
Abstract
Study Design
An overview of the methods used to develop clinical practice guidelines (CPGs).
Objectives
Acute spinal cord injury (SCI) and intraoperative SCI (ISCI) can have devastating physical and psychological consequences for patients and their families. To date, there are several studies that have discussed the diagnostic and management strategies for both SCI and ISCI. CPGs in SCI help to distill and translate the current evidence into actionable recommendations, standardize care across centers, optimize patient outcomes, and reduce costs and unnecessary interventions. Furthermore, they can be used by patients to assist in making decisions about certain treatments and by policy makers to inform allocation of resources. The objective of this article is to summarize the methods used to develop CPGs for the timing of surgery and hemodynamic management of acute SCI, as well as the identification and treatment of ISCI.
Methods
The CPGs were developed using standards established by the Institute of Medicine (now the National Academy of Medicine), the Guideline International Network and several other organizations. Systematic reviews were conducted according to accepted methodological standards (eg, Institute of Medicine, Agency for Healthcare Research and Quality and Patient-Centered Outcomes Research Institute) in order to summarize the current body of evidence and inform the guideline development process. Protocols for each guideline were created. A multidisciplinary guideline development group (GDG) was formed that included individuals living with SCI as well as clinicians from the broad range of specialties that encounter patients with SCI: spine or trauma surgeons, critical care physicians, rehabilitation specialists, neurologists, anesthesiologists and other healthcare professionals. Individuals living with SCI were also included in the GDG. The Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach was used to rate the certainty of the evidence for each critical outcome. The “evidence to recommendation” framework was then used to translate the evidence obtained from the systematic review to an actionable recommendation. This framework provides structure when assessing the body of evidence and considers several additional factors when rating the strength of the recommendation, including the magnitude of benefits and harms, patient preferences, resource use, health equities, acceptability and feasibility. Finally, the CPGs were appraised both internally and externally.
Results
The results of the CPGs for SCI are provided in separate articles in this focus issue.
Conclusions
Development of these CPGs for SCI followed the methodology proposed by the Institute of Medicine the Guideline International Network and the GRADE Working Group. It is anticipated that these CPGs will assist clinicians implement the best evidence into practice and facilitate shared-decision making with patients.
Keywords
Introduction
The Institute of Medicine (IOM, now the National Academy of Medicine) defines clinical practice guidelines (CPGs) as “statements intended to optimize patient care that are informed by a systematic review of the literature and an assessment of the benefits and harms of alternative care options. 1 ” CPGs help to translate the current evidence into actionable recommendations, standardize care across centers, optimize patient outcomes, as well as reduce costs and unnecessary interventions. 2 Furthermore, they can be used by patients to assist in decision making and by policy makers to inform allocation of healthcare resources. In contrast, CPGs should not encourage “cookbook” medicine, trump clinical judgement or be used for reimbursement policies, performance measures, or legal precedents.
The IOM, the Guideline International Network and several other international organizations have proposed standards for guideline development in order to ensure that recommendations are reliable and implementable.1,3 Important principles for generating CPGs are that they must: • Be based on a methodologically sound systematic review of the literature that synthesizes the best available evidence.1,3. • Be developed by a panel that includes representation from key stakeholder groups affected by the recommendations (ie, a multidisciplinary group of clinicians, individuals with lived experience and their caregivers, as well as policy makers). • Consider the values and preferences of providers, patients and policy makers. • Include a rating of both the quality of evidence and the strength of the recommendation. • Provide a clear explanation of the balance between the benefits and risks, alternative care options and resource use. • Outline implementation strategies that consider personal, guideline-related and external factors that may impede knowledge translation. • Be critically appraised by both internal and external reviewers. • Be updated when new evidence arises related to benefits or harms of proposed or alternative interventions.
Furthermore, the process for developing a CPG must be transparent, publicly accessible and minimize intellectual and financial conflicts of interest.
Guideline developers have increasingly adopted the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach to rate the certainty of the evidence and the strength of the recommendations. This system provides structure when assessing the body of evidence and considers several additional factors when rating the strength of the recommendation, including the magnitude of benefits and harms, patient preferences, resource use, health equities, acceptability and feasibility. The objective of this article is to highlight the methodology used to develop CPGs on the timing of surgical decompression and hemodynamic management of spinal cord injury (SCI), as well as the identification and management of intraoperative SCI (ISCI).
Overview of the Guideline Development Process
Figure 1 highlights the 4 steps involved in developing and disseminating CPGs: (i) identify critical knowledge gaps and define the clinical problem; (ii) conduct systematic reviews of the literature to synthesize the available evidence and assess the risk of bias; (iii) translate the evidence into recommendations using the GRADE framework; and (iv) implement the recommendations into clinical practice by identifying and addressing important barriers. An overview of the guideline development process. Extracted from a previously published article in the Global Spine Journal by Tetreault et al (2019) entitled: Development and Implementation of Clinical Practice Guidelines: An Update and Synthesis of the Literature with a Focus in Application to Spinal Conditions.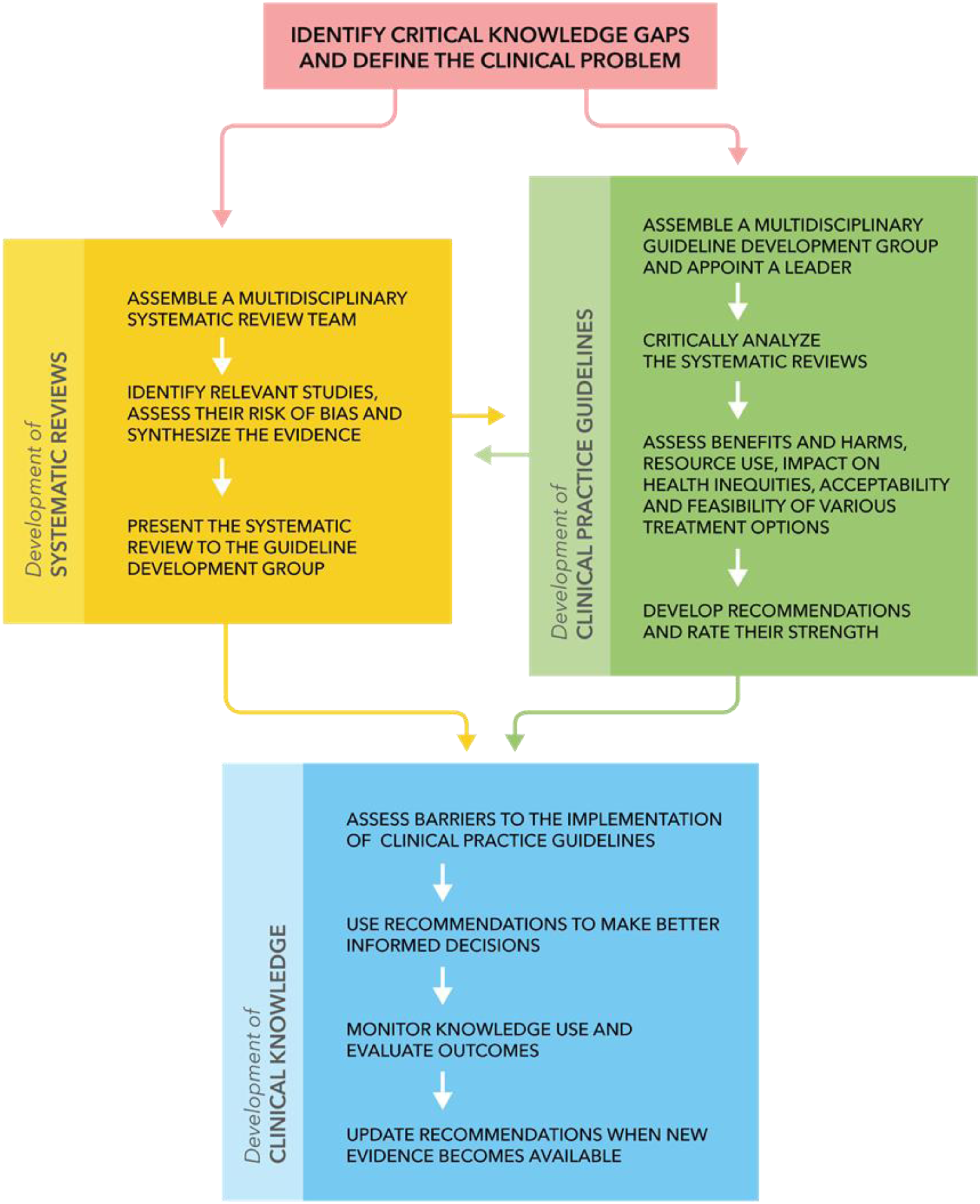
Identify Critical Knowledge Gaps and Define the Clinical Problem
This CPG aimed to develop recommendations on (i) the timing of surgical decompression in acute SCI; (ii) the hemodynamic management of acute SCI; and (iii) the identification and management of ISCI in patients undergoing surgery for spine-related pathology. The leadership group considered these topics to be high-priority as recommendations have the potential to improve healthcare outcomes, enhance quality of life and reduce mortality in individuals with acute or intraoperative SCI. Furthermore, SCI in general is a condition with significant disease burden, cost of management and variability in practice standards. Finally, for the 2 CPGs being updated, the leadership group agreed that there was new evidence available that may impact current recommendations and help resolve controversy or uncertainty around these topics. It was anticipated that CPGs on these topics would help to distill the extensive evidence base available for SCI into actionable recommendations; develop diagnostic and treatment algorithms in an attempt to standardize care across centers; reduce costs and unnecessary interventions; and improve outcomes and minimize permanent disability. Specific objectives of these guidelines include to (i) identify the optimal timing of surgical intervention; (ii) delineate specific mean arterial pressure (MAP) targets and the duration of MAP augmentation therapy; and (iii) standardize the definition of ISCI, summarize the diagnostic accuracy of intraoperative monitoring techniques, determine risk factors of ISCI and propose treatment algorithms for the management of potential ISCI. For further information on the rationale and scope of the CPG, please refer to a separate article in this focus issue entitled “A Clinical Practice Guideline on the Timing of Surgical Decompression and Hemodynamic Management of Acute Spinal Cord Injury and the Prevention, Diagnosis and Management of Intraoperative Spinal Cord Injury: Introduction, Rationale and Scope.”
The key questions addressed by the CPG included:
Timing of Surgical Decompression
• Should we recommend early decompressive surgery (≤24 hours after injury) for adult patients with acute SCI regardless of injury severity and neurological level? • Should we recommend ultra-early decompressive surgery for adult patients with acute SCI regardless of injury severity and neurological level?
Hemodynamic Management
• Should we recommend the augmentation of MAP to at least 75-80 mmHg and not higher than 90-95 mmHg in order to optimize spinal cord perfusion in acute SCI? • Should we recommend the augmentation of MAP for a duration of 3-7 days in order to optimize spinal cord perfusion in acute SCI? • Should we recommend the use of a specific vasopressor in order to achieve MAP-directed goals in patients with acute SCI?
Intraoperative Spinal Cord Injury
• Should we recommend intraoperative neurophysiologic monitoring for patients undergoing spine surgery deemed to be “high risk”? • Should we recommend that patients at “high risk” for ISCI during spine surgery be proactively identified, that after identification of such patients, multi-disciplinary team discussions be undertaken to manage patients, and that an intraoperative protocol including the use of intraoperative neuromonitoring (IONM) be implemented?
The objectives of the timing of surgery and hemodynamic management CPGs were to determine whether early surgical decompression and augmentation of the MAP results in clinically meaningful improvements in functional status and quality of life in patients with SCI. The main outcome of interest was the ASIA Impairment Score (AIS). This tool is used to assess the severity and level of SCI as well as quantify both motor and sensory deficits; improvement on the AIS can translate to significant changes in function that a patient may find meaningful. The aims of the CPGs on ISCI were to identify patient, disease and surgical characteristics that pose higher risk for ISCI during spine surgery, discuss the role of IONM and develop an intraoperative protocol for the treatment of ISCI.
The Systematic Review Team and Guideline Development Group
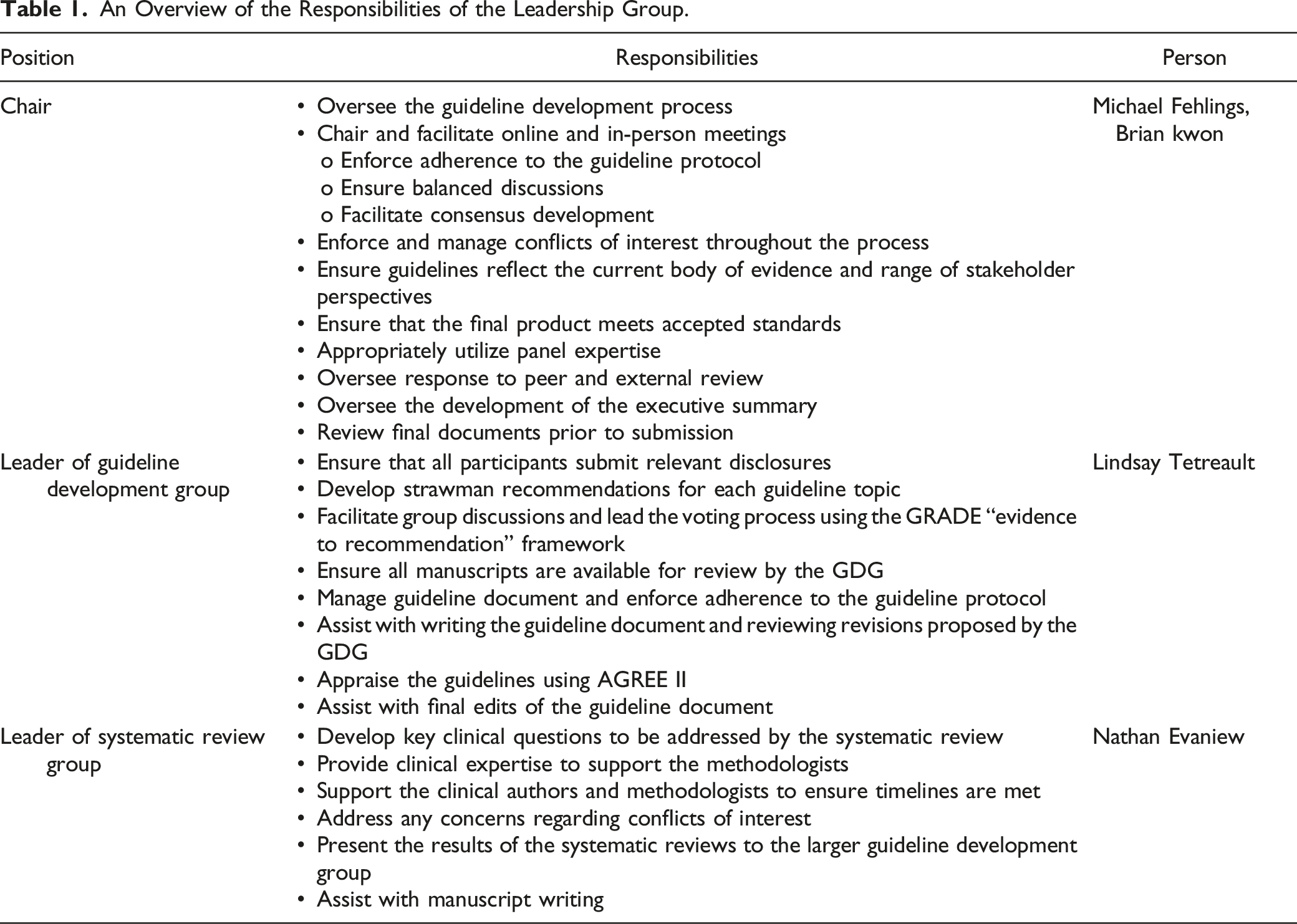
An Overview of the Responsibilities of the Leadership Group.
The systematic review team was multidisciplinary and consisted of spine surgeons, neurologists, critical care physicians and rehabilitation medicine specialists. Members of the systematic review team were responsible for providing clinical input and expertise, as well as drafting the introduction and discussion sections of each manuscript. An independent organization specializing in systematic and comparative effectiveness reviews (Aggregate Analytics, Inc.) guided the process and assisted in rating the strength of evidence. There was some overlap between the systematic review team and the GDG.
Members of the Guideline Development Group.
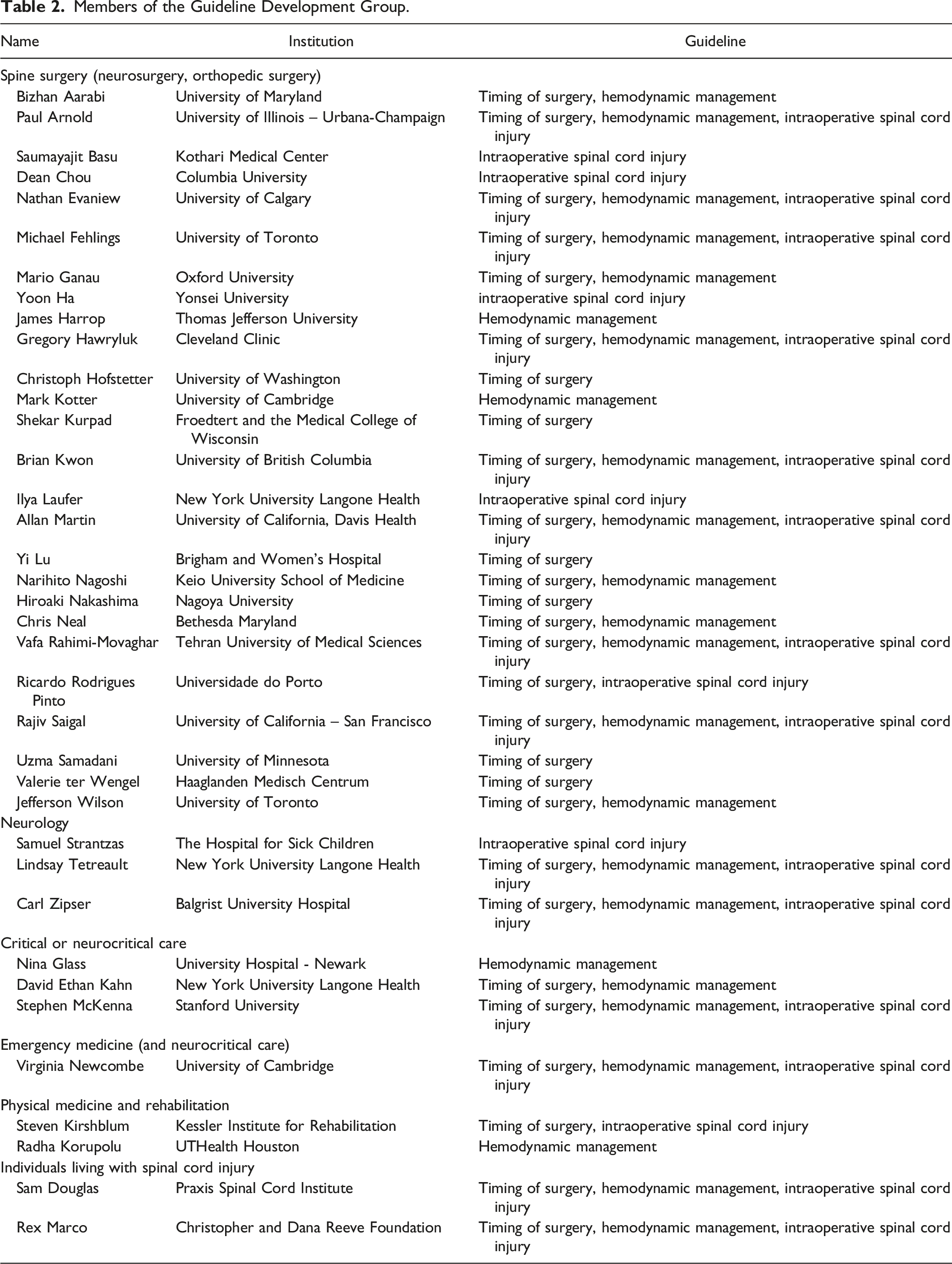
Methodologists from Aggregate Analytics Inc. were non-voting members of the GDG and provided expertise in conducting the systematic reviews of the literature and applying GRADE methodology to formulate recommendations.
Developer
This guideline was developed under the auspices of AO Spine and Praxis Spinal Cord Institute. These funding bodies did not control or influence the editorial content of the articles or the guidelines process and were completely independent from the GDG.
AO Spine is an academic professional society and a Clinical Division of the AO Foundation based in Davos Switzerland. In its vision statement, AO Spine describes itself as a “leading global academic community for innovative education and research in spine care, inspiring lifelong learning and improving patients' lives.” Further, it as “an international community of spine surgeons generating, distributing, and exchanging knowledge to advance science and the spine care profession through research, education, and community development.” The funding from AO Spine comes from intramural and extramural sources. The intramural funding consists of core and additional funding, both of which come from the AO Foundation. The extramural funding comes from various external sources. Praxis Spinal Cord Institute is a Canadian-based not-for-profit organization that aims to accelerate the translation of scientific discoveries into improved treatments for individuals with SCI. In its mission statement, Praxis wishes to “lead collaboration across the global SCI community by providing resources, infrastructure and knowledge.” It is also the purpose of this organization to “accelerate the translation of evidence and best practices to reduce the incidence and severity of SCI, reduce long-term costs, and enhance the quality of life for those living with SCI.” The funding from Praxis Spinal Cord Institute was from Western Economic Diversification Canada.
Systematic Review of the Literature
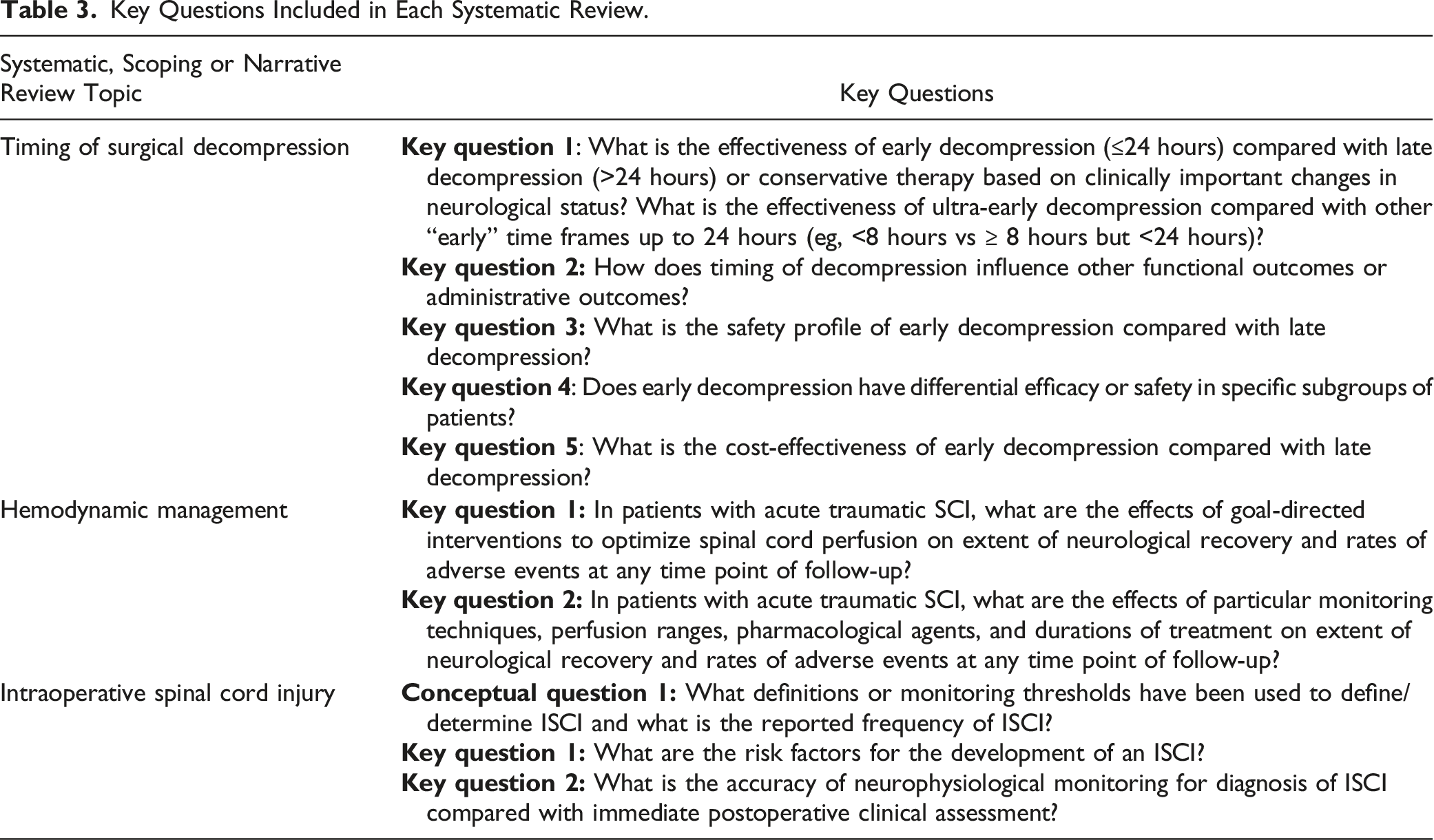
Key Questions Included in Each Systematic Review.
For individual studies, risk of bias was assessed using pre-defined criteria: the Cochrane tool for risk of bias for randomized controlled trials,5-7 the Risk of Bias In Non-randomized Studies of Interventions (ROBINS-I) for observational studies 8 the National Institutes of Health quality assessment tool for non-comparative studies, 9 the Quality in Prognosis Studies (QUIPS) for risk factor studies and the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) for diagnostic studies.10,11 Previous meta-analyses, pooled analyses or published systematic reviews were assessed using AMSTAR-2 criteria and/or guidance related to reporting of specialized analyses.12-16
The GRADE Approach for Assessing the Overall Quality of Evidence: Reasons for Downgrading and Upgrading.
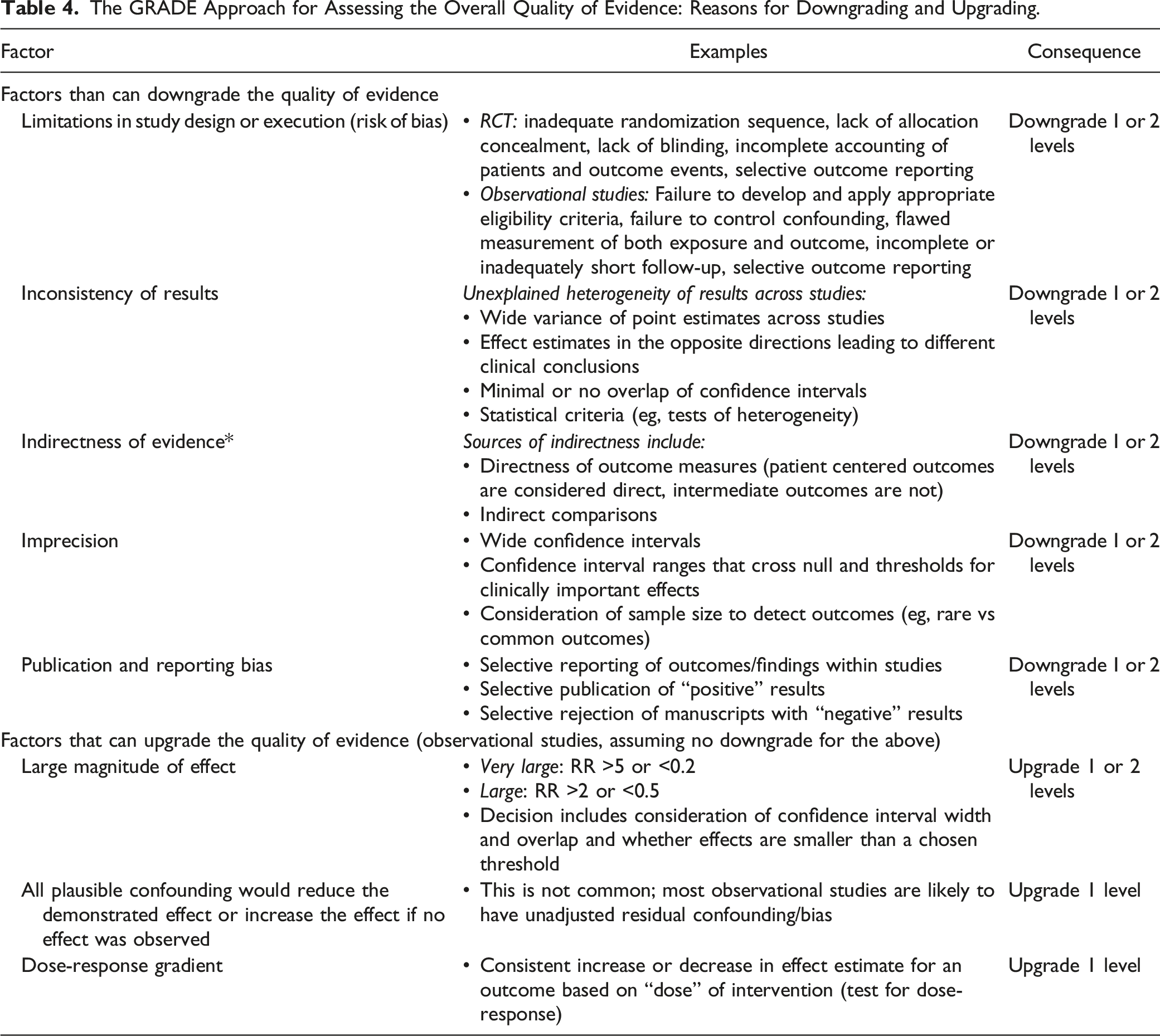
Interpretation of the Grading of the Evidence.
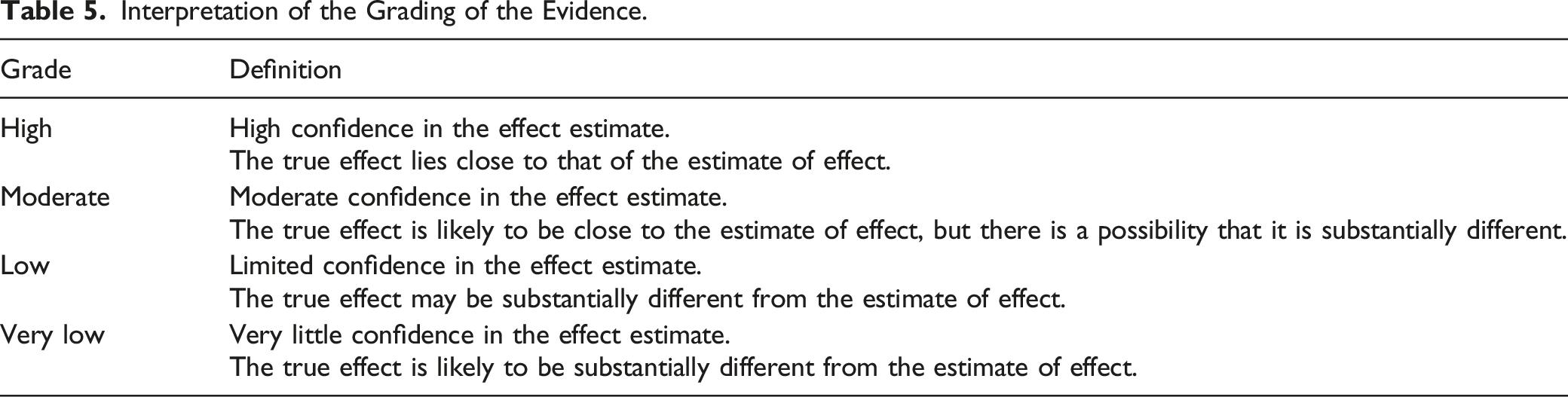
Results from these systematic, scoping and narrative reviews as well as evidence tables were distributed to the GDG and were presented at an online meeting. The systematic review team leader was also a member of the GDG and participated in discussions in order to ensure understanding of the evidence and appropriate interpretation of the effect size for each outcome.
Updating and Developing Clinical Practice Guidelines Using the GRADE Approach
A guideline protocol was formulated using the Conference on Guidelines Standardization (COGS) checklist.28,29 This checklist was created by a multidisciplinary group of individuals with considerable experience in guideline development, dissemination and implementation in order to standardize guideline reporting. The protocol summarizes the focus, rationale and objectives of the CPGs, defines important terms, and highlights the aspects of care covered by the CPG, the proposed users, and implementation strategies. The Checklist for Reporting the Updating Process (CheckUP) was also used to guide the update of the CPG on timing of surgical decompression and hemodynamic management of SCI. 30 The guideline protocol is referenced in A Clinical Practice Guideline on the Timing of Surgical Decompression and Hemodynamic Management of Acute Spinal Cord Injury and the Identification and Treatment of Intraoperative Spinal Cord Injury: Introduction, Rationale and Scope.”
The leadership group was responsible for ranking the outcomes reported in the systematic review based on importance in determining treatment options and influencing decision-making: critically important, important but not critical and of limited importance. The ranking was reviewed during the GDG meetings and any changes were voted on by the GDG. Each guideline document summarizes the outcomes that were deemed to be critically important when developing the recommendations.
The GRADE Evidence to Recommendation Framework.
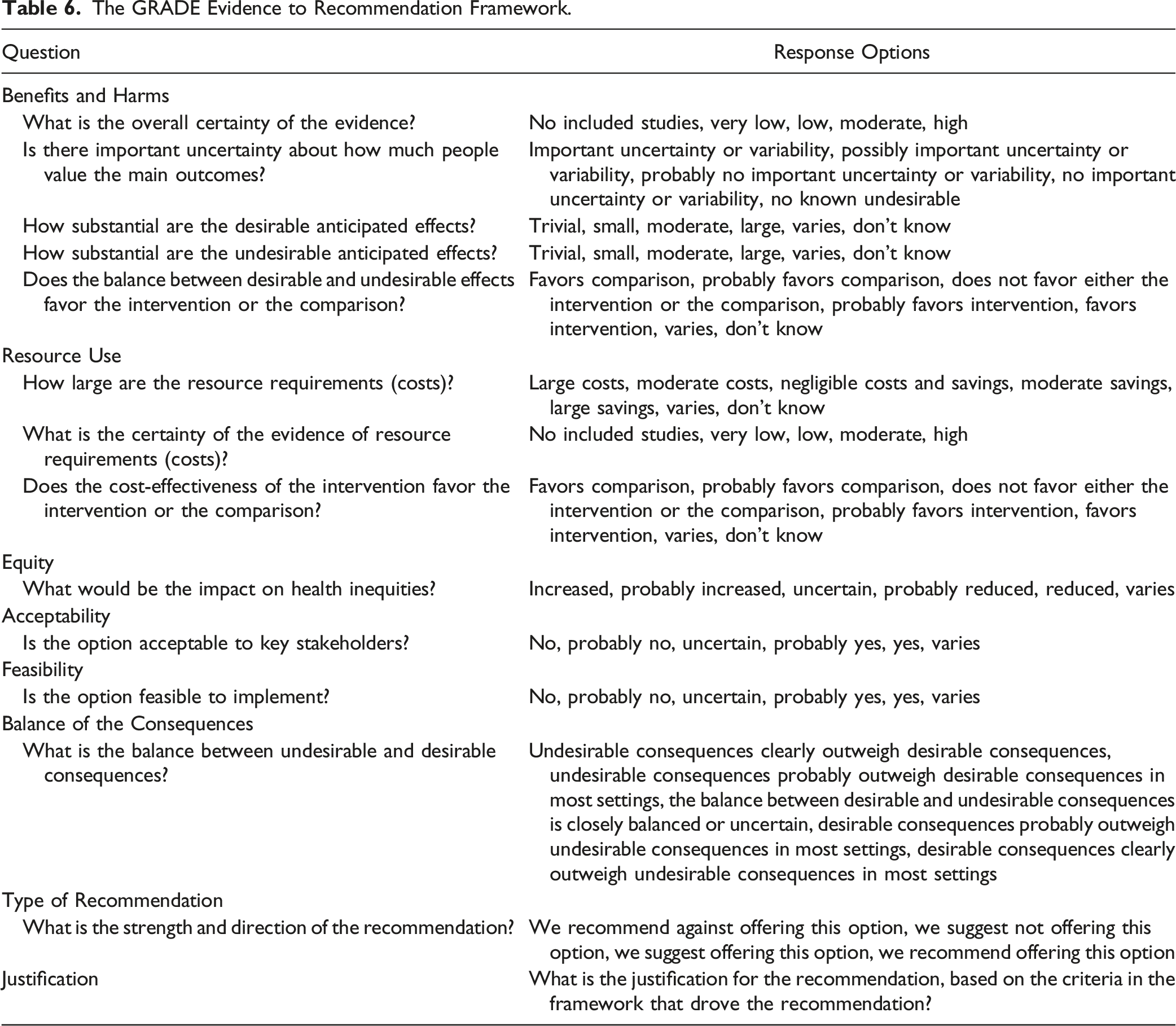
Three separate online meetings were held over Zoom in order to translate the evidence summarized in the systematic reviews into actionable recommendations. In preparation for the guideline development meeting, the leader of the GDG created “strawman” recommendations using the GRADE framework in order to facilitate initial discussions. This document was shared ahead of the meeting and reviewed during the meeting. Members of the GDG anonymously voted on each question in the framework. If there were discrepancies in voting, participants were asked to justify their response by sharing their perspectives, clinical expertise or personal experiences. A threshold of 80% was considered consensus. Results of the voting and discussions were documented throughout the process and are summarized in the “rationale for recommendation” section of each guideline. The final recommendations were created by the leadership group and distributed to the GDG via Redcap for voting. The wording of each recommendation was refined based on the feedback submitted by the GDG.
Interpretation of the Recommendations
GRADE has delineated 4 types of recommendations based on the confidence in the desirable and undesirable consequences. If the GDG was confident (based on overall strength of evidence for benefits and harms) that the desirable effects outweighed the undesirable effects or vice versa, a strong recommendation was generated either for or against a particular intervention. In contrast, if the GDG was less confident about the balance between the desirable and undesirable consequences, a weak recommendation was proposed. For the purpose of this CPG, the strength of the recommendation was reflected in its wording. For example, “we recommend” denotes that the recommendation is strong, while “we suggest” indicates that the recommendation is weak.35-37 In situations where the evidence is insufficient or unavailable, expert consensus was required to formulate the recommendations.
The strength of the recommendation has different implications for patients, clinicians and policy makers. A strong recommendation indicates that most patients would want to and should receive the recommended course of action and that the recommendation can be adapted as policy in most situations.34,37 Furthermore, formal decision aids are unlikely to be needed to assist patients in making a decision consistent with their values and preferences 34 . A weak recommendation reflects that (i) the majority of individuals would want the suggested course of action, but many would not, (ii) clinicians must recognize that different choices will be appropriate for different patients and should help a patient arrive at a decision consistent with his or her values or preferences, and (iii) policy making will require substantial debate and involvement of many stakeholders.34,37
Internal Appraisal
The Appraisal of Guidelines for Research and Evaluation II.
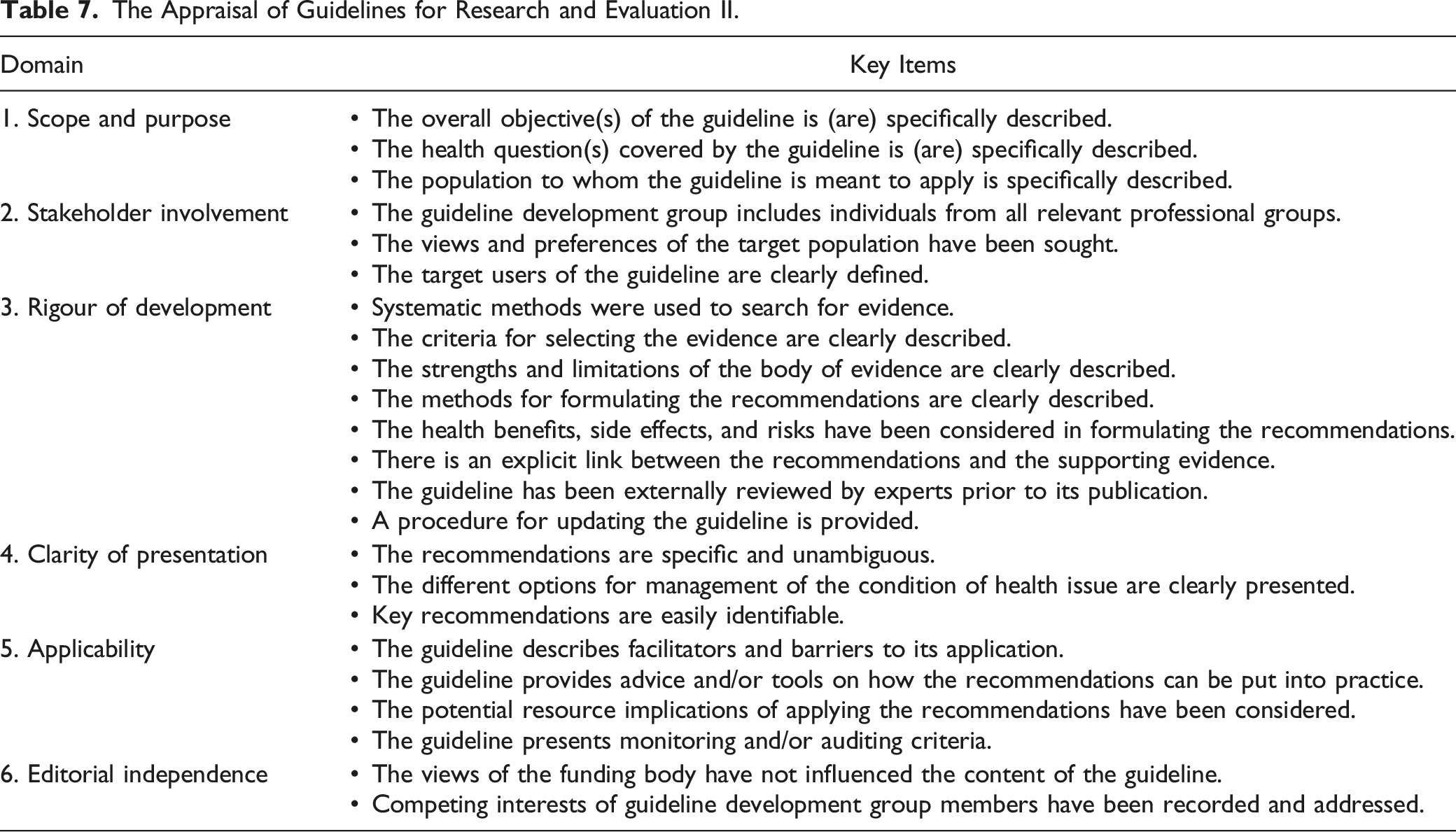
The CheckUP tool also facilitated internal review of the updated guidelines. 30 Given the overlap of items with AGREE-II, only the items specific to distinguishing the updated and previous versions were used to inform final editing. Using these tools, modifications were made to the guideline documents and approved by the GDG.
External Review
A multidisciplinary group of clinicians were invited to externally review the guideline document. These individuals were selected based on their clinical expertise and their willingness to participate. Each reviewer was required to disclose any relevant financial or intellectual conflicts of interest. The CPGs were also reviewed by prominent societies in the fields of spine surgery and critical care. Comments and feedback from these external reviewers were assessed by the GDG leadership and incorporated into the final draft. Substantial changes in the recommendations were subjected to approval by the GDG. The final CPGs were distributed to the AO Spine and Praxis Spinal Cord Institute for their endorsement.
Update Plan
The guidelines will be reviewed by the primary sponsor at 3 to 5 years following publication. A working group will monitor the body of literature and search for new evidence that may influence the proposed recommendations. The working group will discuss the need to update the guideline with the leadership of the sponsoring organization. An update to the CPG is recommended if there are changes in (i) the evidence related to harms and benefits; (ii) outcomes which would be considered important for decision-making; (iii) ranking of current critical and important outcomes; and (iv) available interventions and resources. 40
Footnotes
Acknowledgments
MGF is supported by the Robert Campeau Family Foundation/Dr C. H Tator Chair in Brain and Spinal Cord Research at UHN. BKK is the Canada Research Chair in Spinal Cord Injury and the Dvorak Chair in Spinal Trauma. This Focus Issue was reviewed by the Joint Guidelines Review Committee of the American Association of Neurological Surgeons and Congress of Neurological Surgeons as well as the North American Spine Society. However, this review process does not constitute or imply endorsement of this work product by these organizations.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was financially supported by the AO Foundation, AO Spine and Praxis Spinal Cord Institute. This study was jointly organized and funded by AO Foundation through the AO Spine Knowledge Forum Spinal Cord Injury (SCI) (www.aospine.org/kf-sci), a focused group of international SCI experts, and the Praxis Spinal Cord Institute (![]() ) through funding from Western Economic Diversification Canada. The funding bodies did not control or influence the editorial content of the articles or the guidelines process. Methodologic and analytic support for this work was provided by Aggregate Analytics, Inc, with funding from the AO Foundation and Praxis Spinal Cord Institute.
) through funding from Western Economic Diversification Canada. The funding bodies did not control or influence the editorial content of the articles or the guidelines process. Methodologic and analytic support for this work was provided by Aggregate Analytics, Inc, with funding from the AO Foundation and Praxis Spinal Cord Institute.