
Abstract
Study Design
Retrospective Analysis
Background
Venous thromboembolism (VTE) represents a significant cause of morbidity and mortality in major spine surgery. Placement of prophylactic inferior vena cava filters (IVCF) in patients undergoing major spine surgery was previously adopted at our institution. This study reports our experience and compares VTE rates between patients with and without preoperative IVCF placement.
Methods
A Retrospective comparative study was conducted on adult patients who underwent IVCF placement and those who did not prior to their spinal fusion procedure, between 2013 and 2016. Thoracolumbar fusions (anterior and/or posterior) of 7 or more levels, spinal osteotomies, and a minimum of a 3-month follow-up were included. Traumatic, oncologic, and cervical pathology were excluded. Primary outcomes measured included the incidence of overall VTE (DVT/PE), death, IVCF related complications, and IVCF retrieval.
Results
386 patients who underwent major spine surgery, 258 met the eligibility criteria. Of those patients, 105 patients (40.7%) had prophylactic IVCF placement. All patients had postoperative SCDs and chemoprophylaxis. The presence of an IVCF was associated with an increased rate of overall VTE (14.3% vs 6.5%, P ≤ .05) and DVT episodes (8.6% vs 2.6%, P = .04). The rate of PE for the IVCF group and non-IVCF group was 8.6% and 4.6%, respectively, which was not statistically significant (P = .32). The all-cause mortality rate overall of 2.3% was statistically similar between both groups (P = 1.0). The IVCF group had higher rates of hematoma/seroma vs the non-IVCF group (12.4% vs 3.9%, P ≤ .05). 99 IVCFs were retrievable designs, and 85% were successfully retrieved. Overall IVCF-related complication rate was 11%.
Conclusions
No statistical difference in PE or mortality rates existed between the IVCF and the control group. Patients with IVCF placement experienced approximately twice the rate of VTE and three times the rate of DVT compared to those without IVCF. The IVCF-related complication rate was 11%. Based on the results of this study, the authors recommend against the routine use of prophylactic IVCFs in adults undergoing major spine surgery.
Level of Evidence
III.
Introduction
Venous thromboembolism (VTE) events, including deep venous thrombosis (DVT) and pulmonary embolism (PE), are well-documented causes of morbidity and mortality in orthopaedic surgery. 1 Increased VTE risk often is attributed to decreased mobilization postoperatively and in patients undergoing spine surgery, that is, due to direct manipulation of the large retroperitoneal veins in anterior approaches.2-5 A systematic review of the spine literature estimates the risk of postoperative DVT at approximately 2.1% and PE at .3%, but reported rates from individual studies vary widely. 6 A recent prospective study by the International Spine Study Group examined adult patients undergoing major deformity surgery and reported DVT and PE rates of 2.1% for both. 7
When considering VTE chemoprophylaxis, the surgeon must weigh risks of symptomatic VTE against the risk of neurologic injury from an epidural hematoma. Cain et al 8 found significant morbidity associated with therapeutic anticoagulation postoperatively. A survey of practicing spine surgeons found that epidural hematoma is perceived to be a substantial risk with chemoprophylaxis. 9 Given these findings, multiple studies have addressed placement of prophylactic inferior vena cava filters (IVCF) to prevent symptomatic PE.2,10-13 These studies generally support the efficacy and safety of prophylactic IVCF placement. Still, they are notably retrospective in nature, lack adequate controls, and are potentially underpowered. Further, complications directly associated with IVCF placement/retrieval are more common than previously thought and remain an area of active investigation.14-17
At our institution, prophylactic IVCF filter placement was implemented in a significant portion of patients undergoing major spine surgery. The aim of this retrospective study was 3-fold: (1) report rates of symptomatic postoperative VTE (DVT/PE) and mortality, (2) compare postoperative symptomatic VTE rate between patients with and without prophylactic IVCF, and (3) report IVCF related complications and retrieval rate.
Methods
After Institutional Review Board approval, the University of Pennsylvania Health System’s electronic medical record (EMR) (Epic System Corp., Verona, WI) was queried by CPT code for all patients who underwent “major spine surgery” between January 2013 and August 2016. Major spine surgery procedures included: anterior spine fusion (CPT codes 22558, 22585), instrumented posterior spinal fusion of seven or more contiguous levels (CPT codes 22802, 22804, 22843, 22844), or osteotomy for deformity correction (CPT codes 22212, 22212, 22206, 22207, 22208).
The electronic record of each patient was queried for associated VTE diagnoses after the date of surgery using ICD 9/10 codes for VTE, pulmonary embolism, and cardiac arrest. Inpatient orders were queried for tests associated with VTE diagnosis, including CT chest with contrast, duplex ultrasound of the lower extremity, ventilation-perfusion scan, and venogram. Inpatient orders were searched for initiation of VTE prophylaxis treatment modalities, including; sequential compression devices, TED stockings, unfractionated heparin, low molecular weight heparin, warfarin, aspirin, clopidogrel, ticagrelor, and rivaroxaban. Each subject’s record was searched for a CPT code associated with IVCF placement (CPT codes 37191, 37192, 37193).
Each chart was manually reviewed by independent observers to determine study eligibility and to extract data. Inclusion criteria included: age ≥18 years old at the time of surgery, preoperative medical/cardiology evaluation, intraoperative or immediate postoperative radiograph confirming the presence/absence of an IVCF, postoperative admission to the orthopaedic or neurosurgical service (2-day minimum), and a minimum of 3 months clinical follow-up with the attending surgeon. Exclusion criteria included: cervical surgery, acute spinal trauma, active spine infection, or spinal tumor. Eligible patients’ charts were systematically reviewed for demographic and clinical variables of interest, postoperative diagnosis of VTE, presence of IVCF on a perioperative radiograph, and IVCF-associated complications. Charts were examined for VTE risk factors, including history of VTE, cancer, or diagnosis of thrombophilia. Obesity and anterior spine surgery were not included as VTE risk factors but were collected independently. If the 3-month follow-up minimum was not met, the Social Security Death Index was queried to determine if they had died.
Demographic and clinical variables were reported with descriptive statistics. Univariate statistical analyses were conducted using Pearson’s chi-square test or Fisher’s exact test for categorical or binary variables, and Student’s t-test for continuous variables. A cutoff for significance, P ≤ .10, was used for entry into the multiple regression model. Using statistically significant variables from the univariate analysis and a backward likelihood ratio technique, a multivariate logistic regression model was formulated to determine the variables that were independent risk factors for VTE. Simpler models were generated from the original with continuous variables and compared against the more robust models using the −2 log-likelihood method. When the final model was derived, we performed an area under the curve test to assess the predictive power of the model. Statistics were calculated using SPSS (v 22.0 - SPSS Inc., Chicago, IL).
Results
The medical record query yielded 384 unique patients. 258 patients were eligible, and 126 were excluded: 77 for cervicothoracic surgery, 16 for acute spinal trauma, 6 for active infection, 7 for spinal tumor, 13 cases were deemed not “major spine surgery,” and 7 cases for inadequate follow-up. No patients lost to follow up died according to the Social Security Death Index. There was no missing data for all 258 included patients.
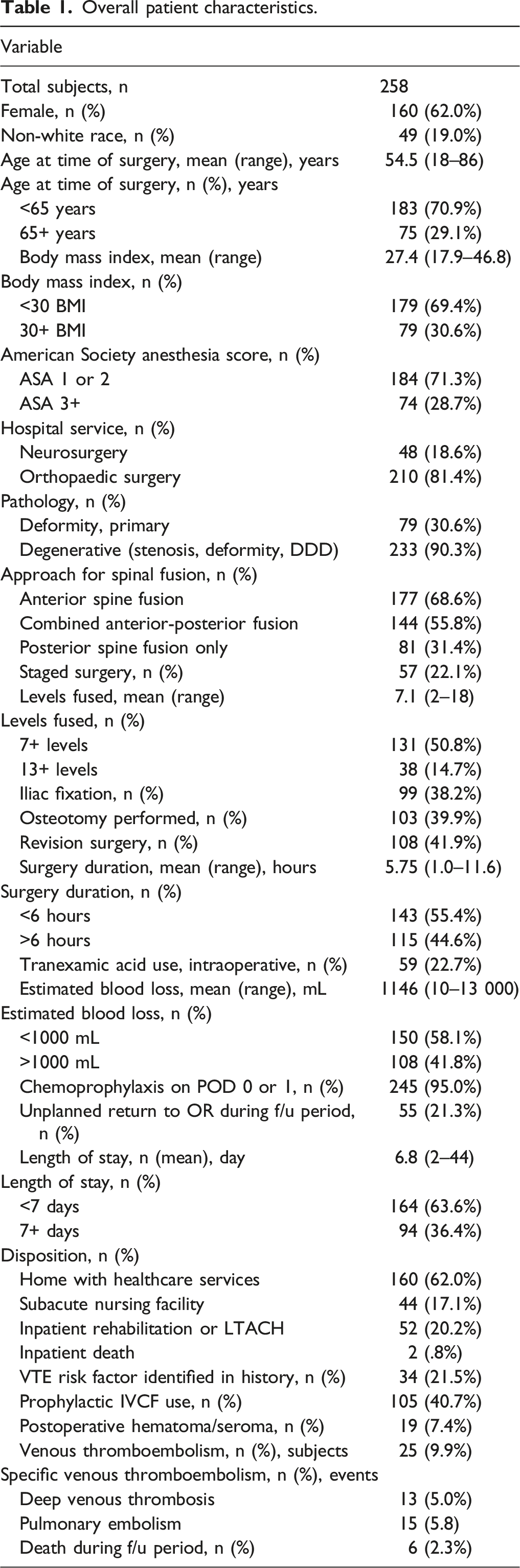
Overall patient characteristics.
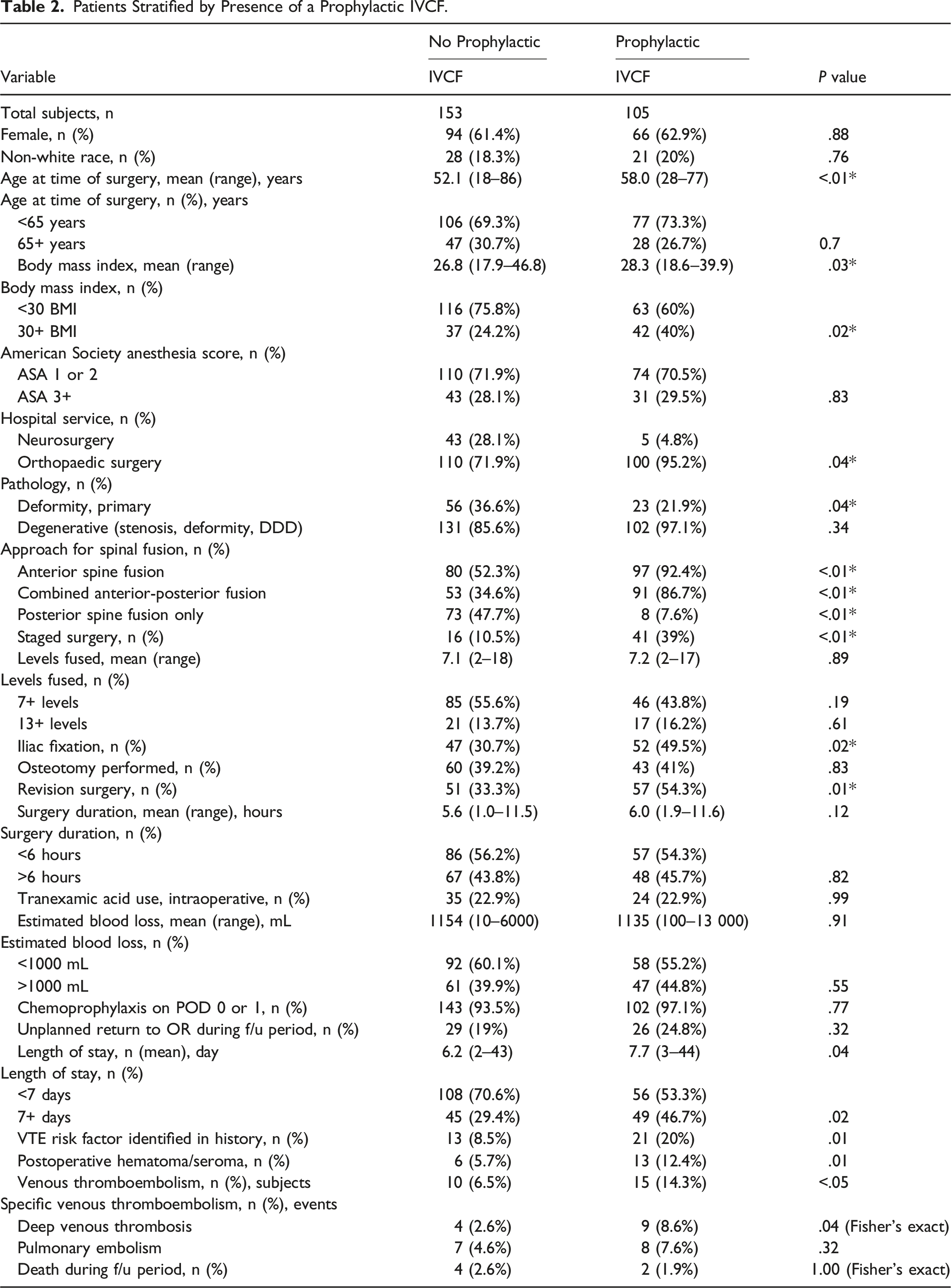
Patients Stratified by Presence of a Prophylactic IVCF.
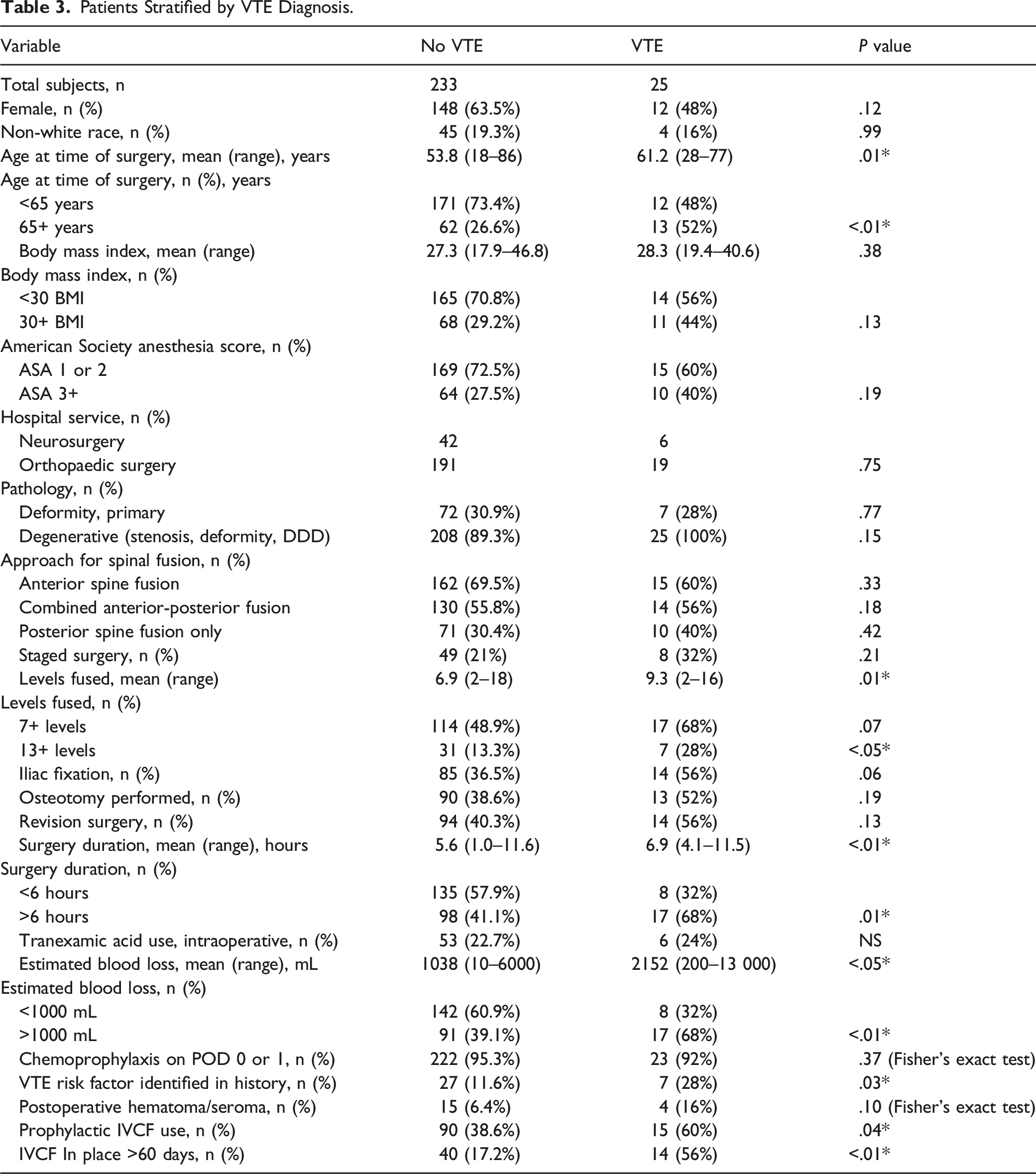
Patients Stratified by VTE Diagnosis.
Multivariate regression model to predict VTE outcome.
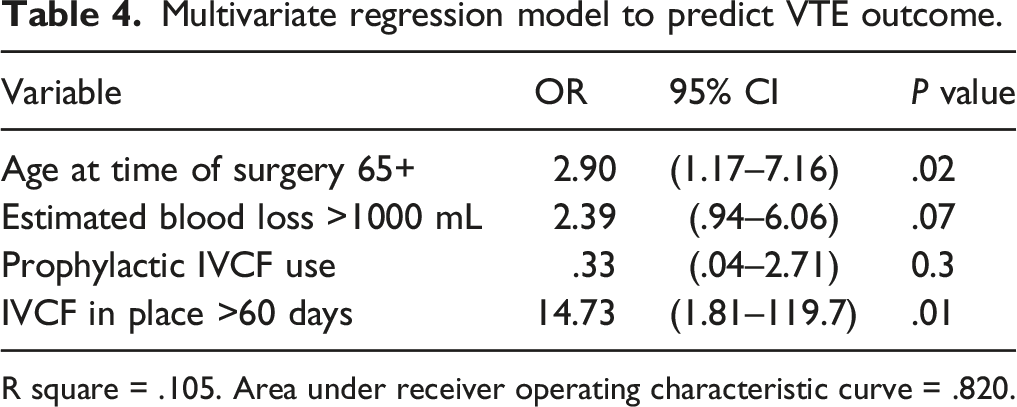
R square = .105. Area under receiver operating characteristic curve = .820.
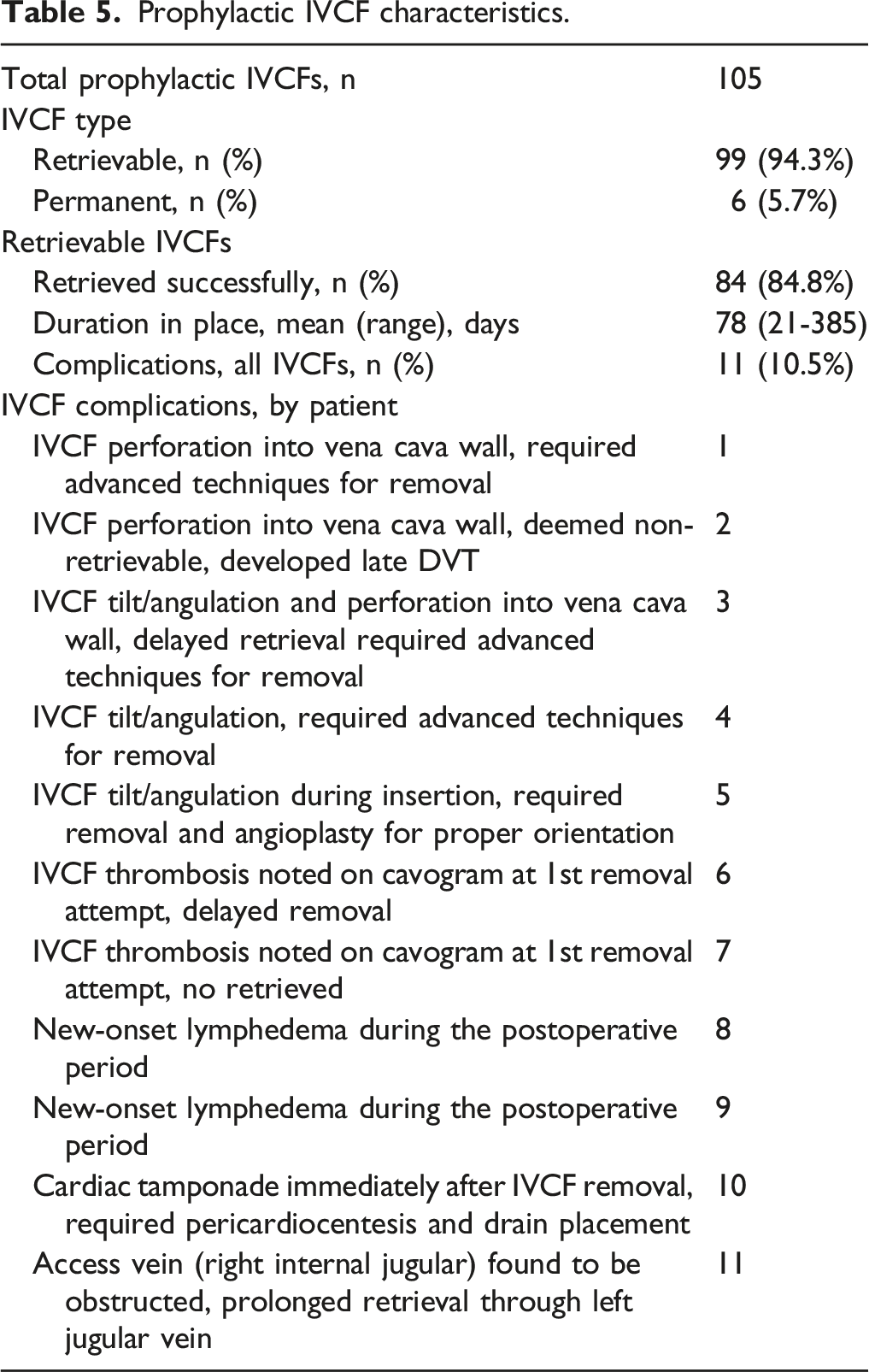
Prophylactic IVCF characteristics.
Discussion
Postoperative VTE and associated symptomatic PE represents a serious acute complication of spine surgery that persists for at least 4 weeks postoperatively. 18 Use of any chemoprophylaxis, a concern for postoperative hematoma, specifically a potentially catastrophic epidural hematoma, exists.8,19-24 The perceived risk 9 of anticoagulant-associated hematoma has prompted prophylactic IVCF placement. The most common accepted indication for placement is a patient with an absolute contraindication for anticoagulation. 25 Other indications, such as VTE prophylaxis in high-risk patients, have expanded in recent years but lack strong supporting evidence.17,26 A few retrospective (level III/IV) studies support the efficacy and safety of prophylactic IVCF use in elective spine patients.2,10-13 A survey of spine surgeons suggested they are used on a case-by-case basis. 9 This study examined all major spine surgery patients at our institution and reported the rate of VTE events and mortality in patients with and without prophylactic IVCFs.
Our overall cohort of patients had VTE, DVT, and PE rates of 9.9%, 5.0%, and 5.8%, respectively (Table 1). Our protocol does not include routine VTE surveillance. Diagnostic testing for VTE was only initiated for symptomatic patients. Differences in patient population and VTE diagnosis cause a wide variation of reported rates (.3-31%). 27 A large systematic review found an aggregate DVT and PE rate of 2.1 and .3%, respectively. 6 A prospective study of adult spinal deformity surgery reported rates of 2.1 and 2.1%, respectively. 7 Our rates of DVT and PE are higher than these studies but within the literature reported ranges. The all-cause mortality rate in our cohort was 2.3%, comparable to other cohorts of adult major spinal surgery.7,13,28
A previous study of 318 major spine reconstruction procedures with two-year follow-up reported overall DVT rates of .3%, symptomatic PE rate of 2.2%, and fatal PE rate of .3. 3 Their study stratified by approach and an anterior component (anterior only or combined anterior-posterior) identified a PE rate of 6.1% and DVT rate of 2.4% utilizing SCDs and thigh-length compression stockings without chemoprophylaxis. 3 The group without IVCF had a similar DVT rate (2.6% in presented study compared to 2.4%) and the overwhelming majority (92.4%) had an anterior component to their approach. The PE rate without IVCF was lower than previously reported (4.6% in presented study compared to 6.1%). 3 In other words, the two studies with similar surgical approaches to the thoracolumbar spine determined similar rates of hypercoaguable diagnoses without IVCF. These rates of hypercoagulable diagnoses create interesting avenues for future research to determine why PE and DVT rates of 8.6% were identified in the presented study. The study cohorts risk factors independent of IVCF are an important consideration to standardize in future investigation in order to determine the true effect on overall rates of an IVCF on VTE.
Our institution has no prophylactic IVCF protocol, placed only by surgeon discretion. Overall, 40.7% of the surgical cohort had prophylactic IVCF placement (Table 2). In our study, patients with IVCF were more likely older, obese, undergo anterior spinal fusion, staged surgery, revision surgery, and have preoperative risk factors. Advanced age and obesity have previously been associated with increased VTE risk in orthopaedic surgery.12,29 Several studies have associated anterior spinal surgery and staged surgery with VTE,2-5 likely due to manipulation of the retroperitoneal vessels. There was no association between IVCF use and length of the fusion construct, need for osteotomy, duration of surgery, or EBL. Interestingly, despite theoretical concerns of hematoma from chemoprophylaxis, IVCF patients received chemoprophylaxis within 24 hours. There was a significantly higher rate of hematoma/seroma amongst patients with IVCFs, possibly a reflection of the higher use of anterior approach in IVCF patients. IVCF use was positively associated with postoperative DVT, but not associated with PE.
Surgeons fixate particularly on PE due to associated morbidity, but this was rare (15 PE events). Given the scarcity of PE, we chose to study symptomatic VTE (DVT/PE). Based on our univariate analysis, risk factors for postoperative VTE included age, number of levels fused, duration of surgery, blood loss, and known VTE risk factor (Table 3). Prophylactic IVCF use was significantly associated with VTE, particularly with longer indwelling duration (>60 days), reflecting the association between IVCF and risk of DVT development.30,31 Interestingly, there was a positive association between greater EBL and VTE, but not between TXA use and VTE. This finding suggests TXA may limit blood loss without increasing VTE risk. Interestingly, BMI and anterior spinal fusion were not associated with increased VTE in our study, despite being recognized as potential risk factors in other studies.2-5,12 Administration of chemoprophylaxis within 24 hours of surgery did not significantly protect against VTE in our univariate analysis.
In the multivariate regression model, significant independent VTE risk factors included age >65 and longer duration of IVCF use (>60 days). Longer duration of IVCF use is confounded by the presence of thrombosis, as a retrievable IVCF would likely remain in place in the setting of DVT. In the multivariate regression model, a prophylactic IVCF was not a significant risk factor for VTE. EBL greater than 1000 mL was approaching significance as an independent risk factor, and along with TXA warrants consideration in future studies.
Complications directly associated with an IVCF are more common than once thought.14,16,17 One study of 464 patients with IVCF reported a 22% complication rate. 17 Commonly reported complications include inferior vena cava wall penetration, thrombotic occlusion, embolization, IVCF movement or fracture, and access site complications. 16 Previous evidence supported that risk increased with duration of IVCF placement, 15 leading to a shift from permanent to retrievable IVCF designs. 14 Most IVCFs in our study were retrievable designs (94.2%). This decision was decided between the patient and physician placing the device, not the attending spine surgeon. Our IVCF retrieval rate (84.8%) is significantly higher than many rates reported in the literature (12-45%). 32 Our IVCF-associated complication rate (10.5%) compares favorably with recent literature. 17 Complications are listed by patient in Table 5.
There are several limitations to our study. The retrospective design causes a lack of randomization (i.e., no prospective control over who received an IVCF) and inherent susceptibility to bias. While IVCF placement varied by surgeon, it was typically due to one or multiple aspects of the patient’s history (Table 2), which creates the possibility of confounding variables contributing to the reported results. Second, retrospective chart reviews are dependent upon manual extraction as well as accurate reporting and coding by the treatment team for complete data collection. Some patients may have received postoperative care outside our hospital system, causing VTE diagnoses to be missed. There is a possibility of bias for patients and physicians to underreport complications, in particular relatively benign or nonspecific complications, from IVCF use such as lymphedema. The outcomes of interest (VTE, DVT, PE, death) were rare in this group of patients, making statistically significant differences challenging to detect. The incidence of VTE was likely underreported, as VTE testing was performed only diagnostically in the setting of symptoms and never for routine asymptomatic surveillance. Finally, we did not address the additional cost of the IVCF implant, its placement, removal, or costs associated with treatment of associated complications.
Conclusion
This study demonstrates that prophylactic IVCF use, specifically duration, and age >65 was associated with an increased risk of symptomatic VTE. Our IVCF related complication rate was relatively low compared to published values, but there were still a clinically significant number of events reported, including one life-threatening event. These conclusions call into question the risk-benefit ratio of routine prophylactic IVCF use and should prompt further study. Given the results of this study performed by an independent observer, the senior author (V.A.) has discontinued prophylactic IVCF use, including in staged anterior and posterior spine surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All data was collected retrospectively under IRB approved protocol (above) at a single academic institution that did not require patient informed consent for data collection. IRB Approval – University of Pennsylvania - IRB # 825753; Principal Investigator: Vincent Arlet, MD; Protocol #: 825753; Review Board: IRB #7; University of Pennsylvania, Office of Regulatory Affairs, 3624, Market Street, Suite 301 S, Philadelphia, PA 19104-6006, Ph: 215-573-2540/Fax: 215-573-9438, INSTITUTIONAL REVIEW BOARD, (Federalwide Assurance # 00004028).