
Abstract
Study Design
Narrative review.
Objective
Degenerative cervical myelopathy is one of the most frequent impairments of the spinal cord encountered internationally in adults. Currently, surgical decompression is the recommended treatment for people with DCM (PwCM) presenting with moderate to severe symptoms or neurological deficits. However, despite surgical intervention, not all patients make a complete recovery due to the irreversible tissue damage within the spinal cord. The objective of this review is to describe the state and gaps in the current literature on rehabilitation for PwCM and possible innovative rehabilitation strategies.
Methods
Literature search.
Results
In other neurological disorders such as stroke and acute traumatic spinal cord injury (SCI), timely and strategic rehabilitation has been shown to be indispensable for maximizing functional outcomes, and it is imperative that appropriate perioperative rehabilitative interventions accompany surgical approaches in order to enable the best outcomes. In this review, the current state of knowledge regarding rehabilitation for PwCM is described. Additionally, various therapies that have shown to improve outcomes in comparable neurological conditions such as stroke and SCI which may be translated to DCM will be reviewed.
Conclusions
We conclude that locomotor training and arm/hand therapy may benefit PwCM. Further, we conclude that body weight support, robotic assistance, and virtual/augmented reality therapies may be beneficial therapeutic analogs to locomotor and hand therapies.
Keywords
Introduction
Degenerative cervical myelopathy is a spinal cord disorder caused by degenerative changes of the vertebral column that result in chronic compression of the spinal cord. 1 Degenerative cervical myelopathy is among the most frequent causes of SCI in adults, occurring in about 2% of the adult population.2,3 While some patients may enter a period of neurological quiescence after the initial presentation, many continue to deteriorate slowly or in stepwise fashion during the period of expectant management. 4 Surgical decompression of the spinal cord is recommended for patients with symptomatically moderate to severe DCM, or for patients with progressing neurological deterioration, 5 however most patients do not achieve full neurological recovery even with successful surgical decompression. 6 Being a disease primarily associated with the process of spinal degeneration and aging, it is expected that the incidence of DCM will continue to increase in countries with aging populations and will impose a significant impact on our health and economic burden.7-11
The importance of rehabilitation in this setting cannot be overstated. Not only can rehabilitation help the disabled attain maximum function but it can also help patients regain a sense of well-being and a personally satisfying level of independence. In addition to optimizing recovery, rehabilitation also helps to minimize secondary medical conditions such as neurogenic bowel and bladder dysfunction, neuropathic pain, spasticity, cardiovascular disease, sublesional osteoporosis, among others. Furthermore, it is known that rehabilitation activities can contribute to neuroplasticity in the critical period of recovery.
Whilst rehabilitation is considered a significant component of care for many neurological conditions including stroke, traumatic brain injury (TBI), and acute traumatic (SCI), it has not yet been well propagated for DCM due to the paucity of clinical studies. 12 Furthermore, access, coverage, and quality of rehabilitation can be highly variable in different healthcare settings. 13 In DCM, there is emerging evidence 14 of potential targets for rehabilitation that could impact recovery in a substantial manner, and based on similar pathophysiology, the existing rehabilitation interventions for traumatic SCI and stroke could also potentially be translatable.
A significant number of research gaps exist in the literature for DCM, and within the AO-Spine funded RECODE-DCM project, 15 Perioperative Rehabilitation has been identified as priority #6 in the top 10 unmet research needs of DCM. The aims of this review are as follows: (1) summarize the current evidence for perioperative rehabilitation for DCM, (2) summarize examples of therapies, and their hypothesized mechanisms of action, from SCI and stroke that have transferable potential for DCM, and 3) provide an insight on potential future directions for perioperative rehabilitation for DCM.
Current Evidence in DCM and Related Neurological Disorders
Description of studies on rehabilitation for DCM.
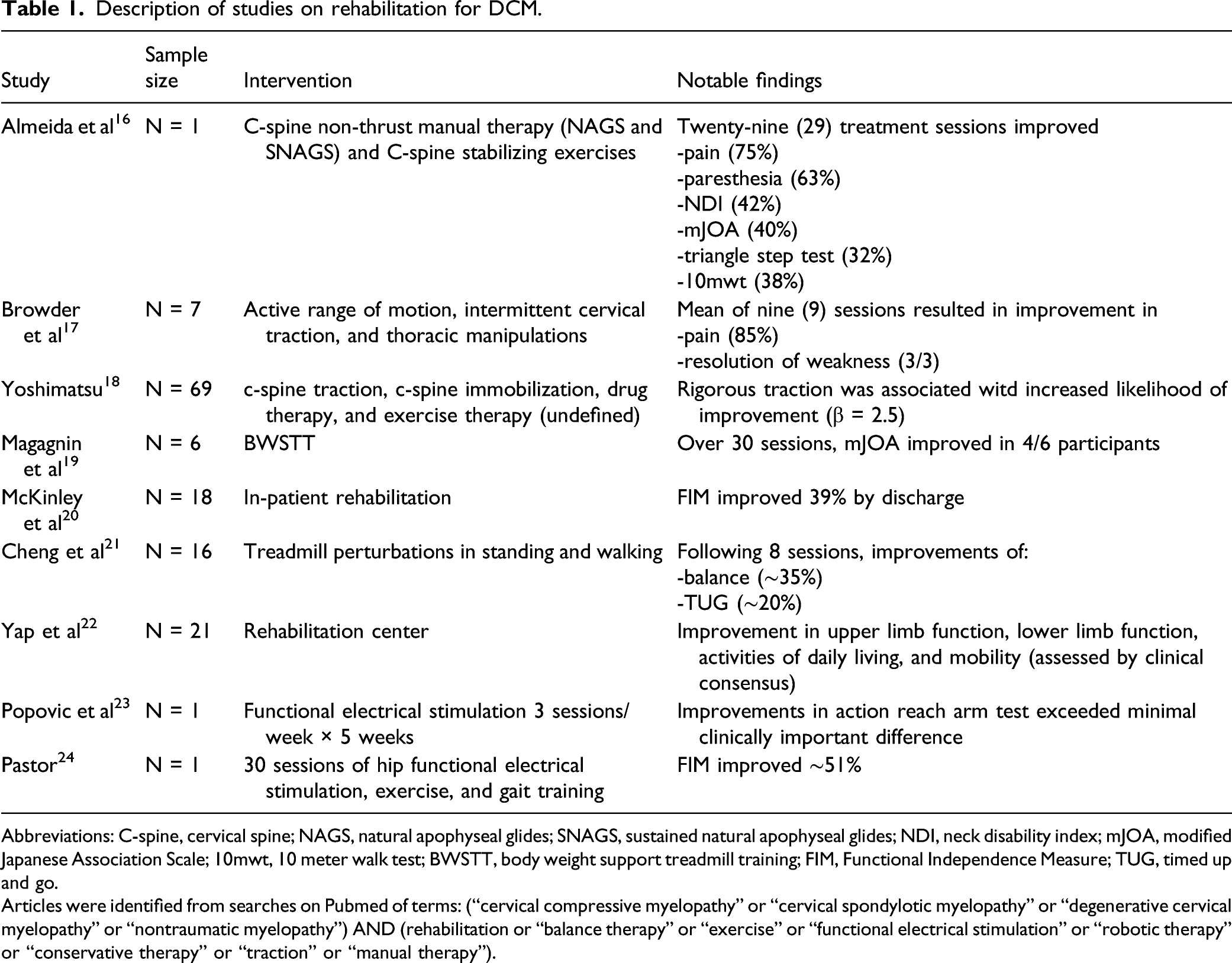
Abbreviations: C-spine, cervical spine; NAGS, natural apophyseal glides; SNAGS, sustained natural apophyseal glides; NDI, neck disability index; mJOA, modified Japanese Association Scale; 10mwt, 10 meter walk test; BWSTT, body weight support treadmill training; FIM, Functional Independence Measure; TUG, timed up and go.
Articles were identified from searches on Pubmed of terms: (“cervical compressive myelopathy” or “cervical spondylotic myelopathy” or “degenerative cervical myelopathy” or “nontraumatic myelopathy”) AND (rehabilitation or “balance therapy” or “exercise” or “functional electrical stimulation” or “robotic therapy” or “conservative therapy” or “traction” or “manual therapy”).
In contrast to DCM, there exists currently a more sizeable body of scientific evidence focusing on various rehabilitation strategies for traumatic SCI and stroke, and these efforts have resulted in meaningful changes in the current clinical practice guidelines adopted around the world. 5 These guidelines, for example, include useful recommendations on rehabilitation of locomotion and hand function, 5 and also guide us on the timing of rehabilitative intervention. While we believe that the various effects of these strategies are likely to be specific to therapeutic targets in related neurological disorders, there are parallels in DCM. For example, the clinical presentation of stroke, SCI, and DCM frequently include spastic hypertonia, reduction in hand dexterity, as well as deficits in proprioception.25-34 As such, functional rehabilitation targets such as accelerating and facilitating motor recovery, training of dexterity and selective motor control, and adaptation to loss of certain sensory modalities, are in fact ubiquitous across these several disease entities. Furthermore, rehabilitation exercises for physical maintenance of muscle bulk, preservation of joint range of motion, and prevention or reduction of nociceptive and neuropathic pain, are equally important for all those CNS insults. Studies have shown that many of the therapeutic targets in DCM such as walking, balance, and pain are largely similar to that of SCI, and more broadly stroke as well.5,35,36 In this review, we will use a framework focusing on published recovery priorities of PwCM. 37
Pain
DCM is the most frequent reason for attending pain clinics for spinal cord related neuropathic pain. 38 The neuropathic pain in PwCM is likely due to disruption of neuronal pathways as a consequence of spinal cord and nerve root compression and intrinsic damage. Amongst patients with DCM experiencing pain, neuropathic quality pain is present in over 70% of individuals. 39 Various non-pharmacological interventions have been proposed for addressing neuropathic pain, 40 including locomotor training (with or without body weight support), transcranial direct current stimulation, electrical stimulation modalities such as transcutaneous electrical nerve stimulation, transcranial magnetic stimulation (TMS), and meditation.
The beneficial effects of exercise on pain have been described in both animal models and in humans with SCI. For example, a recent meta-analysis of animal studies observed that exercise improved mechanical and thermal allodynia in SCI. 41 In humans, robotic-assisted locomotor training reduced pain intensity within a rehabilitation session and across intervention.40,42 There is growing evidence that higher intensity exercise results in more substantial improvements in mechanical hyperalgesia than lower intensity exercise. 43 Potential mechanisms of this improvement are through reductions of inflammatory cytokines in the spinal cord and endogenous opioid pathways. 43 Animal studies have shown that a gradual increase in exercise intensity over time can improve serotonin receptor expression in the spinal dorsal horn, periaqueductal gray, raphe nuclei, and noradrenergic neurons of the locus coeruleus, and improve expression of brain derived neurotrophic factor and reduced micro-glial reactivity in the locus coeruleus in peripheral nerve injury. 44 Unfortunately in spite of research on promising therapies for neuropathic pain, it appears largely unresolved in current practice. For example, one study of ratings of effectiveness of various medications by clinicians rated anti-epileptic drugs (e.g., gabapentoids) as the most effective, and it was only mildly effective or better in only approximately 30% of cases. 38 Thus, currently neuropathic pain may be under-treated by medication therapies alone and represents a particular need for further research with rehabilitation in both humans and animal models.
Walking
The evidence of locomotor training (with or without body weight support or robotic assistance) for improving walking function has been consistent in the literature for those with incomplete SCI. In the context of DCM, higher intensity training has also been shown to give rise to superior benefits. 45 While more impaired individuals may need body weight or robotic assistance, a higher intensity and dosage of locomotor training utilizing body weight or robotic support is likely to be beneficial. Research is needed in areas of actual training regimens, for example rehabilitation of individual muscle groups, dorsal column (proprioceptive) deficits, or general exercise tolerance etc.
In terms of exercise intensity, gait training in persons with incomplete neurological impairment at 70–85% maximal heart rate appears to be superior to training at 50–65% maximal heart rate for improving walking speed. 46 These improvements appear to be mediated through increased serum brain-derived neurotrophic factor and insulin like growth factors, as well in higher intensity exercise and better physical conditioning. 45 Higher intensity exercise also facilitates descending serotonin (5HT) and noradrenergic (NE) drive to the spinal cord, which is critical to increasing the gain of lower motor neurons and locomotor recovery.47,48 This facilitates increased voluntary activity of motor units, facilitating greater locomotor practice, greater re-learning, and thus greater recovery. This may be critical as evidence suggests that 5HT raphe-spinal projections are critical in the recovery of DCM post-decompression in animal models. 14
Body weight support treadmill training and robotic-assisted locomotor training have been well researched in the spinal cord literature and are recommended therapies for treatment of SCI. 5 One major benefit of robotic vs manual locomotor training is in freeing clinician time and energy while increasing the number of steps taken in locomotor practice resulting in substantial reductions in cost to deliver therapy.49,50 It appears that a critical component of locomotor recovery is delivering a sufficient sensory stimulus to the locomotor generating spinal and supraspinal circuits to facilitate healthy step-like movements to facilitate a functional reorganization of these circuits.51-53 For example, a trial using robotic locomotor therapy in patients with cervical/thoracic myelopathy due to ossification of the posterior longitudinal ligament had improvements of leg coordination during walking. 54 Proposed mechanisms of this benefit include neuronal sprouting, improvements in motor evoked potential amplitude and latencies, reduced atrophy, and improved reflex excitability.55,56 Thus, PwCM by virtue of incomplete lesions are excellent candidates for favorable outcomes with this therapy.
A recently published clinical practice guideline has identified 10 level one randomized controlled trials that demonstrated greater improvements in moderate-to-high intensity training than in low-intensity or otherwise conventional physical therapy. 81 According to this exhaustive review, it is suggested that patients with SCI, stroke, and TBI need to train with a high dosage of locomotion rehabilitation, 57 and this form of rehabilitation should be facilitated by various adjuncts such as body weight support treadmill training (BWSTT)/robotics/virtual reality wherever appropriate. 57 This approach is largely coherent with common knowledge in exercise physiology that adaptations are specific to imposed demands. 58 We also agree that more research is needed to develop activity or task specific training frameworks focusing on movement quality and skill acquisition. 59
Arm/Hand Function
Like rehabilitation for walking function, successful rehabilitation of arm and hand function is likely to involve a high intensity exercise component rather than focus on quality alone. Furthermore, exercises should be task specific.60,61 Facilitation of this through adjunctive treatments such as functional electrical stimulation (FES) and rehabilitation robotics may, however, be beneficial. Similar to BWSTT and robotic locomotor therapy, FES and arm/hand robots work to enable greater practice and have shown to be helpful in persons with CNS injuries.5,25,62 Pilot testing using robotic glove therapies have been encouraging for improving hand function and pinch grip strength, 25 and in stroke patients there is considerable research being done on robotic assisted arm and hand therapy. 63 A recent randomized controlled trial reported that greater improvements were observed with high intensity hand therapy when controlled for stroke severity. 62 Thus research on comparative effectiveness of high intensity hand therapy and robotic and/or FES assisted arm/hand therapy should carefully control for degree of myelopathic severity.
Non-invasive neuromodulatory therapies (TMS, transcranial direct current stimulation, etc.) may be employed for arm/hand function, and clinical trials following stroke suggests improvements in hand function, 64 and effects of these therapies are highly parameter specific. Future research should continue to examine stimulation frequency, dosing, as well as the simulation of functional movements.
Balance and Proprioception
For PwCM with reduced somatosensory evoked potential magnitude, vibratory therapies may be a beneficial sensory adjunct to increase the gain of sensory input. Local and whole body vibration are potential therapies that have been shown to be effective in stoke.65-67 Specifically, we now know that wrist tendon vibration during a variety of upper extremity motions can help improve end point stability and reduce proximal muscle activity65,67,68 and whole body vibrations31,33,69 can help improved overall balance. Robotic-augmented therapy focusing on sensing joint position has been shown to be useful in improving leg joint reposition sense and targeted stepping in patients with proprioceptive sensory deficits following insults to the spinal cord, 70 and robot-augmented wrist somatosensory training can improve wrist positional perception in persons with Parkinsonism. 71 Interestingly, virtual reality augmented rehabilitation has shown promise in several studies. 72 For example, semi-immersive virtual reality has been shown to result in improvements in several balance measures including the Berg Balance Scale and the Activities-specific Balance Confidence scale. 73
Sexual Function
Rehabilitation of sexual function is an area which requires a multidisciplinary approach and framework that acknowledges concerns related to biology, self-image, desire, self-confidence, as well as pharmaceuticals. Locomotion exercise has been shown to be efficacious for improving sexual function,74,75 and physical therapy plays a vital role in improving the mobility, strength, and stamina needed. 76 Unfortunately, it seems far more is known about the medical and surgical treatments of sexual dysfunction than the physical rehabilitation aspect. Some evidence does suggest that pelvic floor exercises are likely to be beneficial in improving sexual function in PwCM with erectile dysfunction, pre-mature ejaculation, arousal, orgasm, and satisfaction related problems.77,78
Bladder/Bowel Function
Bladder and bowel regulation is often overlooked as an important aspect of DCM rehabilitation. We know from evidence in spinal injuries that body weight–supported treadmill exercise has a demonstrated benefit for improving bladder and bowel function,74,79 and specifically, bladder fill capacity increases and time needed to defecate decreases following locomotor exercise.74,80 Studies have shown that after assisted locomotor training, bladder function may improve and may even become normal in up to 1/3 of individuals with SCI. 81 Additionally, pelvic floor muscle strengthening may be beneficial in treating urinary incontinence. 82 Further research is needed in the area of how exercise patterns and rehabilitation strategies affect peristalsis, bowel regularity, and sphincter control in patients with DCM.
Spasticity
With regard to spasticity, several potential therapies exist showing promise in other comparable neurological diseases, for example TMS, locomotor training, and vibration therapies.42,83 In a recently published meta-analysis, TMS demonstrated greater effectiveness in reducing spasticity for SCI compared to a sham procedure. In one particular study by Benito et al, 84 the authors demonstrated a 40% reduction in spasticity coherent with the overall reduction in spasticity of the meta-analysis. Thus, based on the similar pathophysiology of an upper motor neuron lesions causing spasticity, we believe that TMS should be closely examined as a part of a rehabilitation program for DCM.
Similarly, a recent systematic review of robotic assisted locomotor training demonstrated a trend in the literature for reducing spasticity with robotic locomotor training. 42 In this review, 42 the methods to assess spasticity were varied between clinician-generated measures (such as the modified Ashworth scale) and other self-reported metrics. Further research is warranted on the effectiveness of robotic locomotor training on reducing spasticity in PwCM.
Mental Health, Quality of life, and Economics
One domain not described in the published recovery priorities of DCM, 37 but of paramount importance is mental health. Depression and anxiety are relatively common in PwCM prior to surgery and those who have depression have worse recoveries of function and mental health following decompression.85,86 PwCM reportedly have worse mental health related quality of life than people with depression, angina, osteoarthritis, cancer, congestive heart failure, diabetes, myocardial infarction, chronic lung disease, and multiple sclerosis.87,88 Recent small scale studies on locomotor training with FES and robotic assistance demonstrated improvements in mental health related quality-of-life in SCI,89,90 and likewise high intensity body weight support locomotor training has also been shown to improve quality of life in people with Parkinsonism. 91 By virtue of improving walking ability, locomotor training may reduce home renovation costs by >US$50,000/person and also substantially reduce lifetime healthcare costs in more impaired individuals.,81,92 thus easing these patients’ overall disease burden. PwCM remain at increased risk of falls and fragility fractures, and due to their sedentary lifestyles they are also prone to developing coronary artery disease, arrhythmias, and strokes.93-96 Considering that DCM impacts ∼2% of the population, proper perioperative rehabilitation has immensely important role to positively impact mental health, quality of life, and personal and societal economics throughout the lifespan. We believe that more research is needed on the actual healthcare savings from the biological benefits gained from various rehabilitation strategies in PwCM. To this end, recent health economic investigations have been conducted related to surgery for PwCM,97,98 and these efforts need to be replicated for perioperative rehabilitation. Of critical, need will be examinations of appropriate timing, intensity, and type of therapies with respect to reducing cost to PwCM, healthcare systems, and society at large.
Emerging Therapies
Ischemic Conditioning
A complimentary therapy emerging in the literature for central nervous system conditions is that of remote ischemic conditioning (IC)—a technique of applying a blood pressure cuff for 5 minutes repeatedly at ischemic pressures. Similar to high intensity exercise, IC acts through humoral, neural, and anti-inflammatory gene up-regulating mechanisms. 99 Ischemic conditioning is believed to facilitate 5HT and NE drive to the spinal cord by producing a build-up of bradykinin, nitric oxide, and other markers of ischemia.99,100 These stimulate thinly and/or unmyelinated group III/IV afferents.99,100 This intervention results in increased sympathetic outflow (which is reduced in PwCM) and stimulates the release of 5HT via the raphe nuclei.99-101 As plasticity of the 5HT raphe-spinal projections are critical in the functional recovery of DCM, 14 IC may facilitate greater motor recovery in DCM. Specifically, in the context of stroke, 7 sessions of IC over 2 weeks resulted in improvements in walking speed and quadriceps exercise endurance time. 102 This was without any other contributing therapy. 102 Importantly, IC resulted in increased gait speed on average equal to the minimal clinically important difference for persons chronically post stroke. 102 Similarly, IC has resulted in improvements in 6-minute walk distance in persons with multiple sclerosis. 103 Thus, IC is an emerging therapy with strong potential to facilitate improved walking speed and endurance in PwCM.
Intermittent Hypoxia
A therapy conceptually similar to ischemic conditioning, it involves alternating breathing air with lower levels of oxygen and normally oxygenated air, and has been shown to be a promising new intervention104-106 which can enhance spinal cellular plasticity evidenced by elevation of brain derived neurotrophic factor and vessel endothelial growth factor. 107 In individuals with injury to the spinal cord, intermittent hypoxia has been shown to increase ankle strength, walking speed, walking endurance, and improve walking balance.104-106 Because intermittent hypoxia also facilitates release of 5-HT, at least to the cervical phrenic motor nuclei, it would likely have additive benefits to other therapies discussed here. 108
Virtual and Augmented Reality
Virtual and augmented reality in rehabilitation has recently become another popular research interest including the field of neuro-rehabilitation. A systematic review recently identified 25 studies examining virtual reality within the context of SCI research alone over the last 20 years. 72 Statistically significant improvements in motor function were noted in 15/17 studies, in aerobic function in 3/3 studies, in balance in 8/10 studies. 72 Notably, however, most (18/25) had a high risk of bias, lower levels of evidence, and lower PEDro scores due to be combinations of non-randomized, non-controlled, and non-blinded. 72 As physical, aerobic, and balance function are all necessary components of walking, virtual reality assisted therapy may be a vital component of successful physical therapy for DCM.
Neuromodulatory Stimulations
One further therapy that should be considered is that of neuromodulatory stimulation therapies such as transcranial direct current stimulation and TMS. One recent systematic review of 8 studies involving individuals post stroke, with Parkinsonism, and SCI reported inconclusive evidence for improving walking beyond gait therapy. 109 Repetitive TMS, however, may improve walking speed in individuals post stroke. 110 Therefore, the evidence for these therapies even in the broader neuro-rehabilitation field is yet inconclusive.
Future Directions
There is converging evidence to suggest that high intensity locomotor training has potential for multi-domain improvements for PwCM. It has been implicated as a potential therapeutic agent in every facet of recovery for PwCM. Yet only 2 cohort studies have examined this in DCM.19,21 These studies observed improvements in bladder/bowel function with robotic-assisted locomotor training and balance with perturbation training during walking.19,21 Thus, there appears ample potential to translate the above-mentioned therapies already demonstrating promise in SCI, stroke, and MS to DCM.
When examined closely, there is substantial convergence in the neurological rehabilitation literature surrounding the importance of the serotonergic and noradrenergic systems. That is, serotonergic raphe–spinal pathways are critical to recovery of DCM and are implicated in recovery of neuropathic pain, walking, and are also important for trunk function.14,47,111 Locomotor training and IC stimulate these pathways44,47,99 making these both sound mechanism based therapies for DCM.
Locomotor training and IC represent well-supported and emerging therapies, respectively, targeting the serotonergic and noradrenergic systems, that are critical to the recovery of DCM. However, therapeutic adjuncts such as BWSTT/robotics and FES may be highly beneficial in facilitating greater active practice and increased dosage.19,50,55,112-116 Additionally, virtual/augmented reality incorporated into rehabilitation may help to reverse the known overreliance on vision for balance in DCM and improve the “reality” of gait training.29,73,117-119 Virtual reality, or mechanical, balance training combined with gait training may have a combinatorial benefit for balance and walking without increasing therapy time.21,72,120-122
Increased benefits of locomotor training occur with intensity.45,46,123,124 Thus, special emphasis for future research should be placed on evaluating most important intensity to achieve optimal therapeutic outcomes. Given the dearth of research on peri-operative rehabilitation, substantial research is needed on all parameters of every therapy investigated. High quality, well-controlled randomized trials must be encouraged to accomplish this research priority.
There are numerous other therapies not included in this review for various therapeutic targets that have demonstrated mixed effectiveness in patients with spinal cord impairments. TMS and transcranial direct current stimulations are 2 such therapies. These are often examined in the context of neurological injury; however, a recent meta-analysis found there was no effect of either on neuropathic pain. 125 Thus, while TMS may be effective in treating spasticity, 83 its effectiveness outside this target may be limited. Other therapies, such as transcutaneous electrical stimulation, and acupuncture, have few studies showing effectiveness or the research is of very low quality.126,127 Certainly these therapies may warrant investigation in DCM; however, there appears to be insufficient evidence to provide firm research recommendations.
Conclusions
The direct evidence of the benefits of peri-operative rehabilitation is sparse. However, there is ample evidence from the broader neurological field to recommend substantial research into locomotor training, arm/hand therapy in conjuncture with body weight–supported treadmill training, robotic-guided rehabilitation, virtual/augmented reality, and FES as a means of peri-operative physical therapy. Therapies such as ischemic conditioning may prove to be promising adjuncts. Finally, strategies focusing on psychological rehabilitation and quality of life for patients with DCM must not be overlooked. Therefore, we conclude that well-structured clinical trials on the benefits of peri-operative rehabilitation (including locomotor training and hand therapy supplemented with robotics, body-weight support, virtual reality, and/or FES) are needed to improve outcomes in PwCM.
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research priorities were organized and funded by AO Spine through the AO Spine Knowledge Forum Spinal Cord Injury, a focused group of international Spinal Cord Injury experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically guided not-for-profit organization. Study support was provided directly through the AO Spine Research Department. MRNK is supported by the National Institute for Health Research (NIHR) Brain Injury MedTech Co-operative based at Cambridge University Hospitals NHS Foundation Trust and University of Cambridge, and BMD a NIHR Clinical Doctoral Research Fellowship. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health and Social Care. This report is independent research arising from a Clinician Scientist Award, CS-2015-15-023, supported by the National Institute for Health Research. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health and Social Care.