
Abstract

Let’s start with a new form of (not yet required) disclosure: this Editorial has not been written with any help or assistance of Chat GPT or any other form of Artificial Intelligence based composition platform. The following are just plain old human ‘stream of consciousness’ musings by some aging spine surgeons reflecting about the current state of the medical/spine world and how we might be able to positively affect future Spine care. It might be helpful to know that the following perspectives were created by members of the ‘Spine Boomer’ generation, an age group of Spine surgeons who got to experience the introduction of the first iterations of commercial mainstream spinal instrumentation systems in the early nineteen-nineties of the last century. Hopefully, this generational lens allows for a broader perspective on the transitions that have significantly impacted our Spine practices from its analog and less structured origins as practiced in the last century to the increasingly digitized current reality along with its expanded governance burdens and the recent dislocations brought on by the SARS CoVID-19 pandemic.
Undoubtedly, the global dislocations brought on by the viral pandemic continue to evolve in many unpredicted ways and have not allowed for a return to ‘business-not-as-usual’. And as of this writing it is not at all clear when or if we ever will return to a previous state of normalcy. A byproduct of this generational pandemia has been the shocking experience of an unprecedented degree of personal control loss for everyone in their everyday lives. The field of healthcare delivery was specifically almost immediately taken over by governmental entities even in countries with functioning democracies. Individualized patient care was subsumed by newly empowered authorities that meted out access restrictions and applied rationing with little or no accountability or reasoning. While there always have been substantial differences in the practice of Spine care depending upon the socioeconomic and political realities of countries around the world, for Spine surgery the advent of the Covid-19 crisis overnight relegated our specialty into a largely second-tier priority subject to harsh triage criteriae. The ensuing loss of physician decision-making authority has been unprecedented in modern history and remains incompletely understood in its long-term implications. For instance, how many patients afflicted with metastatic disease or de novo spine infections were delayed in their detection and prematurely died, how many cervical myelopathy patients progressed into irreversible quadriparesis or sustained central cord injuries from ground level falls? We don’t yet know, as it will take years to sort out these and more indirect fallouts from disruptions of normal care models during the lockdown era of the corona virus pandemic. From a psychological perspective a profound shift in health care ethics has also become apparent as compassionate care for all and especially the vulnerable and weak was thrown overboard as lockdowns were imposed. As isolation became the new mantra the state of public mental health has taken a hit and individual patient focused care has been replaced with overloaded emergency rooms and direct communication lines have become bogged down in unresponsive phone trees.
Continuing beyond the actual pandemic the ensuing continued fiscal strains on many health care systems seems to have made it far more acceptable for fiscally focused administrators to instruct surgeons to emphasize ‘medical treatments’ in lieu of surgical intervention for patients afflicted with more complex problems in order to ‘increase margins to support the mission’, a frequently heard refrain that expresses the quest for profitability of health care systems. These recent developments have finalized the shift away from the premillennial more surgeon/physician driven patient oriented health care delivery model (‘Pyramidal system’). The increased bureaucratic regulatory burden, such as the DRG coding and HIPPAA regulations in the USA introduced after the turn of the century, served as an excuse to end the traditional largely physician directed hierarchical system by introducing a ‘partnership arrangement’ (also referred to as the ‘Dyad’ model), where medical leaders were placed side-by-side with administrators to run hospitals, ostensibly to better cope with the increased compliance requirements.
1
The tag line ‘Let us do the management part and you worry about the medical things’ probably best circumscribes the concept inherent to this partnership. Tellingly, it was during this period of ‘partnership’ that doctors, who had earned their academic titles following many years of arduous selection, studies, tests and challenges, were suddenly relegated into a new class of health care delivery workers – ‘ Three phase model of medical governance Pyramidal System - Pre 2000: Organized under physician leadership Dyad Model 2000-2019- Joint leadership model Administration and Physicians Corporate model 2020 onwards- PostCovid control of healthcare systems through corporate and administrative entities. Physicians are exchangeable workers subject to ‘productivity' and ‘value' criteriae.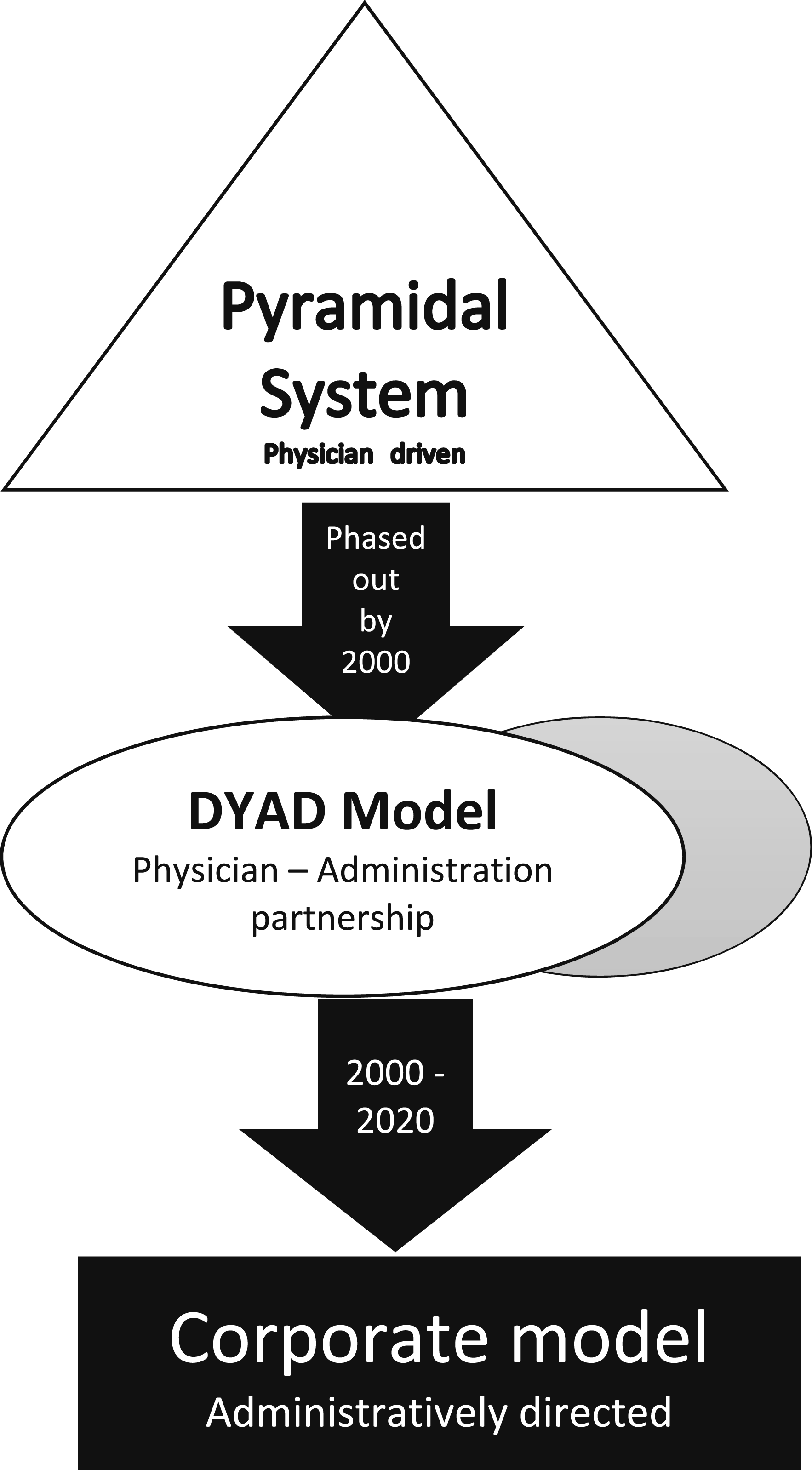
Undoubtedly, the impact of large-scale societal changes, such as an increasingly aging patient population with its greater prevalence of comorbidities have made health care increasingly challenging and expensive, especially in the more developed countries of the world. As there are growing pressures to ration health care and making actual health more efficient new approaches are needed to optimize the purchasing power of health care expenditures. One of the most overlooked factors in driving up health care costs are the rising number of administrators relative to physician numbers. According to the US Bureau of Labor Statistics (NCHS) the numbers of health administrators rose by 500% between 1970 and 1993 and overall exploded by over 3000% since the 1970’s. Remarkably the key surge in the rise of the growth rate occurred in the early ninety-ninetees following the implementation of prospective payment systems (DRG – Diagnosis related groups) in the US along with the creation of federal insurance systems and further fueled by regulatory acts such as the HIPAA (Health Insurance Portability and Accountability Act) and others. In comparison, the number of physicians in the US has remained relatively static over the same time period. Commensurate to this statistical rise in the number of administrators the cost of their compensation has risen similarly, while physician compensation has remained static. Remarkably, back in 1987 the Woolhandler and Himmelstein analysis identified health care spending attributable to administrators to be at least 117% higher in the United States compared to Canada and was responsible for about half the total difference in health care spending between the two neighboring nations. It stands to reason that these differences have only become exacerbated since then.2-5
The more recent statistics consistently identify a remarkable ratio of 10 administrators to each physician in the US. 6 It is highly doubtful that this rise of administrator numbers relative to physicians has been associated with any improvement of actual patient safety or quality of care. Certainly, any meaningful value discussion in Medicine should start and finish with the non-revenue generating overhead structure that most medical systems, such as present in the USA, is saddled with. From a compensation perspective, administrators have also eclipsed physicians dramatically – cemented by their controlling role in the new corporate health care model. In the USA the compensation of the CEO’s of major nonprofit medical center rose by 93% from 1.6 million USD ± .9 in 2005 to 3.1 ± 1.7 million USD in 2015 with the wage gap ratio from CEO to Orthopaedic Surgeons increasing from 3:1 to 5:1 over the same time period, as compared to a 7:1 wage ratio for CEO’s relative to Pediatricians which rose to a gap of 12:1 from 2005 to 2015. In the study by Du et al actual physician performance actually rose as shown in general metrics such as decreased of length of stay of 5% with a 3% increase of outpatient office visits and a 19% increase of ER visits in the comparison time frame of 2005 to 2015. 7
Beyond the unfavorable fiscal impact of the burgeoning bureaucracy work force, future psychological studies may also find a causal connection of physician burnout with administrative overload and disempowerment of physician/surgeon autonomy. As our health care discussions necessarily intensify around creating better value while delivering optimized efficiencies and reducing cost the obvious question is how we can tilt this ratio back towards those who actually provide the value creation in the first place – the physicians/surgeons focused on our direct interaction with patients. That something has to be done soon is clear, in the US direct and indirect healthcare expenditures now devour 18.3% of the gross domestic product. 8
Artificial intelligence (AI) has been described to be a potential tech savior of mankind. 9 One obvious application has been to look at its potential role in medicine such as replacing physician decision making with AI platforms. One recent study attributed a 72% accuracy in making a correct medical diagnosis and recommending final care decisions to the Chat GPT platform based on 36 standardized clinical scenarios. The apparent limitation was not more than a 60% accuracy in making correct differential diagnoses. 10 While this concept opens up interesting perspectives in streamlining primary care and chronic disease management - after completion of appropriate validation studies and thoughtful ethical deliberations, of course - a much more immediate and compelling application would be to streamline administrative overhead by use of AI in many areas such as data entry, analytics, reporting and basic data quality checks for starters. The ramp-up for such functionalities would be far less daunting than replacing physicians. Such implementations could actually reduce the numbers of administrators relative to physicians/surgeons. For instance – it is hard to understand why budget alignment processes as well as coding and insurance appeals processes in the future can’t be taken on by machine learning tools under human supervision instead of doling out these tasks to ever larger number of anonymous administrators, who are increasingly working in outsourced remote and centralized business offices fully detached from the physicians they originally were supposed to serve in their patient care mission. And Human Resources, which have become such a dreaded and frequently politicized suborganization within larger business enterprises, may actually advance their credibility deficiencies by deferring some decision making to an AI driven and potentially more objective algorithm supervised in a collaborative fashion by main stakeholders.
Ultimately, a lasting health compact accepted by the public and patients that will prevail in any open democratic society combines fair access to quality care with cost efficiency and accountability. Making reduction of nonclinical overhead a priority and improving value, as exemplified in smaller private surgeon driven enterprises such as ambulatory surgery centers, should be a common goal in health care. This concept should also hold great merit for other not-for profit organizations and foundations where administrative overbearingness has similarly overtaken the original mission. Better transparent accounting of actual funds spend on mission vs administrative overhead is long overdue. Artificial Intelligence as an organizational efficiency generator formulated and supervised by actual stakeholders holds great promise but cannot be a solution by itself. The time is now for us as surgeons to be engaged in directing how AI frameworks are formulated and where such applications are placed to avoid misuse. And for the sake of overall cost containment lets creatively look at rolling back the tide of unfettered administrative growth and control by applying AI tools to the bureaucratic processes of our hospitals and medically related not-for profits.