
Abstract
Study Design
A single surgeon case series and meta-analysis of literature
Objective
To evaluate the clinical outcome and patient satisfaction following coccygectomy for coccygodynia in adults and children using a curvilinear paramedian skin incision and to conduct a meta-analysis of the literature to determine the associated infection rate with different surgical factors.
Methods
45 consecutive patients (40 adults and 5 children) underwent surgical coccygectomy for persistent coccygodynia symptoms using a paramedian curvilinear incision. Postoperative clinical outcome scores, patients’ satisfaction and wound complications were assessed. A systematic literature search using specific MesH terms was then conducted covering the period from 1980 to 2020. Only those studies reporting infection rates post coccygectomy were included in a meta-analysis.
Results
The average age of patients was 39 years with a mean duration of symptoms prior to surgery of 7.4 years. The mean Oswestry Disability Index improved from 29 to 7.7 (P < .001). The mean pain Visual analogue scale improved from 8 to 2 (P < .001) and the median patient satisfaction score was 8 (out of 10) suggesting good to excellent outcome. The clinical improvement was the same in children and adults. There was a total of 5 (11%) wound infections, 2 of which needed surgical debridement. Meta-analysis of the included studies showed that the use of prophylactic antibiotics for 24 hours, nonabsorbable skin sutures and glue were associated with low infection rate.
Conclusions
Coccygectomy using curvilinear paramedian skin incision for chronic coccygodynia is an effective procedure with similar or lower complication rates as reported in the literature.
Introduction
The prevalence of Coccygodynia is unknown but it has been associated with several factors including female gender and obesity. 1 Commonest reported causes of coccygodynia are trauma (direct or indirect) and idiopathic from sacrococcygeal joint degeneration.1,2 Rare causes include tumours such as chordoma or infection. 2
Most patients usually respond to conservative treatment with simple analgesia or a combination of local anaesthetic and steroid injections. 3 However, patients with resistant coccygodynia may resort to surgical treatment.3,4
Coccygectomy is a relative successful procedure for coccygodynia4-7 but has been associated with high rates of postoperative wound infection and breakdown.6-8 Most infections and wound complications tend to occur in the early postoperative period. Coccygectomy is commonly performed using a straight midline skin incision over the coccyx with variable reported infection rates.6,9-11 Some authors have also used transverse incision 12 or Z-plasty with transposition of flaps. 13
At our centre, the senior surgeon (JS) who performs these procedures has always used a paramedian curvilinear incision centred over the coccyx. The primary aim of this study was to assess if this type of skin incision was associated with lower rate of wound complications. We additionally present and compare the outcomes of coccygectomy in a cohort of adults and children. A meta-analysis of the literature was performed to analyse the associated postoperative infection rates with different surgical modifiable factors.
Methods
Trust review board approval [Ref 19-077] was obtained. Patients who underwent coccygectomy from June 2010 to February 2020 were included in the study. The primary indication for coccygectomy was persistent coccygodynia for a minimum of 6 months and was only considered after all conservative treatment measures had been exhausted (analgesia, activity modifications, use of ring seat cushion and manipulation of coccyx with injection). MRI scans were conducted on all patients as well as manipulation of the coccyx under general anaesthetic to confirm hypermobility of the coccyx. The senior author [JS] performed the surgery in all cases with same standard paramedian curvilinear incision. Baseline characteristics for all the patients were gathered from their medical notes. Informed consent was obtained from the patient for clinical photographs for the purpose of medical publication and the institutional policy was followed throughout.
Surgical Technique
Following general anaesthesia, the patient is placed prone and table is slightly flexed at the waist to bring up the coccyx. The buttocks are abducted by adhesive tapes secured to the sides of table for good exposure. A single dose of antibiotic (Coamoxiclav 1.2 Gram) is administered at induction. The skin is marked with a curvilinear line 1 cm to the right of midline, with the apex away from midline and centred over coccyx (Figure 1A). The surgical field is prepared with chlorhexidine and isolated with surgical drapes. Adhesive transparent sterile drape is applied and the skin incised over the marking followed by tangential dissection down to the coccyx using monopolar electrocautery. Meticulous Soft tissue handling and haemostasis is observed throughout the procedure. Once the dorsum of coccyx is exposed, a subperiosteal plane is developed leaving behind the musculo-ligamentous attachments. The hypermobile portion is confirmed and the intervertebral disc at that level is excised. The coccyx is held with a towel clip and elevated to facilitate its release from the underlying tissues and dissected from proximal to distal (Figure 1B and C). Care is taken to protect the underlying rectum. The coccyx is excised at its most mobile point, not always necessitating complete excision of the coccyx, although most patients typically demonstrate a hypermobile segment at sacrococcygeal junction resulting in total coccygectomy (Figure 1D). Meticulous haemostasis is ensured before closure (Figure 1E). The wound is closed in layers over a suction drain (exiting superolaterally) with absorbable sutures subcutaneously and interrupted Nylon for the skin (Figure 1F). A simple breathable, adhesive absorbent water-repellent dressing is applied. Senior author [JS] did not advocate the use of bulky padded dressing. Postoperatively all patients were allowed to mobilise as tolerated, admitted overnight for drain care and were discharged 1 day postoperatively following drain removal. Patients were given wound care instructions and service contact numbers to facilitate prompt review in case of any problems. Patients were advised to avoid sitting or lying in positions that caused undue pressure on the operative wound site, until the wound healed fully. It was deemed unnecessary to rest the patients in prone position postoperatively. Postoperative protocol included wound check at 1 week with suture removal at week 2 and further surgical review at 6 and 12 weeks. Intraoperative photographs from draping to closure of the skin incision. During surgery the wound edges are gently retracted. The retractors shown here were used whilst taking photographs for demonstrating purpose. (A), Following the marking prepping and draping of the surgical field. The paracentral curvilinear line is marked before the incision. (B & C), following the exposure of the coccyx the hypermobile segment is identified and held with a towel clamp. The intervertebral disk at the mobile level is excised and the coccyx is elevated and gently freed from soft tissue attachment including the ano-coccygeal ligament. (D), the resected coccyx. (E), following excision of the coccyx meticulous haemostasis is ensured and the cavity is closed in layers over a suction drain. (F), the skin is closed with non-absorbable, interrupted nylon suture.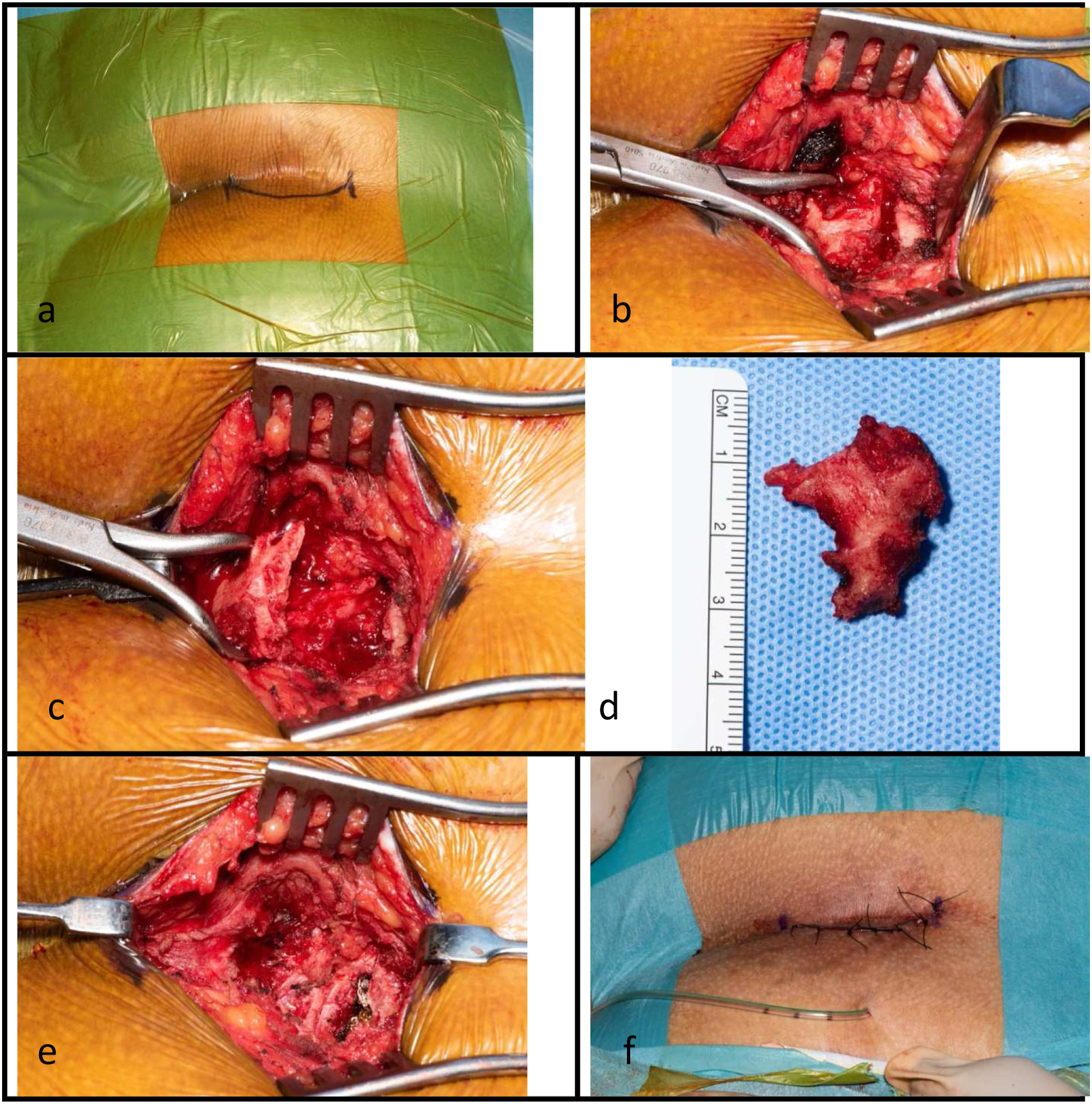
Literature Search
A systematic literature search was conducted on PubMed data base using the terms ‘coccygodynia’ or ‘coccydynia’ and/or ‘coccygectomy’ from 1980 to May 2020. The key word ‘coccygectomy’ was also used in the Google Scholar search engine and top 1000 titles from search results were reviewed. The search was limited to articles in the English language and only case series (minimum of 5 cases) or comparative studies reporting on outcome of coccygectomy were initially included. The articles were considered for final inclusion if they reported the rate of wound infection in addition to reporting at least 1 of the following: prescription of a perioperative diet or bowel preparation, antibiotics usage, use of a postoperative wound drain and whether the wound was irrigated with saline or antibiotics. References of the selected articles were also searched for other publications. The literature search, assessment of eligibility, qualities of the studies and the retrieval of data were conducted by 4 independent authors (SN, ZA, ME &MJ). The quality of the studies was assessed according to the MINOR scale (Methodological Index for NonRandomised studies) for nonrandomised controlled studies. 14
Outcome Measures
For our case series, patient reported outcome measures were assessed preoperatively and at 3 months postoperatively using the 50-point Oswestry Disability Index (ODI) and the pain visual analogue scale (VAS) from 0 to 10 (0 being no pain and 10 the most severe pain). The overall satisfaction rate was scored on scale from 0 to 10 with 0 being unsatisfactory and 10 being excellent – this in turn was based on patient experience through the whole treatment journey. To obtain extended follow-up data and improve follow-up outcome reporting rates patients were consulted over telephone.
Meta-analysis of the literature was conducted to calculate the associated pooled infection rate with the following surgical modifiable factors: prescription of specific diet or bowel preparation, use of prophylactic antibiotics (single or dual antibiotics and duration), wound irrigation with antibiotics, use of drain and the method of skin closure.
Statistical Analysis
The baseline characteristics of patients are presented in contingency tables. Paired t-test was used to compare improvement in ODI and the Wilcoxon Signed Ranks Test was used to assess improvement in pain VAS. Unpaired t-test and Mann–Whitney test were used to compare baseline characteristics and outcome between children and adults. The association between outcome and baseline characteristics was assessed using linear correlation coefficient for linear data (age, duration of symptoms and BMI) and by comparing the means of outcome for categorical data (gender, smoking and cause of coccydynia).
Meta-analysis of proportion 15 was used to calculate the overall pooled infection rates from all studies included from literature search. Univariate analysis was conducted by calculating the pooled infection rate (from all studies) associated with each modifiable surgical factor without adjusting for any other factors. This was also done using meta-analysis of proportion and presented in contingency tables to facilitate comparison. The meta-analysis of proportion was carried out on the StatsDirect software using the inverse variance and the random effect model. Heterogeneity in the metaanalysis was measured using the I 2 index and Cochran’s Q test.
Results
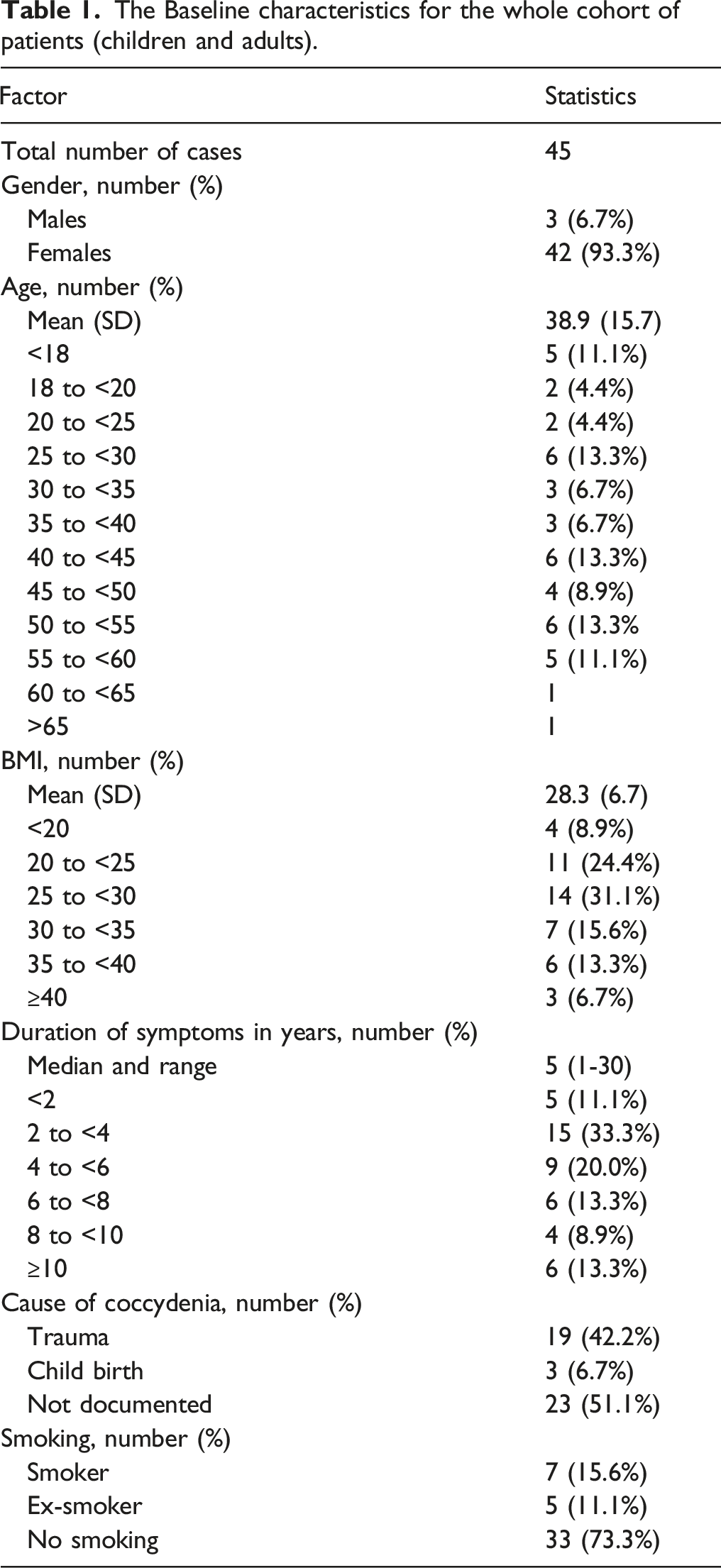
The Baseline characteristics for the whole cohort of patients (children and adults).
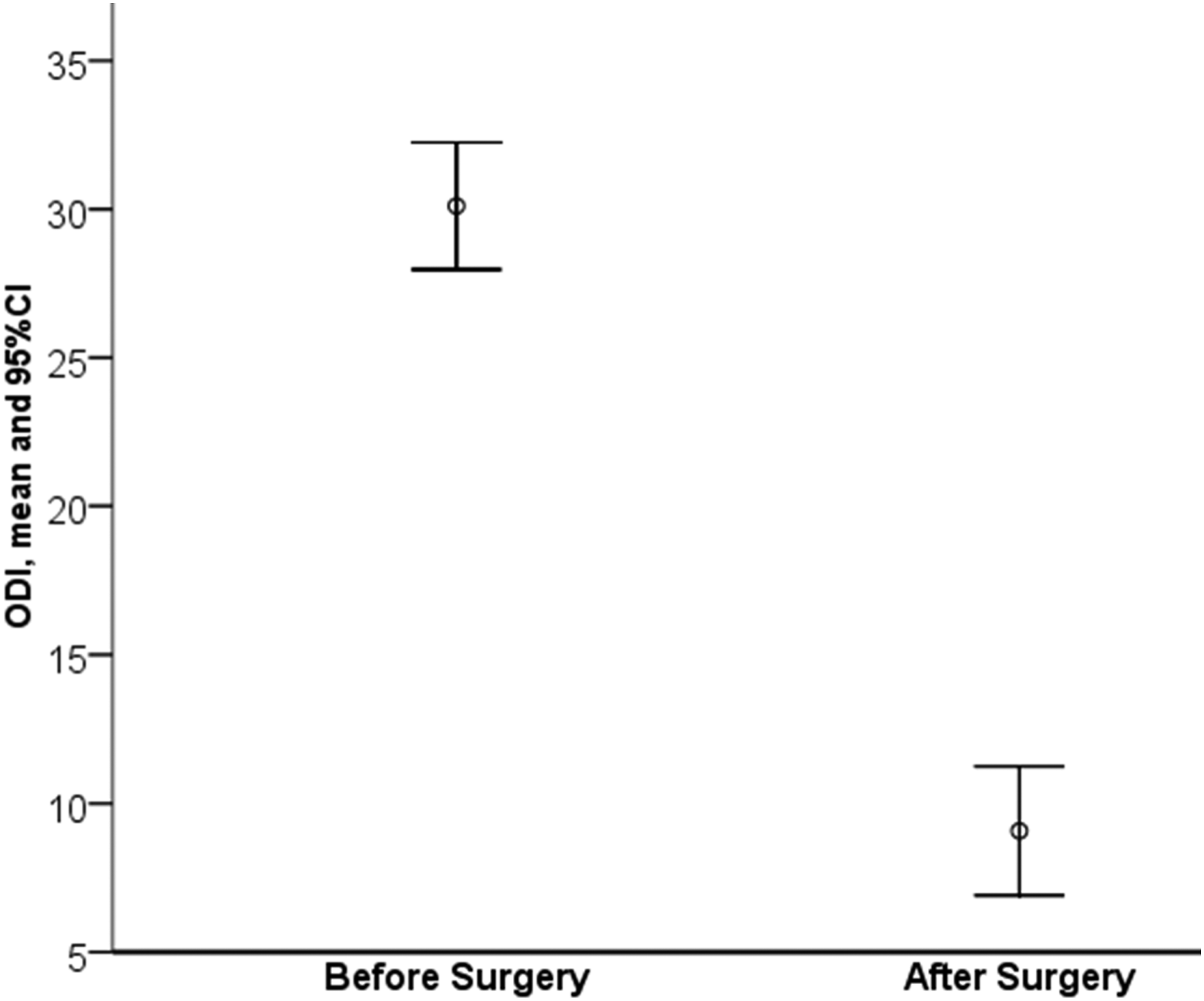
The Oswestry Disability Index (ODI) significantly improved from a mean of 30.11 before surgery to a mean of 9.08 after surgery, p < .001, (paired t test).
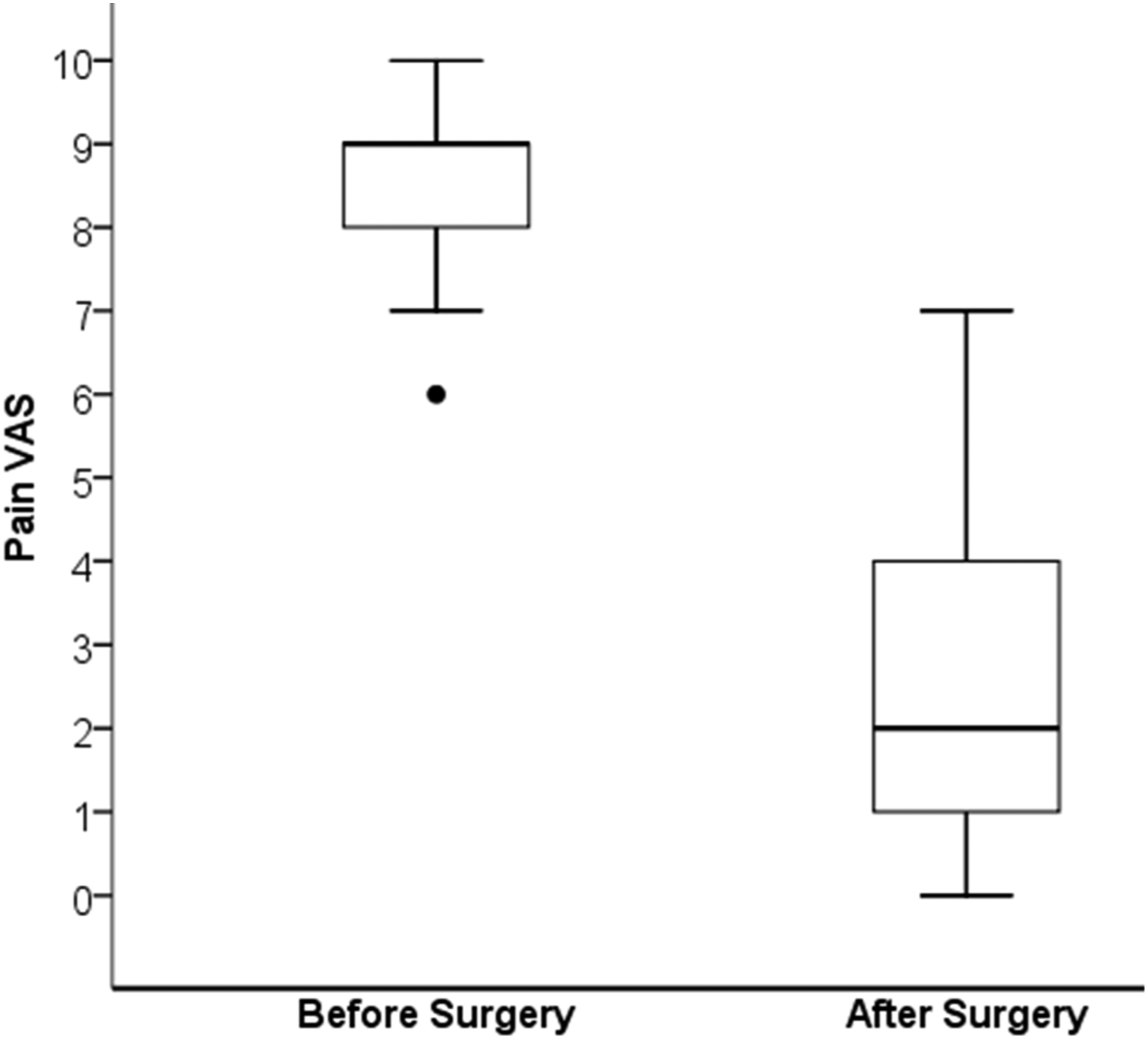
There was a significant improvement in the pain VAS after surgery, p < .001 (Wilcoxon Signed Ranks Test).
Compares baseline and outcome data between children and adults.
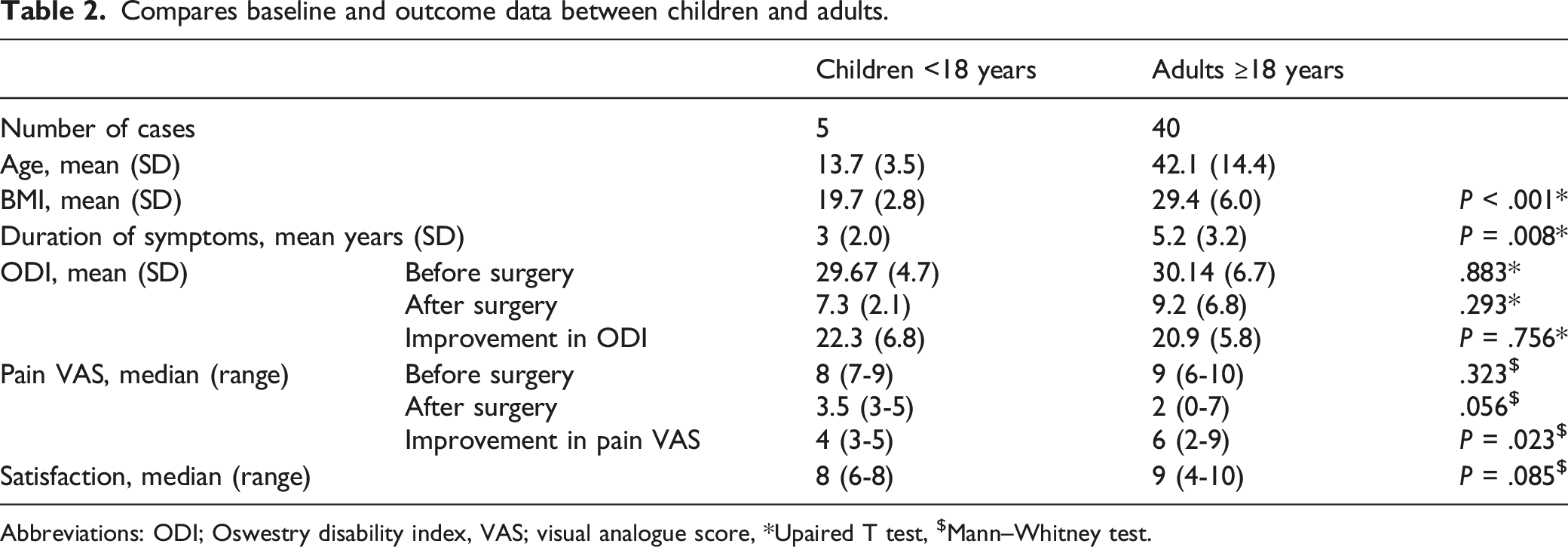
Abbreviations: ODI; Oswestry disability index, VAS; visual analogue score, *Upaired T test, $Mann–Whitney test.
Complications occurred in a total of 5 patients (11%), all of them females and adults. Two patients (4.4%) developed deep infection with wound breakdown. In 1 case, the patient’s drain was inadvertently removed while transferring patient from the operating table. This patient developed a haematoma which subsequently got infected. In the second case, the patient knocked the operative site against a chair arm while sitting down 2 days after discharge from hospital and presented a week postsurgery with wound dehiscence and purulent discharge. Both patients underwent surgical debridement, washout and Vacuum dressing along with intravenous antibiotics. The wounds healed with regular dressings for 4 weeks without long term sequelae. Three patients (6.6%) developed superficial wound infections with serous discharge but without wound breakdown. All 3 were identified at 1 week postsurgery and were treated with oral antibiotics and weekly dressing review. All 3 cases settled without needing surgical debridement or admission. Different types of bacterial organisms were cultured from the wounds. Staphylococcus Aureus was isolated from 2 patients [sensitive to flucloxacillin], 1 patient grew Staphylococcus aureus along with Bacteroides Fragilis [sensitive to flucloxacillin and metronidazole], 1 patient grew Peptoniphilus Asaccharolyticus [sensitive to metronidazole], and 1 patient grew mixed organisms including pseudomonas. The treatment was guided by Microbiologist advice on individual basis. We were unable to establish any association between wound infection and BMI, age or smoking history.
Literature Analysis Results
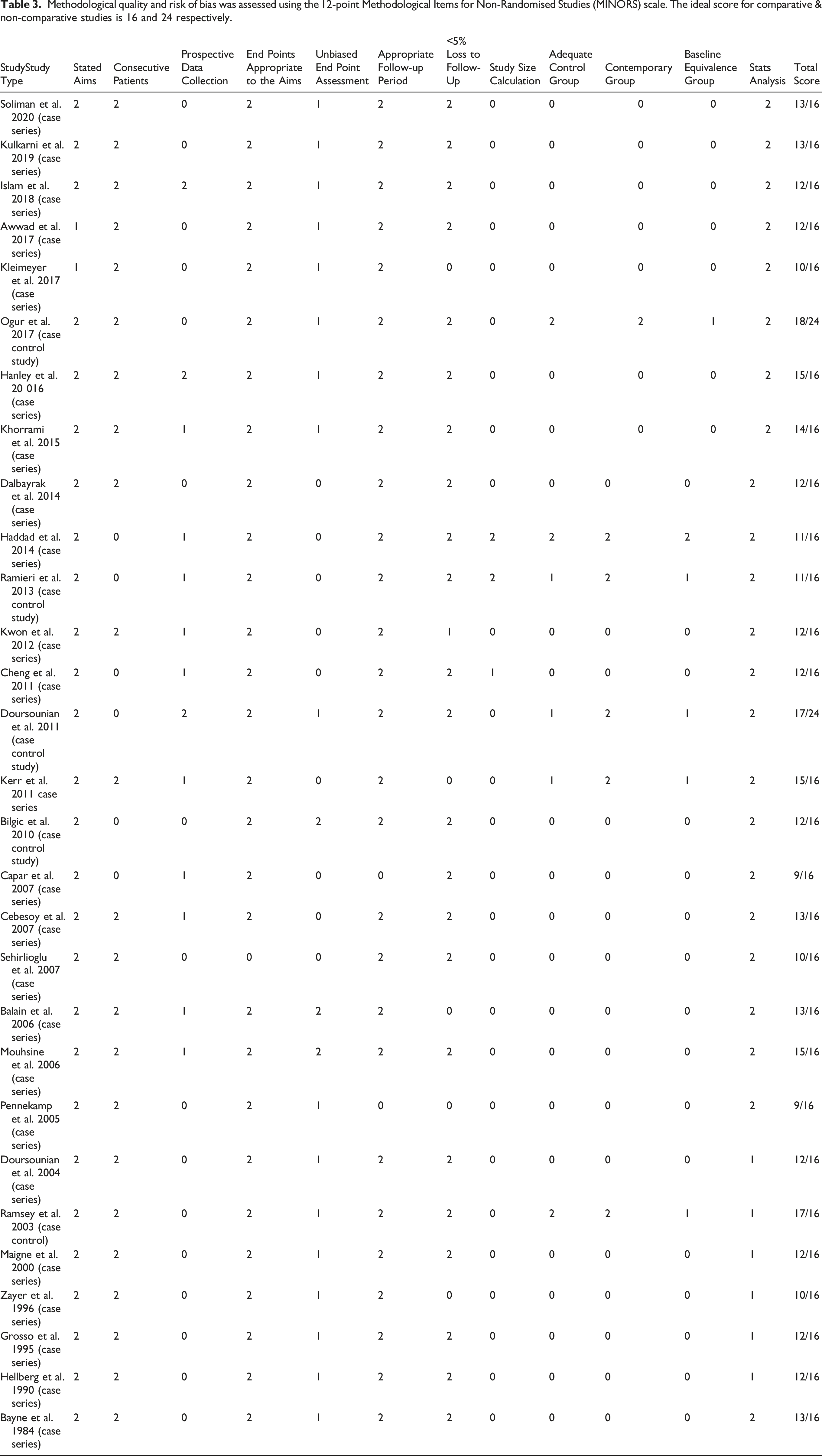
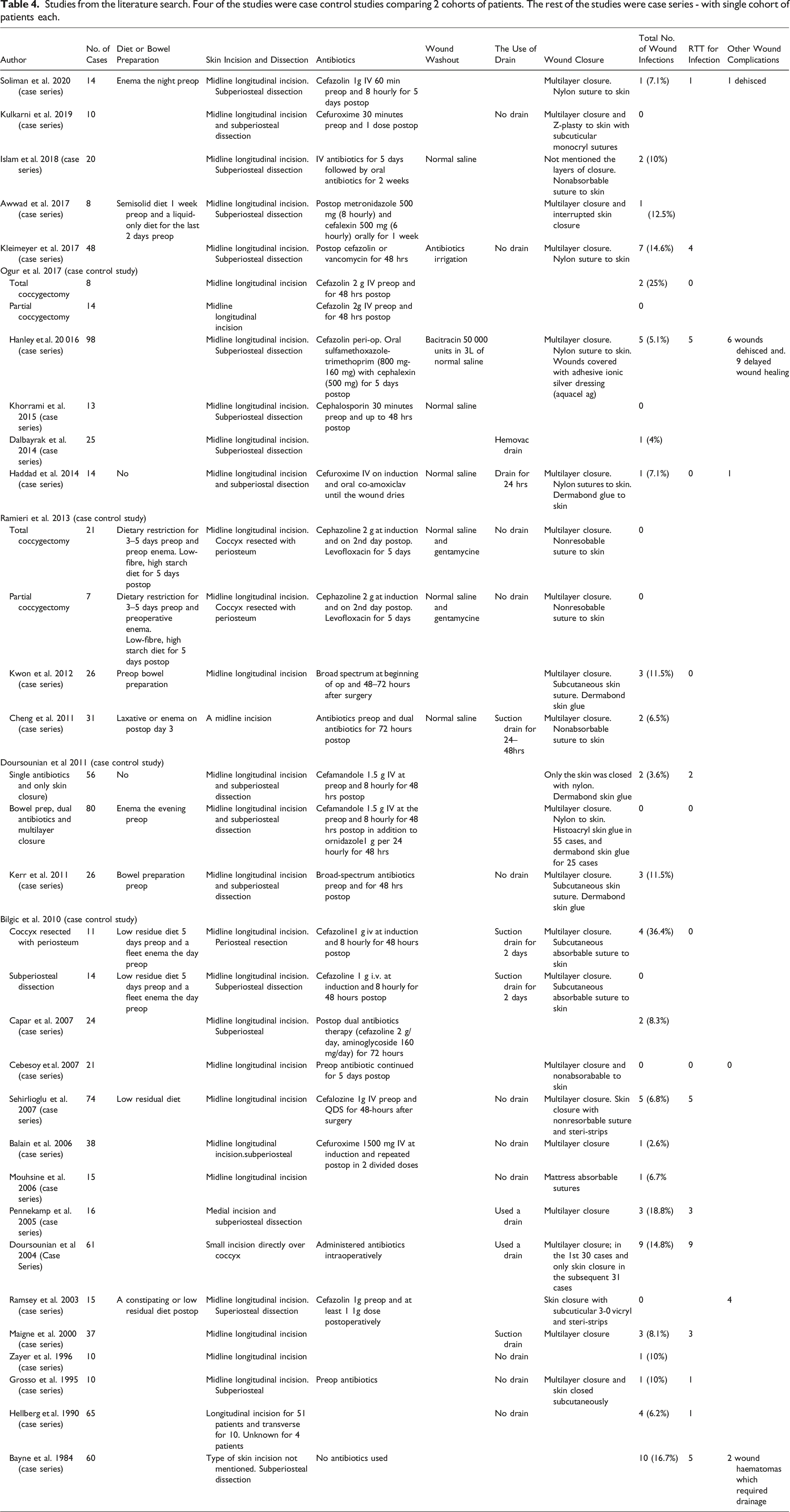
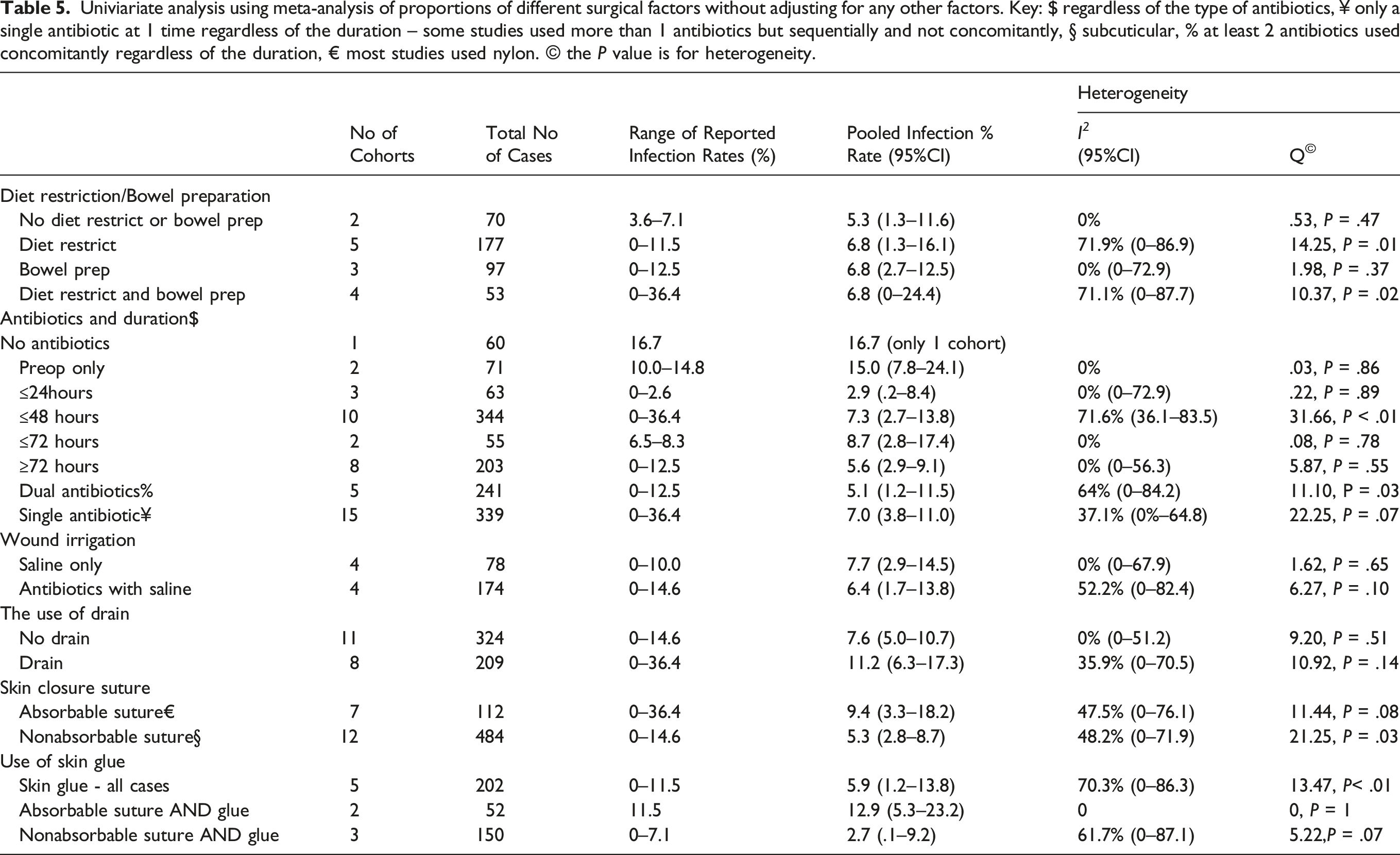
29 studies4,5,7-13,16-35 (4 case controls10,11,23 and 25 case series 4,5,7,8,12,13,16-22,24-35, making a total of 33 cohorts of patients) fulfilled our inclusion criteria (figure 4) and were included in our analysis with a total number of 990 cases. The mean follow-up of the studies ranged between 1.2 and 15 years. Table 3 shows the quality of the studies assessed by the MINORS scale and Table 4 shows details of the studies with their surgical techniques and wound complications (Table 3). Reported infection rate by the studies ranged between 0% and 36% (Table 4) with an overall pooled infection rate of 7.7% (95% CI 5.5–10.3). Univariate analysis of the pooled infection rate (from all studies) in association with different modifiable factors is shown in (Table 5). According to our meta-analysis results, factors that were associated with noticeable low pooled rate of infection include the use of antibiotics (for 24 hours), nonabsorbable sutures especially in conjunction with skin glue. Dual antibiotics and wound irrigation with antimicrobial diluted in saline were also associated with relatively slight reduced infection rate. The use of drain was associated with relatively higher infection rate. Our meta-analysis of the literature failed to show that bowel preparation or diet restriction had a significant impact on wound infections. Flow chart of the systematic search and review process of the articles included in the Meta-analysis. Methodological quality and risk of bias was assessed using the 12-point Methodological Items for Non-Randomised Studies (MINORS) scale. The ideal score for comparative & non-comparative studies is 16 and 24 respectively. Studies from the literature search. Four of the studies were case control studies comparing 2 cohorts of patients. The rest of the studies were case series ‐ with single cohort of patients each. Univiariate analysis using meta-analysis of proportions of different surgical factors without adjusting for any other factors. Key: $ regardless of the type of antibiotics, ¥ only a single antibiotic at 1 time regardless of the duration – some studies used more than 1 antibiotics but sequentially and not concomitantly, § subcuticular, % at least 2 antibiotics used concomitantly regardless of the duration, € most studies used nylon. © the P value is for heterogeneity.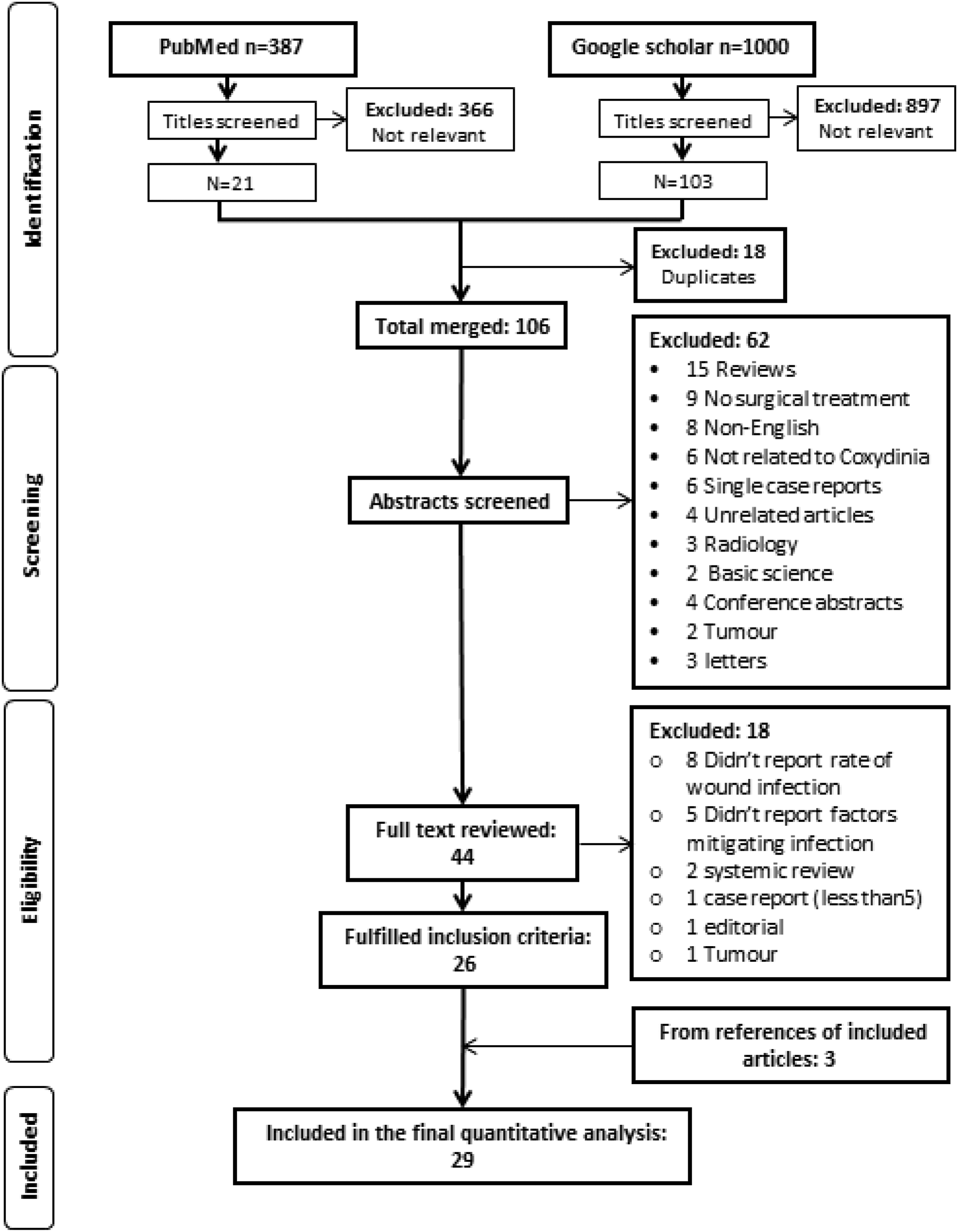
Discussion
In this paper, we have presented the results of a series of coccygectomy cases using a paramedian skin incision. Our results support coccygectomy as an effective procedure for coccygodynia as demonstrated by the significant improvement in ODI, pain VAS, and patient satisfaction in children and in adults.
We believe that the use of paramedian skin incision facilitates good closure of the surgical wound by diverting the wound away from the central cleft where skin maceration and soft tissue tension is relatively higher. The curvilinear nature of the incision also provides a good exposure of the coccyx by increasing the effective length of the incision without putting undue stretch on the tissues during surgery. The overall wound complication rate in our series falls within the range reported in the literature with 5 postoperative wound infections, 3 being superficial and 2 requiring return to theatre. The senior author views the use of a surgical drain as essential in the postoperative management of these patients, with 1 case of deep infection developing following premature drain removal and subsequent haematoma formation. No 1 else in this series developed any postoperative haematoma.
The second case of deep infection resulted following a traumatic dehiscence of the wound, which would support the abstinence of sitting directly on the operative site until the wound had healed, as previously recommended by several authors.5,9,16,19,26
The rate of wound complications and infection has varied considerably in the literature (Range 0%-36%) with an overall pooled infection rate of 7.7%.3,5,6,10,11 Surgeons have resorted to different measures to reduce the risk of infections including diet restrictions,10,13,18,23,27,31 enema bowel preparations,5,7,9,10,16,23,24 different skin incisions ,12,13,20 modified deep dissection techniques,10,11,23 multilayer closure,7,9,19,22 the usage of drains to reduce the risk of haematoma,10,21,22,24 different regimes of antibiotics9,23,25 the use of specific wound dressings5,7,23,27 and strict postoperative wound care protocols.9,23,26 Belgic et al. claimed in a case control study that subperiosteal dissection significantly reduces the infection. 10 Subperiosteal dissection, however, did not eliminate infection in many other studies.4,8-10,19,21,22,25,29 Kulkarni et al. claimed that involving a plastic surgeon and closing the wound using z-plasty technique eliminated the infection in 16 cases. 13 The use of dual antibiotics with multilayer skin closure by Hanley et al. 19 and Capar et al. 25 did not significantly reduce infection with both studies reporting an infection rate of 5% and 8%, respectively. Similarly, Cheng et al. used dual antibiotics and multilayer closure in addition to bowel preparation and reported an infection rate of 6.5%. 24
Contrary to the above, Derousonian et al. 9 claimed that they were able to eliminate infection in 1 of the largest case control studies by the use of bowel preparation, multilayer closure (relative to closing the skin only) and use of dual antibiotics for 48 hours postoperatively. However, it’s worth noting that in addition to this, the patients were kept in hospital for a week postoperatively and wound dressing was changed every second day without removing the skin glue adhesive layer. After discharge, the patients were instructed to rest for 3 weeks with progressive return to sitting position. A similar postoperative wound care and postdischarge instructions were also adopted by Cebesoy et al. 26 who reported a similar rate of infections (0%) in their cohort of 21 patents. This may suggest that keeping patients in hospital for up to a week postoperatively for strict wound care and avoiding sitting on the wound for a longer period time is a significant factor (in addition to other measures) in reducing the infection rate. Keeping patients for 6 days in hospital, however, is not practical in most health care settings, especially following minor surgical procedures.
Our analysis of the literature failed to show that bowel preparation or diet restriction had a significant impact on wound infections. Prophylactic antibiotics (especially for 24 hours), nonabsorbable sutures especially in combination with skin glue were all associated with noticeable lower infection rate. Dual antibiotics therapy and wound irrigation with antibacterial solutions were also associated with relatively slight lower infection rate.
Univariate analysis of the literature showed that drains were associated with higher proportion of infections-compared to when drain was not used. Our experience suggests that the use of a drain is safe and helps reducing the risk of postoperative haematoma and potential subsequent infection. Our experience does not support the results of the univariate analysis, but on further sub analysis, studies that used drains, were also more likely to use absorbable sutures for skin closure and used none or only preoperative prophylactic antibiotics. The latter factors were associated with relatively higher proportions of infection. It is also worth noting that the studies who reported other wound complications such as haematoma and or wound dehiscence did not mention whether they used a drain (Table 4), and hence we cannot infer from our literature analysis if the use of drain had any impact on other wound complications. Therefore, meticulous haemostasis and multiple layer closure to eliminate dead space remain a valuable adjunctive strategy to the use of drain. It is interesting to note that with only a single preoperative dose of antibiotic administered at our centre, the overall infection rate is less than that reported in other studies using the same antibiotic regime (15%) (Table 5).
According to the literature, Staphylococcus Aureus is responsible for a good proportion of infections in additions to Coliforms4,9,19 Doursounian et al. 9 and Kleimeyer et al. 4 reported that the most common organism cultured was Staphylococcus Aureus. Hanley et al. reported mixed organisms including Staphylococcus aureus. 19 This suggests that other systemic factors such as patient comorbidities (e.g. diabetes) are also relevant. Hence, broad-spectrum prophylactic antibiotics and other general measures for reducing infection are important.
Limitations of the Study
The number of cases published in the literature has always remained low because only small proportions of patients fail nonsurgical management.4,20 This is also a limitation of our case series. Hence, distilling reliable conclusion for this procedure based on available current literature can be challenging.
We do not use any radiological classification of coccydynia at our centre but rely on the findings of instability during manipulation of the coccyx under anaesthetics and the response to the injection of steroid and local anaesthetics as a predictor for the likely outcome of subsequent coccygectomy. Hence, we were unable to correlate the outcome with any known radiological classification for our cohort of patients.
Other limitation in our series is the fact that the missing pre and postoperative scores obtained retrospectively through telephonic patient review can be fraught with memory bias.
Conclusion
Coccygectomy offers excellent relief from coccygodynia symptoms in a selection of adults and children who fail conservative modes of treatment. The use of a paramedian curvilinear incision is safe and provides good exposure during surgery with similar low wound complication rate as reported in the literature. According to literature, the use of antibiotics (for 24 hours), nonabsorbable skin suture and skin adhesive glue are associated with lower rate of infections.
Supplemental Material
sj-pdf-1-gsj-10.1177_21925682211058155 – Supplemental Material for Clinical Outcome of Coccygectomy Using a Paramedian Curvilinear Skin Incision in Adults and Children With Meta-Analysis of the Literature Focusing on Postoperative Wound Infection
Supplemental Material, sj-pdf-1-gsj-10.1177_21925682211058155 for Clinical Outcome of Coccygectomy Using a Paramedian Curvilinear Skin Incision in Adults and Children With Meta-Analysis of the Literature Focusing on Postoperative Wound Infection by Satish Nagappa, Zeiad Alshameeri, Mohammad Elmajee, Yousuf Hashmi, Ajay Bowry, Morgan Jones, and Jonathan Spilsbury in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.