
Abstract
Study Design:
Retrospective review.
Objectives:
To evaluate the rate of nonoperative treatment failure for cervical facet fractures while secondarily validating computed tomography–based criteria proposed by Spector et al for identifying risk of failure of nonoperative management.
Methods:
Single-level or multilevel unilateral cervical facet fractures from 2007 to 2014 were included. Exclusion criteria included spondylolisthesis, dislocated or perched facets, bilateral facet fractures at the same level, floating lateral mass, thoracic or lumbar spine injuries, or spinal cord injury. Patients were placed into 3 groups for evaluation: immediate operative management, successful nonoperative management, and failed nonoperative treatment requiring surgical intervention.
Results:
Eighty-eight patients (106 facets) were included. Twenty-one patients underwent operative treatment with anterior cervical discectomy and fusion or posterior spinal instrumentation and fusion without any failures. Sixty-seven of these patients were treated nonoperatively with either a hard collar (n = 62) or halo vest (n = 5). Eleven patients failed nonoperative treatment (16.4%), all with an absolute fracture height of at least 1 cm and 40% involvement of the absolute height of the lateral mass. Of the 56 patients successfully treated through nonoperative measures, 8 (14.3%) had fracture measurements exceeding both operative parameters.
Conclusion:
We conclude that it is safe and appropriate for patients with unilateral cervical facet fractures to receive a trial period of nonoperative management. However, patients who weigh over 100 kg, have comminuted fractures, or have radiographic measurements outside of the proposed computed tomography criteria for nonoperative treatment should be educated on the risks of treatment failure.
Introduction
Cervical facet fractures are a relatively common injury and comprise approximately 10% of all subaxial cervical spine fractures. 1 The primary concern when evaluating cervical facet fractures is the resulting degree of instability that would necessitate surgical intervention. Classification systems such as the Cervical Spine Injury Severity score and Subaxial Cervical Spine Injury Classification system would direct these injuries toward nonoperative management 2 ; however, data from previous studies on facet fractures suggests an unacceptably high rate of failure when treated nonoperatively, with reported failure rates approaching 80%. 3 –6 As a result, optimal management of cervical facet fractures continues to be controversial.
These injuries are easily missed and difficult to diagnose on plain radiographic imaging because they present most commonly as minimally or nondisplaced fractures. 1,7 Previous reports have shown that as many as 67% of the fractures and 45% of the subluxations and dislocations were not detected by physical exam and plain X-ray. 7 Many of the previous facet studies included a wide spectrum of traumatic injuries ranging from nondisplaced fractures to floating lateral mass injuries. 4 –6,8,9 Cervical facet fractures can be very complex in nature, including fractures extending into the posterior cervical elements in a variety of patterns. 10 Applying clinical and radiographic outcomes to the entire spectrum of cervical facet fractures is challenging and highly variable, 9 specifically when comparing severe facet fractures to less severe injuries and the operative versus nonoperative treatments for both.
There are few studies in the current literature that analyze the radiographic features or treatment options of unilateral cervical facet injuries at a single or multiple levels that are not dislocated, subluxated, or perched. 9,11 –15 One study by Spector et al 9 proposed a computed tomography (CT)–based criteria for identifying unilateral facet fractures that are at risk for failure of nonoperative management. The study evaluated various facet measurements and found that patients with unilateral cervical facet fractures at a single level that involve more than 40% of the absolute height of the intact lateral mass or an absolute fracture height greater than 1 cm are at increased risk for failure of nonoperative treatment. Unfortunately, the study is limited by its small sample size of only 24 patients (26 facet fractures). The primary goal of this study is to evaluate the rate of nonoperative treatment failure for unilateral cervical facet fractures at a single or multiple levels treated with a hard cervical collar or halo vest immobilization. Our secondary goal is to validate the utility of CT-based criteria for identifying risk factors for failure of nonoperative management that were proposed by Spector et al. 9
Materials and Methods
After institutional review board approval, we conducted a retrospective review of patients with unilateral cervical facet fractures that presented to a single level 1 trauma center from 2007 to 2014. Patients with a primary diagnosis of unilateral cervical spine facet fracture at a single level or multiple levels were included. Victims of polytrauma were included as long as their associated injuries did not affect management of their cervical spine injuries. Simple and comminuted facet fractures were included. Exclusion criteria included fractures resulting in spondylolisthesis, dislocated or perched facets, bilateral facet fractures at the same level, floating lateral mass, thoracic or lumbar spine injuries, or spinal cord injuries beyond an isolated cervical radiculopathy. Avulsion fractures of the cervical facet, defined as fractures with less than 1 mm in width, were not included for evaluation in this study. In addition, patients without CT imaging or fewer than 8 weeks (56 days) of follow-up were excluded.
Standard patient demographic information was reviewed, including age, date of injury, injury mechanism, type of treatment, presence or absence of radiculopathy, and dates of last follow-up. Initial CT evaluation was performed on all patients using CT-based measurements previously described by Spector et al in 2006. 9 In patients with multilevel facet fractures, radiographic fracture characteristics were evaluated using the single largest fracture. Absolute fracture height was found by measuring from the tip of the facet to the edge of the fracture as shown in Figure 1A. Absolute height of the intact contralateral lateral mass was found by measuring the maximum tip to tip (cephalad to caudad) height as seen on sagittal CT imaging in Figure 1B. Percent involvement of the height of the intact contralateral lateral mass was calculated as the quotient of the absolute fracture height and absolute height of the intact contralateral lateral mass. Comminution was defined as greater than 2 fracture fragments in the cervical facet on the axial or sagittal CT image sequences at the time of diagnosis.
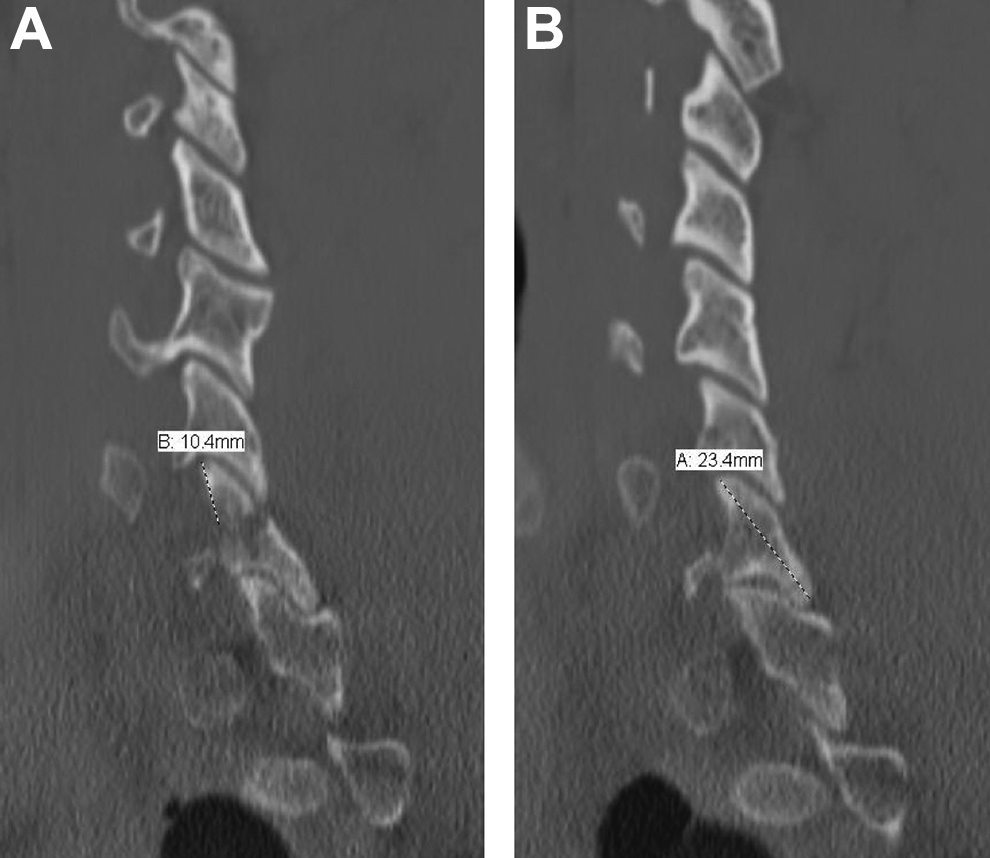
Sagittal CT images showing (A) absolute fracture height found by measuring from the tip of the facet to the edge of the fracture and (B) absolute facet height found by measuring the tip to tip (cephalad to caudad) height of the intact contralateral facet.
Our analysis was done by looking at all study patients first (single and multilevel facet fractures), and then a separate analysis was then done only using isolated (single-level) facet fractures. Patients were grouped based on initial treatment after injury: operative and nonoperative. The nonoperative group was further subclassified based on success or failure of treatment. Patients in the nonoperative treatment cohort were either treated with a hard cervical collar (Aspen collar) or halo vest according to surgeon preference. Patients treated operatively received either an anterior cervical discectomy and fusion or posterior spinal instrumentation and fusion based on traditional criteria (ie, evidence of instability or symptomatic neurologic injury). Radiographic and CT imaging for all patients was reviewed to determine response to treatment. Complications were evaluated with additional CT imaging. Successful nonoperative treatment was defined as radiographic evidence of union at follow-up. Treatment failure was defined as fracture instability, subluxation, or progression of spondylolisthesis, new onset radiculopathy, or persistent radiculopathy caused by nonunion or malunion at time of follow-up requiring surgical treatment after any attempt at conservative management. The patients from each treatment group were then evaluated using the previously mentioned CT-based criteria described by Spector et al. 9
Detailed statistical analysis was used to evaluate our data. Analysis of variance (ANOVA), F tests, and Student’s t tests were used to compare continuous variables, while χ2 and Fisher’s exact tests were used for categorical variables between operative and nonoperative groups. Post hoc analysis using a Bonferroni-corrected method was used to compare demographic and fracture measurement data between the 3 treatment groups. For these analyses, P < .017 was considered statistically significant; otherwise, P < .05 was considered statistically significant. Sensitivity and specificity of radiographic fracture criteria were calculated using standard methods.
Results
More than 1500 patients were identified who had cervical facet fractures, but only 134 patients were found to meet inclusion criteria for the study. On further review, 46 patients had inadequate imaging or short follow-up time and were excluded. In total, 88 patients with 106 unilateral facet fractures at single or multiple levels were included in this study. Of those, 21 patients (24 facets) were initially treated with surgery, and 67 patients (82 facets) were treated nonoperatively. The average age was 43.8 (18-79) years, and 73.9% were male. The mean radiographic follow-up was 14.1 months (range 1.9-106.0). C7 facets represented 37.7% (n = 40) of involved vertebrae, C6 represented 43.4% (n = 46), and C3-C5 contributing to the remaining 18.9% (n = 20). Motor vehicle collisions (including all-terrain vehicle accidents) were responsible for 68 (77.3%) of these cervical injuries. A combination of falls, assaults, accidents, and tornado victims represented the remaining 20 injuries (22.7%).
The 67 nonoperatively managed patients with single and multilevel facet fractures were placed in either a hard cervical brace (n = 61, 91%) or halo vest orthosis (n = 6, 9%). At final follow-up, all patients initially treated with surgery (n = 21) achieved stable union without need for further treatment. Fifty-six (83.6%) of all nonoperatively managed patients were treated successfully; however, 11 (16.4%) failed nonoperative management and required delayed surgical stabilization. Of the patients that failed nonoperative management, the average length of time until definitive surgical intervention was 38.6 days. Demographic information for patients with single and multilevel facet fractures are summarized in Table 1. Age and gender did not differ significantly between the operative, successful nonoperative, and the failed nonoperative groups; however, the average weight of the nonoperative failure group was significantly higher than operative and successful nonoperative groups (100.6 kg vs 78.7 and 82.9 kg, respectively; P < .017). Fracture characteristics for all study patients with single and multilevel facet fractures are summarized in Table 2. Both absolute fracture height and percent involvement of the height of the intact contralateral lateral mass were significantly smaller in the successful nonoperative patients compared to operative patients or nonoperative failures (P < .017). Nonoperative failures had significantly more fracture comminution than successful nonoperative management (P < .017). Fifty-two percent of patients who underwent immediate surgical stabilization had preoperative radiculopathy compared to 17.9% of successful nonoperative patients (P < .017), and 36.4% of the failed nonoperative group had a preoperative radiculopathy.
Patient Demographic Data in Single and Multilevel Fractures*.
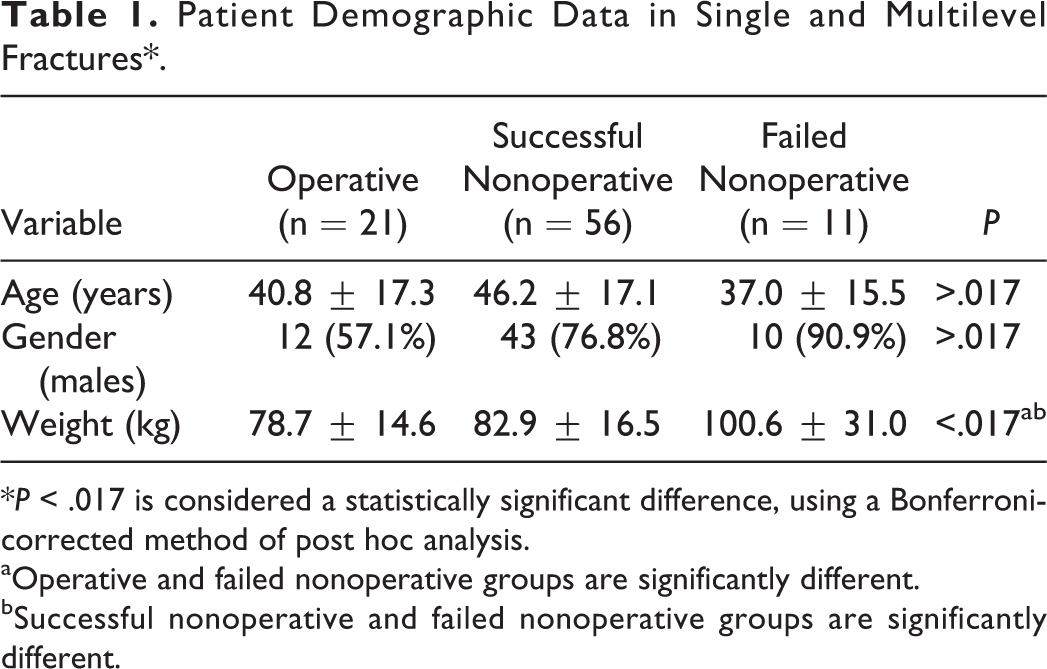
*P < .017 is considered a statistically significant difference, using a Bonferroni-corrected method of post hoc analysis.
aOperative and failed nonoperative groups are significantly different.
bSuccessful nonoperative and failed nonoperative groups are significantly different.
Single and Multilevel Facet Fracture Characteristics*.
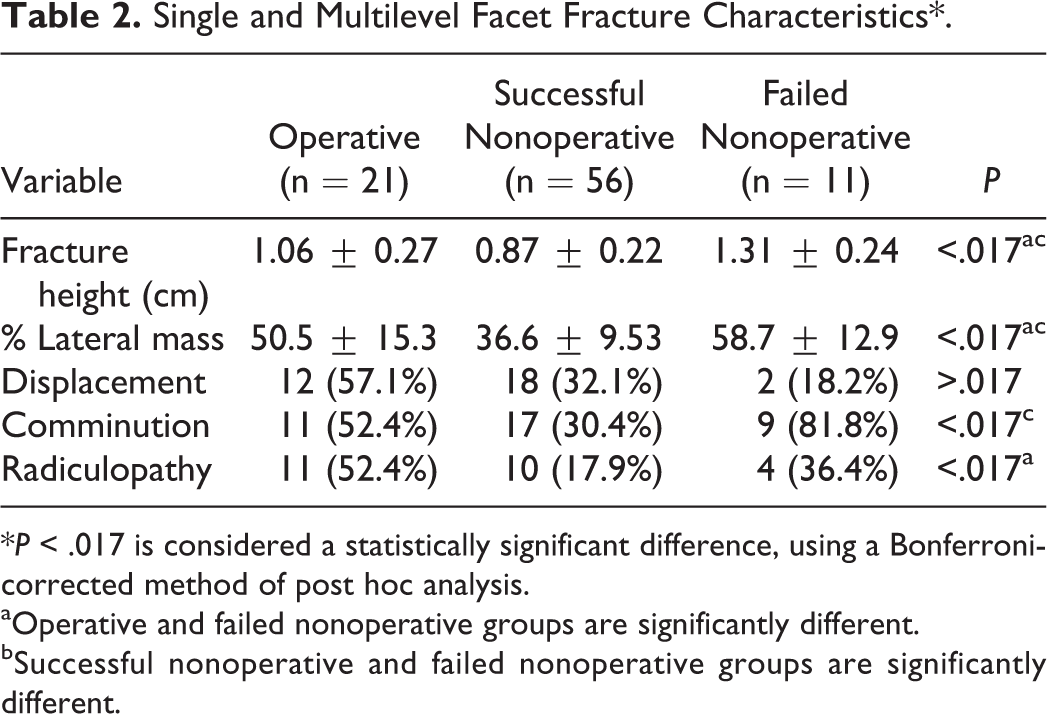
*P < .017 is considered a statistically significant difference, using a Bonferroni-corrected method of post hoc analysis.
aOperative and failed nonoperative groups are significantly different.
bSuccessful nonoperative and failed nonoperative groups are significantly different.
Of all 88 patients in the study, 73 had only a single-level facet fracture. Eighteen (24.7%) of those patients were treated with immediate surgery and 55 (75.3%) were managed nonoperatively and placed in either a hard-cervical brace (n = 50, 90.9%) or halo vest orthosis (n = 5, 9.1%). Forty-five (81.8%) of all nonoperatively managed single-level facet fracture patients were treated successfully, with 10 (18.2%) requiring delayed surgical stabilization. Demographic information for these patients is shown in Table 3. Again, those who failed nonoperative treatment weighed more on average than those who were treated successfully with nonoperative management (P < .017). Otherwise, there were no significant differences in baseline demographic characteristics for these groups. The average length of time from nonoperative treatment until time of definitive surgical intervention was 32.6 days. Facet fracture characteristics for these patients (single level facet fractures) are presented in Table 4. As seen in single and multilevel facet injuries, both fracture height and percent involvement of the height of the intact contralateral lateral mass were significantly smaller in the successful nonoperative patients compared to operative patients or nonoperative failures (P < .017). Furthermore, nonoperative failures had significantly more comminution than successful nonoperative management (P < .017), and operative cases had significantly more radiculopathy than successful nonoperative patients.
Patient Demographic Data in Single-Level Fractures*.
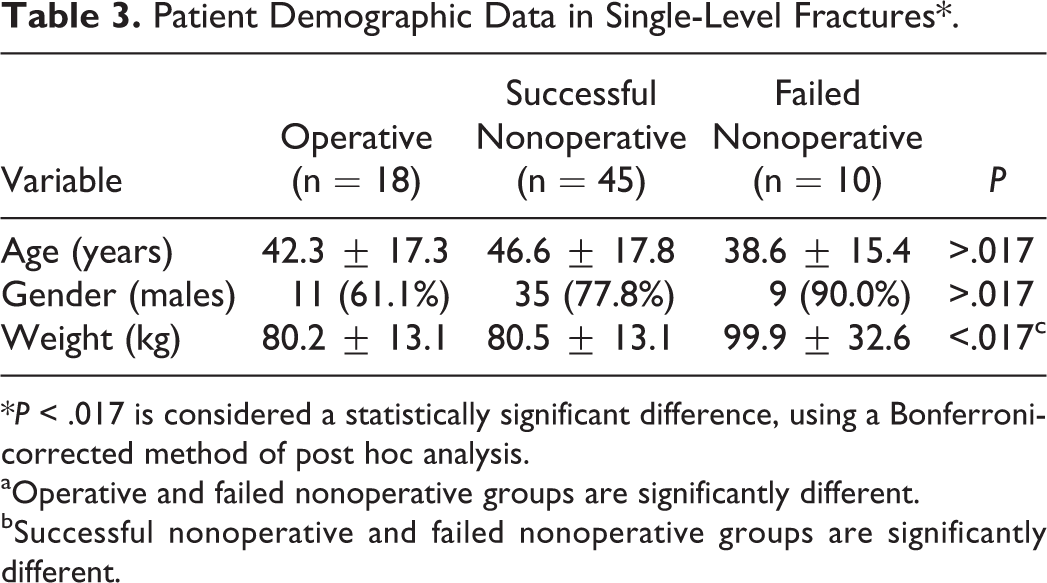
*P < .017 is considered a statistically significant difference, using a Bonferroni-corrected method of post hoc analysis.
aOperative and failed nonoperative groups are significantly different.
bSuccessful nonoperative and failed nonoperative groups are significantly different.
Single-Level Facet Fracture Characteristics*.
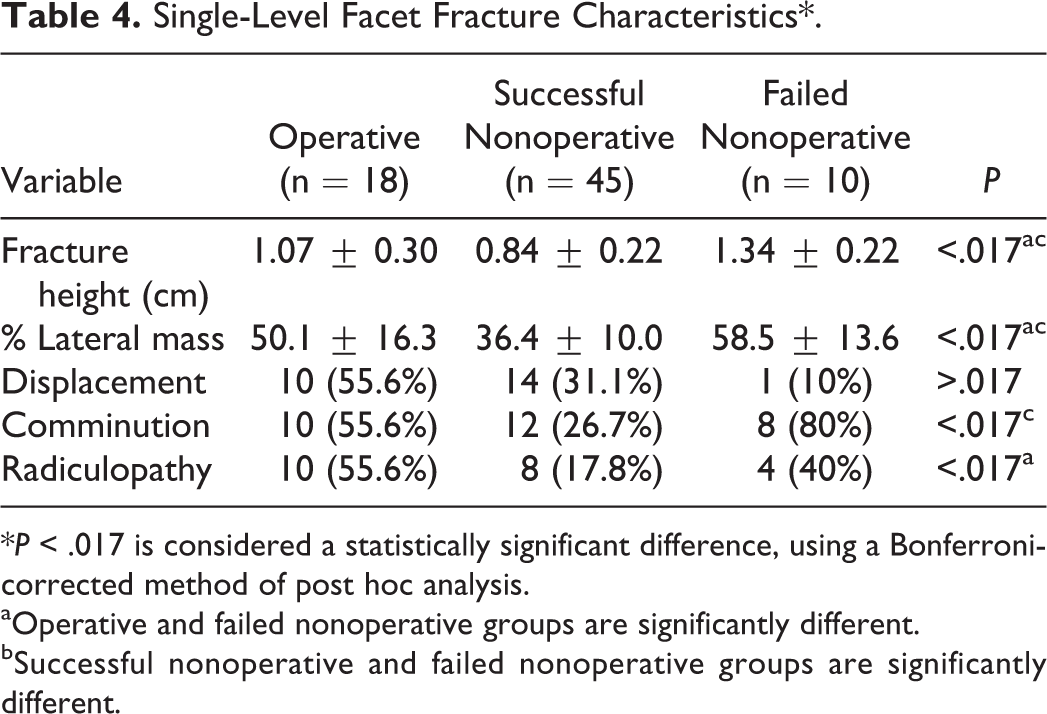
*P < .017 is considered a statistically significant difference, using a Bonferroni-corrected method of post hoc analysis.
aOperative and failed nonoperative groups are significantly different.
bSuccessful nonoperative and failed nonoperative groups are significantly different.
Of the 56 patients with single and multilevel unilateral facet fractures that were successful with nonoperative management, 48 (85.7%) had fractures that were less than 1 cm in height or 40% of the intact contralateral lateral mass, while 8 (14.3%) met both of the proposed fracture criteria for operative treatment and were successfully treated without surgery. Figure 2 displays the sagittal CT imaging of the 8 patients who met both radiographic fracture criteria but were successful with nonoperative management. Of the patients with single and multilevel facet fractures who failed nonoperative management, 11 (100%) had an absolute fracture height of more than 1 cm and greater than 40% involvement of the absolute height of the contralateral lateral mass. Figure 3 displays the key radiographic, magnetic resonance imaging (MRI), or CT imaging showing the spectrum of failures in addition to their prefailure imaging. Table 5 outlines both the mechanism of injury as well as the mechanism of failure for the patients shown in Figure 3.
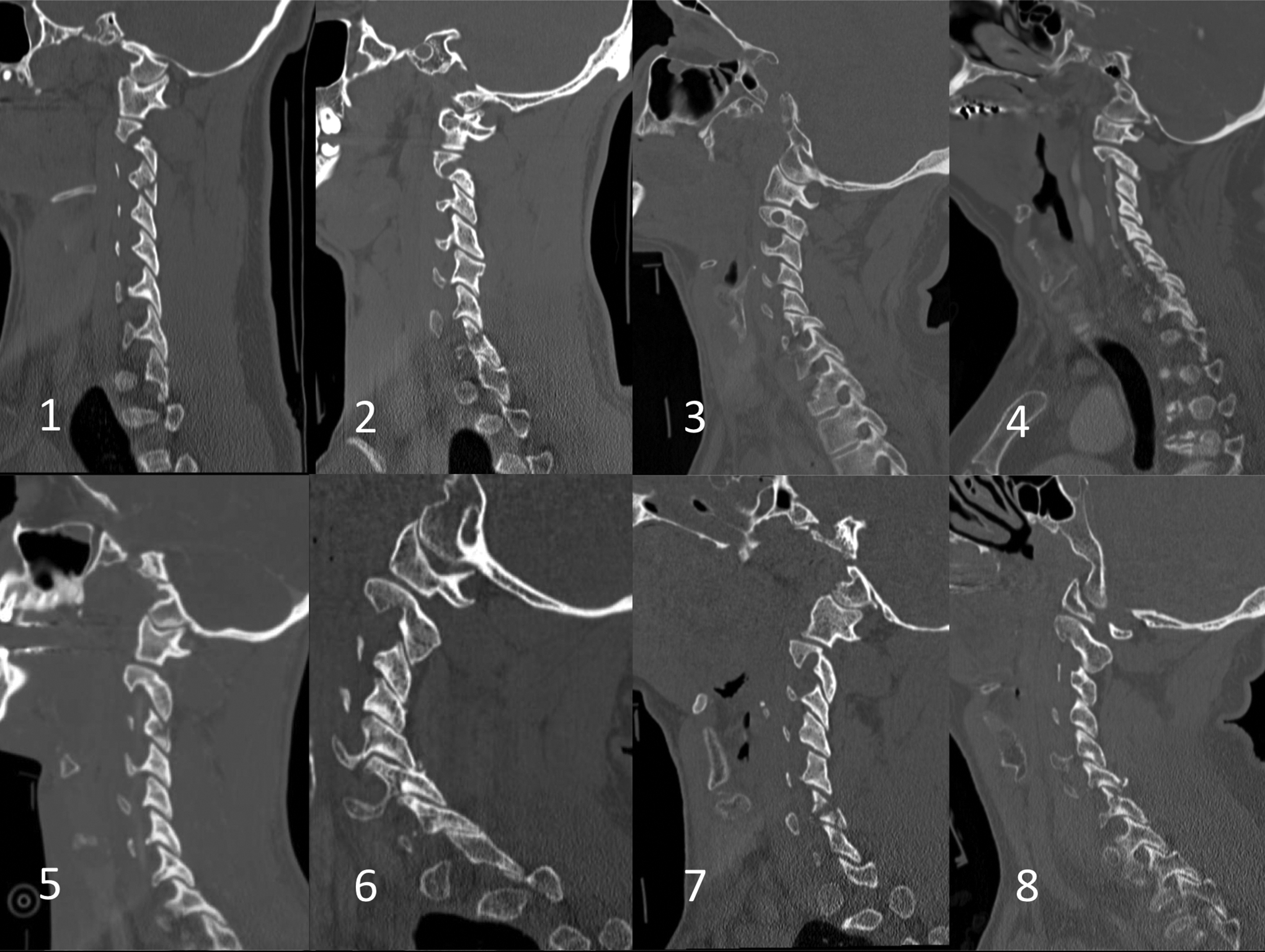
Sagittal CT imaging of the 8 patients who met both radiographic fracture criteria but were successful with nonoperative management.
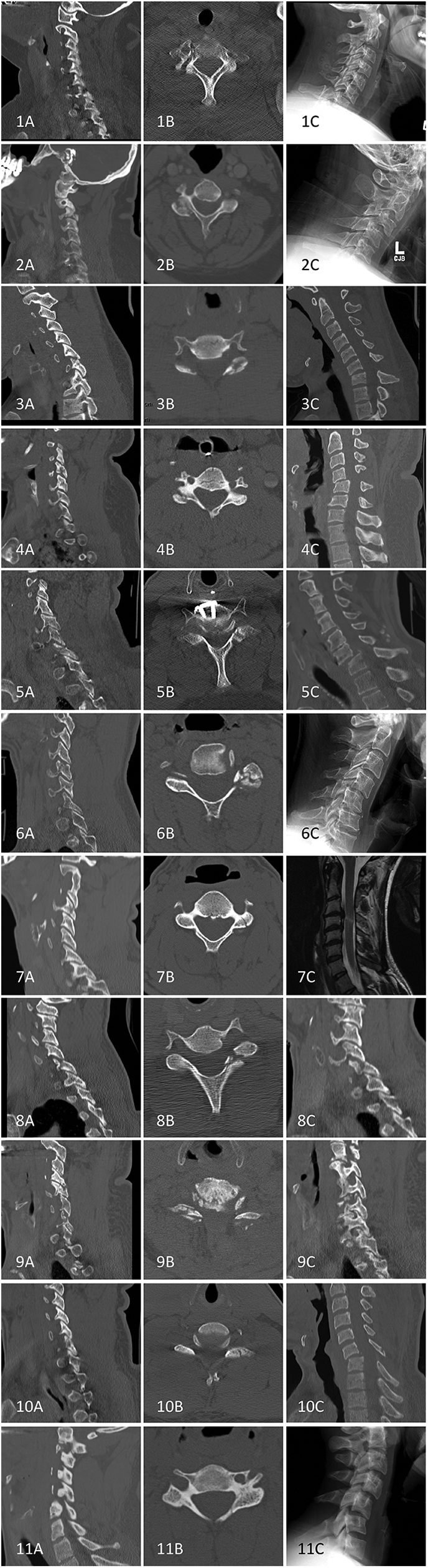
Prefailure sagital (A), postfailure axial (B), and postfailure sagital (C) imaging of the 11 patients that failed nonoperative management and who also met both radiographic fracture criteria.
Mechanism of Failure in Nonoperative Patients.
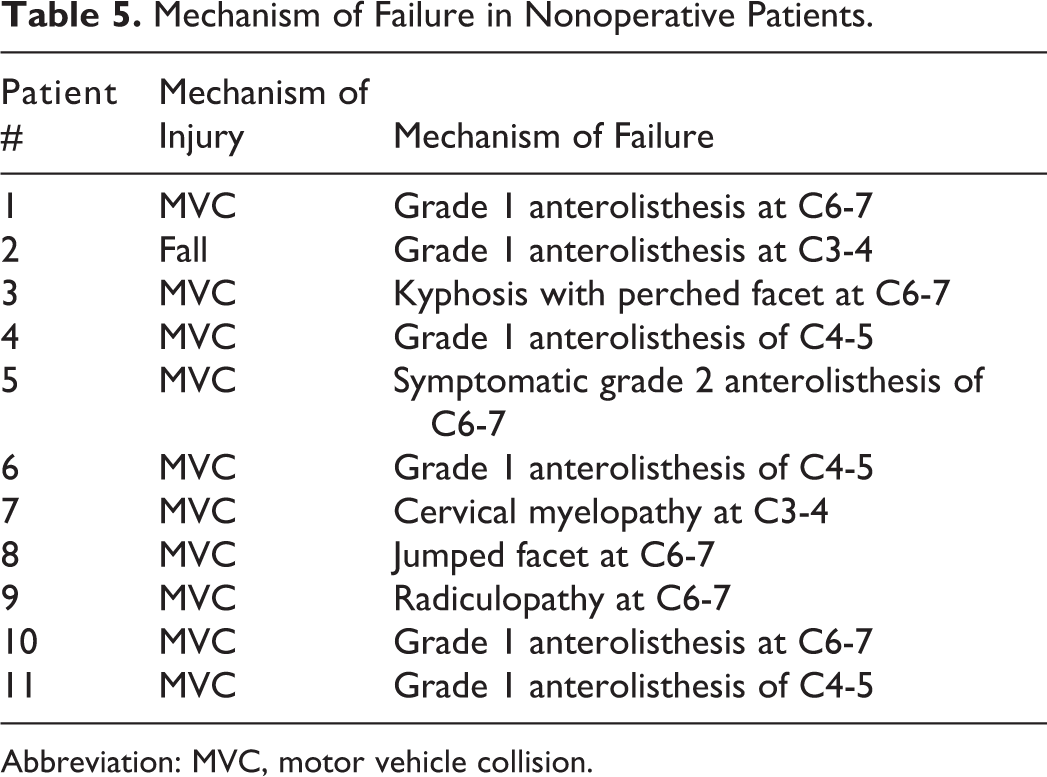
Abbreviation: MVC, motor vehicle collision.
There were 45 patients that had an isolated (single level) unilateral facet fracture that was successfully treated with nonoperative management. Of those, 40 (88.9%) had an absolute fracture height of less than 1 cm or less than 40% of the height of the intact lateral mass, while 5 (11.1%) had measurements above both parameters.
Regarding the form of nonoperative treatment, hard cervical collar was used in 92.9% (n = 52) of nonoperative cases. In the nonoperative failure group, 18.2% (n = 2) were treated in halo vest, while 7.1% (n = 4) of the successful nonoperative group had this treatment.
When evaluating the CT-based criteria proposed by Spector et al, as it pertains to our patient population, the sensitivity was 100% and the specificity was 85.7% as calculated using all single and multilevel unilateral facet fractures that were either successfully treated with conservative measures or failed conservative treatment.
Discussion
Unilateral cervical facet fractures are a commonly encountered injury. 1 As mentioned previously, the current literature is controversial concerning optimal treatment and some studies report a high failure rate for patients treated nonoperatively (20% to 80%). 3 –6 These studies included facet fractures, subluxations, and dislocations, which likely lead to a higher failure rate. Our study was interested in finding out what the failure rate is of those patients treated nonoperatively for unilateral facet fractures as described in detail in the inclusion and exclusion criteria of the methods section.
van Eck et al reported that 9% of nondisplaced, unilateral facet fractures required surgical treatment within the follow-up period for significant radiographic progression of listhesis and/or radicular symptoms. 16 These patients differ from our population because our patients included those with fracture displacement without evidence of spondylolisthesis and also included multilevel fractures. Our study population represents a more severe facet fracture pattern while achieving successful nonoperative treatment in 83.6% of patients.
Classification systems have been used to help guide treatment for many orthopedic pathologies, though isolated facet fractures have not been well categorized into a standard classification system. Despite this, many authors recommend that facet fractures are best managed operatively. 2,4,7,8 We feel that this wide variability in data supports the relatively unpredictable nature of this fracture pattern and the difficulties encountered with treating them. In addition, the wide variation in failure rates can possibly be associated with a diverse fracture morphology included in the data.
Due to the small number of patients with multilevel facet fractures, we were unable to make a direct analysis to determine if multiple unilateral facet fractures are more likely to fail nonoperative management. We instead conducted 2 separate analysis with a cohort of all patients that had single or multilevel unilateral facet fractures and then a cohort with only a unilateral, single-level facet fractures. As our results show, both cohorts had similar outcomes and risk factors.
Our data demonstrates an observed nonoperative failure rate of 16.4% that is consistent with the lower spectrum of rates found in prior reports. In one CT-based study of unilateral cervical facet fractures, Spector et al proposed that an absolute fracture height of greater than 1.0 cm or greater than 40% involvement of the absolute height of the contralateral lateral mass can be used to predict failure. 9 They found a significant difference in absolute fracture height (P = .0002), articular fracture height (P = .008), and percent involvement of the absolute height of the intact lateral mass (P = .026) in patients who failed nonoperative management compared to those who were treated successfully. Furthermore, 100% (n = 5) of the nonoperative failures from their patient cohort had an absolute fracture height greater than 1.0 cm or greater than 40% involvement of the absolute height of the intact lateral mass. Our data supports the radiographic criterion proposed by Spector et al; however, their study suggests each parameter is a risk factor in itself, whereas our data suggests that both criteria are necessary to predict failure as 100% of our nonoperative failures actually met both these criteria. It should be noted that these metrics are sensitive but not specific (100% and 85.7%, respectively), as noted by the 14.3% of successful nonoperative patients that had greater measurement values than those proposed as a cutoff for failure.
In addition, we found that fracture comminution and excessive patient weight were both significant risk factors for failing nonoperative management. We found that patients with comminuted facet fractures were over 3 times more likely to fail nonoperative treatment, as 81.8% of nonoperative failures showed the presence of comminution at the time of injury compared to 30.4% of nonoperative patients that were treated successfully (P < .017). Patient weight was found to be significantly higher in patients who failed nonoperative treatment when compared to operative patients or nonoperative patients treated successfully. The average weight of the nonoperative failure group was significantly higher at 100.6 kg than operative and successful nonoperative groups (78.7 and 82.9 kg, respectively; P < .017). Fracture displacement was not found to be a risk factor for failure of nonoperative treatment in our study population, which is consistent with the current literature. 9 The presence of facet comminution and patient obesity could potentially help predict nonoperative failures in conjunction with the Spector measurements.
The presence of a cervical radiculopathy at the time of injury was noted to be significantly higher in the immediate operative group when compared to the successful nonoperative group. This, in combination with a larger and more comminuted facet fracture, does raise the question of a selection bias in surgeons indicating these patients as operative candidates.
We note several limitations in this retrospective study. Although obtaining patient outcomes data in a long-term fashion is ideal, this does leave room for significant and immeasurable variables that could possibly alter outcomes. Ideally, these patient-centered outcome scores would be obtained at measured time intervals in the short- and long-term follow-up periods to better shed light on a potential degenerative component to this traumatic injury’s outcome. MRI analysis of these patients’ fractures was not routinely used and was therefore not able to be applied, as a whole, to patients in this study. MRI may have elucidated any discoligamentous injuries that occurred at the time of fracture that precluded the failure group to requiring surgery. Also, our rates and duration of follow-up were diverse, ranging from months to years postinjury. Psychosocial and economic factors were not accounted for in this study. These factors have the distinct possibility of contributing to long-term patient outcome scores and could be better analyzed in a well-organized trial.
Conclusion
To our knowledge, this is one of the largest collections of nonoperatively treated cervical facet fractures in published literature. Our data is consistent with a study by Spector et al that reports that cervical facet fractures with an absolute fracture height of more than 1 cm or at least 40% involvement of the absolute height of the intact lateral mass is at a significantly increased risk of failure if treated nonoperatively. However, we propose that both criteria must be met in order to more accurately predict failure. We also found that comminuted facet fractures and patients that weighed an average of 100 kg are at increased risk of nonoperative treatment failure. We conclude that treating unilateral facet fractures with a trial period of conservative measures in a hard cervical collar is safe and appropriate. Patients who weigh over 100 kg, have comminuted facet fractures, or have radiographic measurements outside of the proposed safety criteria for nonoperative treatment should be educated on the risks of treatment failure that may lead to the need for surgical intervention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.