
Abstract
Study Design
Retrospective Cohort Study.
Objectives
To (1) investigate the effect of marijuana use on surgical outcomes following lumbar fusion, (2) determine how marijuana use affects patient-reported outcomes measures (PROMs), and (3) determine if marijuana use impacts the quantity of opioids prescribed.
Methods
Patients
Results
Of the 259 included patients, 65 used marijuana preoperatively. Multivariate logistic regression analysis demonstrated that marijuana use (OR = 2.28, P = .041) significantly increased the likelihood of having a spine reoperation. No other surgical outcome was found to be significantly different between groups. Multivariate linear regression analysis showed that marijuana use was not significantly associated with changes in 1-year postoperative PROMs (all, P > .05). The quantity of pre- and postoperative opioids prescriptions was not significantly different between groups (all, P > .05).
Conclusions
Preoperative marijuana use increased the likelihood of a spine reoperation for any indication following lumbar fusion, but it was not associated with 90-day all cause readmission, surgical readmission, the magnitude of improvement in PROMs, or differences in opioid consumption.
Level of Evidence
III
Introduction
Prior to surgical intervention, treatment of axial back pain and radiculopathy typically involves a combination of analgesic medications and physical therapy.1-3 Opioids are a commonly utilized analgesic option; however, increased opioid use has been associated with higher morbidity and less improvement in pain and physical function following spine surgery.4-6 Given that lumbar fusion procedures are associated with an increased risk of postoperative chronic opioid use, some providers have begun to explore marijuana as an alternative adjunct in analgesic regimens both prior to and following lumbar fusion. 7
In the United States, an estimated 49.6 million adults use marijuana either medically or recreationally according to the Department of Health and Human Services’ (HHA) National Survey on Drug Use and Health, which represents an increase of approximately 55% in estimated marijuana users over the past 5 years.8,9 This dramatic increase can be partly attributed to over 30 states legalizing marijuana for medical and/or recreational use as of January 1, 2022.10-12
Currently, one of the most common indications for a medical marijuana prescription is chronic low back pain with or without concurrent radiculopathy. 13 Translational research studies have suggested that cannabinoids, the pharmacologically active components of marijuana, are effective for modulating neuropathic pain through nociceptor inhibition.14-16 While these findings may provide a basis for the use of marijuana in patients who are candidates for lumbar fusion, there is a paucity of clinical literature investigating how marijuana use affects clinical outcomes following fusion procedures.
Therefore, the objectives of the present study are to (1) investigate the effect of marijuana use on clinical outcomes including surgical complications, readmissions, and reoperations following lumbar fusion; (2) determine how marijuana use affects patient-reported outcomes measures (PROMs) at the 3-month, 6-month, and 1-year postoperative period after lumbar fusion and (3) determine if marijuana use impacts the quantity of opioids prescribed (in milligram of morphine equivalents (MME)) in the preoperative and 1-year postoperative period following lumbar fusion.
Methods
Inclusion Criteria
The study was given exempt status from requiring informed patient consent by our Institutional Review Board (IRB) due to its retrospective design and minimal risk to patients. After IRB approval, all patients greater than or equal to 18 years of age who underwent primary one- or two-level lumbar fusion with documented preoperative marijuana use at our academic medical institution between 2012-2021 were retrospectively identified. Patients were excluded if the lumbar fusion was performed as a revision procedure or was indicated in the setting of trauma, infection, or neoplasm.
Data Extraction
Patient demographics, surgical characteristics, and surgical outcomes were collected through Structured Query Language (SQL) search and manual chart review of the electronic medical records. The electronic medical records were manually reviewed to determine recreational or medical marijuana use up to the last preoperative appointment. Information on the strain, potency, method of intake, or duration of use was not available, therefore, only documented marijuana use was recorded. Cannabidiol (CBD) oil was considered a distinct medication from marijuana use and was not included in our query for marijuana use. A 3:1 propensity match, controlling for patient age, sex, body mass index (BMI), smoking status (non-smoker, current smoker, former smoker), Charlson Comorbidity Index (CCI), and procedure type (posterior lumbar decompression and fusion (PLDF), circumferential fusion (A/PLDF), or transforaminal lumbar interbody fusion (TLIF)) was then performed to match patients with documented marijuana use to patients without marijuana use from an internal database of primary one- or two-level lumbar fusions.
Surgical complications and medical complications were recorded for each patient. Subsequently, 90-day all-cause readmissions and 90-day surgical readmissions were recorded. Spine reoperations within 3 years following the index procedure including incision and drainage, dural repair, hardware failure, revision for recurrent index level stenosis, adjacent segment pathology, or pseudarthrosis were also recorded. Patient-reported outcomes measures (PROMs) were retrospectively collected through our institution’s prospectively collected database (OBERD, Columbia, MO) and were included at the preoperative, 3-month, 6-month, and 1-year postoperative time points. PROMs extracted included the Visual Analogue Scale for back pain (VAS Back) and leg pain (VAS Leg), the Oswestry Disability Index (ODI), and the Mental and Physical Component Scores of the Short-Form 12 (SF-12) Health Survey (MCS-12 and PCS-12, respectively). The change in each PROM score (Δ) at the 3-month, 6-month, and 1-year postoperative points was calculated by subtracting the preoperative from the corresponding postoperative value.
All patients without marijuana use had a complete set of opioid prescription data from our state’s Prescription Drug Monitoring Program (PDMP) database. For all patients included in this study, the total quantity of opioid prescriptions in morphine milligram equivalents (MME) was collected and recorded through our state’s PDMP database from the 1-year preoperative to the 1-year postoperative time point. Patients were considered opioid naïve if they were not provided opioid prescriptions after June 2016.
Statistical Analysis
Descriptive statistics including mean and standard deviation were used to report patient demographics, surgical characteristics, and surgical outcomes. A Shapiro-Wilk test was used to analyze the normality of each continuous variable, and parametric data was analyzed with independent t-tests while non-parametric data was analyzed with Mann-Whitney U tests. Categorical variables were analyzed with Pearson’s chi-square tests. A multivariate logistic regression model was developed to measure the effect of marijuana use on the likelihood of undergoing a spine reoperation for any cause when accounting for age, smoking status, CCI, and the number of levels fused. Multivariate linear regression models were developed to determine the independent association of marijuana use on Δ PROM scores at the 1-year postoperative point. R software, version 3.6.3 (R Foundation for Statistical Computing, Vienna, Austria) was used for all data analysis. Statistical significance was set a P < .05.
Results
Patient Demographics and Opioid Use
Demographics.
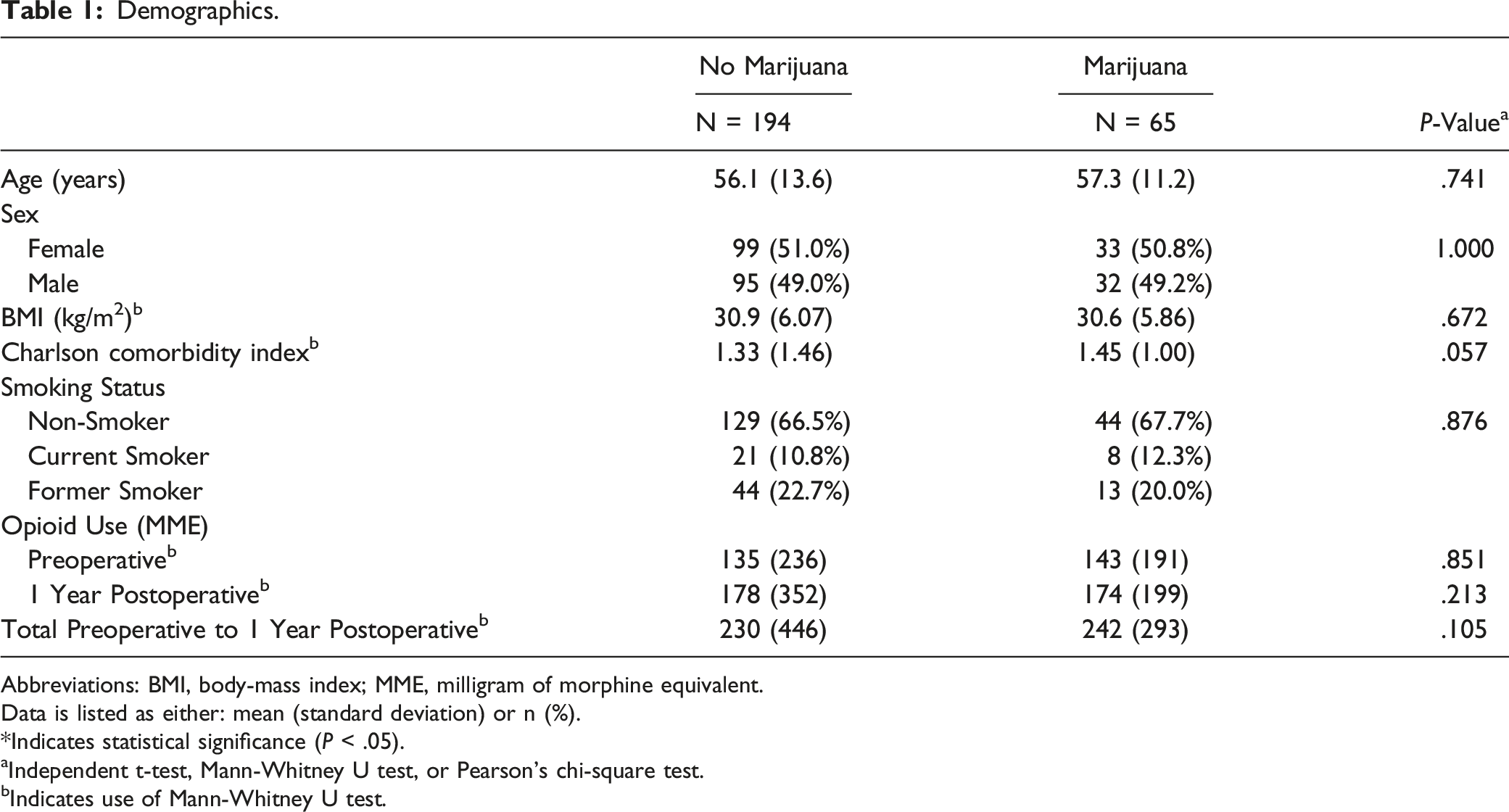
Abbreviations: BMI, body-mass index; MME, milligram of morphine equivalent.
Data is listed as either: mean (standard deviation) or n (%).
*Indicates statistical significance (P < .05).
aIndependent t-test, Mann-Whitney U test, or Pearson’s chi-square test.
bIndicates use of Mann-Whitney U test.
Surgical Characteristics and Outcomes
Surgical Characteristics and Outcomes.
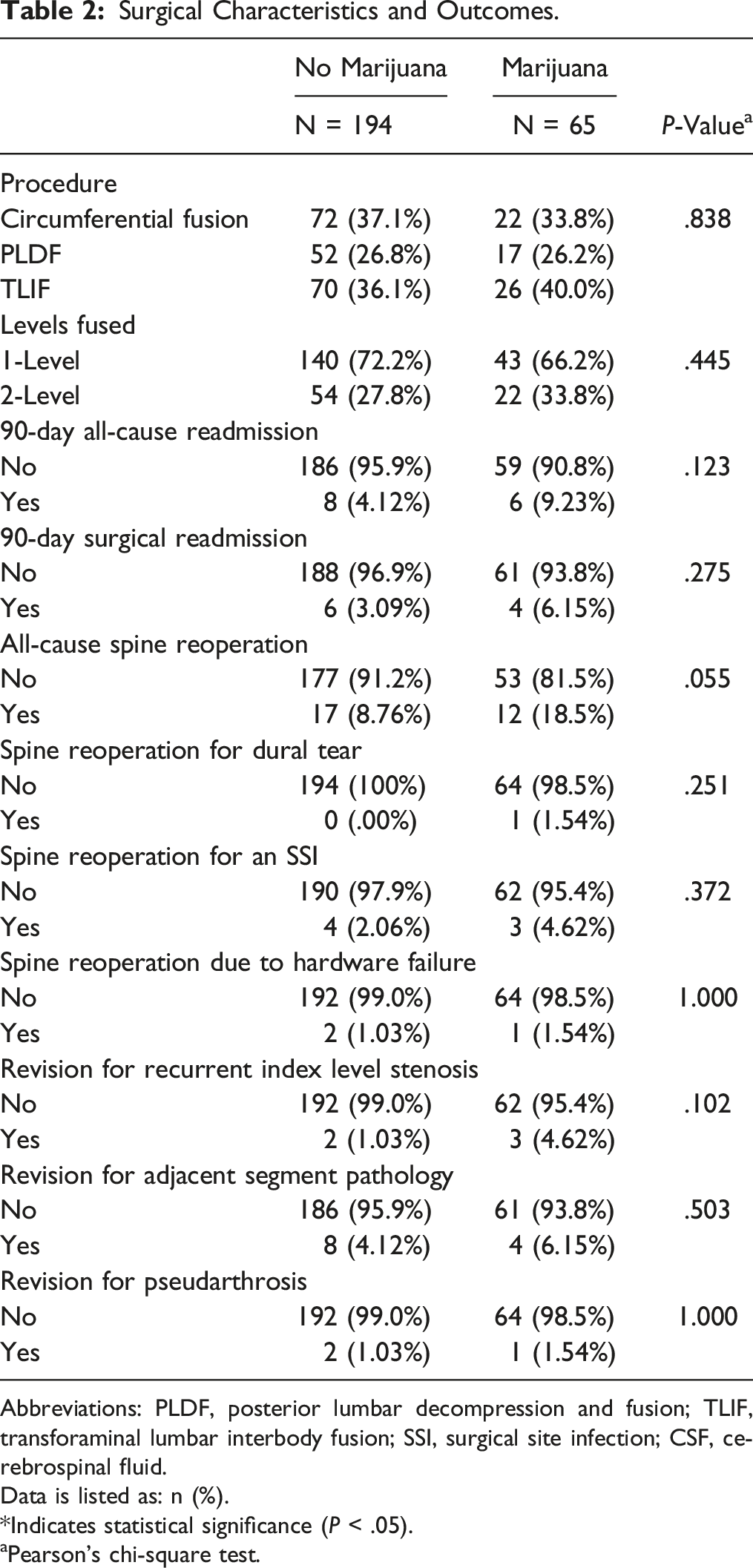
Abbreviations: PLDF, posterior lumbar decompression and fusion; TLIF, transforaminal lumbar interbody fusion; SSI, surgical site infection; CSF, cerebrospinal fluid.
Data is listed as: n (%).
*Indicates statistical significance (P < .05).
aPearson’s chi-square test.
Multivariate Logistic Regression-All-Cause Spine Reoperations.
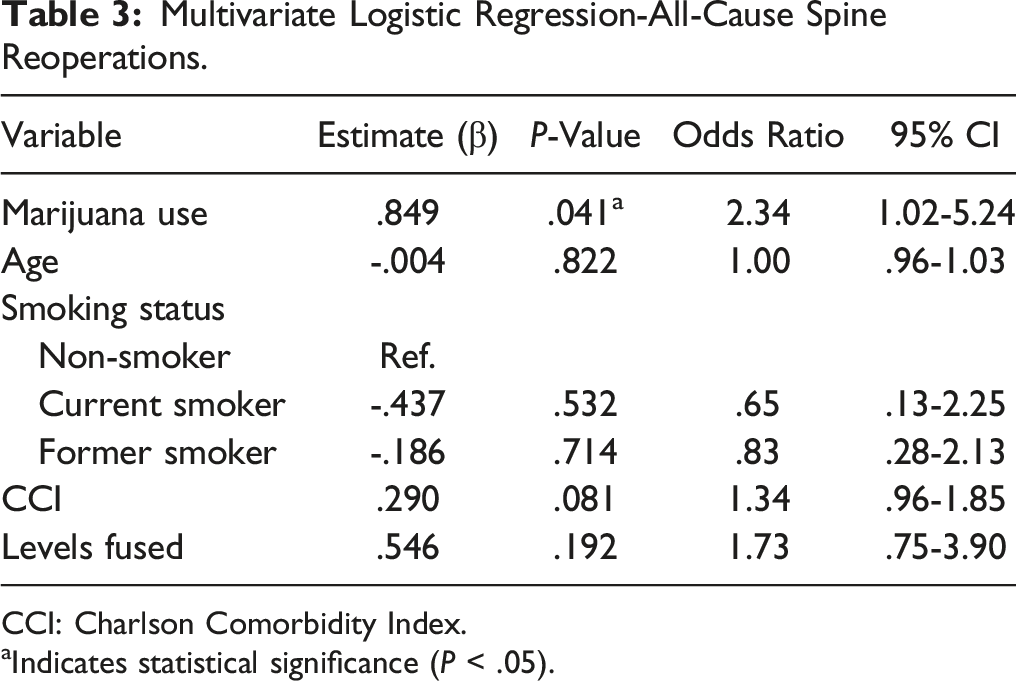
CCI: Charlson Comorbidity Index.
aIndicates statistical significance (P < .05).
Patient-Reported Outcomes
Patient-Reported Outcomes.
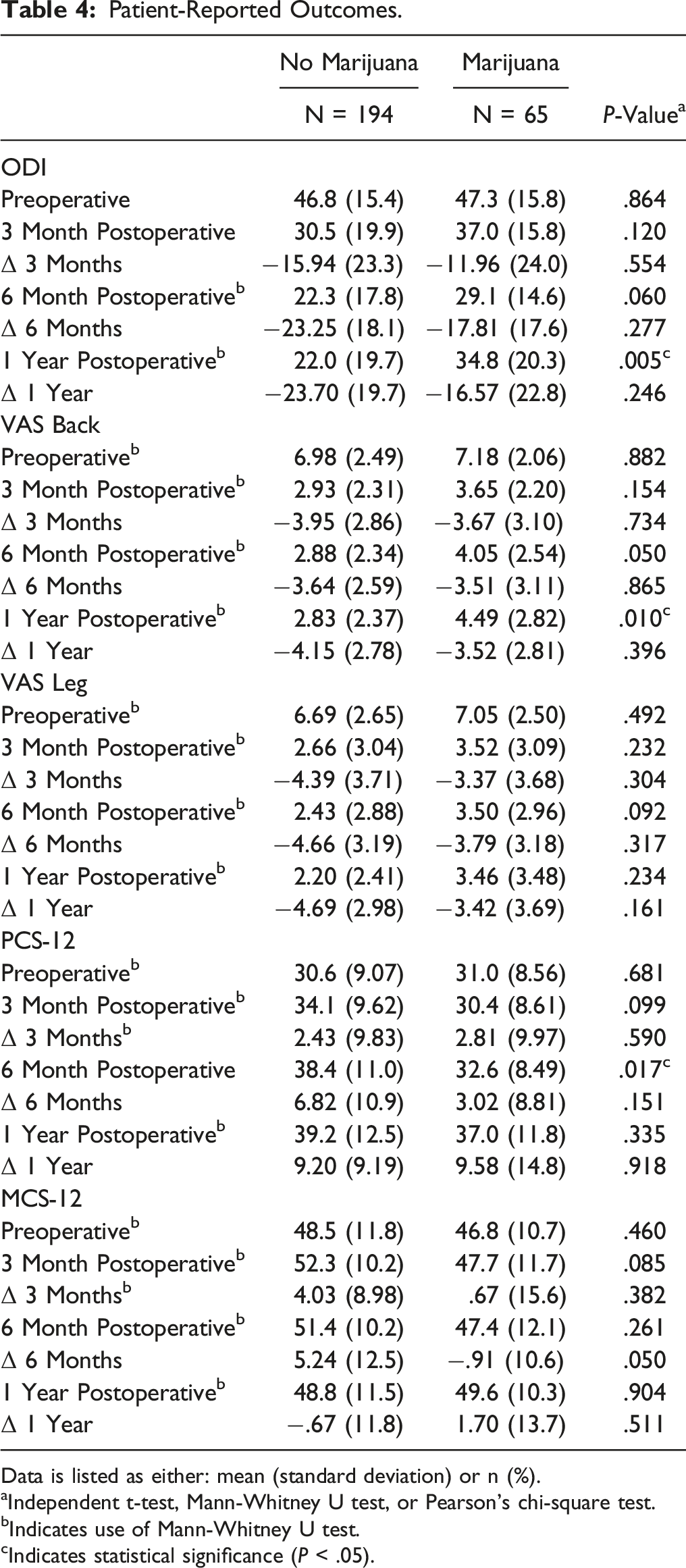
Data is listed as either: mean (standard deviation) or n (%).
aIndependent t-test, Mann-Whitney U test, or Pearson’s chi-square test.
bIndicates use of Mann-Whitney U test.
cIndicates statistical significance (P < .05).
Multiple Linear Regression-Delta PROMs at 1 Year.
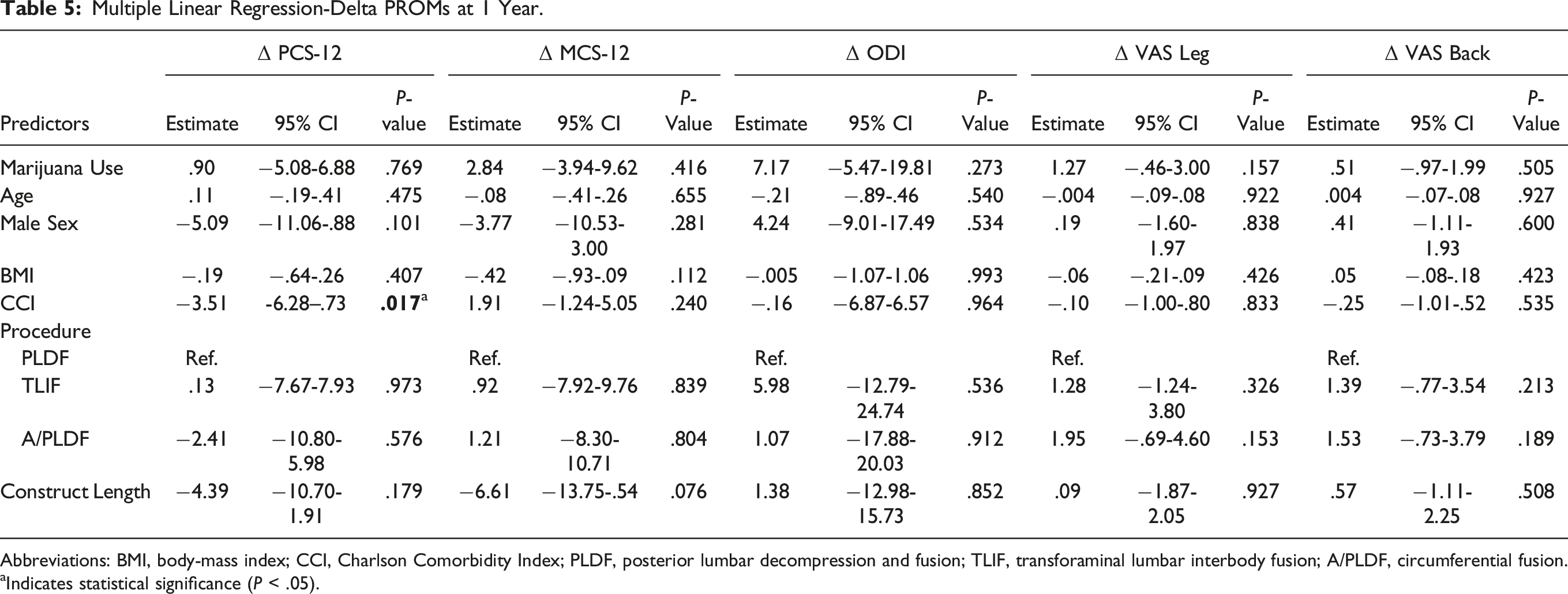
Abbreviations: BMI, body-mass index; CCI, Charlson Comorbidity Index; PLDF, posterior lumbar decompression and fusion; TLIF, transforaminal lumbar interbody fusion; A/PLDF, circumferential fusion.
aIndicates statistical significance (P < .05).
There were no significant differences in preoperative (143 ± 191 vs 135 ± 236, P = .851), 1-year postoperative (174 ± 199 vs 178 ± 352, P = .213), and the total preoperative to 1-year postoperative (242 ± 293 vs 230 ± 446, P = .105) MME prescribed between patients who used marijuana and patients who did not (Table 1). Among patients who used marijuana, those who were opioid naïve had significantly lower MME prescribed 1 year postoperatively (92.4 ± 111 vs 263 ± 236, P = .001). Preoperative marijuana use also did not significantly affect the amount of postoperative opioid prescriptions when accounting for the quantity of opioids prescribed preoperatively (naïve: 92.4 ± 111, non-naïve: 119 ± 260, P = .597) (Supplemental Data 1).
Discussion
The volume of lumbar fusions performed per year in the United States has increased substantially over the last 2 decades and is projected to increase another 20% by 2040.17-19 Identification of perioperative factors affecting surgical outcomes and postoperative opioid utilization are imperative, especially when taking into consideration the current opioid epidemic. As marijuana legislation is rapidly expanding across the United States, it has become a promising alternative therapeutic option for patients with axial back pain and radiculopathy. However, there is a dearth of clinical evidence supporting its use in patients undergoing lumbar fusion. 13 Our results suggest preoperative marijuana use does not significantly influence complication rates, readmission rates, or the quantity of opioids prescribed following lumbar fusion; however, it is associated with increased lumbar spine reoperations within 3 years of the index procedure. Marijuana use also does not have a significant effect on changes in PROMs related to pain, disability, physical function, or mental function at 1-year follow up. This finding is critical, as chronic preoperative opioid use has been associated with significantly lower quality of life and poor clinical outcomes at the 1 year postoperative point following spine surgery. 20
Opioids are a commonly prescribed preoperative and postoperative analgesic medication.6,21-23 The rationale behind offering marijuana as an adjunctive analgesic is based on the potential opioid-sparing effects of cannabinoids. 24 Through activation of cannabinoid-receptor 1 (CB1), cannabinoids inhibit calcium release at the presynaptic membrane and reduce nociceptor signaling.16,25 Cannabinoids can alternatively activate cannabinoid-receptor 2 (CB2) on immune cells either within or outside of the central or peripheral nervous system, resulting in the release of cytokines that indirectly stimulate μ-opioid receptors.26-28 However, chronic activation of CB1 receptors can lead to downregulation, causing increased nociceptive activity, potentially necessitating the use of additional pain medication for patients. 25 While previous research has described the potential of combining cannabinoids with opioids or other μ-opioid agonists to manage pain, our study suggests marijuana use does not alter preoperative or postoperative opioid prescription practices in patients undergoing lumbar fusion. 29 Since our state’s PDMP only indicates the number of opioids prescribed and is unable to account for opioid consumption, future prospective trials are necessary to further characterize the role of marijuana as an opioid-sparing analgesia option in patients undergoing lumbar fusion.
Previous literature has described the relationship between preoperative marijuana use and complications following various elective procedures, including 1 large database study that found marijuana use increased the risk of myocardial infarction in the acute postoperative period. 30 Across all orthopaedic literature, retrospective arthroplasty and spine studies have suggested that preoperative marijuana use is associated with an increased risk of acute postoperative medical complications and 90-day readmissions.31-33 In our study, patients who used marijuana experienced a non-significant higher rate of readmissions due to medical and post-surgical causes, which corresponded to a greater all-cause spine reoperation rate when compared to patients who did not use marijuana. Whether these differences are clinically significant remains to be elucidated; however, in the context of previous literature, spine surgeons should counsel patients that marijuana use may be associated with an increased risk of acute postoperative complications and hospital readmission.
Further discussion on the association between marijuana use and reoperation is warranted given the current limited understanding of marijuana use and its effects on bone and neurologic biology. Our multivariate regression analysis, which accounted for patient demographics and levels fused, demonstrated that marijuana use significantly increased the risk of a lumbar spine reoperation within 3 years following the index procedure. Given that most spine reoperations in marijuana users were due to recurrent index level or adjacent level pathology, surgeons may be “searching” for additional surgical options to improve patients’ 1-year postoperative disability and back pain scores (which were significantly greater than the scores in non-marijuana users). Additionally, surgeons may feel obligated to assist patients in eliminating their reliance on marijuana use for the management of their chronic back pain. Although these hypotheses are purely speculation, this discussion highlights our current lack of knowledge on the association between marijuana and postoperative back pain, especially following lumbar fusion.
The impact of marijuana use on patient-reported outcomes following lumbar fusion is poorly characterized in the spine literature. To our knowledge, only 1 other retrospective study has attempted to evaluate the effect of marijuana use on PROMs following lumbar fusion. The authors found that marijuana use does not significantly affect ODI scores at the 6-month and 1-year postoperative periods following TLIF. 34 Our study, which analyzed PROMs in patients undergoing PLDF, A/PLDF, and TLIF procedures, showed that patients who use marijuana report significantly greater back pain and disability at the 1-year postoperative point, as indicated by greater ODI and VAS Back scores. However, marijuana use did not significantly impact the magnitude of change in ODI or VAS Back scores at the 1-year postoperative point. On multivariate linear regression analysis, which accounted for patient demographics, surgical characteristics, and surgical approach, our results also indicate the magnitude of change in 1-year postoperative PROMs evaluating pain, disability, physical and mental function were not significantly impacted by marijuana use. However, at this time, all studies evaluating the impact of marijuana on postoperative outcomes have all been based on short-term outcomes. There is a significant need for future studies to characterize the relationship between marijuana use and long-term postoperative outcomes.
This study is not without limitations, including those inherent to any retrospective analysis. While each patients’s chart was reviewed for documentation of marijuana use, information on the potency or strain of marijuana used, method of consumption, amount consumed, or the frequency of utilization by each patient was not readily available for the majority of our patients and was not included in the analysis. Additionally, CBD oils were considered distinct medications from marijuana and therefore were not included in our analysis. Since it is unknown if marijuana intake or CBD use affects patient-reported outcomes to different degrees, we chose to only include patients who specifically report marijuana use. However, we acknowledge this may be an interesting avenue for future research. Another limitation of the study was our inability to accurately identify whether patients continued cannabis use in the postoperative period and whether this affected surgical outcomes, patient reported outcomes, or opioid prescriptions. While data on opioid prescriptions was collected from our state’s PDMP, we were unable to verify if each patient consumed the entirety of each prescription that was filled. Further, the lack of granularity in our electronic medical records made it difficult to identify the reason for preoperative opioid use, and the inception of the PDMP in 2016 limited our ability to use this resource to glean additional information on the reason for the preoperative opioid prescriptions, which may have been for non-lumbar spine related pain. Further, the number of opioids prescribed to an individual patient may have been underestimated if the patient filled 1 or more prescriptions in a state that is not registered in our state’s PDMP interstate data-sharing program. 35 It is likely that cannabis use was underreported in our electronic medical records and a more accurate way to identify marijuana use would be through routine preoperative urinalysis, although this would be difficult to implement clinically. Further, our propensity matching did not include medications (including opioids) or the indication for the lumbar fusion, which may affect surgical outcomes. Finally, the variability in the lumbar fusion approach and corresponding postoperative care may have influenced clinical and patient-reported outcomes; however, this may ultimately increase the generalizability of our study
Conclusion
Preoperative marijuana may increase the risk of a spine reoperation within 3 years following a primary lumbar fusion. However, it does not appear to significantly affect changes in patient-reported outcomes measures at the 1-year postoperative point. Further, marijuana use did not significantly impact the quantity of opioids prescribed in the preoperative or 1-year postoperative period. This study highlights the need for future high-quality prospective studies to improve our understanding of the impact of marijuana on outcomes in patients undergoing lumbar fusion.
Supplemental Material
Supplemental Material - The Effect of Preoperative Marijuana Use on Surgical Outcomes, Patient-Reported Outcomes, and Opioid Consumption Following Lumbar Fusion
Supplemental Material for The Effect of Preoperative Marijuana Use on Surgical Outcomes, Patient-Reported Outcomes, and Opioid Consumption Following Lumbar Fusion by Nicholas D. D’Antonio, Mark J. Lambrechts, Jeremy C. Heard, Nicholas Siegel, Brian A. Karamian, Angela Huang, Jose A. Canseco, Barrett Woods, Ian David Kaye, Alan S. Hilibrand, Christopher K. Kepler, Alexander R. Vaccaro, and Gregory D. Schroeder in Global Spine Journal
Footnotes
Authors’ Note
IRB Approval: Control #19D.508.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.