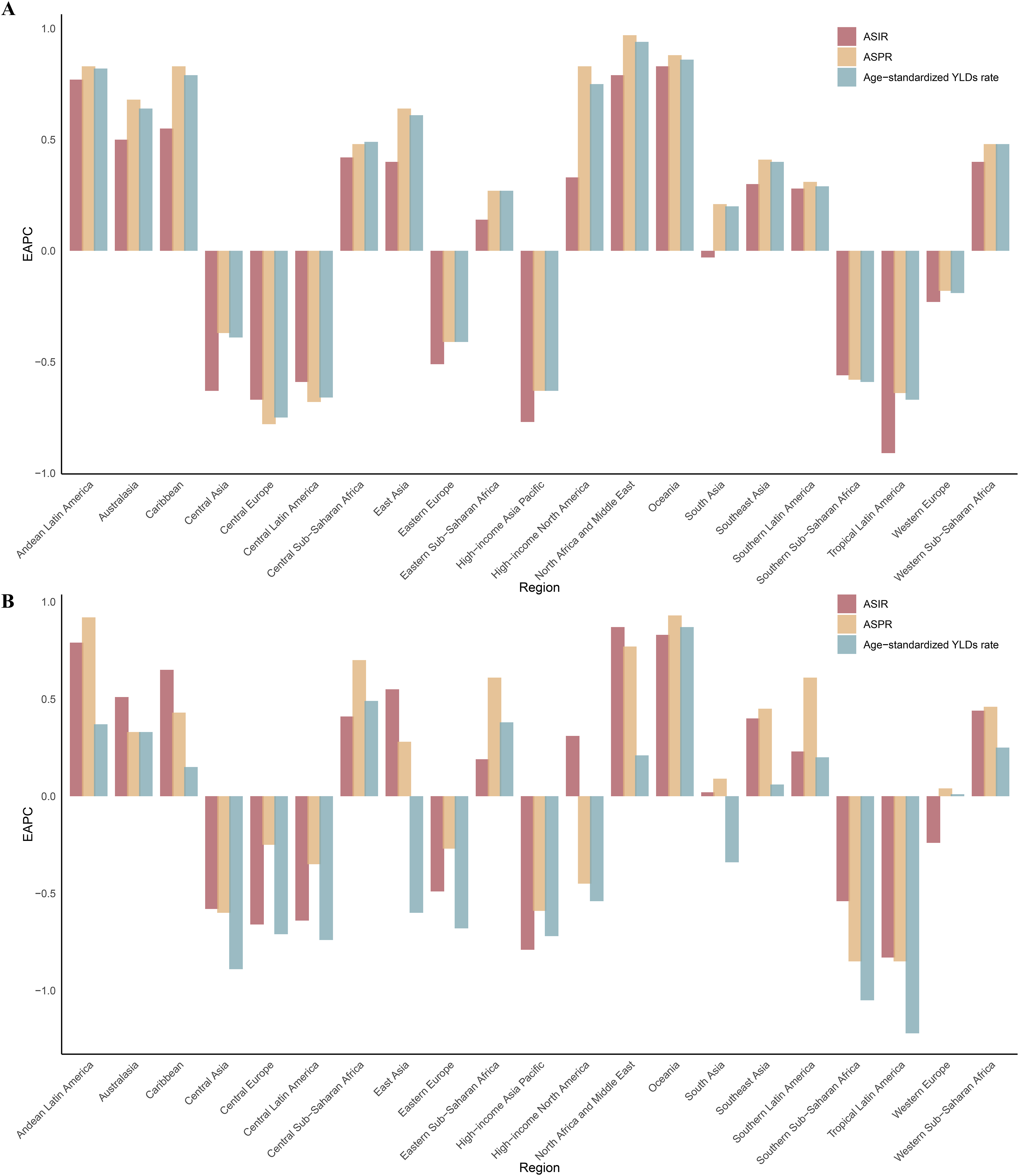

Global Burden and Trends of SCI
Global and Regional Incidence, Prevalence, and YLDs of Spinal Cord Injuries Due to Falls in 2021, and Their Estimated Annual Percentage Changes From 1990 to 2021.
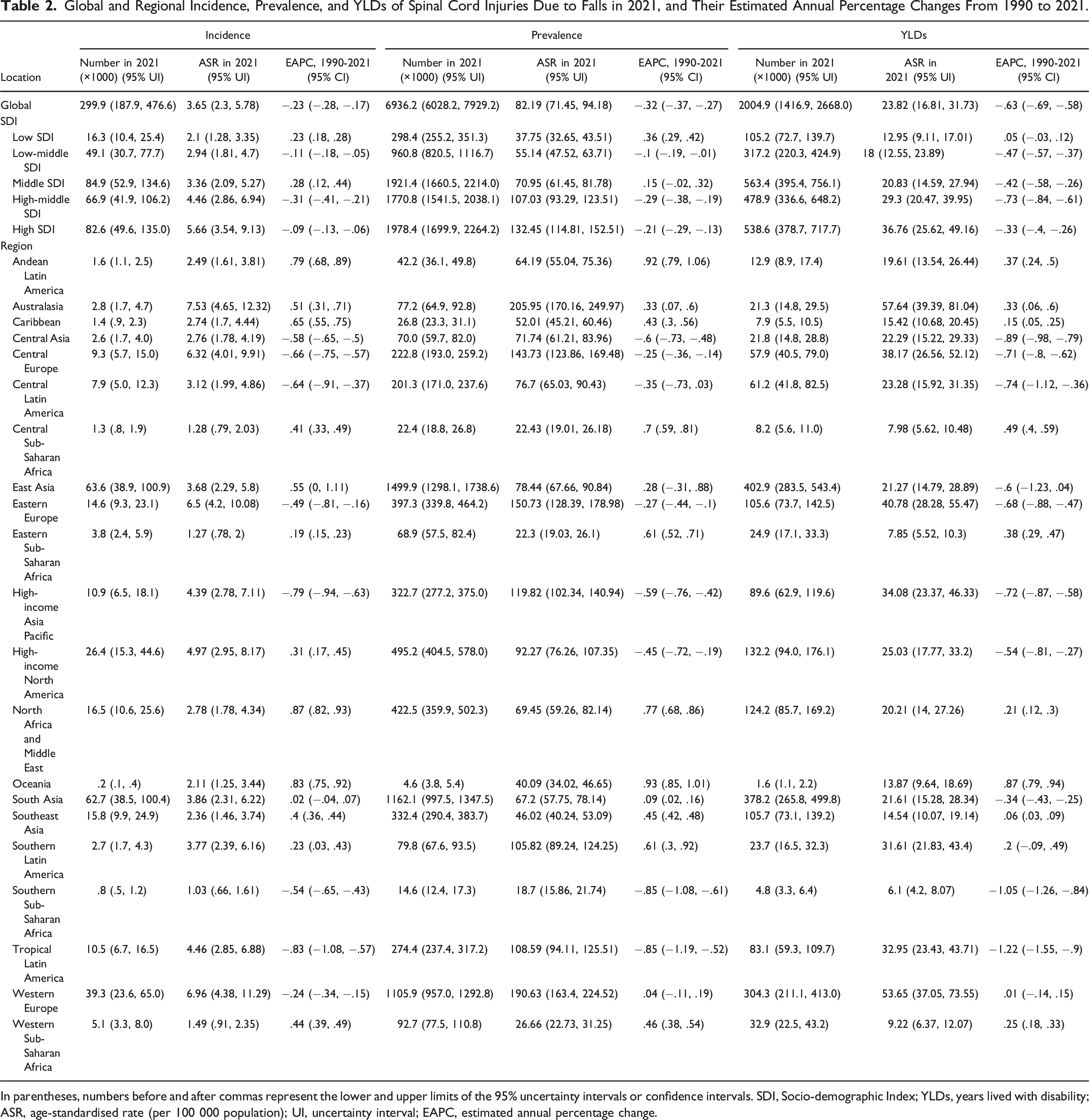
In parentheses, numbers before and after commas represent the lower and upper limits of the 95% uncertainty intervals or confidence intervals. SDI, Socio-demographic Index; YLDs, years lived with disability; ASR, age-standardised rate (per 100 000 population); UI, uncertainty interval; EAPC, estimated annual percentage change.
Subgroup analyses were performed by sex and age group. The trends of SCI were similar in males and females, with the absolute number of incidence, prevalence, and YLDs increasing each year from 1990 to 2021 (Figure 1B). In terms of number, the distribution of incidence in females tends to be more towards the elderly, while the distribution of incidence in males tends to be more towards the middle-aged. The age group with the highest incidence number in males was 35-39 years and in females it was 80-84 years. The age group with the highest prevalence and YLDs in males was 50-54 years and in females it was 65-69 years (Figure S3 D–F). The incidence rate increases with almost age. However, the rates of prevalence and YLDs are parabolic with age. The rates of prevalence and YLDs for SCI were consistently higher in males than in females until age 79 years, but they were higher in females beyond age 80. The highest rates of prevalence and YLDs of SCI were found in males aged 70-74 years and in females aged 80-84 years (Figure S4 D–F and Table S8).
Regionally, Australasia had the highest ASIR (7.53), ASPR (205.95), and age-standardized YLDs rate (57.64) for SCI among the 21 regions (Table 2 and Figure 2B). Among 204 countries and territories (Table S5 and Figure S5), the Kingdom of Saudi Arabia had the highest ASIR (9.59), and the Republic of Finland had the highest ASPR (273.39) and age-standardized YLDs rate (76.77) for SCI. In 21 regions and 204 countries and territories, EAPCs for the burden of SCI were similar to vertebral fractures (Figure 3, Figure S4, and Table S5).
Correlation and Frontier Analysis
Among the quintile SDI groups, the high SDI had the highest ASRs of vertebral fractures and SCI (Table 1 and Table 2). From 1990 to 2021, overall ASRs for vertebral fractures and SCI increased with rising SDI in 21 regions (Figure S6). However, a downward trend occurred approximately after the SDI > .8. The analysis of the time trends revealed that the SDI in all regions grew over time. In regions with low SDI, ASRs of vertebral fractures and SCI in the same region followed an upward trend with SDI growth, while in regions with high SDI, ASRs in the same region followed an upward and then downward trend with SDI growth (Figure S6). Spearman’s correlation coefficient analysis showed that the ASRs of vertebral fractures and SCI in 21 regions were positively correlated with SDI (ρ = .808-.860, P < .001). The SDI in 2021 represents the level and availability of health care in different countries.
Overall ASRs for vertebral fractures and SCI in 204 countries and territories in 2021 increased with the SDI, especially accelerating after the SDI reached .6 (Figure S7). Spearman’s correlation coefficient analysis showed that the ASRs of vertebral fractures and SCI in 204 countries and territories were positively correlated with SDI (ρ = .758-.803, P < .001).
The frontier analysis demonstrated the effective differences between ASRs and ideals for 204 countries and territories, as well as time trends. Among the high SDI countries and territories, the ASRs for a country and territory also have a parabolic relationship with the SDI (Figure S8). The frontier analysis identified the top 10 countries most likely to reduce the burden of vertebral fractures, with effective differences ranging from 138.27 to 203.48 for ASIR, 122.22 to 194.14 for ASPR, and 12.29 to 19.51 for age-standardized YLDs rate (Table S9). Among the top 10 countries most likely to reduce the burden of SCI, the effective differences ranged from 7.43 to 9.82 for ASIR, 203.61 to 260.83 for ASPR, and 56.43 to 72.10 for age-standardized YLDs rate (Table S9). The countries with the greatest potential for reducing vertebral fractures and SCI burden include Andorra, Finland, Belgium, Switzerland, and France, Luxembourg, Austria, New Zealand, Italy, Greenland, Norway, Australia. These countries have higher ASRs than others under similar sociodemographic conditions. Additionally, Figure S8 highlight the 15 countries with the smallest effective differences in low SDI regions and the 30 countries with the largest effective differences in high SDI regions.
Discussion
This study provides the latest data and important insights regarding the burden of falls-induced vertebral fractures and SCI, revealing important trends across sex, age, SDI, and geographic groups. As a part of the GBD 2021 study, this study is the first to systematically assess the global burden of vertebral fractures and SCI due to falls and forecast them for the next 15 years. In addition, for the first time, we analyzed SDI-related differences in burden and trends. Several key findings emerged from this study. First, the burden of vertebral fractures and SCI due to falls has grown steadily and is projected to remain increasing. Second, among females, older adults are more vulnerable, whereas among males, middle-aged adults are more common. Both prevalence and YLDs of them are concentrated in the elderly population. Especially, the burden of SCI tends to decrease after age 70, and the sex difference reverses after age 80. Third, there are considerable regional and national differences in burden and trends, which commonly synchronize across SCI and vertebral fractures. Finally, regional and national burdens are positively correlated with SDI. But in high SDI regions, the burden seems to be decreasing as the SDI rises. Regrettably, frontier analyses show greater effective differences in more developed countries.
Over the past three decades, the global burden of vertebral fractures and SCI caused by falls has increased by more than 50%. In 2021, approximately 4.73 million new cases of vertebral fractures from falls were reported, with 3.67 million prevalent cases and about .37 million YLDs. For fall-related SCI, there were around .3 million new cases, 6.94 million prevalent cases, and over 2 million YLDs. Although the underlying epidemiological trends have softened (with a decline in ASRs), these changes are far from offsetting the impacts of population growth and aging. From 1990 to 2021, the global population grew by approximately 48% (population source: https://populationstat.com/), directly correlating with the rise in absolute case numbers. As life expectancy increases, the impact of falls and osteoporosis is becoming increasingly evident, which inevitably increases the burden of vertebral fractures and SCI, particularly in regions such as Europe.17-19 However, attributing the rising global burden of these conditions solely to population growth and aging oversimplifies the issue, as many underlying factors are influenced by shifting social, environmental, and economic contexts.
Vertebral fractures typically present with acute onset and may stabilize or improve over time, especially with appropriate treatment, such as surgical fixation. 20 Despite the higher incidence, the overall prevalence remains relatively low. In contrast, SCI is often associated with chronic, long-term disability. Once a person suffers a spinal cord injury, the likelihood of recovery is limited, frequently leading to permanent damage. 21 As a result, SCI has a higher prevalence than incidence. This distinction has important implications for the healthcare system and resource allocation, with SCI having a greater need for long-term rehabilitation and support services. 22 The sharp decline in the age-standardized YLDs rate for SCI (EAPC = −.63) is particularly noteworthy, suggesting that improvements in rehabilitation and long-term care have contributed to reducing the overall disability burden. However, we found that the increase in prevalent cases (up 92.9%) and YLDs (up 89.0%) for vertebral fractures was significantly larger than the increase in incidence (up 56.4%), indicating a rising chronic burden, particularly among the elderly. This likely reflects worsening bone health in older adults, making fracture recovery more difficult. 23 Additionally, patients with vertebral fractures often experience chronic pain or functional limitations, leading to increased YLDs. 24 Therefore, we emphasize the importance of preventative measures for bone conditions such as osteoporosis.
Another key finding is the sex difference. The burden of vertebral fractures and SCI caused by falls is higher in males than in females, particularly among middle-aged populations. The dominance of males in SCI cases is well-documented in the literature. Studies by Golestani et al. 25 and Zhang et al. 26 report similar trends, highlighting the higher incidence of SCI among males due to greater exposure to occupational hazards, physical trauma, and risky behaviors. Males working in physically demanding jobs, such as construction, agriculture, and manufacturing, are particularly prone to falls and injuries. 27 Additionally, as males age, the burden of SCI significantly decreases, reflecting reduced exposure to high-risk activities that commonly cause such injuries. In contrast, as females age, particularly post-menopause, the burden of vertebral fractures rises sharply, reflecting the well-known effects of osteoporosis and hormonal changes. 28 The continued rise in fracture incidence with age in females likely mirrors increased fall frequency and heightened osteoporosis risk among the elderly. The reversal of sex differences after age 80 may reflect survivor bias, as females tend to live longer, increasing their chances of accumulating more disability related to spinal injuries. 29 This may also be linked to the fact that older females tend to have weaker musculoskeletal tissues compared to males, making them more susceptible to severe spinal injuries and facing greater challenges in recovery.28,30
Our analysis reveals significant regional and national disparities, with a clear positive correlation between SDI and the burden of vertebral fractures and SCI. In high-SDI regions such as Western Europe, North America, and Australia, the ASIR, ASPR, and age-standardized YLDs rates are significantly higher compared to low SDI regions. This trend can be attributed to several factors inherent to more developed countries, including population aging, higher healthcare-seeking behavior, and advanced medical infrastructure, which ensures more cases are diagnosed and reported. 31 Interestingly, this correlation is not strictly linear. In high-SDI regions, we observed a turning point where, after an SDI of .8, the burden of vertebral fractures and SCI begins to decline. This suggests that as countries reach a certain level of development, they can reduce the incidence and severity of these injuries through effective public health interventions, injury prevention strategies, and advanced rehabilitation services. 32 For example, countries such as Finland, Australia, and the United States have successfully implemented fall prevention programs, osteoporosis management, and rehabilitation services. High-income countries typically emphasize community-based programs to improve balance and muscle strength among the elderly, reducing the risk of falls and related injuries. 33 The observed decrease in YLDs in these countries reflects the success of these interventions, particularly for SCI, where advancements in rehabilitation have reduced long-term disability.
Though high SDI countries have demonstrated the ability to reduce the burden of vertebral fractures and SCI, middle and low SDI regions face a different reality. For example, in North Africa and the Middle East, the ASIR of vertebral fractures is increasing by .79% annually, and in Oceania, it reaches .83%. In these regions, the burden continues to rise as rapid urbanization, industrialization, and population growth increase the risk of falls, motor vehicle accidents, and occupational injuries. 34 Without comprehensive fall prevention strategies and improvements in healthcare services, the burden of spinal injuries in these regions is likely to continue rising. In low SDI areas, such as sub-Saharan Africa and parts of South Asia, the burden of vertebral fractures and SCI is also increasing. Healthcare infrastructure in low SDI regions often lacks the capacity to effectively manage or rehabilitate spinal injuries, leading to higher YLDs. 35 For example, our study found that while the ASIR of vertebral fractures in low-SDI countries is growing at a modest rate (EAPC = .15), the limited availability of treatment services means even slight increases in incidence lead to disproportionately high disability burdens (EAPC = .34). Furthermore, due to insufficient healthcare infrastructure, these regions face significant barriers in accessing, diagnosing, and reporting cases, which means the true burden may be underestimated. 36 Additionally, as these regions experience economic development, they may face similar burdens to more developed areas if preventive measures are not implemented early.
Our frontier analysis further highlights the potential to reduce the burden of vertebral fractures and SCI, particularly in high SDI countries. Despite advanced healthcare systems, countries like Andorra, Belgium, and Switzerland still bear a burden far higher than expected for their level of development. Even in these highly developed regions, there remains significant untapped potential for reducing the burden. The frontier analysis identified countries where improvements in fall prevention programs, expansion of rehabilitation services, and increased public awareness of injury prevention could further alleviate the burden. 37 We stress the importance of addressing this issue and call on policymakers, healthcare institutions, and public health experts to take immediate action. Conversely, low SDI countries face structural challenges that hinder their ability to reduce the burden of spinal injuries. A lack of healthcare infrastructure, limited rehabilitation services, and inadequate preventive care contribute to the increasing burden in these regions. 38 International collaboration and investment in healthcare infrastructure are crucial to alleviating the burden of vertebral fractures and SCI in low SDI regions. 39 Moreover, public health initiatives focused on improving bone health, strengthening road safety, and implementing basic fall prevention programs are essential to curbing the rise of these injuries in the future.
This study has several limitations. First, the data in the GBD come from different countries with varying diagnostic practices, which may lead to inconsistencies and misclassification. Although advanced modeling techniques help mitigate these issues, the findings still heavily rely on model-based estimates, particularly in regions with limited data. In low- and middle-income countries, misdiagnosis, underreporting, and incomplete medical records are common, which may lead to an underestimation of the true burden in these areas. Meanwhile, the burden in earlier years included in the study, such as 1990, was lower, likely due to a higher likelihood of underreporting globally at the time, which may have led to an underestimation of the true burden. Given the uncertainty associated with primary data, caution is warranted when interpreting the burden identified in this study. Second, we did not explore the potential impact of individual factors, such as occupation, or public health events like the COVID-19 pandemic. Furthermore, since the GBD included cases primarily on the basis of disease codes, this led us to identify only vertebral fractures and failed to distinguish between two different types of injuries-traumatic vertebral injuries due to high-velocity falls and low-velocity pathologic fractures (fragility injuries). Due to the complexity of these issues and data availability, they should be explored further in future studies. Third, the time lag in GBD data means that the estimates are based on historical trends, which may not fully capture recent changes in healthcare or lifestyle factors. Lastly, this study does not account for subnational differences within large countries.
Conclusions
This study highlights the global burden of vertebral fractures and SCI due to falls. Despite declining ASRs, population growth, aging, and potential fall risk have increased absolute case numbers. Middle-aged males experience more vertebral fractures and SCI caused by falls due to high occupational and behavioral risks, while older females face a greater risk of injury due to low musculoskeletal strength. Regional and national disparities reflect socioeconomic development, with high SDI countries experiencing higher rates but benefiting from effective interventions that reduce the burden as SDI increases. Urgent action is needed to improve fall prevention, expand rehabilitation services, and address healthcare gaps, particularly in low and middle SDI regions, to reduce the future impact of these injuries.
Supplemental Material
Supplemental Material - Global Burden of Vertebral Fractures and Spinal Cord Injuries Due to Falls From 1990 to 2021: A Population-Based Study
Supplemental Material for Global Burden of Vertebral Fractures and Spinal Cord Injuries Due to Falls From 1990 to 2021: A Population-Based Study by Tianyu Liu, Hanlin Zou, and Haibo Zou in Global Spine Journal.
Footnotes
Acknowledgments
Author Contributions
T.L.: data curation, formal analysis, methodology, visualization, writing-original draft, writing-review and editing. HL.Z.: data curation, writing-review and editing. HB. Z.: funding acquisition, supervision, witing – review & editing. All authors have read and agreed to the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.