
Abstract
Study Design
Retrospective Cohort Study.
Objective
Isthmic spondylolisthesis is frequently encountered in spine surgical practice, though there is a significant variation in surgical management strategies. We sought to evaluate revision rates between patients who underwent anterior-approach lumbar interbody fusion (ALIF) alone, posterolateral fusion (PLF) alone, PLIF/TLIF, and ALIF+PSF.
Methods
This retrospective study utilized a large commercial insurance claims database of patients ≤65 years-old. Patients with isthmic spondylolisthesis who underwent single-level instrumented arthrodesis were included, and those who underwent revision surgery, surgery for deformity, multi-level surgery, or surgery for traumatic, infectious, or neoplastic etiologies were excluded, as determined by ICD-10-CM and CPT codes. Patients were assigned to surgical cohorts of ALIF alone, PLF alone, PLIF/TLIF, and ALIF+PSF based on CPT codes. Additional independent variables included age, sex, decompression at index surgery, and region. The primary outcome was revision arthrodesis or decompression, defined using CPT codes. Kaplan-Meier analysis and Cox Proportional Hazards regression were utilized to assess differences in revision occurrence between cohorts.
Results
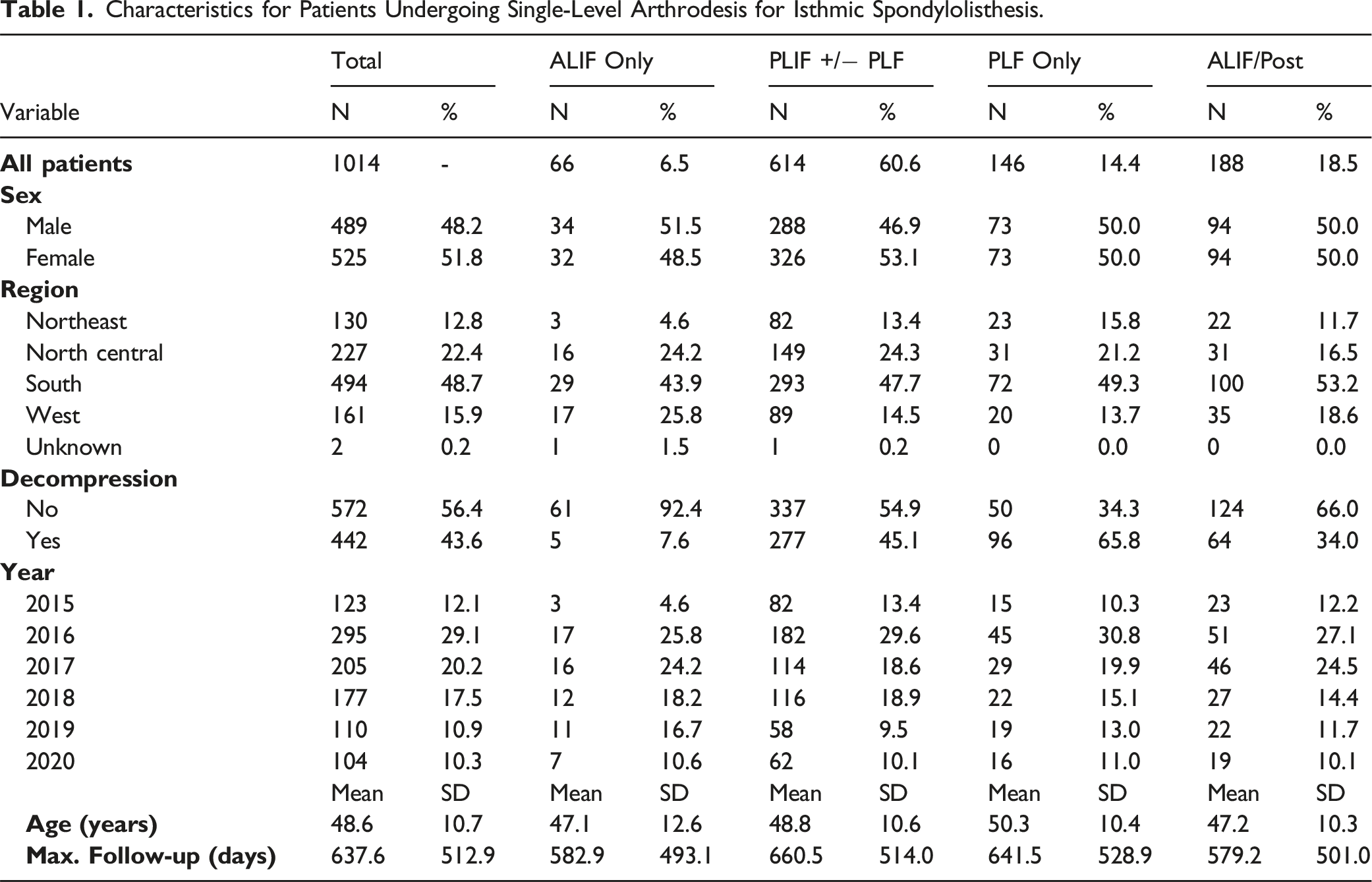
1014 patients who underwent single-level arthrodesis for isthmic spondylolisthesis were included. The mean age was 48.6 years, with a mean follow-up of 637.6 days. The majority of patients underwent PLIF/TLIF (60.6%, n = 614), followed by ALIF+PSF (18.5%, n = 188), PLF alone (14.4%, n = 146), and ALIF alone (6.5%, n = 66). The 5-year revision-rate was 11.0% for all patients in the Kaplan-Meier analysis. In multivariable analysis adjusting for confounding factors, ALIF-alone demonstrated significantly higher occurrence of revision compared to both ALIF+PSF (HR 5.0, P = 0.0026) and PLIF/TLIF (HR 5.8, P < 0.0001) groups. Similarly, PLF alone demonstrated significantly higher occurrence of revision surgery compared to PLIF/TLIF (HR 2.4, P = 0.0379) while other comparisons were not statistically significant.
Conclusions
In this analysis of single-level arthrodesis for isthmic spondylolisthesis, patients who underwent ALIF alone had higher revision rates than those who underwent PLIF/TLIF and ALIF+PSF surgery, and those who underwent PLF alone had higher revision rates than those who underwent PLIF/TLIF. Surgical strategies providing both anterior and posterior column support resulted in lower real-world revision rates.
Introduction
Isthmic spondylolisthesis presents as abnormal vertebral translation in the presence of a defect in the pars interarticularis, most commonly at the L5–S1 level. The instability often leads to persistent lower back pain, radicular leg pain, and functional limitations. 1 Pain with isthmic spondylolisthesis can be caused by various factors, such as nerve root compression by fibrocartilaginous tissue, nerve root traction, disk bulging, and lumbar malalignment leading to muscle strain. 2 While the precise cause remains unknown, some studies have shown that abnormal spinopelvic parameters may contribute to both its onset and advancement of the disease.3,4
Conservative treatments, such as lifestyle modification, physical therapy, and nonsteroidal anti-inflammatory drugs, can often help with symptomatic management, 5 however, a subset of patients require surgical treatment. Several studies have compared posterior or transforaminal lumbar interbody fusion (PLIF/TLIF) and posterolateral lumbar fusion (PLF), with a focus on fusion rates and clinical outcomes.6-11 These studies were mixed with regards to postoperative outcomes, with some studies showing PLIF to be superior to PLF, and others indicating no difference between the 2 treatment options.6,8,9 Anterior column support may be beneficial in isthmic lumbosacral spondylolisthesis due to improved fusion rates while maintaining reduction and appropriate lumbopelvic alignment.12,13 Some studies have found that combined ALIF+PLF approach may provide the most favorable outcomes with regards to the fusion rate. 14
While several studies have evaluated the various surgical approaches and their association with reoperation, most of these studies are limited by small sample sizes.15-17 This study aims to assess real-world revision rates between patients who underwent anterior-approach interbody fusion alone (ALIF, includes anterior lumbar interbody fusion [ALIF], lateral lumbar interbody fusion [LLIF], oblique lumbar interbody fusion [OLIF]), PLF-alone, PLIF/TLIF, and ALIF+PSF surgeries in recent years.
Methods
Data Sources
This retrospective database study utilized the MarketScan Research Database (IBM Health, Ann Arbor, MI). The MarketScan database is a collection of >300 billion claims records from private insurance carriers. Patients included in the database are those ≤65 years-old, and enrolled in plans such as those provided by large, self-insured companies, as well as early retirees, Consolidated Omnibus Budget Reconciliation Act (COBRA) enrollees, and their dependents.
Patient Selection
Patients with a diagnosis of isthmic spondylolisthesis (ICD-10-CM: Q762, M4317) who underwent instrumented arthrodesis from 2015 – 2020 (CPT: 22612, 22630, 22558, 22633, 22840) in either inpatient or outpatient settings were included. Those with codes for trauma, infectious, and neoplastic diagnoses were excluded (ICD-10-CM: S10, S11, S12, S13, S14, S15, S16, S17, S19, S22, S32, C40, C41, C79, D16, D33, D43, D48, M86, M462, M463, M465, M42, M50, M4802, M5412), as were patients who underwent surgery for deformity (CPT: 22800, 22802, 22804), those with codes specifically indicating multi-level surgery (CPT: 22614, 22632, 22585, 22634, 22842, 22843, 22844, 22846, 22847), or codes indicating revision surgery (CPT: 22849, 22850, 22852, 22855, 22830; ICD-10-CM: M960, M961, M963, M964). In order to further isolate those who underwent single-level surgery, any patients with more than 1 posterior arthrodesis code were excluded (CPT: 22612, 22630, 22633).
Outcome
The primary outcome was revision arthrodesis or decompression, defined using CPT codes (arthrodesis [CPT: 22612, 22630, 22558, 22586, 22633, 22808, 22810, 22812, 22800, 22802, 22804], decompression [CPT: 62380, 63005, 63017, 63030, 63042, 63044, 63047, 63052, 63053, 63056, 63087, 63088, 63090, 63091]). Patients who underwent revision subsequently underwent manual review of ICD and CPT codes to determine, to the extent possible with claims data, the indications for revision and the specific nature of the revision surgery.
Independent Variables
The primary independent variable was the surgical approach, grouped as ALIF alone, PLF alone, PLIF/TLIF, and ALIF+PSF (with posterior including codes for both posterolateral fusion and posterior instrumentation alone). The codes used to assign these groups were: ALIF (CPT: 22558), PLF (CPT: 22612, 22840), and PLIF/TLIF (CPT: 22630, 22633). Additional independent variables included decompression performed in index surgery (CPT: 62380, 63005, 63017, 63030, 63042, 63044, 63047, 63052, 63053, 63056, 63087, 63088, 63090, 63091), age, sex, and region.
Statistical Analysis
Descriptive statistics were generated. Kaplan-Meier analysis was performed to assess revision rates over time in an unadjusted fashion. Chi-Square and Kruskal-Wallis tests were utilized for bivariable analyses comparing cohort characteristics. Cox Proportional Hazards regression was utilized in both bivariable, and multivariable analyses to assess the occurrence of revision over time stratified by surgical cohort, accounting for age, sex, region, and decompression at the index surgery. Statistical significance was defined as P < 0.05. Statistical analyses were performed using SAS 9.4 (SAS Institute, Cary, NC).
Results
In total, 1014 patients who underwent single-level arthrodesis for isthmic spondylolisthesis were included. The mean age was 48.6 years (SD 10.7), and 51.8% (n = 525) of the patients were female. Decompression was listed as a separate code in 43.6% (n = 442) of the surgeries. The mean follow-up of all patients was 637.6 days (SD 512.9) after index surgery. Most patients in the cohort were from year 2016 (29.1%) and 2017 (20.2%). Most patients were from the Southern region (48.7%, n = 494), followed by the North Central region (22.4%, n = 227).
Characteristics for Patients Undergoing Single-Level Arthrodesis for Isthmic Spondylolisthesis.
Revision Indications and Surgeries for Patients.
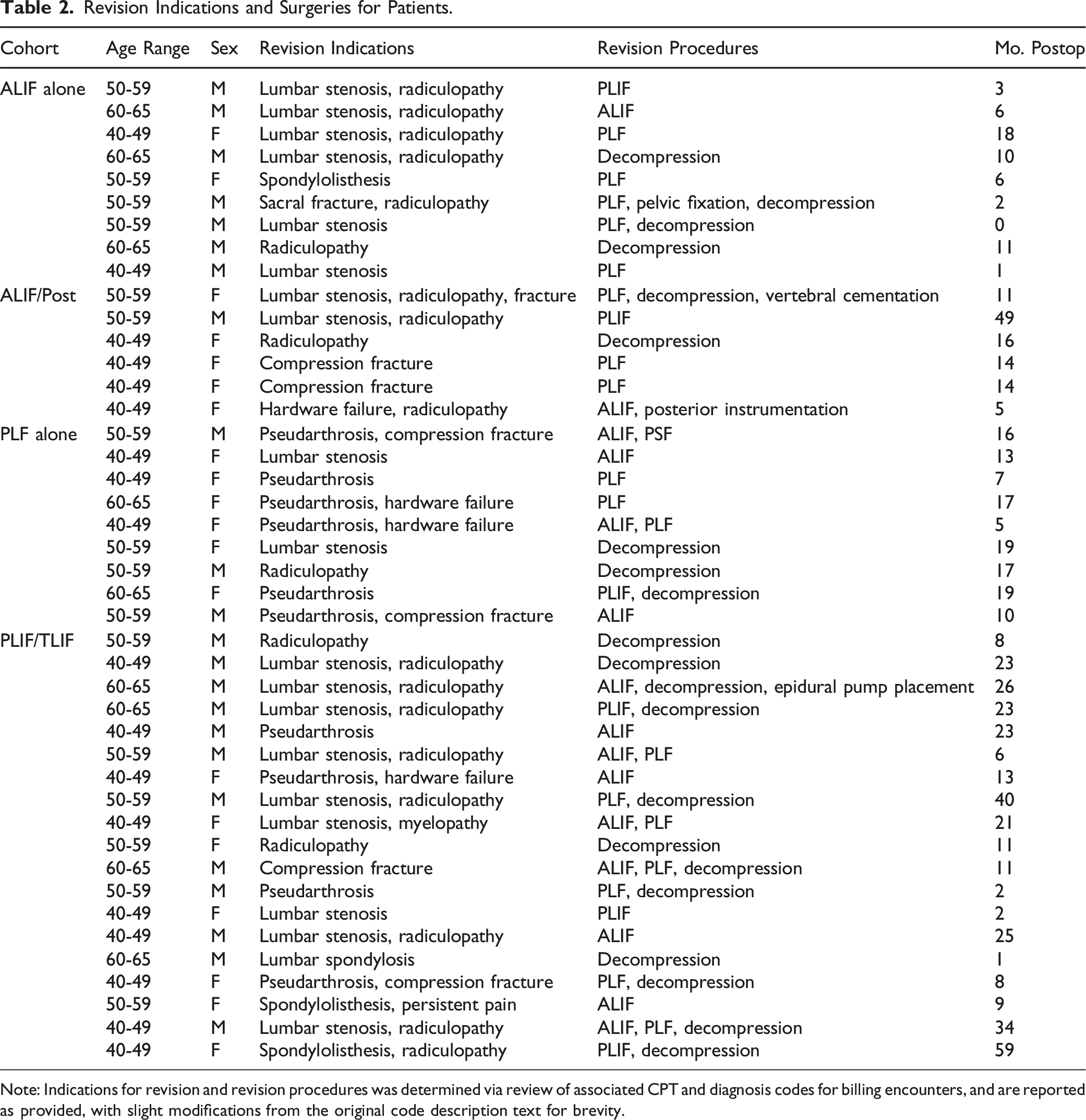
Note: Indications for revision and revision procedures was determined via review of associated CPT and diagnosis codes for billing encounters, and are reported as provided, with slight modifications from the original code description text for brevity.
In the Kaplan-Meier analysis, significant differences were observed between surgical cohorts (P < 0.0001) (Figure 1). In unadjusted bivariable Cox Proportional Hazards regression, patients who underwent ALIF alone exhibited a significantly higher occurrence of revision compared to those in the ALIF+PSF (HR 4.8, P = 0.0030), PLIF/TLIF (HR 5.5, P < 0.0001), and PLF alone (HR 2.6, P = 0.0458) groups. However, no significant difference was observed between PLF-alone and ALIF+PSF (HR 1.9, P = 0.5361) and PLIF/TLIF (HR 2.1, P = 0.0588) groups. In multivariable analysis adjusting for confounding factors, ALIF-alone demonstrated higher occurrence of revision compared to both ALIF+PSF (HR 5.0, P = 0.0026) and PLIF/TLIF (HR 5.8, P < 0.0001) groups. Similarly, PLF alone demonstrated significantly higher occurrence of revision surgery compared to PLIF/TLIF (HR 2.4, P = 0.0379) while other comparisons were not statistically significant. Revision-free survival by cohort.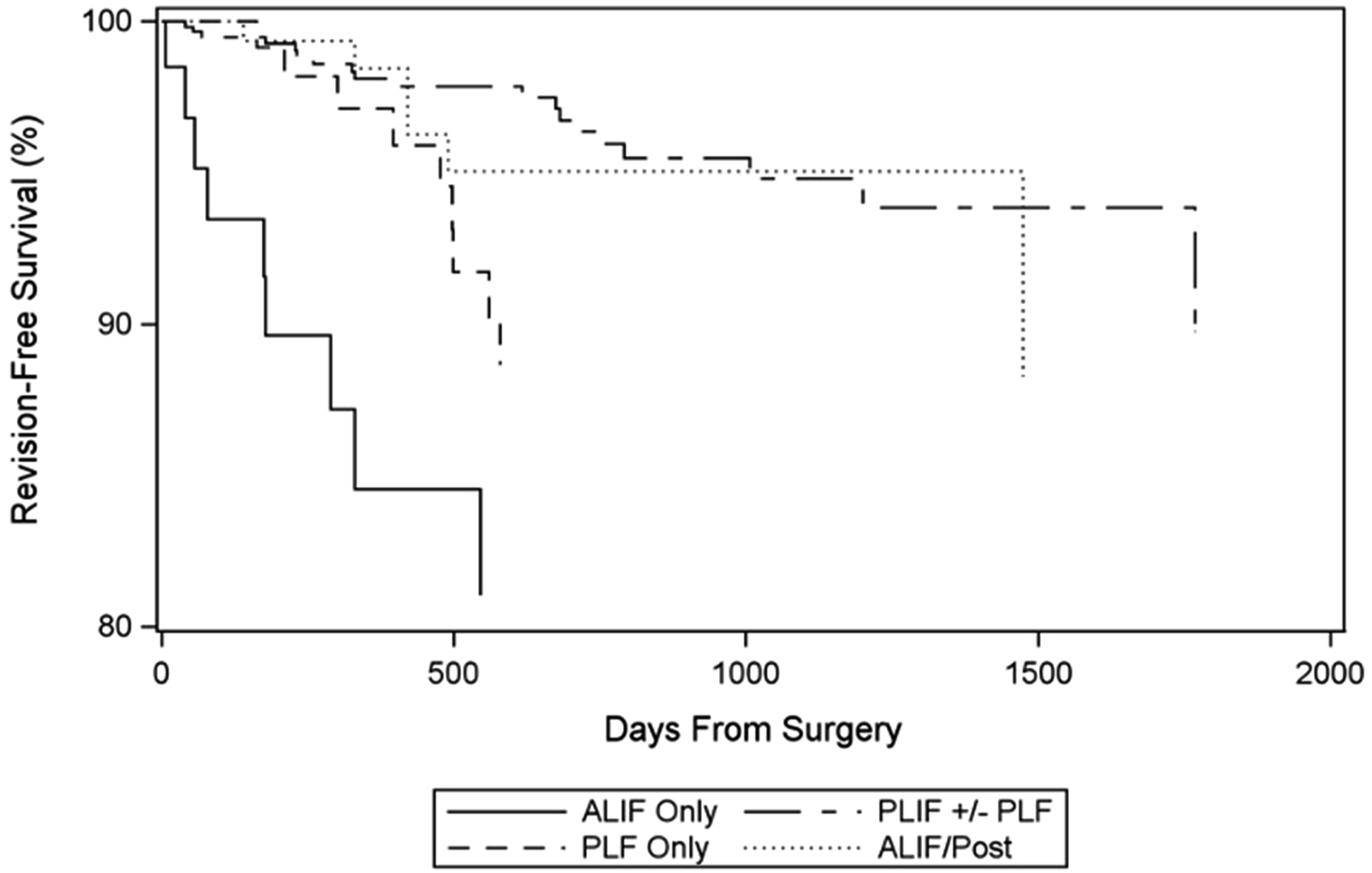
Discussion
This study utilized a large database of commercial insurance claims data to assess revision rates for surgical management of isthmic spondylolisthesis. We found that patients undergoing ALIF only surgeries had higher revision rates than those who underwent PLIF/TLIF and ALIF+PSF surgery, and those who underwent PLF alone had higher revision rates than those who underwent PLIF/TLIF.
Isthmic spondylolisthesis ranks among one of the most prevalent spinal pathologies and typically manifests at the lumbosacral junction. Although various surgical strategies have been developed for the management of isthmic spondylolisthesis, a consensus on the optimal technique remains elusive. With the increasing number of fusion surgeries for isthmic spondylolisthesis being performed, it is imperative to understand the risks and benefits of each surgical approach in concert with the surgeons’ preferences. 18
In this study, we found increased revision rates in the ALIF-alone cohort (ie, includes ALIF, LLIF, etc.) compared to patients that underwent ALIF+PSF or PLIF/TLIF groups. A large proportion of the revisions (48.8%) were performed with decompression in this study. In a study by Fleege et al, they evaluated 72 patients with symptomatic isthmic spondylolysis with a Meyerding degree of I-III and found that both patient cohorts who underwent either ALIF alone or PLIF alone achieved significant pain relief and reduced consumption of pain medication postoperatively. 19 However, they noted that PLIF afforded a superior decompression, which may explain the increased revision rates in ALIF-alone patients seen in our study. 19 Bock et al. utilized data from a German spine registry and evaluated 602 patients with isthmic spondylolisthesis. 20 They observed that there was no difference between ALIF and PLIF in terms of symptomatic benefit, but they noted that ALIF patients required a shorter duration of hospital stay. 20 A meta-analysis by Alhammoud et al., in 2019 found that the reoperation rate was higher in the posterior approach group (TLIF/PLIF+PLF) than in the anterior and posterior combined group (ALIF+PLF/PSF). 21 In a 2023 study by Sharma et al utilizing the National Surgical Quality Improvement Program (NSQIP) database, no significant differences between anterior-alone, posterior-alone, or combined anterior/posterior fusions were observed for hospital length of stay, readmission rates, complication rates, and reoperation rates. It is important to note that these outcomes were limited to 30-day follow-up. Thus, one can only conclude that there is no significant difference in the short-term outcome between anterior-alone, posterior-alone, or combined anterior/posterior fusions for isthmic spondylolisthesis. In our study, we observed higher revision rates in the ALIF-alone cohort at long-term follow-up. Although ALIF with posterior instrumentation increases operative time and exposure, studies have shown that ALIF alone has a higher risk of device failure. Jaeger et al. studied 64 patients (mean age of 46.4 years, 69% undergoing surgery for symptomatic degenerative disc disease, and 31% with L5-S1 isthmic spondylolisthesis) with a mean follow-up of 15.9 months who underwent stand-alone L5-S1 ALIF and found that instrumentation failure occurred in 19% of the patients and pseudoarthrosis in 11% of the patients. 22 Further, isthmic spondylolisthesis was a significant risk factor for instrumentation failure in multivariable analysis. These results are consistent with our findings.
Our study also found higher revision rates in the PLF-alone cohort compared to the PLIF/TLIF group. In a meta-analysis conducted by Luo et al. in 2017, they found no difference in pain scores and patient satisfaction between the 2 groups, but showed that PLF-alone patients had significantly lower fusion rates compared with PLIF. 8 The increased fusion rates seen in PLIF is further corroborated by Musluman et al in their randomized controlled trial where they found 100% fusion rate in the PLIF group compared to 84% in the PLF cohort. 9 They also demonstrated that both lumbar lordosis and the segmental angle had greater improvement in the PLIF group. 9 Interestingly, Lehr et al. evaluated the clinical outcomes of 41 patients at a mean of 11.8 years after single-level instrumented PLF for lumbar degenerative or isthmic spondylolisthesis with neurological symptoms and found favorable postoperative outcomes, including improvement in neurological symptoms and back pain, with only one of the patients requiring revision surgery. 23 Several studies have further demonstrated that there were no significant differences in outcomes between patients who underwent PLIF vs PLF. In a study by Ekman et al. evaluating 163 patients with adult isthmic spondylolisthesis (age range 18-55 years), the levels of pain, the Disability Rating Index (DRI), and the Oswestry Disability Index (ODI), were similar between the PLIF and PLF cohorts at 2-years follow-up. 7 Farrokhi et al. further conducted a randomized prospective study in 80 patients and showed that patients who underwent PLF actually had greater improvement in low back pain and lower incidence of post-operative neurogenic claudication compared to PLIF patients. 10 In a randomized controlled trial performed by Lee at al. in 2014, they evaluated 81 patients aged 60 years or younger with isthmic spondylolisthesis who underwent either PLF or PLIF. 6 They found no difference in clinical outcomes, such as visual analogue scale (VAS) and the ODI, and no difference in postoperative complication rates, such as infection, between the 2 groups. 6 However, none of the above aforementioned studies commented on revision rates following PLIF or PLF. Macki et al. retrospectively reviewed 103 patients comparing PLF vs PLF+PLIF/TLIF and they observed that the PLF+PLIF/TLIF cohort experienced statistically significant greater correction of spondylolisthesis, whereas the PLF-alone group had a significantly higher incidence of reoperation and pseudoarthrosis or instrumentation failure. 24 However, this study also evaluated patients with degenerative spondylolisthesis in addition to isthmic spondylolisthesis, and is further limited by the small sample size.
Sharma et al. noted that the use of combined anterior/posterior approaches increased from 4% in 2012 to 22% in 2020, with a decrease in posterior-alone procedures (87% to 67%) and a mild increase in anterior-alone procedures (9% to 11%). 25 This trend may be due to the increased focus on achieving sagittal alignment goals in the lumbar spine. Lightsey et al. evaluated 70 patients with L5-S1 isthmic spondylolisthesis in a single-center institutional database and found that ALIF with posterior instrumentation demonstrated greater segmental lordosis, regional lordosis, restoration of disc height, as well as greater improvements across patient-reported outcome measures (PROMs) domains compared to TLIF patients. 26
Our current study builds upon previous investigations and furthers understanding regarding the various surgical approaches and their impact on revision outcomes in patients with isthmic spondylolisthesis using a real-world database with a large sample size. Our study observed an overall low number of patients who underwent PLF-alone or ALIF-alone surgeries, and the finding of low utilization of those 2 approaches may reflect the surgeons’ concerns regarding their risks of failure and the need for revision. The findings of our current study revealed an increased revision rate associated with those 2 approaches that supports this concern. Surgical strategies providing both anterior and posterior column support may result in lower revision rates based on current real-world data shown in this study.
There were several limitations to this study. First, this was a retrospective investigation, and there is potential for occult confounding variables. CPT and ICD codes were utilized to extract the data, therefore missing data, errors in coding, and variability in coding data should be considered. Similarly, due to the relative lack of granularity of the CPT coding system, we were unable to differentiate between PLIF and TLIF, as well as ALIF, OLIF, LLIF, etc. Further, different types of ALIF (eg, stand-alone cage, plated, screw fixation, pin fixation, etc.) were unable to be differentiated in this study, both due to lack of coding granularity, as well as relatively lower sample size. The current study also did not evaluate certain clinical data, including patient symptoms, patient reported outcomes, and additional imaging findings, such as degree of kyphosis and slip angle, as this information was not available in the database utilized. Additionally, other significant clinical risk factors for revision spine surgery such as osteoporosis, radiographic spinopelvic parameters, and obesity were not available for comparison. Also, the database utilized in the current student does not continuously follow all patients, so the analysis may miss patients who change or lose insurance. However, we calculated the number at-risk in our survivorship analysis to account for the loss to follow-up. Further, the indications for revision and the specific nature of the revision surgery were not readily available in the database, therefore future studies should evaluate revision indications to further contribute to the current study. Also of note, given lack of direct access to clinical data, this study was unable to determine specifically whether the revision surgery was performed at the index level, an adjacent level, or a remote level. However, the strengths include the large sample of patients and the demographic information that can be obtained.
Conclusion
In this retrospective analysis of single-level arthrodesis for isthmic spondylolisthesis, patients who underwent ALIF-alone had higher revision rates than those who underwent PLIF/TLIF and ALIF+PSF surgery, and those who underwent PLF alone had higher revision rates than those who underwent PLIF/TLIF. Surgical strategies providing both anterior and posterior column support may result in lower revision rates.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.