
Abstract
Study Design
Review of current literature and authors experience.
Objective
Pre-operative planning is an integral part of complex spine surgery. With the advent of computer-assisted planning, multiple surgical plans can be evaluated utilizing alignment parameters, and the best plan for individual patients selected. However, the ability to evaluate and measure surgical correction goals intraoperatively are still limited. The use of patient-specific UNiD rods, created based on pre-operative plans, provided an initial tool for implementation of pre-operative plans in the operative setting.
Methods
A literature review for the use of patient-specific UNiD rods in thoracolumbar spine complex surgery was performed. The articles were selected and reviewed for the initial experience/outcomes of these techniques. Further, the initial experience of the authors at The University of Colorado is described.
Results
The use of UNiD patient-specific rods, in combination with pre-operative planning has been shown to provide a higher rate of patients with spinopelvic alignment parameters within currently accepted ranges. This includes improvement of sagittal vertical axis (SVA) < 50 mm and pelvic incidence (PI)–lumbar lordosis (LL) = ± 10°. Multiple authors have shown improvement in pelvic tilt to age adjusted values but note continued difficulties in obtaining correction goals.
Conclusions
The use of pre-operative planning software and UNiD patient-specific rods has been shown to improve surgeon’s ability to achieve spinopelvic alignment parameters, specifically SVA and PI-LL, along with other possible benefits. Further research is needed regarding long-term value of the technology.
Introduction
Pre-operative planning is an integral part of complex spinal deformity correction surgery. Methods to accomplish this have changed significantly with the advent of planning software such as the UNiD™ Hub, part of the UNiD Adaptive Spine Intelligence™ (Medicrea®, Lyon, France) and Surgimap® (Nemaris Inc., New York, New York). The use of planning software for complex spine deformity cases at the University of Colorado began in 2012. Utilizing validated values for Sagittal Vertical Axis (SVA), Pelvic Incidence–Lumbar Lordosis Mismatch (PI–LL) and Pelvic Tilt (PT), the surgical correction could be planned with great specificity. 1 However, matching these planned values in the operating room (OR) remained difficult.
In 2014, Medicrea® (Lyon, France) obtained FDA approval for implantation of patient-specific spinal rods (PSSR) in surgery. While these rods had been utilized outside the United States, initial use for adult deformity cases was adopted at the University of Colorado Anschutz Medical Campus after FDA approval.
Since then, several studies have evaluated the utility of the rods in combination with pre-operative planning in attempts to improve the radiographic and clinical results in spine surgery. Further, the planning has been augmented by the development of a predictive model that attempts to determine the post-operative thoracic kyphosis (TK) and PT. While a current manuscript has been submitted and is under review with regards to this model, it will be discussed further in this review. This paper details the current experience and results of spine surgery using UNiD™ (Unique Identity) rods.
Methods
This is a review of the current literature, including scientific presentations, on the use of patient-specific spine rods in Adult Spine Deformity. The authors performed a comprehensive search of the PubMed database for all articles published up to February 1, 2021. Key words utilized in the search included “patient-specific,” “spine,” “rods,” and “UNiD.” Terms were searched in combination. Articles were selected based on a set of simple criteria: (1) the articles addressed the use of pre-operative planning and patient-specific spine rods for correction of adult spinal deformity (ASD) surgery, (2) the articles described outcomes related to spinopelvic alignment results with comparison of pre- and post-operative measurements (without restriction on timing of pos-operative results), and (3) the articles focused on thoracolumbar spine deformity. Initially, 7 articles dealing with the adult spine were identified. One was specific to lumbar degenerative cases, and a second related to cervicothoracic spine deformity. The other 5 were reviewed, and 1 further article was identified from the references of these manuscripts. Given the heterogeneity of the follow-up and reporting, we report on the articles and results below.
Further, we report the experience at The University of Colorado with the implementation of a new predictive model from UNiD™ Adaptive Spine Intelligence™, for TK and PT. As an initial evaluation of the model, 2 cohorts were analyzed. Both cohorts included patients undergoing correction of ASD with either sagittal plane imbalance alone or combined sagittal plane imbalance with a coronal deformity. Sagittal plane deformity parameters included PI-LL mismatch >10°, SVA > 40 mm, or PT > 20°. Cohort 1 consisted of 34 patients who had previously undergone surgery and had been planned utilizing methods specific to the authors. When pre-operative TK was <40°, the patients TK was manually corrected to 40° using the planning software. Deformity correction was then planned based on the new thoracic spinal parameters and goal to achieve SVA < 40 mm, PI-LL < ±10, and age adjusted PT “referenced in the literature.” 2 Patients with coronal deformity had combined correction in all planes. If the TK was >40° at pre-op, no adjustment was made prior to planning the deformity correction. The next 23 patients (Cohort 2) were planned using the predictive model for TK and PT. Cohort 2 was planned to achieve the same SVA, PI-LL, and PT goals, as well as coronal correction, as Cohort 1.
Results
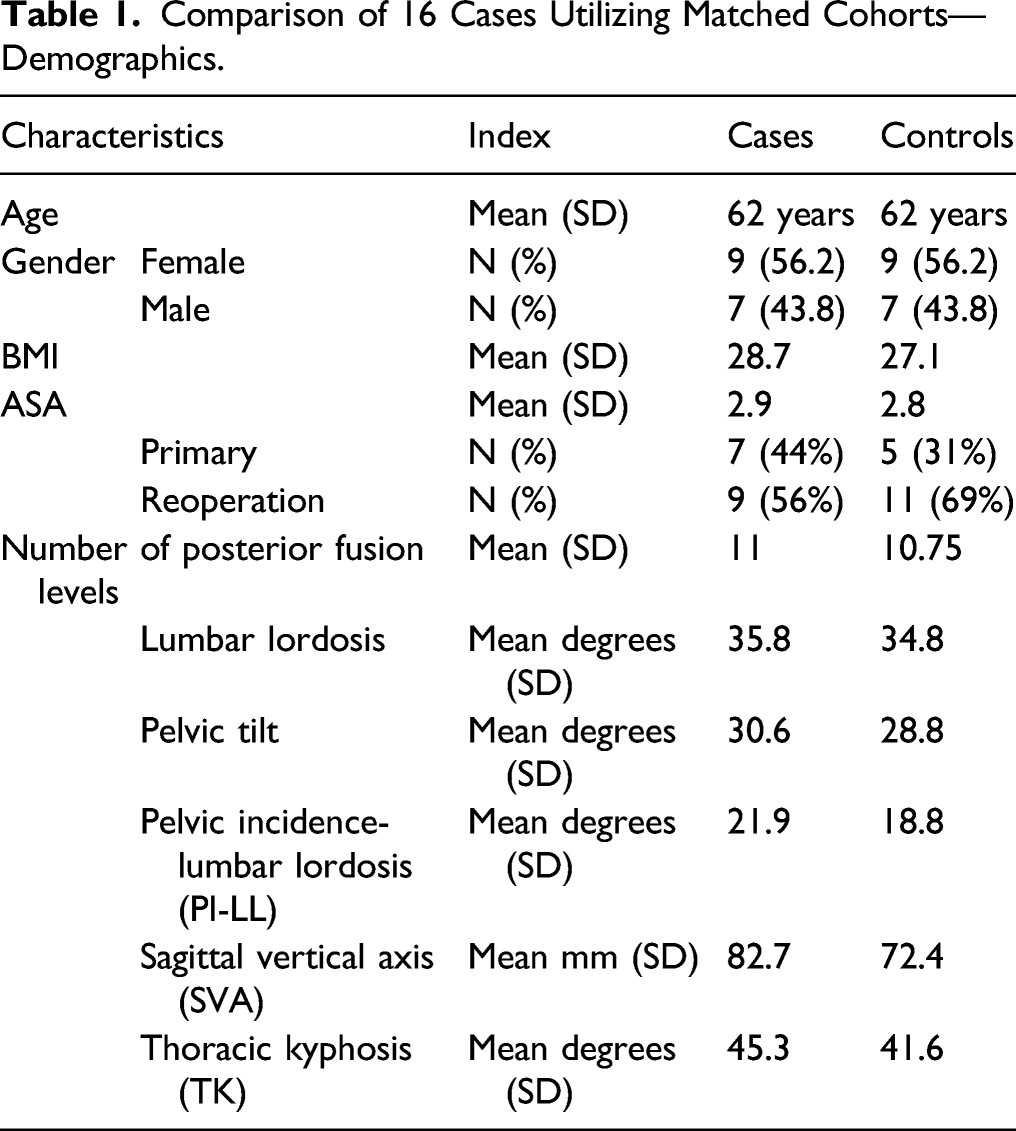
Comparison of 16 Cases Utilizing Matched Cohorts—Demographics.
Comparison of 16 Cases Utilizing Matched Cohorts—Results.
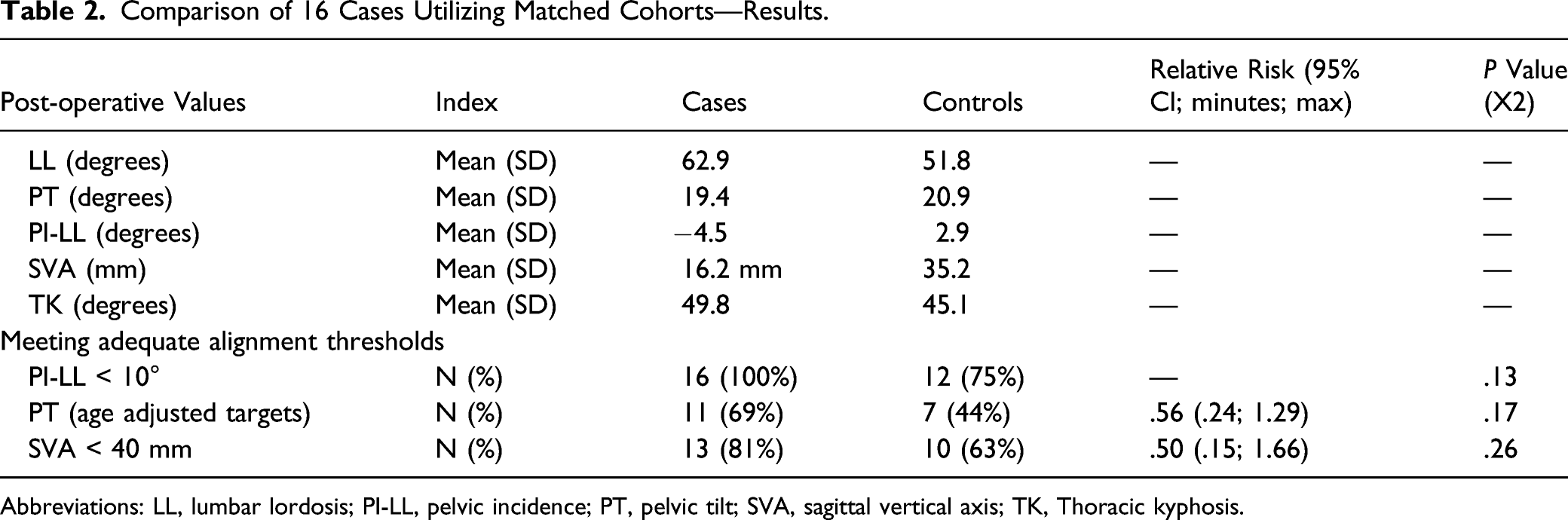
Abbreviations: LL, lumbar lordosis; PI-LL, pelvic incidence; PT, pelvic tilt; SVA, sagittal vertical axis; TK, Thoracic kyphosis.
Similar findings were reported by an international cohort of surgeons in 2018. 4 In this series of 60 patients followed to 1-year post-operative, patients treated with UNiD rods were 2.6 times more likely to achieve normal PI-LL mismatch than previously recorded results In the literature. Again, the authors noted that PT correction was limited and difficult to predict. In fact, PT values at 1-year post-op often remained similar to the PT measured at pre-op.
As longitudinal follow-up continued, 1- and 2-year outcomes for UNiD PSSRs were reported. In 1 publication including 34 patients (all with 1-year follow-up and 14 with 2-year follow-up), correction of SVA, PI-LL, and LL was maintained out to 2 years post-op. 5 These results were superior to historical data for traditional open and minimally invasive deformity correction surgeries. Again, post-operative restoration of PT remained difficult to predict, and the authors concluded that improved prediction of post-operative compensation and individualized alignment goals would lead to improvement in the results.
More recent studies have shown similar results. Two recent short-term studies have been published. In a study looking at immediate post-operative outcomes, the planned and actual post-operative results were shown to have a statistically significant correlation with regards to spinopelvic alignment parameters. 6 In a separate 3 month post-operative evaluation of outcomes of 77 patients, the authors found the planning and use of the rods provided significant improvement in SVA and PI-LL. 7 They again noted, as have previous studies, that PT was improved, but less predictable. They also reported on 86 patients with at least 1 year follow-up. 8 This publication again reported significant improvement in SVA and PI-LL, but they also discussed decreased rates of mechanical complications, 18%.
Predictive Model Results.
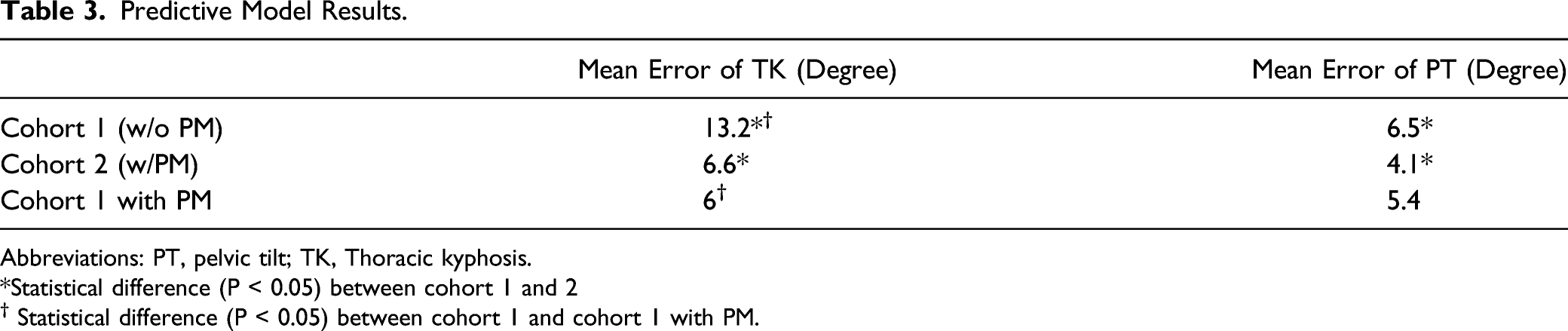
Abbreviations: PT, pelvic tilt; TK, Thoracic kyphosis.
*Statistical difference (P < 0.05) between cohort 1 and 2 † Statistical difference (P < 0.05) between cohort 1 and cohort 1 with PM.
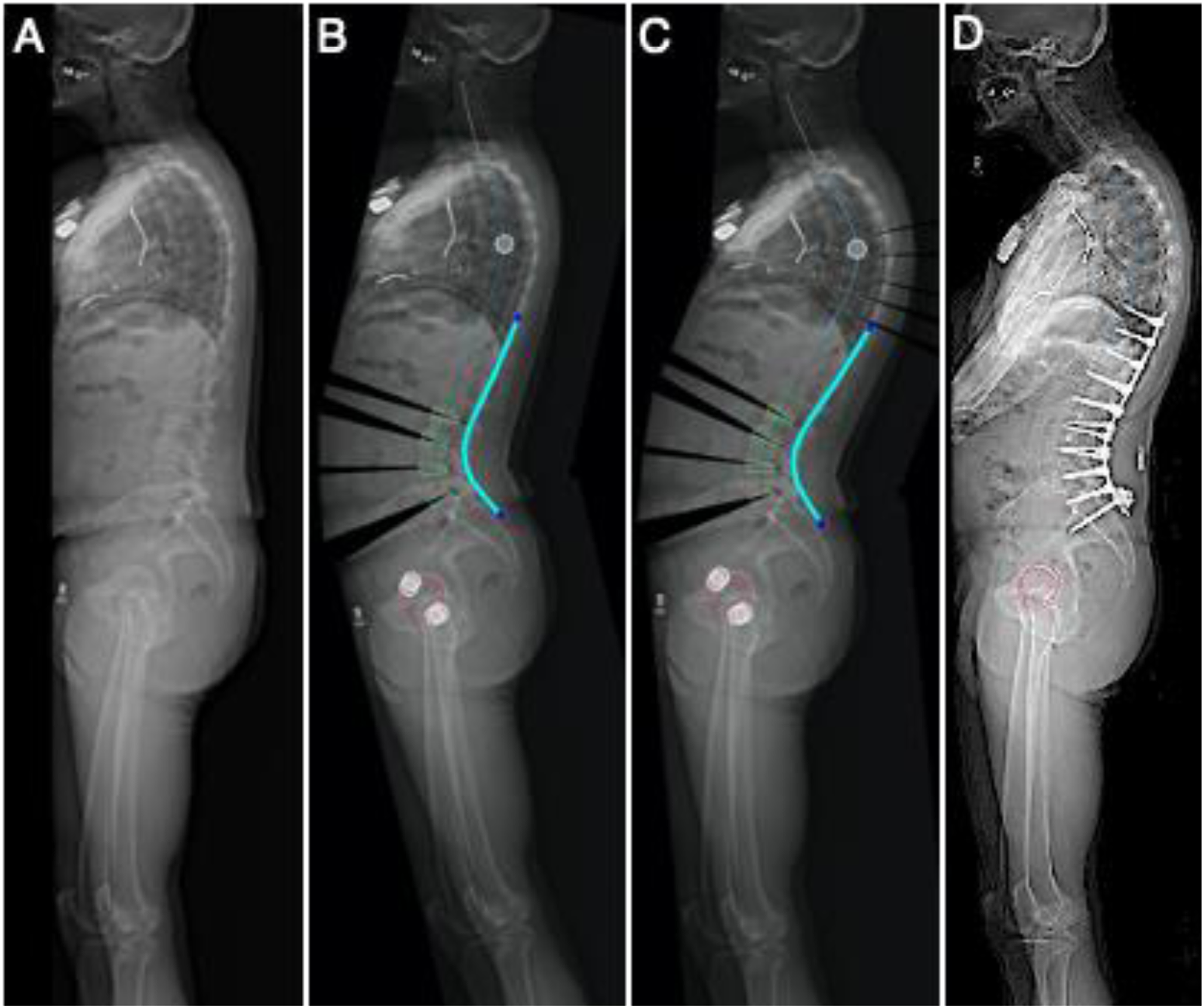
Patient who underwent T10-pelvis fusion, L2-S1 TLIFs. Pre-operative TK and PT were 35° and 27° (A) with planned TK and PT of 35° and 13° (B), predictive model TK and PT of 53° and 22° (C), and 2-year post-operative TK and PT of 54° and 19° (D). Abbreviations: PT, pelvic tilt; TK, Thoracic kyphosis.
Discussion
In addition to the improved ability to achieve and maintain appropriate alignment, other benefits of UNiD rod technology have been identified. Numerous studies have reported rod fracture rates as high as 14.9% in adult spinal deformity.9-12 Fracture rates as high as 22% have been reported in patients who underwent Pedicle Subtraction Osteotomy (PSO). In contrast, 1-year UNiD rod data on 453 patients undergoing ASD surgery revealed a rod fracture rate of 2.2% (4.7% in the 127 patients with at least 1- year follow-up having undergone a PSO.) This initial data has been presented as an abstract, and the manuscript is currently being produced for publication.
UNiD PSSR data has shown promise. However, the research has identified a recurring theme; namely that prediction of post-operative radiographic parameters such as TK and PT is difficult, and failure to do so can adversely affect both radiographic and clinical outcomes after surgery. Thus, efforts have being made to better predict immediate, subacute, and long-term post-operative TK and PT. A consecutive series of 500 patients treated for ASD was analyzed using data available within the UNiD Hub. Pre-operative, planned, and post-operative results were utilized to create a Predictive Model (PT) Algorithm for post-operative TK and PT. The predictive model was evaluated using a series of 34 patients who had previously undergone surgical treatment, and 23 patients undergoing planning for treatment of ASD.
Advancements in technology have improved our ability to plan corrective surgeries for spinal deformity. Several computer-aided systems have been developed to preoperatively simulate different corrective techniques and specific alignment goals. Unfortunately, accurate implementation of pre-operative plans in the OR remains a challenge that can prevent predictable outcomes. This has been noted in several studies comparing planned to post-operative results. Used intraoperatively, UNiD PSSRs help surgeons evaluate and fulfill their pre-operative plans accurately and reliably. The concept is a paradigm shift from the traditional teaching where rod contouring was seen as an art rather than a science; the key being doing enough correction to bring the patient to the rod and not the rod to patient.
Moreover, predictive modeling algorithms are allowing surgeons to create pre-operative plans that more accurately forecast post-operative alignment. This was demonstrated in the initial outcomes utilizing the UNiD predictive model. In addition, the UNiD technology has also been used in our institution to evaluate each individual surgeons’ ability to achieve various alignment parameters. It has also been implemented to help surgeons understand the average correction they achieve with various interbody implants and osteotomy techniques. To this point, the technology is now providing spine surgeon specific results as well as patient-specific outcomes. However, the results (while reaching statistical significance) were achieved in a small number of patients undergoing sagittal plane correction alone. Further evaluation of the predictive models, patient outcomes, and larger patient numbers are required to validate these methods.
Degenerative Cases Compared to Leveque14 Published Results.
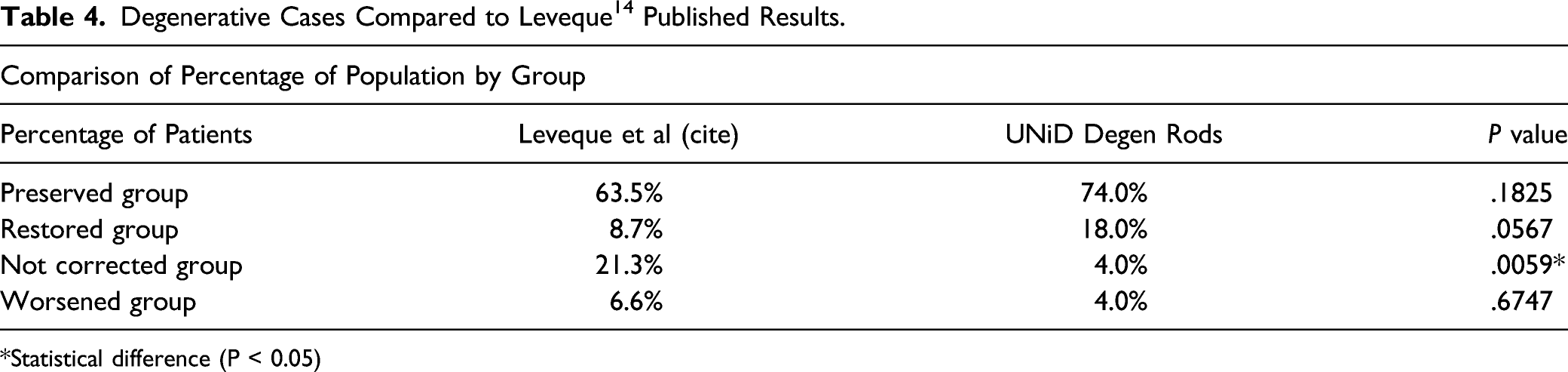
*Statistical difference (P < 0.05)
Conclusion
After review of the literature, and evaluation of a recently developed predictive model, the following key points have been identified. Patient-specific spine rods facilitate achievement and maintenance of planned correction when treating adult spinal deformity. Predictive modeling, based on computer analytics of large data sets, shows promise in the prediction of TK and PT in post-operative follow-up. Technology continues to advance and is transformational in developing patient-specific spine surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article: The research was performed as the authors’ own initiative, no industrial or other outside financial or material support was obtained.