
Abstract
Study Design:
Retrospective cohort study.
Objective:
To report the clinical and radiological outcomes for screw track augmentation with fibular allograft in revision of loose pedicle screws associated with significant bone loss along the screw track.
Methods:
Thirty consecutive patients, 18 men (60%) and 12 women (40%), with a mean age 52 years (range 34- 68). Fibular allograft was prepared by cutting it into longitudinal strips 50 mm in length. Three allograft struts were inserted into the screw track. Six mm tap used to tap between the 3 fibular struts. Eight- or 9-mm diameter, and 45 or 50 mm in length screw was then inserted. The clinical outcomes were assessed by means of the Oswestry Disability Index (ODI), and visual analog scale (VAS) for back and leg pain for clinical outcome. Computed tomography scan (CT) performed at 12 months postoperative visit to assess fibular graft incorporation along the pedicle screw track, any screw loosening and the interbody as well as posterolateral fusion.
Results:
At a mean follow up of 29 months, there were statically significant improvement in the ODI and VAS for back and leg pain. CT scan obtained at last follow-up showed incorporation of fibular allograft and solid fusion in all patients except one.
Conclusion:
The fibular allograft augmentation of the pedicle screw track in revision of loose pedicle screws associated with significant bone loss is a viable option. It allows for biologic fixation at the screw-bone interface and has some key advantages when compared to currently available methods.
Introduction
Pedicle screw fixation has become the most commonly used method of posterior spinal instrumentation as it provides robust, 3-column fixation and does not require intact posterior element. 1 Despite the well-published success of pedicle screw construct, revision fixation is occasionally required, most commonly in cases of pseudoarthrosis. 2
In the setting of revision surgery, a variable amount of pedicle bone loss may be present. This is the result of screw loosening and subsequent screw track widening due to “windshield-wiper effect” of the loose screw.
Further, the bone quality may be poor secondary to osteoporosis, malnutrition, previous infection or smoking. In these difficult cases, multiple techniques have been utilized to enhance the construct strength. Current options for revision pedicle screw fixation include cement augmented screw fixation, cannulated-fenestrated or expandable pedicle screws, and custom-made large diameter screws. Cement augmented pedicle screw fixation is associated with several risks, mostly related to extravasation of cement.3,4 Custom-made large diameters screws are costly and are not readily available because they need to be manufactured prior to surgery.
To authors’ best of knowledge, using fibular allograft in the setting of revision pedicle screw fixation has not previously been reported. The purpose of the current study was to report this technique, assess the clinical and radiological outcomes.
Methods
After obtaining institutional review board approval (University of Toledo Protocol Number: 202449-UT), a retrospective database review of prospectively collected data was performed to identify patients that had revision lumbar spine surgery performed over a 5 year period (January 2014- December 2019) by the senior author at an academic medical center. Patient informed consent was exempt due to the retrospective nature of the current study. Inclusion criteria were patients at least 18 years of age at the time of surgery, revision lumbar spine surgery for aseptic pseudoarthrosis with loose pedicle screws associated with significant bone loss along the screw track due to windshield-wiper effect of the loose screw and a minimum of 12 months of follow up. Exclusion criteria were patients with infection, trauma, and tumor. Thirty consecutive patients had pedicle screw track augmentation with fibular allograft during revision of loose pedicle screws that were associated with significant bone loss along the screw track seen in preoperative CT scan and confirmed during surgery after removal of the screws.
Significant bone loss was identified by the authors as a marked halo around the screw track seen in preoperative CT scan coronal, sagittal and axial views. In addition to intraoperative assessment where after removal of the loose screw, the largest screw diameter in the authors’ institution, which is 9 mm, did not have adequate purchase when inserted in the screw track.
Baseline patient and procedure characteristics that were assessed included age, gender, body mass index (BMI), tobacco use, medical comorbidities such as diabetes, renal disease, chronic obstructive pulmonary disease (COPD), coronary artery disease (CAD) and treatments prescribed prior to the index revision surgery. All patients included in the current study had preoperative computed tomography (CT) or CT myelogram confirmed pseudoarthrosis and bone loss along one or more pedicle screw tracks seen as marked radiolucency along the screw track in the coronal, axial and sagittal images (Figures 1 and 2). Preoperative erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) as well as intraoperative cultures were obtained to rule out infection as the cause of pseudoarthrosis. Preoperative evaluation also included Vitamin D level to rule out deficiency as well as albumin and transferrin to assess nutrition state.
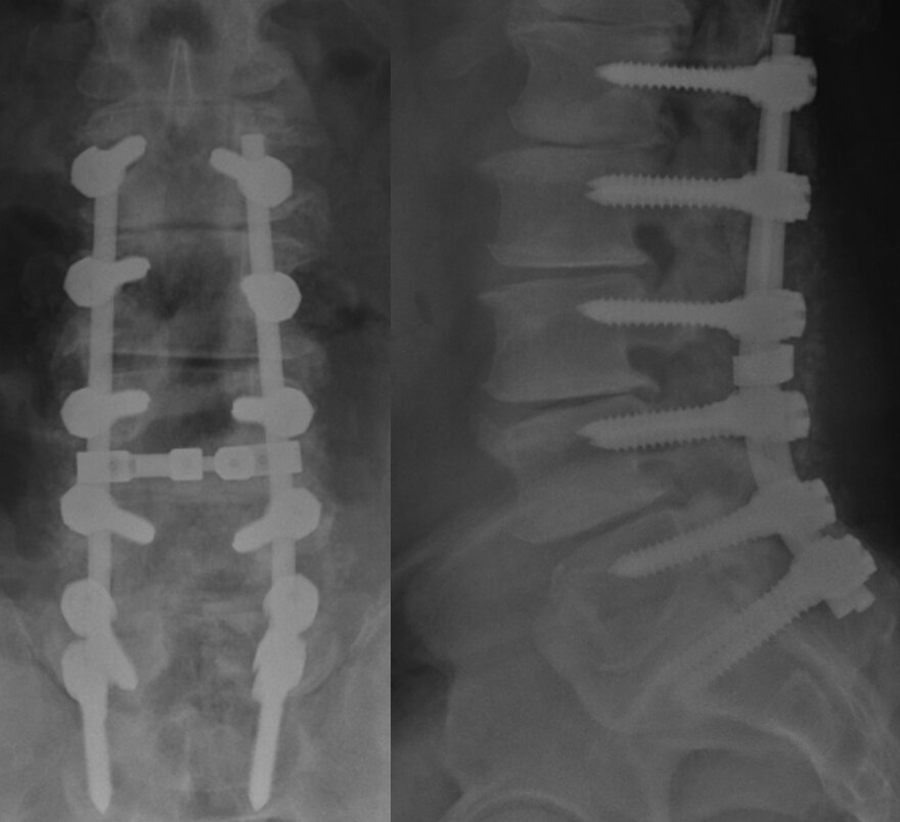
59 years male diabetic patient presented with severe low back pain, preoperative anteroposterior and lateral views showed L1-S1 instrumentation, no posterolateral fusion mass or interbody fusion.
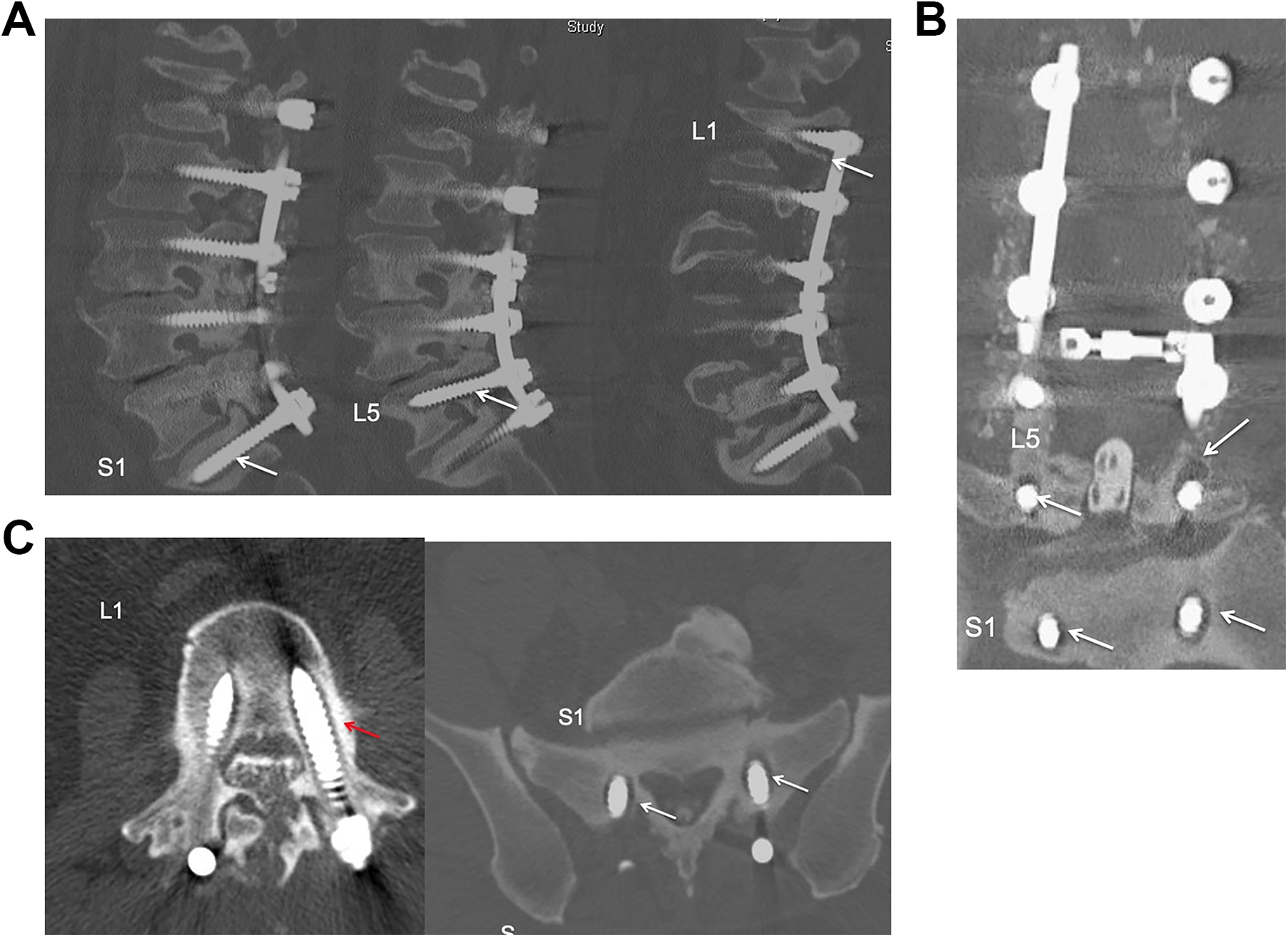
Preoperative CT myelogram sagittal (A), coronal (B) and axial (C) views showed loose S1, L5 and L1 screws (arrows).
Clinical outcome by means of the Oswestry Disability Index (ODI), and visual analog scale (VAS) for back and leg pain were completed by patients preoperatively and at the last follow up.5,6 An independent senior musculoskeletal radiologist reviewed standing anteroposterior and lateral radiographs and CT scans performed at 12 months postoperative visit. Radiographic assessment included fibular graft incorporation along the pedicle screw track, any screw loosening and the fusion. Posterolateral fusions were evaluated as described by Lenke and colleagues, 7 grade A, definitely solid with bilateral stout fusion masses present; Grade B, probably solid with a unilateral stout fusion mass and a contralateral thin fusion mass; Grade C, probably not solid with a thin unilateral fusion mass and a probable pseudarthrosis on the contralateral side; and Grade D, definitely not solid with thin fusion masses bilaterally with obvious pseudarthrosis or bone graft dissolution bilaterally. Following convention, Grades A and B were considered fused, and Grades C and D were considered not fused. Overall fusion ratings were based on assessment of all levels treated, where the lowest rating at any individual level was considered the overall rating.
Surgical Technique
A standard midline lumbar approach was utilized. After hardware removal, a stat gram stain as well as intraoperative cultures were taken to rule out infection. The screw track that was identified to have marked loosening in the preoperative CT scan, was then assessed to confirm the bone loss. An upbiting curette and pituitary rounger were used for screw track debridement removing any soft tissue down to bone. Attention was particularly paid to assess for screw track medial wall deficiency in preoperative CT coronal and axial cuts. In case of identified medial wall deficiency, care was taken in medial wall debridement to avoid any dural tear or nerve root injury.
Fibular allograft, which is readily available prepacked in the freezer at the authors’ institution, was thawed at room temperature and then prepared by cutting it into longitudinal strips 50 mm in length. An oscillating saw was used to cut the graft while holding it with towel clips (Figure 3). Three allograft struts were inserted into the screw track allowing for overhang outside the screw track to avoid any anterior graft migration during screw insertion. Six mm tap was then used to tap between the 3 fibular struts to create a channel for pedicle screw insertion. Eight or 9 mm diameter, and 45 or 50 mm in length screw was then inserted under lateral fluoroscopic guidance. After complete insertion of the pedicle screw, the overhang part of the fibular allograft was trimmed. The remainder of the revision instrumentation and fusion procedure was completed in standard fashion using a mixture of iliac crest bone autograft as well as crush cancellous allograft (Figures 4).

An oscillating saw was used to cut the graft while holding it with towel clips.
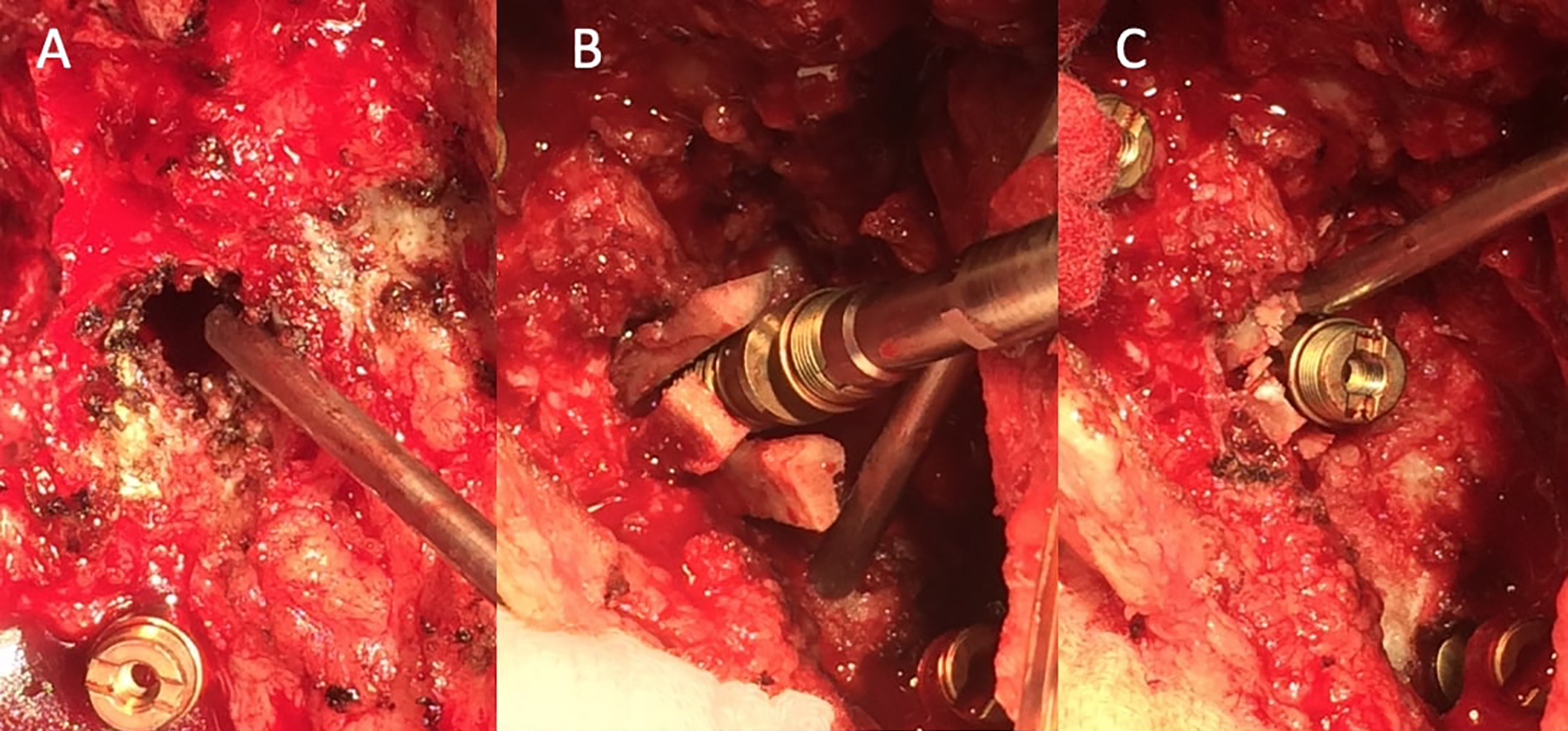
Intraoperative photograph after removal of a loose screw showed significant bone loss around the screw track (A). The 3 allograft fibular strips inserted into the screw track allowing for overhang outside the track to avoid any anterior graft migration during screw insertion (B). After complete insertion of the pedicle screw, the overhang part of the fibular allograft was trimmed (C).
In addition to revision instrumentation and posterolateral fusion the authors of the current study elected to perform transforaminal interbody fusion (TLIF) in some patients especially at L5-S1 to increase the fusion rate if the primary surgery did not include interbody fusion.
Postoperative Care
Mobilization with physical therapy postoperative day one. Prophylactic IV antibiotics for 24 hours. Prophylactic anticoagulation starting first postoperative day and continue while in the hospital. Vitamin D replacement if preoperative assessment confirmed vitamin D deficiency and nutritional supplement if malnourished as assessed by preoperative albumin and transferrin.
Statistical Analysis
Statistical analyses were performed using SPSS 11.0 for windows. Data is shown as mean ± SEM. Student t test was used for the comparison of continuous variables. Fisher’s exact test was used to evaluate the differences of clinical outcomes and fusion rate between the 2 groups. P values below 0.05 were accepted for significance.
Results
Thirty consecutive patients, 18 men (60%) and 12 women (40%), with a mean age 52 years (range 34- 68) at the time of index procedure. The average length of follow up was 29 months (24-61). All patients presented with leg and back pain with history of previous lumbar spine instrumentation and fusion. Computed tomography scan or CT myelogram confirmed pseudoarthrosis in all patient with screws loosening and screw track widening due to windshield-wiper effect. Preoperative ESR and CRP were within normal limits and intraoperative cultures were negative in all patients ruling out infection as the cause of pseudoarthrosis.
All the patients included in the current study had multiple medical comorbidities including overweight-morbidly obese, BMI ≥ 25 (90%), vitamin D deficiency (85%), hypertension (74%) smoking (65%), diabetic (57%), chronic obstructive pulmonary disease (50%), and coronary artery disease (40%).
At a mean follow up of 29 months (12-60), there were statically significant improvement in the ODI and VAS for back and leg pain. The mean ODI score improved from 51 (range, 27–79) preoperatively, to 24 (range, 0–51) at the last follow up (P < 0.05). The mean leg pain VAS decreased from a preoperative score of 75 (range, 42–100) to 41 (range, 5–70) at the last follow up (P < 0.05). The mean back pain VAS decreased from a preoperative score of 68 (range, 45–100) to 33 (range, 2–68) at the last follow-up (P < 0.05).
Radiographic Assessment of Fusion
CT scan obtained at last follow-up showed incorporation of fibular allograft and
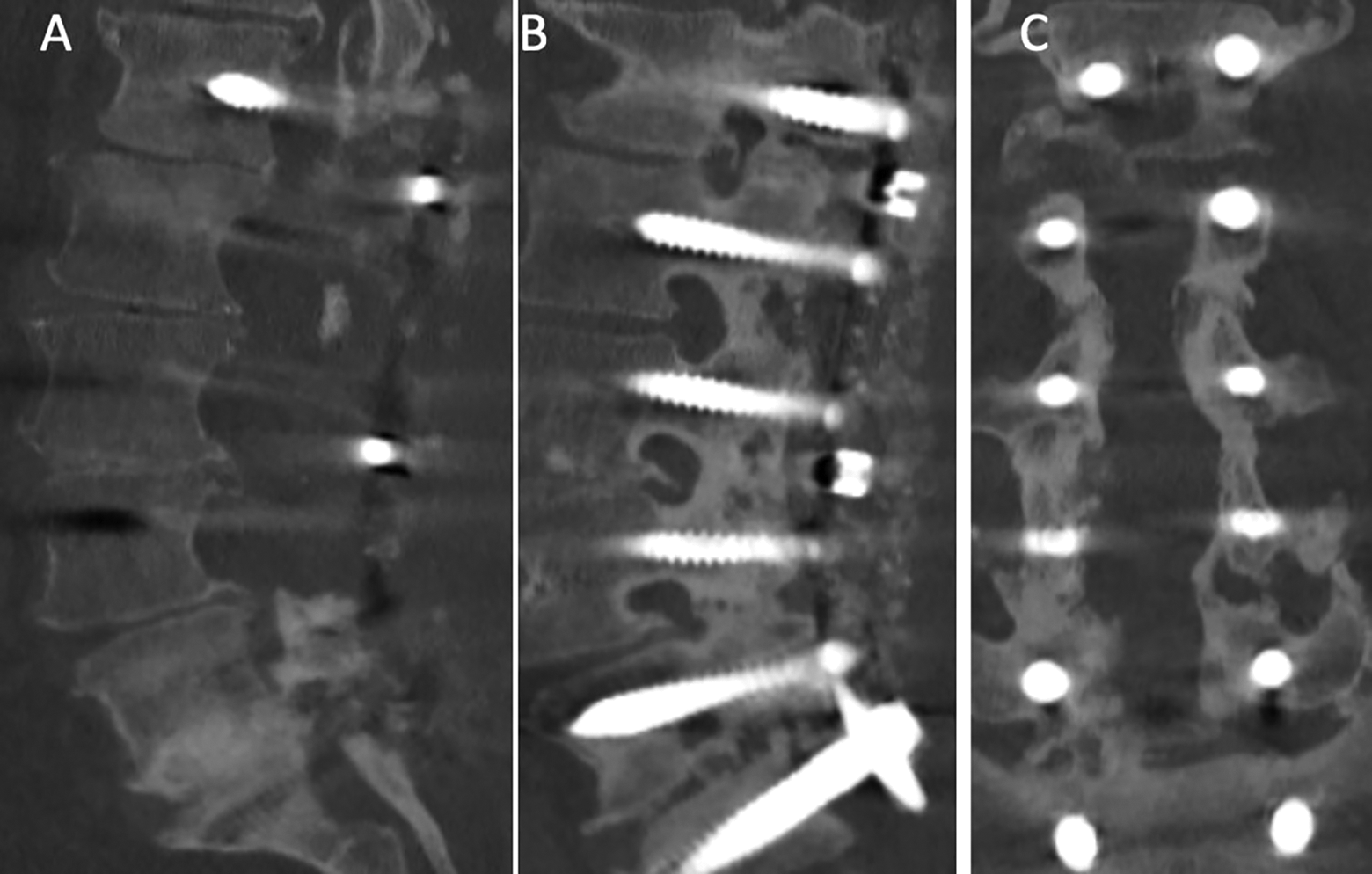
Two years follow up CT scan sagittal (A-B) and coronal (C) views showed solid interbody fusion at L5-S1 with incorporation of the allograft along the L5 and S1 screw tracks.
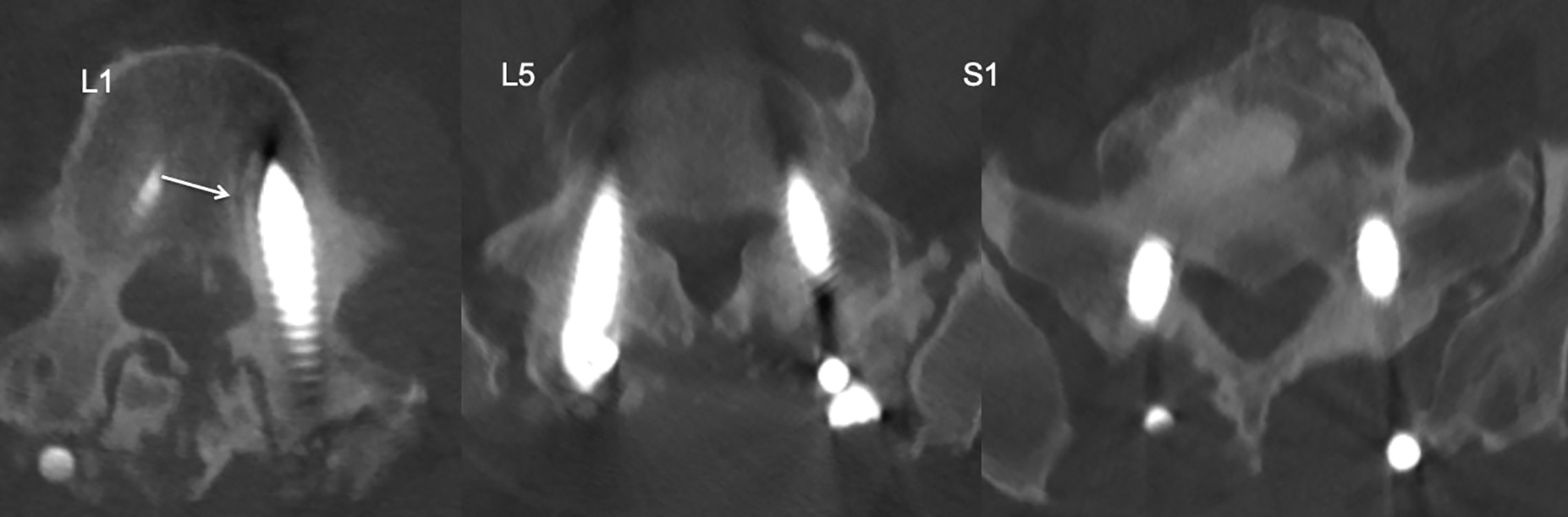
Two years follow up CT scan axial views showed incorporation of the allograft along L1, L5 and S1 screw tracks.
Complications and Return to Operating Room
48-year-old male patient smoker required reoperation for proximal junctional kyphosis and pseudoarthrosis. One patient had a surgical site infection that was treated with irrigation and debridement and intravenous antibiotic for 6 weeks.
Discussion
Pseudoarthrosis is one of the most common complications of lumbar spine surgery. It is a known cause of recurrent pain and disability after spinal fusion and is one of the most common indications for revision lumbar surgery.8,9 During lumbar spine revision surgery for pseudoarthrosis a variable amount of pedicle bone loss may be encountered. This is the result of screw loosening and subsequent screw track widening due to windshield-wiper effect of the loose screw. The bone loss along the screw track can be significant and identified in the preoperative CT scan and confirmed during surgery after screw removal. The largest pedicle screw diameter available in the tray depends on the vendor. When significant bone loss along the screw track is encountered, adequate screw purchase cannot be obtained with regularly available screws.
There are a variety of options and techniques described for enhancing or augmenting pedicle screw fixation. Options include custom made large diameter screws, cannulated-fenestrated screws, and cement augmented pedicle screws. There are some shortcomings with currently available techniques. Custom made screws have been proposed as one of the options when screw tract diameter exceeds the dimension of standardly available screws. Huang et al, 10 described many limitations of this technique. First, significant cost is associated with custom made screws. In contrast, the cost of one unit of fibular allograft in the authors’ institution is 570 USD, though prices may vary between centers. In addition, these screws must be ordered preoperatively which requires additional time. The aforementioned authors reported approximately 4 weeks delay to allow for screw manufacturing. Furthermore, if tapping is required, a custom-made tap must be manufactured in conjunction with the custom screws, which further limits their utility. Clearly this method of revision fixation cannot be used “on-the-spot” while in the operating room. In contrast, the fibular allograft technique is not only cost effective, but it does not require specialized equipment for insertion or pre-order as it is available in the operative room in the majority of hospital for use in orthopedic trauma and reconstructive surgery.
Cement use has been widely supported due to its success in increasing the pullout strength of pedicle screws. Some authors have described it as the “gold standard” for enhancing fixation in osteoporotic spines due to evidence that the enhanced fixation strength is proportionately greater in osteoporotic bone.11-13 However, in a recent study of 165 patients, Janssen et al, 3 reported a 5.5% symptomatic complication rate including pulmonary cement embolism, intraoperative cement anaphylaxis and epidural cement leakage requiring revision surgery. They recommend strict indications and careful patient selection when using this method in order to reduce adverse side effects.
Fenestrated screws are another option used in the setting of revision pedicle fixation. These screws are designed to confine the cement to the vertebral body. These specialty screws may decrease intraspinal cement extrusion, improving the safety of this technique in comparison to standard cement augmentation techniques. However, cement extravasation has still been frequently described despite these improvements.12-15
There are alternative options for revision interventions in these cases. Some spine surgeons may choose to perform ventral fusion and fixation. Others may use the lateral access approach to perform interbody fusion (XLIF). These approaches avoid revision of the entire structure from the back and ensures reliable interbody fusion.
The goals of revision lumbar spine surgery are decompression, stabilization and balancing the sagittal and coronal alignment. The rational for using the interbody fusion in such cases are to improve the fusion rate, increase the neuroforaminal height to improve the foraminal stenosis and in some patient to correct the sagittal and coronal imbalance. Approaching the disc to perform the interbody fusion can be achieved from the back, front or lateral. Each approach has its pros and cons and inherent complications. In addition to revision instrumentation and posterolateral fusion the authors of the current study elected to perform transforaminal interbody fusion (TLIF) in some patients especially at L5-S1 to increase the fusion rate, if the primary surgery did not include interbody fusion.
Pedicle screw track augmentation with fibular allograft as described in the current study is a novel technique with encouraging clinical and radiological results. It allows for biological fixation with the allograft incorporation and has several advantages when compared to currently available methods. The reported technique avoids the complications associated with cement augmented pedicle screws, while achieving screw stability. In addition, it can be used impromptu, when other options are not immediately available. This technique can be employed without specialized instrumentation at significant cost savings when compared to custom made screws.
The limitations of the current study include a retrospective study, a single surgeon series and lack of biomechanical data supporting the results. Literature review showed there was only one report of a biomechanical study using cannulated allograft bone plugs in association with pedicle screws. This was a cadaveric model published by Chrea et al, 16 in which the authors concluded there was no difference in average pullout strength when comparing augmented and non-augmented screws. However, a cadaveric study is limited by the fact that an in vitro model does not account for biologic fixation which may increase with time as a result of graft incorporation.
Conclusion
The fibular allograft technique is a viable option in the setting of revision pedicle screw fixation when significant bone loss is encountered along the screw track. It has several advantages when compared to currently available methods. It can be used impromptu without specialized instrumentation. Future studies are warranted to quantify biomechanical pullout strength and a larger clinical sample size, and a randomized trial would offer more definitive results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.