
Abstract
Study Design:
Systematic review.
Objective:
To perform a systematic review to evaluate the utility of magnetic resonance imaging (MRI) in patients with acute spinal cord injury (SCI).
Methods:
An electronic search of Medline, EMBASE, the Cochrane Collaboration Library, and Google Scholar was conducted for literature published through May 12, 2015, to answer key questions associated with the use of MRI in patients with acute SCI.
Results:
The literature search yielded 796 potentially relevant citations, 8 of which were included in this review. One study used MRI in a protocol to decide on early surgical decompression. The MRI-protocol group showed improved outcomes; however, the quality of evidence was deemed very low due to selection bias. Seven studies reported MRI predictors of neurologic or functional outcomes. There was moderate-quality evidence that longer intramedullary hemorrhage (2 studies) and low-quality evidence that smaller spinal canal diameter at the location of maximal spinal cord compression and the presence of cord swelling are associated with poor neurologic recovery. There was moderate-quality evidence that clinical outcomes are not predicted by SCI lesion length and the presence of cord edema.
Conclusions:
Certain MRI characteristics appear to be predictive of outcomes in acute SCI, including length of intramedullary hemorrhage (moderate-quality evidence), canal diameter at maximal spinal cord compression (low-quality evidence), and spinal cord swelling (low-quality evidence). Other imaging features were either inconsistently (presence of hemorrhage, maximal canal compromise, and edema length) or not associated with outcomes. The paucity of literature highlights the need for well-designed prospective studies.
Keywords
Introduction
Imaging of the spine is an essential part of the early management of the polytrauma patient. 1 Most major trauma centers have a variety of imaging modalities available for acute spinal trauma. The choice of modality is determined by the need to evaluate bony, ligamentous, soft tissue, and neural elements. In the acute setting, imaging should provide a rapid and accurate assessment of spinal stability, as well as guide clinical management. Current trauma protocols rely heavily on computed tomography (CT), 1 as it allows for efficient evaluation of the head, body, and spine and identifies most injuries. High-quality imaging, however, cannot replace a good clinical examination, but rather should supplement and confirm findings of the primary and secondary trauma survey.
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) is not routinely used for initial evaluation of the trauma patient. MRI is usually performed after initial clinical and radiological (CT or X-rays) evaluations, when further delineation of neural structures, such as the spinal cord, nerve roots, or brachial plexus, is required due to the presence of a neurological deficit or the suspicion of a structural problem such as a ligamentous injury. Conventional MRI, including T1- and T2-weighted imaging, provides excellent views of the soft tissue and can readily identify features of spinal cord compression such as intervertebral disc herniation and epidural hematoma. 1,2 Although CT is often able to detect pre- and paravertebral soft tissue swelling, MRI provides a more reliable detection of traumatic injury. Short-tau inversion recovery sequences produce fat-suppressed images that better delineate ligamentous injuries, which can cause mechanical instability of the spinal column. T2-weighted MRI is ideal for demonstrating intramedullary spinal cord edema and hemorrhage; high signal intensity indicates edema, while a focus of acute hemorrhage has low, heterogeneous signal intensity. 3 Gradient echo (GRE) and susceptibility weighted imaging (SWI) are highly sensitive for hemorrhage and can also identify microhemorrhage consistent with cord contusions.
The use of MRI for the initial evaluation of trauma patients is limited largely by long scanning times. Although monitoring is available in many MRI suites, it is not advised to keep trauma patients supine and flat for extended periods of time as a result of pain and hemodynamic instability. Critically ill trauma patients may also have concomitant head and chest injuries that may result in increased intracranial pressure and decreased ventilation during MRI acquisition. 4 The use of a small number of specific sequences with appropriate coils can reduce scanning time. Current guidelines for the use of MRI in acute spine trauma are based on limited available data. 1
The primary goal of this study was to perform a systematic review of the literature to (1) assess MRI features that may affect clinical decision making and outcomes in patients with acute SCI; (2) determine if baseline MRI characteristics can predict neurologic, functional, and patient-reported outcomes; (3) evaluate the safety of MRI in this population; and (4) characterize the cost-effectiveness of MRI in acute SCI.
To accomplish this goal, we aimed to answer the following key questions (KQ) in adult patients with acute traumatic SCI:
Materials and Methods
Electronic Literature Search
We conducted a systematic search of PubMed/MEDLINE, EMBASE, the Cochrane Collaboration Library, and Google Scholar for literature published through May 12, 2015. Citations with abstracts of human studies were considered for inclusion, with no other limits (including language) applied to the search. Reference lists of included studies as well as pertinent reviews were systematically checked to identify additional articles. A summary of the search strategy is presented in the supplemental material (available in the online version of the article).
The search strategy included the use of controlled vocabulary (MeSH terms) as well as keywords. Terms specific to traumatic spinal cord injuries and central cord syndrome as well as those related to MRI and DTI were used. For KQ1, we sought to identify comparative studies that assessed if presurgical MRI influenced management strategies and, consequently, neurologic, functional, patient-reported, and safety outcomes. For KQ1 and KQ4, we only included studies that compared specific treatment strategies (eg, emergency decompressive surgery), outcomes (KQ1), or cost-effectiveness data (KQ4) between groups that did and did not receive presurgical MRI. For KQ2 and KQ3, we attempted to identify prospective or retrospective cohort studies that evaluated lesion characteristics, pattern, and/or length on conventional MRI (KQ2) or DTI (KQ3) as predictors of neurologic change/recovery (eg, Frankel grade, American Spinal Injury Association [ASIA] impairment scale [AIS]), functional outcomes (eg, Functional Impairment Measure [FIM]), patient-reported outcomes (eg, pain), and safety (eg, complications and adverse events). For KQ4, we sought comparative full-economic studies that evaluated the cost-effectiveness of presurgical MRI in patients with acute SCI. Meeting abstracts/proceedings, white papers, editorials, narrative reviews, case reports, nonclinical and animal studies, and studies with less than 10 subjects in total (KQ2 and KQ3) or per group (KQ1 and KQ4) were excluded. Studies on patients with cord compression/spinal cord injuries due to degenerative disease (eg, cervical spondylotic myelopathy, spinal stenosis), tumor, or hematoma were also excluded. The PICO (Patients, Intervention, Comparator and Outcomes) and PPO (Patients, Prognostic Factors and Outcomes) tables provide additional information on inclusion/exclusion criteria (Tables 1 and 2).
Data Extraction
The full texts of potential articles were reviewed by 2 independent investigators (DJF, ACS) to obtain the final collection of included studies. From the included articles, the following data was extracted: study design; patient demographics; inclusion and exclusion criteria; baseline population/disease characteristics; follow-up duration and the rate of follow-up (if reported or calculable); baseline MRI characteristics and assessment; timing of MRI in relation to injury and intervention (if applicable); treatment groups (KQ1); reported information on specific treatment decisions (KQ1); neurological, functional, safety, and quality of life outcomes (KQ1, KQ2, and KQ3); prognostic factors evaluated (KQ2 and KQ3); association between prognostic factors and reported outcomes (KQ2 and KQ3); and cost-effectiveness data (KQ4).
Study Quality and Overall Strength of Body of Literature
Each article was independently critically appraised and evaluated for risk of bias by at least 2 reviewers (DJF, ACS) using criteria set by The Journal of Bone and Joint Surgery, American Volume 5 for prognostic and therapeutic studies, and modified to delineate criteria associated with methodological quality and risk of bias based on recommendations made by the Agency for Healthcare Research and Quality (AHRQ). 6 This appraisal system accounts for features of methodologic quality and important sources of bias by combining epidemiologic principles with characteristics of study design. 7,8 (See Supplemental Material for study ratings; available in the online version of the article.) Any disagreement among the reviewers was resolved through discussion.
The overall quality (strength) of the body of evidence with respect to each outcome was determined based on precepts outlined by the Grades of Recommendation Assessment, Development and Evaluation (GRADE) Working Group 9,10 and recommendations made by AHRQ. 6 Additional qualitative analysis was performed according to AHRQ-required (risk of bias, consistency, directness, precision) and additional domains (dose-response, strength of association, publication bias). 11 In general, risk of bias was determined when evaluating each individual article as described above.
For outcomes related to KQ1, the initial quality of the overall body of evidence was considered “High” for randomized controlled trials and “Low” for observational studies. The body of evidence could be downgraded 1 or 2 levels based on the following criteria: (1) risk of bias (study limitations), (2) inconsistency of results, (3) indirectness of evidence, (4) imprecision of the effect estimates (eg, wide confidence intervals), or (5) failure to provide an a priori statement of subgroup analyses. The body of evidence for observational studies could be upgraded 1 or 2 levels (if no serious risk of bias) based on the following criteria: (1) large magnitude of effect, (2) dose-response gradient, or (3) if all plausible biases would decrease the magnitude of an apparent effect. For KQ2 and KQ3, the initial quality of the evidence was considered “High” if the majority of prognostic studies had low or moderately low risk of bias, and “Low” if the majority had moderately high or high risk of bias. The body of evidence could be downgraded 1 or 2 levels based on the following criteria: (1) inconsistency of results, (2) indirectness of evidence, (3) imprecision of the effect estimates (eg, wide confidence intervals, small sample size), or (4) failure to provide an a priori statement of subgroup analyses. The body of evidence could be upgraded based on the criteria specified above. Two senior systematic review methodologists rated and discussed the overall quality of evidence.
The final overall strength of the body of literature expresses (1) our confidence that the effect size lies close to the true effect and (2) the extent to which the effect is believed to be stable based on the adequacy of or deficiencies in the body of evidence. 10 An overall strength of “High” means that we are very confident that the true effect lies close to that of the estimated effect. A “Moderate” rating means that we are moderately confident in the effect estimate; the true effect is likely to be close to the estimated effect, but there is a possibility that it is substantially different. An overall strength of “Low” means that our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate. Finally, a rating of “Very Low” means that we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimated effect. In addition, this rating may be used if there is no evidence or it is not possible to estimate an effect.
Data Synthesis and Analysis
For KQ1, results and comparative statistics regarding treatment decisions and neurologic outcomes were reported. For KQ2, there was variability in the measurement and reporting of prognostic factors and outcomes. To operationalize outcomes and discern patterns of association, we combined outcomes into 2 categories: neurologic and functional. The latter category included 2 patient-reported outcomes (self-reports of manual dexterity and dysesthetic pain) that may ultimately affect function. Furthermore, authors generally did not report the magnitude of association (eg, effect size estimates with confidence intervals) between predictive characteristics and outcomes, but rather presented P values and/or stated whether there was a significant association. We reported the association between the prognostic factor and the specific outcome (no association, association with a negative outcome, or association with a positive outcome).
Results
Study Selection
The literature search yielded 796 potentially relevant citations that were evaluated against a priori inclusion/exclusion criteria (Tables 1 and 2; Figure 1). After title/abstract review, 741 were excluded, most of which reported on bony fractures or other acute trauma without SCI. Review of the reference lists of included studies as well as relevant reviews did not yield any additional relevant citations. Among the 55 remaining articles, 47 were excluded after review by 2 reviewers. The primary reasons for exclusion were (1) failure to control for confounding factors (especially baseline neurologic status) via multivariate analysis or other statistical methods and (2) the lack of longitudinal information on neurologic or functional recovery.
PICO Table Summarizing Inclusion and Exclusion Criteria for Key Questions 1 and 4.
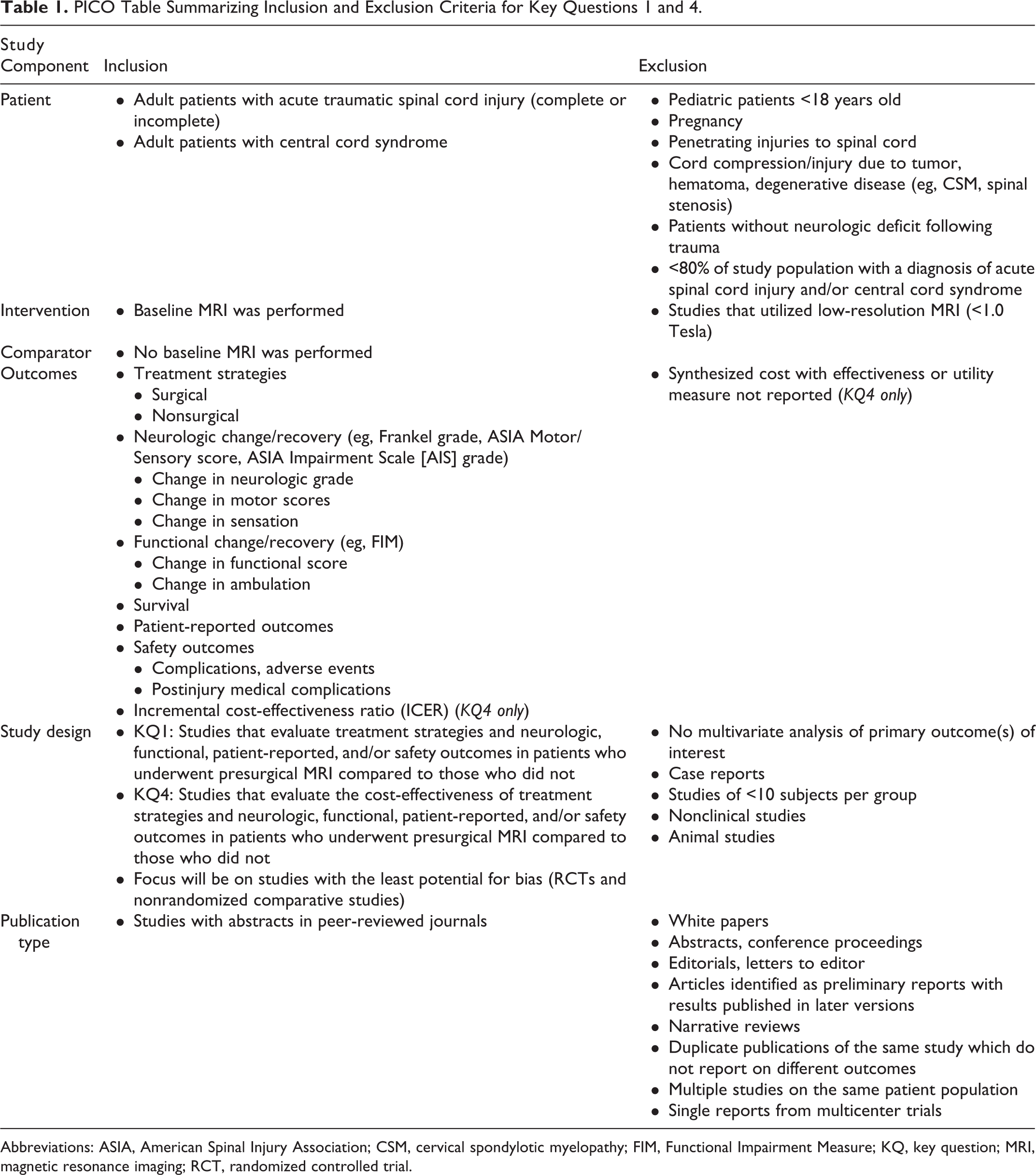
Abbreviations: ASIA, American Spinal Injury Association; CSM, cervical spondylotic myelopathy; FIM, Functional Impairment Measure; KQ, key question; MRI, magnetic resonance imaging; RCT, randomized controlled trial.
PPO Table Summarizing Inclusion and Exclusion Criteria for Key Questions 2 and 3.
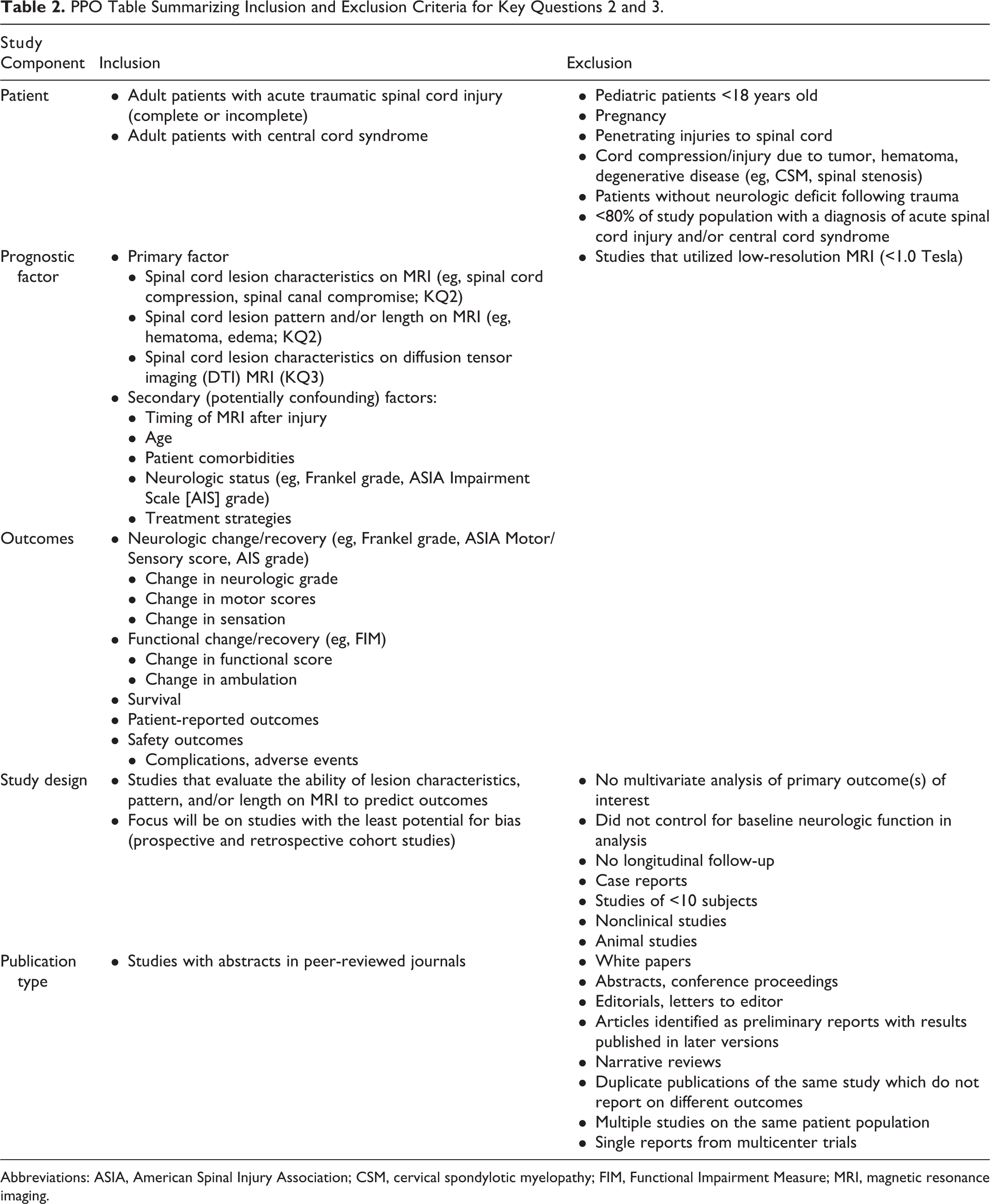
Abbreviations: ASIA, American Spinal Injury Association; CSM, cervical spondylotic myelopathy; FIM, Functional Impairment Measure; MRI, magnetic resonance imaging.
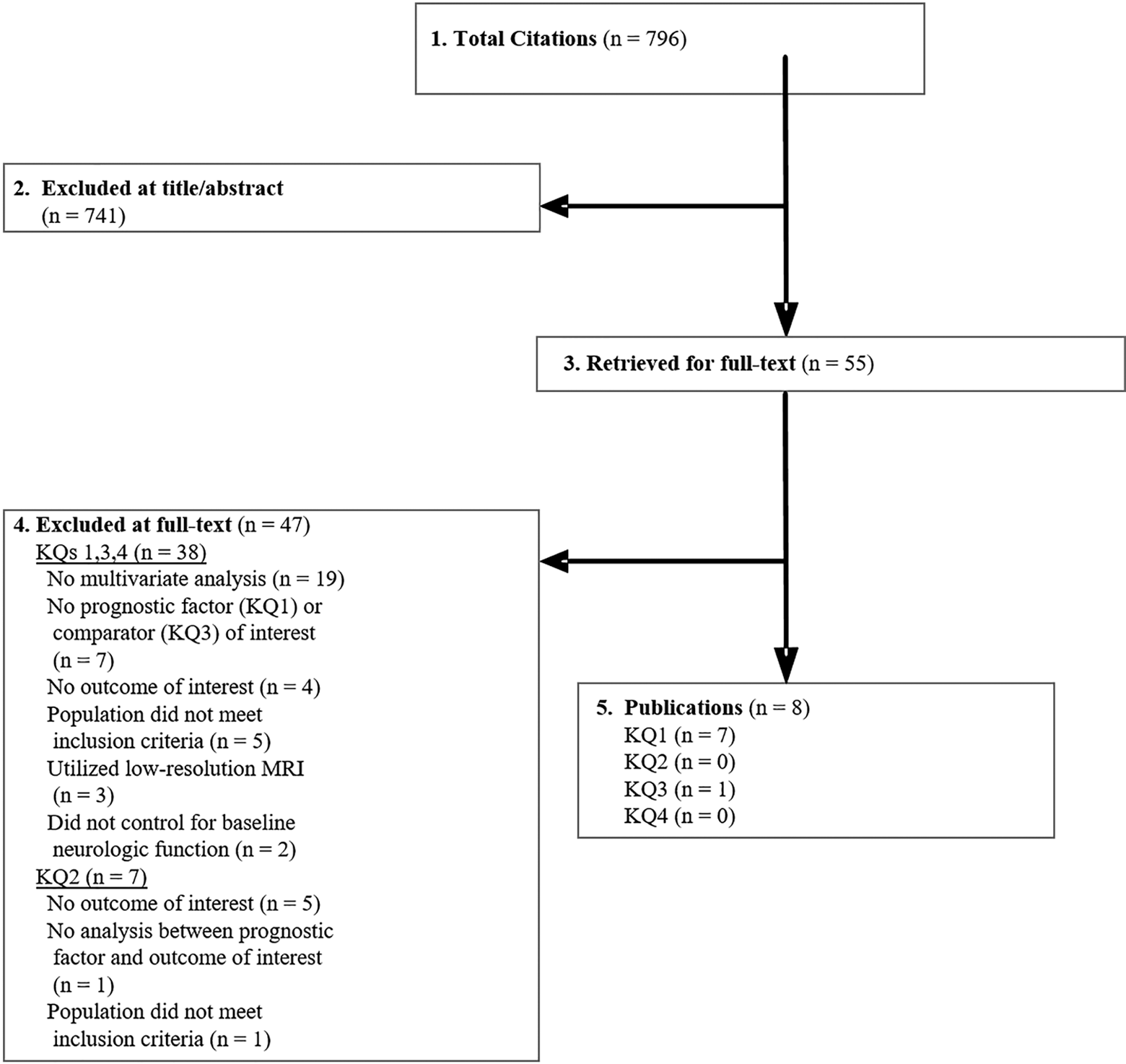
Flow chart showing results of literature search.
For studies evaluating the impact of MRI on clinical decision making, the primary reason for exclusion was the lack of a comparison group with patients that did not receive MRI (KQ1). Additional reasons for exclusion were (1) the absence of outcomes of interest (KQ1, KQ2), (2) the lack of a multivariate analysis or other statistical methods to control for important confounders (particularly baseline neurologic status; KQ2), and (3) no assessment of MRI prognostic factors (KQ2, KQ3). We identified a single study for KQ1 that compared treatment decisions and neurological outcomes between patients with and without pretreatment MRI; 7 studies for KQ2 that evaluated important MRI predictors of outcomes; and no studies relevant for either KQ3 or KQ4. Details of excluded articles are provided in the Supplemental Material (available in the online version of the article).
The Influence of Baseline MRI on Treatment Strategy(ies) and SCI Outcomes
One prospective cohort study 12 (moderately high risk of bias) evaluated the effect of pretreatment MRI on neurological outcome (Frankel grade). Table 3 summarizes the characteristics of this study, while Table 4 reports the influence of a baseline MRI on neurologic outcomes.
KQ1 Characteristics of Studies Evaluating the Impact of MRI on Clinical Decision Making and Neurologic, Functional, Pain, and/or Safety Outcomes Compared to No MRI.
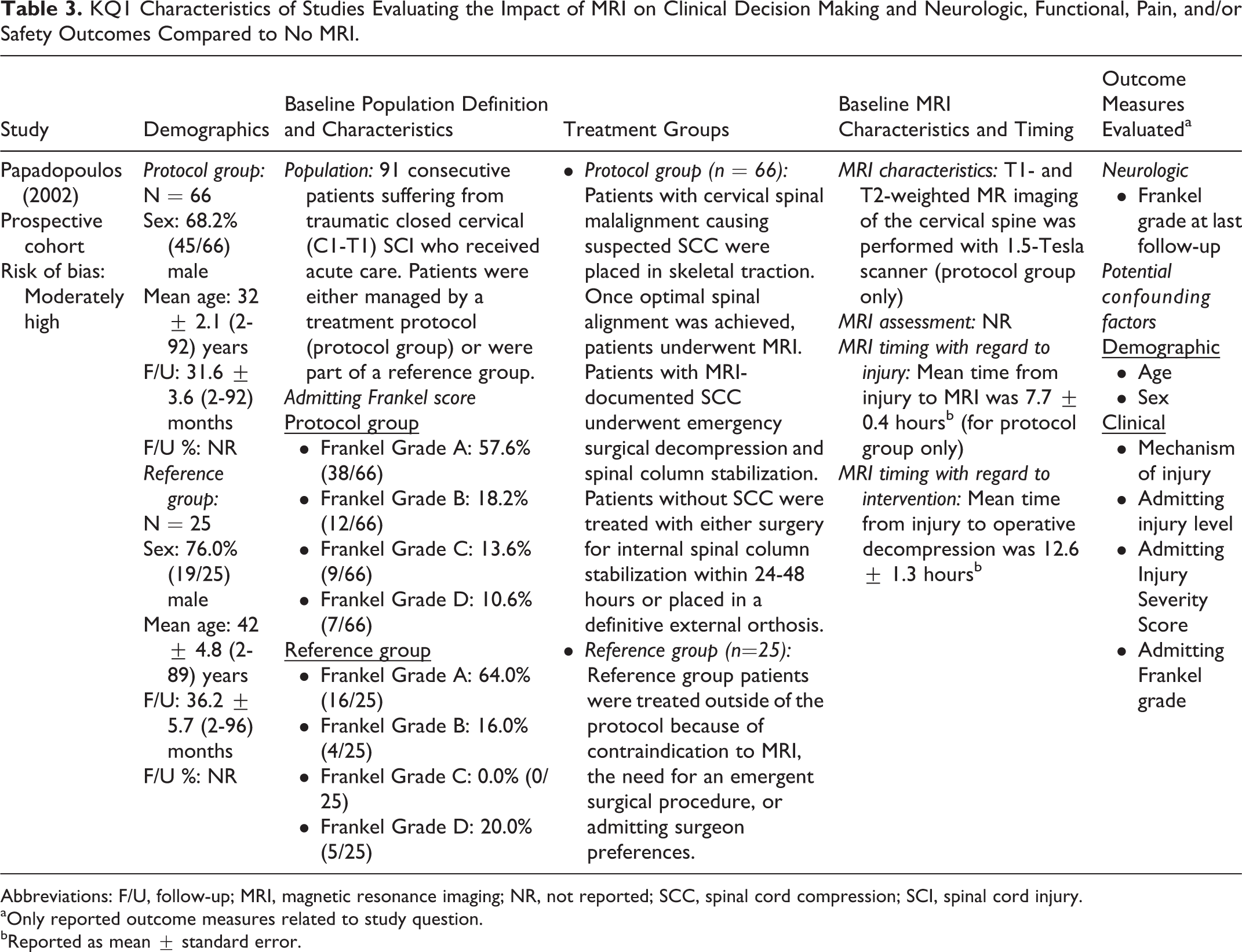
Abbreviations: F/U, follow-up; MRI, magnetic resonance imaging; NR, not reported; SCC, spinal cord compression; SCI, spinal cord injury.
aOnly reported outcome measures related to study question.
bReported as mean ± standard error.
The Impact of Baseline MRI on Treatment Strategies and Neurologic, Functional, and Safety Outcomes in Patients With Acute Spinal Cord Injury.
Abbreviations: MRI, magnetic resonance imaging; NR, not reported.
a P value reported by the authors based on results of multivariate regression analysis that accounted for potential confounders (age, sex, mechanism of injury, admitting injury level, admitting Injury Severity Score, admitting Frankel grade).
bPatients in the Protocol group improved 7/10 of a Frankel grade more than patients in the Reference group.
Papadopoulos et al reported on 91 consecutive patients suffering from traumatic closed cervical (C1-T1) SCI. 12 Sixty-six (72.5%; protocol group) acute SCI patients were managed according to a decision-making protocol (MRI-protocol group) in which the MRI results were used to decide on emergency surgical decompression. This study reported that MRI resulted in no adverse events in all 66 patients and identified ongoing cord compression in 34/66 (51.5%) patients receiving MRI, leading to surgical treatment (mean 9.6 hours after hospital arrival, 13.4 hours postinjury). MRI also identified anterior spinal cord compression (disc herniation, epidural hematoma, malalignment, or bone fragments) in 16/66 patients (24.2%), leading to an anterior surgical approach. The remaining 25 patients (27.5%; reference group) were not managed according to the protocol because of a contraindication to performing MRI, the need for an emergent surgical procedure, or “specific surgeon bias regarding the futility of emergent treatment.” These criteria for group assignment indicate a strong potential for selection bias. The MRI-protocol group was 68.2% (45/66) male with a mean age of 32 ± 2.1 (range 2-92) years, while the reference group was 76.0% (19/25) male with a mean age of 42 ± 4.8 (range 2-89) years. The neurologic follow-up interval for patients in the protocol group was on average 31.6 ± 3.6 (range 2-92) months, while patients in the reference group had a mean follow-up of 36.2 ± 5.7 (range 2-96) months. Unfortunately, details regarding management for the reference group were not reported, and thus no direct comparisons could be made between the groups regarding the impact of MRI on treatment decisions.
The effect of acquiring a baseline MRI (and treatment protocol) was evaluated in a linear regression analysis that adjusted for baseline Frankel grade, age, sex, mechanism of injury, admitting injury level, and admitting Injury Severity Score. Patients in the MRI-protocol group, on average, had an improved Frankel grade compared to those in the reference group (0.7 of a Frankel grade, P < .006). Fifty percent of the MRI-protocol group experienced an improvement in Frankel grade, compared to 24% of the reference group. Eight patients (12%) in the MRI-protocol group improved from a motor-complete injury to independent ambulation, whereas no patients in the reference group patients achieved this improvement.
Spinal Cord Lesion Characteristics, Pattern, and Length Identified on Baseline MRI as Predictors of SCI Outcomes
Table 5 summarizes the characteristics of the included prognostic studies. Of these, 4 prospective cohort studies 13 –16 and 1 retrospective cohort study 17 were considered to have moderately low risk of bias, and 2 retrospective cohort studies 18,19 were considered to have moderately high risk of bias. All studies controlled for baseline neurologic status in multivariate models and followed populations for the primary outcome(s) of interest. One included study (Selden et al) reported the importance of baseline neurological status and various MRI findings in predicting neurological outcomes; however, model details were not provided and results were only assumed to be multivariate.
Across studies, there was variability in the reporting and measurement of prognostic factors and outcomes. Adjusted effect sizes and/or confidence intervals describing the magnitude of association between the predictive factor(s) and outcome were rarely reported. Only a single study 17 reported a follow-up of >80% of subjects. One study 13 compared findings in patients with complete SCI to those with incomplete SCI and also performed a post hoc subgroup analysis in only patients with complete SCI.
Across the included studies, the majority of the patient population was male (65.5% to 87.5%) with a wide range of mean ages (29-58 years). Four studies limited their population to patients with cervical SCI. 13,14,18,19 MRI was performed within 3 days of injury in most studies, with one reporting a median of 8 days (range 5-12 days). The timing from MRI to intervention was inconsistently reported. Follow-up time ranged from 1 to 74 months.
KQ2 Characteristics of Studies Discussing MRI Predictors of Neurologic, Functional, Pain, and/or Safety Outcomes.
Abbreviations: ASIA, American Spinal Injury Association; CCS, central cord syndrome; CT, computed tomography; F/U, follow-up; MCC, maximum canal compromise; MSCC, maximum spinal cord compression; NR, not reported; MR, magnetic resonance; MRI, magnetic resonance imaging; NASCIS, National Acute Spinal Cord Injury Study; NR, not reported; SCI, spinal cord injury.
aOnly reported outcome measures related to study question.
bAarabi (2011): MCC = {1 − Di/[1/2(Da + Db)]} × 100, where Di is the midsagittal diameter of the spinal canal at the point of maximum compression, Da is the diameter of the spinal canal one segment above the highest level of spinal stenosis, and Db is the diameter of the spinal canal one segment below the lowest level of spinal stenosis. MSCC = {1 − di/[1/2(da + db)]} × 100, where da is the diameter of the spinal cord at a normal segment above the highest level of spinal stenosis, db is the diameter of the spinal cord one segment below the lowest level of stenosis, and di is the diameter of the spinal cord at the level of maximum stenosis. Manual dexterity level was defined as the patient’s own perception of dexterity and skill in the following tasks: (1) using a keyboard, (2) playing a musical instrument, (3) buttoning his/her shirt, (4) grooming, and (5) writing. Dysesthetic pain level was a subjective rating on a 0 to 10 analog scale.
cFlanders (1996): Satisfactory quality rating was defined on a sagittal T1-weighted spin echo (or the combination of sagittal T2-weighted fast spin-echo acquisition and sagittal gradient-echo) sequence.
dFlanders (1996): Extremity motor function was assessed by testing key individual muscles in the upper and lower extremities. Each muscle received a score of 0 to 5 for a total possible motor index score of 50 for upper extremity function and 40 for lower extremity function. Minimally useful motor function in an individual muscle was defined as a score of 3 or better on the 5-point manual muscle test. A score of 3 represents the ability for active movement with a full range of motion against gravity.
eMiyanji (2007): MCC/MSCC was defined as described by Fehlings MG, Rao SC, Tator CH, et al. The optimal radiologic method for assessing spinal canal compromise and cord compression in patients with cervical spinal cord injury. Part II: results of a multicenter study. Spine. 1999;24(6):605-613. Soft-tissue injury was defined as an increased signal intensity of the perivertebral tissues on T2-weighted images. Spinal cord lesion length was defined as the distance between the most cephalic and the most caudal extent of the cord signal intensity change on T2-weighted images.
fShepard (1999): Pin prick/light touch score was determined as follows: 29 spinal cord segments were tested bilaterally for response to pin prick and light touch, each of which were scored at 1 = absent, 2 = dysfunctional, and 3 = normal. Sensory scores ranged from a total score of 87 (normal response) to a score of 29 (no response in any segment). Responses for the right side were summed, unless some cord segments could not be tested, in which case responses for the left side were used. Motor function score was determined by bilaterally measuring fourteen muscle roots, with 0 = no contraction, 1 = flicker/trace of contraction, 2 = active movement without antigravity, 3 = active movement with antigravity, 4 = active movement against resistance, and 5 = normal. The responses for the right side were summed and ranged from 0 to 70.
gWilson (2012): The FIM motor score consists of 13 items that assess function across 4 different domains of self-care, sphincter control, transfers, and locomotion. The performance level for each item is strictly defined and ranges in value from 1 to 7, where 1 indicates complete dependence in an activity, and a score of 6 or greater indicates that a patient is capable of performing that activity independently, without supervision or help. The result is a discrete outcome variable with a minimum value of 13 and a maximum value of 91, with a larger value implying superior function. Functional dependence was a dichotomous variable defined as having achieved/not achieved ≥ 6 for all 13 FIM score items.
MRI Predictors of Neurologic Recovery
The association between MRI features and neurological outcomes was reported in 6 studies. For evidence synthesis, the following measures were considered together: AIS grade, Frankel grade, ASIA Motor score, motor function score, upper/lower extremity motor function and minimally useful function, pin prick score, and light touch score (see Table 6). A detailed table of associations is provided in the supplemental material (available in the online version of the article).
Association Between MRI and Other Factors and Neurologic, Functional, and Pain Outcomes.
Abbreviations: ASIA, American Spinal Injury Association; FIM, Functional Independence Measure; MCC, maximum canal compromise; MRI, magnetic resonance imaging; MSCC, maximum spinal cord compression; NS, not significant; SCI, spinal cord injury.
(O) = no association; (−) = association with a negative outcome; (O/−) = no association in one publication
aResults presented as reported by the authors based on multivariate regression analyses, adjusted for baseline neurologic status.
b Neurologic recovery: ASIA Impairment Scale grade, Frankel grade, ASIA Motor score, motor function score, upper/lower extremity motor function and minimally useful function, pin prick score, light touch score. Motor function score was determined by bilaterally measuring 14 muscle roots, with 0 = no contraction, 1 = flicker/trace of contraction, 2 = active movement without antigravity, 3 = active movement with antigravity, 4 = active movement against resistance, and 5 = normal. The responses for the right side were summed and ranged from 0 to 70. Extremity motor function was assessed by testing key individual muscles in each of the upper and lower extremities. Each muscle received a score of 0 to 5 for a total possible motor index score of 50 for upper extremity function and 40 for lower extremity function. Minimally useful motor function in an individual muscle was defined as a score of 3 or better on the 5-point manual muscle test. A score of 3 represents the ability for active movement with a full range of motion against gravity. Pin prick/light touch score was determined as follows: 29 spinal cord segments were tested bilaterally for response to pin prick and light touch, each of which were scored at 1 = absent, 2 = dysfunctional, and 3 = normal. Sensory scores ranged from a total score of 87 (normal response) to a score of 29 (no response in any segment). Responses for the right side were summed, unless some cord segments could not be tested, in which case responses for the left side were used.
c Functional recovery: FIM Motor Score, functional dependence, manual dexterity, dysesthetic pain. Functional dependence was a dichotomous variable defined as having achieved/not achieved ≥6 for all 13 FIM score items. Manual dexterity level was defined as the patient’s own perception of dexterity and skill in the following tasks: (1) using a keyboard, (2) playing a musical instrument, (3) buttoning his/her shirt, (4) grooming, and (5) writing. Dysesthetic pain level was a subjective rating on a 0 to 10 analog scale.
dMiyanji (2007): Soft-tissue injury was defined as an increased signal intensity of the perivertebral tissues on T2-weighted images.
eWhen length of hematoma was added to the statistical model, the only significant predictor in the model was length of hematoma.
The association between neurological outcomes and the presence of intramedullary spinal cord hemorrhage (defined, in the acute period, as a region of decreased signal intensity surrounded by a thin rim of high signal intensity on T2-weighted images) was investigated in 5 studies, each of which used a different assessment measure. Based on multivariate analysis, 2 studies found no association, 13,15 while 3 studies reported that the presence of hemorrhage is predictive of worse neurologic recovery. 14,18,19 In the study by Selden et al, intra-axial hematoma was present in all Frankel grade A patients, none of whom experienced a change in Frankel grade at follow-up. 19
Longer rostro-caudal intramedullary hematoma length was associated with worse neurologic recovery in 2 studies. 13,19 Boldin et al reported that each millimeter increase in hematoma length increased the risk of retaining a complete SCI; patients with complete SCI tended to have a longer hematoma length (median 10.5 mm, range 4-15 mm) than those with incomplete injuries (median 4 mm, range 2-9 mm) and did not exhibit a change in AIS grade at follow-up. This study also reported that 5 patients with a hemorrhage length less than 4 mm demonstrated improvements on the AIS grade at follow-up, suggesting that a length less than 4 mm may be predictive of positive outcomes. 13 Based on a single study, cord compression from extra-axial hematoma was not associated with poorer neurologic recovery in multivariate analysis. 19
The association between maximal canal compromise (MCC) and neurologic recovery was inconsistent across 2 studies. One study 14 found no association, while the other 17 reported that a lower MCC is predictive of a worse neurologic recovery. Maximum spinal cord compression (MSCC) was not associated with neurologic recovery across 3 studies. 14,17,19
The association between neurological outcomes and MRI evidence of cord edema (defined as a region of high signal intensity on T2-weighted images) was evaluated in 3 studies, each of which used a different assessment measure. Presence of cord edema was not associated with neurologic recovery in all 3 studies. 13 –15 Longer edema lesion length, however, was predictive of a worse neurologic recovery in 2 studies. 13,18 In a third study, a significant association was observed between edema lesion length and neurologic recovery following univariate analysis but not following what appears to be multivariate analysis (authors do not provide details of multivariate analysis and cautious interpretation is advised). 19
Two studies reported no association between SCI lesion length and neurologic recovery. 14,17 Cord swelling (defined as an increased spinal cord diameter) was predictive of worse neurological outcomes in one study; 14 a second study indicated no association between length of cord swelling and neurologic recovery. 19 Finally, single studies suggested no association between the following MRI radiographic factors and neurologic recovery: smaller diameter within swollen length of the cord, soft-tissue injury, preinjury stenosis, disk herniation, cord contusion, rostral point of edema, and worse baseline pin prick, light touch, and motor function scores.
MRI Predictors of Functional Recovery
The association between MRI features and functional outcomes was reported in 2 studies. 16,17 For evidence synthesis, the following measures of functional recovery were considered together: FIM Motor score, functional dependence (dichotomous variable based on FIM score), and self-reported measures of manual dexterity and dysesthetic pain (see Table 6). A detailed table of associations is provided in the supplemental material (available in the online version of the article).
In a single study, lower MCC was significantly associated with worse FIM score, but not with patient-reported measures of manual dexterity and dysesthetic pain. 17 MSCC and the spinal canal diameter at MSCC were not predictive of any measure of functional recovery. 17 There was no association between SCI lesion length and FIM score; however, a longer SCI lesion length was related to worse manual dexterity and dysesthetic pain. 17 Finally, based on a single study, MRI signal characteristics consistent with edema or hemorrhage are not important predictors of functional outcomes. 16
Spinal Cord Lesion Characteristics, Pattern, and Length Identified on Baseline Diffusion Tensor Imaging MRI as Predictors of SCI Outcomes
No studies were identified that assessed the association between DTI characteristics and outcomes.
Cost-Effectiveness of Baseline MRI in Patients With Acute SCI
No full economic analyses were identified that assessed the cost-effectiveness or cost utility of MRI in patients with acute SCI.
Evidence Summary
For KQ1, the overall quality of evidence was “Very Low” that patients who received a baseline MRI had an average improvement of 0.7 in Frankel grade compared to those who did not receive an MRI. Definitive conclusions are not possible from this study due to risk of bias (selection bias), lack of precision, and lack of data regarding the outcome of interest; specifically, details on the impact of MRI on clinical decision making were not reported (Table 7).
Quality (Strength) of Evidence Summary for Studies Evaluating the Impact of MRI on Treatment Decisions and Clinical Outcomes.
Abbreviations: MRI, magnetic resonance imaging; SCI, spinal cord injury.
aSerious risk of bias: The majority of studies violated 2 or more criteria of a good-quality cohort (see the supplemental material for details; available online at http://journals.sagepub.com/home/gsj).
For KQ2, Tables 8 and 9 summarize the overall quality of evidence for prognostic factors. There is “Moderate” quality evidence that longer intramedullary hemorrhage and “Low” quality evidence that smaller spinal canal diameter at MSCC are associated with decreased neurologic recovery. There is “Moderate” evidence that lower MSCC, longer SCI lesion length, and cord edema are not associated with worse neurologic recovery. There is inconsistent evidence that presence of hematoma (“Low”), greater edema lesion length (“Very Low”), cord swelling (“Low”), and MCC (“Low”) are predictive of worse neurologic recovery. MCC was the only significant predictor of worse functional outcome (“Low”). There is substantial heterogeneity across these studies with respect to the prognostic factors evaluated as well as in definitions and methods of measurement. Furthermore, there is variability in the measures used to evaluate outcomes, limiting our ability to synthesize findings across studies. In most instances, effect sizes and confidence intervals were not provided, preventing the evaluation of precision and magnitude of effect.
Quality (Strength) of Evidence Summary for MRI Predictors of Neurological Recoverya.
Abbreviations: ASIA, American Spinal Injury Association; DTI, diffusion tensor imaging; FIM, Functional Independence Measure; MCC, maximum canal compromise; MSCC, maximum spinal cord compression; MRI, magnetic resonance imaging; NR, no reported studies; SCI, spinal cord injury.
aNeurologic recovery: ASIA Impairment Scale grade, Frankel grade, ASIA Motor score, motor function score, upper/lower extremity motor function and minimally useful function, pin prick score, light touch score. Motor function score was determined by bilaterally measuring fourteen muscle roots, with 0 = no contraction, 1 = flicker/trace of contraction, 2 = active movement without antigravity, 3 = active movement with antigravity, 4 = active movement against resistance, and 5 = normal. The responses for the right side were summed and ranged from 0 to 70. Extremity motor function was assessed by testing key individual muscles in each of the upper and lower extremities. Each muscle received a score of 0 to 5 for a total possible motor index score of 50 for upper extremity function and 40 for lower extremity function. Minimally useful motor function in an individual muscle was defined as a score of 3 or better on the 5-point manual muscle test. A score of 3 represents the ability for active movement with a full range of motion against gravity. Pin prick/light touch score was determined as follows: 29 spinal cord segments were tested bilaterally for response to pin prick and light touch, each of which were scored at 1 = absent, 2 = dysfunctional, and 3 = normal. Sensory scores ranged from a total score of 87 (normal response) to a score of 29 (no response in any segment). Responses for the right side were summed, unless some cord segments could not be tested, in which case responses for left side were used.
bNo adjusted effect size estimates and/or no confidence intervals reported.
cSingle study; consistency across studies cannot be assessed for this outcome.
dDowngrade for imprecision: Small sample size for subgroup analysis (8 out of 9 patients with ASIA A) in one study (Boldin) and inability to assess precision as effect sizes and confidence intervals were not provided in 4 of the 5 studies.
eDowngrade for imprecision: Small sample size for subgroup analysis (8 out of 9 patients with ASIA A) in one study (Boldin) and inability to assess precision in the other study as effect sizes and confidence intervals were not provided.
Quality of Evidence Summary for MRI Predictors of Functional Recovery and Paina.
Abbreviations: FIM, Functional Independence Measure; MCC, maximum canal compromise; MSCC, maximum spinal cord compression; MRI, magnetic resonance imaging; OR, odds ratio; SCI, spinal cord injury.
aFIM = Functional dependence was a dichotomous variable defined as having achieved/not achieved ≥6 for all 13 FIM score items.
bSingle study; consistency across studies cannot be assessed for this outcome.
cNo adjusted effect size estimates or no confidence intervals reported, therefore cannot assess precision.
dNo confidence interval for the odds ratio was reported, therefore cannot assess precision.
The following list summarizes the findings from the included prognostic studies (Tables 8 and 9):
Longer hemorrhage length (“Moderate Evidence”): Two studies observed an association between longer hemorrhage length and worse neurologic recovery. Of these, one reported substantially longer hematoma length in ASIA A patients (no change in Frankel grade by follow-up) than in ASIA B, C, D patients (lower Frankel grades at follow-up); adjusted estimates were available only for patients with complete SCI.
Hemorrhage (“Low Evidence”): Three studies reported an association between the presence of hemorrhage on MRI and worse neurologic recovery; 2 other studies found no association. Each used different measures of neurologic outcome.
Cord edema: Three studies reported no association between cord edema and neurologic function; each used different measures of neurologic outcome (“Moderate Evidence”). Based on a single study, rostral point of edema was not predictive of neurologic outcomes (“Very Low Evidence”).
Longer edema lesion length (“Very Low Evidence”): A single study reported an association between longer edema lesion length and worse neurologic recovery; 2 other studies found no association.
Lower MSCC: There is no association between MSCC and either neurologic recovery (“Moderate Evidence”) or functional recovery (“Low Evidence”). Three studies reported no association with neurologic recovery. MSCC and the spinal canal diameter at MSCC were not predictive of functional outcomes in one study.
Lower MCC: One study reported an association between lower MCC and worse neurologic recovery; another study found no association (“Low Evidence”). Lower MCC was associated with worse FIM scores but not with manual dexterity or dysesthetic pain in one study (“Low Evidence”).
SCI lesion length: Two studies reported no association between SCI lesion length and neurologic recovery (“Moderate Evidence”). Based on a single study, SCI lesion length was not associated with FIM score (“Low Evidence”); however, a longer SCI lesion length was predictive of worse manual dexterity and dysesthetic pain (“Low Evidence”).
Cord swelling (“Low Evidence”): A single study reported an association between cord swelling and worse neurologic recovery.
Length of cord swelling (“Very Low Evidence”): A single study reported no association between length of cord swelling and neurologic recovery.
There were no studies that assessed DTI MRI characteristics as predictors of SCI outcome (KQ3) or the cost-effectiveness of MRI (KQ4); there is therefore insufficient evidence to draw conclusions for these questions.
Discussion
Magnetic resonance imaging has revolutionized the ability of clinicians to determine the location of traumatic injury in the spinal cord as well as identify disruptions in tissues that constitute the spinal canal. The purpose of this systematic review was to assess the role of MRI in clinical decision making and outcome prediction.
The Role of MRI to Assist Clinical Decision Making (KQ1)
MRI is widely used by many clinicians in the context of acute SCI to assist with clinical decision making. Unfortunately, our review only identified a single study (very low evidence) to address this question. In the study by Papadopoulos et al, the authors indicated that MRI findings influenced the timing of surgery with 34/66 (52%) receiving emergency surgery due to ongoing spinal cord compression and 16/66 (24%) undergoing anterior surgery due to the presence of anterior cord compression. As a result, the authors concluded that “emergency MRI provided an essential tool for the accurate diagnosis of spinal cord compression and directly influenced (our) initial clinical management in the majority of protocol patients.” Unfortunately, details regarding the surgical management of the reference group (no MRI) were not reported, making it impossible to draw firm conclusions about the utility of MRI in decision making. A direct comparison, however, was made in terms of outcome; specifically, patients who received an MRI (and treatment based on MRI results) exhibited an additional improvement of 0.7 in Frankel grade compared to those in the reference group. This study had moderately high risk of bias, including evidence of strong selection bias. The authors assigned patients to the reference group (no MRI) due to a contraindication to MRI, another emergent surgical procedure, or based on “perceived futility of treatment” by the attending physician. These criteria for group assignment likely introduce a systematic bias in subsequent treatment decisions. Thus, the results of this single study are not sufficient to confidently suggest that MRI is beneficial in improving decision making. No other studies were identified that specifically evaluated differences in treatment decisions, such as surgical timing and approach, between subject groups with and without pretreatment MRI. As a result, the overall quality of evidence for KQ1 was very low. This lack of evidence suggests that a profound knowledge gap exists and that future methodologically rigorous comparative studies are needed.
Additional lines of indirect evidence have suggested that MRI can accurately identify specific clinical entities that may be important in clinical decision making. A large number of studies have demonstrated MRI to be useful in identifying ongoing spinal cord compression, ligamentous injury, disc herniation, and vertebral artery injury. 2 These factors may influence surgical timing, approach, and need for instrumentation. However, the vast majority of studies on this topic did not meet our inclusion criteria as they did not (1) provide information on longitudinal follow-up, (2) compare decision-making choices between patients with and without MRI, or (3) provide estimates of effect on clinical outcomes that adjusted for baseline neurological status. Our approach was to focus on studies that evaluated the effect of MRI on treatment decisions and subsequent outcomes; unfortunately, only one study satisfied the inclusion criteria for this key question. The systematic review by Bozzo et al 2 synthesized a broader pool of studies in the context of acute SCI and developed a weak recommendation (based on weak evidence) for the use of MRI to direct clinical management. However, this systematic review had a number of methodological weaknesses and was rated as poor to moderate quality with a score of 5/11 on the AMSTAR scale (see supplemental material, available in the online version of the article). Furthermore, many of the individual studies (1) either did not report the timing of MRI relative to injury or surgical intervention or reported a broad range of acquisition timing (0-14 days) and/or (2) did not report adjusted estimates of effect on recovery at later follow-up. To better characterize the benefits of MRI, there is a need for future research in the form of well-designed prospective studies that compare the impact of MRI on patient management and outcomes to alternate strategies (eg, no use of MRI).
Conventional MRI for Prognostication (KQ2)
Existing evidence suggests that certain MRI characteristics are important predictors of outcomes in acute SCI, including length of intramedullary hemorrhage and the canal diameter at the level of MSCC. Other imaging characteristics may also be useful for prognostication, such as alternative measures of canal stenosis, presence of hemorrhage, and longer edema length; however, findings related to these predictors were inconsistent. Substantial heterogeneity exists with respect to the reporting and measurement of MRI features and clinical outcomes and limits our ability to synthesize findings across studies.
Prognostic studies included in this review identified that length of intramedullary hemorrhage (moderate-quality evidence), spinal canal diameter at the location of MSCC (low-quality evidence), and baseline neurological status are important predictors of outcome. Longer hemorrhage length was independently predictive of worse neurologic outcomes in 2 studies, particularly in patients with complete (AIS A) injuries. In addition, 3 of 5 studies reported that the presence of hemorrhage is associated with worse neurological outcomes, while 2 other studies observed an insignificant association (low-quality evidence). Overall, hemorrhage (length and presence) appears to be a predictor of worse outcomes; however, this finding must be interpreted with caution due to the inconsistency of results across studies. One small study suggested that length of hemorrhage greater than 4 mm is predictive of poor prognosis, 13 and that each millimeter increase in hematoma length increases the risk of retaining complete impairment (AIS A); these results need to be confirmed in larger prospective studies with a priori hypotheses. Similarly, the finding that decreased canal diameter at the location of MSCC is associated with worse neurologic outcome also needs to be replicated in a larger cohort. Two additional MRI features were inconsistently associated with outcomes (MCC and greater edema lesion length) and therefore also warrant further study. Other MRI characteristics were not statistically associated with clinical outcomes; however, the level of evidence was either low or very low, suggesting that future research may yield different results.
These prognostic studies were largely exploratory, investigated numerous MRI features, and had variable definitions of what constitutes SCI lesion, hemorrhage, edema, and swelling. For example, several studies categorized any abnormal T2-weighted signal as a “lesion,” whereas another study combined edema and hemorrhage together in a single variable (edema = 1 point, hemorrhage = 2 points). 11 Heterogeneity in imaging protocols and the use of nonstandardized techniques for geometric measurements such as MCC, MSCC, hemorrhage length, and edema length are also potential confounders. Moreover, none of the included studies reported interrater reliability of these methods. Clinical outcomes varied across studies, with many studies reporting on coarse outcomes such as AIS or Frankel grade, rather than more sensitive measures of recovery such as International standards for neurological classification of spinal cord injury (ISNCSCI) motor/sensory scores and Graded Redefined Assessment of Strength, Sensibility and Prehension (GRASSP). 16 The timing of baseline MRI also varied greatly in the reviewed studies and ranged from hours after hospital admission to 14 days postinjury. The magnitude of effect for associations and corresponding confidence intervals were also not provided in most studies. All of these factors prevented data pooling and synthesis and the development of firm evidence-based conclusions. Given these variations in study design, there remain significant knowledge gaps regarding the association between intramedullary abnormalities in the spinal cord and neurologic, functional, patient-reported, and safety outcomes. Overall, in interpreting the current literature, we have identified that length of hemorrhage (moderate evidence) and decreased canal diameter at the location of MSCC (low evidence) are important predictors of worse neurologic outcomes.
The MRI features extracted from conventional MRI, such as length of hemorrhage, tend to be relatively crude methods for determining the extent of tissue compromise. Computing volume of affected tissue and identifying the location of the pathology in the compromised spinal cord (dorsal vs ventral grey matter and/or specific white matter columns) could further improve prognostic performance. Conventional MRI may have only modest prognostic utility due to its inability to distinguish recoverable from nonrecoverable tissue injury. For example, edema alone, whether limited or extensive, is recoverable. On the other hand, contusion, which may have a MRI signal indistinguishable from edema on T2-weighted images, indicates a more advanced injury condition in which there is permanent loss of neurons. The studies included in this review did not utilize GRE or SWI sequences that are more sensitive for identifying contusion and microhemorrhages. The results of this review highlight the limitations of the traditional T1- and T2-weighted sequences for detecting more specific patterns of injury and quantifying reversible and irreversible components of damage. These findings confirm the need to further develop advanced MRI techniques that can provide a more detailed view of injury to the spinal cord parenchyma, including DTI, SWI, functional MRI, MR spectroscopy, perfusion imaging, and other sequences sensitive to demyelination, such as magnetization transfer and myelin water fraction. 17,18 However, these advanced MRI methods will inevitably be more time consuming and cannot yet be reliably implemented in a clinical setting due to technical challenges; these include the need for improved signal-to-noise ratio, high field strength (3 T or greater), and complex data analysis that is highly labor intensive. Furthermore, these advanced MRI methods would need to be cost-effective and widely available before they are able to be adopted clinically.
The Role of DTI in Prognostication (KQ3)
No articles were identified that assessed the predictive value of DTI in patients with acute SCI; this constitutes an important knowledge gap. Furthermore, there remains a lack of standardization for spinal cord DTI acquisition. All of these issues present an opportunity for future multicenter studies to evaluate the value and practicality of DTI as a prognostic tool in acute SCI. Since certain quantitative metrics derived from DTI appear to correlate with important microstructural features such as axonal integrity, 17 a standardized approach to DTI that can consistently interpret diffusion changes in the SCI zone, as well as remotely in the spinal cord, may offer powerful predictive information following SCI.
Cost-Effectiveness of MRI in Acute SCI (KQ4)
There are no studies that evaluate the cost-effectiveness of MRI using full economic analyses. Our search did identify one conference abstract that investigated the same cohort as Papadopoulos et al. 19 This abstract by Selden et al (1999) reported that the MRI-protocol group had a significantly shorter intensive care unit and hospital length of stay and decreased duration of ventilator support, resulting in an estimated savings of $50 300 per case. However, details of the cost estimates were not included, and the authors did not perform a full economic analysis. Thus, a substantial knowledge gap exists regarding the cost-effectiveness of MRI in the early evaluation of patients with SCI, suggesting a strong need for further investigation.
Knowledge Gaps and Limitations
This review has identified several knowledge gaps regarding the role of MRI in clinical decision making and outcome prediction in patients with acute SCI. For each of the key questions addressed, well-designed studies are required to clearly define the role of MRI, the appropriate methodology of conventional as well as advanced MRI (such as DTI), as well as the cost-effectiveness of these strategies. This future research will help generate clinical practice guidelines that outline the best utility for MRI in SCI.
This systematic review has several limitations. First, although we performed a thorough electronic literature search in several major databases and also manually searched reference lists, it is possible that some relevant studies were missed. We focused this review only on the highest quality studies available that directly addressed the key questions and restricted our inclusion criteria to those that compared MRI versus no MRI for KQ1 and KQ4, and those that performed multivariate analysis for KQ2 and KQ3. As a result, our review included a small number of studies and provides only a limited summary of the research that has occurred to date. However, we felt justified in this approach and believe that broader inclusion criteria would have resulted in the inclusion of lower level evidence and additional heterogeneity.
Conclusions
The overall body of evidence regarding the utility of MRI in acute SCI is limited. It has been established that MRI accurately detects potentially important clinical entities such as cord compression, disc herniation, and ligamentous injury; however, no comparative studies were identified that link MRI with decisions such as surgical approach and timing. Furthermore, only very low quality evidence exists linking the use of MRI in acute SCI to clinical outcomes. It appears that MRI, in addition to baseline neurological status, is useful for prognostication; specifically, moderate-quality evidence suggests that longer intramedullary hemorrhage and low-quality evidence indicates that smaller spinal canal diameter at MSCC are associated with poor neurologic recovery. No literature was identified that investigated DTI as a prognostic tool or assessed the cost-effectiveness of MRI in acute SCI. The paucity of literature in each of these areas highlights the need for well-designed prospective multicenter studies and full economic analyses to better understand the utility and cost-effectiveness of MRI in acute SCI.
Footnotes
Acknowledgements
We are indebted to Nancy Holmes and Ms Chi Lam for their administrative assistance and to Krystle Pagarigan and Erin Anthony-Fick for their assistance with data abstraction and verification.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by AOSpine and the AANS/CNS Section on Neurotrauma and Critical Care. Dr Fehlings wishes to acknowledge support from the Gerald and Tootsie Halbert Chair in Neural Repair and Regeneration and the DeZwirek Family Foundation. Dr Tetreault acknowledges support from a Krembil Postdoctoral Fellowship Award. Methodologic and analytic support for this work was provided by Spectrum Research, Inc, with funding from AOSpine North America.
Supplemental Material
The supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.