
Abstract
Study Design:
Retrospective observational study.
Objective:
There is marked variation in the management of nonoperative thoracolumbar (TL) compression and burst fractures. This was a quality improvement study designed to establish a standardized care pathway for TL fractures treated with bracing, and to then evaluate differences in radiographs, length of stay (LOS), and cost before and after the pathway.
Methods:
A standardized pathway was established for management of nonoperative TL burst and compression fractures (AOSpine classification type A1-A4 fractures). Bracing, radiographs, costs, complications, and LOS before and after pathway adoption were analyzed. Differences between the neurosurgery and orthopedic spine services were compared.
Results:
Between 2012 and 2015, 406 nonoperative burst and compression TL fractures were identified. A total of 183 (45.1%) were braced, 60.6% with a custom-made thoracolumbosacral orthosis (TLSO) and 39.4% with an off-the-shelf TLSO. The number of radiographs significantly reduced after initiation of the pathway (3.23 vs 2.63, P = .010). A total of 98.6% of braces were custom-made before the pathway; 69.6% were off-the-shelf after the pathway. The total cost for braced patients after pathway adoption decreased from $10 462.36 to $8928.58 (P = .078). Brace-associated costs were significantly less for off-the-shelf TSLO versus custom TLSO ($1352.41 vs $3719.53, respectively, P < .001). The mean LOS and complication rate did not change significantly following pathway adoption. The orthopedic spine service braced less frequently than the neurosurgery service (40.7% vs 52.2%, P = .023).
Conclusions:
Standardized care pathways can reduce cost and radiation exposure without increasing complication rates in nonoperative management of thoracolumbar compression and burst fractures.
Introduction
Many types of thoracolumbar (TL) compression and burst-type fractures are treated nonoperatively. 1,2 However, there is no universally accepted nonoperative approach to treating these fractures. 3 Nonoperative management of TL fractures focuses on early mobilization to reduce hospital length-of-stay (LOS), decrease the risk of complications related to prolonged bed rest, and lower the overall cost of treatment. 4 Care pathways have been used in other disciplines to accomplish similar goals. 5,6
Recent studies have suggested there is no significant benefit to using custom made (CM) thoracolumbosacral orthoses (TLSOs) to reduce pain-related disability, kyphosis, or LOS in patients with TL fractures that are being treated nonoperatively. 7,8 The direct and indirect costs associated with CM-TLSOs include the price of the orthotic and potential increase in LOS related to the fabrication time for the device. 9,10 Furthermore, there have been several articles showing negligible benefit from CM-TLSO use in patients with TL fractures. 8,11 -14 A literature review by Karimi argued that the use of orthotics can reduce pain but did not prevent local kyphosis. 13 The majority of current literature focuses on the low utility of CM-TLSOs, which are more expensive and take longer to fit than an off-the-shelf (OS) TLSO. Shamji et al found that LOS in a CM-TLSO treated group was 6.3 days, compared to 2.8 days in a non-TLSO treatment group. 10 In addition, Melchiorre found that the median time to obtain a CM-TLSO was 2 days, with a subsequent 3.5 days to ambulation, resulting in an average 5-day LOS in 27 patients. 15 We are unaware of a study comparing the costs and LOS in patients treated with a CM-TLSO versus an OS-TLSO.
A multidisciplinary group charged with evaluating trauma protocols at our institution identified marked variation in managing TL fractures deemed nonoperative by the attending spine surgeon. This resulted in the creation of a new care pathway for these nonoperative TL fractures focused on reducing the variation in bracing, radiography, and time to mobilization. The goals of this study were to evaluate the effect of the new care pathway on the rate and type of bracing, the number of inpatient radiographs obtained following fracture diagnosis, inpatient costs, LOS, and in hospital complication rates. We also compared these factors between the orthopedic spine service and the neurosurgery service. Again, the aim of this study was to evaluate the process of bracing and the different aspects of care involved with this. The indications for bracing as well as the outcomes between the different groups were not in the scope of this study.
Methods
Creation of Care Pathway
After gaining approval by the institutional review board, a multidisciplinary team including physicians and nurses from the sections of trauma surgery, orthopedic spine surgery, and neurosurgery created a standardized algorithm (care pathway) for the treatment of nonoperative TL fractures. This included 6 physicians (3 orthopedic spine surgeons, 1 neurosurgeon, 2 trauma surgeons, and 2 nurses from the section of trauma surgery). This encouraged the use of either no bracing or OS-TLSO, rather than the use of CM-TLSO (though the ultimate choice of bracing remained up to the spine service managing the patient). In addition, use of serial radiographs (ie, films obtained at 30°, 60°, and 90°) was discouraged unless the provider classified the fracture as potentially unstable. The pathway suggested one set of AP and lateral post-mobilization upright radiographs. Once the fracture was classified as stable by the spine service, mobilization with physical therapy commenced. Use of the pathway was encouraged by formal teaching sessions for the trauma, neurosurgery, and orthopedic residents. The pathway was embedded in the ordering system of the electronic medical record. The pathway was adopted into clinical practice in June 2013.
Patient Population
All patients with TL fractures evaluated by the trauma service at Dartmouth-Hitchcock Medical Center from January 2012 through December 2015 were identified using the hospital’s Trauma Registry, which captures all trauma patients presenting to the hospital through the emergency department. Each patient’s electronic medical record was reviewed, and patients who were treated with spine surgery within 7 days of admission were excluded. The decision to proceed with nonoperative care was determined by the attending spine surgeon, and no strict protocol was used to determine fracture stability. Any patient with a TL fracture classified as compression or burst type by the covering spine service was then included in the study. This included all compression and burst subtypes as defined by the AOSpine type A1, A2, A3, and A4 classifications. Any patient with a LOS greater than 2 standard deviations above the mean was excluded from analysis as the prolonged LOS was most likely unrelated to their spinal injury. The scope of this study was to evaluate only patients that had been braced. Therefore, the determinants and/or indications for bracing are not included in this study.
Data Collection
We performed a retrospective review of the medical records to collect the following variables: patient demographic characteristics, LOS, injury severity score (ISS), consulting spine service (ie, orthopedic spine surgery or neurosurgery), number and type of imaging studies, brace use, type of brace ordered, and fracture pattern classification (compression or burst subtypes) as documented in the electronic medical record by the spine team. Complications, which were captured within the Trauma Registry, were defined as one of the following: urinary tract infection, sepsis, pneumonia, decubitus ulcers, bleeding, coagulopathy, compartment syndrome, deep venous thrombosis, pulmonary embolism, cerebrovascular accident, acute kidney injury, cardiac arrest, myocardial infarction, conversion to surgical treatment, and acute respiratory distress syndrome. 16 Cost data was provided by the analytics institute at Dartmouth-Hitchcock Medical Center and included brace cost, bracing consult fee, which included sizing and fitting of brace, imaging costs, and the per day cost for a bed on a surgical floor. This information was used to calculate the direct cost of the brace (brace cost + bracing consult fee if applicable) and the overall inpatient cost of treating the spine fracture (bracing costs + spine imaging costs + daily hospital rate multiplied by days admitted).
Data Analysis
The primary analysis compared the rate of bracing, type of bracing, inpatient costs, and LOS from prior to the initiation of the care pathway to after the initiation of the care pathway. Secondary analyses compared these outcomes between the orthopedic spine service and the neurosurgery service. Statistical analyses were performed using SPSS (IBM Corp, Released 2015, IBM SPSS Statistics for Windows, Version 24.0, Armonk, NY). Unpaired Student’s t tests were used to calculate the significance of the differences between 2 means. To report statistical significance for proportion data, we used the z-ratio calculation for 2 independent proportions. All statistical analyses were considered significant at a P value <.05. No power analysis was performed as this was a pragmatic, observational study.
Results
A total of 1017 patients were identified through the Dartmouth Hitchcock Trauma Registry as having experienced a thoracolumbar fracture between January 2012 and December 2015 (Figure 1). One hundred and seven (10.5%) patients underwent surgical treatment of their TL fracture and were excluded. An additional 29 were excluded due to a LOS greater than 32 days, which represented greater than 2 standard deviations above the mean, as the extended LOS at this point was likely unrelated to the fracture. Additionally, we included only patients with a surgeon-defined burst or compression fracture (n = 406). The average age of the sample was 54 years, 57.9% patients were male, and the mean injury severity score was 12.89 (Table 1). The attending surgeon classified 33% of fractures as burst fractures and 67% as compression fractures. There were no significant differences in patient or fracture characteristics between the pre-pathway and post-pathway cohorts other than a slightly higher proportion of burst fractures in the post-pathway cohort (37.2% vs 27.9% P = .046).
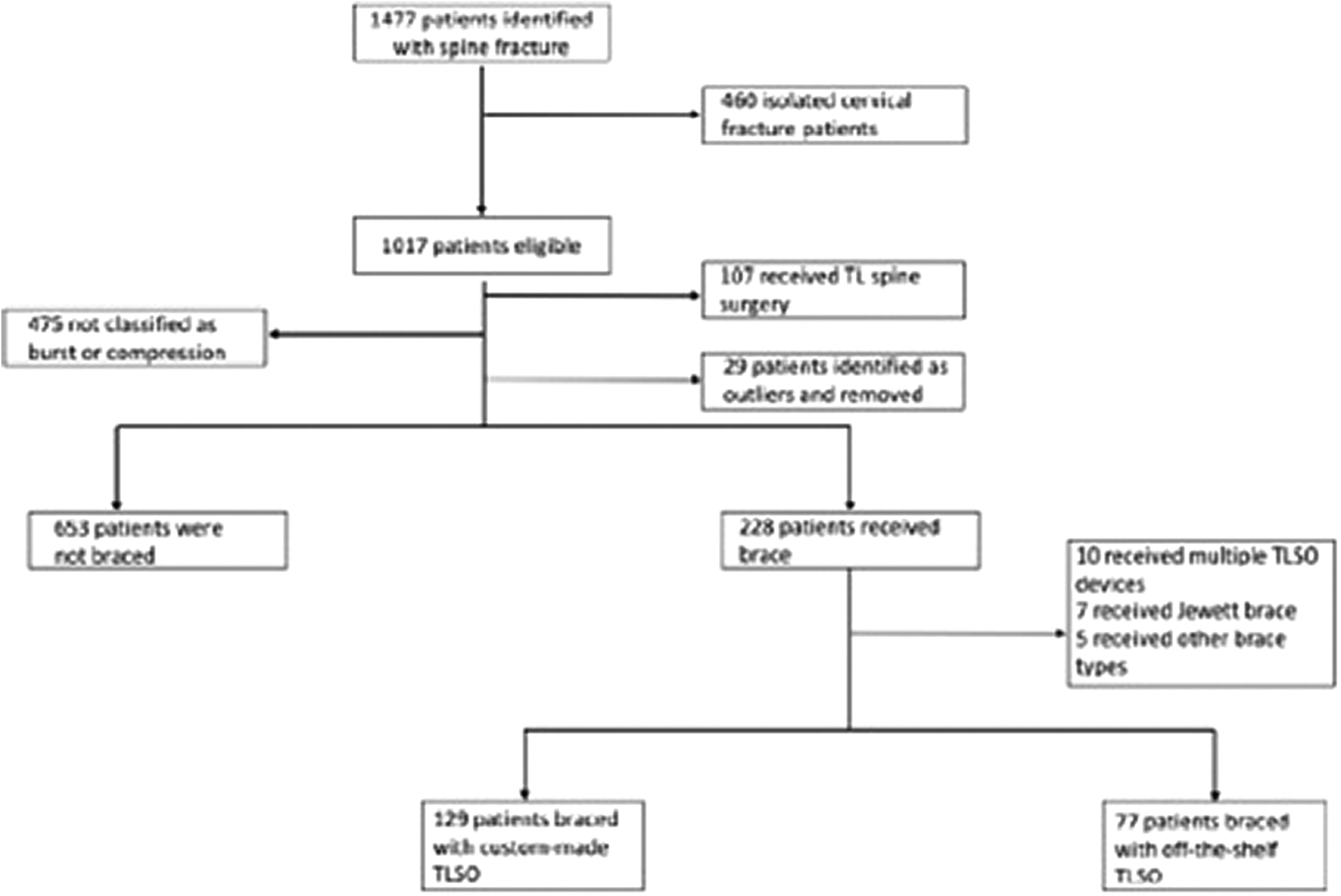
Flow chart of patients included in analysis.
Patient Demographics and Characteristics.
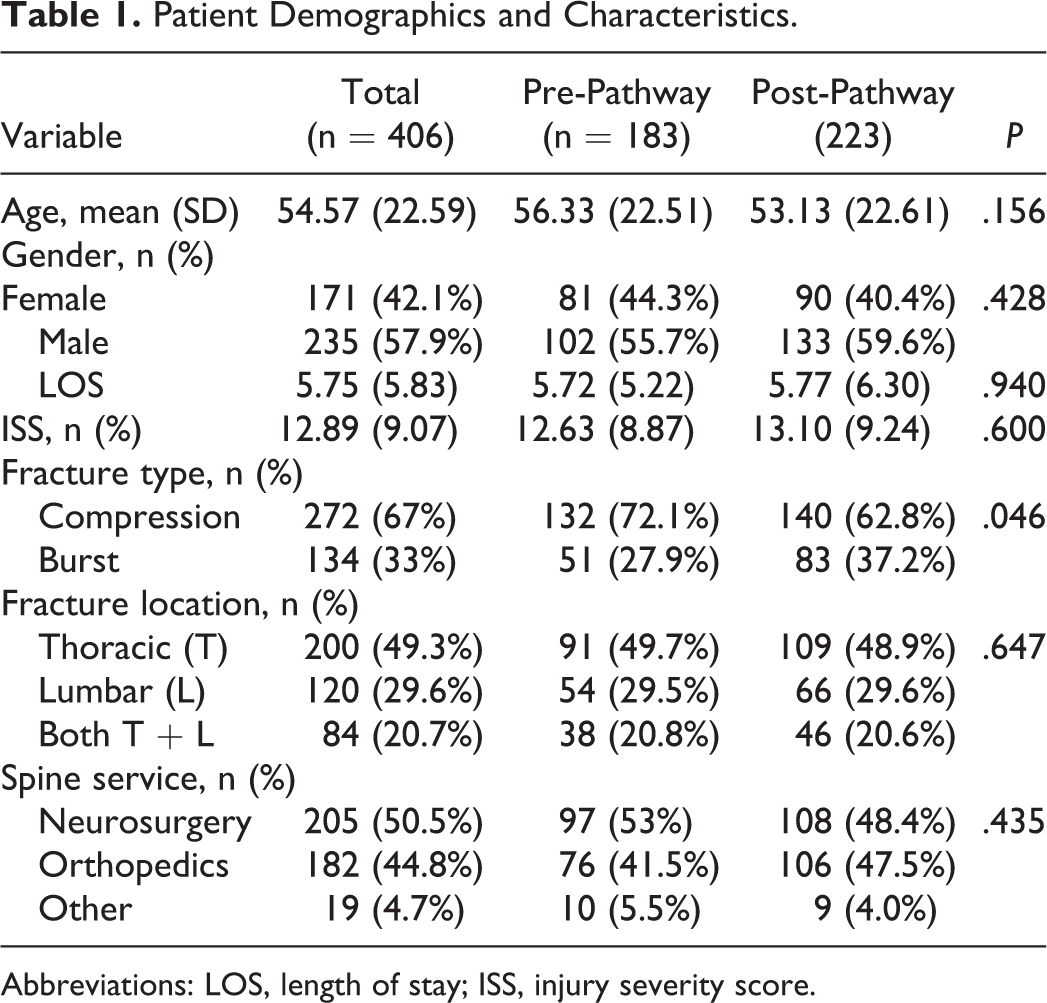
Abbreviations: LOS, length of stay; ISS, injury severity score.
Overall, 45.1% of patients were braced (Table 2). The bracing rate following pathway adoption was similar to the pre-pathway rate (46.6% vs 43.2% P = .485). Before adoption of the pathway, 98.6% of all braced patients received a CM-TLSO. After pathway adoption, the majority (69.6%) of braced patients received an OS-TLSO. The number of post-diagnosis spine radiographs decreased significantly after initiation of the pathway (2.63 vs 3.23, P = .010). The mean LOS did not change significantly following pathway adoption (5.77 days post-pathway compared to 5.72 days pre-pathway, P = .940) (Figure 2). The complication rate was similar after pathway adoption (7.3% post-pathway vs 7.5% pre-pathway, P = .931). No patients developed a progressive neurological deficit following nonoperative treatment.
Pre- Versus Post-Pathway Outcomes in All Patients.
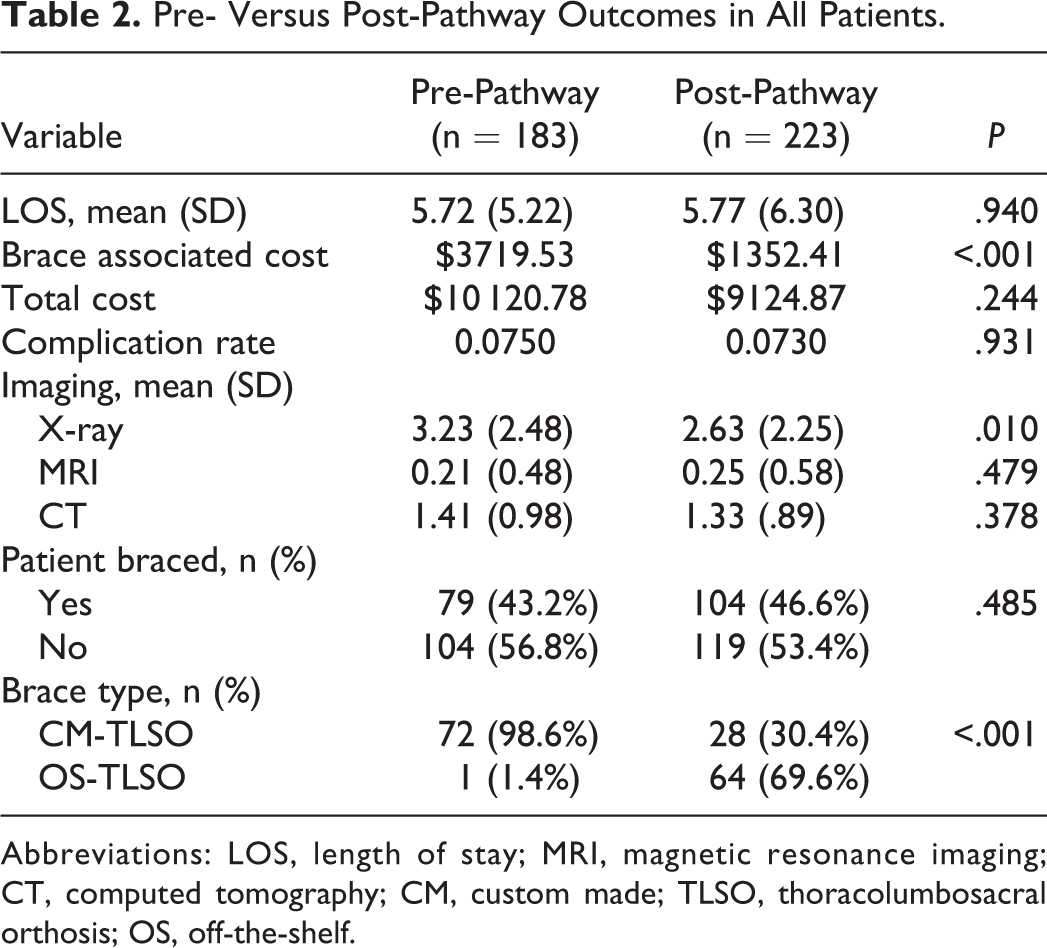
Abbreviations: LOS, length of stay; MRI, magnetic resonance imaging; CT, computed tomography; CM, custom made; TLSO, thoracolumbosacral orthosis; OS, off-the-shelf.
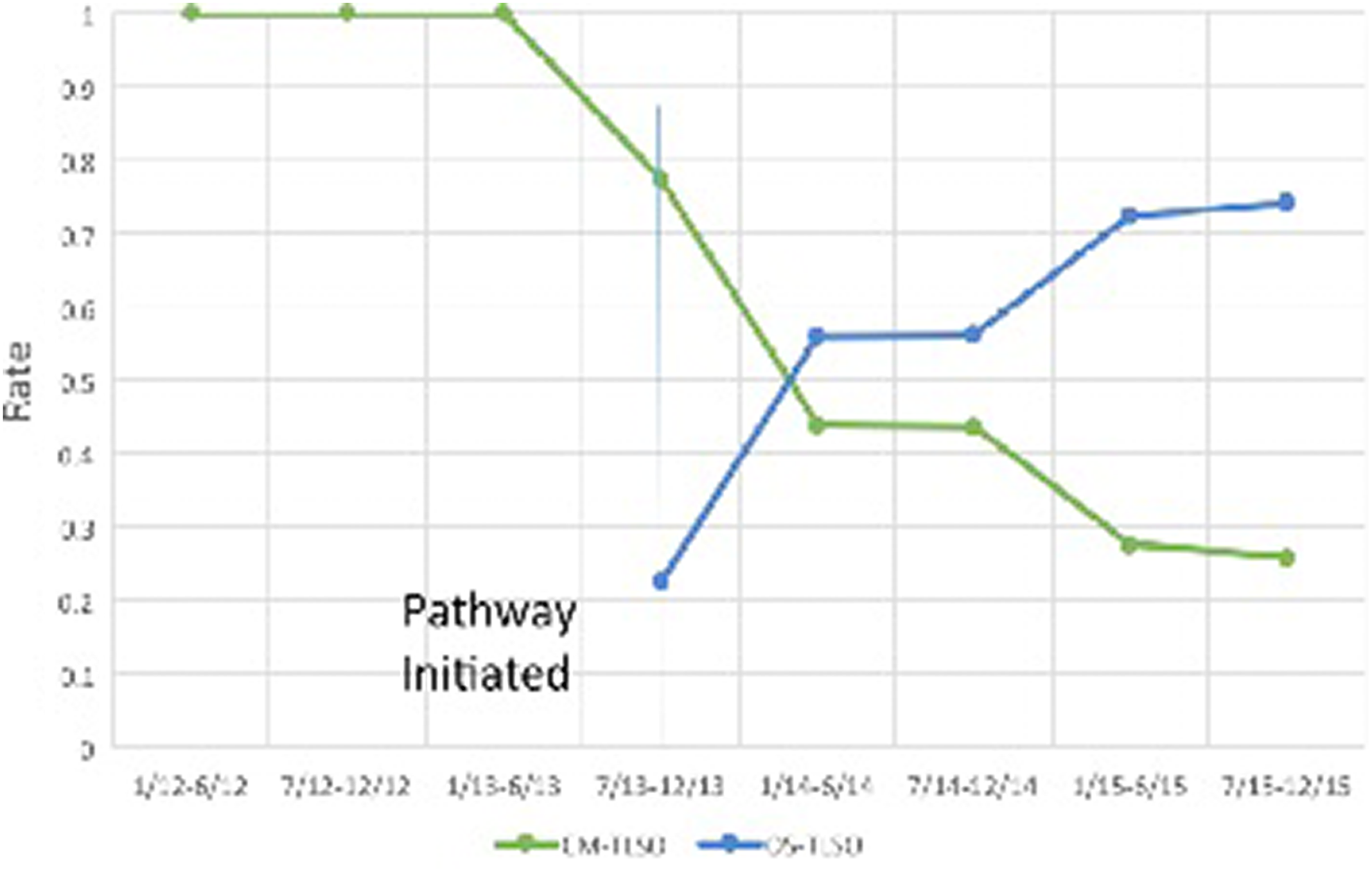
Type of brace ordered (rate) through the study period for both services combined.
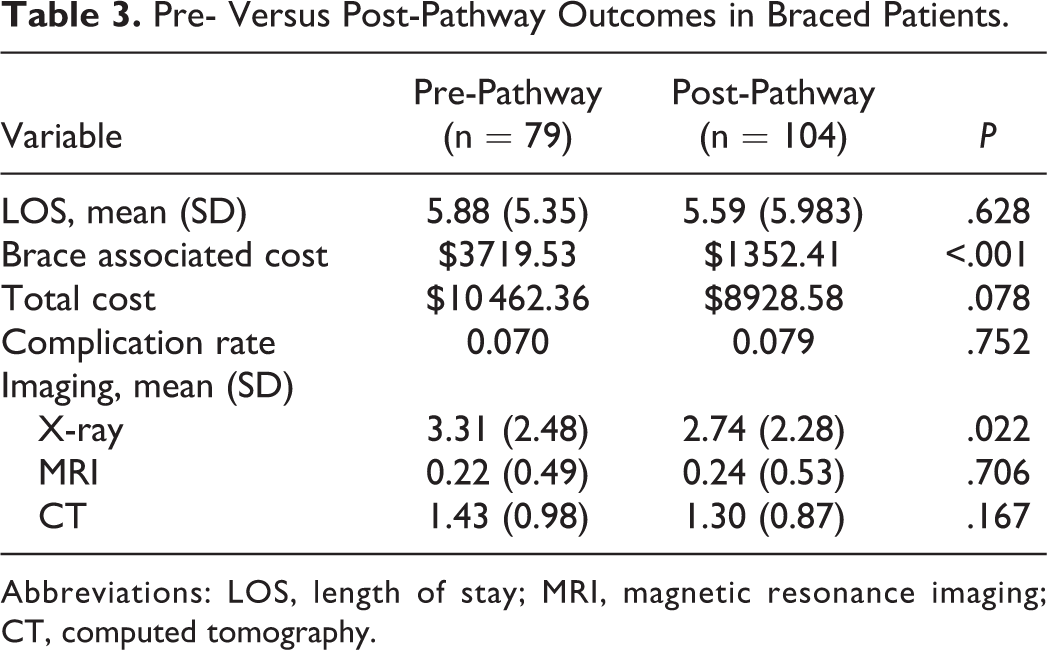
Within the bracing group, bracing-associated costs decreased from $3719.53 pre-pathway to $1352.41 post-pathway (P < .001; Table 3). Overall costs for braced patients also trended lower, from $10 462.36 pre-pathway to $8928.58 post-pathway, though this difference was not significant (P = .078). For braced patients, the mean LOS did not change significantly after pathway adoption (5.88 days pre-pathway vs 5.59 post-pathway days, P = 0.628).
Pre- Versus Post-Pathway Outcomes in Braced Patients.
Abbreviations: LOS, length of stay; MRI, magnetic resonance imaging; CT, computed tomography.
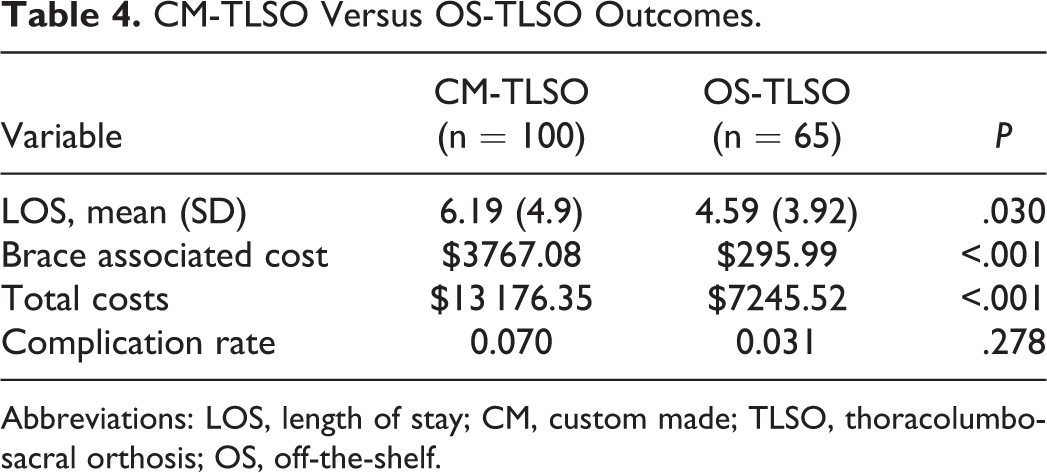
Among braced patients, the mean bracing costs ($3767.08 CM-TLSO vs $295.99 OS-TLSO, P < .001; Table 4) and overall costs per patient ($13 176.35 CM-TLSO vs $7245.52 OS-TLSO, P < .001) were significantly higher for the CM-TLSO patients. Patients treated with a CM-TLSO had a significantly longer LOS compared to those treated with an OS-TLSO (6.19 days vs 4.59 days, P = .030). There were no significant differences in complications between these groups (7.0% CM-TLSO vs 3.1% OS-TLSO, P = .278).
CM-TLSO Versus OS-TLSO Outcomes.
Abbreviations: LOS, length of stay; CM, custom made; TLSO, thoracolumbosacral orthosis; OS, off-the-shelf.
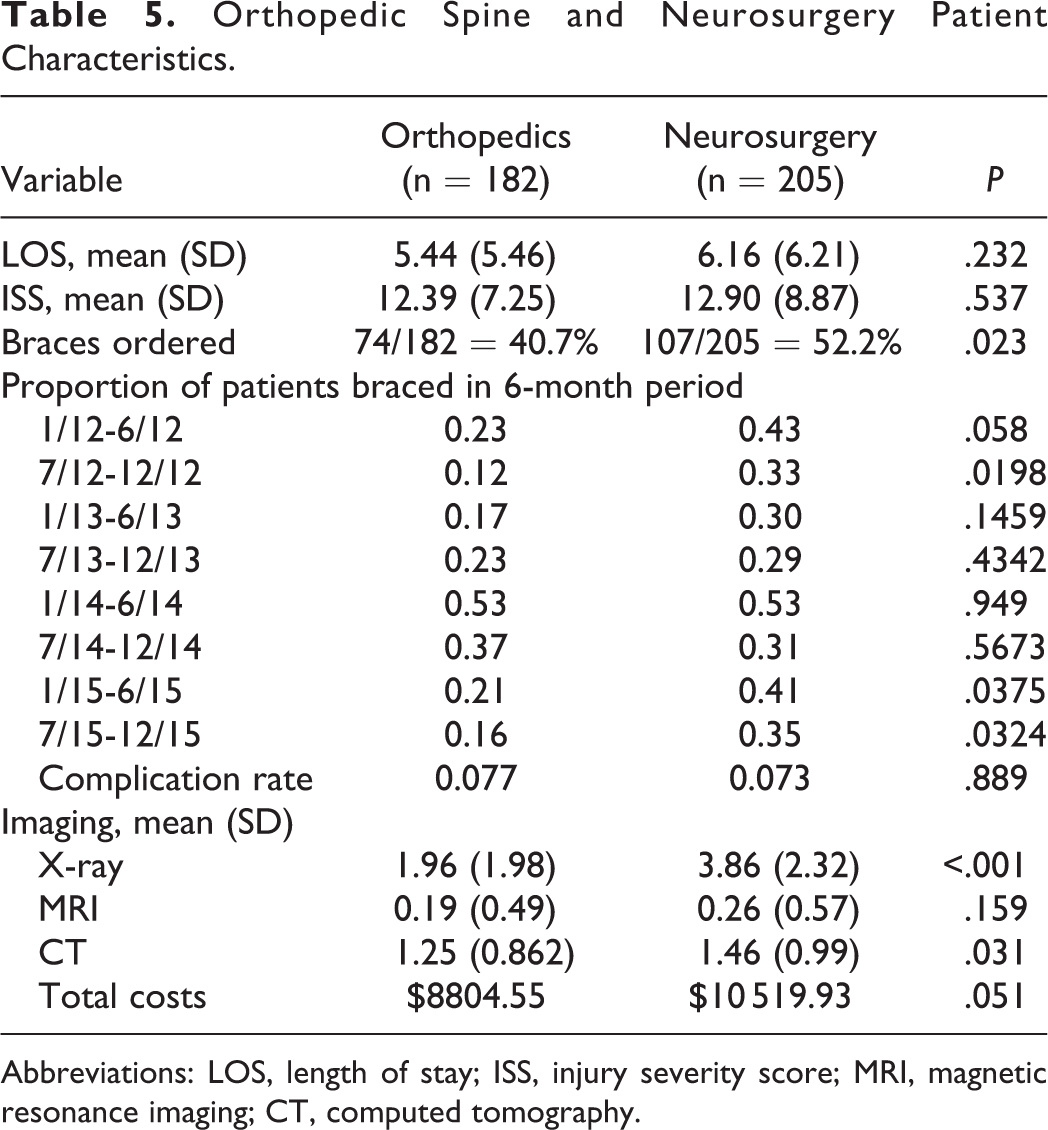
The orthopedic spine and neurosurgery patients did not differ based on ISS (12.39 vs 12.90, P = .537; Table 5) or other characteristics. The orthopedic spine service braced patients less frequently than the neurosurgery service; orthopedics braced 40.7% of TL fracture patients, while neurosurgery braced 52.2% (P = .023). When the pathway was adopted in June 2013, the bracing rate became similar between the spine services (Figure 3). The orthopedic spine service initially increased its bracing rate following pathway adoption. However, this service subsequently reduced their bracing over time such that approximately 20% of their patients were braced in the final 12 months of the study, which was similar to their pre-pathway bracing rate. By the end of the study, the neurosurgery service had reduced its bracing rate compared to its pre-pathway rate. The orthopedic spine surgery service ordered significantly fewer radiographs per patient compared to the neurosurgery service (1.96 vs 3.86, P < .001; Table 5). Patients treated by the orthopedic spine service trended toward having a lower overall cost of care ($8804.55 vs $10 519.93, P = .051). The LOS for patients treated by the 2 services was not significantly different (5.44 orthopedics vs 6.16 neurosurgery, P = .232).
Orthopedic Spine and Neurosurgery Patient Characteristics.
Abbreviations: LOS, length of stay; ISS, injury severity score; MRI, magnetic resonance imaging; CT, computed tomography.
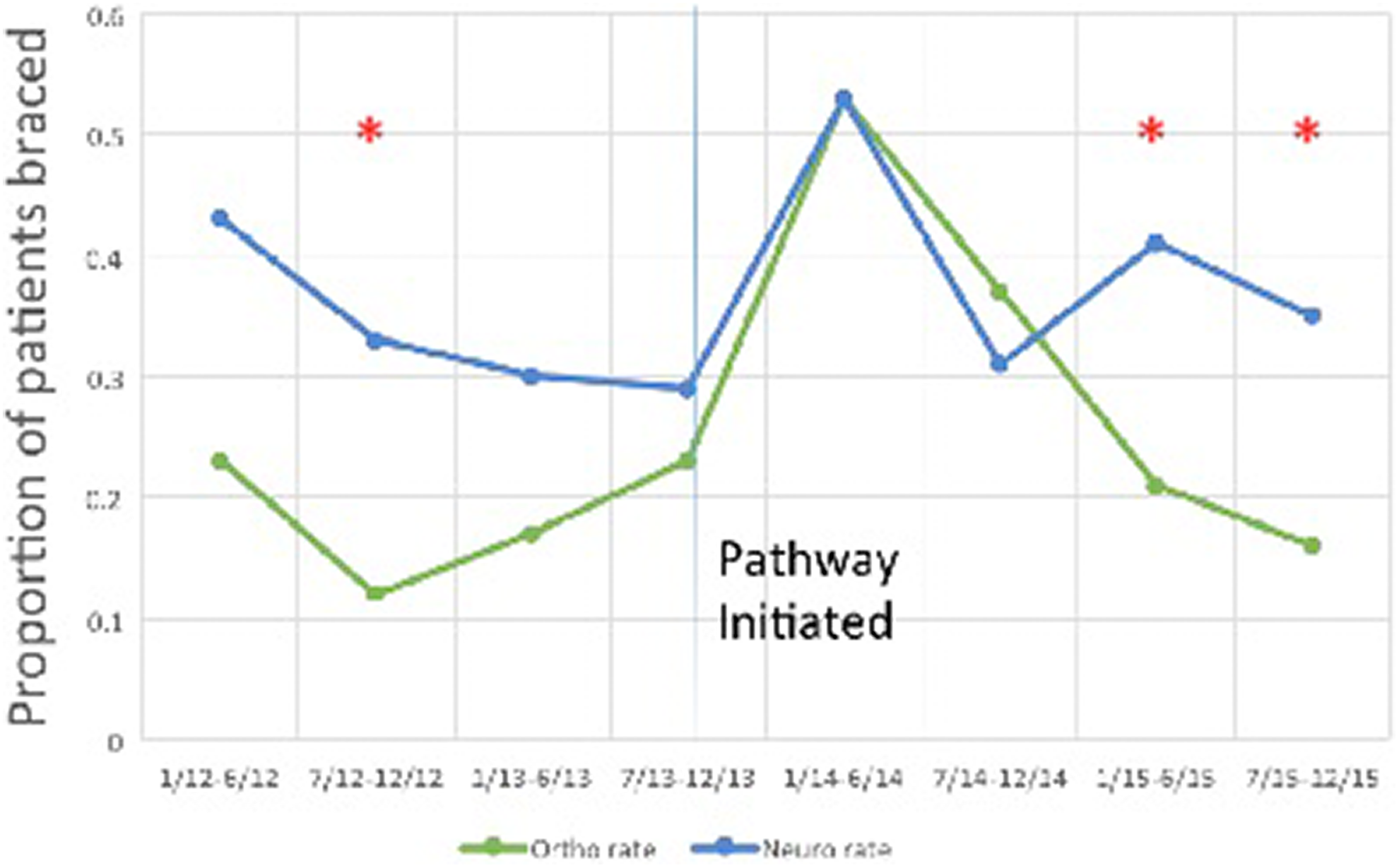
Bracing rates of the 2 spine services throughout the study period. *Shows a statistically significant difference (P < .05) between proportion of braces ordered between the 2 spine services.
Discussion
Thoracolumbar fractures are common injuries, and a large proportion of these fractures can be successfully treated without surgery. 2,17,18 However, most literature on this topic has focused on surgical treatment, with relatively few publications evaluating nonoperative treatment. 2,4,12 To our knowledge, no study has evaluated the effect of a nonoperative care pathway for these injuries. Given the wide variation in treatment observed within our institution, a multidisciplinary team was created to develop a standardized care pathway in an effort to expedite mobilization, reduce complications related to bed rest, minimize radiation exposure, and reduce LOS and cost. This study aimed at quality improvement; our goal was to evaluate the differences in radiographs, costs, LOS, and others, among patients that were braced. The indications for bracing were not in the scope of this study. Furthermore, as previous studies have evaluated outcomes, this study was not intended to compare outcomes of nonoperative treatment. The team reviewed the literature and found little support for the use of expensive CM-TLSOs for the treatment of stable TL fractures. 7,9 -12,14 As such, the pathway recommended either no bracing or use of a less expensive OS-TLSO. Additionally, the use of serial radiographs at 30°, 60°, and 90° was discouraged unless instability was expected, and early mobilization was the default activity order. The use of a templated electronic order set for nonoperative TL fracture care encouraged providers to comply with the pathway.
Adoption of the care pathway was associated with an increased proportion of braced patients treated with the less expensive OS-TLSO and lower bracing costs. The OS-TLSO cost approximately $3500 less than the CM-TLSO (mean bracing cost $3767.08 vs $261.63). The OS-TLSO was typically fit to the patient the same day it was ordered. On the contrary, it took approximately 24 to 72 hours from the time the CM-TLSO was ordered until it arrived for the patient’s use, and this delay likely contributed to a 1.6-day increase in LOS for the CM-TLSO patients. Overall inpatient costs for those braced also decreased by over $1500 following adoption of the care pathway, likely due to the combination of lower bracing costs, fewer radiographs, and lower LOS. However, the primary driver of this decreased cost is likely the lower cost of the OS-TLSO. This study suggests that using the OS-TLSO contributed to the observed cost savings of $5900 per patient when compared to the CM-TLSO. Safety was apparently not affected by pathway adoption as no patient sustained a progressive neurological deficit at any point in the study, and the inpatient complication rate was not significantly different during the 2 different time periods.
Prior studies have shown that adoption of a care pathway reduces variation, improves outcomes, and reduces cost for cancer treatment, kidney surgery, and critical care. 5,6,19,20 Comparison of our results to the literature is difficult as we are unaware of a study reporting the results of a nonoperative care pathway for TL fractures. However, the literature has made it clear that the use of a brace for stable TL fractures does not improve patient-reported outcomes or kyphosis compared to treatment without a brace. 4,7,9 -11,21 As such, we felt it safe to encourage the use of no bracing or a less expensive OS-TLSO despite the fact that no head to head study comparing CM-TLSO to OS-TLSO has been published. Additionally, no study has evaluated the benefit of routine serial radiographs at 30°, 60°, and 90° for TL fracture patients, so we discouraged this practice unless instability was suspected. We observed no neurological complications as the use of serial radiographs decreased. This study suggests that a care pathway for TL fractures that are going to be managed nonoperatively can provide similar benefits as those observed for other conditions.
While some studies have been performed comparing surgical outcomes between orthopedic spine surgeons and neurosurgeons, we are unaware of studies comparing nonoperative spine care between the 2 subspecialties. 22,23 Our study indicates that significant practice variation existed between orthopedics and neurosurgery in our institution. The reduction in variation between the 2 services observed after pathway adoption indicates that change in practice patterns can occur when an evidence-based care pathway is adopted and widely used. We believe that including all stakeholders in the pathway development process was key to its widespread adoption.
There are important limitations to a before-after study design based on a retrospective chart review. While some of the observed changes may have been due to the care pathway, some of the changes may have occurred without the pathway due to individual practice trends (“secular trends”). However, it is not possible to determine the effect of the pathway versus secular trends in an observational study design. Additionally, patient and fracture characteristics could have changed in unmeasured ways over time. Since no randomization occurred, patients treated with different bracing regimens may have had baseline differences driving some of the observed outcomes. This study also did not include patient-reported outcomes or radiographic outcomes. Multiple prior studies have demonstrated the lack of benefit associated with bracing for stable TL fractures, and this study did not aim to replicate those findings. 7,9,11,14 In this study, providers were not compelled to follow the pathway, and fracture stability determination and treatment was ultimately up to their clinical judgment. A greater degree of change may have been observed had we been more stringent in our efforts to ensure compliance with the pathway. However, our goal was to encourage rather than compel compliance with the pathway as we believed this approach would lead to greater levels of adoption. Finally, the study was likely underpowered to detect relatively rare complications. Despite these limitations, we believe this study provides reasonable evidence that a standardized care pathway for nonoperative management of TL fractures can have positive effects on cost and radiation exposure without compromising patient safety.
The use of standardized care pathways can reduce unwarranted variation in treatment; as seen in this study, they can reduce radiation and costs as well. This study demonstrated the effects of a care pathway in the management of compression and burst-type TL fractures treated nonoperatively. Adoption of the pathway was associated with greater use of a less expensive OS-TLSO, fewer inpatient radiographs, and reduced costs for braced patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.