
Abstract
Study Design:
Retrospective, monocentric, observational study in a tertiary health care center.
Objectives:
To analyze prehospital and clinical findings, complications, neurological improvement and follow-up in a young person cohort with spinal cord injury (SCI) and tetraplegia according to the American Spinal Injury Association (ASIA) Impairment Scale (AIS) A to D after diving into shallow water.
Methods:
Included were all persons younger than 50 years with SCI after head-first diving into shallow water between June 2001 and June 2019. All persons with SCI were divided into complete tetraplegia (AIS A) and incomplete tetraplegia (AIS B, C, and D) to test differences.
Results:
A total of 59 males (98.7%) and 1 female with a mean age of 27.7 years suffered an SCI. Alcohol use was documented in 25 cases (41.7%). At the time of admission, 33 people (55%) showed a complete tetraplegia (AIS A) and 27 showed an incomplete tetraplegia with 8 AIS B (13.3%), 15 AIS C (25%), and 4 AIS D (6.7%). At the time of discharge, people with initially complete tetraplegia showed a significant improvement from admission to discharge (P ≤ .004). Persons with incomplete tetraplegia were more likely to improve their neurological status compared with complete tetraplegia patients (P ≤ .001). Especially persons with complete tetraplegia suffered from typical SCI-related problems and complications.
Conclusions:
People with SCI and tetraplegia at the time admission show neurological improvement in 50% of the cases with an overall better outcome in persons with incomplete tetraplegia. The surgical treatment of SCI within 24 hours seems to be associated with a better neurological outcome and a lower level of tetraplegia. The incidence of SCI caused by diving into shallow water remains stable without a significant change, especially in high-risk groups. More education and prevention programs are necessary to avoid these injuries.
Introduction
Spinal cord injuries (SCI) due to diving accidents into shallow water with subsequent tetraplegia especially affects young male people in about 90% of all cases with a mean age between 22 to 28.6 years.1-7 Blanksby et al 8 and DeVivo and Sekar 5 defined shallow water less than 1.5 m depth, with findings of SCI in over 80% of all cases caused by diving into such a shallow water.5,8
The current literature reports 0.6 to 6.3 cases per year per country of American Spinal Injury Association (ASIA) Impairment Scale (AIS) A to D tetraplegia associated with diving accidents.1-4,7,9 Alcohol use at the time of SCI is a risk factor and leads to an extended length of stay (LOS) in the hospital and intensive care unit (ICU), including an increased risk of all types of complications.10,11
Controversy exists in the surgical timing of decompression in persons with SCI. Reviews and a meta-analysis showed that persons undergoing surgery after SCI within 24 hours showed better neurological outcome, especially in persons with incomplete tetraplegia.12-14 The Arbeitsgemeinschaft Osteosynthese Spine (AOSpine) group published in 2017 a clinical practice guideline for the management of patients with acute SCI with the recommendation of decompressive surgery within 24 hours after SCI to improve in clinical outcome. 15 However, a study by Aarabi et al 16 found that the intramedullary lesion length and not the specific timing of surgery best predicts neurological recovery.
Prevention programs (PP) of SCI started in the past 30 years to avoid SCI caused by diving into shallow water or swimming pools.5,17-20 The “ThinkFirst” PP was initiated in the 1980s in the United States and was presented in a study by Kluger et al. 17 This nationwide PP led to the founding of the ThinkFirst National Injury Prevention Foundation with the mission to prevent SCI (and other injuries) through education and research. 21 Damjan et al 20 started in Slovenia in 1992 a national PP under the slogan “Do Not Jump into the Unknown.” Within 3 years the numbers of SCI decreased from 7 to 2 persons per year. What happened after their publication in 1995 is unclear, since no further results were published. Feasible approaches for prevention were also published by DeVivo and Sekar 5 in 1997. They defined high-risk persons as young males, under the influence of alcohol at the time of SCI, who were diving into less than 1.2 m deep water at summer parties.
Education videos at high school or television advertisement were other possibilities for PP described by Bhide et al 19 and Vlok et al 7 in Canada and South Africa in 2000 and 2010, respectively. A possible decline of SCI in these regions after watching the videos or television advertisement was not reported.
However, all the aforementioned studies only published results up to a maximum of 2010.
What has changed in the past 10 to 15 years? Does diving into shallow water with SCI and tetraplegia still affect young males using alcohol at time of SCI, despite PP? How many cases with tetraplegia are still present each year in hospitals? What are the prehospital as well as clinical findings and problems at follow-up (FU) for persons with tetraplegia?
The aim of this study was to determine these questions with special emphasis on differences between people with complete tetraplegia (AIS A) and incomplete tetraplegia (AIS B, C, and D) before, during, and after hospitalization. The authors hypothesized that persons with incomplete tetraplegia benefit more from the multidisciplinary treatment after injury compared to persons with complete tetraplegia with higher rates of prehospital and clinical complications of persons with complete tetraplegia.
Methods
This retrospective, monocentric, observational study was performed at the Department of General and Trauma Surgery and the Department of Spinal Cord Injuries, BG University Hospital Bergmannsheil Bochum, Germany. It has been approved by the local ethics committee (grant number 19-6764-BR).
The SCI department in our hospital was founded in 1952 and was the first in Germany. It is one out of 26 SCI departments in Germany and with its capacity of 78 patient beds (peripheral) and 10 ICU or intermediate care (IMC) patient beds, one of the largest. Per year a total number of 400 to 500 SCI-persons were treated due to acute spinal cord injuries or its complications.
This includes about 80 acute injured tetraplegic persons per year. All medical and therapeutic staff has many years of experience in the treatment of persons with SCI. Numerous studies have already been supervised, and all operative and therapeutic measures are carried out according to existing guidelines. The department is traditional and has a lot of experience in creating and establishing guidelines and treatment standards.
Demographic data, prehospital and clinical findings, level, and type of SCI, AIS at the time of admission and discharge, level of tetraplegia, treatment, LOS in hospital and ICU, complications, and FU, were retrospectively evaluated from our database.
Included were all persons younger than 50 years with SCI and tetraplegia classified as AIS A to D after head-first diving into shallow water between June 2001 and June 2019. Shallow water was defined according to the studies of Blanksby et al 8 and DeVivo and Sekar 5 with a maximum water depth of 1.5 m. Any forms of recreational accidents during water sports that did not meet the aforementioned inclusive criteria, age older than 50 years, and an AIS E were excluded.
Therefore, of 309 persons with an age <50 years and diagnoses of acute tetraplegia or with fractures of the cervical vertebrae (n = 7; C1 n = 1, C2 n = 2, C4 n = 1, C5 n = 1, and C7 n = 2) and AIS E after diving into shallow water, 249 were excluded, resulting in a total of 60 persons who met the criteria and were included in the analysis. All 60 persons with SCI were classified into AIS A to D and were subsequently divided into complete tetraplegia (AIS A) and incomplete tetraplegia (AIS B, C, and D) to test differences.
The type of SCI was characterized as fracture without luxation, fracture with luxation (Figures 1-3) and luxation without fracture (Figure 4) of the cervical vertebrae. The highest level of SCI was always the most proximal injury of the cervical vertebrae in people with multiple SCI. Conservative treatment of SCI was defined as any nonoperative management of SCI like traction, halo, and cervical orthosis. Surgical treatment of SCI was defined as any operative procedure by anterior and/or dorsal approach, for example, decompression and screw or plate fixation with or without graft implantation from the iliac crest or cage implantation. Early surgical treatment was defined as surgical treatment of SCI within 24 hours and late surgical treatment as surgical treatment of more than 24 hours after SCI.
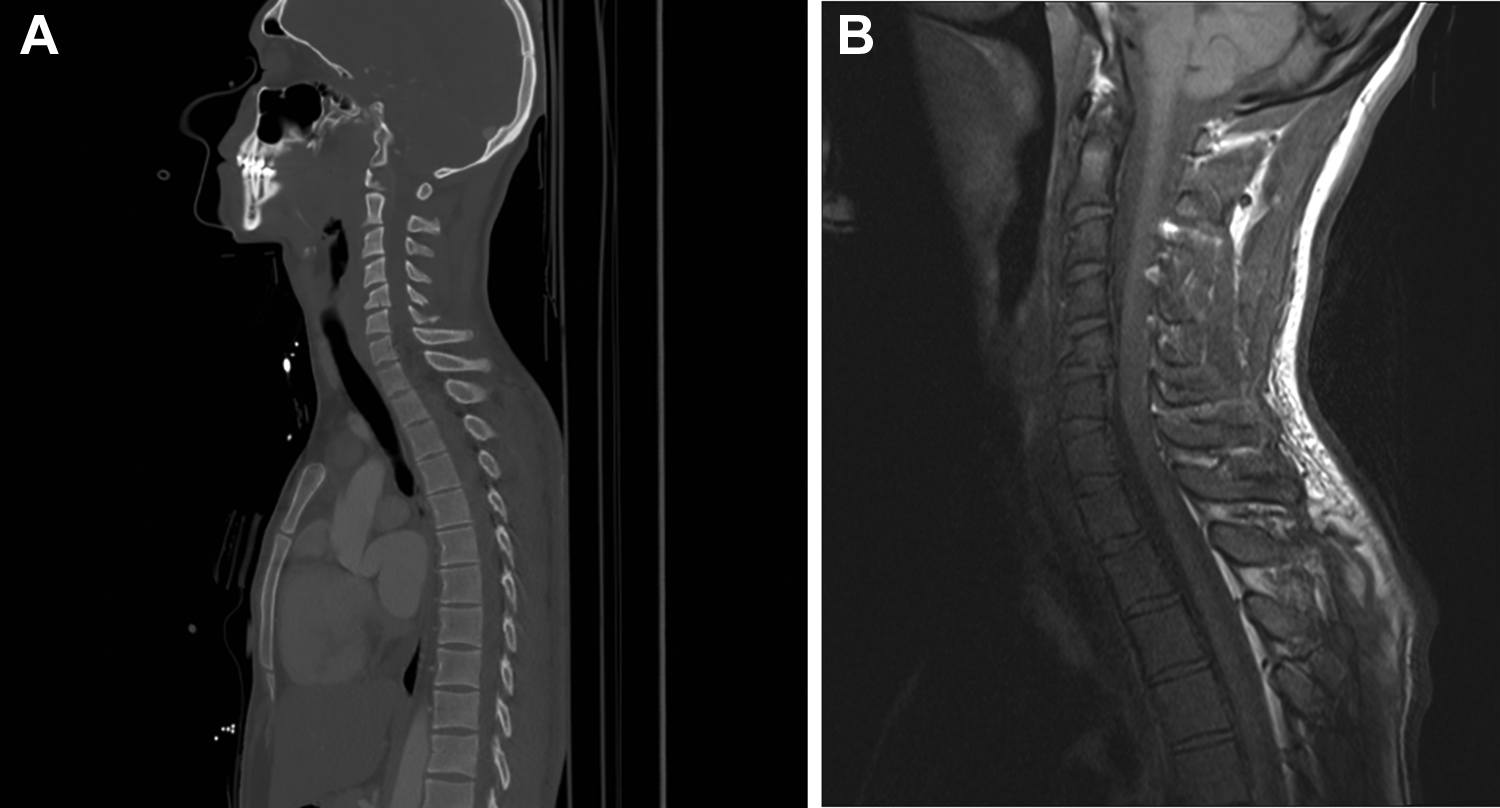
Preoperative computed tomography (A) and magnetic resonance tomography (B) in a person with a luxation fracture of C5/C6.
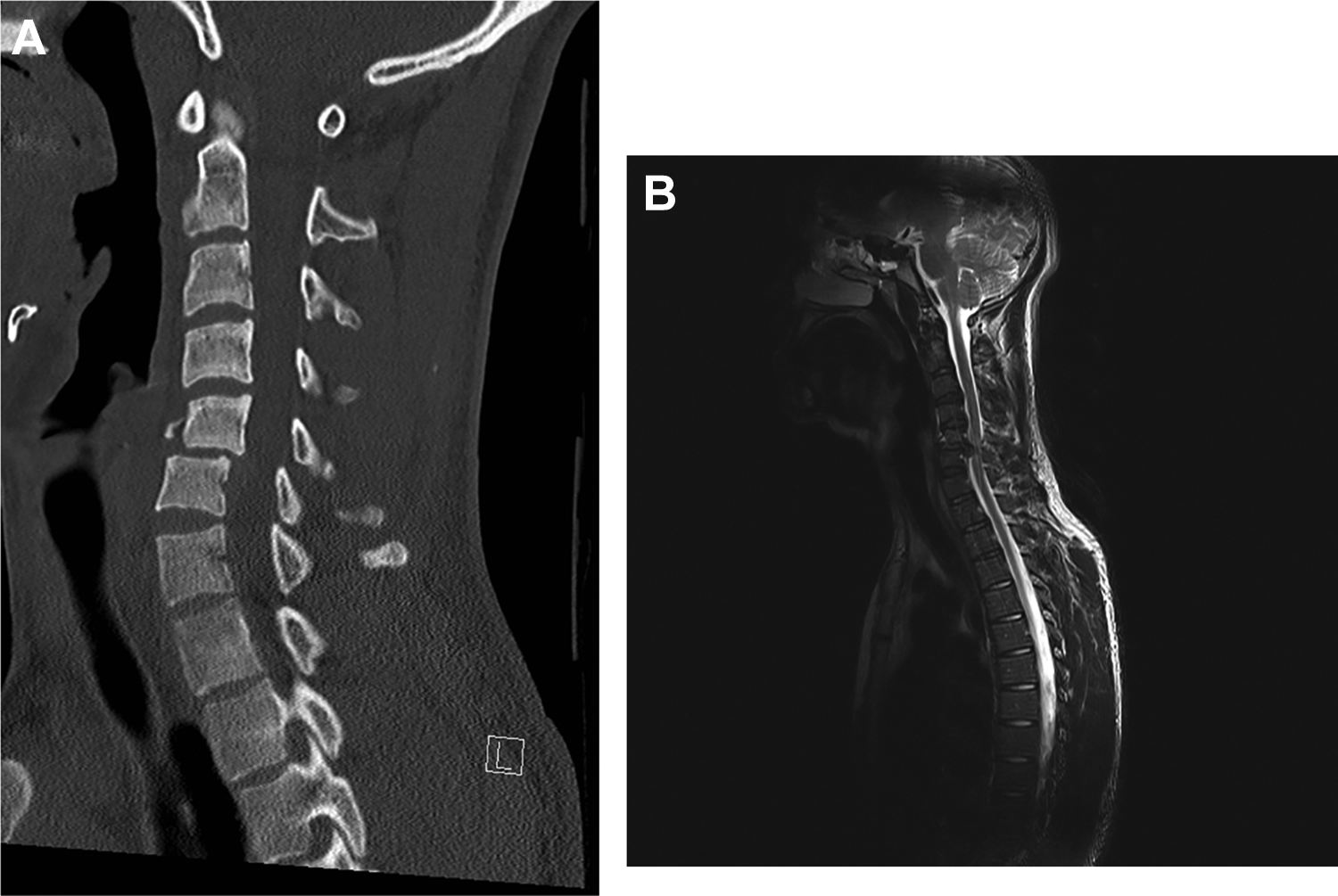
Preoperative computed tomography (A) and magnetic resonance tomography (B) in a person with a teardrop fracture and traumatic disc herniation of C5.
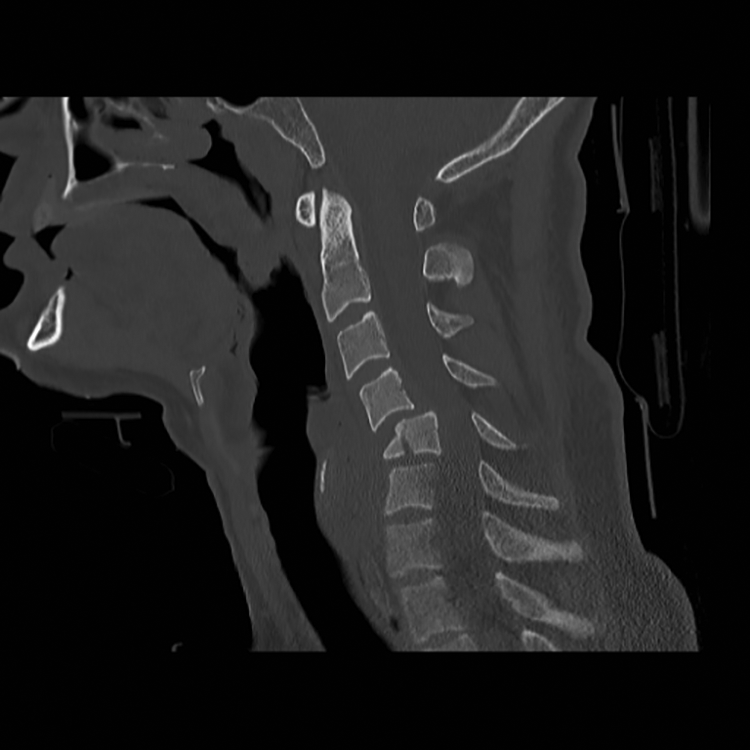
Preoperative computed tomography in a person with fractures of C4/C5/C6.

Preoperative computed tomography in a person with a luxation of C4/C5.
Possible complications were divided into urinary tract infection (UTI), pneumonia, atelectasis, surgical revision, decubitus ulcer, deep vein thrombosis (DVT), acute respiratory distress syndrome (ARDS), cardiopulmonary resuscitation (CPR), ileus, re-intubation, and death. An UTI was defined as positive bacteriuria, leukocyturia, and positive urine culture, including symptoms like fever, increased incontinence, spasticity or increased autonomic dysreflexia.22-24 The management of neurogenic lower urinary tract dysfunction (NLUTD) over the observation period was performed according to national and international guidelines.22-25
Pneumonia was classified as new or progressive and persistent infiltrate on chest radiograph plus 2 of the following symptoms: abnormal white blood cell count (<4000 or >12 000), presence of fever or hypothermia (<36 °C or >38 °C), purulent sputum, and deterioration in gas exchange. 26 Atelectasis was considered as partial collapse or incomplete inflation of the lung, detected on computed tomography or chest radiograph.
Persistent unstable fractures after surgical treatment, failed osteosynthesis, or hematoma led to surgical revision. Decubitus ulcer was divided into stage 1 to 4 according to the National Pressure Ulcer Advisory Panel, 27 a DVT of the leg and pelvic veins was diagnosed by compression ultrasound. ARDS was classified according to the Berlin definition, 28 CPR became necessary, if cardiac arrest, hypoxia, or hemodynamic deterioration because of hypotension below 30 mm Hg systolic blood pressure were present. An ileus was distinguished in paralytic or mechanical ileus, re-intubation was performed because of respiratory deterioration with desaturation and hypoxia or airway obstruction. Death as complication was defined as death of treated persons with tetraplegia during hospitalization.
Common SCI-related problems in the course of treatment of tetraplegia like spasticity, heterotopic ossification (HO), 29 and chronic neuropathic pain or deafferentation pain were detected. Neurological improvement of SCI with tetraplegia on discharge was defined as improvement of one grade or more on the AIS. Outpatient or inpatient further treatment at FU were divided into development or potentiation of spasticity and deafferentation pain, development of decubitus ulcers, or other medical conditions.
Statistical Analysis
Statistical analysis was performed using Microsoft Office Excel for Mac 2019 (Microsoft Corporation) and IBM SPSS Statistics Version 26 2019 (IBM Corporation). The data is presented as mean and standard deviation or as absolute numbers and percentage. Categorial data was tested using the chi-square test or Fisher’s exact test. Continuous data was compared using Student’s t test or Mann-Whitney U test. Significance was set at P ≤ .05.
Results
During an 18-year period (2001-2019), 59 males (98.3%) and 1 female with a mean age of 27.7 ± 9.4 years (range: 18.3-48.7 years) were admitted to our institute with SCI and tetraplegia. A total of 24 persons (40%) were admitted to our department within 24 hours after SCI, while 36 persons (60%) were referred after external surgical treatment. Fifteen participants were injured by diving in the sea (25%), 18 in lakes (30%), 23 in swimming pools (38.3%), and 4 in paddling pools (6.7%).
The general demographic data is listed in Table 1. Participants with complete tetraplegia had significantly more aspirations (n = 29 [87.9%] vs n = 13 [48.1%]; P ≤ .003], prehospital intubations (n = 17 [51.5%] vs n = 7 [25.9%]; P ≤ .004) as well as significantly longer ICU stay (29.6 ± 24.5 vs 10.1 ± 11.7 days; P > .001) and LOS overall (138.8 ± 57.4 vs 85.1 ± 57.1 days; P ≤ .001] compared with those with incomplete tetraplegia.
Demographic Data of Persons With Tetraplegia.a
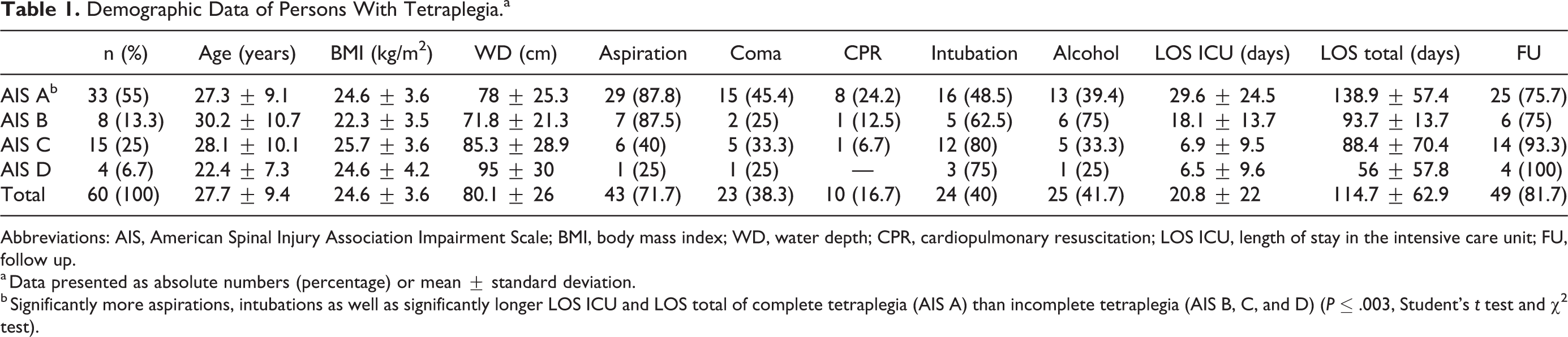
Abbreviations: AIS, American Spinal Injury Association Impairment Scale; BMI, body mass index; WD, water depth; CPR, cardiopulmonary resuscitation; LOS ICU, length of stay in the intensive care unit; FU, follow up.
a Data presented as absolute numbers (percentage) or mean ± standard deviation.
b Significantly more aspirations, intubations as well as significantly longer LOS ICU and LOS total of complete tetraplegia (AIS A) than incomplete tetraplegia (AIS B, C, and D) (P ≤ .003, Student’s t test and χ2 test).
The causes of SCI were fractures in 30 cases (50%), fractures with luxation in 25 (41.6%) and luxation without fractures in 5 cases (8.3%). A total of 51 persons (85%) had a SCI at the level of C4-C6. The main level of tetraplegia was at C5 in 26 cases (44.3%). This data is summarized in Table 2.
AIS on Admission With Levels of SCI and Tetraplegia.a
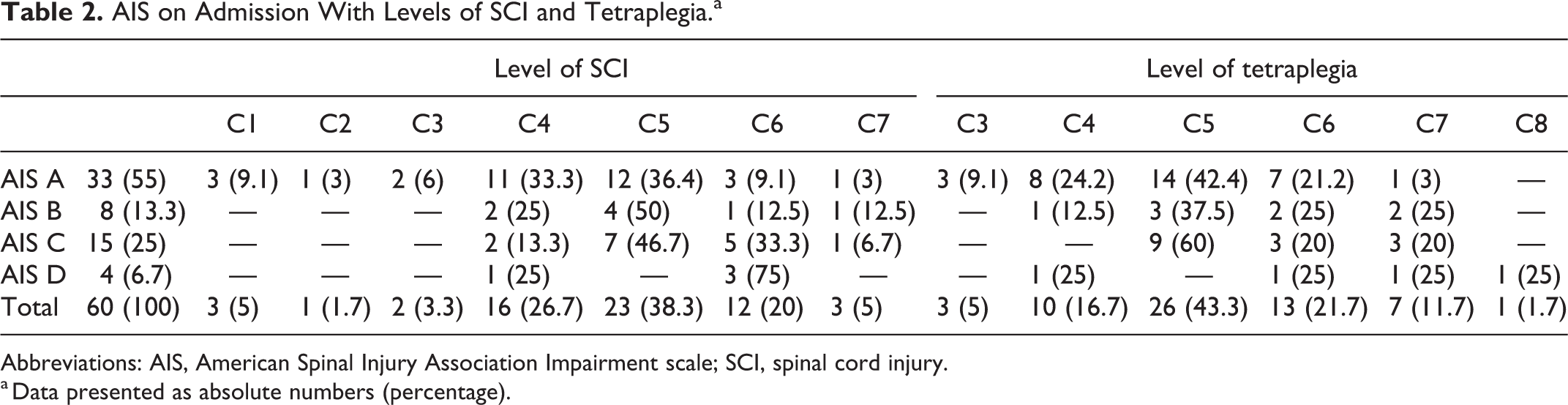
Abbreviations: AIS, American Spinal Injury Association Impairment scale; SCI, spinal cord injury.
a Data presented as absolute numbers (percentage).
Surgical treatment of SCI within 24 hours was performed in 46 persons (76.6%), late surgical treatment in 13 persons (21.7%) and conservative treatment in one person (1.7%). All persons with late surgical treatment were referred to our hospital after diagnosis and/or external surgical stabilization. Twenty-five out of 46 persons (54.3%) with early surgical treatment and 5 out of 14 persons (35.7%) with late surgical treatment or conservative treatment showed neurological improvement during hospitalization. However, there were no significant differences between early or late surgical treatment.
Main strategy for osteosynthesis was a single-stage surgical treatment (n = 48 [80%]) by combination of decompression (n = 56 [93.3%]) and ventral spondylodesis using plate fixation (n = 42 [70%]) including graft implantation from the iliac crest (n = 37 [61.7%]) or implantation of cage (n = 19 [31.7%]). Thirteen patients (21.7%) were treated by ventral and dorsal spondylodesis and 3 persons (5%) by ventral screw fixation without decompression. A dorsal spondylodesis was performed only in 1 case (1.7%). Two-stage surgery became necessary in 6 persons with ventral and dorsal spondylodesis (10%) and in 5 persons because of failed osteosynthesis or hematoma (8.3%).
The level of tetraplegia changed in 5 persons (8.3%) during hospitalization (Table 3). Two persons were neurologically intact after SCI of C7, respectively C8, 2 persons had a lower level of tetraplegia from C5 to C6 and one person from C5 to C7 after surgical treatment. All participants showed an incomplete tetraplegia on admission and neurological improvement on discharge; 4 of them were surgical treated within 24 hours.
Level of Tetraplegia on Admission and on Discharge.a
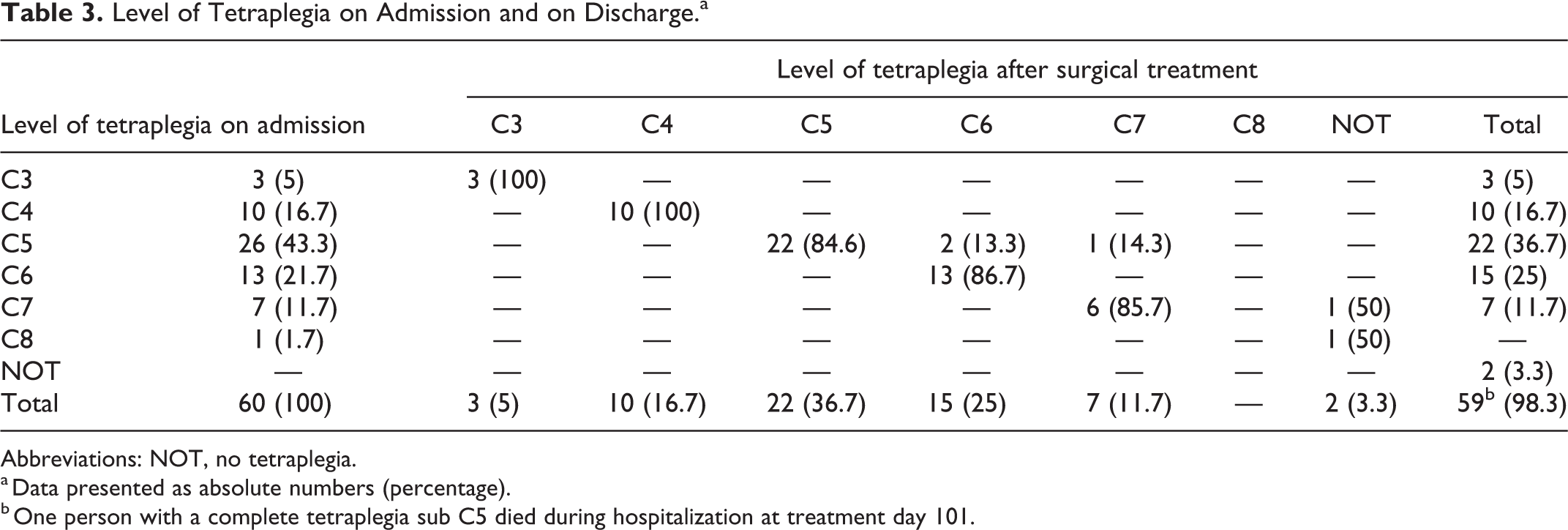
Abbreviations: NOT, no tetraplegia.
a Data presented as absolute numbers (percentage).
b One person with a complete tetraplegia sub C5 died during hospitalization at treatment day 101.
Complications were common during hospitalization and are listed in Table 4. A total of 52 persons (86.7%) suffered 2.5 ± 1.9 complications. Persons with complete tetraplegia had significantly more complications (n = 33 [100%] vs n = 19 [70.4%]; P ≤ .001) and significantly more complications per person (3.6 ± 1.8 vs 1.2 ± 1.2, P ≤ .001) compared to persons with incomplete tetraplegia.
Review of Complications.a
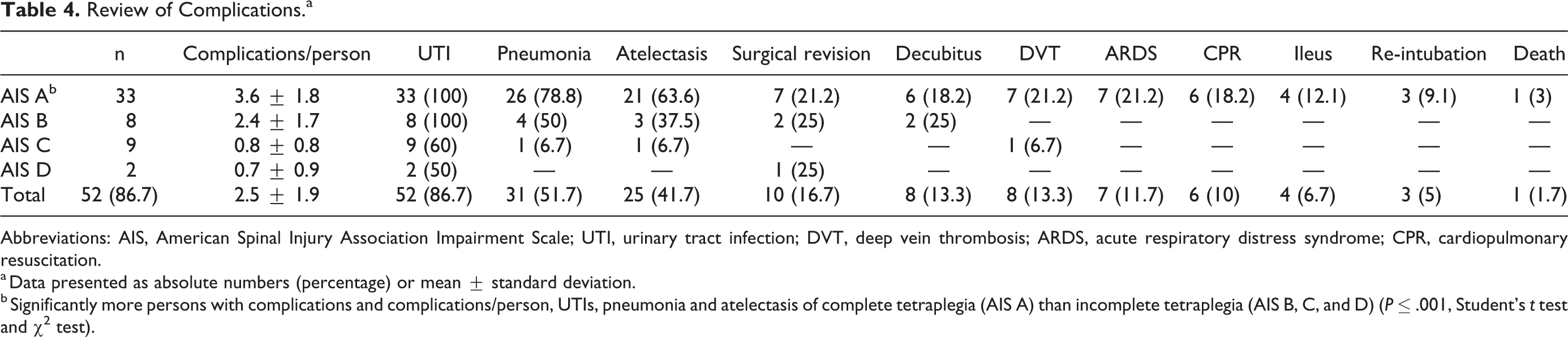
Abbreviations: AIS, American Spinal Injury Association Impairment Scale; UTI, urinary tract infection; DVT, deep vein thrombosis; ARDS, acute respiratory distress syndrome; CPR, cardiopulmonary resuscitation.
a Data presented as absolute numbers (percentage) or mean ± standard deviation.
b Significantly more persons with complications and complications/person, UTIs, pneumonia and atelectasis of complete tetraplegia (AIS A) than incomplete tetraplegia (AIS B, C, and D) (P ≤ .001, Student’s t test and χ2 test).
Persons with complete tetraplegia also suffered significantly more UTI (n = 33 [100%] vs n = 19 [70.4%]; P ≤ .001), pneumonia (n = 26 [78.8%] vs n = 5 [18.5%]; P ≤ .001), and atelectasis (n = 21 [63.3%] vs n = 4 [14.8%]; P ≤ .001) than people with incomplete tetraplegia.
SCI-related problems during hospitalization like spasticity (n = 35 [58.8%]) or deafferentation pain (n = 34 [56.7%]) were also common in persons with tetraplegia without any differences. However, participants with complete tetraplegia showed significantly more HO of the hips in relation to persons with incomplete tetraplegia (n = 12 [36.4%] vs n = 2 [7.4%]; P ≤ .01).
No neurological deterioration was recorded for all persons who survived hospitalization (n = 59). Neurological improvement was seen in 30 participants (50%). At the time of discharge from hospital, 24 persons (40%) with SCI had complete tetraplegia, 33 (55%) were classified as incomplete (4 times AIS B, 10 times AIS C, and 19 times AIS D) and 2 persons (3.3%) were neurologically intact. Detailed information about AIS A to E on admission and on discharge are summarized in Table 5.
AIS on Admission and on Discharge.a
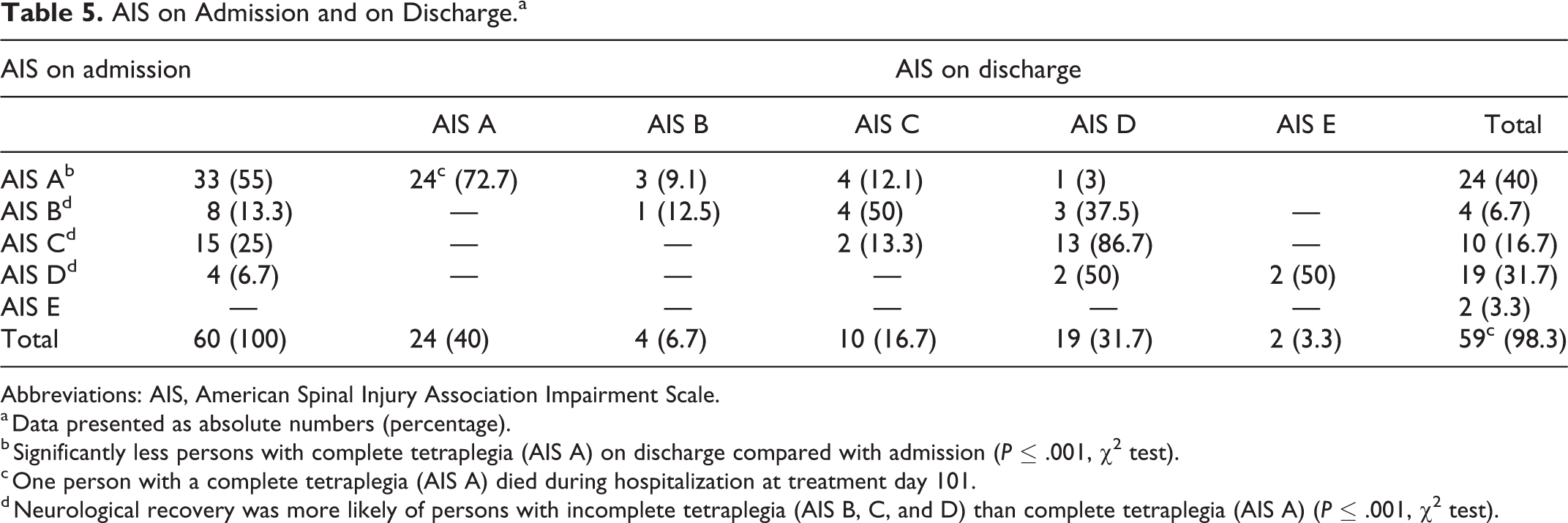
Abbreviations: AIS, American Spinal Injury Association Impairment Scale.
a Data presented as absolute numbers (percentage).
b Significantly less persons with complete tetraplegia (AIS A) on discharge compared with admission (P ≤ .001, χ2 test).
c One person with a complete tetraplegia (AIS A) died during hospitalization at treatment day 101.
d Neurological recovery was more likely of persons with incomplete tetraplegia (AIS B, C, and D) than complete tetraplegia (AIS A) (P ≤ .001, χ2 test).
On discharge, 16 persons (26.7%) with neurological improvement were able to self-care and 22 persons (36.7%) were able to walk alone without assistance. A spontaneous micturition was possible for 17 participants (28.3%) and a clean intermittent self-catherization (CISC) was performed by 9 participants (15%). Fecal continence was seen in 21 people (35%). All these persons had an incomplete tetraplegia or were neurologically intact on discharge.
Neurological recovery was more likely for persons with incomplete tetraplegia than complete tetraplegia on admission (n = 22 [81.5%] vs n = 8 [24.2%]; P ≤ .001). However, significant improvement was also seen in persons with initial complete tetraplegia from admission to discharge (n = 33 [100%] vs n = 24 [72.7%]; P ≤ .004), despite the death of one person with complete tetraplegia during hospitalization at treatment day 101.
A total of 49 persons (81.9%) had a FU with a mean of 4.1 ± 4.1 years. Twenty of these persons (33.3%) did not report any new complaints during FU examination. Problems at FU were persistent or new spasticity (n = 10 [16.7%]) and deafferentation pain (n = 6 [10%]), decubitus ulcer requiring surgery (n = 8 [13.3%]), and 5 other medical conditions (8.3%; coprostasis, cholecystolithiasis, hypertension, nephrolithiasis, and ulceration of the foot). Seven cases of decubitus ulcer requiring surgery and 3 cases of deafferentation pain and spasticity as well as 2 other medical conditions were in persons with complete tetraplegia.
Discussion
SCI with tetraplegia after head-first diving into shallow water typically occurs every year between May and September. Currently, there are data published from 232 participants with SCI and tetraplegia AIS A to D over a period from 1970 to 2010 with a range of 0.6 up to 6.3 cases per year per country.1-5,7
Between 2001 to 2019 a total of 60 persons with SCI and tetraplegia were admitted to our institution for initial treatment and / or for rehabilitation with a mean of 3.3 cases each year. Our data shows that the mean incidence of SCIs with tetraplegia per year is identical over the past 50 years. 18 The population of our study consists of 59 males (98.3%) and 1 female with a mean age of 28 years. These results are in line with other studies.1-7,17,18,20,30 Young males with a mean age between 22 and 28.6 years suffered in 79% to 97% of all cases SCIs with tetraplegia. There is no change of these data since 1961. 18
Alcohol use at time of SCI is an important risk factor for cervical injury. 11 The use of alcohol at time of SCI is described in 37% to 49% of all cases in the literature.5,7,17,18 41.7% of all persons with SCI and tetraplegia had drunk alcohol in our study. Again, there is no change of this data since 1961. 18
A study by Crutcher et al 10 found an association between alcohol use at time of SCI and extended LOS as well as an increased risk of all types of complications after analysis of a national database in the United States with 10.611 persons. 10 These effects were not found in our study or in any other study with the use of alcohol at time of SCI.5,7,17,18 This fact is probably due to the small number of cases in these studies.
Several studies released data with SCI and AIS A to E after diving into shallow water.2-5,7 The retrospective study by Aito et al 1 published results only from SCI with tetraplegia. 1 An analysis of all cases between 1978 and 2002 in Italy was performed. Thirty-five persons with complete tetraplegia and 30 persons with incomplete tetraplegia were included. Neurological improvement (31%) was only seen in 3 persons with complete tetraplegia and in 17 persons with incomplete tetraplegia on discharge. Persons with AIS B to D showed better results than persons with AIS A without any significance. This impression was confirmed by Borius et al 3 based on the results of 17 people with tetraplegia after diving in swimming pools. Similar results were also published by Amorim et al 2 in 2011 in 77 persons with tetraplegia on admission.
Neurological improvement on discharge was only seen in 21 persons (15%) in their study. However, significant improvement was shown for persons with incomplete tetraplegia on discharge compared to complete tetraplegia. All these findings are relatively consistent with those of our study.
Neurological improvement in our study was higher (50%) than previously described. Persons with incomplete tetraplegia showed significantly better results than persons with complete tetraplegia. Again, there is no change since 1978. 1 However, on discharge were significantly less participants with a complete tetraplegia than on admission. This fact is new and shows that people with SCI and initial complete tetraplegia after diving into shallow water also have the potential of neurological improvement.
Persons with early surgical treatment (54.3%) of SCI showed more neurological improvement than persons with late surgical treatment (35.7%) without any significance in our study. This fact is probably due to the small number of cases during our observation period. The literature also seems to support that surgery within 24 hours results in improved clinical outcomes for acute SCI patients.12-14
However, we have to address that the AOSpine guideline paper with the recommendation of surgical timing in SCI within 24 hours is based on the findings of the surgical timing in acute spinal cord injury study (STASCIS) by Fehlings et al.15,31 A total of 222 persons with acute cervical SCI were enrolled in a multicenter, prospective cohort study between 2002 and 2009. 31 Early surgery (19.8%) resulted in superior neurological recovery compared to late surgery (8.8%), defined as at least a 2 grade AIS improvement at 6 months’ FU. In addition, the positive effects of early surgical decompression in traumatic SCI were confirmed in other recently published studies.32,33
Other results were published by Aarabi et al 16 in a retrospective analysis of prospectively collected data of 72 persons with cervical traumatic SCI. They investigated the effect of timing of decompression on long-term neurological outcome in persons with complete spinal cord decompression confirmed on magnetic resonance imaging. Only intramedullary lesion length was a predictor of AIS grade conversion to a better grade and not the timing of surgery. Based on our and the available data, we believe that early surgery be offered as a treatment option for persons with acute traumatic cervical SCI to improve in neurological outcome.12-15,31-33
Prehospital complications were common in our study. Aspiration was noted in 71.7% and coma in 38.3% of all persons with the need of CPR in 16.7% and/or intubation in 40% of all cases. Especially participants with complete tetraplegia showed significantly more aspirations with the need of intubation. Coma and CPR tended also to be higher in this group without any significance. However, data of prehospital complications was not presented in any study for comparisons.1-7,17,18,20,30
In-hospital complications were also common in our study. A total of 52 persons (86.7%) suffered complications during hospitalization with 2.5 complications per person. Participants with complete tetraplegia had significantly more complications and suffered significantly more UTIs, pneumonia, and atelectasis than people with incomplete tetraplegia. Only persons with complete tetraplegia received ARDS, CPR, ileus, re-intubation as well as death (Table 3).
The high rates of pneumonia, atelectasis and ARDS, especially in persons with complete tetraplegia, could be explained by the high prehospital rates of aspiration and intubation as well as the level of complete tetraplegia.
Complications like CPR, ileus, and re-intubation during hospitalization may have been caused by physiological consequences of SCI, level of complete tetraplegia or complications of cannula changes.34,35
UTI was the most common complication in persons with SCI in our findings without any trends over time. This is in line with recently published literature with a rate of UTI up to 68%.36-39 Profound alterations in urodynamic function and reliance on urinary catherization for bladder management increases the risk of UTI among participants living with SCI and tetraplegia. The clean intermittent catherization (CIC) is considered to be the gold standard in the management of NLUTD in persons with SCI.24,40,41 The management of NLUTD over the observation period was performed according to national and international guidelines with CIC in persons with SCI.22-25 The reason for our high rate of UTI may have been the long LOS in the ICU with a mean of almost 21 days. CIC was not performed during the ICU stay.
The study by Borius et al 3 showed that all persons with complete tetraplegia received complications. This finding is equal to our data. The distribution of complications in participants with incomplete tetraplegia was not accomplished. Aito et al 1 reported of complications in 15 persons (21%) that were more severe in persons with complete tetraplegia. A DVT was the main complication, followed by pneumonia and UTI.
Their results are completely different to our data with a smaller number of all types of complications as well as other distributions of DVT, pneumonia, and UTI.
SCI-related problems during hospitalization in our study group were also common. HOs were present in 23% of all cases with significantly more HOs in persons with complete tetraplegia. Deafferentation pain and spasticity were treated in almost 60%. FU was documented in over 80% with 3 main problems: development or potentiation of spasticity (16.7%) and deafferentation pain (10%) as well as decubitus ulcer requiring surgery (13.3%). SCI-related problems, especially at FU as well as decubitus ulcer are well known problems after initial treatment of SCI.42-44 Unfortunately, no studies described SCI-related problems during hospitalization and at FU so that a comparison of our data could not be performed.1-7,17,18,20,30
Any cited study in this article, which presented risk factors, PP, or results of SCI with tetraplegia made suggestions for PP or started a PP.1-7,11,17-20,30 But what has changed in the past 10 to 15 years? Despite all PP, SCI and tetraplegia after diving into shallow water still affects young males <30 years old with the use of alcohol at time of SCI. The incidence of SCI with tetraplegia per year remains unchanged. Especially in Europe, we urgently need more education and PP to avoid these injuries.
Limitations
The present study has several limitations. First, it is a retrospective study that included a relatively small sample of persons over an 18-year period. Second, it is conducted monocentric at a level 1 trauma center. Third, the significance of the study results and conclusion may clearly be limited by the retrospective design. However, the study is documented on many parameters and the epidemiological findings are carefully described. Moreover, it is the first study that presented results of persons with tetraplegia after diving into shallow water before, during, and after hospitalization.
Conclusion
Persons with SCI and tetraplegia on admission show in 50% of all cases neurological improvement during hospitalization. We confirm that persons with incomplete tetraplegia on admission present better outcomes than persons with complete tetraplegia. However, people with initially complete tetraplegia also have the potential of neurological improvement. The surgical treatment of SCI within 24 hours seems to be associated with better neurological outcome and a lower level of tetraplegia, notably in persons with incomplete tetraplegia. Complications and SCI-related problems in persons with SCI and tetraplegia after diving in shallow water are common, especially in persons with complete tetraplegia. Despite of PP there is no change in high-risk groups of SCI since 1961: Young males <30 years old with the use of alcohol at time of SCI. We need more education and PP to avoid these injuries.
Footnotes
Author Contributions
CU and MK had full access to all data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. CU, EY, and MK are responsible for the study design. CU, EY, OJ, SL, TS, MA, and MK contributed substantially to the study design, data analysis and interpretation and the writing of the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study has been approved by the local ethics committee (Ruhr-University Bochum, Germany, grant number 19-6764-BR). We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research.