
Abstract
Study Design:
Systematic review and meta-analysis.
Objective:
To systematically review the available articles on topical vancomycin powder (TVP) use in pediatric spine surgeries exploring the usefulness and safety of such practice.
Methods:
We conducted an independent and duplicate electronic database search in PubMed, EMBASE, and Cochrane Library till March 2020 to identify all relevant literature on the use of TVP for pediatric spine surgeries. Surgical site infection (SSI) rate, specific reported complications, reoperation rate, microbial flora pattern in reported SSIs, and safety profile were the outcomes analyzed. Analysis was performed with the R platform using OpenMeta[Analyst] software.
Results:
No prospective studies were available to evaluate the use of TVP in pediatric spine surgeries for the prevention of SSIs. Neither standardized protocol, nor drug dosage, nor safety profile was established for pediatric use. Three retrospective cohort studies including 824 patients (TVP/control: 400/424) were included in the meta-analysis. There was low-quality evidence suggesting no significant difference between the 2 groups in SSI rate (RR = 0.474; 95% CI = [0.106,2.112]; P = .327) with significant heterogeneity (I2 = 70.14; P = .035). The TVP group showed a significant benefit on cost analysis in one of the included studies. However, TVP did not prevent gram-negative coinfection on SSI in the TVP group.
Conclusion:
From the literature available at present, TVP does not qualify to be recommended as a safe and useful option to prevent SSI following pediatric spine surgeries. High-quality prospective interventional studies are needed to arrive at a consensus on its use along with appropriate dosage and method of application.
Introduction
Surgical site infection (SSI) remains a major problem in spine surgery despite major advancements in surgical technique and patient care to decrease its incidence. 1 Risk factors for SSI pediatric and adult populations are varied and unique. 1 Some cohorts of the pediatric population are at increased risk of infection. 2 For example, SSI incidence in patients with spinal dysraphism range from 8% to 41.7%, and for those with cerebral palsy, it ranges from 6.1% to 15.2%. 2 Moreover, these candidates with growing spines are required to undergo multiple surgical procedures throughout their treatment and are at a greater risk of infection than the general pediatric orthopedic population, with an increased risk of infection at each subsequent surgery. 2 -5
Various methods have been developed and implemented to prevent SSI in the pediatric population. The practices vary among different groups of surgeons, based on their training and expertise. 2 One such practice is the application of topical vancomycin powder (TVP) in the surgical wound before closure. Vancomycin powder is increasingly used off-label as TVP to prevent infection in spine surgeries. 6 It is, however, unclear whether TVP has an impact on SSIs. Several review articles support the use of TVP in adult spine surgeries. 7 -10 This has encouraged a few surgeons to try TVP in the pediatric population to achieve a similar benefit out of it. In a survey by the Paediatric Orthopaedic Society of North America (POSNA) to generate a consensus statement in combating SSIs in spine surgery, 24% of pediatric spine surgeons were using TVP. 11
Only a few studies were available in the literature on TVP use in the pediatric population, giving conflicting evidence without a consensus on the practice. 12 To date, no systematic reviews or meta-analyses are available to demystify the conflicting literature evidence and arrive at a clear picture of the practice. This was the first study of its kind to review the available articles on TVP use in pediatric spine surgeries and explore the usefulness and safety of such a practice.
Materials and Methods
This meta-analysis was conducted following the guidelines of Back Review Group of Cochrane Collaboration 13 and reported based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 14 We developed a null hypothesis that TVP use in pediatric spine surgeries did not reduce SSIs. We conducted this systematic review and meta-analysis to test the null hypothesis.
Search Strategy
Two reviewers performed an extensive independent search of electronic databases such as PubMed, EMBASE, and the Cochrane Library to identify all the relevant studies using the following keywords: vancomycin, spine, surgery, SSI, and infection, along with the Boolean operators AND, OR, and NOT. The reference list of the selected articles was also searched to identify studies not identified in the primary search. According to the inclusion and exclusion criteria, eligible studies were included in the meta-analysis. The discrepancy between the authors was resolved through discussion until a consensus was obtained. A detailed study selection flow diagram is given in Figure 1.
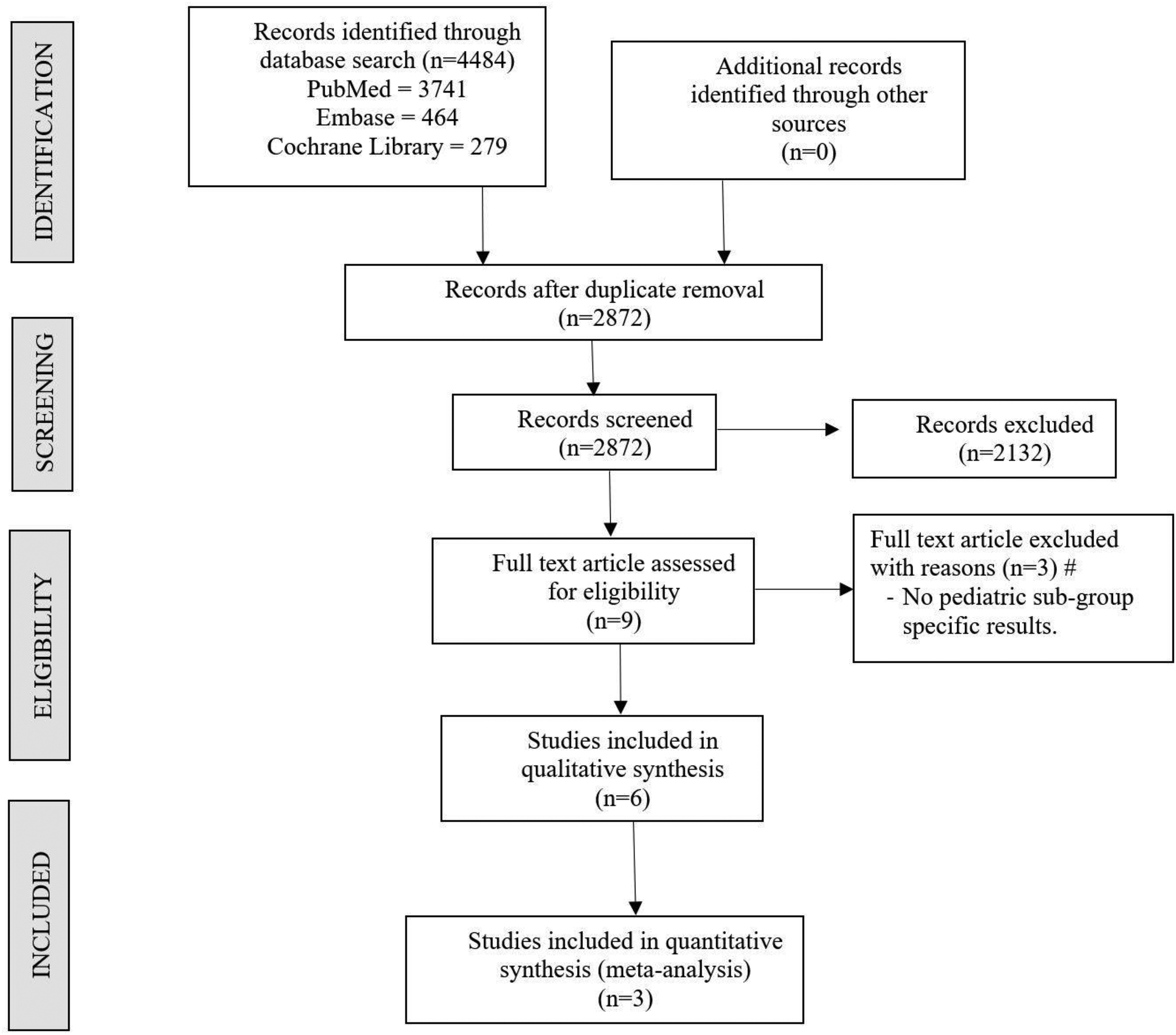
PRISMA flow diagram of the included studies.
Inclusion Criteria
All studies were included if they met the following PICOS criteria: Population: pediatric patients undergoing spine surgery Intervention: use of TVP before wound closure Comparator: use of placebo or nonuse of TVP before wound closure Outcomes: SSI rate, specific reported complications, reoperation rate, microbial flora pattern in reported SSI Study design: any study design satisfying PICO criteria
Exclusion Criteria
Trials were excluded if they had the following characteristics: studies involving TVP in the adult population and studies involving both adult and pediatric populations without specific results for the pediatric subgroup; subjects involving animal models; and studies in which TVP was used in areas other than the spine.
Data Extraction
Two reviewers retrieved independently relevant data from articles included for analysis. The following data was extracted: Study characteristics: year of publication, authors, country, number of patients enrolled Baseline characteristics: mean age, gender proportions, preoperative diagnosis, vancomycin dosage, TVP application protocol Primary outcomes: SSI rate Other outcomes: specific complications, reoperation rate, microbial flora pattern in reported SSI, safety profile
Quality and Risk of Bias Assessment
The quality of the included studies was assessed by the Newcastle-Ottawa Scale. 15 The scale is designed to assess the quality and the risk of bias of nonrandomized studies for inclusion into meta-analyses. The scale has 3 domains of assessment—namely, selection, comparability, and outcome. We also used the GRADE approach to evaluate the quality of evidence available on the subject.
Statistical Analysis
Meta-analysis was conducted using the R platform with OpenMeta[Analyst]. 16 For dichotomous variable outcomes, risk ratios (RRs) with 95% CIs were used, and for continuous variable outcomes, weighted mean differences with 95% CIs were used. Heterogeneity was assessed using the I2 test. If I2 was <50% and P was >.1, we used a fixed effects model to evaluate; otherwise, a random-effects model was used. Sensitivity analyses were performed to explore the source of heterogeneity when it existed.
Results
Search Results
An electronic database search resulted in 4484 articles, which after initial screening for duplicate removal gave a total of 2872 articles. Title and abstract screening were done in those articles, and 2132 of them were excluded; 9 articles qualified for a full-text review of which 3 were excluded, and 6 articles qualified for qualitative review of which only 3 were eligible for meta-analysis. A list of the studies excluded and reasons for their exclusion are given in Annexure 1 (available online). Three studies 17 -19 with 824 patients (TVP group, 400; control group, 424) were included in our meta-analysis. A PRISMA flow diagram of study selection is given in Figure 1.
Quality and Risk of Bias Assessment
The methodological quality of the included studies is given in Table 1. All the included studies were rated using the Newcastle Ottawa Scale and scored ≥5 stars.
Quality of Included Studies Based on the Newcastle-Ottawa Scale. 15

General Characteristics
Three studies that qualified for meta-analysis were of level 3 evidence according to Oxford Center for Evidence-Based Medicine because all of them were retrospective cohort studies. 20 All studies defined SSI according to the US Centers for Disease Control and Prevention guidelines. 21
The general characteristics of the studies included in quantitative (Serial No.: 1-3) and qualitative analyses (Serial No.: 4-6) are given in Table 2. All 3 studies taken for meta-analyses were from the United States. No significant differences between the 2 groups were found in the baseline characteristics. TVP protocols followed in the included studies are given in Table 3.
Characteristics of Included Studies.
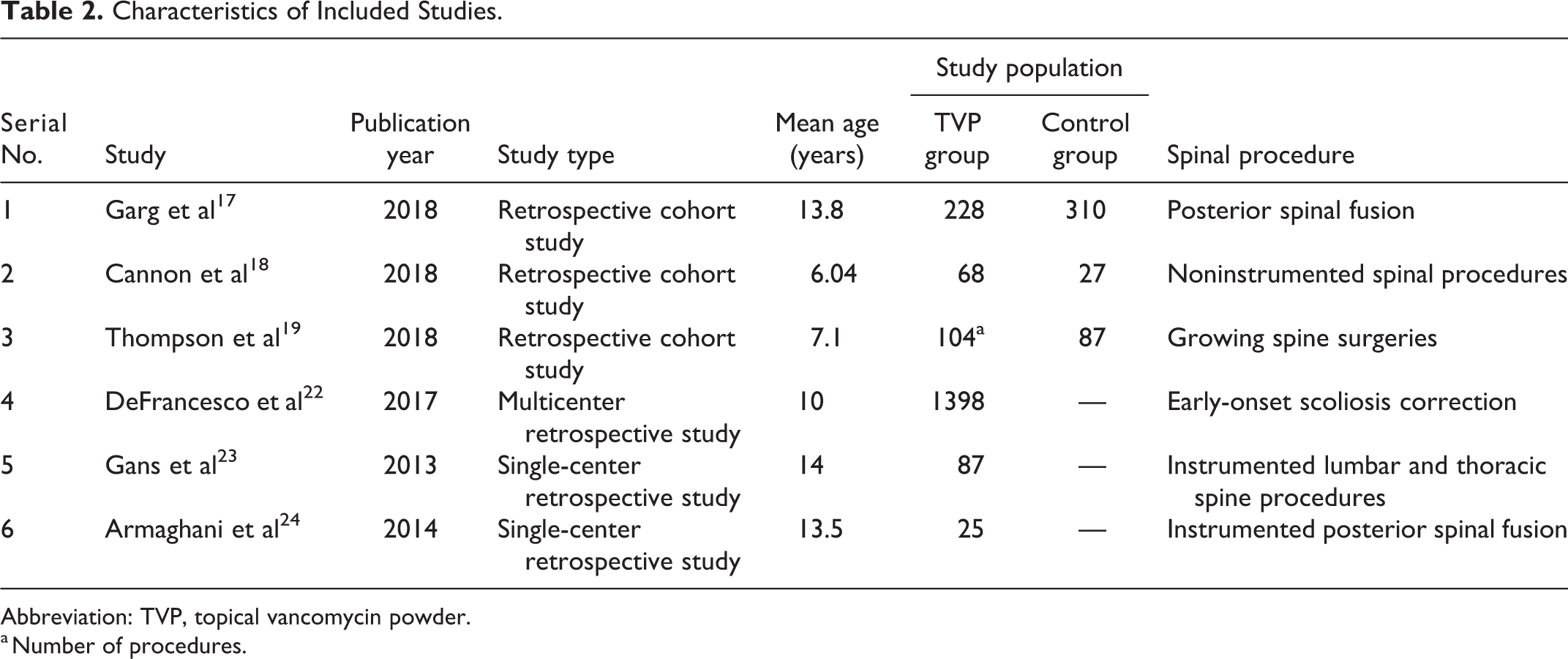
Abbreviation: TVP, topical vancomycin powder.
a Number of procedures.
Vancomycin Protocol of Included Studies.
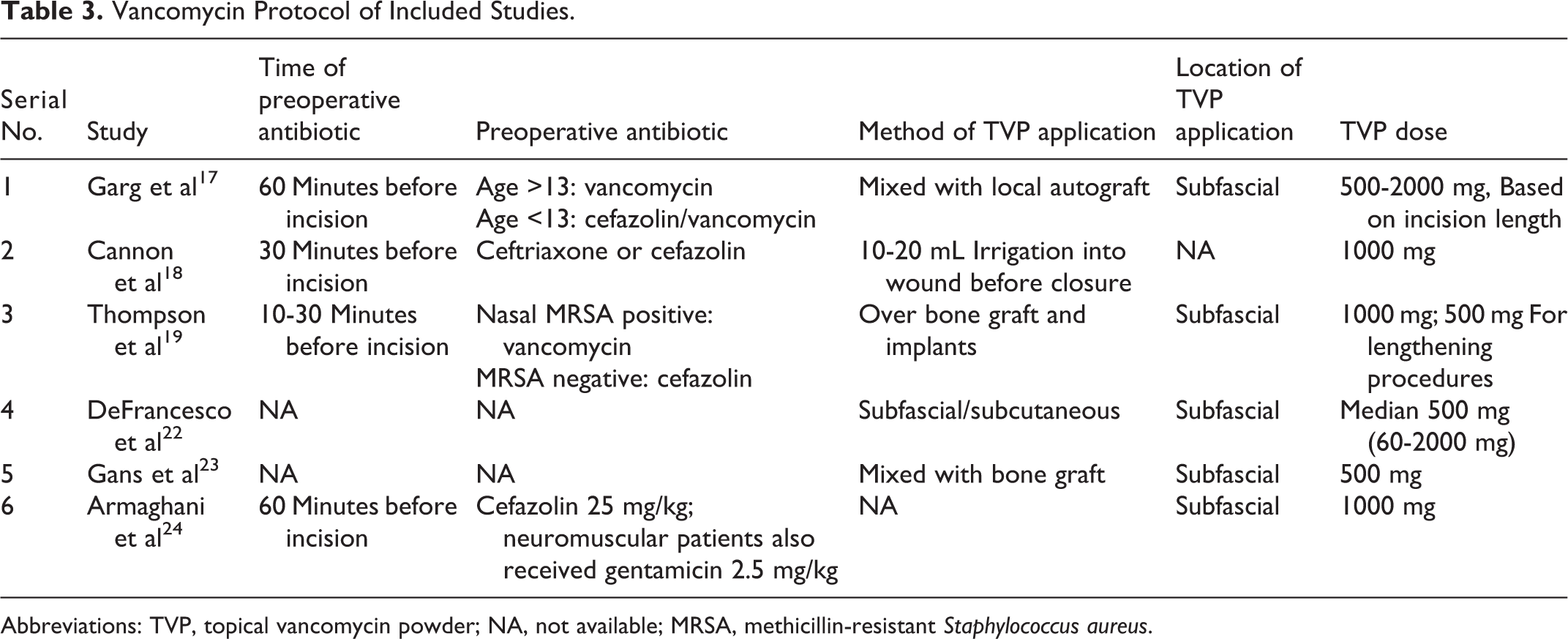
Abbreviations: TVP, topical vancomycin powder; NA, not available; MRSA, methicillin-resistant Staphylococcus aureus.
The predominant primary diagnosis in the studies included for meta-analysis comprised neuromuscular scoliosis, adolescent scoliosis, congenital and syndromic scoliosis, kyphosis, and spondylolisthesis. There was no uniformity among the included studies concerning the preoperative antibiotics, vancomycin application protocol, and dosage, as shown in Table 3.
Primary Outcome
SSI Rate
Incidence of SSI from the meta-analysis between the TVP group and control group among the 3 included studies with 824 patients showed no significant difference between the groups (RR = 0.474; 95% CI = [0.106,2.112]; P = .327), as shown in Figure 2. Significant heterogeneity existed between the studies (I2 = 70.14; P = .035), and hence, a random-effects model was used for analysis. Sensitivity analysis was also performed, and the results were not significantly altered by sequentially omitting each study in the meta-analysis.
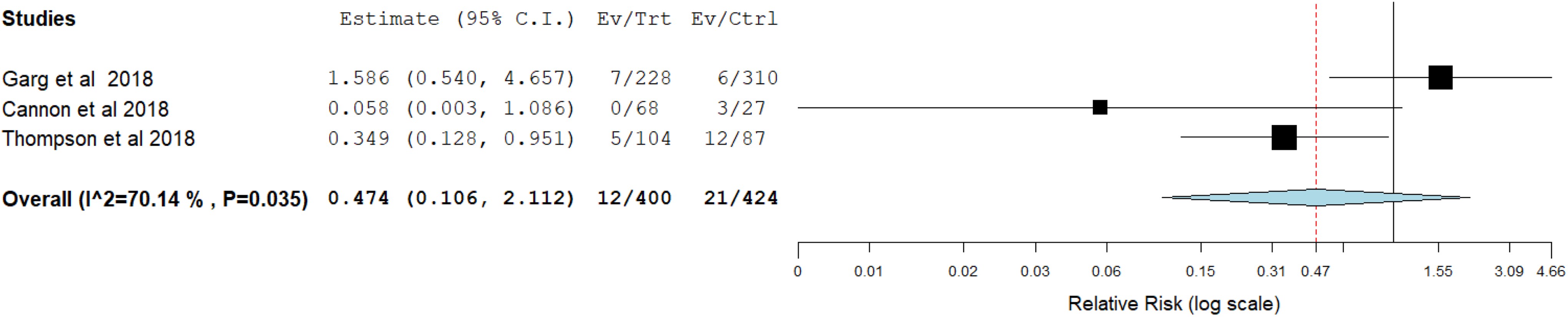
Forest plot of the included studies comparing the primary outcome measure—surgical site infection.
From the above analysis, we accepted the null hypothesis because no significant difference was noted between the groups. Furthermore, we assessed the quality of the evidence for the primary outcome analyzed with the GRADE approach. The quality of evidence to accept the null hypothesis was low, as shown in Table 4.
GRADE Table of Evidence.
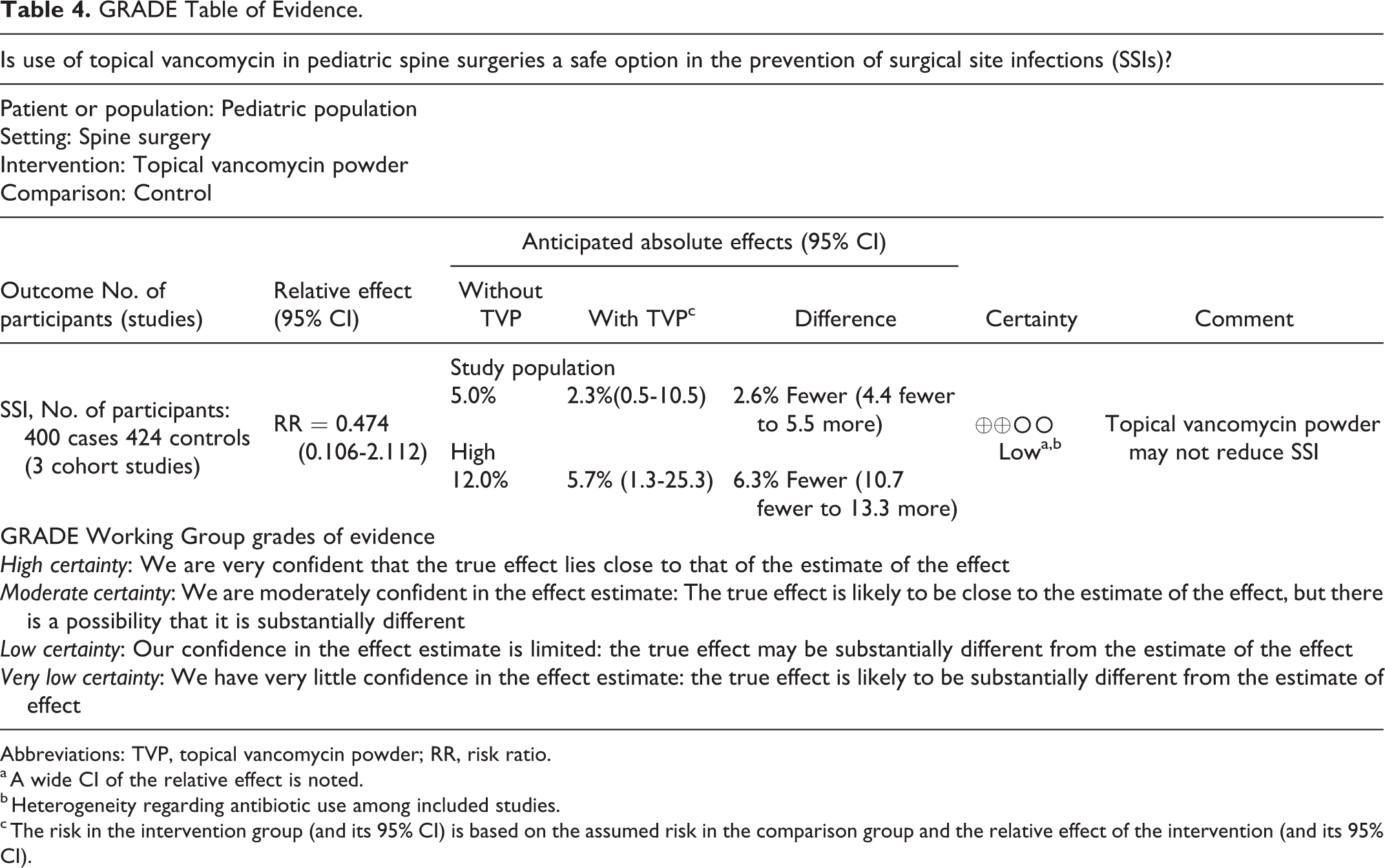
Abbreviations: TVP, topical vancomycin powder; RR, risk ratio.
a A wide CI of the relative effect is noted.
b Heterogeneity regarding antibiotic use among included studies.
c The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
Other Outcomes
Specific Complications
DeFrancesco et al 22 carried out a multicenter retrospective study to analyze the clinically apparent adverse reactions of TVP application in early-onset scoliosis and concluded that adverse reactions are rare following TVP. They had only 1 adverse event in their study in a 10-year-old child with transient rash following 1500 mg TVP. Garg et al 17 noted 1 case of pseudoarthrosis among their TVP group. However, significant association could not be made.
Reoperation Rate
In their study, Garg et al 17 had a 6% reoperation rate among the TVP group involving 228 patients, whereas a 4% reoperation rate was noted in the control group with 310 patients, and no significant difference was noted between them (P = .291). Cannon et al 18 did a cost analysis and found that the use of TVP significantly reduced the cost of overall treatment by preventing SSIs and its further treatment procedures.
Microbial Flora Pattern
In their study, Garg et al 17 noted methicillin-sensitive Staphylococcus aureus, methicillin-resistant S aureus (MRSA), and Staphylococcus epidermidis to be the predominant organisms in the 7 patients with SSIs in the TVP group. It was also noted that in 2 of their patients, there was a coinfection with Pseudomonas and Escherichia coli. Gans et al 23 in their series noted Enterobacter and MRSA to be the predominant organisms in culture profiles in 3 patients with SSIs in the TVP group.
Safety Profile
Gans et al 23 studied the postoperative serum vancomycin and creatinine levels in 87 pediatric cases and concluded that TVP is safe as far as the systemic effects are concerned. In 25 patients, Armaghani et al 24 analyzed the serum and drain levels of vancomycin and concluded that 1 g of TVP produced nontoxic serum vancomycin levels with supratherapeutic drain levels. The average drain vancomycin levels on the day of surgery and postoperative day were 403 (range 25-800) and 251 (34-422) μg/mL, respectively. The average serum vancomycin levels were 2.5 and 1.9 μg/mL, respectively, on postoperative days 0 and 1. None of them had toxic levels in serum, which is more than 25 μg/mL.
Of significant note is that 5 out of 6 studies advocated the subfascial application of TVP, as shown in Table 3.
Discussion
Application of vancomycin powder prophylactically in spine surgery wounds began as early as 2011 when Sweet et al 7 demonstrated reduced deep wound infections in thoracolumbar fusion surgeries after addition of 2 g of intrawound TVP to the traditional intravenous antibiotic prophylaxis. Since then, the use of TVP over the instrumentation and graft has gradually been accepted as a new standard of care in spine surgery. Thompson et al, 19 when they presented their early results of TVP use in growing spine surgeries involving growth rod constructs and vertical expandable prosthetic titanium rib, demonstrated reduced SSI following the addition of TVP into their SSI prevention protocol. However, as with any observational study, it was imprecise to give a causal relationship to the variable under analysis, and conclusions based on them were not acceptable until and unless it could be supported by well-designed randomized controlled trials (RCTs). 25 Hence, it is imperative to have a systematic review and meta-analysis of the available literature before the assimilation of TVP into the SSI prevention protocol for the pediatric spine population.
Main Finding
From the available literature, on systematic review and meta-analysis, we can only conclude that TVP usefulness in pediatric spine surgeries is doubtful, and further RCTs are needed to support their routine use in the SSI prevention protocol for pediatric spine surgeries.
Safety of TVP in Pediatric Spine Surgeries
All the above-mentioned studies have taken into account only the clinically apparent adverse reactions such as red man syndrome, rash, nephrotoxicity, proteinuria, hepatotoxicity, or ototoxicity in their limited subset of patients. However, there are studies indicating rare but clinically significant events following local vancomycin use in adults. Ghobrial et al 26 conducted a systematic review of adverse events recorded following TVP use and identified the rate of adverse events following TVP to be 0.3%. The adverse events included nephropathy, ototoxicity, and seroma formation. Hypersensitivity reactions have been described following TVP. Mariappan et al 27 reported a case of circulatory collapse following TVP, and Nagahama et al 28 described development of the red man syndrome following TVP in cranial surgery. Acute renal failure following vancomycin-impregnated bone cement use has been documented by Dovas et al, 29 Curtis et al, 30 and McGlothan et al. 31
High vancomycin levels at the surgical site have been shown to have various other local adverse effects in animal models and in vitro studies. Goldschmidt et al 32 studied the effect of vancomycin on dural cell cultures. They showed that doses in the range of 400 to 4000 μg/mL inhibited dural cell proliferation, induced cell death, and altered cell morphology in a concentration-dependent fashion. Thus, TVP affects dural healing after intentional or unintentional durotomy in spinal surgery. Clippinger et al 33 also studied the effect of TVP on dura in rat models. They observed a higher grade of epidural fibrosis 30 days after the application of high-dose TVP when compared with the low-dose and control groups.
Chu et al 34 and Bariteau et al 35 studied the effect of vancomycin powder on human mesenchymal stromal cells (hMSCs) at various concentrations. They concluded that the higher the concentration of vancomycin, the lower the hMSC viability and osteogenic differentiation. Eder et al 36 analyzed the effects of TVP on osteoblasts and concluded that local concentration above 3 mg/dL had a deleterious effect and may increase the risk of nonunions in fusion procedures.
These in vitro and animal studies emphasize the need to identify the ideal dose of vancomycin to be used that does not affect dural healing or osteogenic activity, if at all TVP is found to be useful in preventing infection. Whether the suprafascial application of TVP as proposed by Clippinger et al 33 will help in preventing the deleterious effect of TVP on dura should also be studied, although 5 out of 6 studies included in the analysis recommended subfascial application.
Apart from the above-mentioned local and systemic safety concerns, another demerit of unindicated use of TVP is the selection pressure that it may put on microorganisms, leading to the development of resistant strains and increased incidence of gram-negative infections. Gande et al, 37 in 2019, analyzed the selection pressures caused by widespread TVP use in adult spine surgeries and concluded that widespread TVP use increases the chances of polymicrobial and gram-negative SSIs and that TVP use should be restricted to high-risk groups. In our review also, we noted gram-negative coinfection in SSIs occurring in the TVP group.
Although our results could not disprove the null hypothesis, we could not completely accept the hypothesis either considering the low quality of evidence. The quality of the available evidence and the above-mentioned safety concerns make the recommendation of TVP for routine use in pediatric spine surgeries highly questionable. Given that consensus has not been achieved regarding the use of TVP in adults 37,38 and that FDA approval is lacking, its use in the pediatric population should be avoided unless future evidence gives us robust supportive data. The sporadic adverse effects in adults can only be extrapolated as a more frequent occurrence in the more delicate pediatric population. Moreover, the risk factors for infection in children are different from those in adults, 1 and so protective measures must be tailor-made for them and cannot be generalized from that in the adult population.
Limitations
The current study has several limitations. There was only limited data available on the use of TVP in pediatric spine surgeries. Hence, only 824 patients in total were included for meta-analysis. The TVP protocol used by the included studies had no uniformity in the method of application or dosage of TVP, resulting in marked heterogeneity among the included studies. Moreover, all of them were retrospective cohort studies from the United States, and hence, future prospective multicenter studies with large sample sizes are needed to arrive at a consensus on TVP use.
Conclusion
TVP does not qualify to be recommended as a safe and useful option to prevent SSI following pediatric spine surgeries, based on the literature available at present. High-quality prospective interventional studies are needed to arrive at a consensus regarding its use, the appropriate dosage, and methods of application.
Supplemental Material
Supplemental Material, Annexure_1 - Is Use of Topical Vancomycin in Pediatric Spine Surgeries a Safe Option in the Prevention of Surgical Site Infections? A Meta-analysis and Systematic Review of the Literature
Supplemental Material, Annexure_1 for Is Use of Topical Vancomycin in Pediatric Spine Surgeries a Safe Option in the Prevention of Surgical Site Infections? A Meta-analysis and Systematic Review of the Literature by Muthu Sathish and Chellamuthu Girinivasan in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.