
Abstract
Study Design:
Narrative literature review.
Objectives:
Placental tissue, amniotic/chorionic membrane, and umbilical cord have seen a recent expansion in their clinical application in various fields of surgery. It is important for practicing surgeons to know the underlying science, especially as it relates to spine surgery, to understand the rationale and clinical indication, if any, for their usage.
Methods:
A literature search was performed using PubMed and MEDLINE databases to identify studies reporting the application of placental tissues as it relates to the practicing spine surgeon. Four areas of interest were identified and a comprehensive review was performed of available literature.
Results:
Clinical application of placental tissue holds promise with regard to treatment of intervertebral disc pathology, preventing epidural fibrosis, spinal dysraphism closure, and spinal cord injury; however, there is an overall paucity of high-quality evidence. As such, evidence-based guidelines for its clinical application are currently unavailable.
Conclusions:
There is no high-level clinical evidence to support the application of placental tissue for spinal surgery, although it does hold promise for several areas of interest for the practicing spine surgeon. High-quality research is needed to define the clinical effectiveness and indications of placental tissue as it relates to spine surgery.
Keywords
Introduction
The use of mesenchymal stem cells (MSCs) in orthopedic and spinal surgery has become a popular topic in recent years with the introduction of numerous different products of various cellular origins, ranging from bone marrow, adipose tissue, synovial tissue, to placental tissue. 1 –5 Placental tissue has gained particular popularity as a tissue source identified as a rich source of MSCs as well as other growth factors beneficial to tissue repair and regeneration. 6 Several commercially available products have been introduced recently as a clinical alternative for spinal injuries and pathologic conditions, ranging from intervertebral disc degeneration to traumatic spinal cord injuries. However, the evidence supporting the clinical application of these products often lags behind marketing strategies. The goal of this article is to review the science and evidence relating to the clinical application of placental tissue in treating various spinal pathology.
Placental Tissue
The membranes surrounding the developing fetus are a complex structure of various tissue subtypes that play a critical role in fetal development and sustenance. The membranes consist of 4 distinctly different structures: the amnion, chorion, umbilical cord, and placenta (Figure 1). Of these, the fetal-derived tissues, the amnion, chorion, and umbilical cord, have been investigated as potential source of MSCs for clinical application.
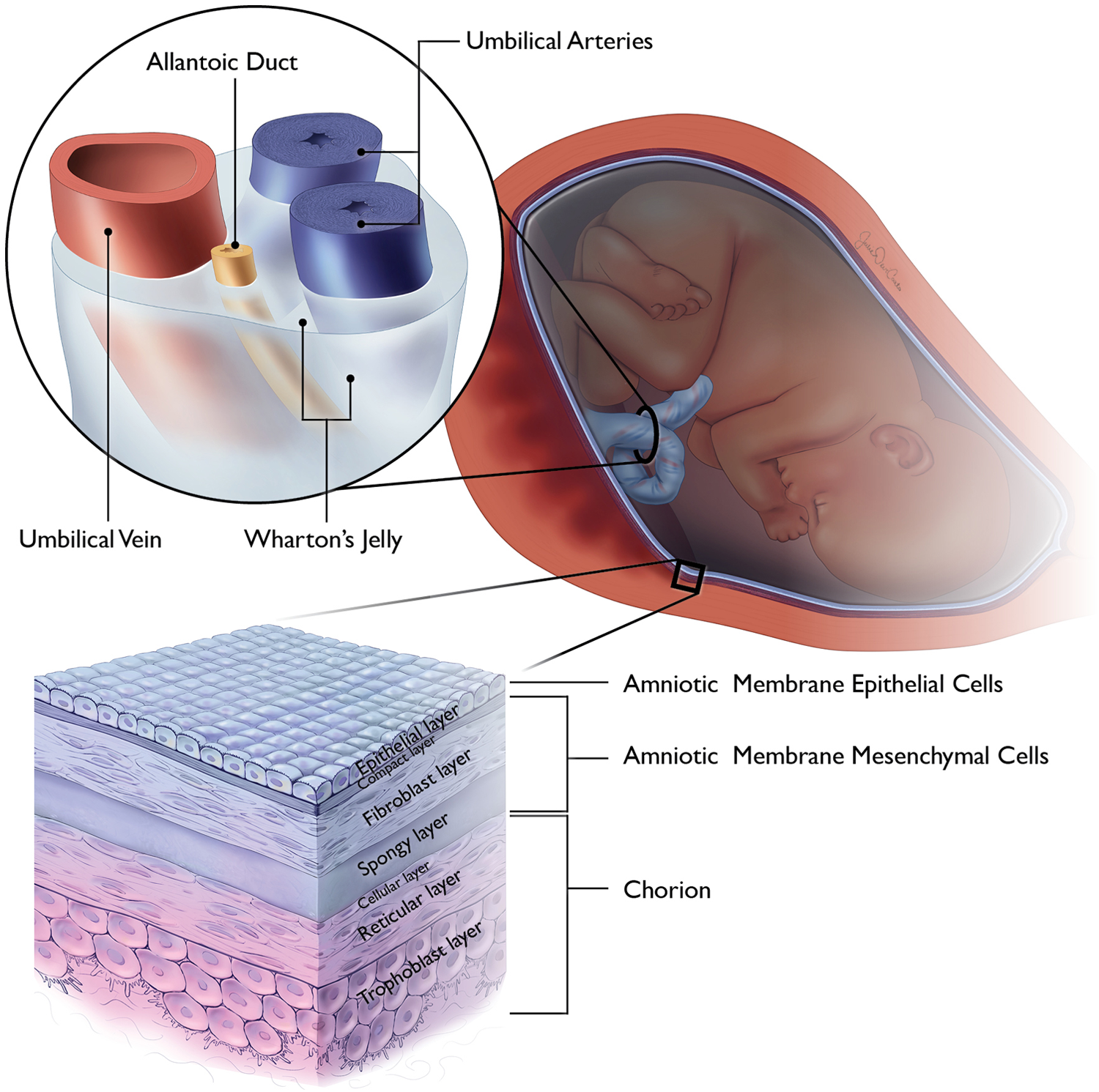
Illustrative image depicting the placenta membranes and the cellular organization of the amnion, chorion, and umbilical cord.
Amnion
The amnion is a thin tissue, derived from the trophoblast that completely surrounds the developing fetus and facilitates fetal nutrition via diffusion. 7,8 The amnion contains 3 distinct histologic layers: the epithelial layer, the basement membrane, and the mesenchymal layer (Figure 1).
The epithelial layer is the innermost layer of the amnion, consisting of a single layer of cuboidal amniotic epithelial cells (AECs). AECs are derived from the epiblast, developing on the eighth gestational day 9 and have been shown to produce basic fibroblast growth factor, epidermal growth factor, keratinocyte growth factor, and hepatocyte growth factor. 8,10 Through the production of these factors, AECs have been shown to promote epithelization, 10 inhibit angiogenesis, 11 inhibit fibroblast activation through the inhibition of transforming growth factor-β, promote neural differentiation, 12 –14 provide immunosuppression via inhibition of both innate and adaptive immune systems, 15 promote tenocyte proliferation, 16 as well as possess the capability for trilineage cell differentiation, or differentiation into all 3 germline lineages. 17
The mesenchymal layer is a vascular layer that abuts the chorion and contains 3 distinct sublayers: the compact, fibroblast, and spongy layers (Figure 1). 8,18 The fibroblast layer provides for the structural integrity via type I and III collagen, arranged in parallel bundles, 18 and contains the embryonic mesoderm derived mesenchymal stromal cells(AMSCs). 8 AMSCs have shown capabilities for trilineage cell differentiation. 17 In addition to a higher proliferative rate than adult-derived MSC sources, 19 AMSCs have been found to promote angiogenesis through the expression of proangiogenic factors 8 and suppress the innate and adaptive immune systems. 15 The spongy layer is abundant in proteoglycans and glycoprotenins, particularly hyaluronic acid, which is thought to serve as a primary inhibitor of transforming growth factor-β, resulting in cessation of scar formation. 20 Additionally, the spongy layer possesses a loose, nonfibrillar collagen network connecting it to the adjacent chorion, 18 which is exploited for tissue separation for various commercial graft products that are isolated amnion.
Combined, AECs and AMSCs have shown a particular capacity for osteogenic and chondrogenic cellular differentiation. 21 Although numerous studies have investigated this osseous and chondral differentiation, the AEC and AMSC cells largely require induction using various mediums or growth factors. 22 –26
Chorion
The chorion is an extra-embryonic entity with a bilayered structure that represents the outermost layer of the placental tissue. Its villous trophoblast area serves as the primary location of nutrient exchange between the mother and developing fetus. 6 As such, it has also been shown to have cross-contamination with maternal cells, present in approximately 30% of chorionic MSCs. 27,28 Chorionic membrane cells have been identified as pluripotent with the capacity for trilineage germ line differentiation, 29,30 but with a decreased capacity compared with other MSC cell sources. 31 In addition, chorionic membrane cells demonstrate immunosuppressive effects as well as promote angiogenesis. 27
Umbilical Cord
The umbilical cord is a unique structure of extra-embryonic origin that connects the fetal and maternal circulatory systems for nutrition and waste exchange. 6 The umbilical cord is composed of the umbilical epithelial exterior, containing connective tissue, termed Wharton’s jelly, and blood vessels. MSCs have been isolated from both the epithelium and Wharton’s jelly 32 –35 ; however, Wharton’s jelly has been found to have the highest concentration of MSC, not just of the umbilical cord, but of all MSC sources. 36 Umbilical cord–derived MSCs (UC-MSCs) have shown potential for multilineage cell differentiation, with a particular capacity for neural differentiation 37 –39 and immunosuppression. 1,40,41
In addition to the umbilical cord tissue, the blood contained within the umbilical vessels has been identified as a source of MSCs, although present in significantly smaller quantity than other sources. 36,42 The predominant stem cell population is CD34 positive hematopoietic stem cells, but this source has also been shown to express characteristics in common with bone marrow MSCs. 43 In addition, umbilical cord blood has also shown potent production of motor-neuron-related markers, making it a prime target for motor nerve regeneration research. 44
Methods
A literature search was conducted to retrieve previous publications regarding the use of placental tissue in various avenues relating to spine surgery. A PubMed search was performed using the terms “Amnion,” “Chorion,” “Amniotic Membrane,” “Umbilical,” and “Umbilical Cord” and “Spinal” or “Spine.” Using this broad search strategy, 4 main categories of clinical application were identified, consisting of intervertebral disc pathology, epidural fibrosis, spinal cord injury, and closure of spinal dysraphism. These 3 categories were individually inserted in a search strategy using PubMed and MEDLINE search engines between 1960 and 2017. Inclusionary criteria consisted of English language articles and investigating the application of human placental tissue for the 4 identified clinical applications. Review articles and non-English articles were excluded. Terminology for search parameters consisted of (1) “Amnion or Amniotic Membrane or Chorion” and (2) “Umbilical or Umbilical Cord,” with each of the 4 clinical applications. Search results are summarized in Table 1. The results and analysis of systematic review, broken down according to subgroup headings, are summarized in Appendix 1 (available in the online version of the article).
Summary of Basic Science Research as It Related to the Various Placenta Tissues and Their Cellular Capabilities.

Epidural Fibrosis
Epidural fibrosis is considered as a cause of continued back pain following decompressive surgery, as well as a factor complicating revision spine surgery. 45 Three articles were identified, investigating the application of amniotic membrane (AM) with and without the adjacent chorion on the development of epidural fibrosis (Table 2). Choi et al 46 investigated the application of irradiated human AM grafts applied to a rat laminectomy model, compared to an untreated laminectomy cohort. Gross observation of surgical sites performed at 1, 3, and 8 weeks following surgery found a decreased overall amount of scarring in the AM cohort with less inflammatory cell infiltration and fibroblast proliferation on histologic examination. Similar findings were reported by Tao and Fan 45 using an adult mongrel dog lumbar laminectomy model, comparing freeze-dried AM, cross-linked AM, autologous free fat, and untreated control. Gross observation and histology examination found decreased scar formation in the AM cohort cross-linked with glutaraldehyde. The freeze-dried AM membrane, interestingly, demonstrated no difference in comparison to the control samples on gross analysis with complete degradation of the graft demonstrated on histologic examination at 12 weeks following implantation. Quantitative analysis of fibroblasts at the surgical site found that the autologous free fat cohort has significantly less fibroblasts than the remaining cohorts, significantly lower than both AM groups.
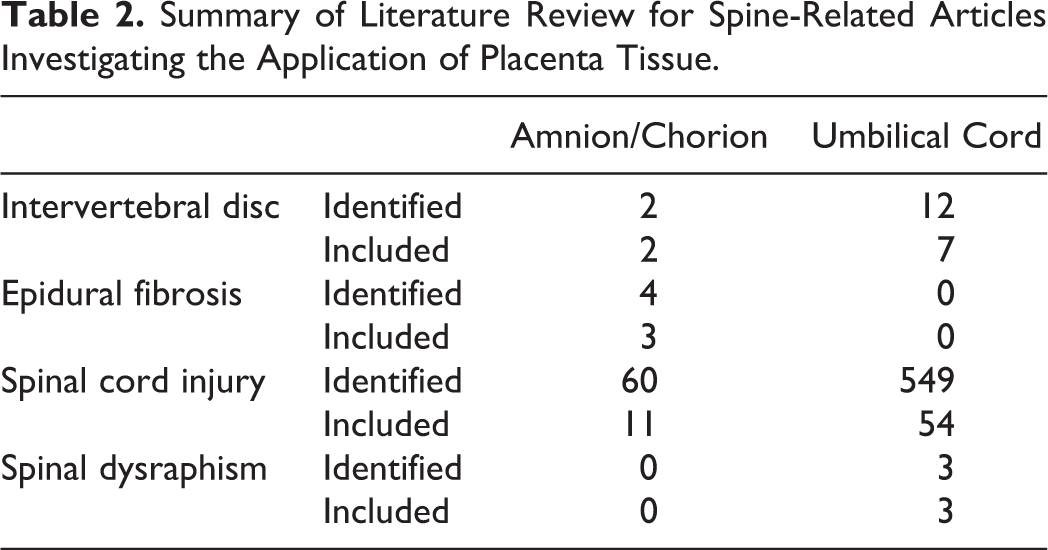
Summary of Literature Review for Spine-Related Articles Investigating the Application of Placenta Tissue.
Subach and Copay 47 were the only authors to report on the clinical application of a dehydrated combined amnion/chorion graft. They reviewed a case series of 5 patients undergoing revision lumbar surgery after implantation of a combined amnion/chorion graft performed during primary transforaminal lumbar interbody fusion. At the time of revision surgery, 80% (4/5) of the patients had easily detachable tissue adjacent to the dura, with the authors concluding that combined amnion/chorion grafts have favorable effects on epidural fibrosis.
Intervertebral Disc Pathology
Low back pain is a pervasive condition, affecting more than 70% of the adult population at least once during their lifetime. 48 Disc degeneration is one progressive etiology that has gained considerable attention in therapeutic attempts to facilitate regeneration. 49 Literature review identified one article investigating the in vitro application of placental tissue and 7 articles investigating umbilical cord blood and tissue for intervertebral (IV) disc repair (Table 2). Ni et al 50 found that placental-derived MSCs could be facilitated toward nucleus pulposus-like cell differentiation with increased proliferation when cultured under hypoxic conditions, suggesting it as a possible agent for IV disc repair. Similar cell culture studies were identified for umbilical cord blood and tissue, indicated inducible proliferation of nucleus pulposus-like cells, 51,52 with production of proteoglycan-rich extracellular matrix (ECM) in a chondrocyte-like phenotype. 53 Beeravolu et al 54 reported on the in vivo application of umbilical cord MSCs and chondroprogenitor cells (CPGs) derived from the umbilical cord MSCs to damaged IV discs in a rabbit model. The CPGs-treated animals demonstrated significant improvement in histologic appearance, as well as ECM protein and glycosaminoglycan (GAG) content production while having significantly higher expression of nucleus-pulposus specific markers.
Tam et al 55 compared the intravenous and intradiscal delivery of multipotent stem cells derived from umbilical cord blood in a damaged IV disc mouse model. Analysis performed 14 weeks after treatment found limited homing ability of the implanted cells without engraftment or expansion of the cells. Direct injection was found to better preserve disc height with a slight decrease in histologic degeneration.
Leckie et al 56 performed a blinded, randomized, placebo-controlled in vivo rabbit study using umbilical cord tissue–derived cells in a degenerative disc model. Animal were subdivided into 4 groups, un-punctured control, punctured without treatment, and punctured with umbilical cord tissue injection with or without a hydrogel carrier. Serial magnetic resonance imaging (MRI) was performed out to 12 weeks following treatment with histologic examination performed at 12 weeks. There was no difference in the MRI analyses between the treatment groups with qualitative analysis showing less degeneration overall when compared with the untreated punctured group. Histologically, treated IV discs showed some improvement in cellularity and disc architecture in comparison to the untreated punctured cohort but were distinctly different from the un-punctured control cohort.
Investigating the application of these grafts when the disc degeneration is beyond potential for repair, Goldschlager et al 57 applied AECs to an ovine model of cervical discectomy and fusion with an interbody cage. They found that when AECs were combined with a hydroxyapatite-tricalcium phosphate graft, there was a significant negative effect on the fusion rate, with a 0% fusion rate at 3 months following surgery.
Two clinical studies were identified that investigated the application of placental tissue for discogenic pathology (Table 2). Pang et al 49 reported the outcomes of 2 patients with chronic discogenic low back pain who underwent treatment with transplantation of UC-MSCs with 2-year follow-up. Visual analog pain scale measurements were found to significant decrease at 2-year follow-up with an improvement in function according to assessment with the Oswestry Disability Index (ODI). Anderson et al 58 performed a prospective, randomized controlled trial in 80 subjects undergoing lumbar microdiscectomy with or without a cryopreserved amniotic tissue graft applied to the annular defect. Patients were monitored for 24 months using functional outcome measures and visual analog pain scales, as well as for the incidence of reherniation. They found that there was significant greater improvement in mean ODI scores for patients in the cryopreserved amniotic tissue cohort as well as improved Short Form-12 physical component scores. Overall, there were no reherniations in the amniotic tissue cohort, compared with 3 in the control group and 2 control patients requiring subsequent fusion for persistent symptoms.
A review of ongoing clinical trials (www.clinicaltrials.gov, accessed August 31, 2017) reviews that there is one current trial investigating the 5-year postoperative outcomes of patients undergoing discectomy with application of cryopreserved amniotic membrane and umbilical cord grafts. Additionally, there are 4 trials investigating the use of an amniotic membrane–derived allograft combined with various bone graft products for application in lumbar and cervical spine fusion procedures.
Spinal Dysraphism Closure
Spinal dysraphism closure, performed in utero, has proven to significantly decrease morbidity and mortality in comparison to postnatal repair. 59 Grafts are occasionally required to facilitate dural closure with several graft subtypes described in the literature. 60 –62 Papanna et al 60 reported on the application of cryopreserved umbilical cord patch during in utero spina bifida repair in a sheep model. In comparison to a biocellulose film adhesive, umbilical cord patch was found to be significantly superior for facilitating closure and subsequent healing, with a larger spinal cord area and greater number of preserved anterior horn cells. In a subsequent study, Papanna et al 63 reported on the neurological outcomes in a separate cohort of umbilical cord patched sheep and compared with normal control and untreated spina bifida cohorts. The cryopreserved umbilical cord patch cohort was found to have improved neurologic outcomes with improved Texas Spinal Cord Injury Scale scores and improved bladder control.
A single clinical study was reported on the use of cryopreserved human umbilical cord for in utero myeloschisis repair in 2 fetuses in which primary closure was unattainable. 64 Both pregnancies were uncomplicated following midgestation repair, with births occurring at 37 weeks by planned cesarean delivery. Both repair sites were intact without cerebrospinal fluid leakage, and normal function of the lower extremities.
Spinal Cord Injury
The role of regenerative interventions has expanded in recent years with regard to treatment of patients with spinal cord injuries (SCI). Placental tissues have been extensively investigated with regard to their role in facilitating neurologic recovery given their neurotrophic capabilities. 12 –14,37 –39,44 AECs and umbilical cord tissue and cord blood have been particular targets in this line of research. In vivo animal models have shown that AECs can promote neural cell differentiation, 65 reduce secondary neural damage associated with inflammation and apoptosis associated with SCI, 66 modulate spinal cord microglia activity to suppress mechanical allodynia, 67 promote remyelination of nerve fibers and promote sprouting of nerve fibers, 68 and improve functional recovery. 68 –70
Umbilical cord tissue has similarly shown a capacity to facilitate axonal regeneration, 71 increase the number of surviving neurons, 72,73 minimize allodynia and hyperalgesia, 74 alter the local SCI microenvironment to minimize IL-1 expression, 75 and improve functional recovery. 38,71,73 –77 These physiologic effects can additionally be accentuated with the co-administration of various growth factors, to include brain-derived neutrophic factor, 71 glial cell-line neutrophic factor, 72 and neurotrophin-3. 78
Umbilical cord blood is an additional source of mesenchymal and multipotent stem cells that has shown superiority in animal models for SCI. Ryu et al 73 compared the effect of bone marrow–derived, adipose-derived, umbilical cord tissue, and umbilical cord blood MSCs on neural regeneration in a canine SCI model. All MSCs groups were found to have significant improvement in locomotion, with an increase in the number of surviving neurons and neurofilament-positive fibers. Although there was no difference in functional outcome, umbilical cord blood–derived MSCs induced significant more nerve regeneration, and anti-inflammatory activity with reduced IL-6 and COX-2 levels. In contrast to UC-MSCs, umbilical cord blood has shown improved release of neutrotrophic growth factors, 79 –86 downregulation of caspase-3 extrinsic pathway, Fas, and other apoptotic genes to produce an anti-apoptotic milieu at the injury site, 87,88 increase residual white matter, 89 upregulate matrix metalloprotease-2 to reduce glial scar formation, 86,90 and facilitate oligodendricyte and neural cell differentiation. 91
Clinical studies have attempted to extrapolate the preclinical data. Liu et al 92 investigated the effect of a single or repeated intrathecal injection of UC-MSC in 22 patients with mixed cord–level lesions treated at an average of 56 months following injury (range 2-204 months). No patient with a complete cord injury demonstrated any treatment response, while 81% of patients with an incomplete injury demonstrated a treatment effect, defined as any improvement in American Spinal Injury Association (ASIA) sensory or motor score. No patient reported an adverse effect following treatment.
Cheng et al 93 investigated the use of UC-MSCs in thoracolumbar SCI patients, using a cohort of 34 patients subdivided into a control group of rehabilitation only and a UC-MSC transplantation group, receiving 2 treatment cycles. Patients in the UC-MSC group showed improved urodynamic parameters with 70% of patients reporting a neurologic improvement. Zhao et al 94 combined UC-MSC with a collagen scaffold that was surgically implanted in 8 patients with chronic SCI after undergoing surgical scar resection with clinical observation for 1 year. Patients demonstrated expansion of sensation and motor-evoked potential responsive area, improved finger control, enhanced truncal stability, and autonomic neural function recovery without developing any adverse effects.
Yao et al 95 performed a controlled cohort analysis of either intravenous or intrathecal application of umbilical cord blood administration in 25 patients with chronic (>6 months) SCI, compared with 25 control patients treated with traditional rehabilitation alone. They did find that 24% of treated patients demonstrated improved urinary control and 36% had improved somatosensory evoked potentials, despite a lack of difference in ASIA score when compared to pretreatment data. Zhu et al 96 reported the results from their Phase I-II clinical trial investigating the intrathecal application of umbilical cord blood of varying dosages in 28 patients with chronic SCI, C3-T11 level injuries. There was a lack of treatment uniformity (vast difference in MSC dosages) and a mixture in adjuvant treatment (methylprednisolone, lithium); 5 patients converted from complete to incomplete SCIs (2 sensory, 3 motor) with a significant improvement in ability to ambulate 10 meters (7% vs 75%) and improvement in urinary and bowel control (0% vs 60%).
A review of ongoing clinical trials (www.clinicaltrials.gov, accessed August 31, 2017) identified one study investigating the application of UC-MSCs in patients with spinal cord injury that is currently enrolling patients, with 3 recently completed clinical trials.
Conclusions
Human-derived placental tissues have been identified as a source of pluripotent cells, with promising potential for spinal surgical applications, most especially with traumatic SCIs. Specific tissue effects can be expected, understanding the underlying anatomical and biochemical differences of the various subtypes of placental tissues. However, there is currently no evidence to support the clinical application of placental tissues in spine surgery. High-quality research studies are needed to investigate the potential use of placental tissue in spine surgery.
Supplemental Material
Supplemental Material, Placenta_Appendix - The Science and Clinical Applications of Placental Tissues in Spine Surgery
Supplemental Material, Placenta_Appendix for The Science and Clinical Applications of Placental Tissues in Spine Surgery by K. Aaron Shaw, Stephen A. Parada, David M. Gloystein, and John G. Devine in Global Spine Journal
Footnotes
Authors’ Note
The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or reflecting the views of the Department of Defense or the US government. The authors are employees of the US government. This work was prepared as part of their official duties and as such there is no copyright to be transferred.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.