
Abstract
Study Design:
Prospective randomized control trial.
Objective:
To investigate the role of cervical collars in postoperative care following 1- and 2-level instrumented anterior cervical discectomy and fusion (ACDF).
Methods:
The Cervical Spine Research Society Resident Fellow Grant funded this project. Fifty consecutive patients undergoing 1- or 2-level ACDF surgery were randomized into groups receiving either no brace or a cervical brace for 6 weeks postoperatively. Neck Disability Index scores were recorded preoperatively and at regular follow-up visits up to 1 year. Computed tomography scans were read 1 year postoperatively to determine fusion rates, and subsidence was measured as change in middle vertebral distance between initial postoperative and 6-month follow-up lateral cervical radiographs.
Results:
Twenty-two patients were in the no-brace group, and 22 patients were in the brace group at final follow-up, with an average age of 50 and 55 years, respectively. The no-brace group had a total of 32 operative levels, whereas the brace group had 38 operative levels. There was no statistically significant difference in 1-year postoperative Neck Disability Index scores between the brace (9.30) and no-brace (6.95) groups (P = .28), in 6-month subsidence of all operative levels between the brace (0.85 mm) and no-brace (0.79 mm) groups (P = .72), or in the proportion of fused levels between the brace (89%) and no-brace (97%) groups (P = .37).
Conclusions:
Our results suggest no advantage in wearing a cervical brace following 1- or 2-level ACDF surgery with respect to 1-year outcome scores, 1-year fusion rates, and 6-month subsidence.
Keywords
Introduction
Postoperative immobilization with a rigid cervical orthosis is widely utilized following anterior cervical discectomy and fusion (ACDF). However, in their seminal paper from 1958, Smith and Robinson reported that brace immobilization of the neck was not used for 1-level fusions and was reserved for multilevel procedures. 1 –3 The utility and necessity of postoperative cervical bracing may be questioned since the advent of anterior plating as a means of increasing stability and decreasing micromotion across a fusion segment, acting as an internal brace. Anterior plating has become widely adopted due to its association with higher fusion rates, lower rates of graft extrusion and subsidence, and improved outcomes regardless of number of fused levels. 4 –12 Despite the success of ACDF with anterior plating, pseudarthrosis and subsidence remain relevant complications, at least partially related to excessive motion about a fusion segment postoperatively, which is thought to be mitigated by use of postoperative rigid cervical orthoses. 13 –18
The rigid cervical collar remains a common means by which to limit cervical motion postoperatively. 19,20 By preventing excessive motion, the cervical collar may reduce the risk of complications such as graft subsidence and nonunion. However, the breadth of literature is divided on the benefits of postoperative use of a rigid cervical collar. Some studies suggest collars restrict excess motion and may be associated with improved postoperative outcomes, 21 –23 while others report contradictory results showing no correlation with collar use and improved outcomes or fusion rates after 1-level instrumented ACDF. 24 Additionally, reports of cervical collars causing airway obstruction and dysphagia call into question not only their efficacy but also their safety during use in the acute postoperative period. 25,26
The controversy surrounding the efficacy of cervical collars postoperatively demonstrates the need for further exploration of the effects collar use has on clinical and radiographic outcomes following ACDF surgery. Surgeons may continue to use rigid collars primarily because of a lack of quality evidence directly comparing outcomes with or without bracing. The aim of this prospective, randomized control study was to investigate the role of the cervical collar in postoperative care following 1- and 2-level instrumented ACDF.
Methods
Patient Sample
The Cervical Spine Research Society Resident Fellow Grant provided funding for this institutional review board–approved prospective study. This study was designed and carried out with adherence to the CONSORT statement for randomized controlled trials. A flow diagram detailing the enrollment, allocation, follow-up, and analysis is summarized in Figure 1. A total of 50 patients were enrolled in the study. After obtaining signed consent, patients were randomized into treatment groups using a randomizing computer generator in a 1:1 ratio. The first 10 patients were assigned a random number between 1 and 10 without duplicate numbers, ensuring a 1:1 ratio. Even numbers were assigned to the brace cohort and odd numbers were assigned to the no-brace cohort. This process was repeated for each subsequent set of 10 cases. Twenty-five patients were allocated to the no-brace group and 25 patients to the brace group. Five patients were lost to follow-up (2 in the brace group and 3 in the no-brace group), and 1 additional patient in the brace group was excluded from analysis due to removal of painful hardware before final follow-up. All patients underwent anterior arthrodesis with a cortico-cancellous machined allograft (Puros-S2 Allograft, Zimmer, Warsaw, IN) and static anterior plating (Invizia Cervical Plating System, Zimmer, Warsaw, IN). The braced cohort was fitted with an appropriate size semirigid cervical orthosis for 6 weeks postoperatively (Miami J Cervical Orthosis, Ossur American, Foothill, CA).
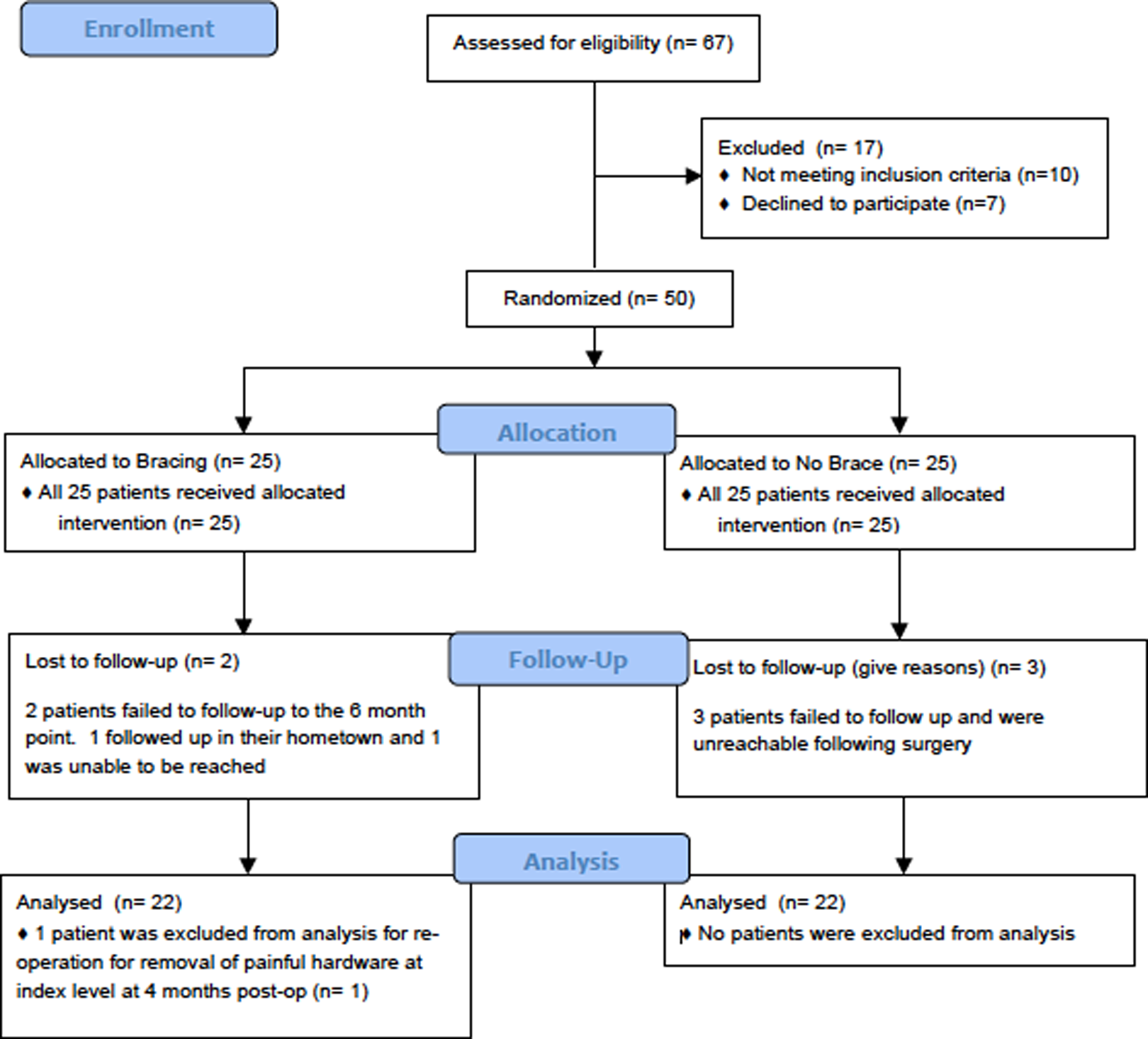
CONSORT flow diagram of patient enrollment and allocation into each cohort.
Indications for operative treatment were radiculopathy or myelopathy that had failed a minimum of a 6-week course of nonoperative management. Inclusion criteria for the study were no prior attempted cervical arthrodesis, no prior posterior cervical foraminotomy, no prior anterior cervical discectomy with or without fusion, no prior posterior laminectomy with or without fusion, and persistent radiculopathy or myelopathy attributed to 1- or 2-level disease after a minimum of 6 weeks of nonoperative management. All patients in the study were instructed to refrain from vigorous or contact physical activity for a total of 3 months or until the first radiographic evidence of fusion.
Clinical and Radiographic Information
Clinical outcome was measured for all groups with documentation of the Neck Disability Index (NDI) score preoperatively and 2 weeks, 6 weeks, 3 months, 6 months, and at final follow-up 1-year postoperatively. The NDI score is reported as a numerical value out of 50 points. Radiographic outcomes included subsidence and fusion rates assessed at 6-month and 1-year follow-up, respectively. Subsidence was measured as the change in middle vertebral distance between initial postoperative films taken on postoperative day 1 and 6-month lateral cervical radiographs. All radiographs were standing films to most accurately assess subsidence and promote internal consistency. In brief, middle vertebral distance is defined as the distance from the middle of the superior endplate of the superior operative vertebrae to the middle of the inferior endplate of the inferior operative vertebrae. Subsidence was recorded and analyzed for each fused level individually in all radiographs, with the most cephalad level denoted as first level and the caudad level denoted as second level in 2-level procedures. Fusion was assessed by an independent, blinded neuroradiologist with computed tomography scan at 1-year postoperatively. Fusion was defined as marginal bridging trabeculae, from endplate to endplate, through or around the graft.
Statistical Analysis
IBM SPSS (Armonk, NY) was used to perform all statistical analyses. All continuous, numerical comparisons between groups were conducted with an unpaired or paired t test where appropriate. All contingent categorical proportions between groups were analyzed by Fisher’s exact test. Results were taken to be statistically significant if P < .05.
To better understand the effect of perioperative factors such as diabetes, 2-level fusion, age, and preoperative NDI between the brace and no-brace groups, we conducted a stepwise multiple linear regression to determine the effect of these predictor variables on postoperative NDI scores that were statistically different at any of our postoperative time points, as well as NDI scores at the 1-year final follow-up. Stepwise multiple linear regression excludes any variables that do not improve the overall fit of the regression model, and therefore, we report only the variables that were included in the final model.
A power analysis was conducted based on difference in NDI scores between a braced group and not braced group found in the literature. 24 Statistically significant differences in NDI scores was found at about 9 points. Anecdotally our standard deviation in NDI scores from our institution’s population is around 10. This standard deviation remains consistent with the results reported in this study. Using a power analysis calculator with 9 points as our expected difference in the mean NDI scores with a standard deviation of 10, we estimated 19 subjects in each group, totaling 38. We had 22 subjects in each group at final follow-up, suggesting we had sufficient power. With respect to subsidence and fusion rates, the paucity of literature on subsidence in bracing, the different methods used to measure subsidence, and the wide range of fusion rates reported in the literature, subsidence and fusion rates were not incorporated into our power analysis.
Results
Patient Characteristics
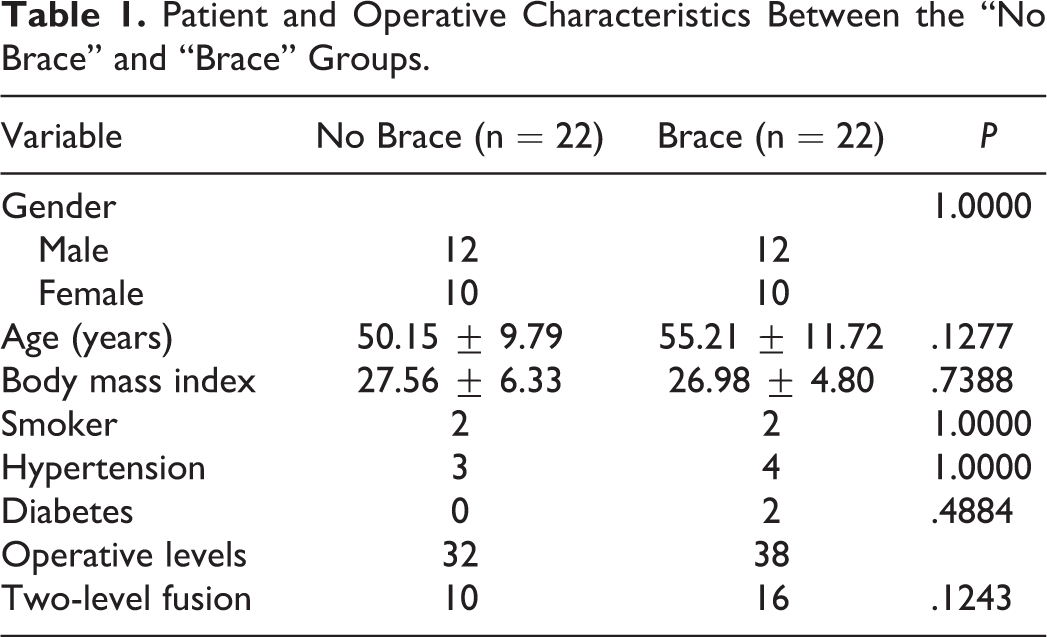
A total of 44 patients were analyzed at final follow-up, 22 in the no-brace group and 22 in the brace group. Demographic and operative information between the groups is summarized in Table 1. There were no significant differences with regard to gender, age, body mass index, smoking status, hypertension, or diabetes. There was a greater number of 2-level fusions in the brace group (16/22) when compared with the no-brace group (10/22), but this was not statistically significant.
Patient and Operative Characteristics Between the “No Brace” and “Brace” Groups.
Neck Disability Index Scores
The preoperative versus postoperative NDI scores for both the brace (P < .0001) and no-brace (P < .0001) groups showed significant improvement over the course of treatment to final follow-up. The NDI scores at time intervals of preoperative, 2-week, 6-week, 3-month, 6-month, and 1-year final follow-up were recorded for all procedures, 1-level procedures, and 2-level procedures as displayed, respectively, in Tables 2, 3, and 4. Additionally, the preoperative and postoperative NDI scores at final follow-up between the 2 groups showed no significant difference (Tables 2-4). However, the no-brace cohort displayed a significantly lower NDI score at 2 weeks postoperatively for all levels and at 6 months for 2-level procedures. Taking half of our preoperative standard deviation for each group as the minimal clinically important difference, only 2 patients in the no-brace group and 1 patient in the brace group did not reach minimal clinically important difference at 1-year final follow-up (P = >.99).
Summary of Preoperative and Postoperative NDI Scores (Out of 50 Points)a.
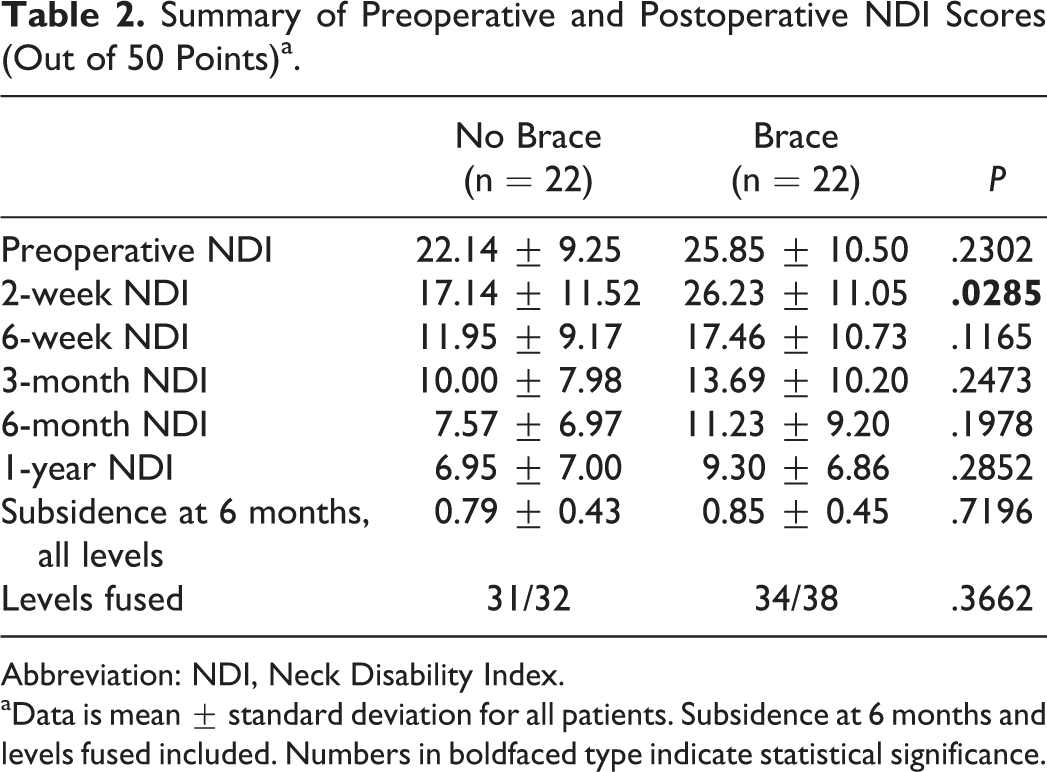
Abbreviation: NDI, Neck Disability Index.
aData is mean ± standard deviation for all patients. Subsidence at 6 months and levels fused included. Numbers in boldfaced type indicate statistical significance.
Summary of Preoperative and Postoperative NDI Scores, Subsidence, and Fusion Rates for Single-Level Procedures Only.
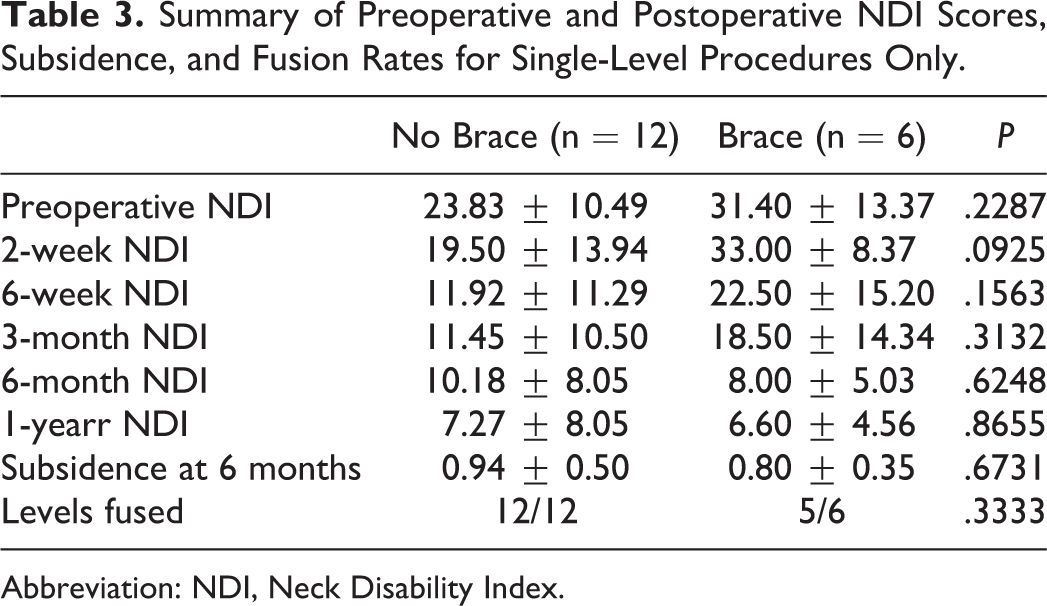
Abbreviation: NDI, Neck Disability Index.
Summary of Preoperative and Postoperative NDI Scores, Subsidence, and Fusion Rates for 2-Level Procedures Only.
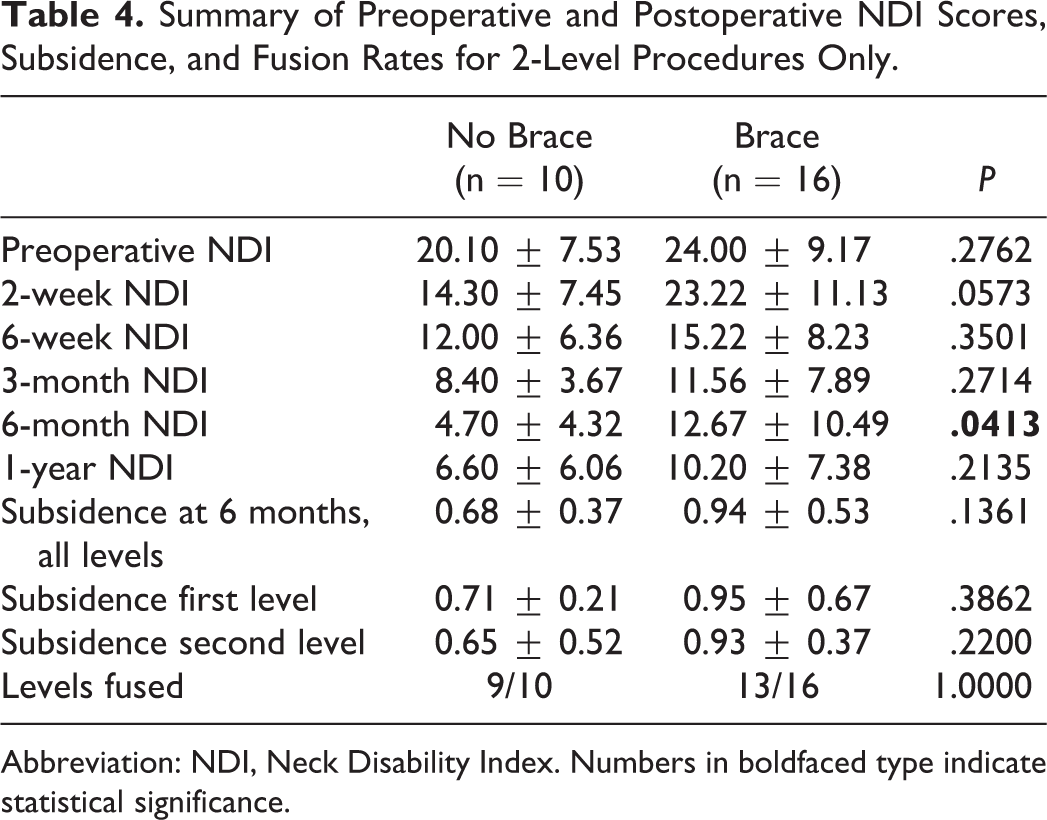
Abbreviation: NDI, Neck Disability Index. Numbers in boldfaced type indicate statistical significance.
Predictors of NDI Scores at Various Time Points
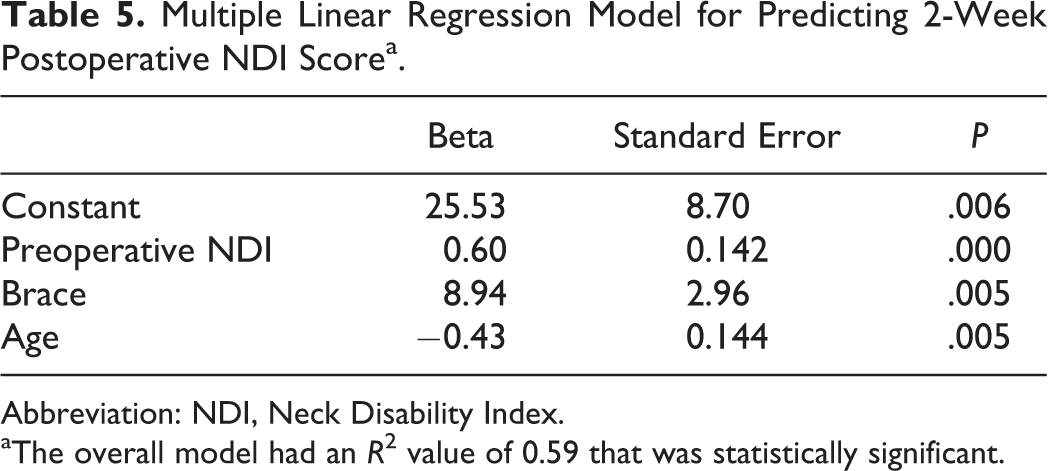
We conducted 3 separate stepwise multiple linear regressions with independent variables preoperative NDI, age, diabetes, 2-level procedure, and postoperative brace. Our dependent variables were 2-week postoperative NDI, 6-week postoperative NDI, and 1-year postoperative NDI. These 3 dependent variables were chosen because the 2-week and 6-week time points were shown to be statistically different between the no-brace and brace groups on previouzs analyses (Tables 2 and 4). For the 2-week postoperative NDI model, the overall model fit was R 2 = 0.592, and the variables included in the final model were preoperative NDI, brace, and age, as these were the only variables that improved the model fit and had a statistically significant effect on the dependent variable (2-week NDI; Table 5). The model for 6-week postoperative NDI had an overall fit of R 2 = 0.424, and the only statistically significant predictor was preoperative NDI with a beta weight of 0.64 (P = .000). For 1-year NDI, there were no statistically significant predictor variables. Of note, diabetes and 2-level procedures were excluded from every model.
Multiple Linear Regression Model for Predicting 2-Week Postoperative NDI Scorea.
Abbreviation: NDI, Neck Disability Index.
aThe overall model had an R 2 value of 0.59 that was statistically significant.
Subsidence
The average subsidence at 6 months per level for all operative levels in the brace (0.85 ± 0.45 mm) and no-brace (0.79 ± 0.43 mm) groups was not significantly different (P = .72; Table 2). When analyzing 2-level procedures, the average subsidence for the cephalad levels was greater than the caudad levels in both the brace (0.95 ± 0.67 mm) and no-brace (0.71 ± 0.21 mm) groups, though the difference between braced and no-brace groups was not significant (P = .39; Table 4). Additionally, no significance was found in the caudad-level subsidence, which measured 0.93 ± 0.37 mm in the brace group and 0.65 ± 0.52 mm in the no-brace group (Table 4). When examining the difference in proportion of levels with greater than 1 mm subsidence, we observed 11/38 levels in the brace group and 4/32 levels in the no-brace group, which was not statistically significant (P = .14).
Fusion Rates
The success of fusion between the 2 groups was not found to be significant (Tables 2-4). The 1-year fusion rate, as designated by a blinded neuroradiologist via computed tomography imaging, for all levels for the brace group was 86%, whereas the fusion rate for the no-brace group was 95% (P = .5768). When analyzing 1- and 2-level procedures separately, no significant differences were found in fusion rates between the 2 groups.
Revision Surgery
One patient in each cohort developed symptomatic nonunion requiring revision surgery. The patient in the no-brace group had a 2-level procedure and had a revision operation 30 months postoperatively. The patient in the brace cohort underwent a single-level index procedure and had a revision surgery 15 months postoperatively. Both patients had resolution of symptoms following revision.
Discussion
Cervical orthoses have been used historically as a means to mitigate excessive motion about fusion segments postoperatively. However, even prior to the advent and wide acceptance of anterior plating, much heterogeneity existed among surgeon utilization of cervical bracing. Smith and Robinson employed postoperative bracing only after multilevel fusions. 3 Other pioneers of the procedure, such as Cloward, used bracing routinely after all ACDFs, regardless of number of levels fused. However, even Cloward acknowledged in his 1958 study that his group abandoned routine use of bracing after the first several cases. 27
Limiting excessive motion across a fusion segment is one of the many ways surgeons can improve fusion rates and clinical outcomes. This basic concept first prompted surgeons to use cervical orthoses as a means of external immobilization. The advent of anterior plating in ACDF was fostered based on this principle as well. Anterior plating was implemented in ACDF to act as an internal brace, controlling for motion through a fusion segment by direct immobilization. This pivotal advancement in the field has been shown to increase fusion rates and improve clinical outcomes and has been widely validated throughout the literature. 4 –12 As plating acts as a superior means of immobilization, it seems intuitive that anterior plating would have curtailed the use of cervical bracing. However, many surgeons still employ routine use of postoperative cervical bracing, largely due to the paucity of high-level literature directly comparing bracing versus not bracing after instrumented ACDF. According to a questionnaire study sampling spine surgeons attending the “Disorders of the Spine” conference (January 2008, Whistler, Canada), 63% of spine surgeons employed routine postoperative cervical bracing following ACDF. 19 In this level II prospective randomized study, we sought to elicit any difference that may exist in radiographic and patient-reported outcomes after 1- and 2-level ACDF with or without a brace.
Along with a lack of clinical literature comparing braced versus non-braced patients, there is also a lack of biomechanical evidence that braces actually significantly limit motion in the cervical spine. Sandler et al 28 reviewed 3 types of commonly used cervical braces and demonstrated that no collar restricted the motion of any of the subjects to less than 19° of flexion-extension, 46° of axial rotation, or 45° of lateral bending, and most subjects demonstrated significantly more motion. Additionally, Bell et al 29 highlighted the challenges of correctly fitting commercially available braces and demonstrated that ill-fitting braces not only failed to limit excess motion but also contributed to morbidity postoperatively.
Our results showed no difference in radiographic fusion rates, graft subsidence measurements, NDI scores at final 1-year follow-up, or complication/reoperation rates among patients, braced or not, following 1- and 2-level ACDF. However, interval NDI scores at 2 weeks postoperatively were significantly lower in the no-brace cohort for combined 1- and 2-level procedures and at the 6-week time point for 2-level procedure. Given the potential effect of the 2-level procedure, as well as the older age, higher number of patients with diabetes, and higher preoperative NDI scores in the brace group, we conducted a stepwise multiple linear regression to determine if these variables had an effect on NDI scores at the 2- and 6-week postoperative time points. We found that at 2 weeks, preoperative NDI, wearing a brace, and younger age all had a statistically significant effect on worse NDI outcomes, and only preoperative NDI had a statistically significant effect on 6-week NDI score. Diabetes and 2-level procedures did not have a statistically significant effect on outcomes at any time point. The preoperative NDI score was 3.71 points higher in the brace group than the no-brace group, which contributes to the statistical difference seen at the 2-week time point for all levels. We would expect increased preoperative NDI score to lead to higher postoperative NDI score, but wearing a brace was also found to be a statistically significant predictor of higher NDI score by 8.94 points (Table 5) at the 2-week postoperative time point. This may be related to discomfort from brace-wear about a fresh incisional wound or perhaps even related to subsequent neck stiffness from prolonged neck immobilization. Our results echo those reported by Campbell et al in their retrospective study evaluating single-level fusions. 24 We therefore agree with their conclusion that bracing is not necessary after 1-level fusion, with further validity, and expand on these claims to include 2-level fusions via our prospective model.
Our results clarify the existing debate on the advantages and disadvantages of cervical collars. Some reports profess that the use of rigid cervical collars improves postoperative patient outcomes, while others echo our results and demonstrate no association with improved outcomes. 21 –23 Given our results and additional reports that have reported adverse safety events from using cervical collars, we advise against their routine use in postoperative care following cervical spine surgery. 25,26
The results of this study may change the way spine surgeons manage patients postoperatively. We provide evidence that may allow surgeons to opt not to brace patients postoperatively, effectively eliminating the patient discomfort and potential morbidity associated with bracing. 30 –32 The cost burden of ACDF is also lessened as the price of purchasing braces, which frequently cost upwards of US$100, is mitigated.
This study has several limitations. First, although the study was a prospective randomized trial by design, it was relatively low-powered. Additionally, as with any radiographic measurement, our subsidence measurements were calculated using computerized measuring tools, which may not account for radiographic magnification and/or artifact error. Finally, although all patients had similar demographic information, there was no means of truly objectifying host status, which plays a significant role in any spinal fusion procedure.
Conclusions
The use of routine postoperative cervical bracing following 1- and 2-level ACDF, though widely practiced, has little high-level evidence to support its use. The results of this prospective randomized controlled trial demonstrated no advantage to postoperative brace use as patients exhibited no difference in fusion rates, measurable subsidence, complications, or reported outcomes. Additionally, results of this study suggest braced patients have worse NDI scores at the 2-week postoperative time point.
Footnotes
Acknowledgements
The authors acknowledge the Cervical Spine Research Society for providing the Resident Fellow Grant to conduct this research.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SK has received personal fees from Globus Medical and Zimmer. AH has received personal fees from Medtronic, Stryker, and Zimmer. SQ has received personal fees from Globus Medical, Medtronic, Stryker, Zimmer, and Orthofix Inc. These disclosures presented no conflicts of interest relevant to this research study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Cervical Spine Research Society Resident Fellow Grant.