
Abstract
Study Design:
Retrospective matched cohort study.
Objectives:
Identifying candidates for isolated percutaneous screw fixation (PSF) in thoracolumbar fractures based on Thoracolumbar Injury Classification and Severity (TLICS) score.
Methods:
Patients underwent PSF were split into 3 TLICS-score categories, then matched with groups having similar scores managed either non-operatively or via open screw fixation (OSF). Each category was assessed for corrective power and loss of correction by comparing initial and 1-year Cobb angles as well as Oswestry Disability Index and rates of fracture healing at 1 year.
Results:
A total of 102 patients (40 females) with age range 19 to 51 years, were admitted 1 to 25 hours following trauma. Each of TLISC categories consisted of matched treatment groups for comparison. In TLICS-3 fractures (2 treatment groups, n = 12 each), PSF showed similar outcomes but longer time to ambulation and length of stay (LOS) compared with nonoperative management. In TLICS-4 fractures (3 treatment groups, n = 18 each), PSF showed comparable corrective power and outcomes as OSF but was better in terms of operative time, blood loss, time to ambulation, LOS, and cosmesis. Despite higher LOS when compared with nonoperative cases, PSF showed superior radiologic and functional outcomes. In TLICS-5 fractures (2 treatment groups, n = 12 each), PSF showed shorter admissions and time to ambulation but lower corrective power, functional recovery, and tendency to lower healing rates.
Conclusions:
Isolated PSF is a valid choice in managing TLICS-4 thoracolumbar fractures; however, it did not surpass conventional methods in TLICS-3 or TLICS-5 fracture types. Further studies are needed before the generalization of findings.
Introduction
Several classification systems have been described for thoracolumbar injuries. Among these systems, the Thoracolumbar Injury Classification and Severity (TLICS) score described by the Spine Trauma Study Group in 2005 has proven to be notably useful taking into account the neurological status in addition to the morphological features of injury. 1 The score has demonstrated acceptable reliability and validity in various studies and its recommendations were suggested to be of probable higher reliability than those of the AO thoracolumbar injury classification system particularly for guiding the surgical management of unstable burst fractures. 2 Although the resulting score can categorize patients into nonoperative (TLICS ≤ 3) and operative (TLICS ≥ 5) candidates, those patients with score 4 represent an indistinct group where either operative or nonoperative management may be conducted. Moreover, the score does not state the specifics of surgery in surgical candidates, basically, the surgical approach (anterior versus posterior) and the fixation type (open vs minimally invasive)
Despite the immense growth in popularity of percutaneous spinal fixation over the last decade, percutaneous placement of internal spinal fixators has been reported as early as 1977 by Magerl. 3 Since then, several studies have been published comparing percutaneous pedicle screw fixation without fusion to conventional open techniques. 4 -7 However, the best candidate for percutaneous pedicle screw fixation without fusion is yet not defined, especially within practical classification systems like TLICS. On the other hand, cases with severely injured anterior columns, those with highly unstable 3-column fractures and those with associated neurological deficits are considered noncandidates for such procedures owing to the lack of anterior reconstruction, fusion, and neurological decompression. The aim of this study was to explore the best TLICS grade in which percutaneous pedicle screw fixation without fusion would provide better management over the conventional techniques.
Patients and Methods
Study Design
This was a retrospective cohort study with a matched historical control group.
Source of Data and Ethical Approval
The study included 2 groups of patients with thoracolumbar fractures; a percutaneous screw fixation (PSF) group, and a conventional group managed in the usual protocol as indicated by their TLICS scores (ie, nonoperative management for TLICS < 4, operative management for TLICS > 4 and either for TLICS = 4). The data was obtained from the medical records of patients admitted to the department of neurosurgery with the diagnosis of thoracolumbar fractures during the period of 8 years between May 2010 and April 2018. The study was approved by our local institutional review board MFM-IRB (MS/16.04.76) and informed written consents were obtained from all patients in conventional and PSF groups.
Criteria of Selection
All consecutive patients with thoracolumbar vertebral body fractures (AO A1-4) presented with no neurological deficits were initially included. According to the TLICS score, the selected fractures had morphological scores 1 or 2 and neurological status scores 0. The status of their posterior osseo-ligamentous complexes was intact, indeterminate, or definitely injured (0, 2, or 3). Patients with severe anterior column injury (with Load Sharing Classification score 8 ≥7), multiple fractured levels and those having American Spinal Injury Association (ASIA) score 9 A to D were excluded. Moreover, patients with osteoporosis, associated neurosurgical/major orthopedic injuries and those with coagulopathy not corrected at the time of surgery were also excluded. Finally, cases with missing data and those who did not complete the self-assessment outcome tool at 1 year (illiterates or lost from follow-up) were omitted from the studied population. According to the selection criteria, final TLCS scores ranged from 3 to 5 in PSF group and from 1 to 5 in the conventional group.
Data Collection
At the end of the selection process, 219 patients (42 in the PFS group and 179 in the conventional group) were provisionally included and data was collected and prepared for the matching process. The authors collected the following data; age, sex, marital status, smoking status, occupation (blue vs white collar), educational stage completed (primary, preparatory, secondary, or college), time to presentation, ASIA, TLICS, and Load Sharing Classification scores, spinal level fractured (thoracic, thoracolumbar junction, or lumbar), type of management, time to surgery since presentation, number of screws inserted and segments fixed, duration of surgery, volume of blood loss, intraoperative complications, screw positions, screw-related complications, postoperative ASIA score, Cobb angle (initial, immediate, 6 and 12 months postoperative), time to ambulation, duration of hospital stay, cosmesis score of surgical wounds, fracture site healing at 3, 6, and 12 months and Oswestry Disability Index (ODI) score at the end of follow-up.
Matching Process
The PSF group was split into 3 TLICS categories (TLICS-3: “12 cases”, TLICS-4: “18 cases” and TLICS-5: “12 cases”). Retaining only conventional cases with similar TLICS scores, the cases were also grouped into 3 TLICS categories for comparison. For PSF cases within each TLICS category, best matches among conventional cases with same TLICS scores were selected. A propensity score–matched analysis was performed in order to create groups balanced on observed covariates. The propensity score (PS) was defined as the probability (0 to 1) of a case to receive PSF based on demographic and clinical characteristics. The matching process produced groups balanced on the PS, thus expected to be balanced on all covariates.
The process of PS-matching passed in the following stages:
Generation of the PS: using the whole sample, a multivariate logistic regression analysis was conducted with “treatment group” (PSF = 1/conventional = 0) as the dependent variable and the various patients’ characteristics (demographic and clinical) as independent variables.
Balancing the data: matching of cases among treatment groups within individual TLICS categories was done using a caliper width of 0.2 of the pooled standard deviation of the logit of the propensity score. 10 Balancing was based on 1:1 or 1:1:1 matching within the pre-specified caliper width depending on the number of treatment groups within each TLICS category; whether 2 or 3, respectively.
Assessing the matching quality: using a 2-sample t test or 1-way analysis of variance (ANOVA) to check for any significant differences in covariate means and ensure balance among the groups. Detection of any significant differences mandated remedial measures to be done in the generation process of PS.
Surgical Methods
Cases in PSF group were operated using Viper 2 MIS spine system provided by DePuy Synthes Spine. Surgery was performed under fluoroscopic guidance after marking pedicle projections over the skin of the back (Figure 1). The process of screw insertion was performed in the standard technique described elsewhere. 11 The vertebra above and that below the fractured vertebra received 2 screws each, in addition to 1 or 2 additional screws in the fractured level (Figure 2). In the conventional group, cases with TLICS score ≤3 were managed nonoperatively, while those with scores ≥5 were managed using an open screw fixation (OSF) method. Patients with TLICS scores 4 were managed either operatively (OSF) or nonoperatively depending on the surgeon’s preference and patient’s general condition. In cases who underwent OSF, screws (EXPEDIUM 5.5 Spine System, DePuy Synthes) were inserted by direct exposure of anatomic landmarks in the traditional way. Similarly, screws were inserted one level above and one level below with unilateral or bilateral screws at the index level. Posterior bony fusion obtained from the iliac crest was performed after decortication of posterior elements in all OSF cases, but no laminectomy in any. Nonoperative cases were managed using controlled pain killers and application of customized rigid thoraco-lumbo-sacral orthosis (TLSO) for individual patients. The orthosis was fitted and evaluated by the physiotherapist to assess the degree of tolerance, pressure areas and to determine the need for any final adjustments before discharge.
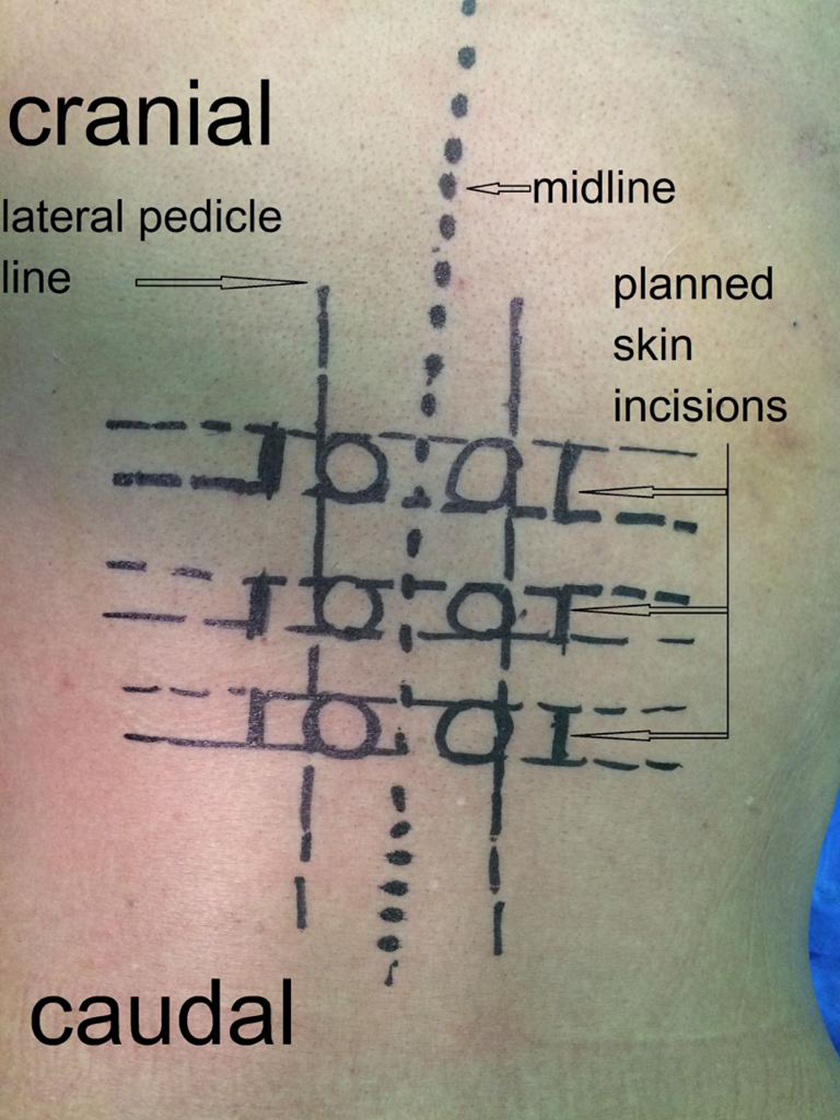
Initial skin markings for pedicles projections and planned skin incisions under fluoroscopic guidance.

The number of screws/case used in percutaneous fixation group. Left: 6 screws/case (2 in the level above, the level below and fractured level), with anteroposterior and lateral fluoroscopic views and sutured skin incisions at end of the procedure. Right: 5 screws/case (2 in the above and below levels and 1 screw in the right pedicle of the fractured vertebra) with fluoroscopic views and skin incisions.
Definitions and Clarifications
Screw Positions
The pedicle screw position referred to the relation of screw borders to medial and lateral walls of the pedicles. It was classified into 3 groups; perfect positioned (screw borders lying totally within the pedicle), laterally malpositioned (with lateral cortical breaches), and medially malpositioned (with medical cortical breaches). Medial malposition was graded according to the distance between the medial edges of the screw and pedicle into 3 zones: “safe” zone (<3 mm), “potentially hazardous” zone (3-6 mm), and “absolutely hazardous” zone (>6 mm; Figure 3).
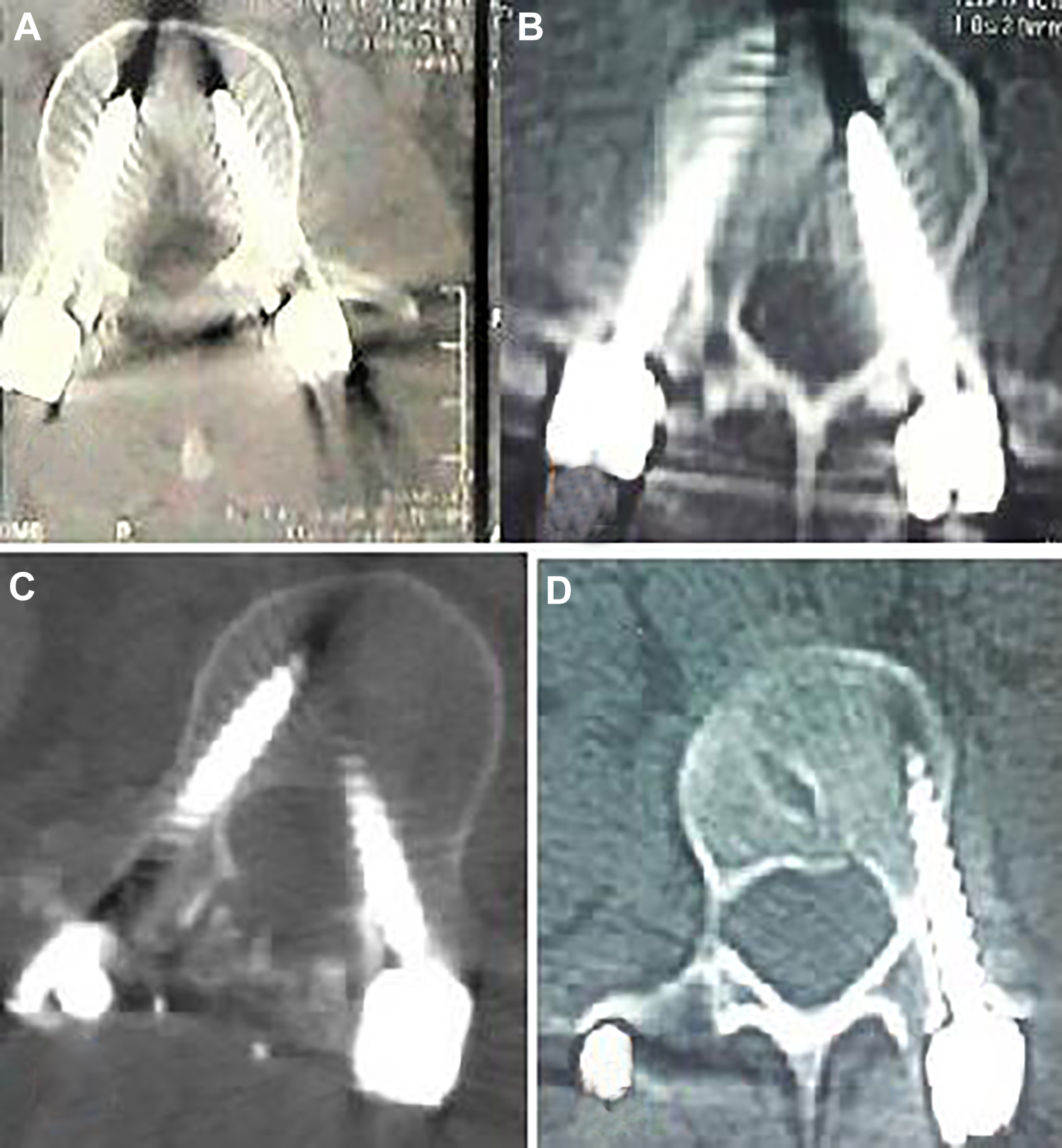
Various screw positions. (A) Perfect position of screws bilaterally. (B) Laterally malpositioned screw (outside pedicle) on the right=side with medially malpositioned screw (safe-zone) on the left side. (C) Perfect position of screw on the right side with medially malpositioned screw (safe-zone) on the left side. (D) Laterally malpositioned screw (outside pedicle) of the left side. None of these cases developed screw-related complications or required screw removal.
Screw-Related Complications
Complications developed by screw insertion. It included pedicle fractures, cerebrospinal fluid leaks, spinal cord or root injuries and vascular or visceral injuries.
Time to Ambulation
The time passed after conducting the definitive management until the moment when a patient can get out of bed and walk around unsupported. All patients were encouraged to mobilize as soon as tolerated after the definitive management was performed. The protocol used in our institute for nonoperative cases was to apply the custom-made rigid brace (which becomes available within 24 hours of ordering it) in a supine position, then asking the patient to turn lateral and prone in bed. If pain was tolerated, a trial to mobilize and walk was performed under the supervision of the senior resident. If pain was intolerable, a retrial of ambulation after 6 to 8 hours was accomplished. A similar protocol of ambulation was followed in operated cases with the first trial of mobilization 8 hours after surgery, retried every 6 to 8 hours till became tolerable by the patient. Patients who became able to stand and walk underwent radiological assessment on the same day. The discharge was decided on the next day of ambulation.
Cobb Angle
Cobb angle was measured between the superior and inferior endplates of the vertebral bodies above and below the injured vertebra, respectively. This selected method of measurement has a significantly higher inter- and intraobserver reliability in measuring thoracolumbar kyphosis. 12 All Cobb angles (initial, early postoperative, and follow-up angles) were assessed by 2 independent raters and mean values were taken.
Oswestry Disability Index
A valid translated version of the ODI 13, 14 was used and self-filled by all patients at the end of follow-up period (12 months).
Cosmesis Score
The visual analogue scale (VAS) was used by both the patient and an independent surgeon to evaluate and rate a high-quality cell phone–captured photo of the wound. The cosmesis score was then calculated as the mean of both VAS scores for each patient.
Fracture Healing
Healing was defined as the absence of the hypodense fracture lines within the fractured vertebra, being replaced by the dense bone formation in axial computed tomography (CT) cuts (Figure 4). Follow-up CT scans were assessed by an independently certified neurosurgeon blinded to study details.
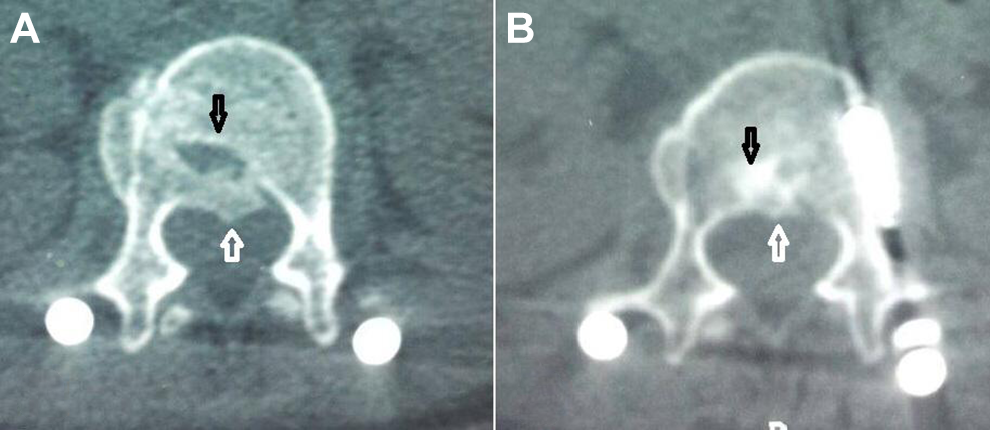
Fracture site healing. (A) The fractured vertebra shows a gapped hypodense fracture line in its body “black arrow” with a retropulsed bone fragment with the spinal canal “white arrow”. (B) Healing at the fracture site as appears in a follow-up computed tomography scan done at 1 year. The fracture line was replaced by dense bone healing “black arrow” with remodeling and desorption of the retropulsed bony fragment “white arrow.”
Statistical Analysis
Descriptive statistics was presented as means and standard deviations (SD) for continuous parametric data, as median and interquartile range (IQR) for continuous nonparametric data and as numbers and proportions for categorical data. The patients were divided into groups based on their TLICS scores and analytic statistics included comparison of treatment modalities in each of the TLICS groups as regard to different outcome variables. Continuous variables were tested for normality using the numerical Shapiro-Wilk test with significance values greater than .05 indicating normality of data. Paired-sample t test and repeated-measures ANOVA were used to compare continuous variables among 2 and 3 treatment groups, respectively. Binomial (categorical) variables were compared using chi-square test unless the expected values in any of the cells of the contingency tables are less than 5; a situation in which Fisher’s exact test was used instead. All statistical procedures were done using the Statistical Package for the Social Sciences (SPSS Statistics) for Microsoft Windows (Version 20.0, 2011; IBM Corp, Armonk, NY, USA). The statistical significance level (alpha) was a P value ≤.05 based on a 2-sided hypothesis test.
Results
This study included 102 patients (40 females and 62 males) whose ages ranged from 19 to 51 years with a mean of 36 ± 9 years. Almost three quarters (74%) of patients were married, 65% were nonsmokers with a majority (57%) of white-collar workers. Nearly half of patients (48%) were college graduates and 10% received primary education only. The time window between trauma and presentation to medical care ranged from 1 to 25 hours with a median of 7 hours and IQR of 5. All patients were ASIA E, with mostly thoracolumbar junctional (T11-L2) fractures (86 cases) and TLICS scores of 3 (24 cases), 4 (54 cases), and 5 (24 cases). The load sharing classification scores were 3 (in 36 cases), 4 (in 41 cases), 5 (in 14 cases), and 6 (in 11 cases). The mean load sharing score was 3.5 in TLICS-3 group, 3.7 in TLICS-4 group, and 5.6 in TLICS-5.
Thirty patients (29.4%) were treated nonoperatively, 42 patients (41.2%) underwent PSF and 30 patients (29.4%) received OSF. Cases treated surgically were operated 11 to 22 hours following presentation with a mean of 16 ± 3 hours with no significant difference in timing of surgery among PSF and OSF procedures (p = 0.612). The duration of surgical procedures ranged from 95 to 180 minutes with a mean of 138 ± 25 minutes. The duration of percutaneous procedures had a mean duration of 123 ± 24 minutes; while that of open procedures was 156 ± 12 minutes, which was found to be a statistically significant difference (paired t test, P < .001). A strong negative statistically significant correlation was noticed between the serial order of the percutaneous procedures and their durations (Pearson correlation, r = −0.809, P < .001), while such correlation was found to be a weak negative none significant one in the open conventional group (Pearson correlation, r = −0.191, P = .448).
The total number of screws used in surgical procedures was 397 screws; 230 in PSF (5 screws/case in 22 cases and 6 screws/case in 20 cases) and 167 in OSF (5 screws/case in 13 cases and 6 screws/case in 17 cases). These figures represented comparable numbers of screws/case (Wilcoxon test, P = .673). In all cases (PSF and OSF), only 2 motion segments were fixed (one level above and below with 1 or 2 screws at index level). The number of malpositioned screws were 20/230 in PSF (1 screw in 8 cases and 2 screws in 6 cases) and 7/167 in OSF (1 screw in 5 cases and 2 screws in 2 cases), which represented an insignificant difference between the 2 groups (Wilcoxon test, P = .215). There were 14 medially malpositioned screws within the “safe” zone (12/PSF and 2/OSF) and 13 laterally malpositioned screws (8/PSF and 5/OSF). However, none of the cases with malpositioned screws developed screw-related complications or required screw removal.
The volume of intraoperative blood loss was 142 ± 37 mL in a percutaneous group and 330 ± 97 mL in the conventional group with a significant statistical difference in favor of percutaneous fixation (paired t test, P < .001). Eleven intraoperative complications in the form of unilateral pedicle fractures at the index level were reported, in which a single index screw was inserted on the intact side and all cases experienced uneventful postoperative hospital stay. Other cases with a single screw at the index level were planned preoperatively due to detected pedicle injuries before surgery. All cases were ASIA grade E at discharge and during the follow-up period. Comparing the cosmesis scores between the 2 surgical groups revealed significantly better scores among the PSF (Wilcoxon test, P = .023).
The population set included 3 TLICS-score categories, each composed of matched treatment groups for comparison. The TLICS-3 category received either nonoperative management or PSF (12 cases each). In TLICS-4 group, patients were treated either nonoperatively, by PSF or by OSF techniques (18 cases each). However, all patients in the TLICS-5 group were treated surgically by either PSF or OSF (12 cases each). There were no statistical differences between treatment groups within each TLICS category regarding various demographic and clinical variables as groups were sufficiently matched.
In TLICS-3 patients, the time to ambulation, as well as, the overall hospital stay was significantly shorter in nonoperatively managed cases compared to cases that underwent PSF procedures (within 8 hours following brace application). At admission, Cobb angles were comparable in both groups; however, the predischarge angles and angles at the end of follow-up were significantly better in PSF group with no significant loss of correction over follow-up period in both groups. On the other hand, despite the better correction provided by PSF, no significant differences were detected between the 2 treatment groups regarding ODI scores and healing rates at final follow-up (12 months; (Table 1).
Comparison Between Treatment Groups in TLICS-3 Category.a
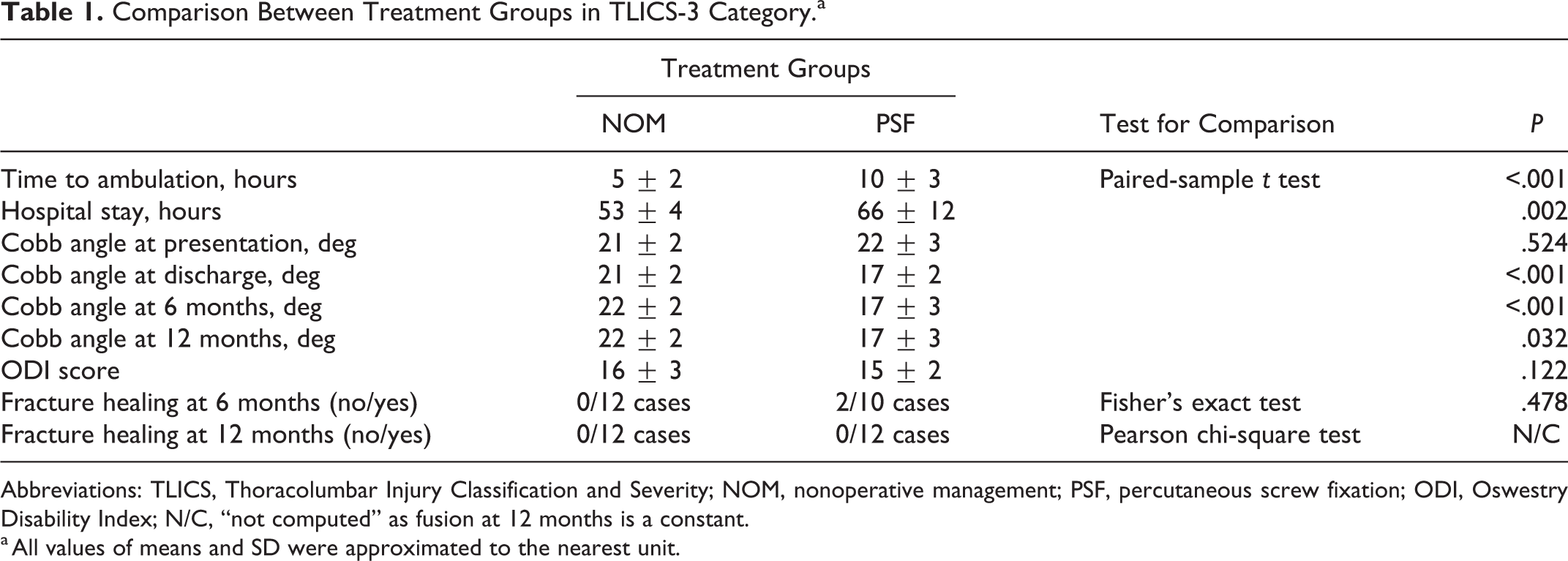
Abbreviations: TLICS, Thoracolumbar Injury Classification and Severity; NOM, nonoperative management; PSF, percutaneous screw fixation; ODI, Oswestry Disability Index; N/C, “not computed” as fusion at 12 months is a constant.
a All values of means and SD were approximated to the nearest unit.
When the same variables were compared among the 3 treatment modalities used in TLICS-4 group, repeated-measures ANOVA revealed a significant difference between groups in regard to the time to ambulation, duration of hospital stay and Cobb angles at discharge and final follow up but not at presentation (Table 2). Bonferroni post hoc correction revealed a significantly longer time to ambulation in OSF group compared with the other 2 groups (P < .001) with comparable values between nonoperative and PSF groups (P = .983). However, hospital stay was marginally shorter in the nonoperative cases than PSF group (P = .080) whose hospital stay was significantly shorter than OSF group (P = .002). The post hoc test also revealed that Cobb angles of the traumatic kyphosis at final follow-up were significantly bigger in nonoperative cases compared with either percutaneous or open cases (P = .006 and P = .004, respectively), but did not differ significantly between the 2 surgical groups (P = .996). At the end of follow-up (12 months), the repeated-measures ANOVA with post hoc test revealed that ODI scores were significantly higher in nonoperative cases compared with PSF (P = .007) and OSF (P = .002) groups), but comparable between the 2 operative groups. Healing rates did not differ significantly among the 3 treatment groups (Table 2).
Comparison Between Treatment Groups in TLICS-4 Category.
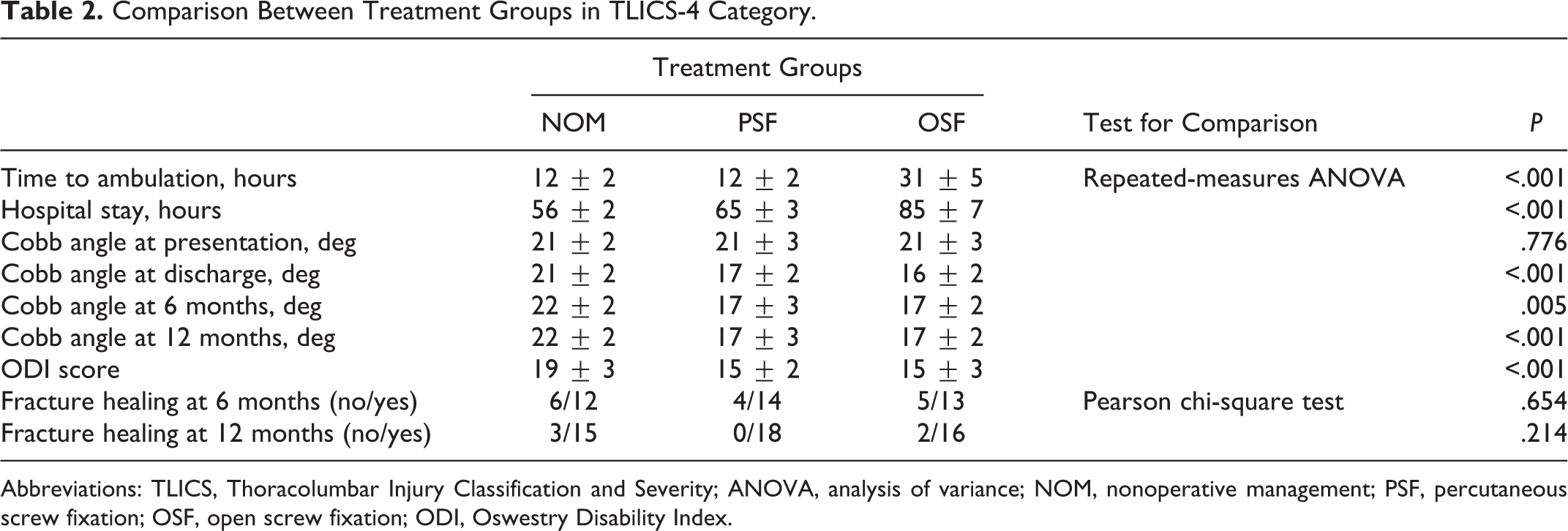
Abbreviations: TLICS, Thoracolumbar Injury Classification and Severity; ANOVA, analysis of variance; NOM, nonoperative management; PSF, percutaneous screw fixation; OSF, open screw fixation; ODI, Oswestry Disability Index.
Although PSF group was associated with a significantly shorter time to ambulation and overall hospital stay compared to the OSF group among TLICS-5 patients, there was a significant difference in favor of open fixation as regard its initial corrective power and loss of correction at final follow up. Despite the marginally higher healing rates of OSF at 12 months (P = .069), this statistical tendency was considered to be clinically significant (50% healing in PSF vs 92% healing in OSF). PSF group was associated with significantly higher final ODI scores indicating lower functional recovery (Table 3).
Comparing Treatment Groups in TLICS-5 Category.
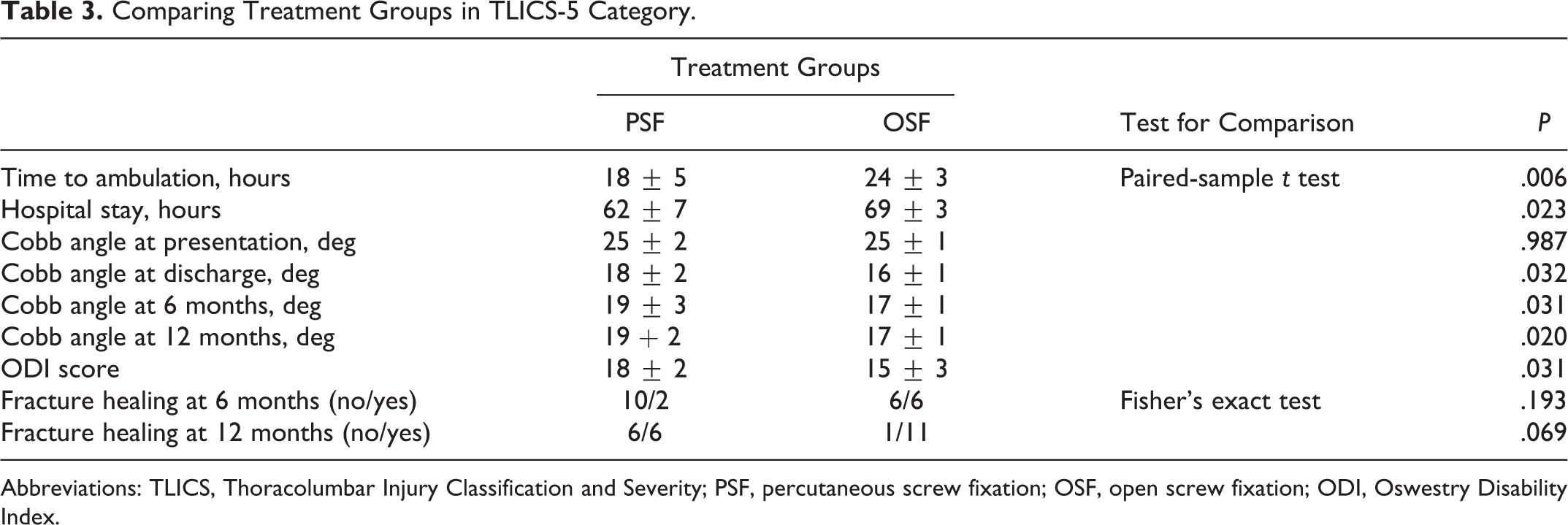
Abbreviations: TLICS, Thoracolumbar Injury Classification and Severity; PSF, percutaneous screw fixation; OSF, open screw fixation; ODI, Oswestry Disability Index.
Discussion
The TLICS score is a relatively recent, reliable, widely used classification system and a safe decision-making tool in thoracolumbar fractures. 15 However, some injuries treated conservatively according to the TLICS score especially burst fractures in neurologically intact patients may require a delayed surgical intervention for correction of local kyphosis and/or persistent pain. 16 -18 Such injuries may be referred to as “delayed unstable” fractures, 19 in which the injured spines may support some physiological load but are at risk of progressive deformity and pain worsening. These types of injury may not be severe enough to indicate an aggressive open fixation and not safe enough to be treated nonsurgically; making them suitable candidates for minimally invasive fixation techniques, like PSF, which is seen by some authors as an intermediate method between the traditional open surgery and conservative treatment. 20,21
The PSF technique proved to be time preserving, less bloody, and associated with shorter time to ambulation after surgery compared with the conventional open technique. These results are consistent with previous studies. 22 -24 The faster postoperative ambulation can be explained by the less tissue damage minimizing the postoperative inflammatory response and pain in the early postoperative period. Previous studies reported significantly lower pain levels in the first postoperative week in patients undergoing percutaneous fixation. 25, 26 The strong negative correlation noticed between the serial order of the percutaneous procedures and their operative duration indicates that the successive procedures are getting significantly shorter and less time-consuming. The frequency of malpositioned screws in the percutaneous group was found comparable to the open group, the majority happening within early-operated patients with no related complications. These findings suggest a steep learning curve of the technique which is consistent with the results of previous research studying the technique. 27 Not surprisingly, the percutaneous technique was found much more cosmetic when compared to the conventional method as previously reported by others. 24
In the TLICS-3 category, the nonoperatively managed cases were mobilized earlier with a trend toward shorter hospital stay compared to those who underwent PSF. In addition, the lack of costs of using implants and operation theatre makes nonoperative management a highly economic choice in this category of patients. It was reported that faster mobilization, shorter rehabilitation, and earlier job return reduce the overall 1-year cost. 28 Although final Cobb angles were smaller with PSF than in nonoperative management, initial Cobb angles showed no progression at final follow up in nonoperatively managed cases. On the final follow up, nonoperative management was found to be equally effective to the PSF in terms of healing rates and ODI scores. None of the nonoperatively treated TLICS-3 patients required a delayed surgical intervention in our study in contrary to some authors who reported delayed surgical intervention for patients with TLICS scores less than 4 who were initially treated conservatively. 18,29,30 Such cases ranged from 5% 18 to as many as 26.4% of cases 30 who suffered from persistent pain and/or kyphosis interfering with normal mobilization. The absence of such cases in our study may be due to the lower load sharing scores (mean 3.5 points) in this group of patients. Higher load sharing scores among patients with TLICS scores less than 4 were associated with increased failure of conservative treatment requiring delayed surgical procedure. 30
In the TLICS-4 category, the percutaneous technique was superior to both nonoperative and OSF groups. It showed significant earlier ambulation and shorter hospital stays compared with the OSF method. In addition to shorter operative time, less blood loss and better cosmesis, earlier mobilization and hospital leave—with potential overall cost reduction 28 —in PSF make it a preferable modality of management over OSF. Moreover, the percutaneous technique proved to be of similar corrective power as the OSF technique. The kyphosis correction power of PSF is reported by several authors to be as effective as conventional techniques. 7,20,31 A combination of lordosis and distraction was found effective in providing indirect reduction forces that help spinal realignment during percutaneous techniques. 31,32 Although the healing rates were comparable among the 3 groups, more disability (higher ODI scores) was reported among nonoperative cases as compared with the other 2 groups. This may be explained by the noncorrected healing of fractures among nonoperative cases likely resulting in a kyphosis that may impair sagittal balance and requires overacting trunk and pelvic muscles.
On the other hand, we did not detect the same superior performance of the percutaneous technique in the TLICS-5 category of patients. Although the PSF group showed faster ambulation and shorter overall hospital stay, it did not achieve comparable initial or final corrective power as compared with the OSF technique. The mean preoperative Cobb angle across the fracture sites did not differ significantly among the 2 groups but was significantly lower at discharge at the final follow-up visit in the OSF group. This may be explained by the more severe trauma, more fragmentation, more vertebral collapse and higher kyphosis associated with TLICS-5 fractures in this study. This may demand more dissection, wide exposure, and soft tissue release as performed during open techniques to achieve a better degree of correction. In our study, TLICS-5 group was associated with higher grades of load sharing classification score compared with TLICS-3 and TLICS-4 groups (5.6 vs 3.5 and 3.7, respectively), indicating more bony destruction with potential fragmentation and/or deviation at the fracture site. The use of isolated percutaneous fixation in fractures with significant deviation is controversial and it should be preferentially used in the slightly deviated fractures. 33 According to Court and Vincent 34 in their review article, percutaneous fixation without grafting seems suitable for minimally displaced fractures with intact tension band (Magerl A1, A2, and A3.1) with the exception of Magerl B2 fractures (moderate anterior compression with the posterior distraction of bony structures) which are considered an excellent candidate. For other fractures, they recommended the addition of a bone graft through anterior approach or the use of combination techniques. In an algorithm proposed by Dhall et al, 35 the authors recommend that patients with TLICS scores >4 undergo instrumented fixation with a bony fusion via either a conventional open or mini-open approach. Although this algorithm was based on the review of relevant literature, it is supported by our findings of lower functional recovery (higher ODI scores) and the statistical trend (that reached a clinical significance) toward lower healing rates at final follow-up in TLICS-5 fractures managed with isolated percutaneous fixation.
The aim of this study is the demonstration of best candidates for percutaneous fixation among thoracolumbar fractures based on the TLICS score; however, it carries 2 main limitations. First; being retrospective and observational in nature with no randomization of recruited patients made it prone to selection biases. We tried to minimize the potential selection biases by the creation of propensity score–matched treatment groups within each TLICS category that were balanced on all covariates. A second limitation is that the sample size in each of the compared groups was relatively small. We used the available sample of PSF performed over the period of 8 years and selected best matches (in 1:1 ratio) among the much bigger group of patients managed by conventional ways during the same period. These limitations indicate the careful interpretation of current findings and further conduction of future, prospective, larger, observational, or randomized controlled trials comparing the utilized treatment modalities within each TLICS category before generalization of results.
In conclusion, the percutaneous fixation techniques proved to be a safe, effective, and time-preserving technique with less blood loss, faster recovery, and more cosmesis than open techniques. When performed in well-selected patients, its clinical and radiological outcomes are comparable to conventional techniques with better early postoperative recovery. Our results suggest that isolated percutaneous fixation may be a good choice in the management of TLICS-4 thoracolumbar fractures due to faster recovery, better cosmesis with potentially lower overall costs as compared with OSF; in addition to being a better corrective tool with a lower disability as compared with nonoperative management. However, in view of its comparable results to non-operative treatment in TLICS-3 fractures and its marginally inferior results to OSF in TLICS-5 fractures, its isolated use in the management of these fractures could not be supported by current results. This raises the need for future, larger, prospective studies to re-assess these objectives and replicate current findings before generalization.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.