
Abstract
Study Design:
Prospective cohort study.
Objectives:
The objectives of this study were (1) to determine the characteristics of patients sustaining spinal trauma in India and (2) to explore the association between patient or injury characteristics and outcomes after spinal trauma.
Methods:
In affiliation with the ongoing INternational ORthopaedic MUlticentre Study (INORMUS), 192 patients with spinal injuries were recruited during an 8-week period (November 2011 to June 2012) from 14 hospitals in India and followed for 30-days. The primary outcome was a composite of mortality, complications, and reoperation. This was regressed on a set of 13 predictors in a multiple logistic regression model.
Results:
Most patients were middle-aged (mean age = 51.0 years; median age = 55.5 years; range = 18.0 to 72.0 years), male (60.4%), injured from falls (72.4%), and treated in a private setting (59.9%). Fractures in the lumbar region (51.0%) were most common, followed by thoracic (30.7%) and cervical (18.2%). More than 1 in 5 (21.6%) patients experienced a treatment delay greater than 24 hours, and 36.5% arrived by ambulance. Thirty-day mortality and complication rates were 2.6% and 10.0%, respectively. Care in the public hospital system (odds ratio [OR] = 6.7, 95% CI = 1.1-41.6), chest injury (OR = 11.1, 95% CI = 1.8-66.9), and surgical intervention (OR = 4.8, 95% CI = 1.2-19.6) were independent predictors of major complications.
Conclusions:
Treatment in the public health care system, increased severity of injury, and surgical intervention were associated with increased risk of major complications following spinal trauma. The need for a large-scale, prospective, multicenter study taking into account spinal stability and neurologic status is feasible and warranted.
Keywords
Introduction
Injuries due to trauma have rapidly been increasing in number worldwide, particularly in low- and middle-income countries (LMICs) such as India. 1,2 This is partially due to the rapid motorization over the past 2 decades. Excessive speed, nonusage of helmets, driving under the influence of alcohol, and poor road design and infrastructure-related factors are some major risk factors for the increasing number of road traffic accidents. 3,4 As per the first global status report on road safety of the World Health Organization (WHO), India has the highest number of deaths due to road traffic accidents, with 375 deaths and more than 1200 injuries per day due to road accidents in the country. 5 Trauma is projected to be third largest killer in the developing world by 2020, with a large number of these injuries comprising of spine trauma and traumatic spinal cord injury. 3,6
Spinal trauma may result in spinal cord injury (TSCI), an injury to the spinal column resulting in severe compromise to neurologic structures, resulting in possible paralysis, sensory loss, bladder or bowel dysfunction, and mortality. 7 –10 The devastating effects of TSCI are not just limited to an individual’s health, but also create enormous financial burdens on families and society at large. The burden of TSCI and its sequelae is enormous, particularly in the developing world. 8,9,11 –14 A thorough epidemiological understanding is vital for implementing preventative measures and planning clinical services, as well as understanding disease morphology and burden. 15
Because of limited resources and the large volume of patients seen in LMICs, the demographics of spine trauma patients, mechanisms of injury, method of arrival to hospital, timing and type of care provided, and postinjury outcomes remain largely unknown. Such information would provide direction for future policy, collaboration, and research initiatives critical to understanding and mitigating the burden of spine trauma worldwide. To address this, we conducted a collaborative, prospective observational study in India to determine the current magnitude and prognostic factors for outcomes following spine trauma. The primary objectives of this study were (1) to determine the characteristics of patients sustaining spinal trauma in a LMIC and (2) to explore the association between patient or injury characteristics and 30-day mortality and morbidity in patients after spinal trauma.
Methods
Patients and Study Design
We conducted a prospective multicenter observational investigation of orthopedic trauma patients in affiliation with the ongoing INternational ORthopaedic MUlticenter (INORMUS) study which includes 14 hospitals in India (see the appendix). The protocol for this study has been previously published and is available on clinicaltrials.gov. 16 The study was approved by the Hamilton Health Sciences Research Ethics Board and by the respective ethics boards at each participating institution. A total of 192 patients with traumatic spine injuries were recruited during an 8-week period. The most common sites of spinal trauma were the All India Institute of Medical Sciences, Ganga Hospital, and Post Graduate Institute of Medical Education and Research.
The following inclusion criteria were used to determine eligibility in the study: male or female patients aged >18 years, acute or subacute trauma presenting within 8 weeks of injury, and presence of a spinal fracture or fracture-dislocation, defined as occurring in any of the 3 spinal columns from the occipitocervical junction to the sacropelvic junction. Selection bias was minimized because all patients meeting the eligibility criteria were consecutively included. Patients were followed up to 30 days to determine rates of mortality and adverse events. Mortality and reoperation are objective outcomes thereby limiting the potential for bias in their assessment.
Patient Recruitment
A designated research assistant was present in each of the recruited centers that screened patients in the emergency department, surgery wards, preoperative assessment clinics, surgical lists, fracture clinics, and preoperative waiting areas. Orthopedic residents kept a running list of new eligible patients that were reviewed with the research assistant daily. Research personnel interviewed patients and recorded age, gender, medical history, place and mechanism of injury, socioeconomic status, time to reach hospital, and nonorthopedic injuries of the head, neck, chest, and abdomen.
Complication rates of deep vein thrombosis (DVT), pneumonia, acute respiratory distress syndrome (ARDS), multiple organ failure (MOF), urinary tract infection (UTI), infection and reoperation were assessed. To increase the event rate and thus power and to provide an overall estimate of effect, a composite outcome, termed “major complications,” was created. A composite event was considered to have occurred if at least one of the following outcomes were present: death by any cause, unplanned reoperation, and complications (if at least one of 7 subcomplications occurred). Our primary aim was to identify significant predictors of major complications amongst patients presenting with spine fractures.
Statistical Analysis
The sample size consisted of all 192 patients with spine fractures from the INORMUS pilot study. All statistical analyses were 2-sided using an alpha level of 5%. Baseline characteristics were reported using standard summary descriptive statistics such as means, percentages, and standard deviations. PASW Statistics 18 (IBM Corp, Armonk, NY, USA) was used to conduct all statistical analyses.
Binary logistic regression was used to identify significant predictors of the composite outcome. Independent variables were selected for inclusion into the regression model based on 2 methods. First, a guided approach was taken whereby all variables hypothesized to be predictive of the composite outcome were identified. The initial guided approach to model building identified 15 variables for inclusion into the logistic regression model. Public versus private hospital, mean income, time from admission to stabilization, gender, age, smoking and alcohol status, the presence of chest injury in addition to spine injury and surgical status were included because treatment at a public hospital, low household income, extended time from admission to stabilization, male sex, increasing patient age, smoking, alcohol consumption, additional injuries and surgery were hypothesized to increase the odds of the composite event occurring. Two dummy variables were included for thoracic and lumbar injuries with cervical injuries as the reference group because injuries to the cervical region are generally more significant. 17 Dummy variables allow nominal variables with more than 2 categories to be coded whereby each of the coded variables is assigned 1 if present and 0 if absent and the reference variable is always assigned the value 0. Temporary stabilization was hypothesized to reduce the odds of the composite and was thus likewise included.
Subsequently, the model derived from the guided approach was compared with a model produced by stepwise regression (P < .05 entry, P > .10 removal) and variables were either added or removed in light of the results. Stepwise regression identified public versus private hospital, alcohol consumption, chest injury, surgical status, and temporary stabilization for inclusion into the model. Since the model produced from stepwise regression did not include income and smoking, and because income and smoking contained a high proportion of missing data (14/192 = 7.3% and 23/192 = 12.0% for income and smoking, respectively), these variables were dropped from the final model. The final regression results including and excluding income and smoking did not differ to an appreciable extent and all conclusions remained the same. The likelihood ratio test for the inclusion of income and smoking (χ2 = 0.355, df = 2, P = .837) suggested that they were not important predictors. This justified the exclusion of income and smoking.
Multicollinearity, defined as extensive correlation amongst predictor variables, was considered if the variance inflation factor from any parameter was greater than 10 or if the standard error of any β coefficient was greater than 2. The standard errors for all β coefficients were ≤2 and the variance inflation factors for all independent variables were less than 5. Therefore, no further modifications to the model were made. The final model included 13 variables: public versus private hospital, gender, age, alcohol consumption (yes/no), chest injury (yes/no), surgical status (yes/no), injury to thoracic and lumbar region dummy variables, time from admission to stabilization and brace, traction, Philadelphia collar and spine board/bedrest temporary stabilization. The final regression model was then used to explore important predictors of the composite outcome. Regression results were summarized according to parameter estimates, associated standard errors, odds ratios (ORs) along with 95% confidence intervals (CIs) and P values.
The goodness of fit of the model was assessed by the deviance statistic and the Hosmer-Lemeshow test. 18 The Hosmer-Lemeshow test compares observed and predicted composite events, and was used to test the null hypothesis that the model’s estimates adequately fit the data. The Wald statistic for each parameter was examined to determine the significance of each individual predictor. When P values for the Wald statistic were less than .05, the corresponding predictor was considered significant after adjusting for the rest of the predictors in the model.
Missing data was assumed to be missing completely at random (MCAR) such that the missing values depended on neither observed nor unobserved information. Consequently, all data was analyzed using listwise deletion, which only considered patients with complete data across all variables. We tested the MCAR assumption using Little’s MCAR test. 19 The impact of outliers was explored through a sensitivity analysis. An additional sensitivity analysis was conducted for analyzing time from admission to stabilization as three categorical variables (<6 hours, 6 hours to 2 days, >2 days) rather than a single continuous variable.
Results
Characteristics of Study Patients
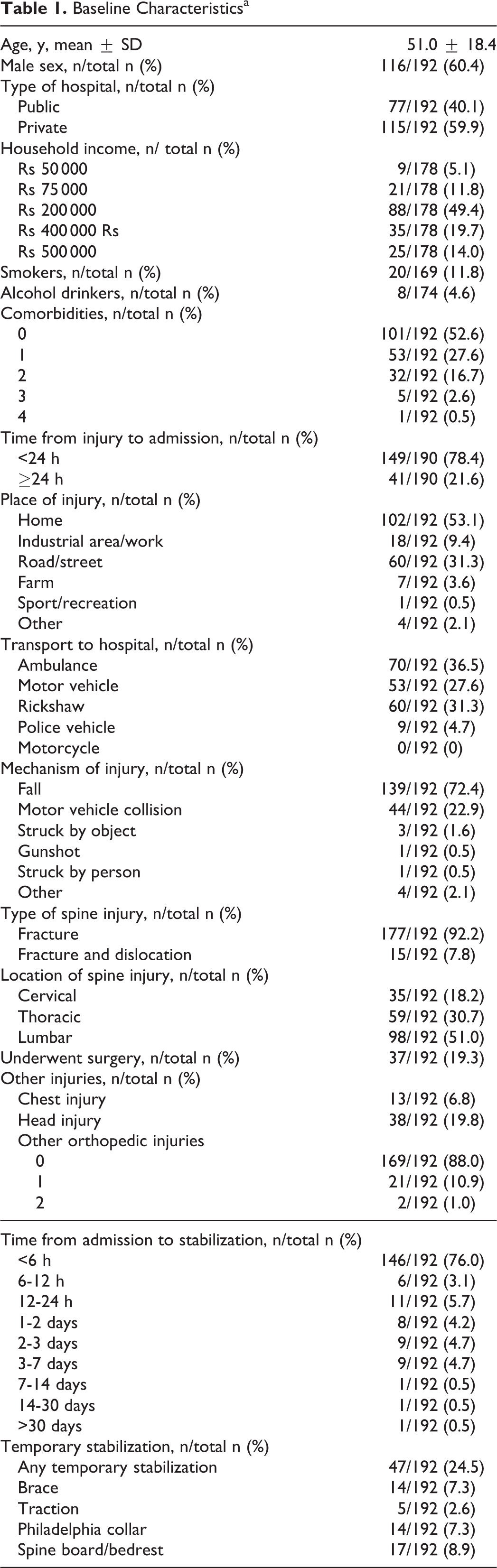
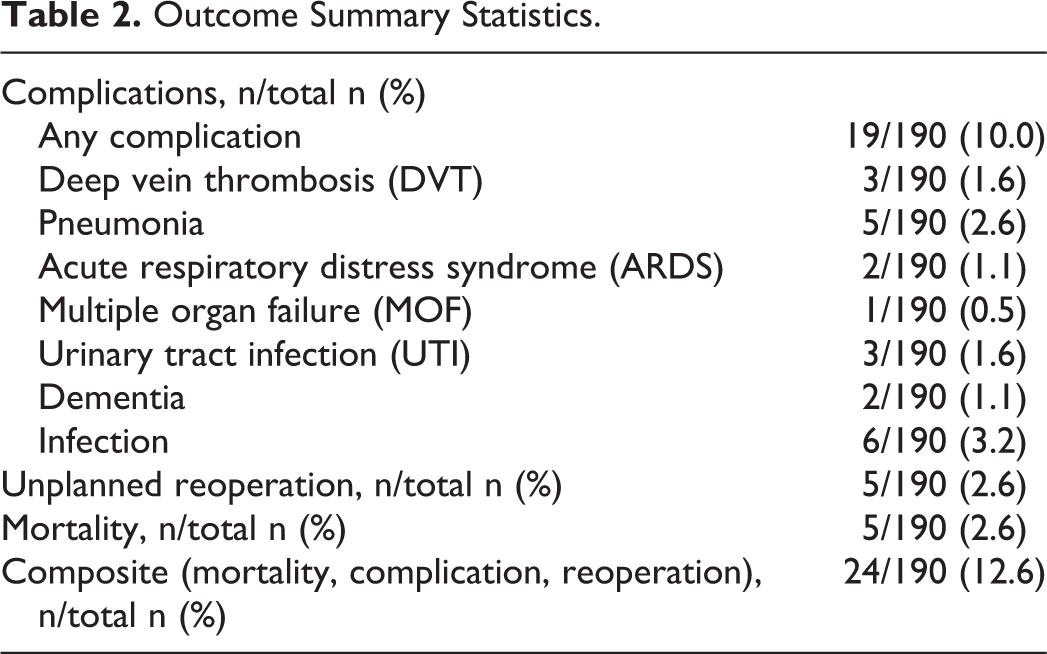
We enrolled 192 patients with spine fractures (n = 192). Baseline characteristics of the study patients are presented in Table 1. Most patients were middle-aged (mean ± SD age = 51.0 ± 18.4 years) and male (60.4%). Fractures were caused primarily by falls (72.4%) or road traffic accidents (22.9%). Treatment took place in either public (40.1%) or private (59.9%) hospitals. Cervical spine fractures were present in 18.2% of patients, thoracic in 30.7%, and lumbar in 51.0% (Figure 1). Almost one-quarter (21.6%) of patients arrived later than 24 hours, and only 36.5% were transported to hospital by ambulance. Thirty-day mortality and adverse event rate (complication) was 2.6% and 10.0%, respectively. The composite event of mortality, reoperation and complications was present in 12.6% of patients (Table 2).
Baseline Characteristicsa
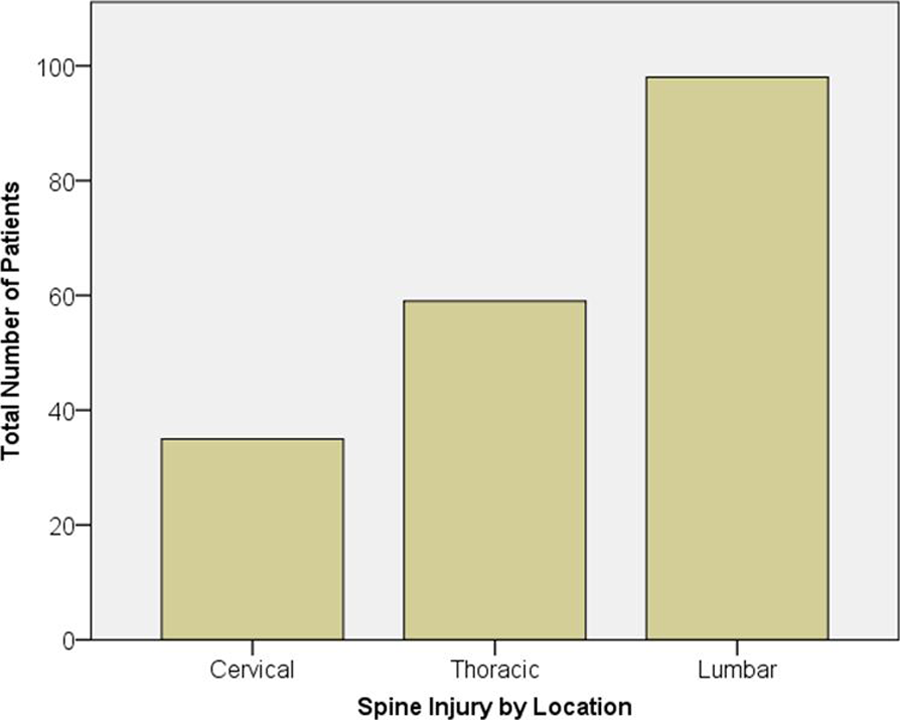
The distribution of spinal injury by location. Patients predominantly suffered fractures to the lumbar region of the spine (51.0%) followed by the thoracic (30.7%) and cervical (18.2%) regions.
Outcome Summary Statistics.
Predictors of Major Complications
Our results suggested that treatment at a public hospital (β = 1.9, P = .04, OR = 6.7, 95% CI = 1.1-41.6), the presence of chest injury (β = 2.4, P = .01, OR = 11.1, 95% CI = 1.8-66.9), and undergoing surgery (β = 1.6, P = .03, OR = 4.8, 95% CI = 1.2-19.6) significantly predicted major complications within 30 days of arrival to hospital (Table 3). Our analysis suggested a potential interaction between the decision of whether to operate and patient age indicating that increasing age increased the odds ratio for surgical status.
Logistic Regression Analysis Predicting the Composite Outcome of Death, Complications, and Reoperation.
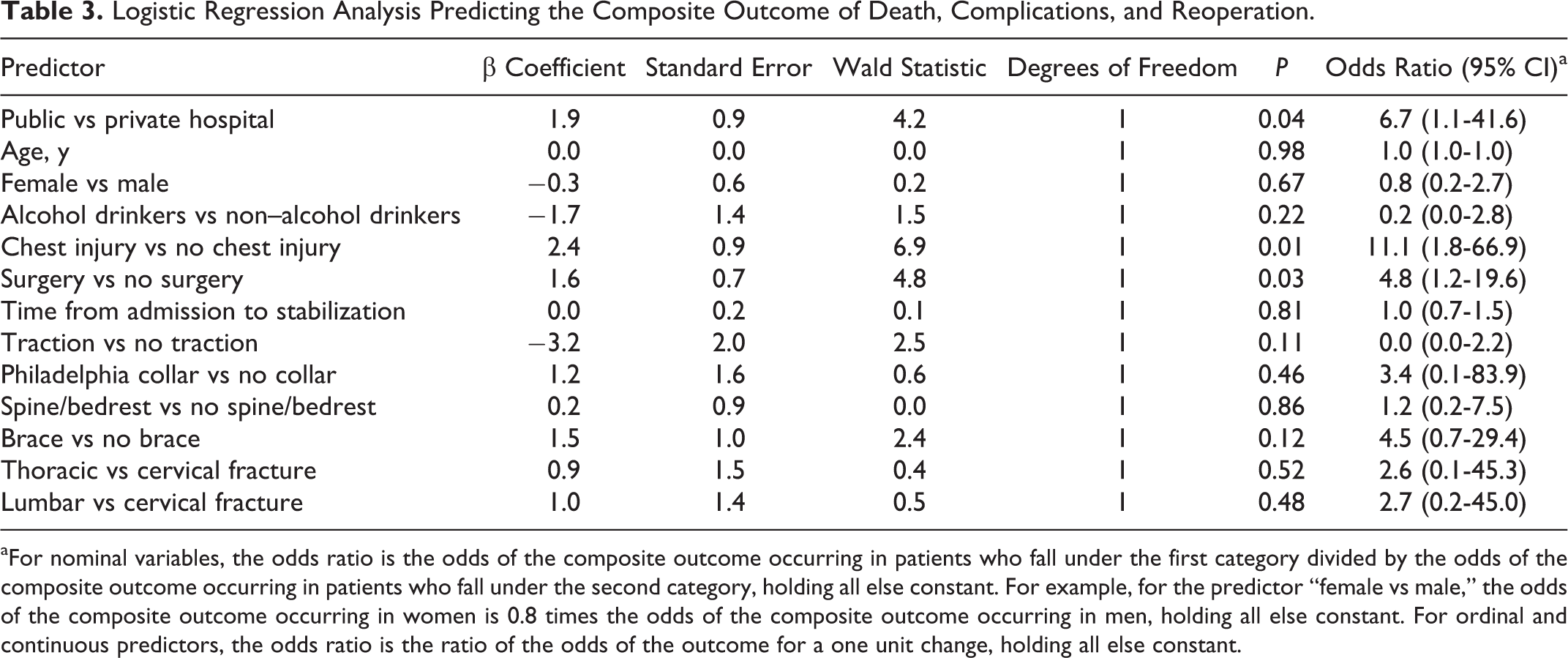
aFor nominal variables, the odds ratio is the odds of the composite outcome occurring in patients who fall under the first category divided by the odds of the composite outcome occurring in patients who fall under the second category, holding all else constant. For example, for the predictor “female vs male,” the odds of the composite outcome occurring in women is 0.8 times the odds of the composite outcome occurring in men, holding all else constant. For ordinal and continuous predictors, the odds ratio is the ratio of the odds of the outcome for a one unit change, holding all else constant.
The Hosmer-Lemeshow test (χ2 = 10.365, df = 8, P = .240) indicated that the model was appropriate. The receiver operating characteristic (ROC) curve produced from the final model with the composite outcome as the state variable and predicted probabilities as the test variable, had an area under the curve of 0.901, which can be considered outstanding (Figure 2). 18
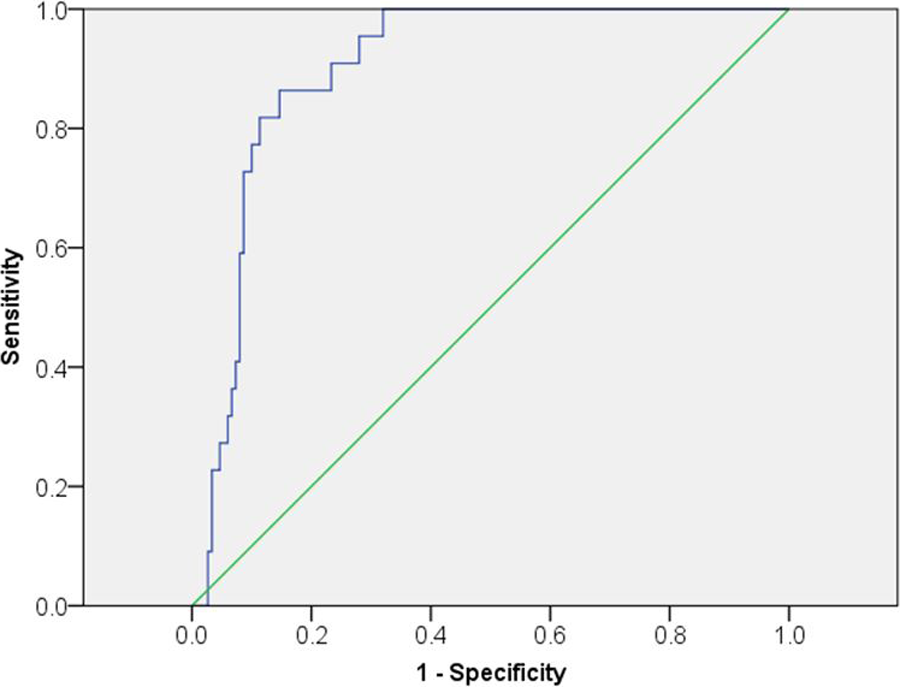
Receiver operating characteristic (ROC) curve plotting sensitivity versus 1 − specificity for various cut points with area under the curve equal to 0.901. Predicted probabilities from the final model above a given cut point were considered positive test results and when the patient also had the composite event, this was deemed a true positive. Sensitivity was then true positives divided by the total number of patients with the composite event. Predicted probabilities from the final model below a given cut point were considered negative test results and when the patient was also free of the composite event, this was deemed a true negative. Specificity was then true negatives divided by the total number of patients without the composite event. The diagonal green line is the reference line.
Completeness of Data
Using complete case analysis, 172/192 (89.6%) patients with complete data were used in the binary logistic regression for the final chosen model. One patient had a standardized residual of 3.68 and deviance residual of 2.31, which was considered extreme. The deletion of this observation caused the coefficient for surgery to become nonsignificant (P = .03 to P = .12), yet because the observation represented valid data, it was not excluded from the final analysis.
Discussion
The primary finding of the present study was that treatment at a public hospital, additional chest injury and surgical treatment significantly predicted the ensuing 30-day composite outcome comprising mortality, unplanned reoperation, and complications. However, on univariate analysis which did not control for other predictors, only treatment from a public hospital was associated with each component of the composite. In contrast, chest injury in addition to spinal fracture and surgical treatment only significantly increased the risk of complications. Consequently, the influence of these 2 predictors on the incidence of complications was likely responsible for their significant impact on the composite outcome in logistic regression. The present study also documents the demographic characteristics, mechanisms of injury, treatments provided, and 30-day outcomes from spine trauma patients in 14 hospitals in India with wide geographic distribution. We found that patients and injuries sustained were considerably different from those of developed nations, highlighting the unique challenges specific to LMIC countries. Whereas the majority of patients in our study were young males, the majority of fracture burden in developed nations involves elderly patients with fragility fractures, implying a distinctly different area of focus for patients from these countries. 20,21
Furthermore, our data suggests significant barriers to primary trauma care for spine patients. In almost one-quarter (21.6%) of all patients, hospital admission took longer than 24 hours from the time of injury. Patients waited over 6 hours from the time of admission to receive stabilization in nearly one-quarter (24.0%) of the study sample. This is considerably different from developed nations where Emergency Medical Services (EMS) generally arrive within 1 hour after an accident. 22 Out of all patients waiting more than 6 hours, over half (63.0%) of those patients waited more than 24 hours to receive stabilization. Only 36.5% of patients were transported to hospital in an ambulance and a comparable proportion (31.3%) were transported via a rickshaw. Given the magnitude of spine trauma, EMS response must improve and road systems should be developed to enable efficient access to trauma sites.
Public Versus Private Care
Our exploratory analysis found that the odds of incurring a major complication for patients treated at a public hospital, was 6.7 times (95% CI = 1.1-41.6) the odds of incurring a major complication for patients treated at a private hospital, after adjusting for other factors in the final model. Treatment at a public hospital also increased the risk of each component of the composite outcome in univariate analysis. These results illuminate the challenges facing public hospitals in India where there exists a large discrepancy in the quality of care between public and private hospitals. 23
The Indian health care system faces the challenges of a predominance of a rural population (almost three-quarters of the country’s population), low per capita income, inadequate transportation capabilities, overcrowding, illiteracy, inadequate resources, lack of supporting services such as orthopedic nursing and rehabilitation services, unstructured referral practice and a meager health insurance system. 24 The National Rural Health Mission of the Ministry of Health and Family Welfare in India state that only 10% of Indians have some form of health insurance. 24 Furthermore, specialized spine procedures, requiring a technically up-to-date infrastructure and costly implants, are practically out of reach for most patients. In rural India, the condition is even worse, as primary health centers are practically devoid of any orthopedic or spine services. 11,13
Public hospitals in India are often plagued with issues of overcrowding, understaffing, and inadequate access to certain medications. 23 These problems are compounded by a deficient health care infrastructure, which has come under scrutiny for having a high proportion of nonfunctional hospital beds and limited water and electricity. 23 Nonetheless, public hospitals are often the only affordable alternative for patients. 23 The results of the present study also add empirical support to the arguments posed by Bajpai. 23 Bajpai 23 presents 6 potential explanations for the dismal state of many public hospitals in India: (1) deficient infrastructure, (2) deficient manpower, (3) unmanageable patient load, (4) equivocal quality of services, and (5) high out-of-pocket expenditure. Interestingly, Bajpai’s solution to India’s health care woes rests less on policy and technological change and more on destabilizing the power of the elite social classes. 23 Comparatively, private and corporate hospitals are located mostly in large cities, often equipped with modern diagnostic and imaging facilities, good operating environments and intensive care units. 25 Some of them also run dedicated trauma services. However, there are no norms to govern their standards and their relations with the public trauma system. 25 Furthermore, affordability of care is a matter of concern for the low- and middle-income groups. Research that continues to emphasize the disparity in India’s health care system will be instrumental toward mobilizing policy makers and the working classes and ultimately exacting meaningful change.
The Government of India, in partnership with the Ministry of Health and Family Welfare developed a plan known as “Capacity Building for Developing Trauma Care Facilities in Government Hospitals on National Highways” beginning in 2007 and culminating in 2012. 26 The proposal, which fell under the 11th plan, aimed to create a pan-India trauma care network. The objective was to ensure that no patient would require transportation further than 50 kilometers and to have a designated trauma care facility at every 100 kilometers. Four levels of Trauma Care Centers were to be implemented ranging from level IV to level I. 26 The level IV center was to essentially be a mobile hospital ambulance provided by the National Highways Authority of India. Level III Trauma Care Centers would provide initial stabilization followed by definitive and comprehensive care at levels II and I centers. Level I centers would be designated for trauma super specialties. 26 The health care received by spine trauma patients would still vary between public and private hospitals under this framework. Spine trauma patients in the public hospitals are admitted to a trauma unit first and then may be transferred to a spine ward. Usually, spine units in public hospitals are small with limited beds. In contrast, the private hospitals all have special spine units. An additional 85 trauma care facilities are to be instituted under the 12th plan, spanning the years 2012 to 2017. 27
The Role of Prehospital Immobilization
This study further found that of 18.2% of patients that sustained cervical spine fractures, only 44.4% were immobilized in a cervical collar on presentation to hospital. However, we found no association with immobilization in a cervical collar and development of the composite outcome, which is remarkably different from standard protocol in North America where the vast majority of institutions mandate prehospital immobilization on arrival to hospital in patients with suspected spinal injuries. 28 Despite its widespread use, however, the clinical benefits of routine prehospital spinal immobilization have recently been questioned. 29,30 Hauswald et al 31 argue that spinal cord damage is done at the time of injury and subsequent movement is generally not sufficient to cause further damage. Furthermore, trauma patients may have fractures or ligamentous injuries to the spine that may not cause inherent instability, and hence will not benefit from immobilization. It has been estimated that over 50% of trauma patients in North America with no neck or back pain are transported with full spinal immobilization. 32 Previous retrospective studies have reported numerous adverse events with spinal immobilization, including airway difficulties, increased intracranial pressure, increased risk of aspiration, restricted respiration, dysphagia and skin ulceration. 33 –39 Additionally, it has been suggested that prehospital spinal immobilization has never been shown to affect outcome and that estimates in the literature regarding the incidence of neurologic injury due to inadequate immobilization may be overrepresented. 31,40,41 This data questions the present routine use of prehospital spinal immobilization. In a Cochrane Review updated in 2009, Kwan et al 42 searched the literature and found a paucity of evidence for or against the routine use of pre-hospital immobilization in spine trauma patients. The majority of studies were retrospective in nature and no randomized trials were reported. The authors highlighted the need for large prospective studies to compare different immobilization protocols on clinically important outcomes, and further validate the decision criteria in patients with high risk of spinal cord injury. 43 Given that a randomized trial may not be feasible in trauma patients due to ethical considerations, as well as the fact that the medical and legal concern of missing a cervical spine injury warrants strong support for liberal use of spinal immobilization, a large-scale multicenter international prospective study is warranted to further elucidate the practice of prehospital spinal immobilization on rates of mortality. 34
Age and Mortality
This study further found that age modified the relationship between surgery and the composite outcome. Surgery shared a greater association with developing a composite event for older patients relative to younger patients. This finding strengthens the long-held belief that a decision to perform surgery in elderly patients should be considered prudently. 44,45 Furthermore, increasing age may predict surgical mortality and morbidity. One retrospective study demonstrated an increase in surgical morbidity of 0.71% per year for patients between the ages of 20 and 99 years. 46 Turrentinie et al 46 discuss that elderly patients often present with extensive comorbidities, which can complicate surgical procedures. Although increasing age is associated with other risk factors for surgical mortality and morbidity, increasing age itself was shown to be an independent predictor of these adverse outcomes. 46 The authors hypothesized that as patients age, their ability to satisfy the functional demands of an operation is diminished. The ramifications of such a finding are far-reaching and highlight the need for careful preoperative evaluation in geriatric surgical care, including adequate risk assessment with special attention being paid to risk factors or other preexisting comorbidities. 46
Limitations
The primary limitation of this exploratory investigation is low sample size and a particularly low total event rate (24 total composite events). In logistic regression, parameters are estimated using maximum-likelihood estimation, which is an approximate large sample method. In small samples, this method tends to become unstable. 18 Moreover, another drawback of the study relates to clustering effects. Patients were recruited from 14 hospitals in India and therefore patients within a given hospital may be more alike than patients in different hospitals. The regression methods employed in this analysis tend to ignore the correlation of outcomes that are expected within each hospital and tend to underestimate the standard errors. Consequently, an alternative approach would be to use multilevel analysis, which accounts for clustering. Future investigations in this area will clearly record and adjust for the specific center or hospital to which a patient presents. Furthermore, this study only looked at a follow-up period of 30 days, so it is possible that complications occurring beyond this period would not be captured by this study. The primary mortality window for these injuries, however, is within 27 days of trauma, so it is anticipated that the majority of outcomes will be captured in the 1-month time frame. 47
Finally, although surgery was an independent risk factor for major complications, findings must be interpreted with caution. It is possible and likely that patients that underwent surgery had a higher proportion of unstable spinal injuries or greater neurological compromise preoperatively. This study did not take into account spinal stability or presenting neurologic status after injury. These factors, specifically higher American Spinal Injury Association (ASIA) grade, high cervical injury or injuries where spinal stability is compromised may be risk factors for early mortality and would need to be accounted for in a larger future study. 48 Moreover, in univariable analysis, surgery did not significantly increase mortality. Instead, a patient’s operative status was more influential toward incurring nonfatal complications. Finally, it is important to emphasize that this investigation was exploratory in nature due to a low total event rate. Consequently, any definitive conclusions regarding the risks of surgical treatment should be withheld until further research is conducted.
Conclusions
In summary, for patients with spinal fractures in an LMIC, treatment in the public health care setting, additional chest injury and surgical treatment are predictive of adverse outcomes within thirty-days. There is currently a need for a large-scale, global, prospective, multicenter study taking into account spinal stability and neurologic status to definitively quantify the global burden of spine trauma and identify modifiable factors that predict all-cause mortality. The results of such a study will not only inform the current magnitude and prognostic factors for outcomes following spinal trauma in LMICs, but will also provide direction for future policy and research initiatives critical to mitigate the burden of spinal injury worldwide.
Footnotes
Appendix
List of Study Centers (and Catchment Area Population) in India (Total Catchment = 55 268 093 People).
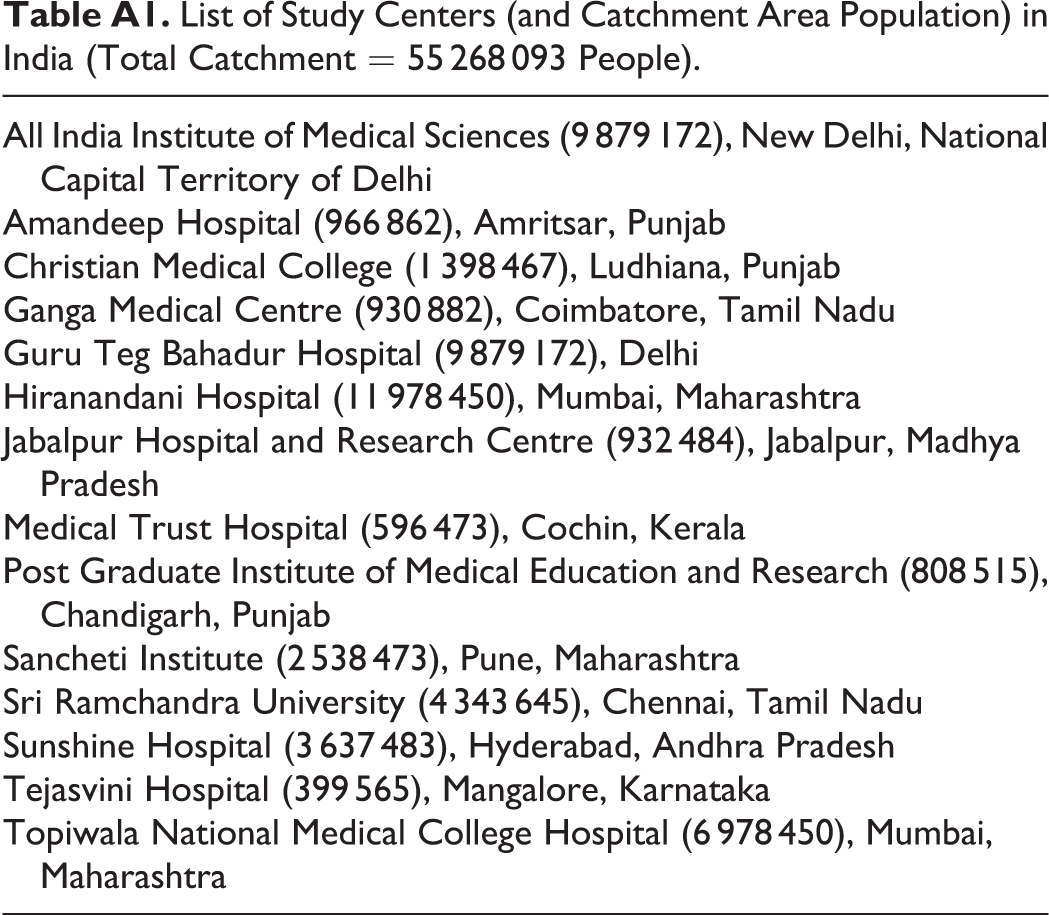
| All India Institute of Medical Sciences (9 879 172), New Delhi, National Capital Territory of Delhi |
| Amandeep Hospital (966 862), Amritsar, Punjab |
| Christian Medical College (1 398 467), Ludhiana, Punjab |
| Ganga Medical Centre (930 882), Coimbatore, Tamil Nadu |
| Guru Teg Bahadur Hospital (9 879 172), Delhi |
| Hiranandani Hospital (11 978 450), Mumbai, Maharashtra |
| Jabalpur Hospital and Research Centre (932 484), Jabalpur, Madhya Pradesh |
| Medical Trust Hospital (596 473), Cochin, Kerala |
| Post Graduate Institute of Medical Education and Research (808 515), Chandigarh, Punjab |
| Sancheti Institute (2 538 473), Pune, Maharashtra |
| Sri Ramchandra University (4 343 645), Chennai, Tamil Nadu |
| Sunshine Hospital (3 637 483), Hyderabad, Andhra Pradesh |
| Tejasvini Hospital (399 565), Mangalore, Karnataka |
| Topiwala National Medical College Hospital (6 978 450), Mumbai, Maharashtra |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by Regional Medical Associates, AO International, Hamilton Health Sciences Trauma Fund, and a Canada Research Chair.