
Abstract
Study Design
Cross-sectional, international survey.
Objectives
To examine current international practices as well as knowledge, adoption, and barriers to guideline implementation for acute spinal cord injury (SCI) management.
Methods
A survey was distributed to members of AO Spine. The questionnaire was structured to obtain demographic data and preferred acute SCI practices surrounding steroid use, hemodynamic management, and timing of surgical decompression.
Results
593 members completed the survey including orthopaedic surgeons (54.3%), neurosurgeons (35.6%), and traumatologists (8.4%). Most (61.2%) respondents were from low and middle-income countries (LMICs). 53.6% of physicians used steroids for the treatment of acute SCIs. Respondents from LMICs were more likely to administer steroids than HICs (178 vs. 78; P < .001). 331 respondents (81.5%) answered that patients would receive mean arterial pressure (MAP) targeted treatment. In LMICs, SCI patients were less likely to be provided with MAP-targeted treatment (76.9%) as compared to HICs (89%; P < .05). The majority of respondents (87.8%) reported that patients would benefit from early decompression. Despite overwhelming evidence and surgeons’ responses that would offer early surgery, 62.4% of respondents stated they encounter logistical barriers in their institutions. This was particularly evident in LMICs, where 57.9% of respondents indicated that early intervention was unlikely to be accomplished, while only 21.1% of respondents from HICs stated the same (P < .001).
Conclusion
This survey highlights challenges in the implementation of standardized global practices in the management of acute SCI. Future research efforts will need to refine SCI guidelines and address barriers to guideline implementation.
Keywords
Introduction
The instant in which a traumatic spinal cord injury (SCI) occurs has far-reaching physical, social and financial consequences for both patients and their families. Despite decades of progress, effective neuroregenerative therapies capable of restoring neurologic and functional recovery in patients with SCI are lacking.
And yet, the field of SCI research has generated many preclinical studies elucidating key mechanisms underpinning the pathobiology of the disease. 1 This knowledge of secondary injury pathobiology resulted in the development and testing of neuroprotective management strategies for patients with acute spinal cord injuries (SCIs). 2 Careful analysis of this clinical research to improve SCI care has been adopted into recommendations that include the 2013 AANS/CNS and the 2017 AO Spine guidelines on SCI management.3,4 However, despite the need to integrate knowledge generated by research into clear guidelines, there remains an inherent tension between incomplete certainty regarding the use of steroids, optimal hemodynamic management, the timing of surgical decompression, and optimizing acute SCI care in real-world circumstances.
Three important acute SCI controversies are i) the type, dose, and duration of steroid administration, ii) the optimal hemodynamic target blood pressures, the duration and mode of blood pressure management, and iii) the most effective timing of surgical decompression. The continuing uncertainty affects the extent of guideline implementation and is further accentuated in an increasingly heterogeneous SCI patient population, with some patients seemingly more suitable for certain therapeutic strategies than others.
The objective of this survey was to examine knowledge, adoption, and challenges in the implementation of standardized practice around these three key areas of SCI management. We sought to examine opinions and current international practices of spine care professionals regarding the acute administration of steroids, hemodynamic management, and timing of surgical decompression in acute SCI.
Methods
In collaboration with the AO Spine SCI Knowledge Forum, an English-language 38-item survey (Supplementary Material) was designed to examine the current practices of spine care professionals around the three key aspects of acute SCI management stated above. The survey questions were selected by consensus-based agreement to evaluate potential controversy impacting guideline implementation for acute SCI management. An e-mail request to participate in the survey was distributed to all members of AO Spine on October 1st, 2021. At the time of this survey, >6500 individuals were members of AO Spine with professional backgrounds in spine surgery, orthopaedic surgery and neurosurgery, including academic and private practice professionals, as well as related researchers. The link to this survey was available for 30 days, with one reminder sent out during this period. REDCap™ was used as the web-based platform.
For statistical analyses, the responses to each question were tabulated with the corresponding percentage for each response. Missing values were excluded in the tabulations. Categorization of countries based on the level of income was defined by the gross national income (GNI) per capita (query WorldBank as of Nov 1st 2021). Hypothesis testing was done with a chi-squared test using an alpha value of .05. Statistical analyses were performed using Stata version 16.1.
Results
Demographics of Respondents
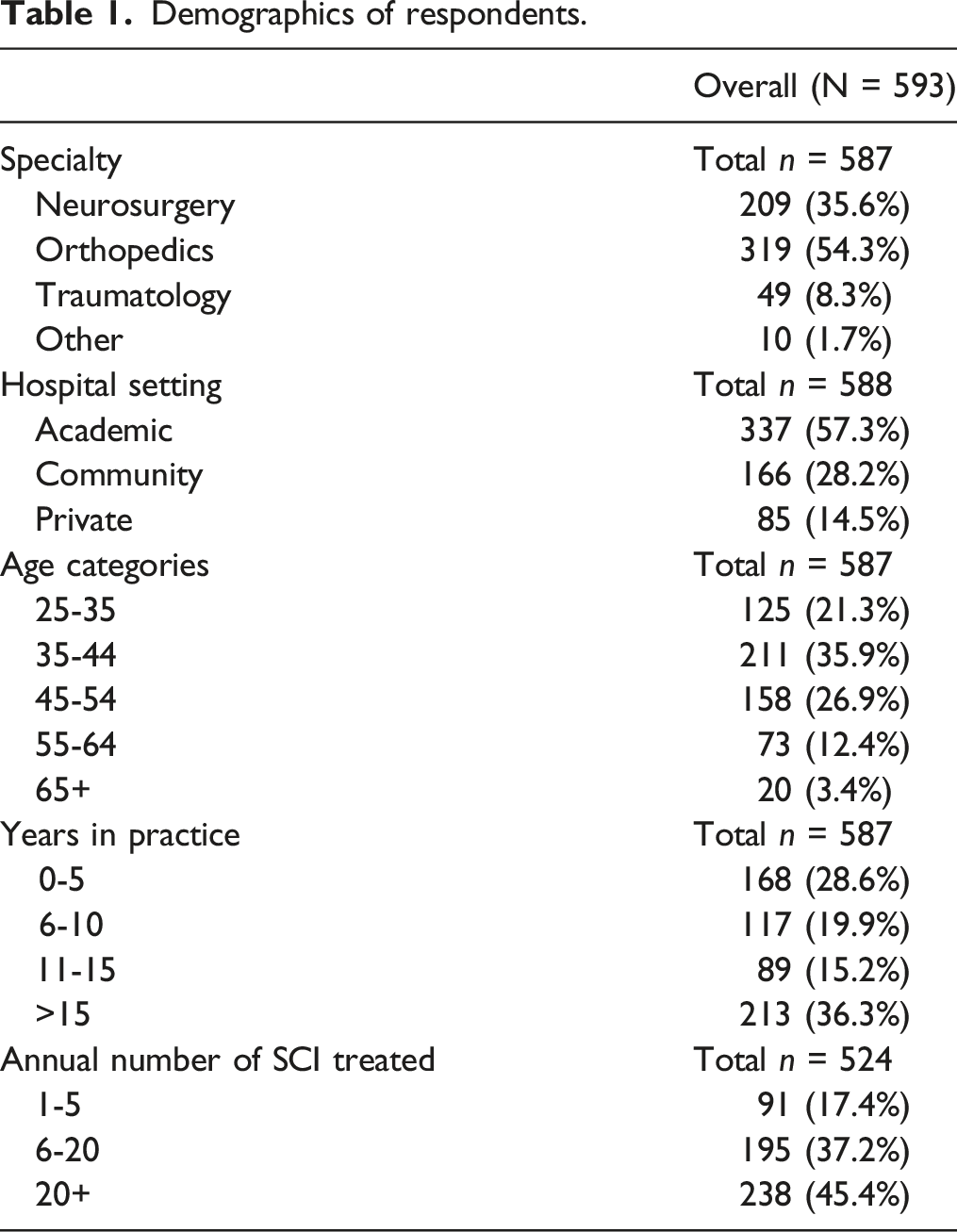
Demographics of respondents.
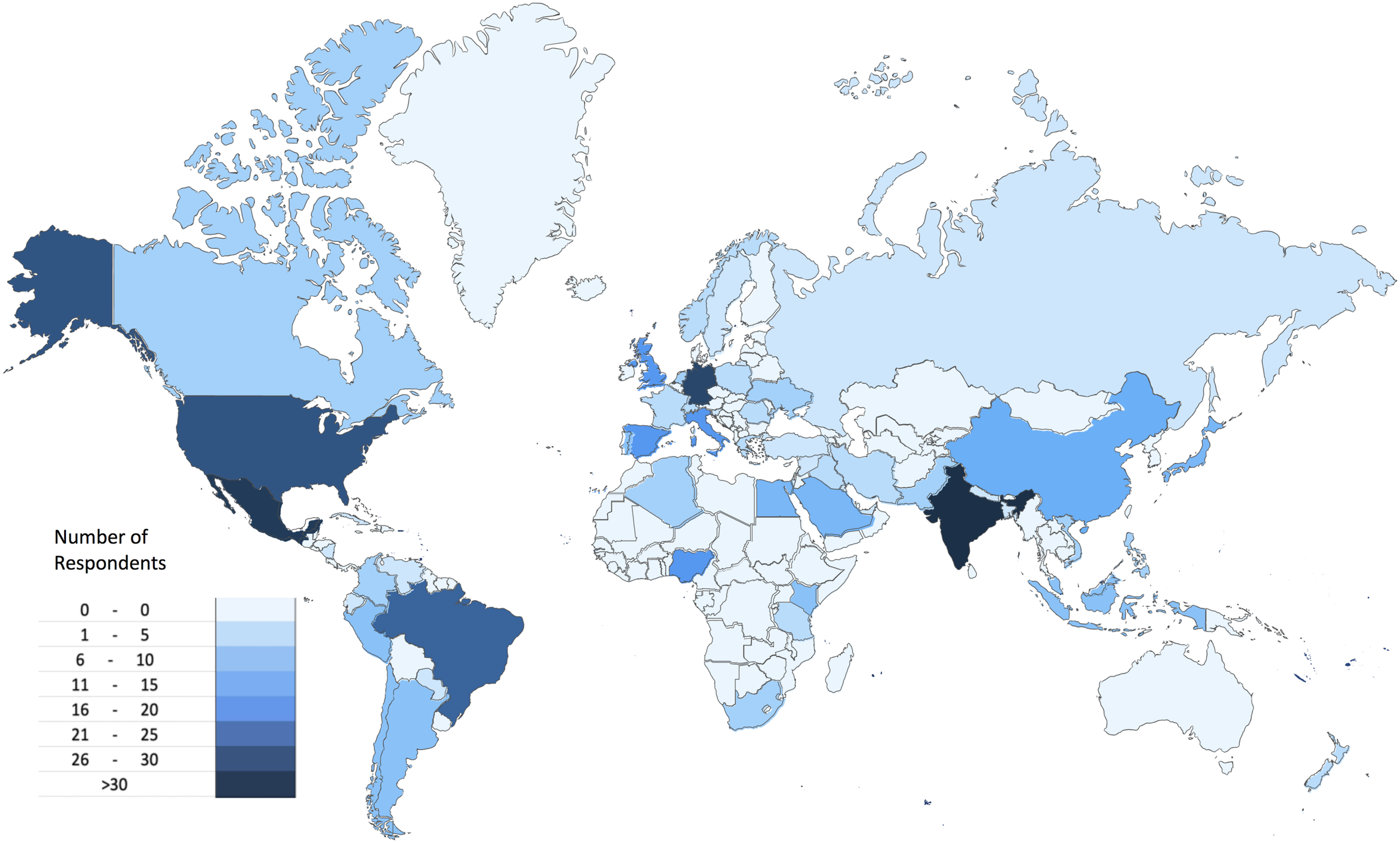
Heat map showing the geographic distribution of the respondents (n = 593).
Regarding institutional affiliation, 57.3% of participants indicated that they were practicing in a university affiliated hospital (n = 337), while 28.2% were affiliated with a community hospital (n = 166) and 14.5% with a private practice (n = 85). There were 45.4% (n = 238) of respondents working at high-volume institutions (>20 SCIs treated per year), while 37.2% (n = 195) worked at middle-volume institutions (6-20 SCIs per year), and 17.4% (n = 91) at low-volume institutions (1-5 SCIs per year).
Management with Steroids
Summary of responses related to steroid administration.
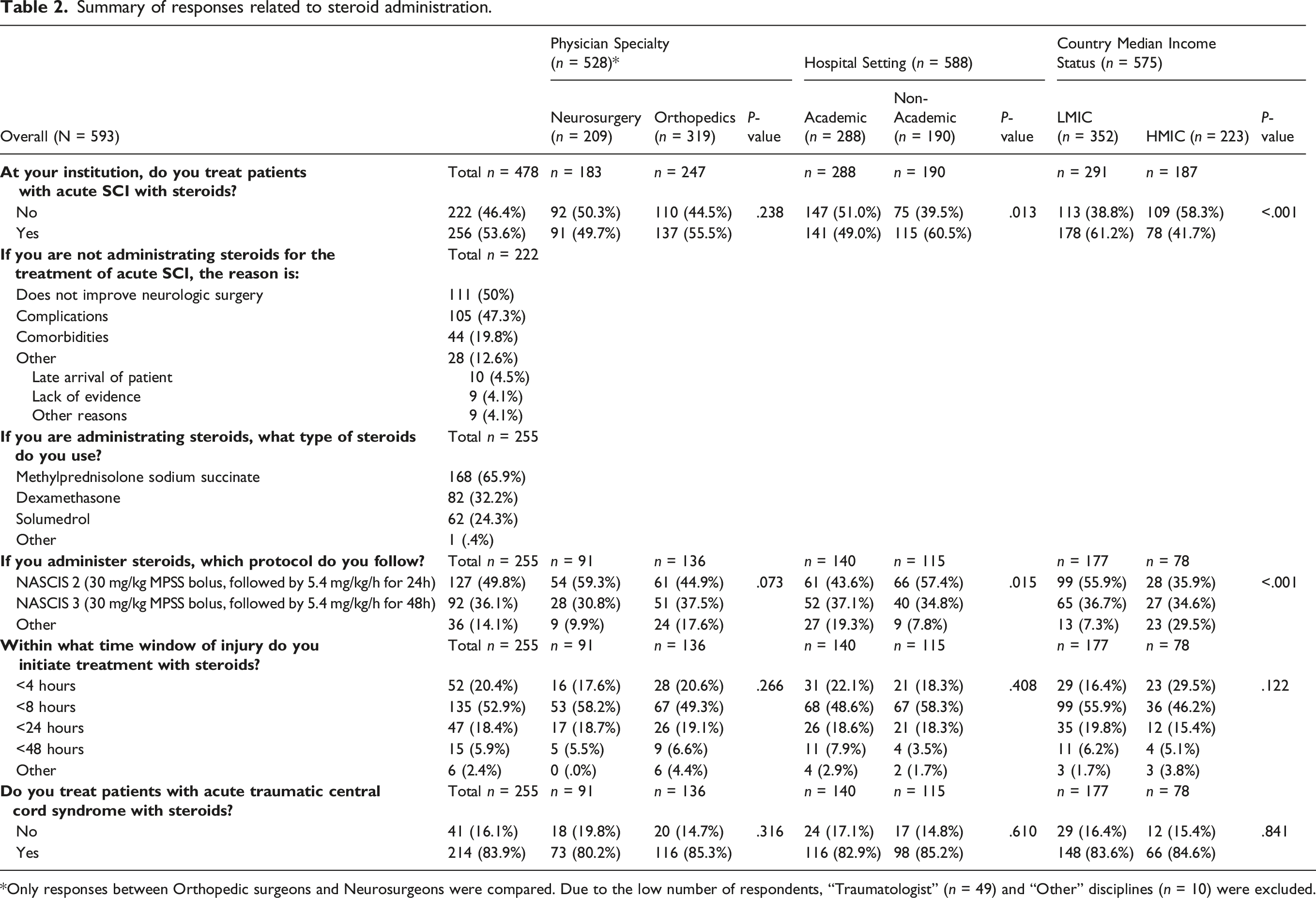
Only responses between Orthopedic surgeons and Neurosurgeons were compared. Due to the low number of respondents, “Traumatologist” (n = 49) and “Other” disciplines (n = 10) were excluded.
In terms of therapeutic protocol, the National Acute Spinal Cord Injury Study II (NASCIS II) treatment regimen (30 mg per kg bodyweight of MPSS as a bolus, followed by 5.4 mg per kg per hour for 24h), where treatment would be initiated within 8h of SCI, was the favored protocol used to administer steroids (49.8%; n = 127), followed by the NASCIS III protocol, which used the same dosage, however, for a duration of 48 hours if treatment was initiated within 3-8 hours of injury (36.1%, n = 92). As such, the majority of respondents indicated that they would initiate steroid treatment within 4 (20.4%; n = 52) and 8 hours of injury (52.9%; n = 135), while only 18.4% (n = 47) and 5.9% (n = 15) stated they would initiate treatment within 24 and 48 h of injury, respectively.
Interestingly, AIS A patients were less likely to receive steroids (72.6%; n = 185) than AIS B (82.7%; n = 211) and AIS C patients (76.5%; n = 195) (Figure 2A). Only 50.9% would administer steroids to patients with AIS grade D SCIs (n = 130). A clear majority of respondents who administer steroids to SCI patients would choose to treat cervical (96.1%; n = 245) and thoracic SCIs (87.4%; n = 223), while only 47.8% would administer steroids to lumbosacral SCIs (n = 122) (Figure 2B). Finally, most of the respondents who support the use of steroids (83.9%; n = 214) would consider administering steroids to patients with acute central cord syndromes. A) Bar plot showing the responses for steroid administration by American Spinal Injury Association (ASIA) Impairment Scale (AIS) grade (Y-axis represents raw numbers). B) Bar plot showing the responses for steroid administration by level of injury (Y-axis represents raw numbers).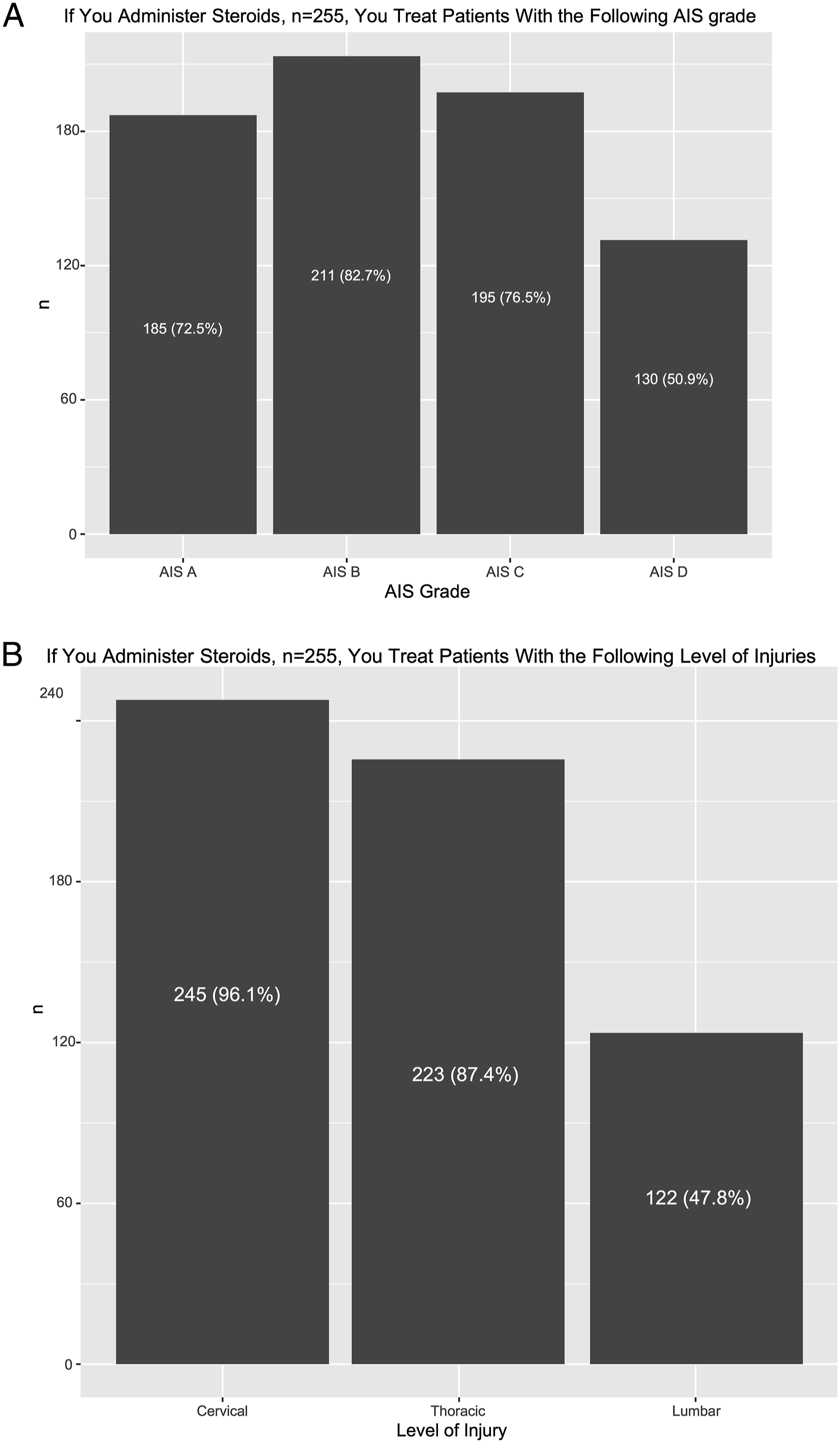
Hemodynamic Management
Summary of responses related to hemodynamic management.
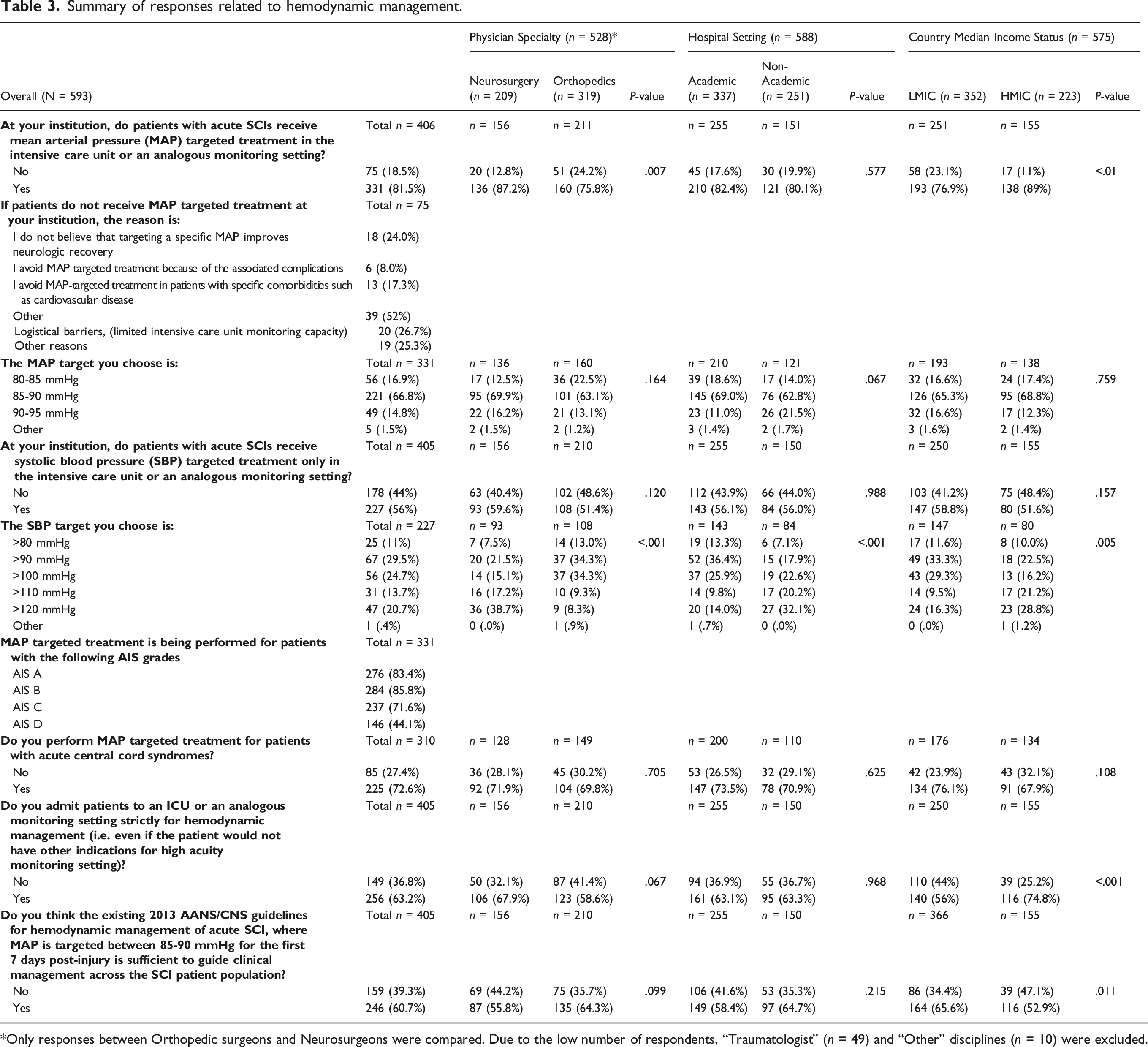
Only responses between Orthopedic surgeons and Neurosurgeons were compared. Due to the low number of respondents, “Traumatologist” (n = 49) and “Other” disciplines (n = 10) were excluded.
The most commonly chosen MAP target was 85-90 mmHg (66.8%; n = 221), which reflects the 2013 AANS/CNS guideline recommendations. And yet, there was ambiguity across the respondents as to whether the 2013 AANS/CNS guidelines would be sufficient to guide hemodynamic management. As such, 60.7% of respondents (n = 246) stated that the guideline recommendations would be sufficient to guide clinical management, whereas 39.3% (n = 159) did not. 56% (n = 227) would consider systolic blood pressure (SBP) targeted hemodynamic management with the chosen targets displayed in Table 3.
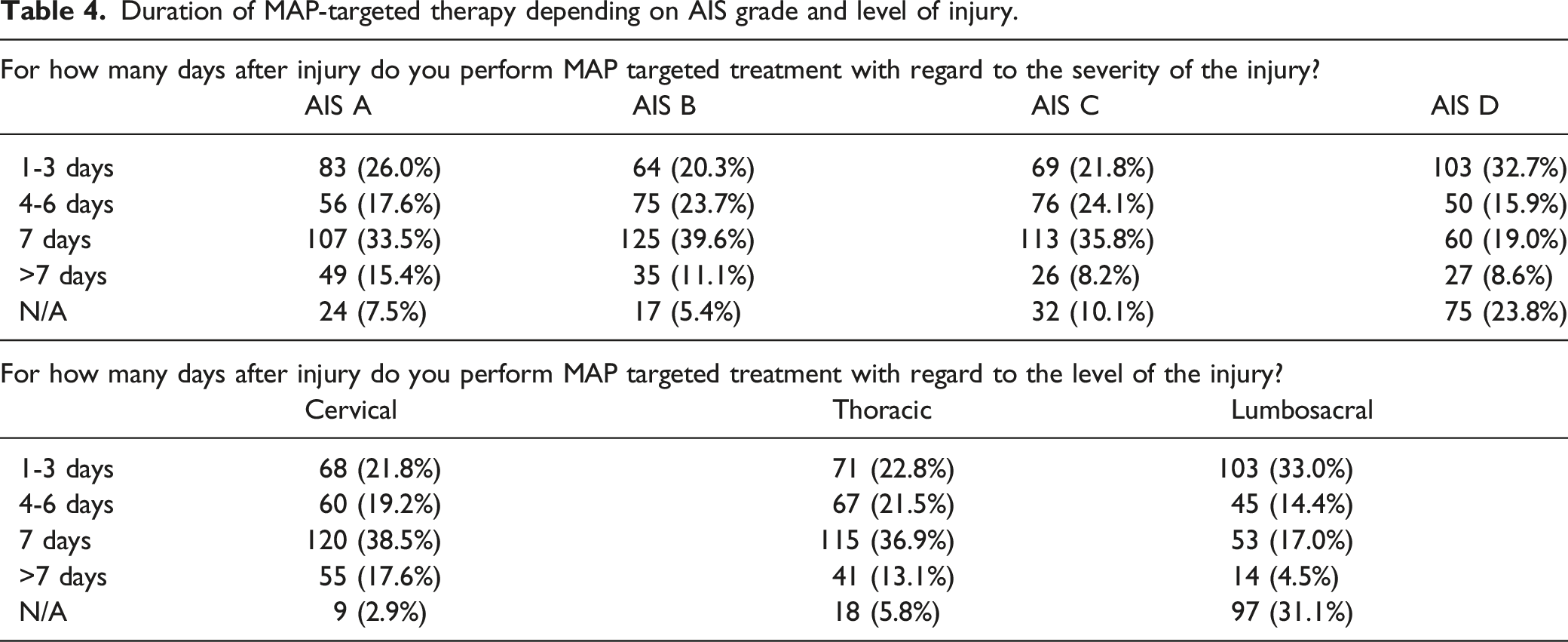
Duration of MAP-targeted therapy depending on AIS grade and level of injury.
Timing of Surgical Decompression
Summary of responses related to timing of surgical decompression.
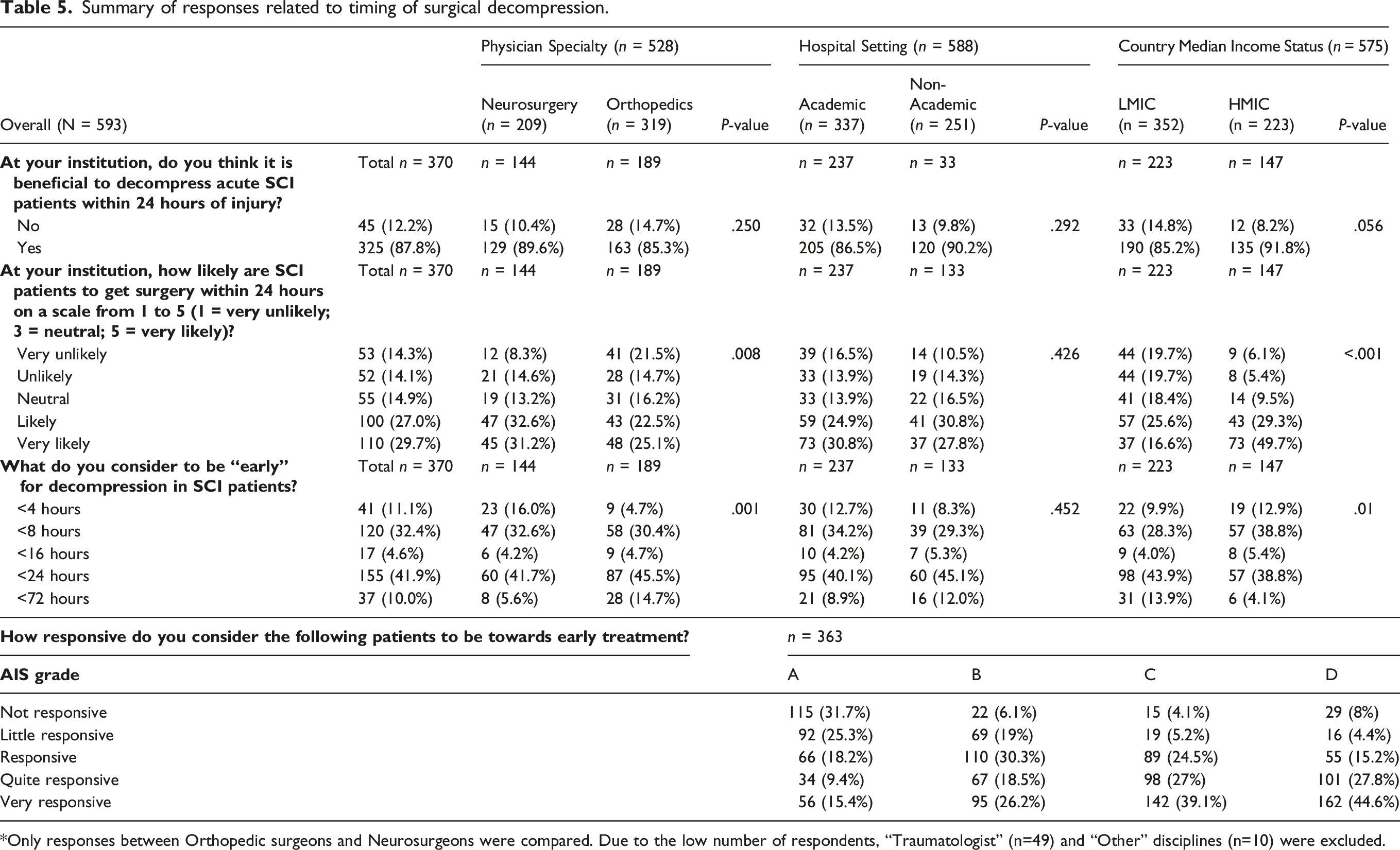
Only responses between Orthopedic surgeons and Neurosurgeons were compared. Due to the low number of respondents, “Traumatologist” (n=49) and “Other” disciplines (n=10) were excluded.
In terms of likelihood of achieving surgery within 24 hours of injury, 27% (n = 100) and 29.7% (n = 110) of respondents indicated that early surgery would be likely and very likely to be accomplished at their institution. A striking difference was evident when comparing LMICs with HICs, where 57.9% (n = 129) of respondents from LMICs indicated that early surgery would be rather unlikely to be achieved as compared to 21.1% (n = 31) from HICs (P < .001). Notably, significant differences were observed among surgical disciplines, 52.4% of orthopaedic surgeons (n = 100) indicated that early surgical decompression would be unlikely to be achieved at their institution, while only 36.1% of neurosurgeons (n = 52) reported the same (P = .008).
Barriers to early surgery.
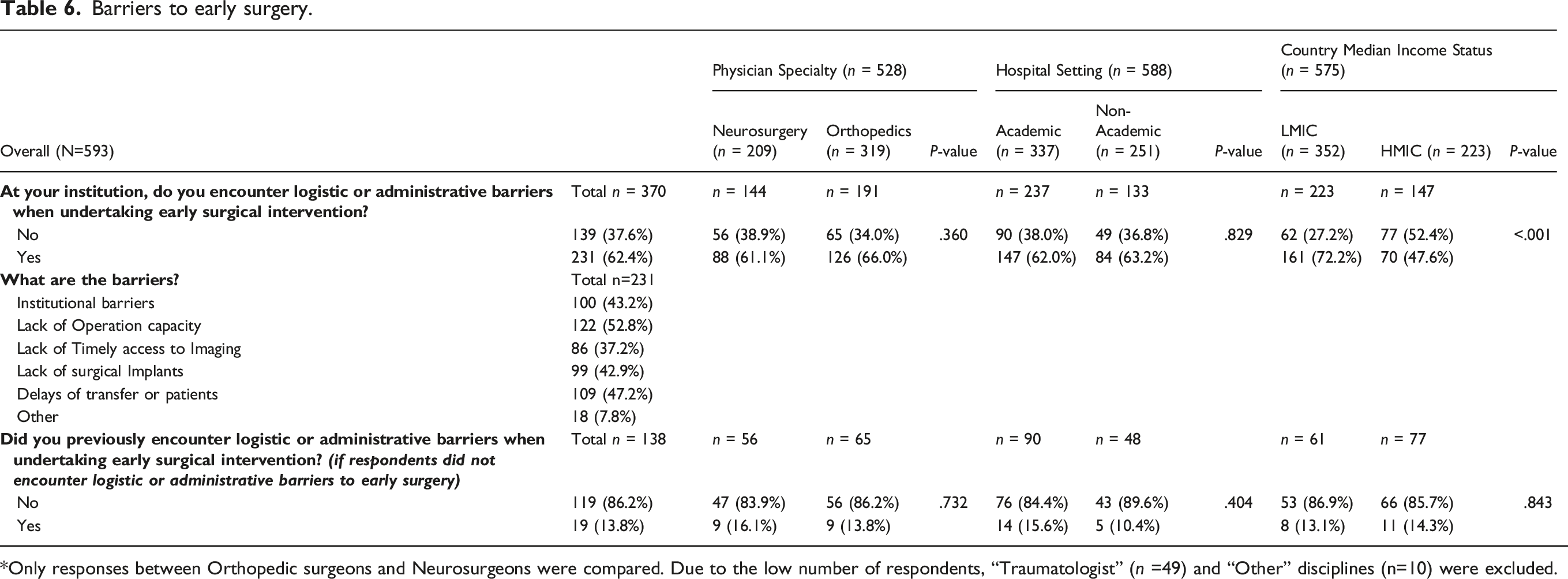
Only responses between Orthopedic surgeons and Neurosurgeons were compared. Due to the low number of respondents, “Traumatologist” (n =49) and “Other” disciplines (n=10) were excluded.
There was a considerable degree of heterogeneity as to how the injury severity, as indicated by the AIS grade, would influence the potential for neurologic improvement from earlier surgical decompression. 31.7% (n = 115) of respondents would deem AIS A patients not responsive and 25.3% (n = 92) little responsive to early surgical decompression (Table 5). Figure 3 displays patient-related factors which would play a role in decision-making for early surgical treatment. Of note, more than 60% of respondents ascribe high importance to the initial AIS grading for surgical-decision making. The common definitions of treatment success for AIS A patients reported were change in total motor score (28%; n = 205), motor levels gained (21.6%; n = 158) and AIS conversion (19.3%; n = 141), (Supplementary Table 1). Likert Plot showing the perceived importance of factors impacting decision-making for early surgical intervention for patients with acute spinal cord injury.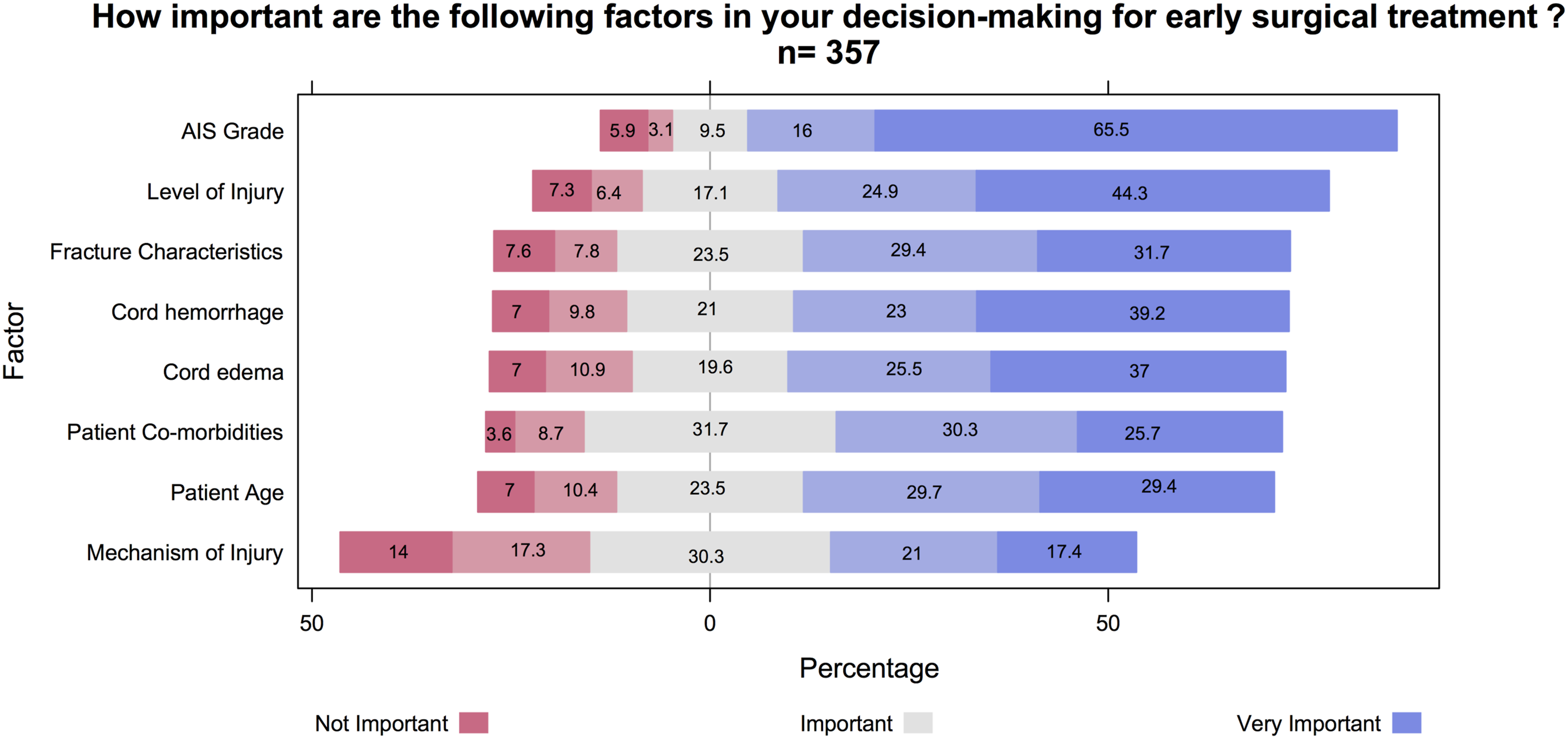
Respondent’s perception of the reliability of the initial neurologic exam done in the emergency room for the assessment of neurological function is displayed in Supplementary Table 2.
Discussion
This global survey with 593 respondent members of AO Spine highlights heterogeneities in practice patterns surrounding the administration of steroids, hemodynamic management, and timing of surgical decompression in patients with acute traumatic SCIs. The majority of respondents (61.2%) were from LMICs. As such, our sample approaches a similar trend reflecting the continuously growing population in developing countries, which has been numbered at 83% of the world’s total population. 5 With a growing burden on SCI occurring in developing countries, it becomes imperative to appraise the limitations of acute SCI care that are encountered in these environments.6,7 Ideally, knowledge generated by systematic studies in more advanced countries is transferred to those that are developing their trauma systems. However, limited resources, logistic barriers, and a lack of knowledge transfer often complicate the implementation of novel guidelines in developing countries. Despite a preponderance of respondents affiliated with academic institutions (58.3%, n = 337) and a majority of spine care professionals working at high-volume institutions (45.4%, n = 238), adherence to contemporary guidelines was heterogeneous. Several factors are thought to contribute to the heterogeneity in practice patterns observed in this survey: i) knowledge gaps and limitations in knowledge transfer, ii) new evidence, which has not yet been implemented in updated guidelines, and iii) logistical barriers complicating guideline implementation.
Management with Steroids
Steroids, with the most common drug used in this survey being MPSS (53.7%; n = 168), are potent synthetic glucocorticoids, which are thought to counteract the inflammatory response encountered during the secondary injury phase of traumatic SCI through upregulation of anti-inflammatory cytokines and blockage of lipid peroxidation of neuronal cell membranes.8,9 While newer studies have shown inconsistent results related to the efficacy of MPSS treatment in animal models of SCI, 10 historical results from preclinical studies showing enhanced tissue sparing and neuronal survival after administration of intravenous (IV) MPSS8,9 supported proceeding to large-scale randomized clinical trials (RCTs) investigating the efficacy and safety of MPSS in patients with acute SCIs.
The ongoing decades-long debates on the role of steroid administration in the management of acute SCIs 11 are reflected in this survey, where responses on the use of steroids were notably dichotomous: 53.6% (n = 256) of respondents would use this neuroprotective option while 46.4% (n = 222) would not. However, disparities became evident when comparing LMICs with HICs, whereby respondents from LMICS were more likely to administer steroids (61.2%, 178/291) than respondents from HICs (41.7%, 78/187; P < .001). The underlying reasons for these observations remain elusive, but reasons that might account for the higher rates of steroid administration observed in LMICs include: i) delayed and incomplete dissemination of knowledge in developing countries, and ii) infrastructural barriers, which limit the use of alternative neuroprotective options (blood pressure augmentation, early surgery), and therefore may favor steroids as a last-resort therapeutic option.
For decades, clinical trials have sought to determine effective dosages and the optimal timing of steroid administration in an attempt to enhance neurologic recovery following acute SCIs.12-15 Ultimately, administration of MPSS within 8 hours of injury according to the NASCIS II protocol (30 mg per kg body weight, followed by 5.4 mg per kg per hour for 23 h) was shown to have superior results in terms of AIS motor scores (changes of 16.0 vs. 11.2 points, P = .03), sensation to pinprick (change of 11.4 vs. 6.6 points, P = .02), and touch (change of 8.9 vs. 4.3, P = .03), while at the same time not significantly increasing the rates of complications. 13 While subsequent studies did not find any benefits in neurologic recovery when MPSS was administered according to the NASCIS II-regimen,15,16 a 2017-meta-analysis of four RCTs and two non-randomized cohort studies provided moderate evidence that patients receiving MPSS within 8 hours of injury were able to achieve an additional 3.2 points (95% CI: .1-6.33; P = .04) of motor score recovery compared with patients receiving placebo or no treatment. Notably, the authors did not find any statistically significant differences in the pooled risk of mortality and complications between treatment and control groups. 17 It is the latter study that provided the foundation for the 2017 AO Spine Clinical Practice Guidelines on the use of MPSS: with weak strength of recommendation and moderate quality of evidence, a 24-hour infusion of high-dose MPSS could be offered to adult patients within 8 hours of acute SCI as a treatment option. As such, the NASCIS II protocol was the preferred therapeutic regimen to administer steroids in this survey (49.8%; n = 127). Interestingly, while the AO Spine guidelines suggest not offering a 48-hour infusion of high-dose MPSS to adult patients with acute SCI (strength of recommendation: weak), 36.1% (n = 92) of respondents would administer steroids for 48 hours. Common reasons not to consider steroids in the management of acute SCI parallel concerns seen throughout the literature and entail disbelief that administration of steroids would improve neurologic recovery (38.5%; n = 111), followed by the avoidance of potential drug-associated complications (36.5%; n = 105).
A large proportion of published literature on the role of steroids in SCI involved large numbers of patients with cervical level SCIs. It, therefore, is understandable that if respondents administer steroids, they would treat cervical SCIs in 96.1% (n = 245) followed by thoracic (87.5%; n = 223) and lumbosacral SCIs (47.8%; n = 122). While results from a pooled analysis of four large prospective datasets did not provide evidence to support the routine use of MPSS in the management of acute SCI, 18 contemporary evidence does not account for the widespread heterogeneity of the SCI patient population. It is surprising to see that AIS A patients were less likely to receive steroids (72.6%; n = 185) than AIS B (82.8%; n = 211) and AIS C (76.5%; n = 195) patients. One potential explanation for this might be found in the severity of injury in AIS A patients and the potential for concomitant injuries and risk of complications, which in turn may deter spine care professionals from exposing patients to any potential risks associated with MPSS therapy.
Future research efforts are warranted to address the heterogeneity of the SCI patient population, thereby identifying subgroups of patients with the highest potential to benefit from anti-inflammatory therapies such as steroids. This survey picked up a higher number of institutions in LMICs where steroids are given in the management of acute SCI. The relatively common administration of steroids for acute SCI in LMICs represents a potential opportunity to investigate the neurologic effects in certain subgroups of SCI, although generating the kind of high-quality data necessary to interpret such efficacy is challenging, even in centers with well-established research infrastructure.
Hemodynamic Management
It was only in the early 1990s that ischemia due to compromised spinal cord perfusion was identified as a major component of the secondary injury cascade promoting protracted neuroglial cell death, thereby impacting functional recovery in the post-injury period. 19 Recognition and understanding of the vascular processes involved during the secondary injury period has driven clinical research and ultimately corroborated the concept of hemodynamic management of acute SCI. Despite a paucity of evidence, early findings have been compiled in an attempt to develop the first guidelines on blood pressure management in the setting of acute SCIs. 20 And yet, owing to a paucity of new high-quality data, these guidelines remained unchanged in the 2013 AANS/CNS updates. 3 The best evidence we have to date is therefore of class III: in the intensive care unit or an analogous monitoring setting, systemic hypotension should be avoided by maintaining the systolic blood pressure of >90 mmHg and a MAP of 85-90mmHg during the first 5-7 days following the injury.
With the majority of respondents providing MAP targeted treatment (81.5%, n = 331), the importance of hemodynamic management has seemingly gained wide recognition. Yet, 18.5% (n = 75) of respondents would not provide MAP targeted treatment, a number which becomes significantly different when comparing LMICs, where 23.1% (n = 58) would not provide MAP targeted treatment, against HICs (12.8%; n = 20; P = .002). Notably, common reasons not to provide MAP targeted treatment included logistical barriers, such as lack of ICU beds or monitoring capacity. It is estimated that in HICs, generally between 5 to 30 ICU beds are available per 100,000 people, whereas in LMICs there are only .1 to 2.5 ICU beds per 100,000 people. 21 With many countries transitioning from LICs to lower MICs, less international healthcare aid is being allocated which further limits resources available for expanding capacity. 22 These findings highlight the predicament in guideline implementation in LMICs, where the capacity for critical illness care is oftentimes a limiting factor.
Contemporary guidelines have given rise to several ongoing concerns, which might explain uncertainty as to whether the 2013 AANS/CNS guidelines would be sufficient to guide hemodynamic management. 39.3% (n = 159) of respondents stated that the guideline recommendations would not be sufficient to guide hemodynamic management. As an example, the risks of using vasopressors or IV fluids in the setting of concomitant injuries or comorbidities might outweigh the benefits of preserving spinal cord perfusion, and therefore warrants careful evaluation on an individual basis. A single-center retrospective cohort study of 131 patients found the two most commonly used vasopressors, dopamine (48%) and phenylephrine (45%), to be independently associated with increased rates of complications (Dopamine, OR: 8.97, P<.001; Phenylephrine, OR 5.92, P = .004). 23 Of note, a recent study highlighted the challenges of achieving the recommended MAP targets of 85-90 mmHg using IV fluids and vasopressors. The authors collected high frequency data during the first 5 days following SCI and found that only 24 ± 7% of MAP recordings were within the targeted range. 24 Finally, the 2013 AANS/CNS guideline does not contain the level of granularity necessary to guide whether patients with different AIS grades and levels of injury require the same regimen of hemodynamic management, including blood pressure targets and duration of monitoring. These uncertainties are underpinned by the varied responses seen in this survey surrounding the duration of hemodynamic management for patients with different AIS grades and levels of injury.
The paucity of evidence is further reflected in this survey, where responses on certain aspects of hemodynamic management were notably heterogeneous. As an example, 66.8% (n = 221) of respondents would choose MAP targets of 85-90 mmHg, while 33.2% would target either lower (80-85 mmHg) or higher (>90 mmHg) values. A single-center study, where SCI patients were treated with MAP targets of 85-90 mmHg, analyzed high-frequency MAP data for 100 patients and found higher average MAP values correlating with improved AIS grade recovery. Importantly, patients who had less frequent MAP values below the threshold of 85 mmHg were more often found to achieve >1 grade of AIS grade improvement, particularly within the first 2-3 days following injury. 25 And yet, while MAP and SBP were the most commonly chosen parameters used to guide hemodynamic management, other authors have highlighted the potential for spinal cord perfusion pressure (SCPP) to be a more relevant physiologic measure, similar to how cerebral perfusion pressure is utilized to guide treatment in traumatic brain injury.26-28 Hence, SCPP-guided management with targets of 60 to 65 mmHg was shown to be a better indicator of improved neurologic recovery as compared to other parameters such as MAP or cerebrospinal fluid pressures. 27 It is important to note, however, that management according to SCPPs would necessitate invasive monitoring techniques such as intrathecal catheters. With exciting technologies on the horizon, including intrathecal pressure monitors and epidural near-infrared spectroscopy sensors, further evaluation is needed to assess their safety as well as efficacy, and these are considered investigational at this time.
Timing of Surgical Decompression
Based on the survey results on surgical timing of SCI, it is evident that spine surgeons around the world recognize the importance of early decompression to improve neurologic recovery in patients with SCI. This high level of awareness validates the efficacy of the “Time is Spine” campaign that resulted from finding a benefit to early intervention in support of the STASCIS trial published almost a decade ago, and which was recently reinforced by a pooled analysis of four large SCI databases.18,29 Nevertheless, the achievement of this time-oriented goal is limited by several constraining variables that may lead to a gap in knowledge translation. These factors, however, are highly polarized between HICs and LMICs, resulting in a likelihood difference between the two groups. In our survey, for example, 57.9% of surgeons from LMICS and 21% in HICs expressed that early surgery is perceived as unlikely in their institutions. A study by Thompson et al. showed that in developed countries, administrative factors are the main barrier to early surgery including transfer delay, delay before surgical plan completion, and waiting time for the operating room. 30 This is in contrast to LMICs, where additional issues related to infrastructure and finance may play a significant role. Grimes and colleagues summarized in a systematic review several patient- and surgeon-perceived roadblocks to surgical care in developing countries and divided them into three broad categories, which include structural issues (e.g., lack of facilities), cultural factors (e.g., adverse attitudes and beliefs), and financial cost (e.g., direct and indirect expenditures). 31 Our survey results collectively ascertain the existence of these health care delivery factors in LMICs that need to be addressed in order to achieve early surgery in SCI patients. Overcoming these issues will require a concerted effort from the government and private sector to ensure that adequate infrastructure, a reliable transport system, sufficient manpower, and sustainable funding are all available.
The optimal timing of surgery, including the definition of “early” intervention, remains controversial. Our survey asked respondents about the surgical cut-off period they considered “early” in patients presenting with SCI. Although responses varied, the majority favored a 24-hour time cut-off after the injury. These results highlight not only the existing worldwide practice variation among spine surgeons, but also reflect the current state of research on this topic. While the 2017 joint AO Spine North America, AO Spine International, and AANS/CNS clinical practice guideline for the management of patients with acute SCI recommended early intervention using the 24-hour mark to delineate early from late surgery, 32 a newer body of evidence shows that a much earlier cut-off of 12 or 8 hours may lead to better neurologic recovery after SCI.33,34 On the other end of the spectrum, some authors advocate extending this cut-off to 48 to 72 hours to provide greater leeway in low-resource settings where considerable challenges to early surgery exist.35,36 The generalizability and applicability of these studies advocating earlier or later surgery are limited by their small sample size and single-center enrolment.
Our survey results showed that the patient’s baseline neurologic status plays a significant role in decision-making to proceed with early intervention. Respondents have a perception that patients with an incomplete injury (e.g., AIS B, C, D) are more responsive to early surgery than those who sustain a complete SCI (e.g., AIS A). While this concept is in line with historical notions that motor complete SCI patients have a uniformly dismal prognosis, recent studies have been endorsing a mindset favoring early surgery because a relatively higher rate of conversion to AIS B (28-40%) is expected compared to historical evidence of AIS conversion in this patient population (15-20%).29,37 Our results underscore that this a pervasive concept and corroborates earlier findings of a survey done in the UK and Canada, which showed that spine surgeons favor the provision of more urgent surgical attention in incomplete SCI patients than in those with complete injuries.38,39 This preference is in line with evidence that the initial neurologic injury severity is an important predictor of recovery after SCI. 40 By decompressing the cord early, surgeons hope that patients with incomplete injury will recover additional motor/sensory function by minimizing secondary insults and establishing an environment more conducive for other medical interventions.
Limitations
This study has some limitations which warrant further discussion. The first limitation is the response rate of at most 9.1% (with >6500 AO Spine members). However, we observed that the geographical representation of the respondents according to the level of income of their respective countries reflects the distribution of the global population living in LMICs and HICs. This is an important aspect, given the varied responses observed in this study highly depend on the country level of income. Additionally, not all of the >6500 members are spine care professionals involved in the management of patients with acute SCIs and as such, the number of eligible members is further reduced. Finally, the response rate in this study is comparable with previous surveys among AO Spine members.41,42 A second limitation is that clinical guidelines and recommendations may vary between societies on the international and national level, and thus the guidelines mentioned in this survey might not account for every institution and member of this survey. However, guidelines and recommendations on the management of acute SCI are sparse and adherence to the best available evidence is pivotal. It is therefore our belief that this global study provides valuable insights into current practice patterns in the management of acute SCI.
Conclusion
This survey highlights challenges in the implementation of standardized practice regarding the use of steroids, hemodynamic management, and practical use of early surgical intervention, despite clear evidence for surgeon preference to implement a “Time is Spine” approach. Challenges become particularly evident in countries and institutions with limited logistical and infrastructural resources such as in low- and middle-income countries. Therefore, future research efforts will need to address barriers to guideline implementation, such as logistic hurdles in the implementation of early decompressive surgery or allocation of limited resources for SCI patients in need of hemodynamic therapy. Moreover, this work highlights the importance of continuing to refine guidelines and strengthening modalities of knowledge transfer, as the rapidly evolving realm of SCI research continues to produce pivotal evidence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Spinal Cord Injury, a focused group of international Spinal Cord Injury experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through AO Network Clinical Research. NH is supported by the Research Fund of the University of Basel for Excellent Junior Researchers. MGF is supported by the Robert Campeau Family Foundation/Dr. C.H. Tator Chair in Brain and Spinal Cord Research at UHN.