
Abstract
Study Design
Systematic review.
Objective
The aim of this study was to conduct a systematic overview of the pathogenesis and the treatment options of combined odontoid and atlas fractures in geriatric patients.
Methods
This review is based on articles retrieved by a systematic search in the PubMed and Web of Science databases for articles published until February 2021 dealing with combination fractures of C1 and C2 in geriatric patients.
Results
Altogether, 438 articles were retrieved from the literature search. A total of 430 articles were excluded. The remaining eight original articles were included in this systematic review depicting the topics pathogenesis, non-operative treatment, posterior approach, and anterior approach. The overall level of evidence of the studies is low.
Conclusion
Combined odontoid and atlas fractures in the geriatric population are commonly caused by simple falls and seem to be associated with atlanto-odontoid osteoarthritis. Non-operative treatment with a cervical orthosis is a feasible treatment option in the majority of patients with stable C2 fractures. In case of surgery posterior C1 and C 2 stabilization and anterior triple or quadruple screw fixation are possible techniques. Some patients may also deserve an occipito-cervical fusion. A possible treatment algorithm is proposed.
Introduction
Combined fractures of the atlas (C1) and axis (C2) can be seen in about 3% of cervical spine injuries. 1 They are caused by high-energy trauma in young patients with good bone quality and are associated with high incidence of neurological impairment.1,2 In contrast, combined injuries (CI) in geriatric patients are commonly seen after ground level falls and appear typically without neurologic deficits.3-5 Several studies dealing with this injury pattern included both young and elderly patients with a wide variety in treatment strategies being used.1,6 Treatment ranged from non-operative strategies to posterior approaches and various anterior surgical strategies.1,5-9 The purpose of this study was to systematically review the literature and to sum up the evidence for combined odontoid (C2) and atlas (C1) fractures with respect to pathogenesis and treatment strategies.
Methods
The literature search included articles dealing with geriatric patients (age > 65) suffering from odontoid process fractures in combination with fractures of C1.
A systematic search of the literature was performed by two of the authors (UJS, MP), including all articles until 02/13/2021. In each case, the two databases PubMed and Web of Science Core Collection were considered and searched. Since data collection had already been completed at the time of PROSPERO registration, this review could not be registered with PROSPERO. Using the PICO scheme,
10
the following review questions were defined: • What is the pathogenesis of these fractures? • What is the expected outcome in geriatric patients suffering from odontoid process fractures in combination with fractures of C1? • What are the treatment strategies of such fracture combinations?
The following search terms were used: (“Odontoid” OR “atlas” OR “axis” OR “upper cervical spine”) AND “fracture” AND (“geriatric” OR “elderly” AND “English [Language]” NOT (“case reports”[Publication Type] OR “comment”[Publication Type] OR “congress”[Publication Type] OR “review”[Publication Type]). All articles that were published during the years starting in 1990 were included.
Subsequently, all relevant original articles were analyzed based on their levels of evidence and their appropriate conclusions. The following topic areas were defined: • Pathogenesis • Non-operative treatment • Posterior approach • Anterior approach
Results (Spiegl, Krause, Keil, Perl)
Altogether, 438 abstracts were retrieved from the literature search (Figure 1). Of these, 408 articles were excluded based on abstract content. Most of the excluded studies were excluded because of the following reasons: no combination fractures, no geriatric patients included, solely review articles, or articles investigated other pathologies, respectively. One article was excluded based on the publication date.
6
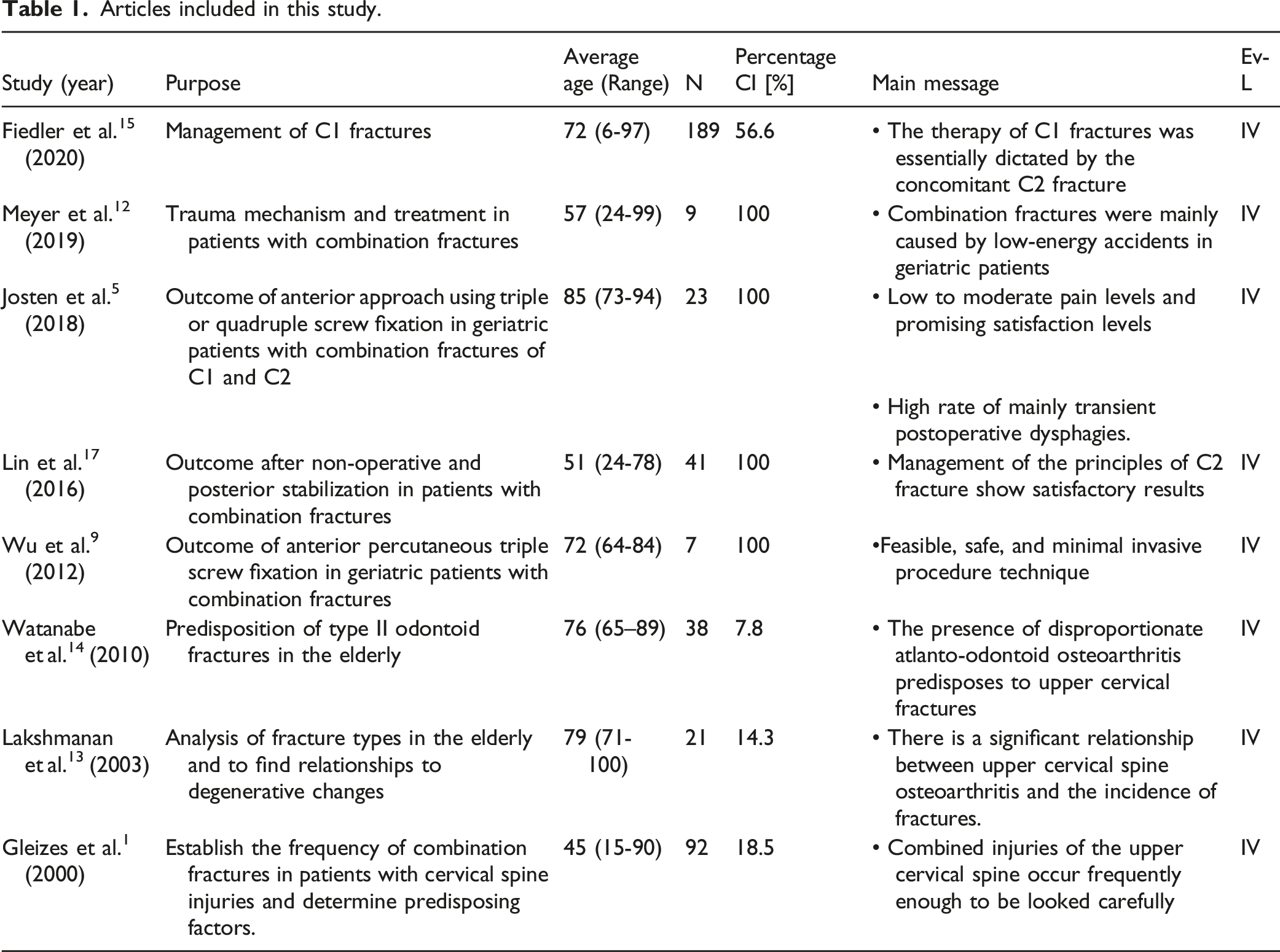
Altogether, 29 articles underwent complete workup. Of these, 21 articles were additionally excluded for the following reasons: not focusing specifically on acute combination fractures of the upper cervical spine, no sufficient number of geriatric patients included, or insufficiently describing the methods, respectively. Altogether, 429 articles were excluded (Figure 1). The 8 remaining original articles, which covered the period from 2000 to 2020, are summarized in Table 1. Levels of evidence were defined as described by Bassler and Antes.
11
Flow chart of the systematic literature review. Articles included in this study.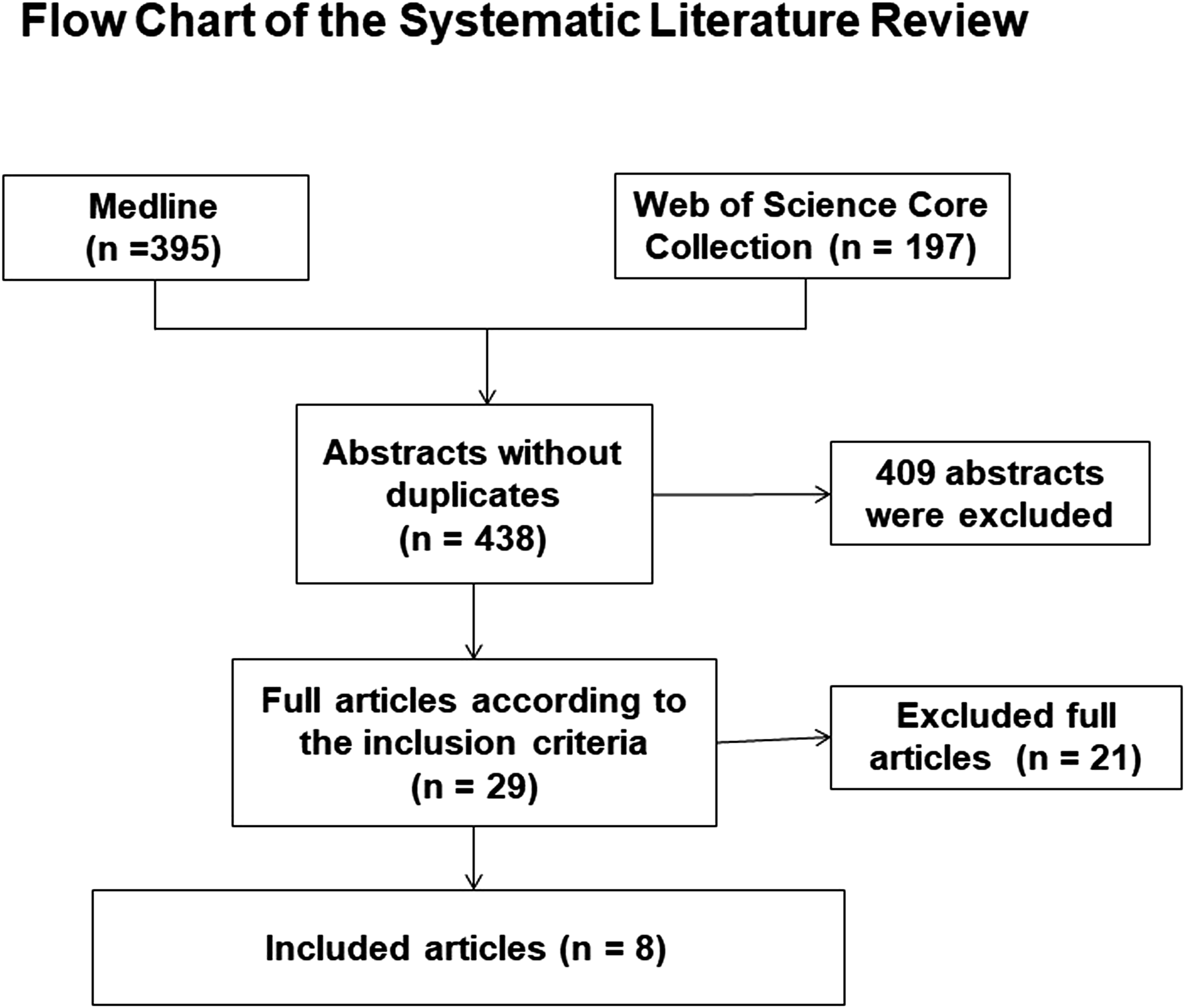
Pathogenesis
A total of 6 articles reported epidemiologic data or discussed fracture pathogenesis.1,5,12-15 The combination of a fracture of the first cervical vertebral body and the odontoid process is not uncommon and represents nearly 3% of cervical spine injuries.1,5,16 Normally, this injury complex is the result of low-energy trauma in older patients due to domestic plunges, as confirmed by the results of Meyer et al. 12 Fiedler et al 15 reported a rate of 56.6% of combined C2 fractures in geriatric patients suffering of a C1 fracture. In a cohort of 21 patients with an average age of 84.6 years, Josten et al 5 described low-energy trauma like simple falls as the predominant mechanism. Hereby, atlanto- odontoid osteoarthritis seems to be essential.5,13 In this context, Lakshmanan et al 13 demonstrated that the presence of a significant atlanto-odontoid osteoarthritis increases the risk of sustaining type II odontoid fracture. Watanabe et al 14 compared 17 patients with type II odontoid fractures with a cohort of 21 patients with other axis fractures showed that patients with osteoporosis and disproportionate degenerative changes between the atlanto-odontoid and lateral atlantoaxial joints were more likely to have a type II odontoid fracture than other axis fractures. Josten et al 5 proposed that the reduced C1/2 motion due to osteoarthritis causes a selective stress to the odontoid process just below C1 by sudden translational and rotational forces. The result is a type II odontoid fracture. In case of further bending or axial force, thus an additional fracture of C1 may occur.
Non-Operative Treatment
Most studies on combined C1/C2 fractures in geriatric patients included into this analysis focused on operative treatment. However, a total of 3 studies included patients that were treated non-operatively.1,15,17 When looking at these studies non-operative treatment consisted of cervical orthosis or Halo fixation. Fiedler et al 15 managed 37 (34.5 %) of the 107 patients with combined C1/C2 injuries by non-operative treatment. In the cohort of 31 combined upper cervical fractures reported by Gleizes et al., 1 58 % were treated non-operatively. Both studies did not present any outcome results after non-operative treatment. Lin et al 17 treated 3 patients with cervical collar and 19 patients with a halo fixator. They reported comparable improvement of the neck disability index (NDI) reduction after both surgical and non-surgical treatment after a mean of 19 months. The mean NDI was 10.7 ± 5.3 at the latest follow-up. The mean time until bony fusion was documented was 5.7 months after non-surgical treatment and 6.0 months after surgery. There was a total one non-union visible after non-operative treatment (4.5%). All other studies analyzed did not in particular report on non-operative treatment of combined C1/2 fractures.
Lin et al 17 included both geriatric and non-geriatric patients. Twenty-two of the included 41 patients were treated non-operatively. After an average of 19 months, the VAS pain score was 2.0 (0-4) and the neck disability index was 9.6 ± 4.5. A complication rate of 9.1% was reported.
Posterior Approach
None of the included studies specifically dealt with posterior approach in geriatric patients. One study included combined injuries only with a smaller proportion of geriatric patients with an average age of 50.9 (range 24-78). 17 Lin et al 17 analyzed 41 patients suffering from CI fractures. Nineteen were treated by a posterior approach, 17 analogue to Harms et al 18 and 2 using a posterior stabilization including the occiput. After an average follow-up of 19 months (range 12-45 months) the average pain level was 1.7 ± 1.2 after operative treatment. The NDI was 9.6 ± 4.5 and the complication rate was reported to be 15.8%.
Anterior Approach
A total of 2 studies included patients that were treated by an anterior approach only.5,9 Wu et al 9 included 7 geriatric patients with combined fractures. The average age was 74.4 years. An anterior triple screw fixation was performed in percutaneous technique including one screw in the odontoid process and a C1-2 transarticular screw on both sides. Average follow-up was 13 months and no complications were reported. Union was seen in all patients. Rotation was limited to 40° and two patients reported of pain while rotating the neck. Josten et al 5 included all patients ≥ 70 years with Anderson type II odontoid fracture with an accompanied C1 fracture. The average age of the 23 patients was 84.6 years. Atlanto-odontoid osteoarthritis was obvious in all cases. Anterior triple or quadraple screw fixation with one or two screws in the odontoid process and C1-2 transarticular screws on both sides was performed via an open technique in all patients. Transient dysphagia was noted in 26.1%, and revision was necessary in one patient. A follow-up after 1 year was possible for 78.3% of patients and revealed a mortality rate of 21.7%, and a mean pain level and satisfaction rate of 2.5 (± .9) and 7.3 (± .7), respectively. No non-unions were detected.
Discussion
Due to the heterogeneity of the data of the included studies, a narrative presentation of the results was chosen. The studies had a wide range of inclusion criteria, especially regarding the age of the included patients and the rate of combination injuries in the patient collective. General evidence level is low; all included studies were retrospective cohort studies or case series, so evidence level was IV in all studies.
The evaluated parameters in both the therapeutic and the diagnostic studies varied substantially. This accounts for description of symptoms, pre-operative evaluation of the clinical status and imaging assessment. All studies used computed tomography as main diagnostic tool. The description of the fracture pattern was mostly morphologic, only some authors used established classification systems like Gehweiler classification 19 for C1 fractures.5,15
Trauma mechanism was evaluated in several studies that did not report of outcome data.12,15 It was shown that around half of the accidents were ground level falls. This seems to be associated with moderate to severe atlanto-odontoid osteoarthritis.5,13 Generally, this is in line with other fractures in elderly people where a high proportion of fractures results from low-energy trauma. 20 This underlines the necessity of adequate diagnostics regardless of the trauma mechanism when symptoms are present or injury of the cervical spine is suspected.
No sufficient outcome data are presented in those studies reporting from non-operative treatment. Since the majority of the C1 fractures are stable 15 the C2 fracture morphology seems to have the highest impact on the decision between non-operative and operative treatment.
In accordance to the treatment recommendation of geriatric type II odontoid fractures, non-operative treatment is a valuable treatment strategy in very old patients (≥85 years) without signs of gross dislocations. A semi-rigid cervical orthosis for a minimum period of 6 weeks can be recommended. 21 Unfortunately, no further information about the influence of age particularly between old and very old patients on the frequency of occurrence and the outcomes are available. Thereby, the highest impact on the frequency of occurrence seems to the grade of degeneration of C1/2 and not the age of the patients. 13 In order to gain further evidence to this important unawareness, further research is desirable.
The described surgical procedures such as C1-2 internal fixator, transarticular screw fixation according to Magerl and occipito-cervical fusion via a posterior approach offer a greater stability in osteoporotic bone or with accompanying stiffening disease in comparison to the anterior technique with one/two screws. 21
Generally, there are recommendations preferring an initially posterior approach in patients or injuries with a high biomechanical instability, thus as geriatric patients with a stiffening disease (M. Bechterew or Forestier) or with highly unstable translational injuries. 22
As long as closed reduction is feasible, posterior stabilization as described by Magerl
23
or an anterior approach is possible. The Magerl technique is a less-invasive procedure to treat atlanto-axial traumatic instability, particularly when performed in a percutaneous way. The anterior approach for combined fractures of atlas and axis in geriatric patients was firstly described by Agrillo et al in 2006.
24
The triple/quadruple techniques consisting of one or two odontoid screws plus bilateral transarticular C1/2 screws has been reported in CI.5,9 Thereby, transient dysphagia is a common complication.
5
Josten et al
25
reported a significant reduced number of complications using a auadruple technique including odontoid screws in the treatment geriatric type II odontoid fractures. They argued that the increase stability might be particularly useful in this patient special patient population associated with relevant reduced screw hold. Posterior C1 and C2 fusions described by Harms
18
is the most predictable technique and is particularly indicated in displaced fractures. Lin et al
17
discussed the option for occipitocervical fusion critically as it restricts spinal motor function and should be an approach of last resort. In accordance to Lin et al the authors see the indication for an occipitocervical fusion in the following situations: 1. Congenital anomalies of the upper cervical spine, particularly of the vertebral artery anomalies 2. Comminuted C1 fractures (comminuted Gehweiler type III or IV fractures
19
) or widening of the C1 arch
Generally, the evidence level is low. However, a treatment recommendation for this common fracture combination might help to improve the quality of treatment and would be a start to improve the quality of treatment in the future. Based on the evidence and on the experience of the authors, a treatment algorithm for CI of C1 and C2 was generated and is presented in Figure 2: Therapeutic recommendation for combined C1 and C2 fractures. Prior decision making a sufficient diagnostic work-up is essential including a CT of the cervical spine. In order to detect instabilities extension and flexion views particularly under fluoroscopy can be performed by an experienced spine surgeon or radiologist. Additionally, an MRI can be helpful to detect concomitant ligament injuries, spinal canal compromises and to differ between old and acute fractures. Non-operative treatment seems to be particularly indicated in patients with high biological age characterized by low activity levels rather than high chronological age. Posterior percutaneous and anterior techniques are good treatment alternatives in patients with unstable fractures that can be reduced anatomically by closed reduction techniques. Open C1/2 stabilizations or fusions in accordance to Harms are possible patients with dislocated fractures with the option to include the occiput if necessary.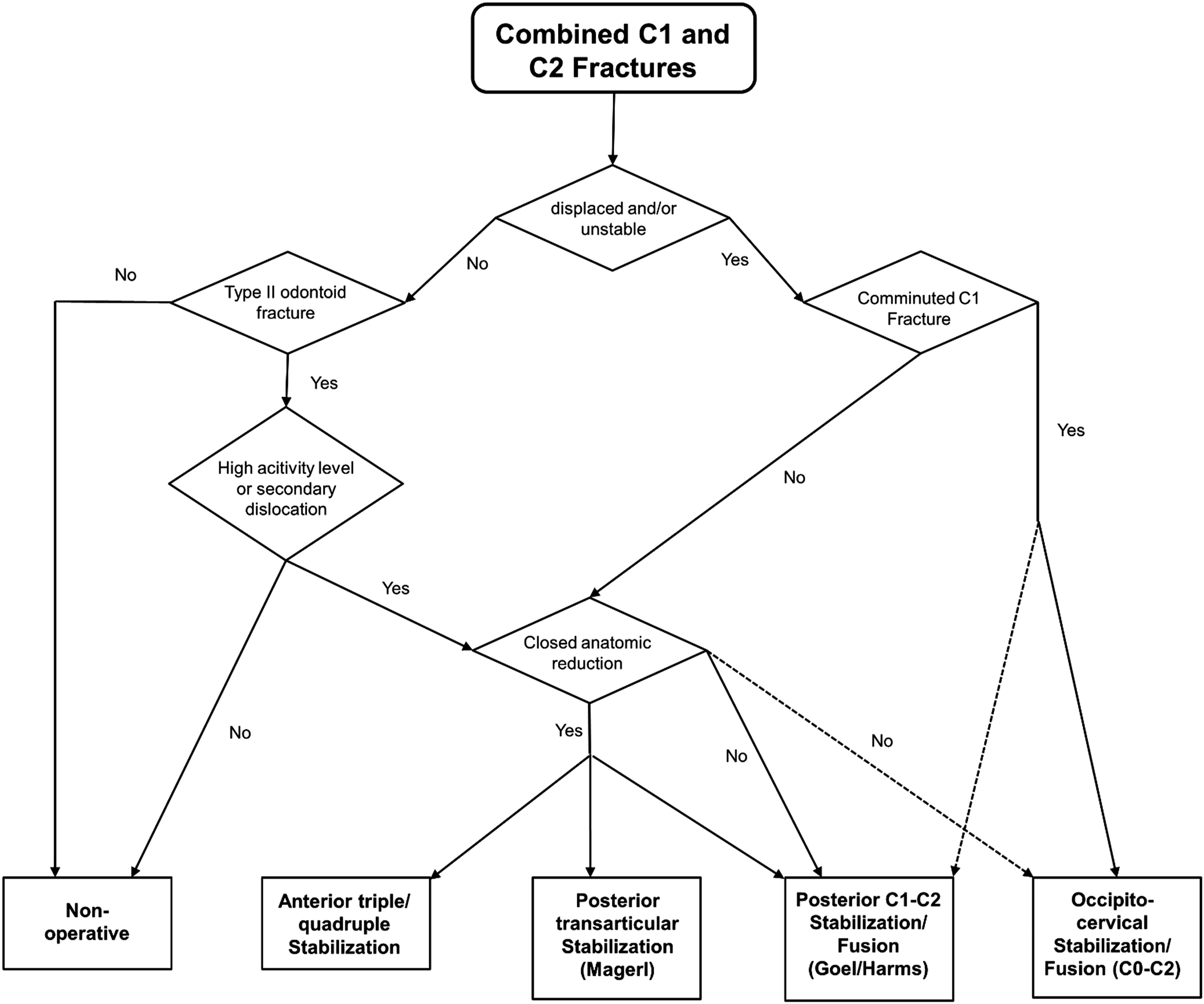
Limitations
As described above, the main limitation of this review are the heterogeneous data available regarding this topic. Thus, a systematic review was not possible and the analysis can be descriptive only. Hence, the aim that evidence based recommendations regarding diagnosis and treatment concepts of combined C1/C2 could be condensed from the available studies was not achievable. Even though this fracture entity seems to be more common this has not yet been investigated sufficiently. Additionally, some surgical techniques such as the percutaneous posterior stabilization by Magerl and the anterior triple/quadruple techniques may be less familiar to several spine surgeon. This might be associated with inferior results. Generally, new research is necessary in order to improve the quality of treatment. Particularly, studies investigating the outcome of surgical and nonsurgical treatment in geriatric patients with combined injuries of C1 and C2 are warranted.
Conclusion and Recommendation
Combined odontoid and atlas fractures in the geriatric population are commonly caused by simple falls and seem to be associated with atlanto-odontoid osteoarthritis. Non-operative treatment with a cervical orthosis is a viable treatment option in the majority of patients with stable C2 fractures. Both, posterior C1 and C2 fusion, posterior Magerl’s stabilization and anterior triple or quadruple screw fixation can be used. Posterior transpedicular C1 and C2 fusion is indicated in highly unstable fractures and in fractures in which closed reduction is not feasible. Occipitocervical fusion can be a necessary alternative in patients with comminuted C1 fractures, high instability or relevant bone loss. Moreover, the decision towards an operative treatment may also be chosen by failure of non-operative treatment. Persistent pain in spite of adequate pain management and/or increasing dislocation in 2 or more subsequent CT scans may warrant operative management of combined C1 – C2 fractures. Furthermore, failure of non-operative treatment such as progredient skin lesions due long term immobilization on the one side and high comorbidity on the other side may also direct treatment towards operative or non-operative, respectively.
Footnotes
Author Contributions
Spiegl: Advisory Board: European Journal of Trauma and Emergency Surgery
Schnake: Consultant: Medtronic, Swiss Medical Concepts; Honorarium: AO Spine International
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was organized and financially supported by Deutsche Gesellschaft für Orthopädie und Unfallchirurgie e.V. (DGOU).