
Abstract
Study design
A retrospective study.
Objectives
The quality of care (QoC) for spinal column/cord injury patients is a major health care concern. This study aimed to implement the QoC assessment tool (QoCAT) in the National Spinal Cord/Column Injury Registry of Iran (NSCIR-IR) to define the current state of pre- and post-hospital QoC of individuals with Traumatic Spinal Column and Spinal Cord Injuries (TSC/SCIs).
Methods
The QoCAT, previously developed by our team to measure the QoC in patients with TSC/SCIs, was implemented in the NSCIR-IR. The pre-hospital QoC was evaluated through a retrospective analysis of NSCIR-IR registry data. Telephone interviews and follow-ups of patients with SCI evaluated the QoC in the post-hospital phase.
Results
In the pre-hospital phase, cervical collars and immobilization were implemented in 46.4% and 48.5% of the cases, respectively. Transport time from the scene to the hospital was documented as <1 hour and <8 hours in 33.4% and 93.9% of the patients, respectively. Post-hospital indicators in patients with SCI revealed a first-year mortality rate of 12.5% (20/160), a high incidence of secondary complications, reduced access to electrical wheelchairs (4.2%) and modified cars (7.7%), and low employment rate (21.4%).
Conclusion
These findings revealed a significant delay in transport time to the first care facilities, low use of immobilization equipment indicating low pre-hospital QoC. Further, the high incidence of secondary complications, low employment rate, and low access to electrical wheelchairs and modified cars indicate lower post-hospital QoC in patients with SCI. These findings imply the need for further planning to improve the QoC for patients with TSC/SCIs.
Introduction
Traumatic Spinal Column and Cord Injuries (TSC/SCIs) are disabling illnesses associated with long-term and potentially permanent impairments, resulting in enormous financial expenditures for the afflicted, their families, and the health care system. 1 This public health issue affects 40-80 people per million annually, with a reported range between 4 and 195 patients per million worldwide.2,3 As a result of the considerable burden and expense associated with TSC/SCIs, regional and national program initiatives have been developed in Iran. The National Spinal Cord Injury Registry of Iran (NSCIR-IR) is one such program.4–6 Health care systems have struggled to increase treatment accessibility and quality of care (QoC) for those with TSC/SCIs. However, research on the quality of care for patients with TSC/SCIs is scarce, the majority being based on national registries. 7
Based on a recent review, 7 QoC in TSC/SCIs can be categorized into three domains: 1 health system structure, 2 medical and para-medical processes, and 3 patient outcomes. These concepts have been formulated into indicators, such to serve as comprehensive assessment tools that assess the QoC for TSC/SCIs patients. Further, the QoC for TSC/SCI patients can be classified into three discrete time periods: 1) Pre-hospital phase, consisting primarily of emergency medical services, police stations, and transportation/logistics facilities. 2) In-hospital phase, when medical personnel and facilities are the primary components. 3) Post-hospital phase, where education, rehabilitation, and TSC/SCIs outpatient clinics are the primary components. 8
Providing an appropriate care to the patients with TSC/SCIs in the prehospital setting includes timely transport to care facilities and a well-equipped and trained EMS (emergency service) 9 team. Timely care in SCI patients has been shown to be important for improving neurologic recovery and outcomes,10,11 and it is advised that, if possible, surgical decompression be completed in less than 24 h,12,13 or even just 8 h. 14 This illustrates the need to early and efficient transport of patients with SCI to the proper care facilities.
The quality of the post hospital care can be evaluated in several aspects. The functional independency of the patients, the burden on their caregivers, the access to different required facilities, the prevalence of secondary complications, and the quality of life (QoL) of the patients. These areas can be measured and define the quality of the provided care for these patients, as in our recent work 12 indicators of post-hospital QoC for patients with TSC/SCIs were introduced. 8 The in-hospital QoC has been reported in a previous work (Sadeghi-Naini et al unpublished data, February 2023) and herein, the purpose of the current study is to evaluate the QoC of TSC/SCIs patients from the NSCI-IR dataset to understand the current pre- and post-hospital QoC of these individuals in Iran.
Materials and Methods
Study Population and Data Collection
The NSCIR-IR dataset is a prospective patient registry, which includes the pre-hospital and in-hospital QoC indicators, as well as demographic data of patients with TSC/SCIs. Previously, through a comprehensive review, 7 we retrieved and classified the indicators of QoC in TSC/SCIs and the accepted indicators formed the content of the QoCAT. The QoCAT design is described in a previous manuscript. 8
The pre-hospital QoCAT included three main questions (Figure 1). On the basis of these questions, in a retrospective manner, the pre-hospital information of patients (n = 3550) from October 2015 to November 2021 were collected. All 3500 registered patients with TSC/SCI were included in the prehospital phase and demographic data, transport time to the first care facility and transport time to final care facility, percentage of cervical collar, and backboard usage was extracted. The time to first care facility was defined as the time period between injury and the time that patients were admitted in triage in the first care facility where the patients were stabilized. Time to the final care facility was defined as the time between injury and the time that patients were admitted in the triage of the referral hospital where the definitive care (surgical or non-surgical) was provided. The percentage of cervical collar usage and backboard was calculated in the patients with cervical trauma (n = 912) and all 3550 patients, respectively. Pre-hospital and post-hospital quality of care indicators. Three pre-hospital and 12 post-hospital indicators of quality of care in patients with traumatic spinal cord/column injuries are represented.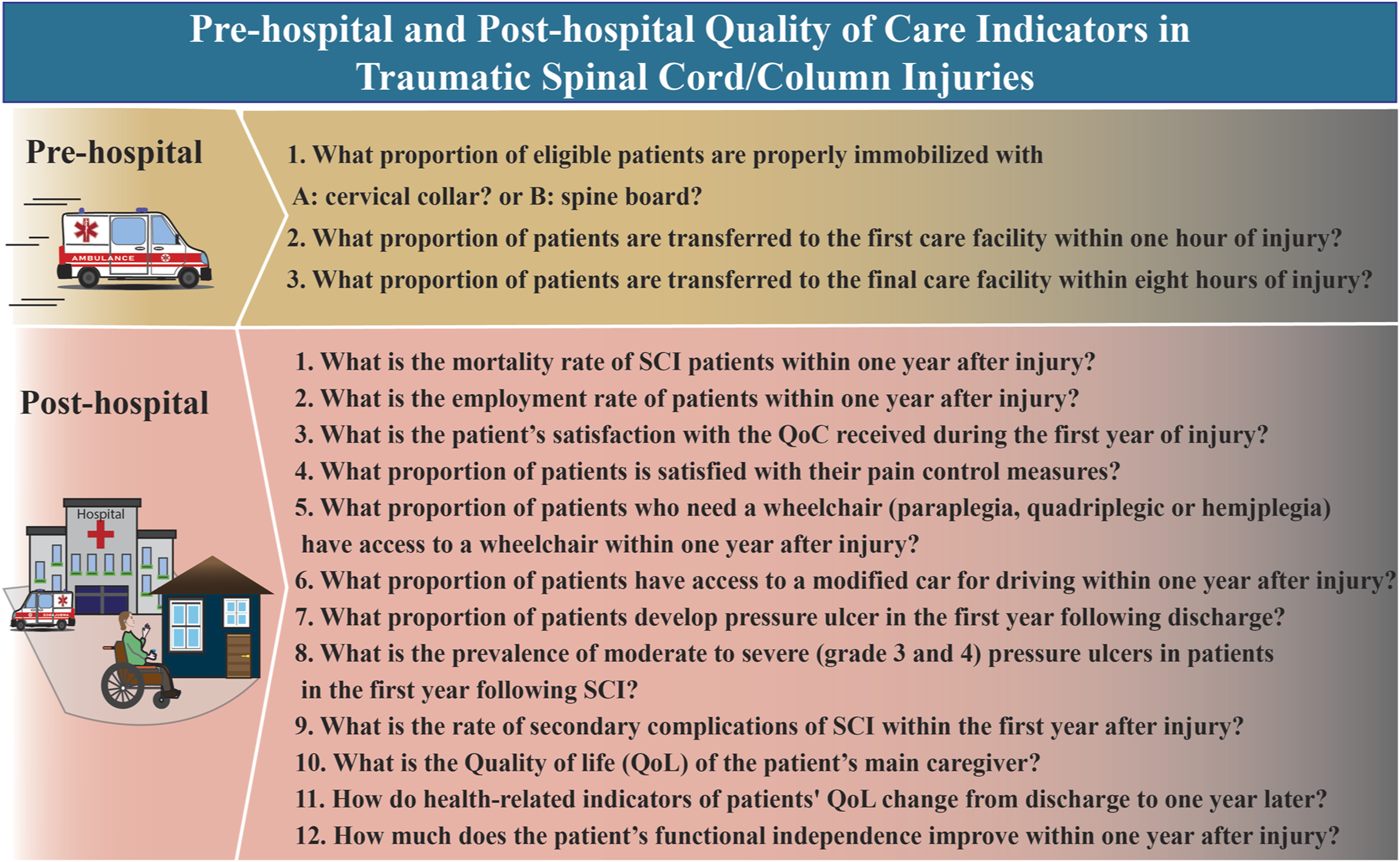
To assess the post-hospital QoC in SCI patients a retrospective telephone interview was implemented as a new phase to NSCIR-IR. A retrospective cohort was performed on a sample size of 160 SCI patients. Twenty patients died within one year after injury therefore, we evaluated the remaining indicators (except for mortality rate) in the 140 remaining patients. Inclusion criteria for post-hospital phase were: Any patient who (i) was identified by the NSCIR-IR registry centers from October 2015 to November 2021 with greater than one year from their injury (ii) was diagnosed with SCI, and (iii) was discharged from the hospital, the patients were excluded if: they were unable to answer telephone follow-up in situations such as vegetative state, they were not available, they did not give consent to participate in the study. Registered patients with SCI were sorted based on the date of injury and three physicians, familiar with the goals of the study and registry system, contacted patients in order from the most recent to the oldest date of injuries. If the patients were unavailable, a second attempt was done and if unavailable again, physicians contacted the next patient of the list.
In the telephone follow-up, 12 indicators of post-hospital QoC based on QoCAT were investigated (Figure 1) as follows: The mortality rate was measured by dividing the number of deaths within the first year after discharge to the total number of 160 patients (asked from the caregiver). The employment rate was defined as the percentage of patients who were employed within one year after their injury. The proportion of patients with access to wheelchairs or modified cars within 1 year after their injury was measured. The proportion of patients who reported having secondary complications (chronic pain, pressure ulcer (PU), urinary tract infection (UTI), spasticity, or autonomic dysreflexia) within the first year after their injury to the total 140 patients were measured. The incidence of pressure ulcer after injury and after discharge was separately reported. All adverse events and complications were explained to the patients for transparency of care. Unfortunately, the grade of the pressure ulcer (PU) were unable to be assessed through telephone follow-up. Therefore PU grade was excluded from the current study.
The pre-and post-hospital phase was conducted under the approval of the Sina Trauma and Surgery Research Center Review Board (Approval number: 98-3-93-45593). Regarding the prehospital data, the registry information was utilized, patients provided verbal informed consent to be involved in the study. Further, verbal informed consent was provided for the post-hospital phase.
To assess patients’ satisfaction of their quality of received care and pain control, at the time of interview, the Visual Analogue Scale (VAS) was used as a metric. Caregiver’s Burden Scale (CBS, Persian translated version)15,16 was obtained from the patient’s main to evaluate the burden of responsibility of the patient’s main caregiver at the time of interview where higher scores indicate greater burden on the caregiver. 17 The quality of life of the patients with SCI at the time of interview was measured by the Quality of Life 23-items questionnaire (SCIQL-23) (Persian translated version).18,19 Spinal Cord Independence Measure III questionnaire (Persian translated version) (P-SCIM-III) 20 was used to evaluate the functional independency of patients with SCI at the time of interview (Supplementary). Regarding the SCIM III, the patients were grouped based on their time from injury to the interview in three groups, and these groups were compared. In group A, B, and C the time between injury and the interview was <24 months, 24-48 months, and >48 months respectively.
Statistical Analyses
Quantitative variables were described as mean and standard deviation or median and interquartile range. Categorical variables were described as percentage and frequencies. The SCIM-III scores in the three time groups were compared using one-way ANOVA test. The level of significance was considered at P < .05. Data were analyzed using SPSS V19 software.
Results
Pre-Hospital Quality of Care
Pre-Hospital Quality of Care Indicators in Registered Patients in NSCIR-IR.
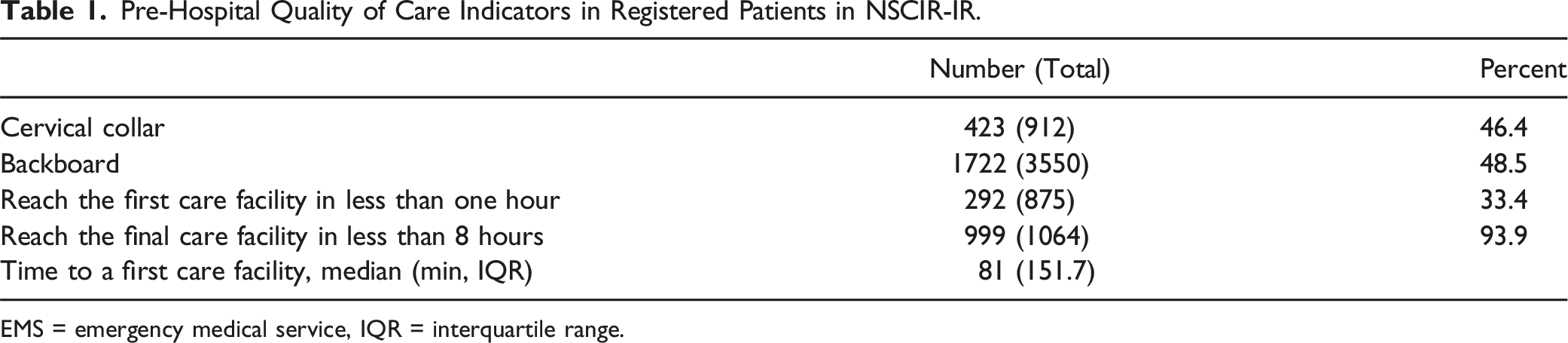
EMS = emergency medical service, IQR = interquartile range.
Post-Hospital Quality of Care
Post Hospital Indicators of Quality of Care in Patients With SCI. a
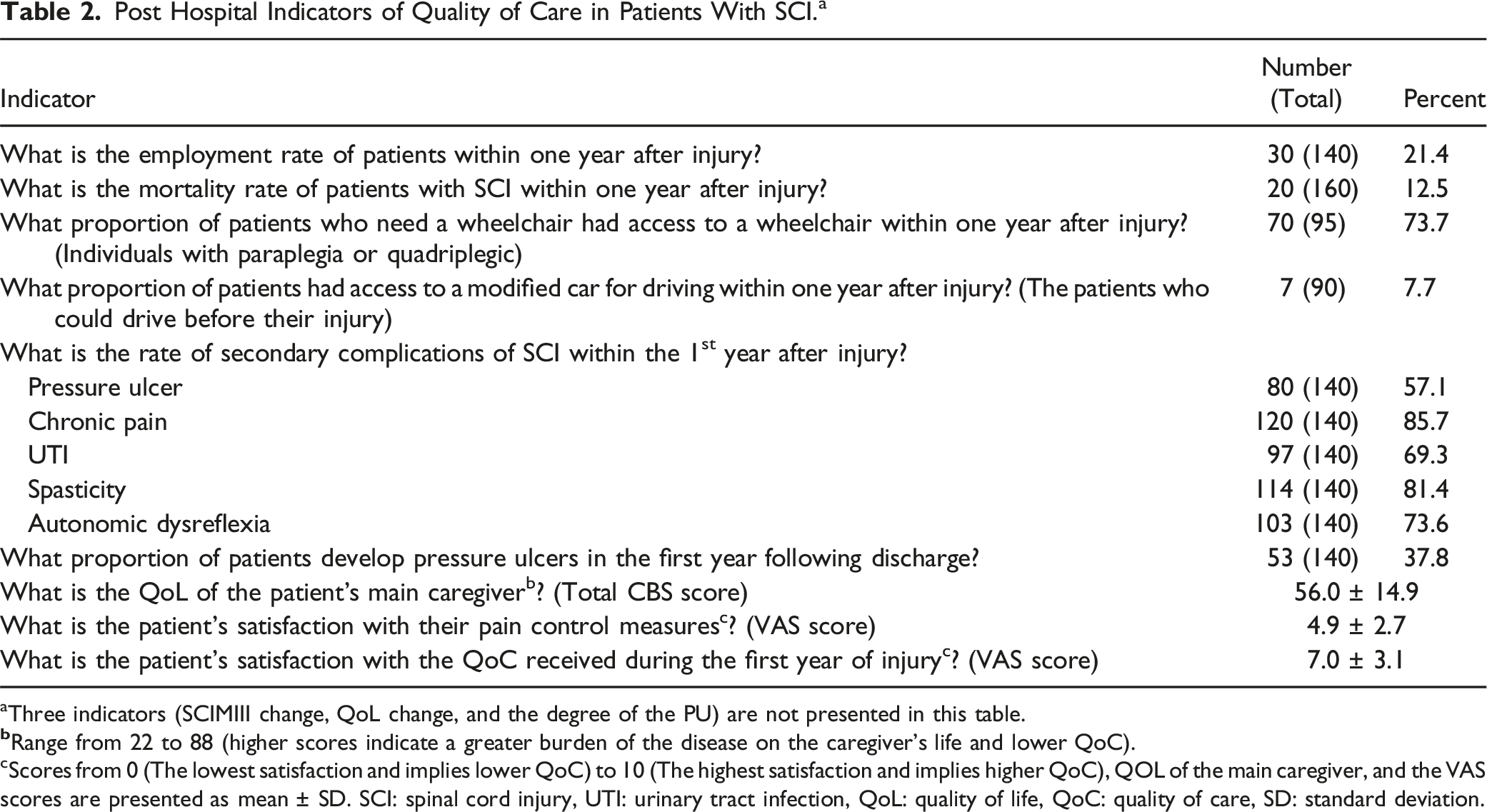
aThree indicators (SCIMIII change, QoL change, and the degree of the PU) are not presented in this table.
cScores from 0 (The lowest satisfaction and implies lower QoC) to 10 (The highest satisfaction and implies higher QoC), QOL of the main caregiver, and the VAS scores are presented as mean ± SD. SCI: spinal cord injury, UTI: urinary tract infection, QoL: quality of life, QoC: quality of care, SD: standard deviation.
In the first year following SCI, chronic pain was the most prevalent morbidity from the injury; a considerable percentage of 57.1% of the patients reported PU after injury and 37.8% after discharge. The frequency of the factors related to developing PU in the post hospital care revealed that 86.1% of the patients had intimate caregiver, 75.3% had access to an appropriate mattress, 70.7% were educated about the care of PU, and 18.4% had a university educational degree (Supplementary, Table S1).
The percentage of patients with SCI employed after injury was 21.4%. The wheelchair access among patients who required a wheelchair (paraplegic, hemiplegic or tetraplegic), was 73.7% (70 of 95), of whom 95.8% had mechanical, whereas only 4.2% had access to an electric wheelchair and among the patients with tetraparesis or tetraplegia only 6.6% used electrical wheelchair. Only 7.7% (7/90) of patients who could drive prior to the injury had access to a modified vehicle for their disability. According to the VAS scoring system, the mean satisfaction score for pain control and for post-hospital QoC was reported to be 4.9 ± 2.7 and 7.0 ± 3.1 respectively (Table 2).
Spinal Cord Independence Measure III Scores in Patients With SCI Based on the Duration Time From the Injury.
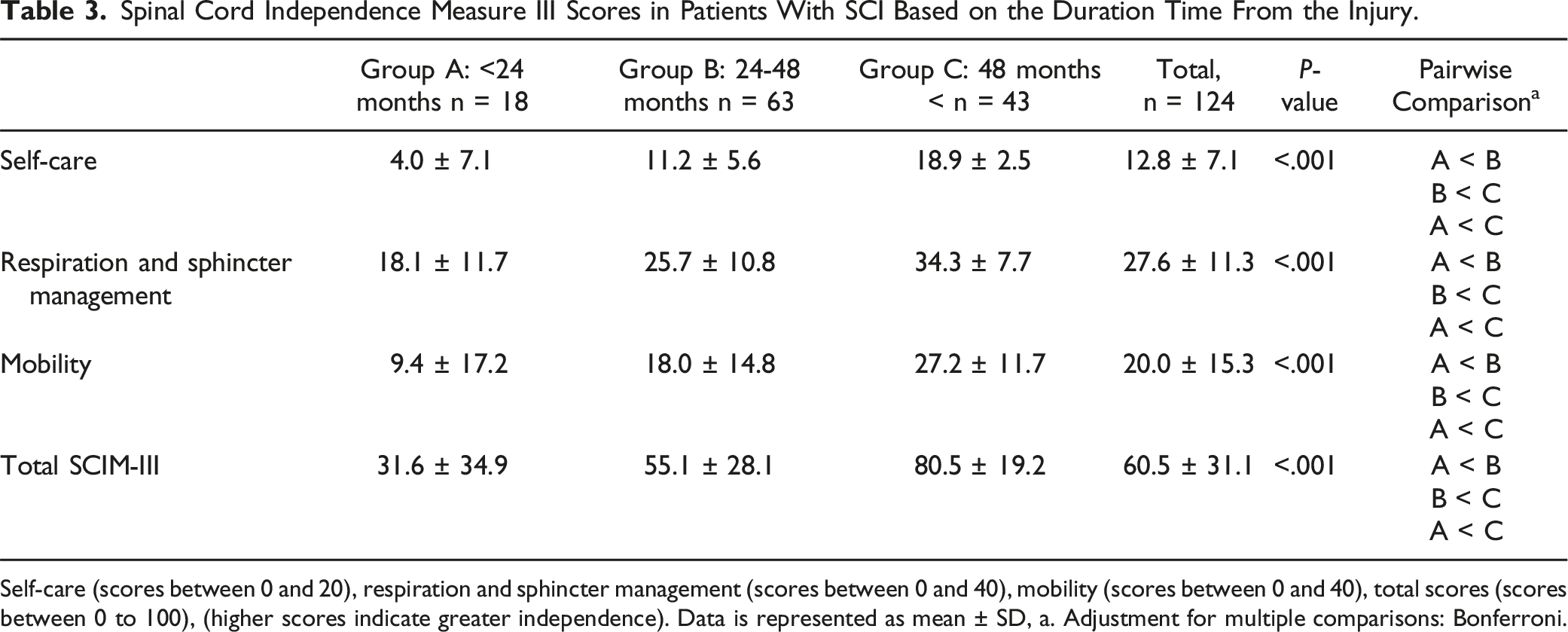
Self-care (scores between 0 and 20), respiration and sphincter management (scores between 0 and 40), mobility (scores between 0 and 40), total scores (scores between 0 to 100), (higher scores indicate greater independence). Data is represented as mean ± SD, a. Adjustment for multiple comparisons: Bonferroni.
Quality of Life 23-Items Questionnaire Scores in the Patients With SCI.
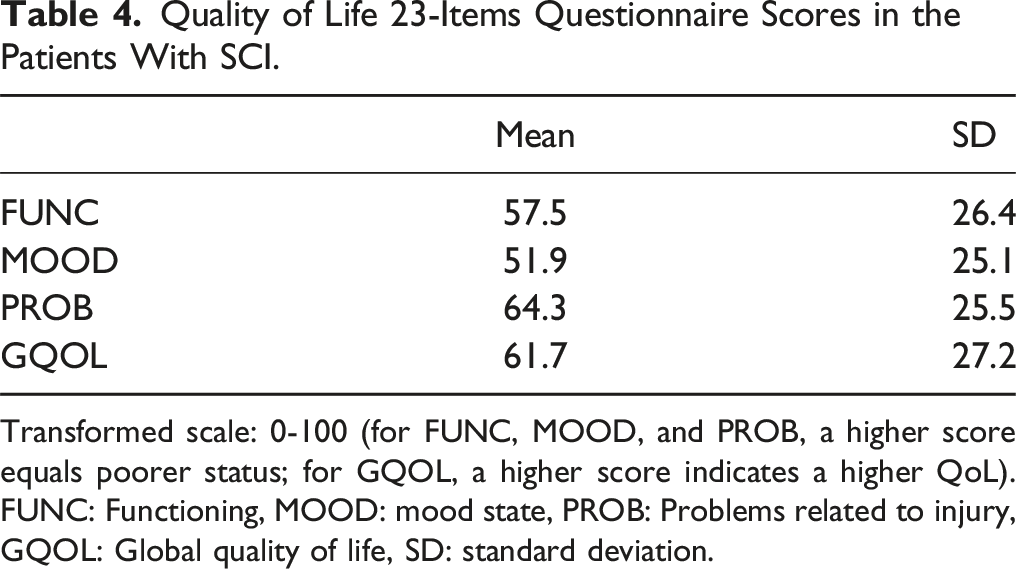
Transformed scale: 0-100 (for FUNC, MOOD, and PROB, a higher score equals poorer status; for GQOL, a higher score indicates a higher QoL). FUNC: Functioning, MOOD: mood state, PROB: Problems related to injury, GQOL: Global quality of life, SD: standard deviation.
In terms of CBS, 98 caregivers participated in the research study. This group consisted of: 27.8% parents, the major caregiver, followed by the children, siblings, and spouses in 10.3%, 22.7%, and 36.1%, respectively. The mean ± SD scores of the CBS domains was as follows: Total CBS score (56.0 ± 14.9), General strain (20.8 ± 7.06), Isolation (7.7 ± 3.09), Disappointment (13.9 ± 4.18), and Emotional involvement (5.9 ± 2.54), Environment (7.56 ± 2.62).
Discussion
In the current study, a comprehensive assessment tool in the NSCIR-IR to evaluate pre-hospital and post-hospital QoC in patients with TSC/SCIs in Iran was implemented. The results revealed a low QoC in the pre-hospital and post-hospital settings for TSC/SCIs patients per the NSCIR-IR registry.
Pre-Hospital Quality of Care
Cervical Collar and Spinal Backboard Immobilization
Pre-hospital care goal for TSC/SCI patients is to stabilize neurological function and reduce potential neurological impairments. In 2014, a descriptive study from Iran of 5614 trauma patients noted very low utilization of cervical immobilization (5.1%). 21 This study notes a higher use of cervical and spinal immobilization, however, there is a considerable opportunity to improve care such to reach 100% despite contrasting views on the advantages of utilizing spinal collars.22,23 Present guidelines recommend that the pre-hospital care of trauma patients with TSC/SCIs must have adequate spinal cord immobilization.9,24 Unfortunately, data from low and middle income countries revealed that most first responder programs providing TSC/SCIs care operated without cervical collar access 25 and few instructed members on full spinal immobilization.26–29
Despite the guidelines’ recommendations, inadequate training or experience of EMS personnel may result loss opportunities of improved care. 30 Another reason for not using immobilization equipment is that emergency ambulances, particularly in low-income countries, lack the necessary equipment25,31 whereas these are more available in high-income nations. In a level 1 trauma German study, patients with TSCI were immobilized in 78.3% of cases with cervical collars and in 69.9% of cases with spine boards or vacuum mattresses. 32 In order to prevent SCI, Bernhard et al 33 suggested meticulous immobilization for TSCI patients.
Transport Time to Hospital
In this study, 33.4% of TSC/SCIs patients reached first care facility in less than one hour after the injury with the median time of 81 m. The results are similar to a previous Iranian retrospective study on TSCI patients, the median time between injury and first hospital arrival was one hour (IQR: 1-2). 27 In a 2017 German study, it was demonstrated that the mean ± SD time from accident to the emergency ward was 61.3 ± 28.7 minutes, which is shorter than the 150 minutes in this study. 32 Contrarily, Yusuf et al., 34 noted an estimated mean arrival time of 45.0 ± 85.4 h in Nigeria. Delay in transport of trauma patients to the hospital has been shown to be associated with increasing mortality29,35 and secondary morbidity.34,36 It is vital to understand that for patients with TSCI timely arrival to hospital and surgery is extremely important to their outcome. 37 Middleton et al 36 estimated a 1.7 times higher odds of delay in transport (≥24 h) for patients injured in a major city compared to other areas in New South Wales. However, the odds of delay in transport (≥24 h) of patients with SCI was much higher in developing countries.29,38,39 Additionally, Middleton et al 36 suggested that patients with SCI with multiple trauma were more likely to experience delays in reaching a trauma center compared to those with isolated SCI. Furthermore, referral bias, inability to pay for EMS services owing to a lack of insurance, insufficient public infrastructure, and inadequate credibility of first responders may further influence delays in transporting patients with TSCI.29,34,38
Despite the low proportion of the patients reaching the first care facility in less than one hour, fortunately 93.9% of the patients in the present study reached the final care facility in less than 8 h after injury. Several studies demonstrated that early surgery in less than 8 h could significantly improve the neurological outcomes for TSC/SCI patients.40–42 Therefore NSCIR-IR patients appears to have access to an in-time care in final care facility. However, considering the acute nature of TSC/SCI the time to first care facility still required to be improved.
Post-Hospital Quality of Care
Secondary Complications in Patients With SCI
Several secondary problems may occur as a result of a traumatic SCI. In two studies,43,44 the estimated prevalence of autonomic dysreflexia was 43% and 1.4%, respectively. Other documented consequences include UTI, pulmonary difficulties, and gastrointestinal issues.43–46 According to this study, the most frequent secondary adverse event after a traumatic SCI was resulting chronic pain. This finding was similar to Madasa et al. 45 However, this study did not classify the patients according to the level of their injuries. Overall, compared to other research, the rate of secondary morbidities from traumatic in this study was rather high and may be due to obtaining the information from the patient’s perspective.47,48
For instance, 57.1% of the patients reported PU in the first year after discharge, which is noticeably high when compared to the global pooled prevalence of PU in a recent meta-analysis, (57.1% vs 32.4%). 49 To further understand the reason of this high rate of PU, we evaluated the factors related to PU and considerably the majority of the patients had access to appropriate mattress (75.3%), had intimate caregiver (86.1%), and were educated the ways to prevent and treat PU (70.7%). This indicated that whether the patients and their caregivers did not apply the required care appropriately, it could be due to low educational level of the patients as it is shown that only 18.4% had university degree or the in-hospital care was poor resulting in PU that took months after discharge to be resolved.
The first-year incidence of PU in this study was 37.8% with SCI. In a systematic review by Chen et al the pooled incidence rate of PU in 29 studies around the word was reported to be 23% and in Asian and developing countries was 16% and 27% respectively which indicated that higher incidence of PU in the current study in a period of one year, in addition the included studies in the work be Chen et al 50 did not restrict their incidence period to just one year and included different time periods. Collectively, the high prevalence of PU in the short period of less than a year after discharge illustrates the QoC in these selected eight academic centers of Iran needs overview. Public health policymakers need to be informed such that policy changes can be initiated. Further, education to the care providers in hospitals, individuals with SCI, and their caregivers should be improved.
With improved preventive care provided to SCI patients there is the possibility to decrease PU develops, therefore, the grade of the PU has been proposed as an indicator of QoC. However, this study was not able to assess this indicator by telephone follow-up. 49 Early transfer of patients with TSCI to specialized centers of care, may reduce the mortality rate and possibility associated secondary morbidity issues through improved education and protocols. 51
The Mortality Rate in Patients With SCI
The mortality rate of traumatic SCI patients is 2 to 5 times higher than those without SCI, with the risk of mortality is greatest in the first year after injury. 52 This study noted a 12.5% mortality rate in the first year following SCI. Only seven of these deaths (5% first-year mortality rate after discharge in 140 SCI patients) occurred after discharge indicating an appropriate QoC regarding this indicator. According to other studies, the first-year survival following TSCI ranged between 79% and 100% depending on the level of injury and other risk factors. 53 Thietje et al 54 noted that the level of neurologic injury was associated with mortality. Paraplegic patients had higher life expectancies than those with tetraplegia. Furthermore, it was shown that tetraplegic patients had a significant rate of suicide-induced death. Notably, the majority of causes of death are curable, including septicemia, cardiovascular disease, and respiratory illness, among others.45,54,55 Therefore, patients with SCI should be given adequate rehabilitative care such to prolong their lives.
Access to Wheelchair and Modified Car for Patients With SCI
Financial and equipment support for patients with SCI is crucial to their QoC. These results revealed that 73.7% of patients required a wheelchair for mobility, and only 6.6% of tetraparetic patients were using electrical wheelchairs. Furthermore, only 7.7% of patients that were driving prior to their injury had access to modified cars. Despite the necessity of these devices, 26.3% of the patients had no access to a wheelchair, whereas the majority of patients with SCI in a research conducted in the Netherlands had multiple wheelchairs. 56 The lack of access to customized cars and the relatively low availability of wheelchair devices in Iran as compared to other e nations can be best explained by the patients’ economic situation. In addition to raising the financial QoC indices, providing this equipment to patients with SCI may also increase their level of satisfaction with their care, which is also crucial to their QoC. 57
Satisfaction of Pain and Quality of Care in Patients With SCI
This study noted a relatively average patient satisfaction for pain control, however, it was noted that the observed patients’ satisfaction with the QoC they received was greater. In a case-control study involving 27 patients with 11 controls, Budh et al., 58 reported a comprehensive pain management program that reduced levels of anxiety and depression and was likely to improve quality of sleep in patients with SCI. Unfortunately, SCI-related disabilities can result in reduced patient satisfaction with care. Consequently, establishing programs to improve their functional independence in the post-injury follow-up can ensure patients’ ability to work as well as benefit their overall QoC. 59
Spinal Cord Independence Measure III in Patients with SCI
Regarding SCIM-III scores at the periods post-injury, a significant increase in the total SCIM-III score and subscales was seen in all the patients, indicating a substantial improvement in functional independence. The functional independence of the patients with SCI increases over time with neurologic improvement. Möller et al 59 also reported a stable SCIM-III score over time in a long-term follow-up. Despite our findings, Majamäki et al 60 reported that time from injury is negatively associated with SCIM-III scores. However, the periods in their study were much greater. This study categorized patients based on time from injury in < 2-year, 2-4-year, and > 4-year, although, it is recommended to evaluate the SCIM-III in 72 h after discharge and then at regular follow-ups. RHSCIR Community Follow-up Questionnaire also has a SCIM Self-Report at one, two, and 5 years after injury, 61 but due to the COVID-19 pandemic we could not evaluate the SCIM-III at discharge. However, similar to our findings, Ackerman et al 62 reported a significant increase in TSCI within the first year after injury. Concerning the QoC, this significant improvement in SCIM-III scores implies that these patients had adequate QoC. Furthermore, functional independence may directly or indirectly affect the patient’s ability to return to work after an SCI event. 63
The Employment Rate in SCI Patients
In this study, 21.4% of SCI patient were employed at one year after injury. Although this figure was lower than in three other studies (21.4 vs 47.0%, 29.5%, and 31.0%, respectively),63–65 it was greater than the employment percentage reported by Kurtaran et al 66 (14.6%). Murphy et al., 67 evaluated several characteristics to predict the likelihood of employment for patients with TSCI. They reported that the three most influential predictors of employment were the Functional Independence Measure (FIM) score at discharge, high-skill pre-injury employment, and perceived community integration (SCIM score at discharge). According to James S. Krause, 68 it takes an average of 4.8 years from the time a SCI first manifests to obtain a job following an injury, and 6.3 years to find a full-time job. Furthermore, a North American study revealed racial disparities in SCI victims' job patterns. These disparities can significantly widen the gap between a SCI event and job prospects. 69 The employment rate of just about 21.4% after a year, indicates that the care system, social policymakers, and the laws and the executive coordination for people with SCI needed to be reconsidered in Iran.
Quality of Life in Patients With SCI
Comparing the SCIQL-23 scores of this study to Jain et al noted higher scores (poor QoL) in the FUNC, MOOD, and PROB domains and lower scores in GQOL (poor QoL). However Jain et al 70 categorized the patient scores on associated factors like age and level of injury, yet they demonstrated results indicative of improved QoL in each category. Both of these studies examined SCI patients with a post-SCI period exceeding one year. The varying economic conditions of the countries may account for these disparities, and the level of injury of the patients may be different and have had an impact on the QoL of patients with SCI.
In a 2017 study in Iran, the QoL of patients with SCI, 71 SCIQL-23 scores noted better QoL compared to our findings. However, the fact that they did not assess only TSCIs, nor determined the length of time between injury and interview; these two factors we believe significantly influenced their results. Additionally, the high PROB and FUNC scores in our study suggest that the cord injury in patients was more severe. Collectively the low QoL in SCI in this study indicates low post-hospital QoC in patients with SCI registered in NSCIR-IR.
Caregiver Burden Scale in Patients With SCI
Even though the total mean CBS score in this study was greater than in previous studies (56.04 vs 51.5, 26.2, 2.2, and 2.7, respectively),16,72–74 this study noted that compared to isolation and emotional involvement, general strain, disappointment, and environment scores were relatively higher and consistent with previous research.16,73,75,76 A low CBS was noted in domain 4 emotional involvement, which was also the case in three other studies.72,74,76 These results demonstrate that even though the majority of caregivers for people with SCI experienced greater general strain, disappointment, or environmental impact, they frequently had emotional reassurance and did not feel isolated. Simpson and Jones 73 demonstrated in caregivers of patients with traumatic brain injury or SCI that caregivers with greater resilience had a mean CBS score of 46.7 which was lower than those with a lower resilience (54.4). Overall, the evidence indicates that caregivers of patients with tetraplegic SCI (9.93 vs 8.98) and substantial complications (9.54 vs 8.98) have higher mean CBS scores. 75 Collectively, the caregiver burden in our study indicates a high burden that needed to be improved by precisely further evaluations.
Interventions and Suggestions to Improve Pre-and Post-Hospital QoC for TSC/SCIs Patinets
The quality of care in individuals with TSC/SCIs is affected by numerous factors in both the short-term and long-term outcomes. To enhance pre-hospital QoC, education of EMS personnel, emergency department staff, and also public education, especially in developing countries, are crucial. Equipment for EMS can be provided by financial support from related organizations and charities.77,78 The present study aim is to clarify existing gaps and deficiencies in pre-hospital settings and cause further changes in policy makings.
The establishment of SCI care units in referral hospitals with trained personnel is recommended to better manage adverse events in early rehabilitation and educate patients and their caregivers. Regular educational programs on appropriate care, psychological support, and rehabilitation programs consisting of regular examinations can enhance the satisfaction of provided care and quality of life in individuals with SCI. These programs could be held online or on-site in rehabilitation centers. 79 In addition. Financial support of these individuals is impotent due to their expensive care facilities and disability which cause difficulties in finding a job. 63 This could be obtained through changes in policy-making in health insurance to cover as much as possible the rehabilitation services like physiotherapy, wheelchairs, drugs, hygiene items, wavy mattresses and other facilities for these individuals.
Limitations
Several limitations are apparent in the current study. Most of our population had more than 1-year from their injury and due to COVID-19 pandemic the baseline data and follow up were incomplete. All questions in the QoCAT for the post-hospital evaluation were not implemented as it was not possible to accurately evaluate the grade of the pressure ulcer by telephone follow-up, the QoL and Spinal Cord Independence Measure-III (SCIM-III) scores of the patients at discharge. For the several indicators, patients were asked how their state was in the first year as they remembered: access to wheelchair and modified car, rate of secondary complications, employment rate, and development PU and for the following indicators we asked the state at the time of the interview: CBS score, QoL of the patients, patients’ satisfaction of the pain control and QoC received, and the SCMI-III score.
The post-hospital phase on a sample size of 160 patients were evaluated. The selected 160 patients from the registry data list did not cause biases in our findings since level of injury, level of education, and the distribution of the province where the patients live, were not statistically different between these patients and the remaining registered patients with SCI.
Regarding the SCIM-III score, we could not exclude patients with anatomical deformities without examination which may affect the results. To eliminate any biases, we requested that the caregivers answer the questions outside of the patients’ presence; however, we could not guarantee this for the telephone follow-up. Of note, because unavailability of the caregivers, and poor cooperation of some patients in answering the questionnaires of CBS, SCIQL-23, and SCIM-III, the total number of patients were different for these questionnaires. To more effectively utilize the QoCAT for assessing the QoC in patients with SCI, it should be administered at discharge and one year following the injury. On-site examination or clinical documentation of individuals with SCIs can promote a more accurate evaluation of the post-hospital care of these individuals.
Conclusion
This study noted that spinal immobilization in the form of cervical collars and spine backboards were poorly implemented. In addition, the transfer time to the hospital from the scene of injury needs further improvement. Although the first-year mortality rate was low and the SCIM-III scores were acceptable, post-hospital QoC indicators can be improved due to a number of factors, including the high incidence of various secondary complications, especially pressure ulcers, low employment rate, and limited access to wheelchairs and modified vehicles. These findings highlight the need for setting appropriate strategies to improve pre- and post-hospital care in patients with TSC/SCIs in NSCIR-IR.
Supplemental Material
Supplemental Material - Pre-Hospital and Post-Hospital Quality of Care in Traumatic Spinal Column and Cord Injuries in Iran
Supplemental Material for Pre-Hospital and Post-Hospital Quality of Care in Traumatic Spinal Column and Cord Injuries in Iran by Arman Zeinaddini-Meymand, Vali Baigi, Mehdi Mousavi-Nasab, Sina Shool, Mohsen Sadeghi-Naini, Zahra Azadmanjir, Seyed Behnam Jazayeri, Samuel Berchi Kankam, Mohammad Dashtkoohi, Aidin Shakeri, Esmail Fakharian, Leila Kouchakinejad-Eramsadati, Habibollah Pirnejad, Homayoun Sadeghi-Bazargani, Laleh Bagheri, Yasaman Pourandish, Malihe Amiri, Ahmad Pour-Rashidi, James Harrop, and Vafa Rahimi-Movaghar in Global Spine Journal
Ethical Statement
Ethical Approval
The Ethics Committee of National Institute for Medical Research Development of Islamic Republic of Iran (NIMAD) approved the study. The reference number is IR-NIMAD-REC-1397.519. In addition, the Ethics Committee of Tehran University of Medical Sciences approved the study [Reference number: IR. TUMS.VCR.REC.1398.332] and the NSCIR-IR with approval ID of IR. TUMS.MEDICINE.REC.1401.133.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The research reported in this publication was supported by Elite Researcher Grant Committee under award number [972056] from the National Institutes for Medical Research Development (NIMAD), Tehran, Iran. Also, Sina Trauma and Surgery Research Center, Tehran University of Medical Sciences [grant number: 98-3-93-45593], and Tehran University of Medical Sciences [Grant number: 98-01-38-41516] funded this work. We acknowledge the Deputy of Research and Technology, Ministry of Health and Medical Education of Iran’s support for the NSCIR-IR.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.