
Abstract

Introduction
Occasionally, we are asked why patients undergoing a surgical procedure cannot act as their own controls in a clinical study. After all, prior to their procedure they exhibit a certain level of pain and disability, and after the procedure there is a change; often they have less pain and less disability. Is this not the result of the procedure? The short answer to the question whether the change is due to the procedure is simply, “maybe, maybe not.” While it is true that the change occurred when the surgical procedure was given, the change is not necessarily the effect of the surgical procedure itself. How can this be? The answer is that the treatment response is about more than the surgical procedure. It is about the cultural meaning of treatment: the way the surgery is proposed by the surgeon, the ceremony around the procedure, and the expectations of the surgeon and patient. These all have an impact on outcome. Does this seem improbable to you? Welcome to the strange world of the placebo response.
It is difficult to identify exactly when placebo (Latin, “I shall please”) first entered into medical practice. In 1785, A New Medical Dictionary described placebo as “a commonplace method or medicine.”
1
Thomas Jefferson, in his letter to Dr Caspar Wistar in 1807, wrote, “One of the most successful physicians I have ever known, has assured me, that he used more bread pills, drops of colored water, powders of hickory ashes, than of all other medicines put together.”
2
A few years prior, a British physician, John Haygarth, reported using a placebo treatment in a small crossover study of 5 patients. He compared expensive metal rods (Perkins tractors) intended to draw out disease, to wooden lookalike tractors. Four of 5 patients with “rheumatism” reported improved pain with either rod.
3
Drug studies administering placebos to patients with angina followed in the early 20th century and found no benefit of various drugs compared to placebo.
4,5
At about the same time, a placebo controlled study tested the popular idea from earlier observations that vaccines were successful in preventing the common cold. The study reported no difference between the effectiveness of placebo and vaccine, concluding, One of the most significant aspects of this study is the great reduction in the number of colds which the members of the control groups reported during the experimental period. In fact these results were as good as many of those reported in uncontrolled studies which recommended the use of cold vaccines.
6(p1172)
Placebo Response Versus Placebo Effect
Over time, we have come to recognize that there is not one response to a placebo but many. 7 We refer to the sum total of patients’ responses to the administration of the placebo as the placebo response. This includes some proportion of the response that likely would have occurred in the absence of any treatment such as the natural history of a disease, regression to the mean, and response bias. Natural history denotes the change, up and down, of the symptoms over time. Regression to the mean refers to a statistical principle that if a variable is extreme on its first measurement, it will tend to be closer to the average on its second measurement, and vice versa. Response bias is the tendency for study participants to provide answers they believe investigators want to hear. The placebo effect is the proportion of improvement or worsening that remains after controlling for all the other incidental effects (Figure 1). 8
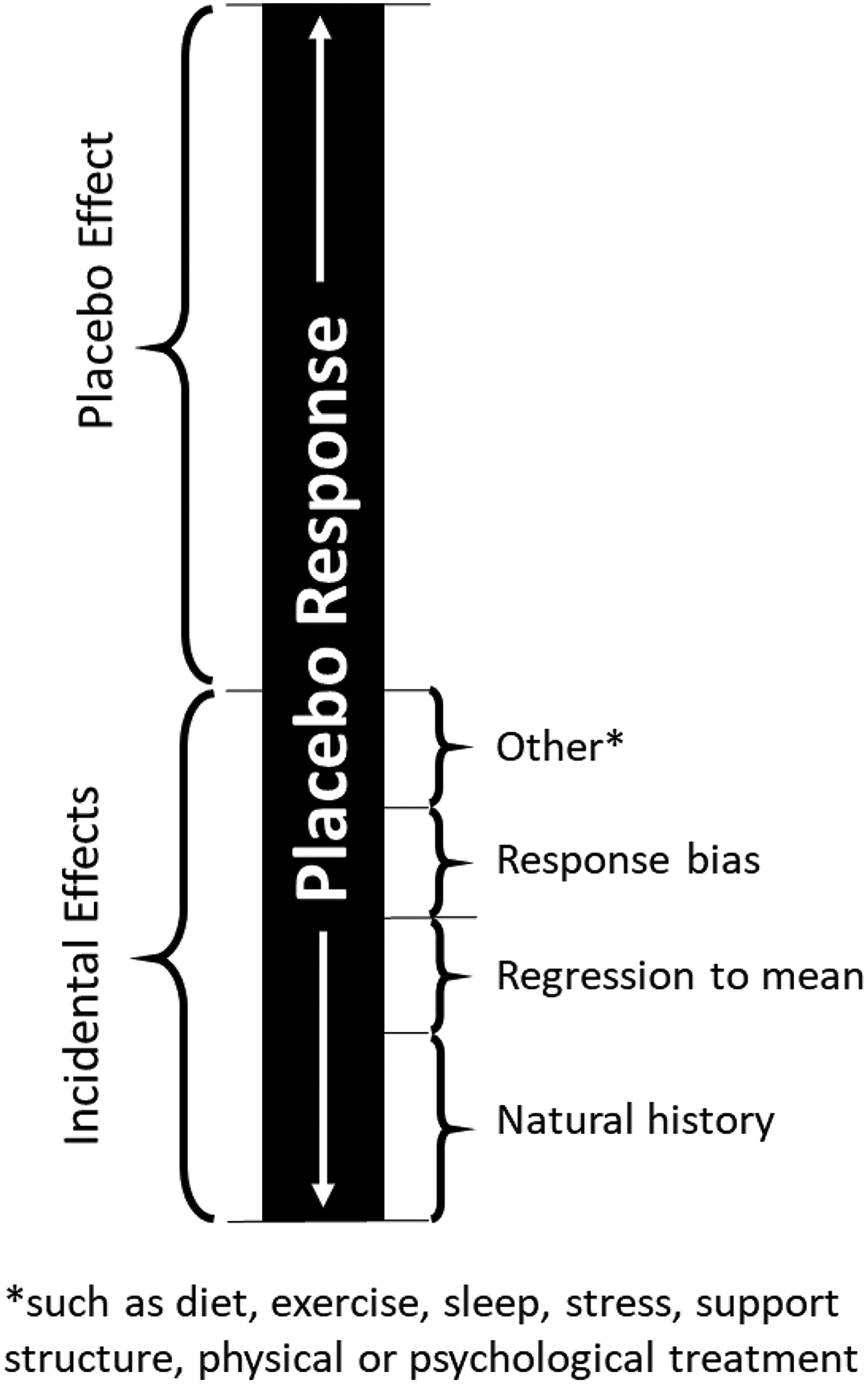
Placebo response.
Improbable Responses of Placebos
Below is a sample of some bizarre results from placebo administration.
Four sugar pills are more effective than 2 pills. One study reported that a placebo allotted 4 times/day resulted in greater duodenal ulcer healing compared with placebo administered 2 times/day.
9
The route of placebo administration is important. In the case of migraine pain, placebo injection of saline was more effective than oral placebo in relieving migraine pain
10
and in reducing hypertension.
11
Factors contributing to the placebo response can be combined. In patients with irritable bowel syndrome, placebo acupuncture alone resulted in greater symptom improvement than waitlist controls; and placebo acupuncture augmented by practitioner warmth, attention, and confidence resulted in the greatest symptom improvement of all.
12
How the placebo is presented affects results. Flashy brand name packaging, for example, enhanced the effect of aspirin and placebo sugar pills compared with bland, neutral boxes in women with headaches.
13
Placebo (sham) surgery is effective in a host of conditions. It has been shown to reduce pain and disability in trials of vertebroplasty.
14,15
Furthermore, sham surgery was effective in treating knee osteoarthritis
16
and degenerative meniscus tears
17
as well as pain conditions, obesity, reflux disease, endoscopic procedures, and percutaneous procedures.
18
Finally, sham surgery has been shown to reduce symptoms in Parkinson’s disease in part due to its effect on the release of dopamine.
19
People’s expectations moderate health benefits. In one study a group of female room attendants were told that the work they do (cleaning hotel rooms) is good exercise and satisfies the Surgeon General’s recommendations for an active lifestyle. Subjects in the control group were not given this information. Though behavior did not change, 4 weeks after the intervention, the informed group perceived themselves to be getting significantly more exercise than before. And, compared with the control group, they showed a decrease in weight, blood pressure, body fat, waist-to-hip ratio, and body mass index.
20
Another example of the power of patient expectation is a study comparing the effectiveness of analgesic drugs administered by a computer-controlled infusion pump without the patient’s knowledge versus open administration of the drug by a clinician and described to the patient as a pain-relieving intervention. The effects of the blinded administration via the infusion pump was markedly reduced compared with open administration by the clinician.
21
Clinicians’ expectations also influence the placebo response. In an elegant study of clinician expectation, 3 different agents were given to patients having wisdom teeth extraction: saline injection, fentanyl, or naloxone. Patients were split into 2 groups. In the first group, the clinicians giving the treatment, though blinded to the treatment, were told rightly that they would be giving 1 of the 3 treatments. In the second group, the clinicians were deceived and told that they would only be giving placebo or naloxone when in reality they also were administering 1 of the 3 treatments. The clinicians believed that no one in the second group would receive the pain-relieving fentanyl. Even though a similar proportion of patients in each group received fentanyl, the first group experienced significantly less pain.
22
Contribution of Effects Following Surgical Intervention
When evaluating a surgical procedure in a clinical trial, 3 different choices for a control group exist: no intervention, active agent (eg, nonsurgical control or another surgical method), or a placebo control. The selection of the control group helps investigators identify the magnitude of effect that is additive from the various aspects contributing to the overall effect (Figure 2). Comparison of surgery versus no intervention allows inferences about the efficacy of the surgical procedure ruling out contributions from the natural history. Comparison of surgery to another treatment (surgical or nonsurgical intervention) allows interferences of the added effect of the treatment of interest, its equivalence, and even its comparative safety. Adding a placebo group enables investigators to distinguish the true effect of a surgical procedure itself from the natural history and the other components of the placebo response.

Conceptual contribution of effects following a surgical intervention.
Summary
A treatment response is about more than the surgical procedure. It is about the cultural meaning of treatment; the way the surgery is proposed by the surgeon, the ceremony around the procedure, and the expectations of the surgeon and patient. These all have an impact on outcome. The placebo response is the total response to the administration of a placebo. This includes any response as a result of the natural history of a disease, regression to the mean, and response bias. The placebo effect is the proportion of improvement or worsening that remains after controlling for all the other incidental effects. Choosing a certain control group in a clinical trial helps investigators identify the source of the effect of a surgical procedure. Whether the use of placebo surgery is ethical in clinical trial research is a subject of great debate, and beyond the scope of this article. However, clinical researchers need to think carefully about inferences drawn from trials that have no placebo intervention. The placebo response magnifies the importance of a comparison group in any study designed to evaluate the effectiveness or efficacy of a specific treatment. The results of a single-arm study (ie, case series) should rarely ever be reported as supporting the effectiveness of a specific surgical intervention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Analytic support for this work was provided by Spectrum Research, Inc. with funding from AOSpine.