
Abstract
Study Design/Setting:
Systematic review/meta-analysis.
Objectives:
The objective of this review was to assess how the risk of infection following lumbar spine surgery varies as a function of the timing of preoperative corticosteroid spinal injections (CSIs).
Methods:
A systematic review and meta-analysis was performed in accordance with the PRISMA guidelines. PubMed and EMBASE databases were searched and data was pooled for meta-analysis.
Results:
Six studies were identified for inclusion. Two (33.3%) demonstrated a significant relationship between the timing of preoperative CSIs and the risk of postoperative infection, while 4 (66.7%) demonstrated no impact. A total of 2.5% (110/4,448) of patients who underwent CSI <1 month before surgery experienced a postoperative infection, as compared to 1.2% (1,466/120, 943) of controls, which was statistically significant (RR = 1.986 95% CI 1.202-3.282 P = 0.007). A total of 1.6% (25/1,600) of patients who underwent CSI 0-3 months before surgery experienced a postoperative infection, as compared to 1.6% (201/12, 845) of controls (RR = 0.887 95% CI 0.586-1.341, P = 0.569). A total of 1.1% (199/17 870) of patients who underwent CSI 3-6 months before surgery experienced a postoperative infection, as compared to 1.3% (1,382/102, 572) of controls (RR = 1.053 95% CI 0.704-1.575, P = 0.802). Differences in infection risk for 0-3 months and 3-6 months were not statistically significant.
Conclusions:
CSIs <1 month prior to lumbar spine surgery are a significant risk factor for infection, while CSIs beyond that point showed no such association. Surgeons should consider avoiding CSIs <1 month of the use of CSIs of the spine.
Introduction
Corticosteroid spinal injections (CSIs) play an important role in the management of back pain and radicular pain associated with facet arthropathy, intervertebral disc herniation, spinal stenosis, and other degenerative conditions of the spine.1-7 Roughly 2.3 million CSIs are performed annually among Medicare patients alone, making them the most commonly performed procedure in pain clinics in the United States. 8 The popularity of CSIs is largely driven by their diverse utility as a diagnostic and prognostic tool, in addition to their therapeutic role in the treatment of spine pathology. As a diagnostic and prognostic intervention, CSIs provide valuable information to the surgeon and patient regarding the source of back and radicular symptoms, as well as the likelihood of response to surgical intervention. Furthermore, while CSIs are rarely used as definitive treatment for back and radicular pain, they are frequently used as a temporary bridging measure in patients who may eventually require surgical management.4-6,9
Given the value of CSIs, it is estimated that roughly 10%-20% of patients undergo CSIs during their preoperative course prior to definitive surgical management.10-12 Despite the ubiquity of this treatment modality prior to surgery, however, there is growing debate as to the impact of CSIs on the subsequent risk of infection following surgical intervention. While corticosteroids have the beneficial impact of interfering with the immune pathways responsible for inflammation and pain, these same pathways are responsible for the immune response to infectious agents. Through inhibition of pro-inflammatory pathways like the prostaglandin and cyclo-oxygenase pathways, mRNA and protein synthesis, and white blood cell activity, steroids can decrease the body’s ability to fight pathogens and increase the risk of infection.13,14 While the risk of infection associated with CSIs has been documented in both epidural steroid injections (ESI) and facet injections,15-27 recent reports suggest that preoperative CSIs may also increase the risk of postoperative spine infections. Multiple studies have demonstrated that undergoing a CSI within 0-6 months of surgical treatment is a significant risk factor for infection. Given the significant morbidity and cost associated with postoperative infection, these studies have strongly recommended against the administration of CSIs within 3 months of operative treatment.28-32 However, many of these studies are case reports or case series that fail to reach the adequate number of patients necessary to draw definitive conclusions, which is a source of controversy.
Concerns regarding the impact of preoperative CSIs on subsequent surgical infection risk are not unique to spine surgery. In fact, preoperative CSIs have been identified as a risk factor for postoperative infection in a wide variety of orthopaedic procedures, from shoulder and hip arthroscopy, to total shoulder and total joint arthroplasty (TJA).33-45 Based on these findings, it is commonplace in the field of TJA, for example, to delay operative treatment for 3 months following intraarticular CSI.42,46 Even in the field of TJA, however, where these practices are largely standard-of-care, the growing number of studies, systematic reviews, and meta-analyses refuting this association have caused some to take pause and reassess the validity of this commonly held practice.47-50
Much like the field of TJA, there is mounting evidence in the field of spine surgery that questions the association between the timing of preoperative epidural and facet injections and postoperative spine infection.2,10-12,51,52 Such studies demonstrate that, even in the months leading up to surgery, CSIs do not appear to increase the risk of infection. Given the morbidity associated with untreated spine pathology and the relative urgency of treating certain spine conditions, the ability to deliver CSIs for pain relief in closer proximity to surgery would be of great therapeutic value. An improved understanding of the association between the timing of CSI prior to surgery and infection risk is therefore extremely important in order to optimize the risk-benefit profile of this important tool. The goal of the current study was to perform a systematic review and meta-analysis of the available literature to examine the effect of timing of preoperative CSI administration on postoperative infection risk in spine surgery.
Materials & Methods
Search Strategy
This systematic review and meta-analysis was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 53 The EMBASE and PubMed databases were searched on July 13th, 2020 utilizing a broad search strategy in order to maximize identification of the relevant literature. The following search strategy was used: “spine AND surgery AND injection AND infection.” No publication type limits or date restrictions were applied to our initial search.
Following the development of a reference library, results were imported into EndNote X7 (Thomas Reuters, 2015) and duplicates were removed as previously described by Bramer et al. 54 Following de-duplication, articles were screened by title and abstract in order to identify studies pertaining to the current review. Articles that appeared relevant were marked for full-text review and screened further based on the inclusion/exclusion criteria for this review.
Eligibility Criteria
The inclusion criteria for this study were as follows: 1) peer-reviewed journal publications, 2) assessed primary lumbar spine surgical intervention, 3) and specifically assessed the impact of preoperative CSI timing on subsequent risk of postoperative infection.
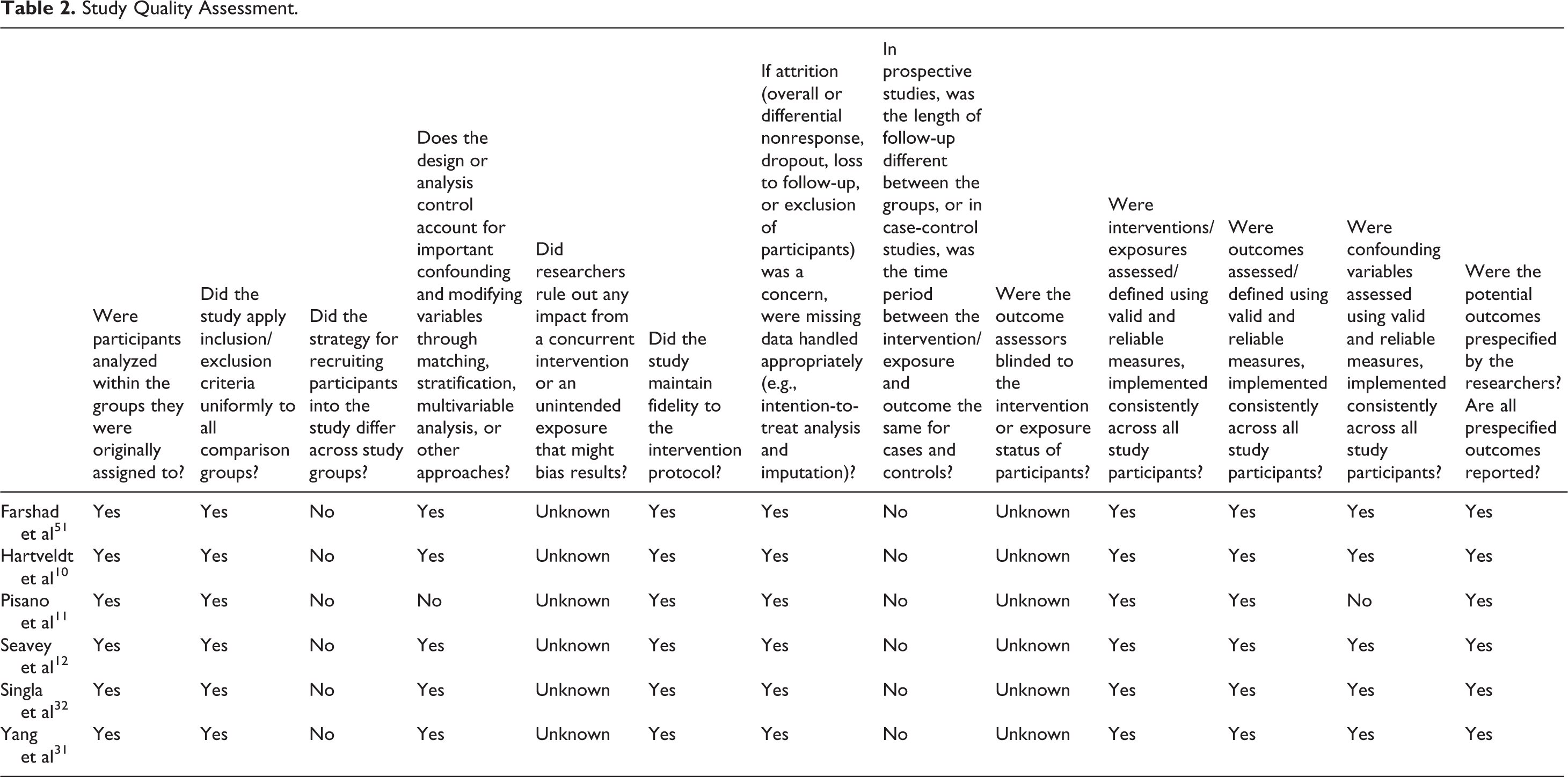
The exclusion criteria for this study were as follows: 1) revision spine surgery, 2) review, systematic review, meta-analysis, or case report, 3) no description of the timing of CSI relative to the index procedure (even if the association between CSI and infection risk was studied), 4) not a peer-reviewed journal publication (such as a conference poster or presentation), 5) analyzed the same data as a different study in the published literature, or 6) only assessed non-lumbar spine surgery (cervical, thoracic, etc.). No restrictions were made based on the location, level, approach, or technique of the surgical intervention under study. Quality assessment was performed based on the study-design-specific guidelines for the assessment of study bias published by the Agency for Healthcare Research and Quality (AHRQ). 55 Assessment of study quality can be found in Table 2.
Meta-Analysis
After systematically reviewing the available literature, clinically relevant data was aggregated for meta-analysis. Data regarding postoperative infection as a function of preoperative CSI timing was aggregated for the following timing groups: CSI <1 month before surgery, CSI 0-3 months before surgery, and CSI 3-6 months before surgery.
Statistical analysis was performed using OpenMetaAnalyst (2018) software. 56 Infection rates were assessed using a binary-effects model, and were presented as risk ratios (RR) and 95% confidence intervals (CI) for comparison. Heterogeneity was assessed for each variable using the I 2 statistic (I 2 = 0% indicates low heterogeneity; I 2 = 100% indicates high heterogeneity) for the 3 CSI timing groups. Groupings with statistically significant levels of heterogeneity (P < 0.05) were assessed using the DerSimonian-Laird random effects model. When heterogeneity was not statistically significant, a fixed-effect inverse variance model was used. A “leave-out” meta-analysis, in which included studies are sequentially dropped out of the analysis and results are interpreted in their absence, was also performed for each timing group in order to determine if the omission of any single study had the ability to change the outcome of our meta-analysis.
Results
Search Results
Our search identified 349 studies from EMBASE and 326 from PubMed for a total of 675 results. A total of 60 duplicate results were identified and eliminated, yielding 615 unique results. These results were then screened for inclusion according to the study inclusion/exclusion criteria using study title and abstract, which yielded 24 studies for full-text review. From this list, 6 studies were included in our final analysis. While a study by Donnally et al 29 fit the inclusion criteria for our meta-analysis, it described the same data from the same database (same CPT codes from PearlDiver) as Yang et al. 31 Because Yang et al 31 included one additional CPT code compared to Donnally et al, 29 we chose to include this study over Donnally et al 29 in order to avoid omitting any of the available data in the literature. The results of our search are demonstrated in the PRISMA flow diagram in Figure 1. A summary of the studies included in this systematic review is demonstrated in Table 1.
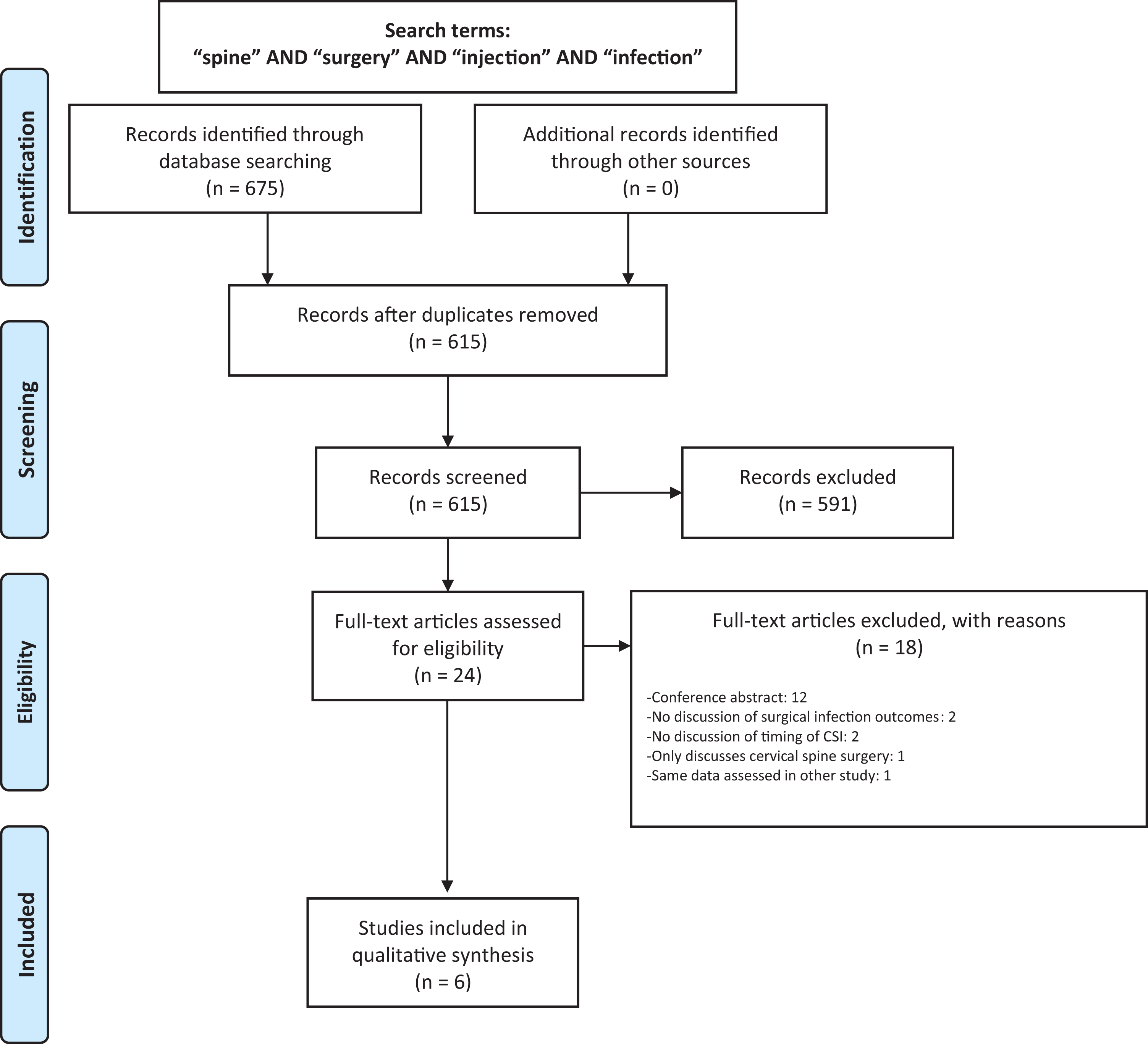
PRISMA flow diagram. A total of 6 studies were included in the final systematic review.
Summary of Studies Included in the Systematic Review.
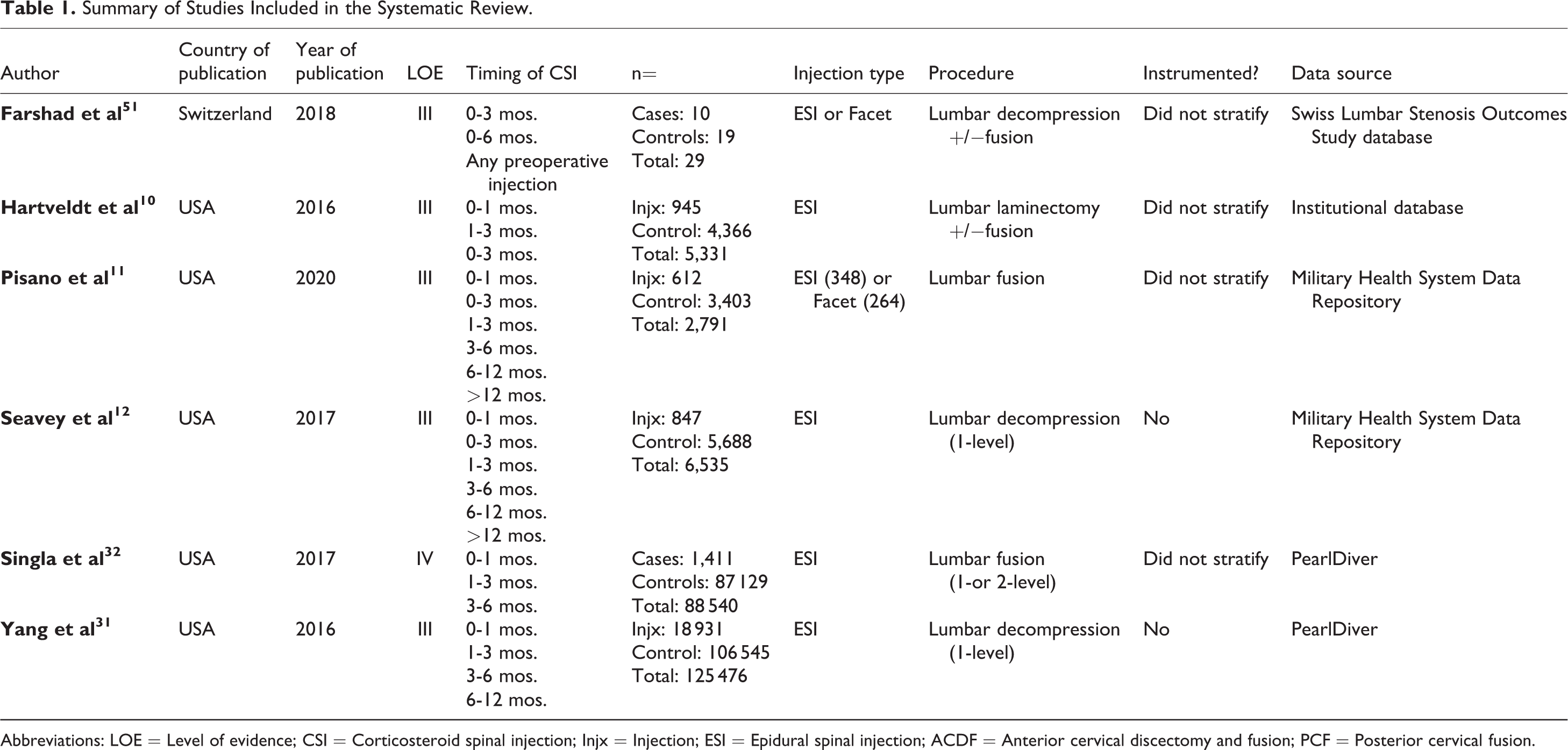
Abbreviations: LOE = Level of evidence; CSI = Corticosteroid spinal injection; Injx = Injection; ESI = Epidural spinal injection; ACDF = Anterior cervical discectomy and fusion; PCF = Posterior cervical fusion.
Study Quality Assessment.
Systematic Review
Of the 6 studies identified for review, 4 (66.7%) assessed the impact of ESIs on infection risk, while 2 (33.3%) assessed the risk of both ESIs and facet injections Table 1.
A total of 2 (33.3%) studies demonstrated a significant relationship between the timing of preoperative CSIs and the risk of postoperative infection,31,32,57 while 4 (66.7%) demonstrated no impact.10-12,51 Singla et al 32 and Yang et al 31 found a significant increase in the risk of infection if CSIs were performed <1 month before surgery (P < 0.0001) or 1-3 months before surgery (P < 0.0002) in patients undergoing 1-or 2-level lumbar fusion or 1-level decompression, respectively. Though the results of Donnally et al 29 were not included in our meta-analysis due to the fact that they discuss the same data as Yang et al, 31 this study found no increase in risk associated with CSIs occurring <1 month before lumbar decompression and fusion, but that CSIs performed 1-6 months prior to surgery were associated with a significant increase in the risk of infection (P < 0.001). In opposition to these findings, Farshad et al, 51 Hartveldt et al, 10 Pisano et al, 11 and Seavey et al 12 found no impact of CSI timing on infection risk, including injections occurring 0-1 month and 0-3 months prior to surgery. A summary of these study findings is demonstrated in Table 3.
Summary of Results.a
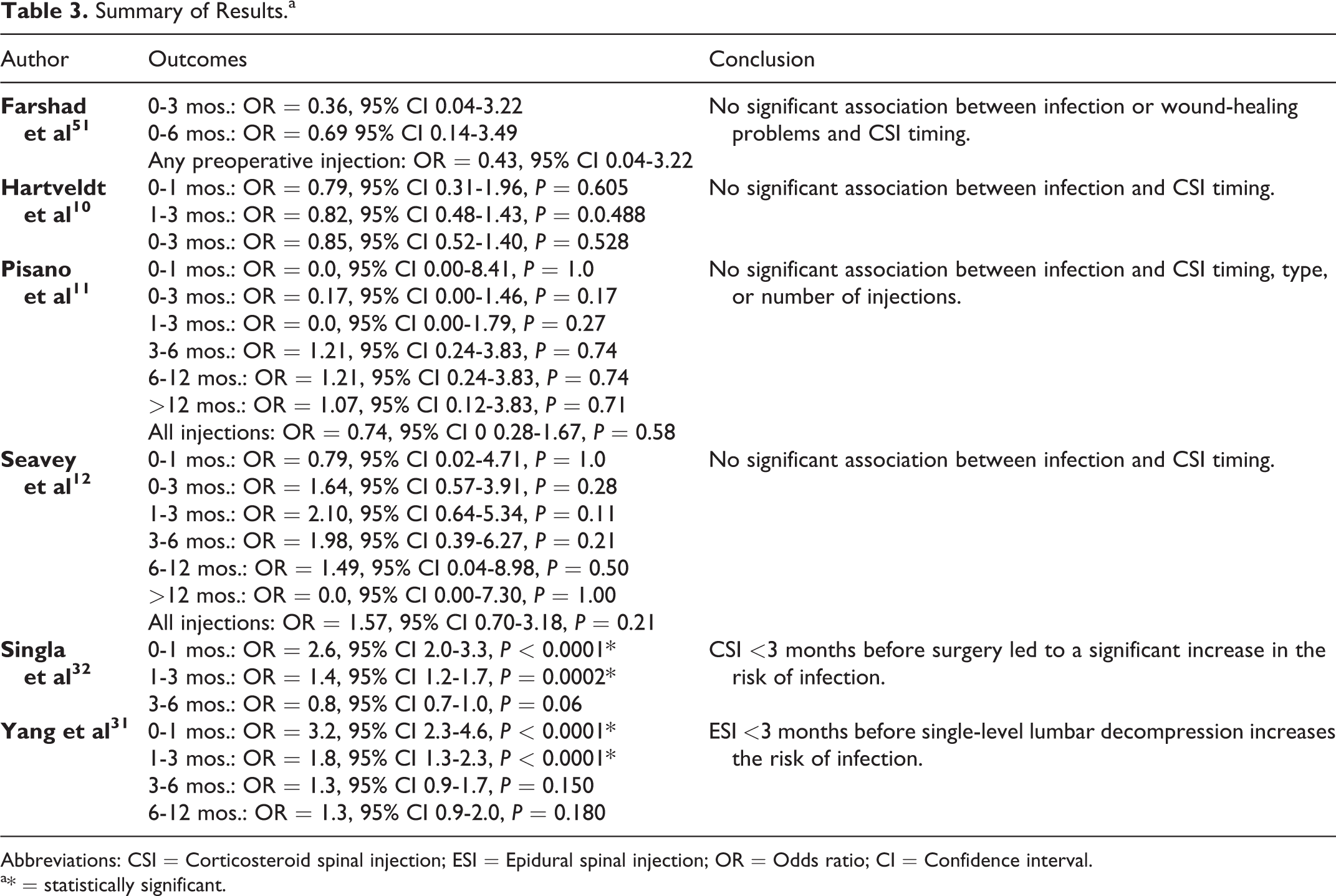
Abbreviations: CSI = Corticosteroid spinal injection; ESI = Epidural spinal injection; OR = Odds ratio; CI = Confidence interval.
a* = statistically significant.
Meta-Analysis
Five studies10-12,31,32 were included in the meta-analysis of postoperative infection risk following CSIs <1 month before surgery. A total of 2.5% (110/4,448) of patients who underwent CSI <1 month before surgery experienced a postoperative infection, as compared to 1.2% (1,466/120 943) of controls (Table 4), representing a statistically significant increase in infection risk (RR = 1.986 95% CI 1.202-3.282 P = 0.007) (Table 5). Forest Plots are shown in Figure 2.
Summary of Data Included in the Meta-Analysis.
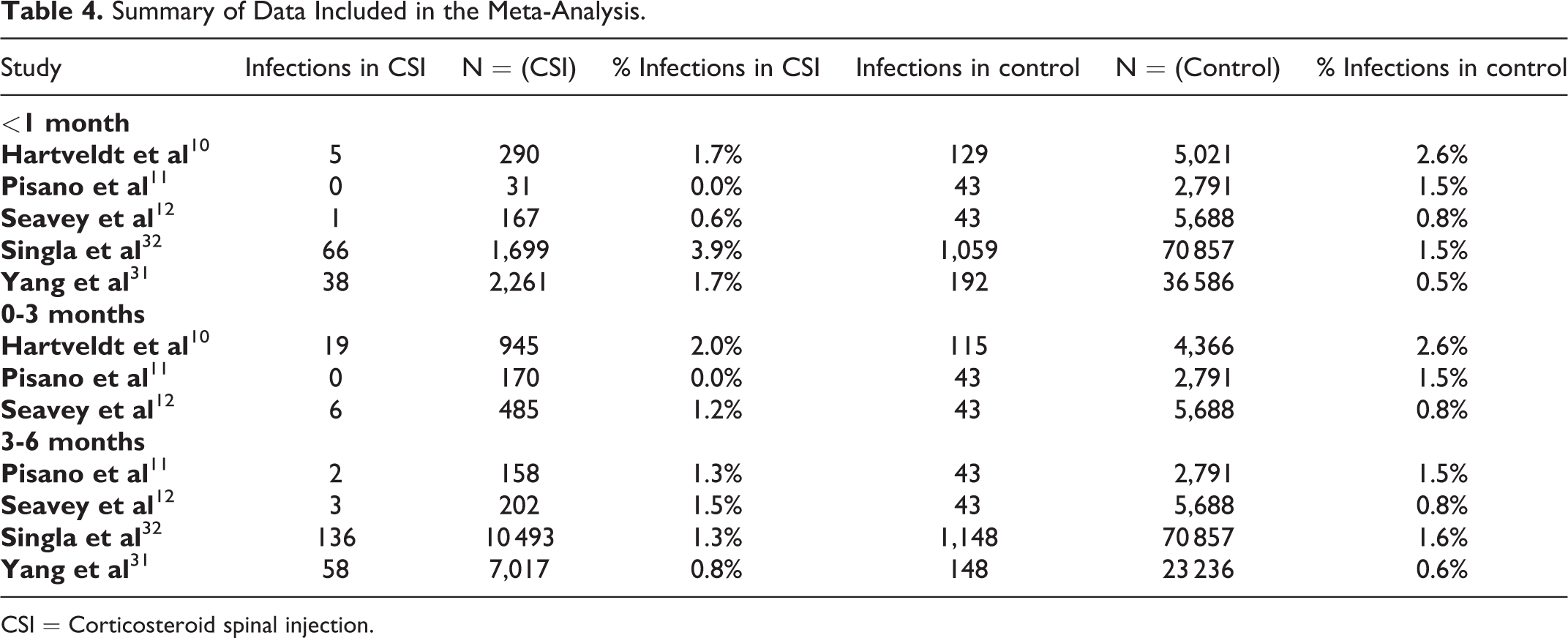
CSI = Corticosteroid spinal injection.
Results of Meta-Analysis. Summary of Meta Analysiis.

Abbreviations: CSI = Corticosteroid spinal injection; RR = Relative risk; CI = Confidence interval.
a indicates a statistically significant level of heterogeneity, necessitating a random-effects model; bindicates a statistically significant difference between the CSI and control groups in the meta-analysis.
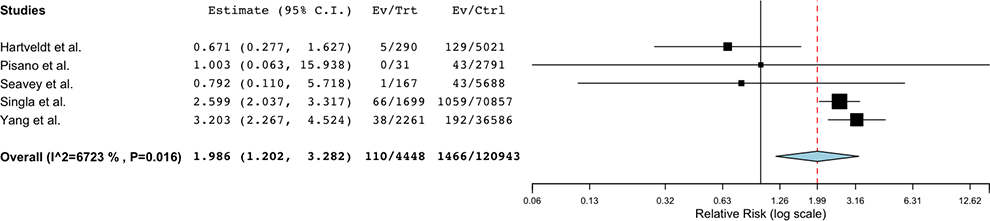
Forest plot comparing the risk of postoperative spine infection following CSI <1 month preoperative compared to controls.
Three studies10-12 were included in the meta-analysis of postoperative infection risk following CSIs 0-3 months before surgery. A total of 1.6% (25/1,600) of patients who underwent CSI 0-3 months before surgery experienced a postoperative infection, as compared to 1.6% (201/12 845) of controls (Table 4), which was not statistically significant controls (RR = 0.887 95% CI 0.586-1.341, P = 0.569) (Table 5). Forest Plots are shown in Figure 3.

Forest plot comparing the risk of postoperative spine infection following CSI 0-3 months preoperative compared to controls.
Four studies11,12,31,32 were included in the meta-analysis of postoperative infection risk following CSI 3-6 months before surgery. A total of 1.1% (199/17 870) of patients who underwent CSI 3-6 months before surgery experienced a postoperative infection, as compared to 1.3% (1,382/102 572) of controls (Table 4), which was not statistically significant (RR = 1.053 95% CI 0.704-1.575, P = 0.802) (Table 5). Forest Plots are shown in Figure 4.
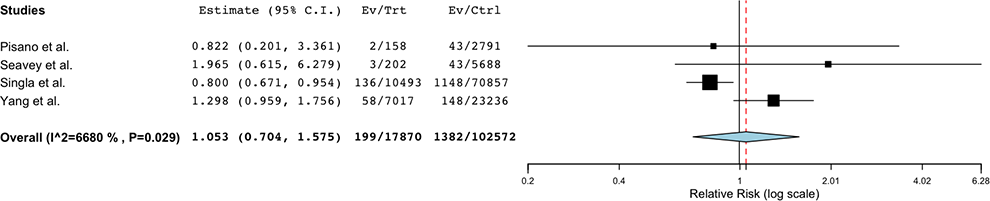
Forest plot comparing the risk of postoperative spine infection following CSI 3-6 months preoperative compared to controls.
In the “leave-out” meta-analysis, eliminating the results of Singla et al 32 and Yang et al 31 both independently reversed the outcome of the meta-analysis, indicating that exclusion of these studies would eliminate the observed finding that CSIs <1 month prior to spine surgery augment the risk of infection (Table 6). “Leave-out” meta-analysis demonstrated no changes in the statistical significance in assessments of 0-3 or 3-6 months.
“Leave-Out” Meta-Analysis for the CSI <1 Month Preoperative Grouping.
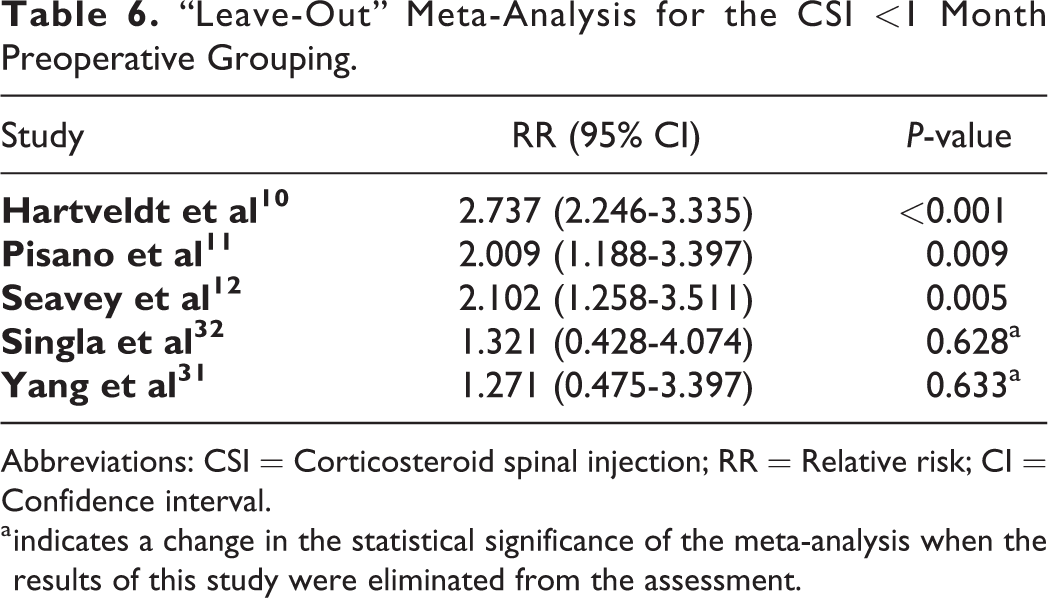
Abbreviations: CSI = Corticosteroid spinal injection; RR = Relative risk; CI = Confidence interval.
a indicates a change in the statistical significance of the meta-analysis when the results of this study were eliminated from the assessment.
Discussion
The timing of CSIs prior to spine surgery has been a matter of substantial debate. As potent immunosuppressants, CSIs may diminish a host’s defense against exogenous infectious organisms and endogenous bacterial skin fauna, predisposing the patient to postoperative infection. It has been theorized that CSIs can also lead to epidural scarring, hypervascularization, and local degeneration, which may serve as independent risk factors for infection or may promote intraoperative surgical deviations and complications that may also raise the risk of infection.28,57,58 The data on CSI timing and infection is varied. Some have argued that CSI <3 months prior to surgical intervention exposes the patient to an increased risk of infection postoperatively,29,31,32 while others report that this risk is increased even at 3-6 months prior to surgery. 29 Still, others have found no risk associated with the timing of preoperative CSIs,10-12,51 even with injections occurring <1 month preoperatively.11,12,59 Given this conflicting data, the true impact of the timing of preoperative CSIs on infection risk is unclear.
In the current systematic review and meta-analysis, we found a relative paucity of literature describing the impact of preoperative CSI timing on subsequent postoperative infection risk. While 33.3% of the studies identified an increased risk associated with CSIs, this effect was mediated by the timing of administration preoperatively. All studies found that injections >3 months prior to surgery were not associated with an increased risk of infection. Though the literature demonstrated mixed results with respect to the impact of injections during the period <3 months prior to surgery, the results of our meta-analysis demonstrated that injections performed during the 0-3 month period had no impact on infection risk. However, our meta-analysis did demonstrate an increased risk of infection when assessments were restricted to injections performed solely <1 month prior to surgery. Based on these findings and limited data, we recommend consideration of delaying surgery in patients who underwent a CSI <1 month prior to the proposed date of surgery. However, we recommend against limiting the use of CSIs in the 1-3 month preoperative period, since our data analysis suggests there is no appreciable increased risk for infection in this time period.
While the overall risk of infection following lumbar spine surgery is low, the increased risk of infection associated with ESI within 1 month of surgery is not trivial. Surgical site infections are associated with significant patient morbidity, with a risk of vertebral osteomyelitis, discitis, and epidural abscesses, which can lead to chronic pain, chronic infection, neurologic deficits, disseminated infection, and death. Logistically speaking, these infections also lead to increased hospital costs, length of stay, and hospital readmission rates.60-64 Due to the large number of lumbar spine procedures performed in the US and across the globe each year, the absolute increase in the number of infections associated with this treatment strategy is likely significant.
However, it is important to note that the output of a meta-analysis is generally only as accurate as the input data that was used to derive the analysis. In the case of the current meta-analysis, there is a large potential source of bias among the studies demonstrating an impact of CSI timing on subsequent postoperative infection risk. Namely, the 2 studies identifying an association between injection timing and infection risk used data from the same national Medicare database, PearlDiver. As demonstrated in our “leave-out” analysis, elimination of either of the PearlDiver-derived studies has the ability to eliminate the association between infection and CSIs in the <1 month preoperative period. Therefore, the results of the current analysis are susceptible to large deviation due to any underlying errors in this input data. While this database is a frequently used and trusted source of orthopaedic data, the fact that the only studies demonstrating a link between the timing of CSIs and postoperative infection utilized this source is concerning. Additionally, 2 PearlDiver studies that did not meet the inclusion criteria of this meta-analysis, also found a relationship between the timing of CSIs and infection risk.29,65 It is possible that, whether a function of the way the dataset is coded or a function of the patient population included in this database, there exist underlying confounders that skew the data toward demonstrating a link between the timing of preoperative CSIs and infection. Sources of this potential error include miscoding and noncoding among physicians, which has been demonstrated to lead to national coding error rates of 3.9% in Medicare databases. 66 The notion that underlying confounders may skew the data in PearlDiver toward demonstrating a positive association between CSI and infection is partially supported by the finding that PearlDiver-derived analyses regarding the timing of CSI prior to arthroscopic shoulder surgery and TKA, for example, are also among the only studies to identify a link between CSI and subsequent postoperative infection in these fields.37,39-42,44,45,67,68
There are other limitations to the current systematic review and meta-analysis. Because much of the data included in the current study was from large registry databases, it is difficult to perform sub-group analyses to identify risk factors and drivers that may modulate the risk of infection following CSI. The ability to identify differences in risk between epidural and facet CSIs, corticosteroid composition, route of administration, surgical approach, surgery type, and the presence or absence of instrumentation would be valuable for risk stratification. Additionally, while data from Farshad et al 51 was included in the systematic review, there was insufficient data to be included in the meta-analysis. Furthermore, by excluding certain studies from our assessment in the “leave-out” meta-analysis, this secondary assessment may bias the results and bias the findings of this study. Further studies are required in order to determine if preoperative CSIs <1 month prior to spine surgery are a true risk factor for infection, or the result of unintentional biases within the databases from which these findings are derived.
Conclusions
Based on the current available data, CSIs <1 month prior to spine surgery appeared to be a significant risk factor for infection, and for this reason, we recommend significant precautions and considerations prior to the routine use of CSIs during this preoperative period. However, the use of CSIs >1 month prior to spine surgery was not associated with an increased risk of infection.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.