
Abstract
Study designs
Retrospective Observational Study
Methods
In this study, the medical records of elderly patients ≥ 65 years of age who underwent spine surgery under total intravenous anesthesia with propofol or inhalational anesthesia with sevoflurane were reviewed. The primary outcome was the incidence of POD after propofol- and sevoflurane-based anesthesia. Secondary outcomes included postoperative 30-day complications, length of postoperative hospital stay, associations of patient characteristics, and surgery- and anesthesia-related data with the development of POD, and associations of anesthetics with clinical outcomes such as postoperative 30-day complications, and length of postoperative hospital stay.
Results
Of the 281 patients, POD occurred in 29 patients (10.3%). POD occurred more frequently in the sevoflurane group than in the propofol group (15.7% vs. 5.0%, respectively; P=.003). The multivariable logistic regression analysis showed that sevoflurane-based anesthesia was associated with an increased risk of POD compared with propofol-based anesthesia (odds ratio [OR], 4.120; 95% confidence interval [CI], 1.549−10.954; P = .005), whereas anesthetics were not associated with postoperative 30-day complications and the length of postoperative hospital stay. Older age (OR, 1.242 CI, 1.130−1.366; P < .001) and higher mean pain score at postoperative day 1 (OR, 1.338 CI, 1.056−1.696; P = .016) were also associated with an increased risk of POD.
Conclusions
Propofol-based anesthesia was associated with a lower incidence of POD than sevoflurane-based anesthesia in elderly patients after spine surgery.
Introduction
With the increased life expectancy, the number of elderly patients undergoing spine surgery is increasing. Postoperative delirium (POD) is a common complication following anesthesia and surgery in elderly patients, with an incidence between 4% and 41% in elderly patients undergoing spine surgery.1,2 It can contribute to serious complications such as prolonged hospitalization, reduced quality of life, and increased morbidity and mortality.3,4 Therefore, multicomponent strategies based on modifiable risk factors have been introduced to prevent POD. 5
The mechanism of POD is not fully understood and may be multifactorial. Anesthetics may affect the development of POD because their main target is the brain. 6 Currently, total intravenous anesthesia with propofol and inhalational anesthesia with sevoflurane are widely used for maintenance of general anesthesia in clinical practice. The effects of propofol and sevoflurane on the brain remain unclear. Some experimental studies showed that sevoflurane exerted neuroprotective effects against cerebral injuries,7,8 whereas other studies reported the neurotoxicity of sevoflurane.9-11 The neuroprotective10,12 and neurotoxic properties13,14 of propofol on the brain have also been suggested in experimental studies.
The mechanisms of action of propofol and sevoflurane have not been clearly determined, and may not be the same in the brain, although most general anesthetics mainly target the inhibitory γ-aminobutyric acid type A receptors. 6 Therefore, their effects on the development of POD may be different. Several studies have suggested the effects of propofol and sevoflurane on POD; however, the reported results were controversial.15-17 In the present study, we retrospectively evaluated the incidence of POD after propofol and sevoflurane-based anesthesia in elderly patients undergoing spine surgery.
Methods
This study was approved by the Institutional Review Board (IRB) of our hospital (no. 20-2020-14, date of approval: February 26, 2020), and the requirement for written informed consent was waived by the IRB. This study was conducted in compliance with the Declaration of Helsinki. Elderly patients ≥ 65 years of age who underwent spine surgery under total intravenous anesthesia with propofol or inhalational anesthesia with sevoflurane between January 2015 and December 2019 were retrospectively identified using the electronic medical records from our hospital without an a priori sample size calculation. Patients with preoperative delirium, a history of dementia, psychiatric disease, alcoholism, hepatic or renal dysfunction, requirement for postoperative mechanical ventilation, a history of surgery within the recent six months, or maintenance of anesthesia with combined anesthetics (propofol and sevoflurane) were excluded. Patients with incomplete medical records were also excluded.
At our institution, no premedication was administered to patients undergoing spine surgery. Anesthesia was maintained using total intravenous anesthesia with propofol or inhalational anesthesia with sevoflurane. The choice of drug for maintaining anesthesia was decided based on the personal preference of anesthesiologists, except for the case that intraoperative neurophysiological monitoring was performed. In this situation, total venous anesthesia was provided using propofol. Intraoperative analgesia was administered by continuous infusion of remifentanil or intermittent bolus injection of fentanyl. Anesthetic depth was maintained using the bispectral index between 40 and 60. Anesthesiologists of our institution usually decreased the dose of propofol and discontinued the infusion of it under the guidance of the bispectral index before the end of surgery earlier compared with sevoflurane, because longer times from sedation stop to awake are needed in total intravenous anesthesia with propofol than inhalation anesthesia with sevoflurane. An intravenous patient-controlled analgesia device with fentanyl was connected to the patients at the end of the surgery.
Patient characteristics, including age, sex, body mass index, American Society of Anesthesiologists (ASA) physical status, smoking, and comorbidities, were recorded. Perioperative data included the type of surgery, type of admission (elective or emergency), duration of surgery and anesthesia, drugs used for the maintenance of anesthesia (propofol or sevoflurane), intraoperative bispectral index, occurrence of hypotension, estimated blood loss, amount of infused fluids, perioperative transfusion (intraoperative and postoperative), perioperative pain scores (numerical rating scale ranging from 0 to 10), rescue use of opioids for analgesia during the first three days, POD, postoperative 30-day complications and length of postoperative hospital stay. Hypotension was defined as a systolic arterial pressure of <90 mmHg or decrease in the mean arterial pressure of 20% from the baseline value. Postoperative 30-day complications included cardiovascular events (angina and myocardial infarction), cerebrovascular events (transient ischemic attack and stroke), respiratory events (pneumonia), thromboembolic events (deep vein thrombosis and pulmonary embolism), acute kidney injury, and infection. Occurrence of POD during the hospital stay was assessed based on the review of electronic medical records. At our institution, POD was regularly screened by the attending nurses based on delirium characteristics of the Nursing Delirium Screening Scale (disorientation, inappropriate behavior, inappropriate communication, hallucination, and psychomotor retardation) during the hospital stay. 18 If at least one or more features of five characteristics were observed in the Nursing Delirium Screening Scale, the patient was consulted to a psychiatrist for proper diagnosis and management. We defined POD according to the diagnosis by psychiatrist.
The primary outcome was the incidence of POD after propofol or sevoflurane-based anesthesia. Secondary outcomes included postoperative 30-day complications, length of postoperative hospital stay, association of patient characteristics, and surgery- and anesthesia-related data with the development of POD, and the association between anesthetics and clinical outcomes, such as the incidence of postoperative 30-day complications, and length of postoperative hospital stay.
Statistical analysis was performed using the Statistical Package for the Social Sciences (version 26; IBM Inc., Armonk, NY) and R (version 4.0.3; Foundation for Statistical Computing, Vienna, Austria, http://www.r-project.org/) software. Data normality was tested using the Shapiro–Wilk test. Continuous data are expressed as mean ± standard deviation (SD), and categorical data as numbers (%). Categorical variables were analyzed using the chi-square or Fisher’s exact test, and continuous variables were analyzed using the Student t-test or Mann-Whitney U test. Univariable and multivariable logistic regression analyses were performed to analyze the risk factors of POD. All covariates with P-value of <.1, including age, ASA physical status, diabetes mellitus, postoperative pain scores, and postoperative rescue use of opioids and drugs for the maintenance of anesthesia, were entered into backward logistic regression model for analyzing the incidence of POD by the multivariable analysis. With respect to secondary outcomes, a univariable logistic or linear regression analysis was used to determine the association of anesthetic agents with the incidence of 30 days complications and length of postoperative hospital stay. The multivariable analysis using backward variable selection method with anesthetic agents forced into the model was conducted, for adjustment to avoid confounding effects, and all covariates with the P-value of <.1 were included in the univariable analysis. Statistical significance was set at P < .05.
Results
Of the total 1038 patients who underwent spine surgery between January 2015 and December 2019, 501 patients were excluded as they were <65 years of age, and 130 patients were excluded because they did not meet the inclusion criteria. Of the remaining 407 patients, 216 underwent spine surgery under total intravenous anesthesia with propofol and 191 patients under inhalational anesthesia with sevoflurane. Subsequently, 75 patients in the propofol group and 51 patients in the sevoflurane group were excluded owing to incomplete medical records. Finally, 141 patients in the propofol group and 140 patients in the sevoflurane group were analyzed (Figure 1). Flow diagram of medical records identified and reviewed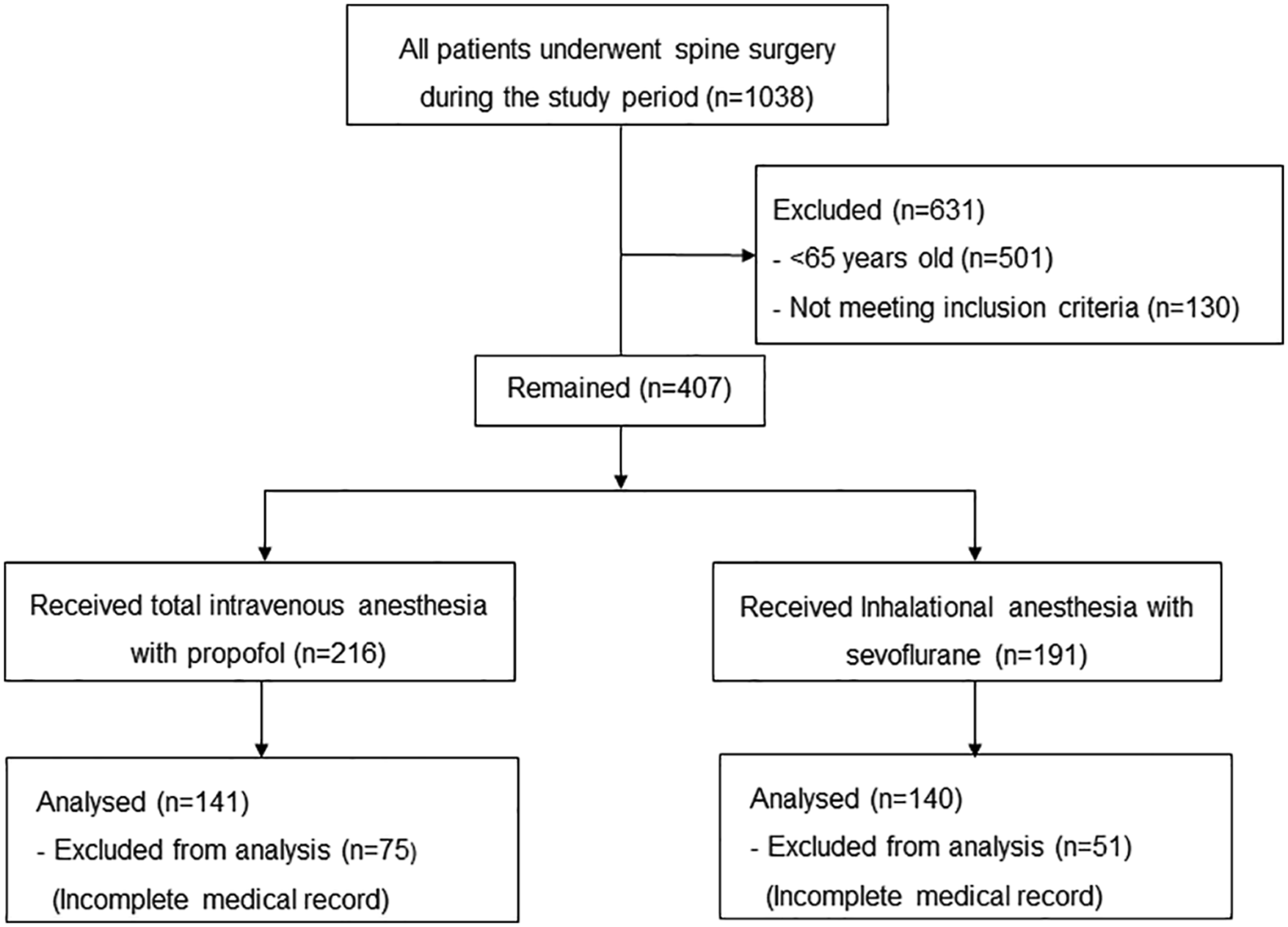
Patient characteristics
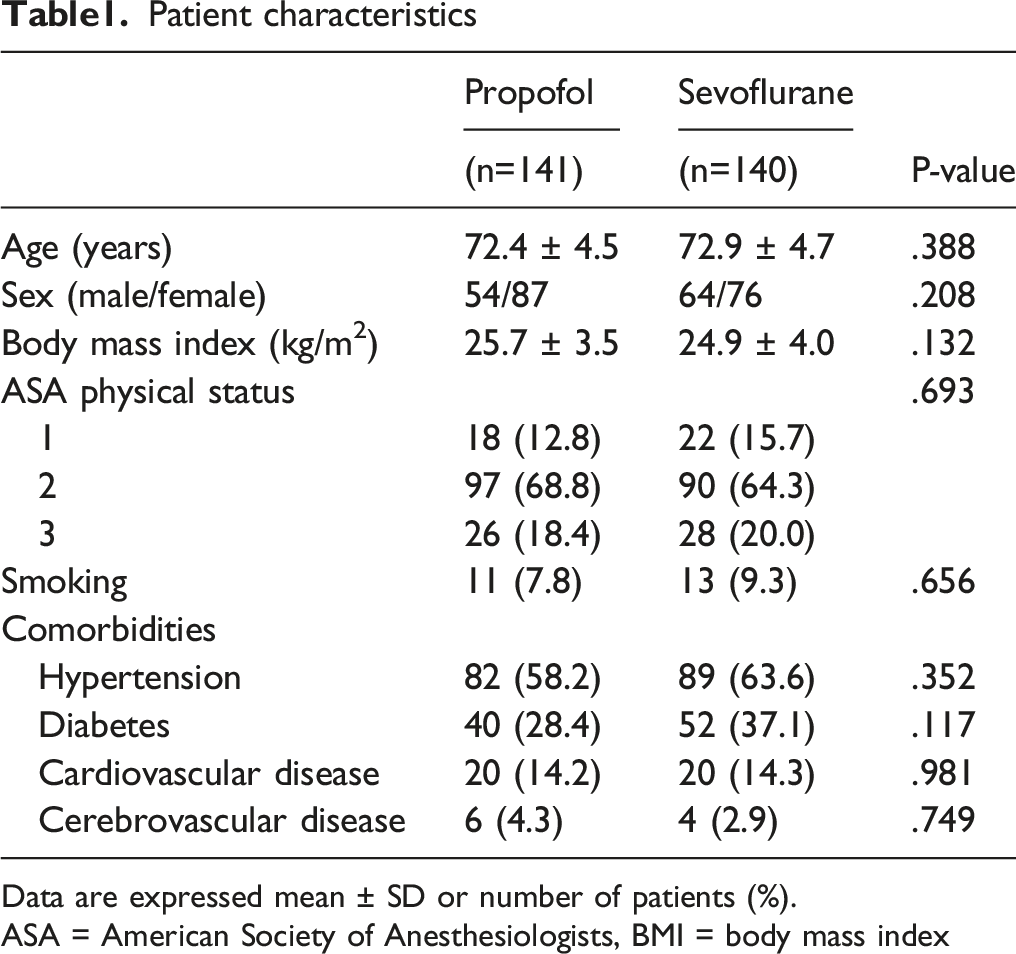
Data are expressed mean ± SD or number of patients (%).
ASA = American Society of Anesthesiologists, BMI = body mass index
Data related to surgery and anesthesia
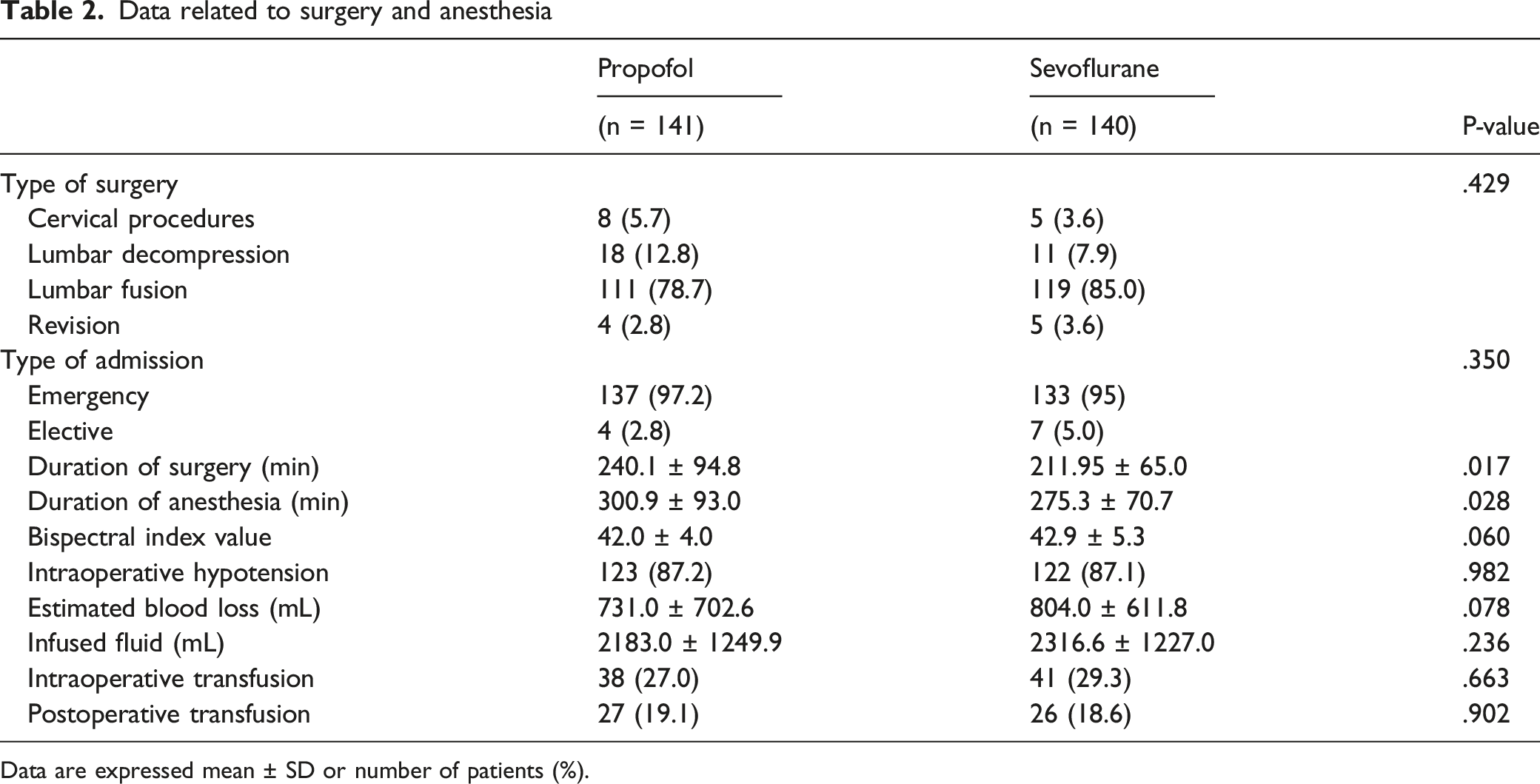
Data are expressed mean ± SD or number of patients (%).
Postoperative data
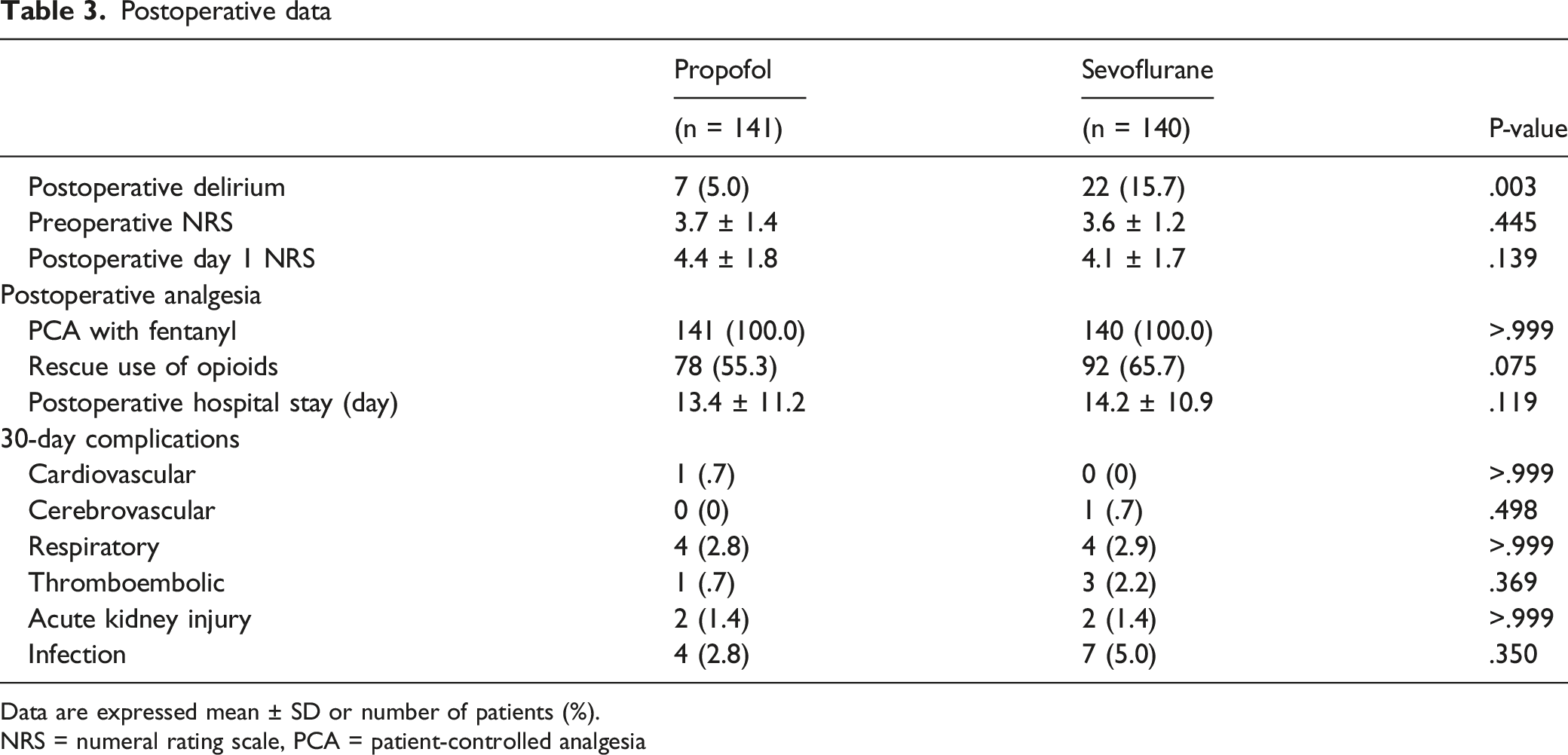
Data are expressed mean ± SD or number of patients (%).
NRS = numeral rating scale, PCA = patient-controlled analgesia
Univariable and multivariable logistic regression analyses of risk factors for postoperative delirium
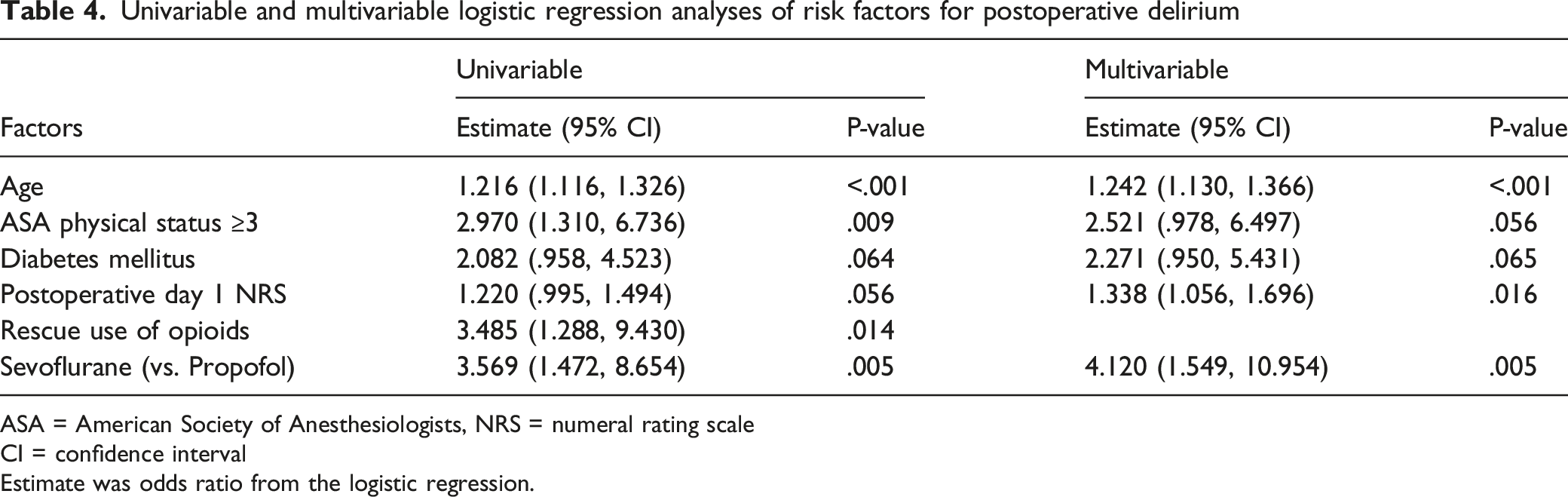
ASA = American Society of Anesthesiologists, NRS = numeral rating scale
CI = confidence interval
Estimate was odds ratio from the logistic regression.
Association between anesthetics with the length of postoperative hospital stay and postoperative 30-day complications
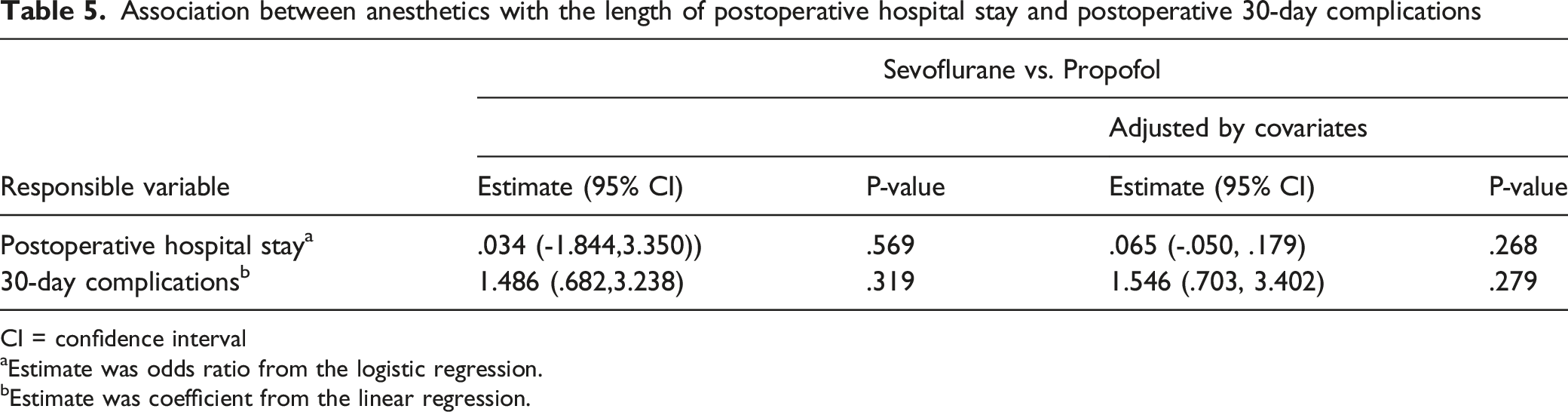
CI = confidence interval
aEstimate was odds ratio from the logistic regression.
bEstimate was coefficient from the linear regression.
Univariable and multivariable logistic regression analyses with adjustment for potential confounders showed that the type of anesthetics was also not associated with 30-day complications (P=.319 and P=.279, respectively)
Discussion
This study demonstrated that propofol-based general anesthesia is associated with a lower occurrence of POD when compared with sevoflurane-based general anesthesia in elderly patients undergoing spine surgery.
Elderly patients are at increased risk of POD after major surgery. 3 Spine surgery is one of the most commonly performed surgeries in elderly patients. 19 Our results showed that the overall incidence of POD after spine surgery was 10.3%, which are consistent with the reported incidence of POD between 4% and 41% in elderly patients after spine surgery.1,2 This study revealed that POD developed in 5% cases in the propofol group and 15.7% cases in the sevoflurane group, which is comparable with a study reporting that propofol produced less effect on the occurrence of POD than sevoflurane in elderly patients undergoing gastrointestinal surgery (6.9% vs 26.7%, respectively). 15 However, a study involving elderly patients who underwent laparoscopic surgeries showed that the incidence of POD was not different between propofol- and sevoflurane-based anesthesia. 16 Furthermore, a study involving elderly patients who underwent total hip or knee replacements reported that the incidence of POD was not different between propofol and sevoflurane anesthesia, although days of POD were higher with propofol anesthesia than with sevoflurane anesthesia 17 . However, the authors in the latter two studies mentioned that their studies were not powered to detect a difference in POD between propofol and sevoflurane anesthesia.16,17
The development of POD is associated with various factors, such as age, physical status, diabetes mellitus, preoperative cognitive function, intraoperative blood loss and transfusion, electrolyte disorder, perioperative pain, and duration of surgery.1,4,20 This study demonstrated that the risk of POD was increased with age, postoperative pain, and the use of sevoflurane. Among elderly patients, the higher incidence of POD may be attributed to impaired physiologic compensatory capability against stress, changed production of central neurotransmitters, decreased brain volume, and decreased oxygen supply to the brain caused by the narrowing of vessels or impaired blood pressure regulation, and increased comorbidities.4,20-22 Furthermore, pain induces a pro-inflammatory response and a disturbance of central cholinergic activity,23,24 which is similar with a mechanism of delirium. 3 This supports that pain may decrease the threshold of the development of delirium and contribute to development of delirium. 25 Although old age is a non-modifiable risk factor, recognizing it as a risk factor may contribute to the timely management of POD by early diagnosis. In addition, changes in modifiable risk factors, such as pain and anesthetic agents, could help reduce the incidence of POD. However, larger prospective studies are needed to consolidate the findings of this study and provide strong clinical evidence.
Although the mechanisms underlying the lower occurrence of POD after propofol anesthesia are unclear, they may include the followings: first, emotional stress and quality of recovery may affect the occurrence of POD. Propofol anesthesia provides a greater comfort to patients than sevoflurane anesthesia, which may contribute to a lower incidence of POD in propofol anesthesia compared to sevoflurane anesthesia. Propofol produces less postoperative nausea and vomiting, a better sense of well-being, and a better quality of postoperative recovery.26-28 According to the previous studies, the emotional state, which was evaluated using psychometric test, was significantly better after propofol-based anesthesia than sevoflurane-based anesthesia, 27 and the quality of recovery, including physical comfort, emotional state, physical independence, psychological support, and pain, was also significantly greater in the propofol group than in the sevoflurane group. 28 Second, although the pathophysiology and mechanism of POD have not yet been clearly determined, anti-inflammatory and anti-apoptotic properties of propofol may contribute to the lower incidence of POD compared with sevoflurane. Sevoflurane and propofol may exhibit different modulations in neuroinflammation and neuropathogenesis. Sevoflurane exerts expression of pro-inflammatory cytokines and neuropathogenesis of Alzheimer’s disease by inducing apoptosis and accumulation of beta-amyloid protein.9-11 Further, propofol may reduce inflammation and apoptosis, and even attenuate the neurotoxic effect provoked by sevoflurane.10,12 However, neuroprotective effect against ischemic brain injury, such as preconditioning potential in sevoflurane7,8 and neurotoxic effect in developing brain regarding propofol,13,14 have also been reported.
Postoperative cognitive dysfunction (POCD) is one of the cognitive disorders occurred after surgery and anesthesia. 6 According to a previous study. 29 propofol-based general anesthesia decreased the incidence of POCD when compared with sevoflurane-based anesthesia in elderly patients undergoing major cancer surgery. Currently, it is unclear whether POD and POCD are different diseases with distinct pathophysiologies or overlapping states on a continuum of impairments in brain function.30,31 However, clinical studies suggested that POD could be related to persistent neurocognitive deficit32,33 and increased risk of dementia.34,35 Therefore, further research is needed to elucidate the mechanism of POD and its correlation with cognitive dysfunction. If a definite correlation between POD and POCD exists, active intervention for the prevention of POD may contribute to reduce the occurrence of neurocognitive dysfunction after surgery.
This study has several limitations. First, this was a retrospective study based on a review of medical records. Although POD was assessed using a standardized tool, the Nursing Delirium Screening Scale, the details and severity of delirium could not be precisely evaluated through the medical records. In particular, hypoactive delirium or less severe delirium could have been neglected. Therefore, the incidence of POD may have been underestimated. Second, this was a single-center study involving elderly patients undergoing spine surgery. Third, medical records were retrospectively reviewed following a standardized protocol. However, potential selection bias and confounding factors could not be eliminated owing to unidentified variables such as preoperative cognitive function, or emergence time after anesthesia.
In conclusion, Propofol-based anesthesia was associated with a lower incidence of POD than sevoflurane-based anesthesia in elderly patients after spine surgery. In addition, older age, even among elderly patients, and higher mean pain score at postoperative day 1 were associated with the development of POD. Large-scale prospective studies are required to confirm whether propofol-based anesthesia reduces the occurrence of POD, compared with sevoflurane-based anesthesia.
Footnotes
Author Contributions
Jee-Eun Chang and Seong-Won Min contributed equally to this study and share the role of first author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.