
Abstract
Study Design:
Cross-sectional, international survey.
Objectives:
This study addressed the global perspectives concerning perioperative use of pharmacologic thromboprophylaxis during spine surgery along with its risks and benefits.
Methods:
A questionnaire was designed and implemented by expert members in the AO Spine community. The survey was distributed to AO Spine’s spine surgeon members (N = 3805). Data included surgeon demographic information, type and region of practice, anticoagulation principles, different patient scenarios, and comorbidities.
Results:
A total of 316 (8.3% response rate) spine surgeons completed the survey, representing 64 different countries. Completed surveys were primarily from Europe (31.7%), South/Latin America (19.9%), and Asia (18.4%). Surgeons tended to be 35 to 44 years old (42.1%), fellowship-trained (74.7%), and orthopedic surgeons (65.5%) from academic institutions (39.6%). Most surgeons (70.3%) used routine anticoagulation risk stratification, irrespective of geographic location. However, significant differences were seen between continents with anticoagulation initiation and cessation methodology. Specifically, the length of a procedure (P = .036) and patient body mass index (P = .008) were perceived differently when deciding to begin anticoagulation, while the importance of medical clearance (P < .001) and reference to literature (P = .035) differed during cessation. For specific techniques, most providers noted use of mobilization, low-molecular-weight heparin, and mechanical prophylaxis beginning on postoperative 0 to 1 days. Conversely, bridging regimens were bimodal in distribution, with providers electing anticoagulant initiation on postoperative 0 to 1 days or days 5-6.
Conclusion:
This survey highlights the heterogeneity of spine care and accentuates geographical variations. Furthermore, it identifies the difficulty in providing consistent perioperative anticoagulation recommendations to patients, as there remains no widely accepted, definitive literature of evidence or guidelines.
Introduction
Venous thromboembolism (VTE) is a preventable cause of perioperative morbidity and mortality. The incidence of VTE after spine surgery varies widely, ranging between 0.3% and 31%. 1 -11 Multiple factors contribute to this heterogeneity. These studies have consisted of patients undergoing surgery for elective, trauma, or oncologic indications (as some present with higher baseline rates of VTE), and also lack consistency in the method and timing of diagnosis. Given the heterogeneity of medical comorbidities, spinal pathology, and surgical techniques, a need for patient-specific anticoagulation guidelines is mounting.
Early patient mobilization, sequential compression devices (SCDs), and compression stockings are common nonpharmacologic approaches to VTE prophylaxis. 12 -14 Several pharmacologic agents exist that are prescribed for VTE prophylaxis, such as heparin, low-molecular-weight heparin (LMWH), and warfarin. These medications directly target factors involved in the coagulation cascade. 15 -20 Other medications indirectly target similar factors, such as factor Xa. 21 -23 A combination of these modalities are often parts of the multimodal VTE prevention strategy. Unfortunately, pharmacologic VTE prophylaxis can also cause a postoperative epidural hematoma or persistent wound drainage leading to higher rates of infection.
Recent practice guidelines have been generated related to the type and timing of VTE prophylaxis for patients with acute spinal cord injury, although uncertainty remains regarding the optimal timing for the initiation of therapy. 24 Moreover, there is no consensus about perioperative VTE prophylaxis for patients undergoing spine surgery in patients with disorders other than an acute SCI. The risk of developing a clinically significant VTE must be balanced with the risk of early postoperative bleeding and epidural hematoma formation. 25 -27 Several attempts to create surveys have been made to elicit perioperative VTE prophylaxis patterns. However, several surveys have noted that the use of thromboprophylactic medications in the perioperative setting differed greatly 28,29 and that there is no clear consensus on its use. 30 Previous studies are limited by small sample sizes that prevent extensive assessment of risk factors and heterogeneity among anticoagulation methods. They also do not account for the different perspectives of spine surgeons globally. In addition, in 2009, the North American Spine Society attempted to create clinical guidelines on antithrombotic therapies in spine surgery. 18 Although comprehensive, these guidelines have yet to be widely adopted worldwide.
Given the lack of consensus surrounding perioperative anticoagulation management in spine surgery, we conducted a global survey of spine surgeons to gauge their knowledge, attitudes, and practices on this topic. These results will shed light on how spine surgeons manage thromboprophylaxis over multiple countries, specialties, time in practice, type of practice, and many other specific variables. We hypothesize that the survey responses will show heterogeneity in anticoagulation practices with few instances of general consensus surrounding perioperative thromboprophylaxis in spine surgery.
Methods
Survey Design
A survey questionnaire was developed, including demographic information regarding surgeon and their practice, general anticoagulation principles, and scenarios based on patient factors, comorbidities, and region of spine pathology necessitating surgical intervention. The questions were developed by the Global Spine Journal Editorial Board and the Regional Research Chairs of AO Spine. Question selection was based on a Delphi-esque style for consensus, following several rounds of review before finalization.
Demographics were obtained on geography, specialty training, time in practice, practice type, and surgical volume. The general anticoagulation questions focused on current rationale for anticoagulation following spine surgery, risk stratification applications, the use of published/unpublished guidelines to guide treatment, and the use of multidisciplinary teams. The specific anticoagulation section was further subdivided into cervical, lumbar, and thoracolumbar surgery. Questions sought to assess perioperative factors that affect the timing of anticoagulation prophylaxis, how the diagnosis of a spinal cord injury affects thromboprophylaxis, period of bridging (the use of short-acting anticoagulants during interruption of warfarin therapy), and individual anticoagulation treatments based on medical comorbidities and previous episodes of thrombosis and/or embolus.
The survey was subsequently designed on a SurveyMonkey platform (San Mateo, CA) and distributed to the AO Spine membership through emails that classified themselves as independently performing spine surgery and who agreed to receiving such surveys via email (n = 3805 members out of approximately 6000 members). The survey recipients were provided a total of 4 weeks to complete the survey. The responses were anonymized and stored separately from the list of respondents.
Statistical Analyses
All statistical analyses were performed with Stata version 13.1 (StataCorp LC, College Station, TX). Graphical representation of survey responses was performed using RStudio v1.2.1335 (RStudio Inc, Boston, MA). Interpretation and categorization of all free-response survey answers were made by one independent reviewer to group similar categories for analyses. Calculation of percentages and means was made for count data and rank-order questions, respectively. Depiction of data was performed using a combination of RStudio’s ggplot2, rworldmap, PieDonut, and other required packages. Basic statistical analyses were performed to assess significant differences in count data using a combination of Fisher’s exact and χ2 tests. Differences in continuous variables between groups was assessed using analysis of variance (ANOVA). The threshold for statistical significance for all tests was established at P < .05.
Results
Overall, 316 spine surgeons from 64 countries completed the survey (Figure 1). The largest number of responses were from the United States (12.3%), India (10.1%), and Germany (6.0%). When stratified by continent, Europe had the largest survey representation (31.7%), followed by South America/Latin America (19.9%) and Asia (18.4%).
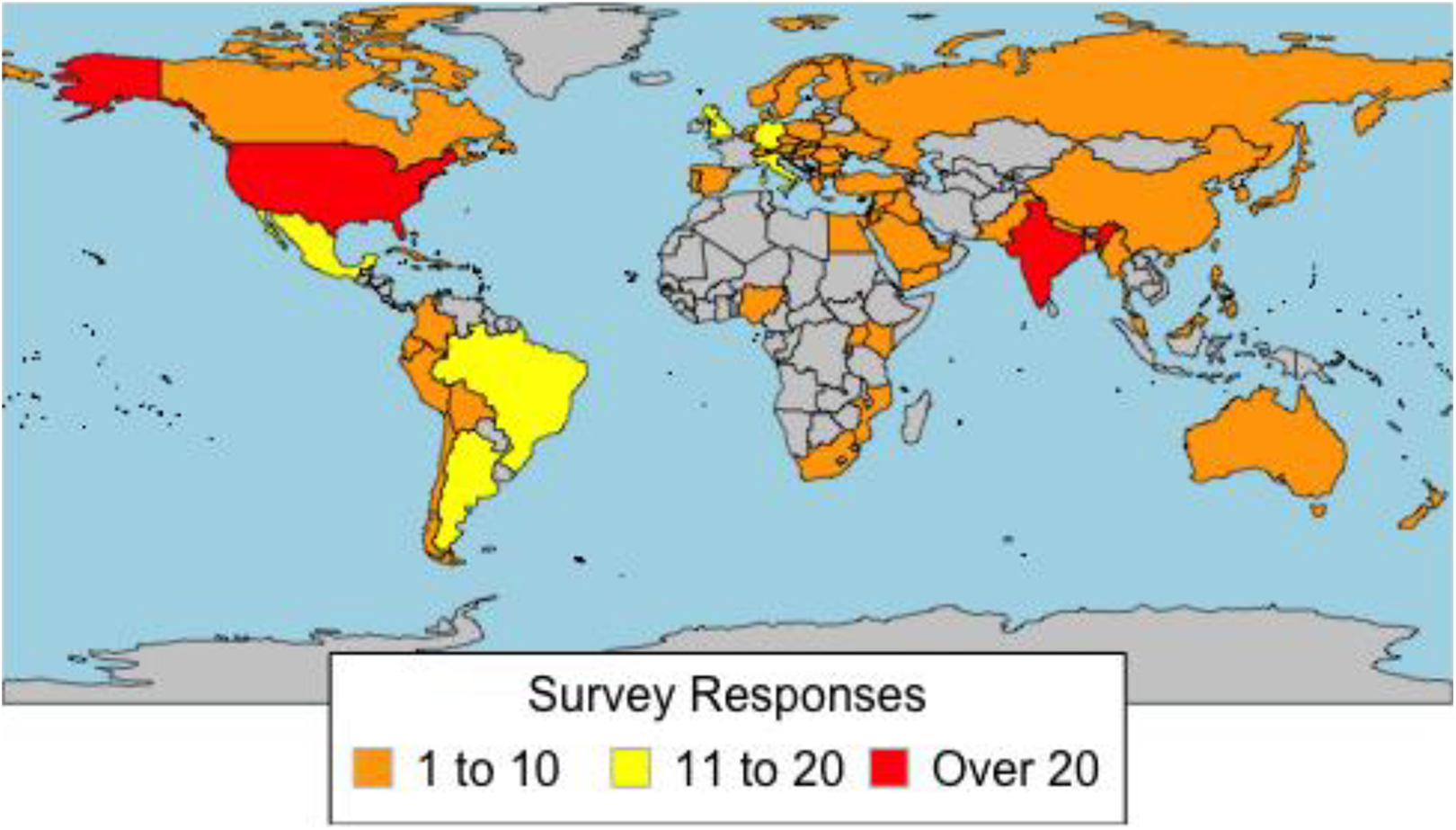
Distribution of survey responses by country.
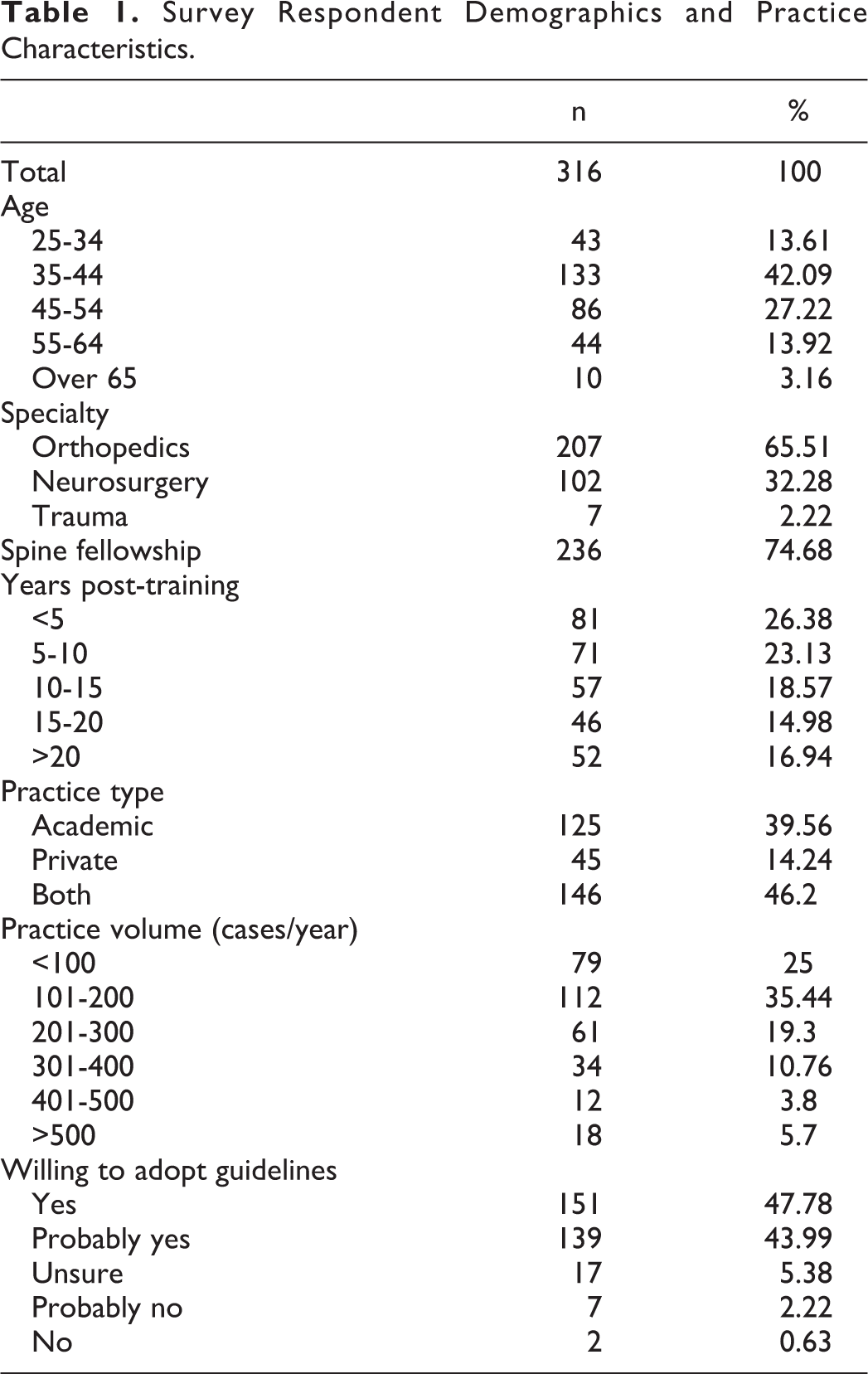
Respondents were between the ages of 35 to 44 (42.1%) and 45 to 54 (27.2%) years, and were typically fellowship-trained (74.7%) and orthopedic surgeons (65.5%). Most were within 5 years (26.4%) or 5 to 10 years (23.1%) of completing their training, and they practiced at academic (39.6%) or combined private/academic institutions (46.2%). The vast majority of respondents performed an estimated 101 to 200 cases per year (35.4%). Nearly all surgeons answered that they would likely adopt anticoagulation guidelines, if established (91.8%; Table 1).
Survey Respondent Demographics and Practice Characteristics.
Regarding current practices, most surgeons (70.3%) admitted to routine anticoagulation risk-stratification techniques, irrespective of geographic location. Of these respondents, the most common risk-stratification method cited use of a comorbidity-based evaluation (31.5%) followed by the use of either hospital, national, or other unspecified guidelines (14.4%). Overall, reported methods were roughly similar between continents, though significant differences were observed in the number of recipients who reported use of multiple risk-stratification techniques (P = .01). Among recipients who reported no use of routine risk-stratification, when a reason was specified, most reported indiscriminate anticoagulation use (23.1%). No significant differences in reporting for risk-stratification abstinence was noted between continents (Tables 2 -4; Figures 2A, 2B, and 2C).
Do You Perform Risk Stratification for Anticoagulation?a
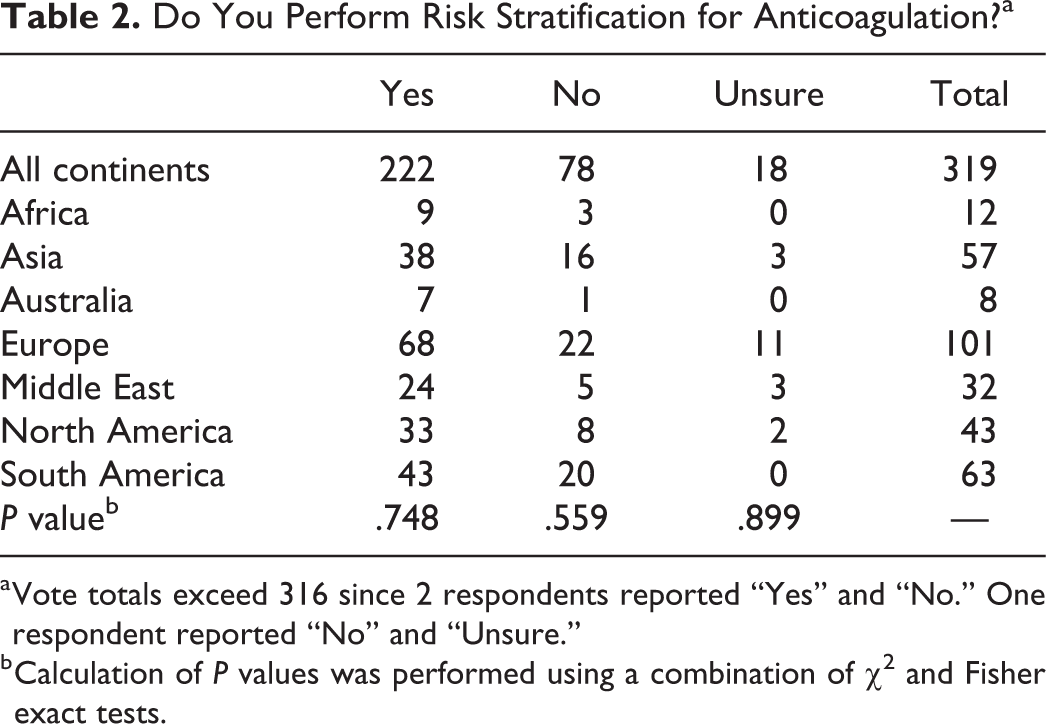
a Vote totals exceed 316 since 2 respondents reported “Yes” and “No.” One respondent reported “No” and “Unsure.”
b Calculation of P values was performed using a combination of χ2 and Fisher exact tests.
Reasons for Risk Stratification.
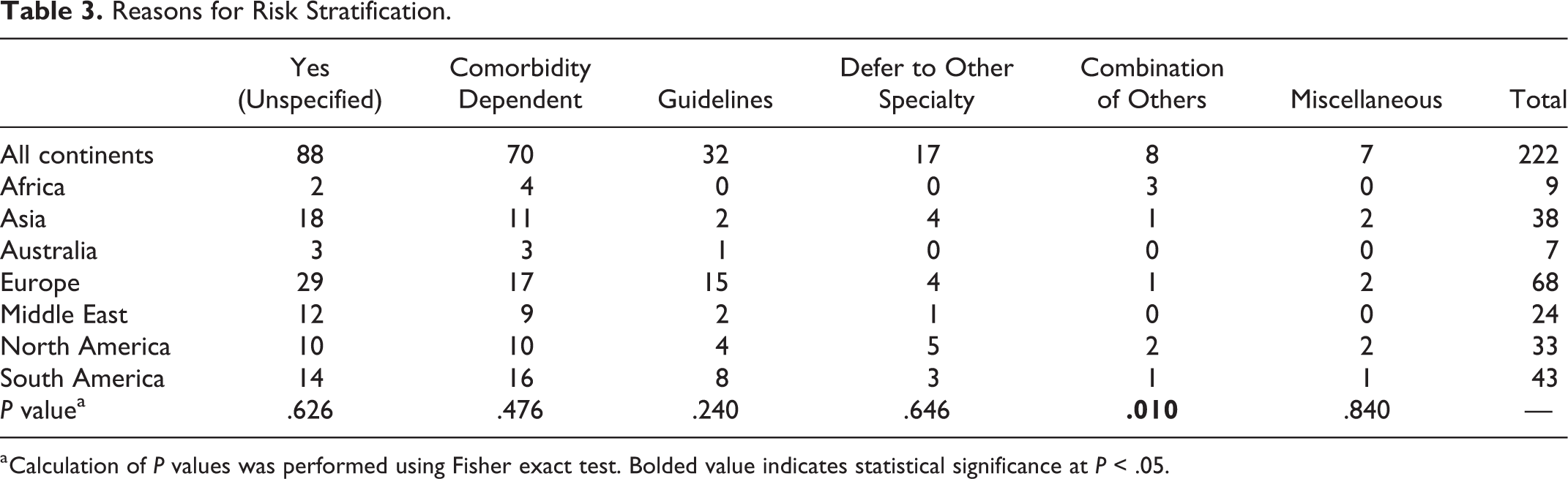
a Calculation of P values was performed using Fisher exact test. Bolded value indicates statistical significance at P < .05.
Reasons for No Risk Stratification.
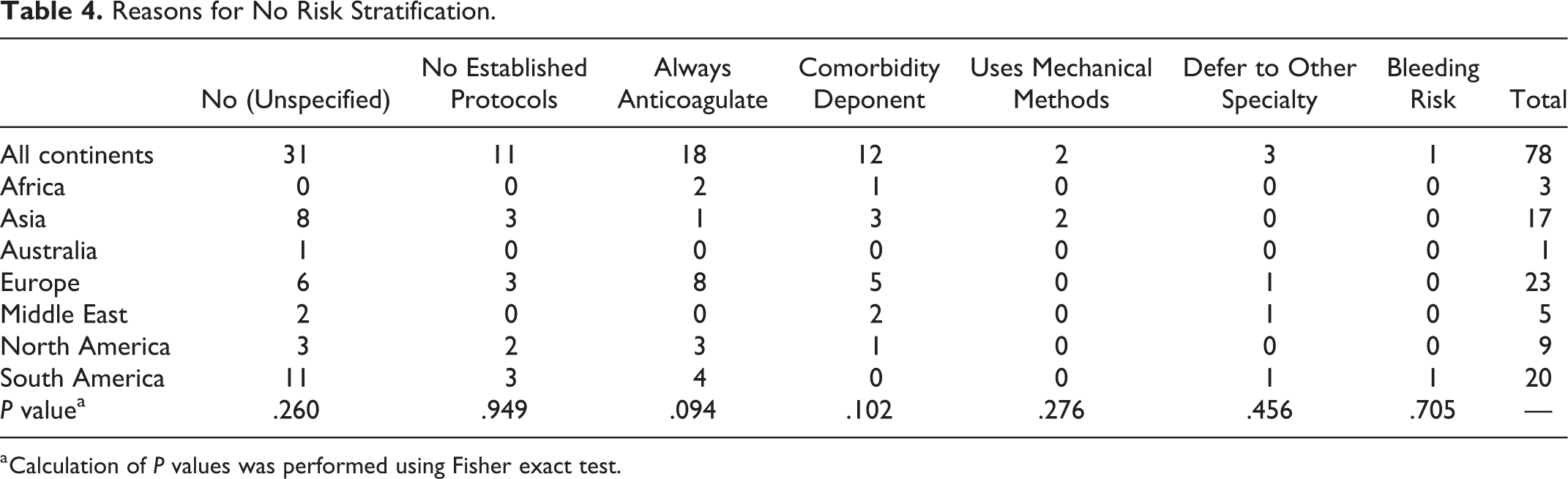
a Calculation of P values was performed using Fisher exact test.
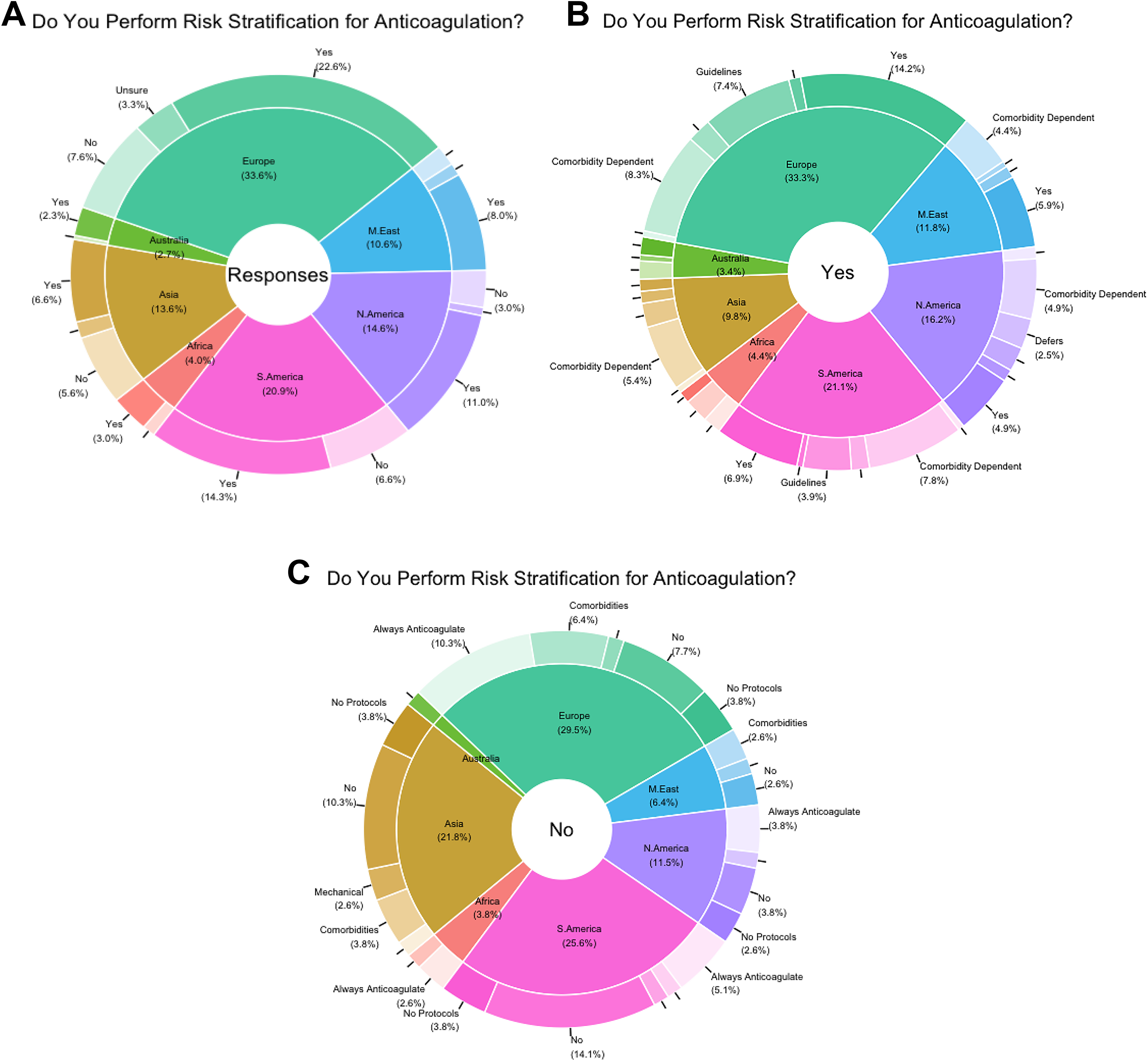
(A) Overall responses by continent. (B) Yes responses. (C) No responses.
When querying recipients on factors considered during anticoagulation initiation and cessation, significant differences were seen in reporting between continents. Specifically, significant differences in perceived importance of fellowship training (P = .016), unspecified guidelines (P = .022), and choice of specialty (P = .025) were observed between continents in anticoagulation initiation practices, while usage of medical clearance (P < .001) and reference to the literature (P = .035) differed during anticoagulant cessation. Moreover, within continents, differences were seen between mean rankings for various categories for initiation and cessation as well (Tables 5 and 6). Similarly, for specific patient-related factors employed in initiation of anticoagulation, significant differences in importance of length of operation (P = .036) and body mass index (P = .008) were also observed by geographic location (Table 7; Figures 3A, 3B, and 3C). Interestingly, no significant differences were seen between continents regarding anticoagulation methodology employed in the setting of spinal cord injury (Tables 8 and 9).
Mean Importance for Factors Influencing Anticoagulation Initiationa.
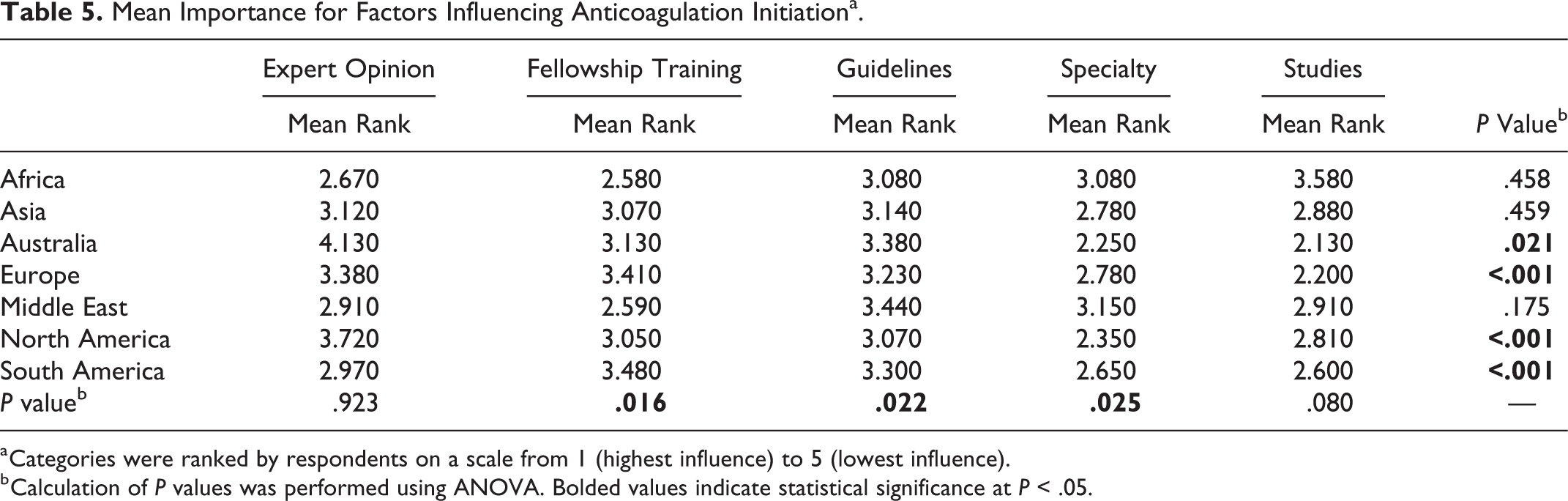
a Categories were ranked by respondents on a scale from 1 (highest influence) to 5 (lowest influence).
b Calculation of P values was performed using ANOVA. Bolded values indicate statistical significance at P < .05.
Mean Importance for Factors Influencing Cessation of Anticoagulationa.
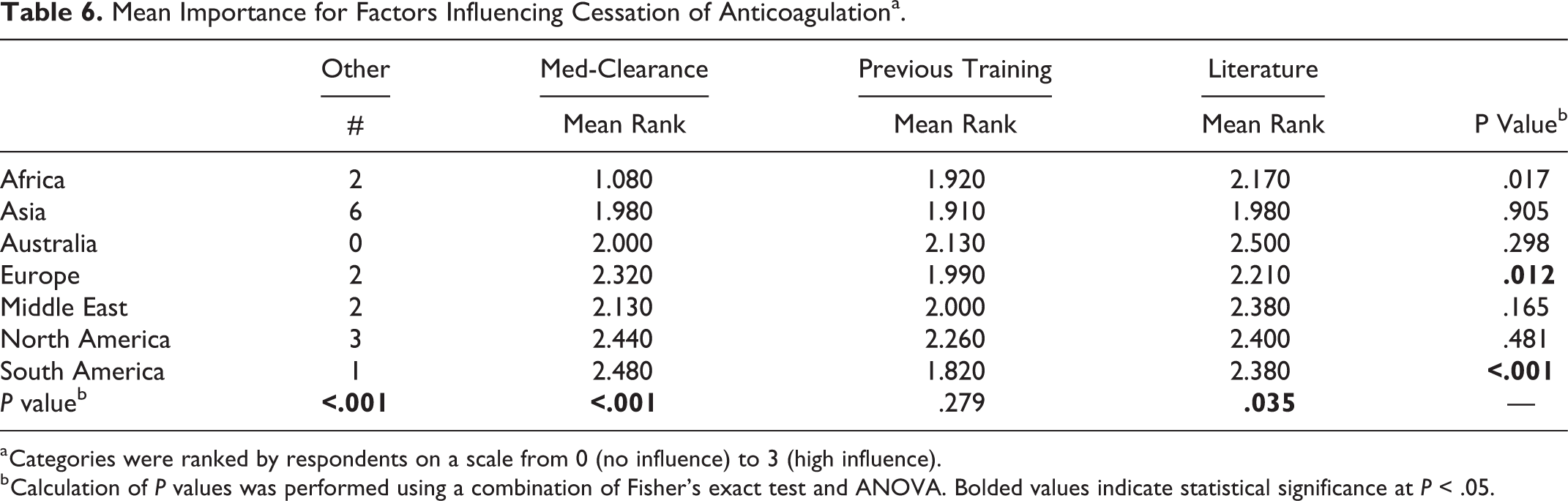
a Categories were ranked by respondents on a scale from 0 (no influence) to 3 (high influence).
b Calculation of P values was performed using a combination of Fisher’s exact test and ANOVA. Bolded values indicate statistical significance at P < .05.
Mean Importance for Patient-Specific Factors Influencing Initiation of Anticoagulationa.
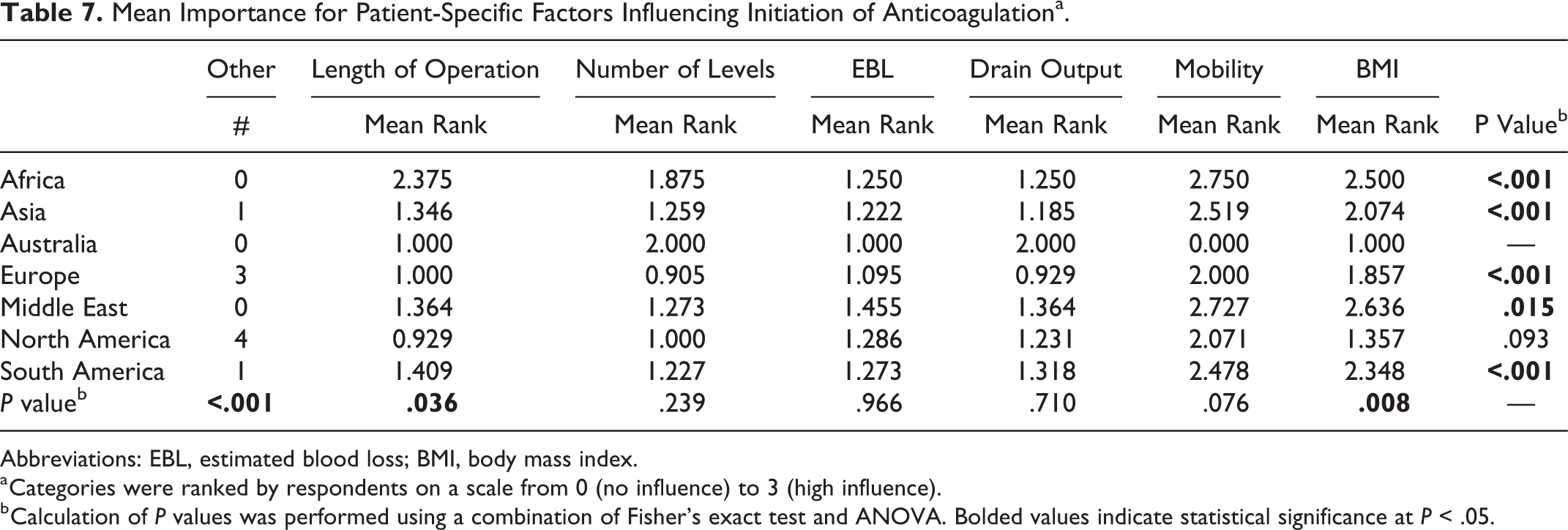
Abbreviations: EBL, estimated blood loss; BMI, body mass index.
a Categories were ranked by respondents on a scale from 0 (no influence) to 3 (high influence).
b Calculation of P values was performed using a combination of Fisher’s exact test and ANOVA. Bolded values indicate statistical significance at P < .05.
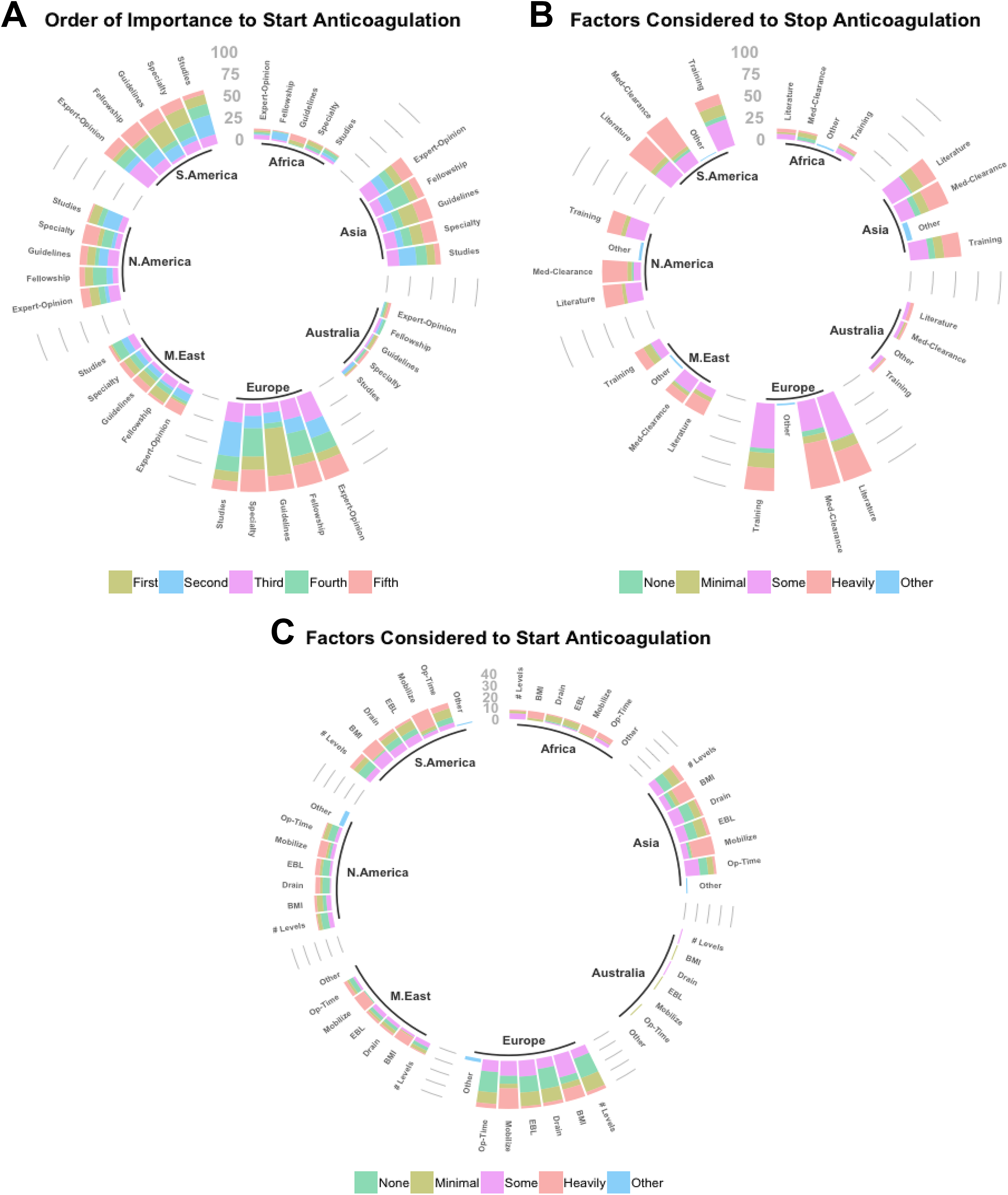
(A) Ranking of importance for factors influencing anticoagulation initiation. (B) Ranking of factors influencing anticoagulation cessation. (C) Ranking of patient-specific factors influencing anticoagulation initiation.
Spinal Cord Injury.
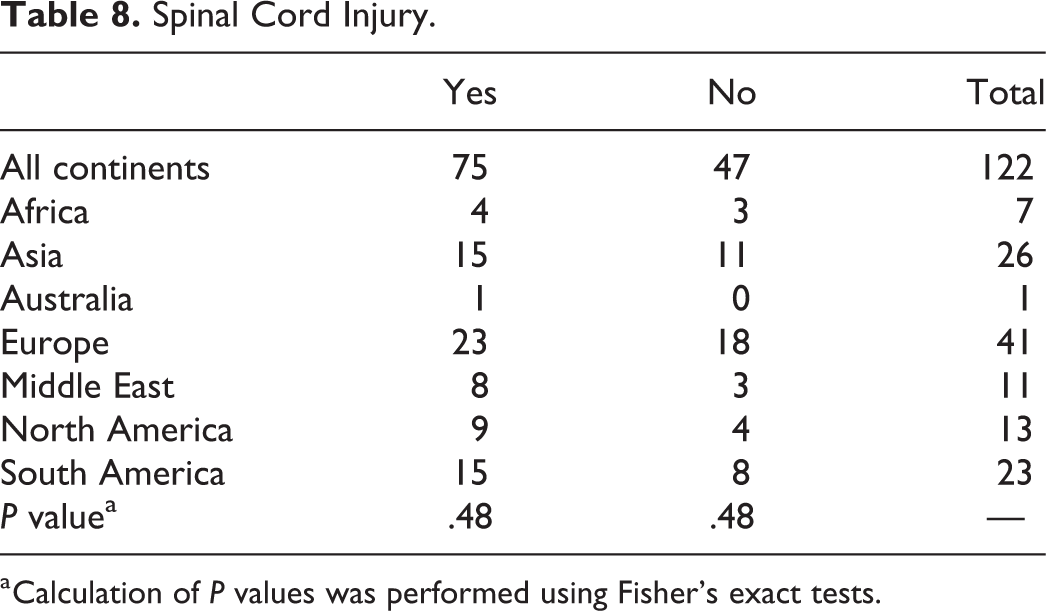
a Calculation of P values was performed using Fisher’s exact tests.
Anticoagulation Methods when Considering Spinal Cord Injury.
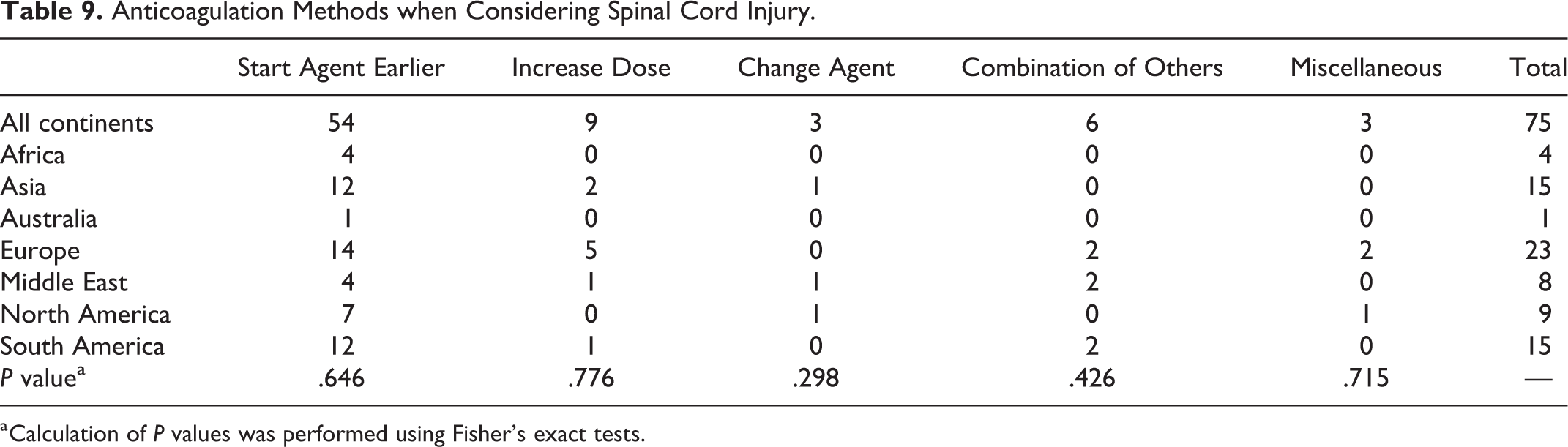
a Calculation of P values was performed using Fisher’s exact tests.
Regarding techniques employed during various hypothetical scenarios, the vast majority of providers noted use of mobilization techniques (range: 71-82 votes), LMWH (range: 62-77 votes), and mechanical prophylaxis (SCD range: 39-46 votes; compression socks range: 35-44 votes) irrespective of the given patient history (Table 10). Similar trends were observed even where patients were utilizing prescribed anticoagulation preoperatively (Table 11).
Anticoagulation (AC) Methods for Hypothetical Scenarios Without Baseline AC Use.
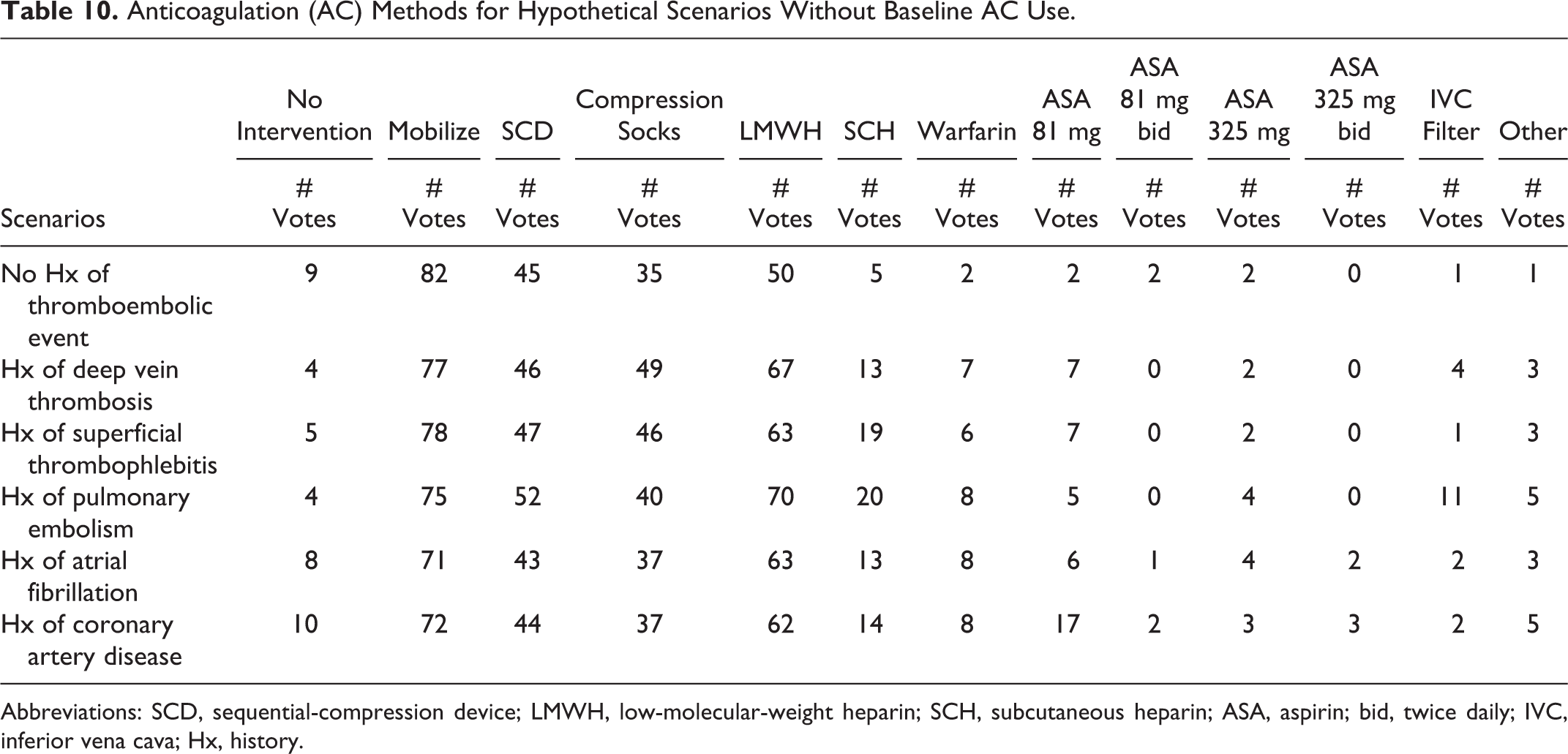
Abbreviations: SCD, sequential-compression device; LMWH, low-molecular-weight heparin; SCH, subcutaneous heparin; ASA, aspirin; bid, twice daily; IVC, inferior vena cava; Hx, history.
Bridging Methods for Hypothetical Scenarios with Baseline Anticoagulation Use.
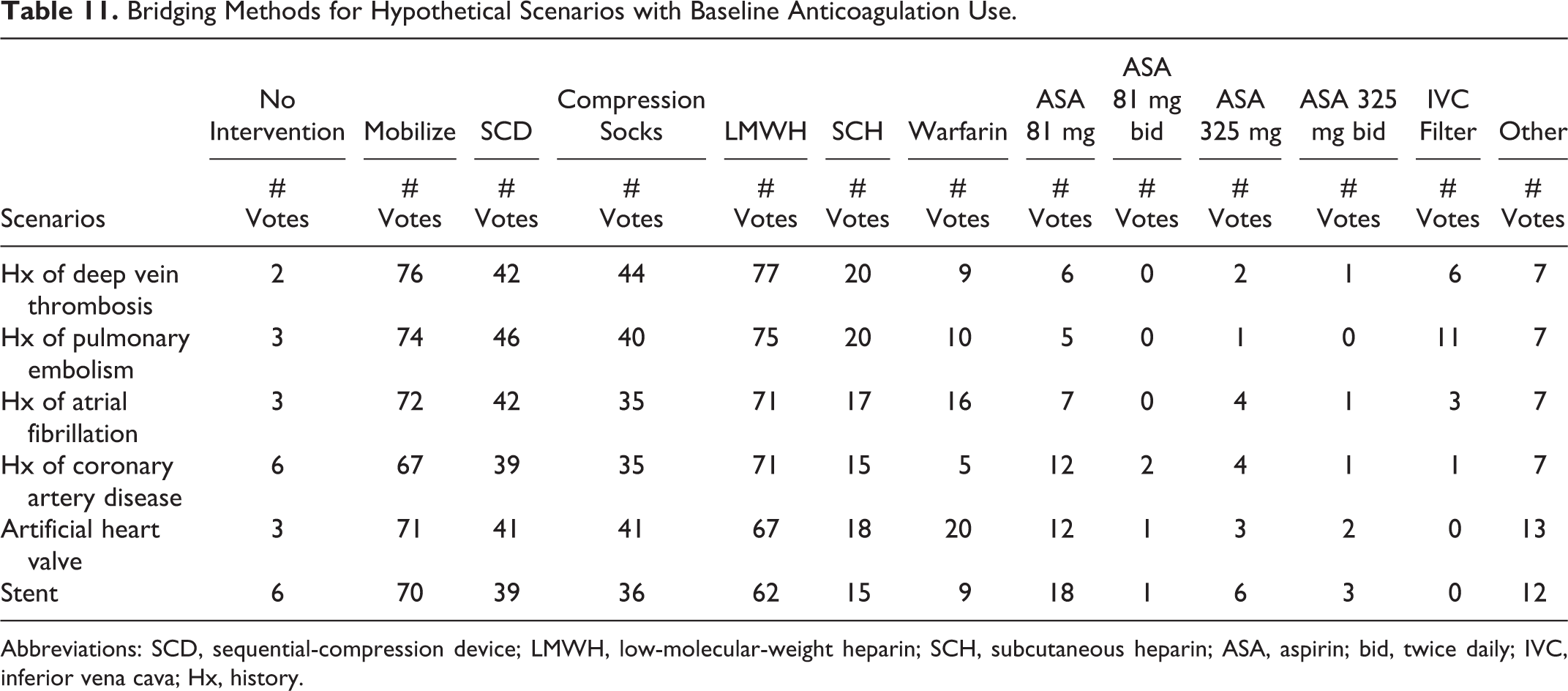
Abbreviations: SCD, sequential-compression device; LMWH, low-molecular-weight heparin; SCH, subcutaneous heparin; ASA, aspirin; bid, twice daily; IVC, inferior vena cava; Hx, history.
Last, when queried on timing of anticoagulant initiation (for patients not previously on anticoagulation), the vast majority of respondents noted initiation on postoperative day 1 (range: 22-25 votes), followed by postoperative day 0 (range: 9-22 votes; Table 12; Figure 4). Conversely, bridging regimens appeared bimodal in distribution, with most providers electing initiation of aspirin, warfarin, or another agent on postoperative day 1 (range: 13-26 votes) or day 0 (range: 11-28 votes), as well as on day 5 (range: 8-20 votes) or day 6 and beyond (range: 7-15 votes; Table 13; Figures 5A and 5F).
Start Time (Days) for New Anticoagulation Regimen.
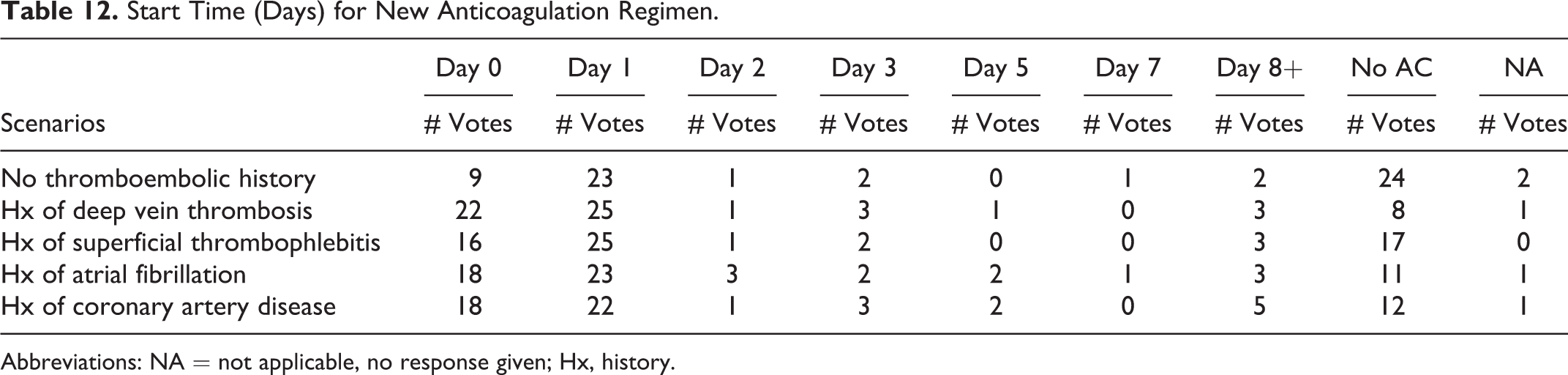
Abbreviations: NA = not applicable, no response given; Hx, history.
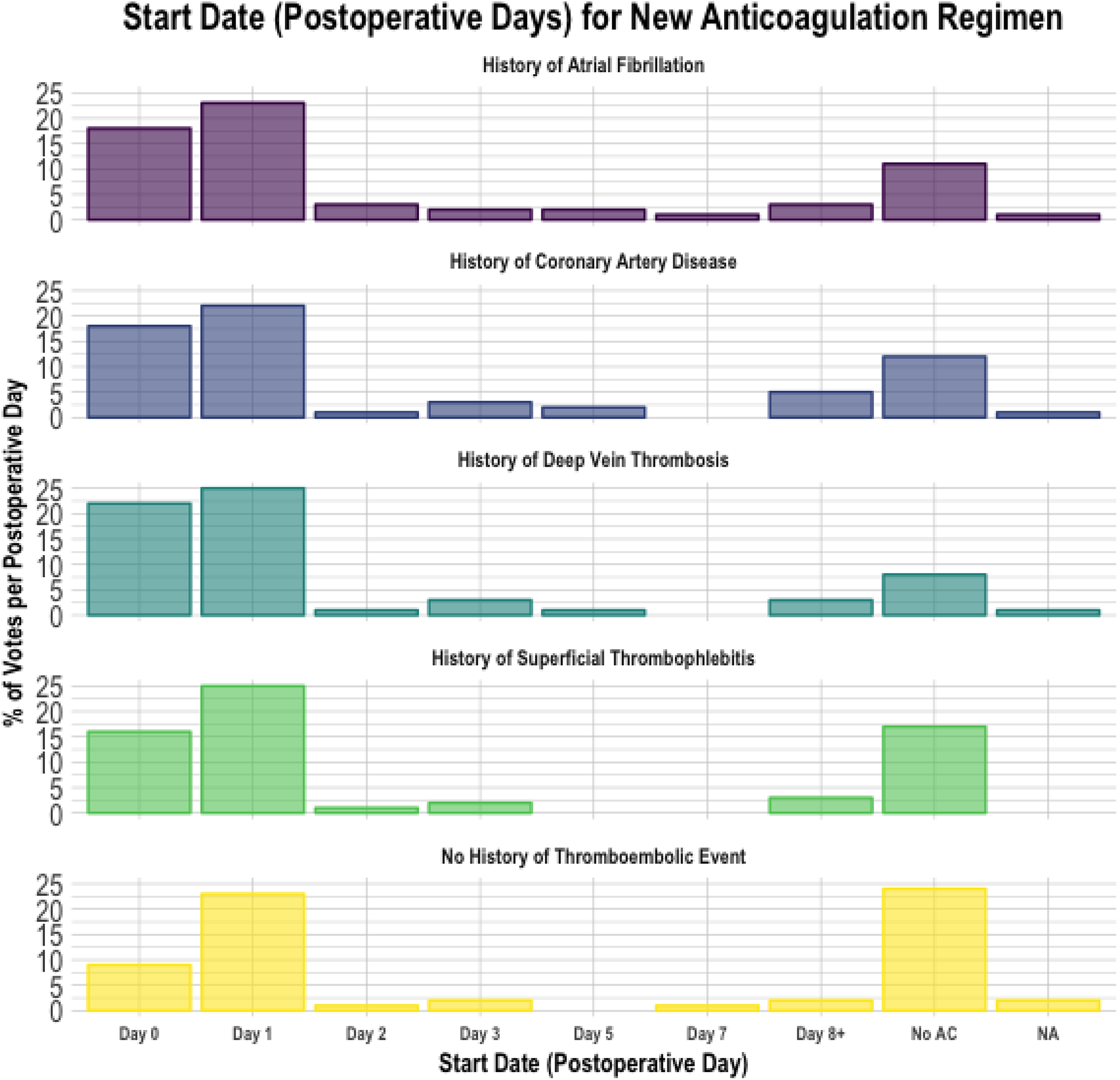
Start date for new anticoagulation regimen.
Bridge Time (Days) for Previous Anticoagulation Regimen.
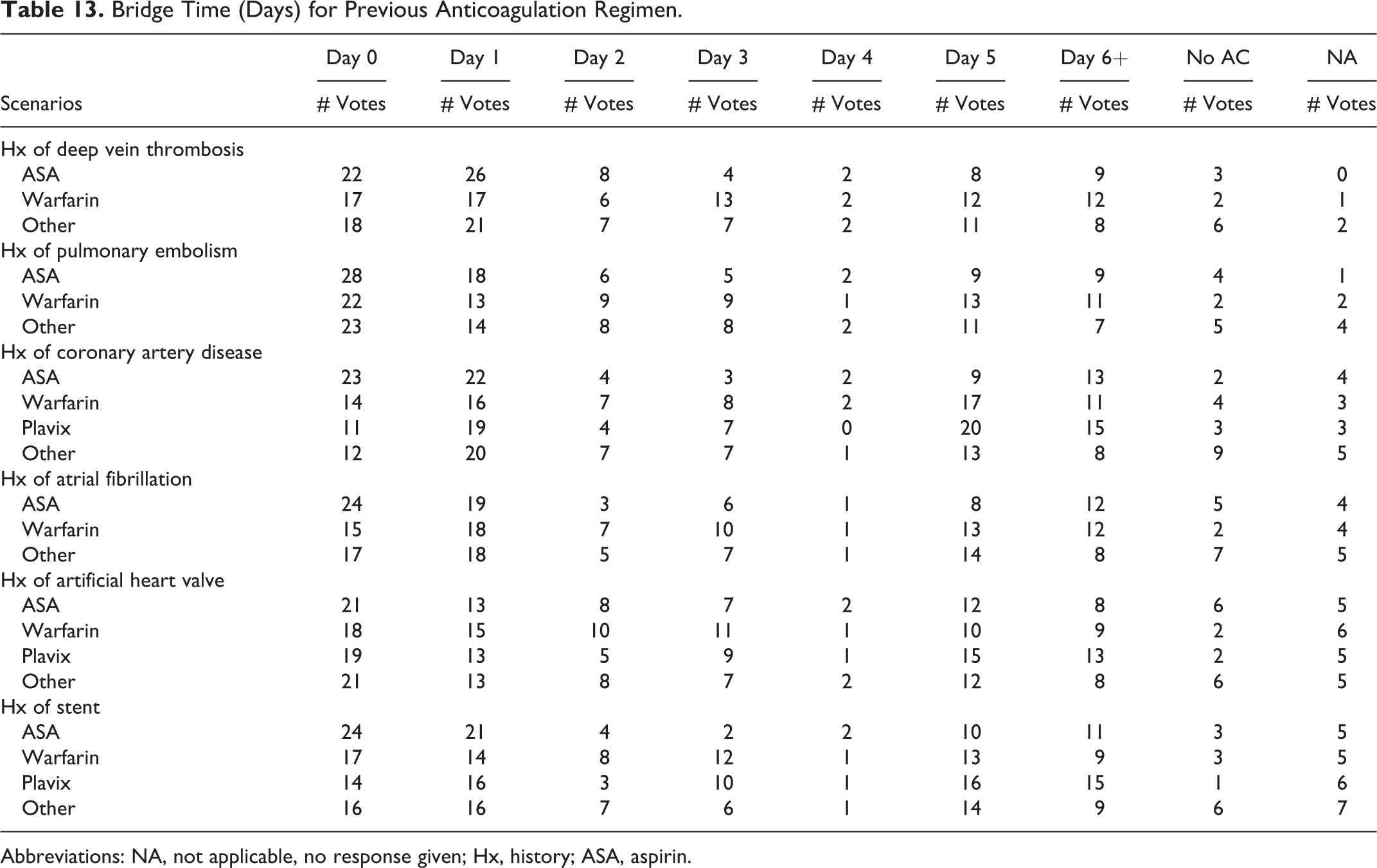
Abbreviations: NA, not applicable, no response given; Hx, history; ASA, aspirin.

(A) History of DVT: Start date (postoperative days) for bridging regimen. (B) History of A-Fib: Start date (postoperative days) for bridging regimen. (C) History of CAD: Start date (postoperative days) for bridging regimen. (D) History of PE: Start date (postoperative days) for bridging regimen. (E) History of stent: Start date (postoperative days) for bridging regimen. (F) Artificial heart valve: Start date (postoperative days) for bridging regimen.
Discussion
Timing and use of perioperative thromboprophylaxis is controversial given the lack of consensus on best strategies. This topic remains challenging given the heterogeneity in patient presentation and difficulties in balancing the risks of developing clinically significant VTE versus early postoperative bleeding. As the largest survey to directly focus on perioperative anticoagulation practices in spine surgery to date, we brought to light the heterogeneity in practices worldwide. Most important, nearly all surgeons answered that they would likely adopt anticoagulation guidelines, if established (91.8%). Most surgeons (70.3%) admitted to routine anticoagulation risk-stratification techniques, irrespective of geographic location. The most common risk-stratification method used a comorbidity-based evaluation (31.5%) followed by the use of guidelines (14.4%). Among recipients who did not use any routine risk-stratification, when a reason was specified, most reported indiscriminate anticoagulation use (23.1%). Significant differences were observed in perceived importance of fellowship training, unspecified guidelines, and choice of specialty between continents in anticoagulation initiation practices. While usage of medical clearance and reference to the literature differed when considering timing of anticoagulant cessation. For specific patient-related factors employed in initiation of anticoagulation, significant differences in importance of length of operation and body mass index were also observed by geographic location. Interestingly, no significant differences were seen between continents regarding anticoagulation methodology employed in the setting of spinal cord injury.
The vast majority of providers used mobilization techniques (range: 71-82 votes), LMWH (range: 62-77 votes), and mechanical prophylaxis (SCD range: 39-46 votes; compression socks range: 35-44 votes) irrespective of the given patient history. Similar trends were observed even where patients were utilizing prescribed anticoagulation preoperatively. The vast majority of respondents who used chemoprophylaxis initiated it on postoperative day 1 (range: 22-25 votes), followed by postoperative day 0 (range: 9-22 votes). Conversely, bridging regimens appeared bimodal in distribution, with most providers electing initiation of aspirin, warfarin, or another agent on postoperative day 1 (range: 13-26 votes) or day 0 (range: 11-28 votes), as well as on day 5 (range: 8-20 votes) or day 6 and beyond (range: 7-15 votes).
Only a limited number of surveys have been published that describe perioperative VTE prophylaxis patterns. In a survey created for spine and trauma-trained surgeons, Ploumis et al 28 concluded that spine trauma surgeons do not routinely use chemical prophylaxis after cervical spine surgery, and that the use of thromboprophylaxis was tailored to the risk factors involved with each patient’s presentation. However, this survey consisted of only 47 surgeons focusing primarily on patients presenting following spine trauma. Based on a survey of 40 spine surgeons practicing in Switzerland, Baschera et al 29 concluded that the administration and discontinuation of thromboprophylactic medications in the perioperative setting differed vastly between different units and surgeons. This survey focused on the decision to start several anticoagulation medications based on various surgeries. However, the survey was distributed in only one country, which may limit generalizability. Similarly, 8 different clinical scenarios were presented to 50 spine surgeons at a British Association of Spine Surgeon by Bryson et al. 30 This group concluded that there was no clear consensus in thromboprophylaxis in any of the surgeries. These findings highlight the discrepancies and uncertainties, likely attributable to the paucity of literature examining VTE in spinal surgery. Last, in 2009, the North American Spine Society attempted to create clinical guidelines on antithrombotic therapies in spine surgery. 18 Albeit comprehensive, these guidelines have yet to be widely adopted; as only 14% of our respondents described following hospital, national, or other unspecified guidelines.
The results of this survey highlights the lack of consensus on various aspects of thromboprophylaxis in spine surgery. Although a large percentage of respondents subscribed to routine anticoagulation risk-stratification techniques, reported methods differed largely irrespective of geographic location. Additionally, when querying respondents on factors considered during anticoagulation initiation and cessation, significant differences were seen in reporting between geographic locations of practice. Specifically, the utilization of medical clearance and adherence to the practices described in literature also widely varied geographically. Among recipients who reported no use of routine risk-stratification, when a reason was specified, most reported indiscriminate anticoagulation use. One area in which there was relative agreement was the approach to thromboprophylaxis in the setting of spinal cord injury (SCI). Patients with acute SCI have been shown to present with the highest risk of VTE among hospitalized patients, ranging from 50% to 100% in untreated patients, and pulmonary embolism is the third most common cause of mortality in these patients. 31 -33 The global adherence to thromboprophylactic principles in SCI patients are likely a result of the various well-studied and widely established/distributed recommendations and protocols for this presentation. 24,34 -37
Despite the large amount of data published on specific thromboprophylactic therapies for various spine surgery indications, well-established guidelines and algorithms have had difficulty gaining widespread acceptance and adherence. 2,15 -18,20 -23,38 -43 Although spine surgery VTE prophylaxis recommendations from North American Spine Society and American College of Chest Physicians have been published, these groups describe “spine surgery” as a broad category, not taking into account the differing VTE and bleeding complication risks associated with specific surgical procedures and the location in the spine. 18,44 To this point, Eskildsen et al 45 worked to develop an algorithm for thromboprophylaxis in spine surgery. This group created a score based on patient-related and surgery-specific risk factors for elective spine surgeries. This algorithm has difficulty addressing scenarios in which patients are unable to receive standard prophylaxis and fails to provide a score for some spine surgeries. Nonetheless, this algorithm may help guide spine surgeons when deciding on thromboprophylaxis in the majority of clinical situations. Despite these attempts at creating widely accepted recommendations and algorithms, this survey shows that reference to these published items is not commonly practiced globally. The question remains how we can fundamentally address thromboprophylaxis as a spine community and develop a widely accepted algorithm or guideline to reference worldwide. Although difficult, future prospective studies are necessary to determine whether certain recommendations and algorithms can improve outcomes in VTE and bleeding complication rates following common spine surgeries. We plan to use the information from this survey to better understand global-, training-, and practice-specific indications for perioperative thromboprophylaxis to design a prospective randomized trial that can develop future guidelines and algorithms.
As with any survey, there are limitations to our current survey and its findings. The survey distribution was limited to current spine surgeon members of the AO Spine network that opted-in to receive email notifications, survey requests falling into this category. As such, there is still questionable generalizability, especially in regions in which there were very few or no respondents, and potential selection bias that may represent a unique make-up of those spine surgeons opting to receive the survey as opposed to those that did not. The survey was sent out to 3805 spine surgeons worldwide; however, only 316 surgeons responded (8.3%). Although the response rate may appear low, perhaps we have captured respondents who take special interest in this topic and have placed greater thought to their anticoagulation practices. Previous studies have described that a low response rate does not necessarily mean the study results have low validity, they simply indicate a greater risk of this. Therefore, response rates can be informative, but independently should not be considered a good proxy for study validity. 46 -48 Furthermore, such a response rate affiliated with AO Spine surveys distributed to the membership have been consistent. Given the length limit of surveys in general, we were not able to capture all of the possible patient comorbidities, specific spine surgeries, nor pharmaceutical options. However, given the variety of unique presentations and treatment practices worldwide, our goal was to capture the majority of spine surgeons. Although these limitations exist, this remains the largest, international survey to date focused on perioperative anticoagulation practices during spine surgery.
Conclusions
This AO Spine Anticoagulation Global Survey is the largest to date focusing on perioperative anticoagulation attitudes, practices, and beliefs among spine surgeons worldwide. Through the distribution of this large, global survey directly focused on perioperative anticoagulation practices in spine surgery, our study highlights the heterogeneous practices across geography, specialties, time in practice, type of practice, and several other variables. The one area of agreement across various backgrounds is the thromboprophylaxis treatment plan in patients presenting with spinal cord injury. This survey raises awareness and quantitatively highlights the difficulty in providing consistent perioperative anticoagulation recommendations to patients as there have been no widely accepted guidelines to date. Future studies will utilize this data to better understand global-, training-, and practice-specific indications for perioperative thromboprophylaxis to design robust future study designs, such as prospective randomized trials, that can develop future guidelines and algorithms or the need for expert group consensus recommendations for anticoagulation management.
Footnotes
Acknowledgements
The authors wish to thank Jayr Bass, Regula Bleuler, Niccole Germscheid, and Kaija Kurki-Suonio from AO Spine for providing administrative support, and with assistance in survey building and circulation to members.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.