
Abstract
Introduction
A mass-casualty incident (MCI) is an emergency in which the number of casualties exceeds the available medical resources (Einav et al., 2004; Rimstad & Braut, 2015; Rimstad & Sollid, 2015). Managing the pre-hospital response of emergency medical services (EMS) is a challenge for MCI commanders and requires them to cope with a lack (Rimstad & Sollid, 2015) or excessive amount of information and limited resources (Perry, Jaffe, & Bitan, 2019). Thus, improving the MCI commander’s decision-making process is vital, and exploring the differences between novice and expert commanders’ decision-making processes can potentially improve novice commanders’ training.
The differences between novice commanders and experienced commanders were explored (Berndt & Herczeg, 2019) previously based on the Situational Awareness theory (Endsley, 1995, 2021). The main differences were in the ability of incident commanders to perceive changes in the MCI, comprehend their effects, and project their consequences. In contrast, preliminary leaders could only perceive changes. Perry, Jaffe, & Bitan (2022a) used quantitative data from MCI field simulations to explore the decision-making process of paramedic students at the end of their MCI management qualification harnessing the “dual-process” model (Kahneman, 2003; Norman, 2009). Because field simulations are known to improve communication skills (Gordon et al., 2016; Jorm et al., 2016), knowledge (Zinan, Puia, & Kinsley, 2015), clinical skills (Currie, Kourouche, Gordon, Jorm, & West, 2018), and performance (Bajow, Alassaf, & Cluntun, 2018), they provide the most realistic exposure to gain experience toward managing a real MCI (Gillett et al., 2008).
The "dual-process model" represents two decision-making processes known as System 1, which is an “instantaneous” process, and System 2, which is a "considered" process and it is widely used to model, analyze, and explore medical decision-making processes (Croskerry, 2009; Djulbegovic, Hozo, Beckstead, Tsalatsanis, & Pauker, 2012; Marcum, 2012; Tsalatsanis, Hozo, Kumar, & Djulbegovic, 2015). Perry, Jaffe & Bitan (2022a) found that the decision-making process of paramedic students changes over the MCI timeline. At first, commanders rely on the MCI protocol, which guides them during the chaos and uncertainty that characterizes the first moment after arrival to a MCI (i.e., System 1). As the event unfolds, a commander responds immediately (i.e., System 1) to new information and, toward the end, initiates actions without any new information (i.e., System 2).
The goal of this study was to explore the conditions under which veteran paramedic and paramedic students utilized System 1 and System 2 responses, and to elucidate the differences between experts and novice commanders’ decision-making processes.
Methods
As this study followed previous paramedic students’ decision-making while managing an MCI (Perry, Jaffe, & Bitan, 2022b), it utilized a data collection method dedicated for MCI simulations that was previously harnessed (Perry, Jaffe, & Bitan, 2022a).
Study Design
Two data sets of MCI simulations were used, one of paramedic students and a second of a veteran paramedic. The simulation was divided into interactions, defined as "information exchanges between two or more persons without an interruption”. Each interaction was first tagged as a cue or an action. A cue was defined as “input of verbal, visual, and/or auditory information”. An action was defined as “an order given by the commander” For example, an interaction initiated by the commander to upload a casualty to an ambulance was tagged as an action.
Two categories of cues were defined: cues with a following response, and cues without a response. This distinction was based on the assumption that a response indicates that the commander managed to complete a decision-making process (e.g., managed to find a solution to a certain problem). Following the definitions of cues, three action categories were defined: a response following a cue, an action without a cue, and an action following the MCI protocol. The three categories were differentiated according to the following assumptions. An action following the protocol was defined “as an action that was included in the EMS MCI protocol and was performed without any cue”. The other two categories of initiated action, following a cue and without a cue, referred to interactions whose content was not included in the MCI protocol. These two categories differed by the presence of the stimuli that triggered the action following a cue and by the stimuli that were missing from the action without a cue.
Normalization Method
To compare different simulation timelines, each timeline was normalized into time frames. Let
MCI Simulations
Data from eight MCI simulations of paramedic student were collected. These simulations were part of a paramedic MCI training course, in which most of the students were medics in the EMS, with 2 or 3 years of experience as military medics, but no experience as MCI commanders. The exercised scenario was a simulated missile attack on an urban area and included approximately 20–30 actors as casualties. The local EMS participated in the simulation and provided all the necessary resources (e.g., ambulances, drivers, medics, stretchers, and communications equipment). In addition, a dedicated dispatch was assembled in the EMS dispatch center to communicate with the MCI commander.
The data of the veteran paramedic is a part of the yearly operational EMS training. The exercised scenario was a terror incident at a live concert and included 40–50 actors as casualties and 100 actors as a crowd. In these events, a dedicated EMS team is deployed to provide medical and evacuation services in case of a medical event or an MCI. The setup included several medical units scattered at the concert area, a pre-made treatment and evacuation plan, and an experienced commander qualified to manage an MCI. The data of all simulations were tagged interdependently by two observers (O.P. and T.K.) using OBSERVER XT software. A third observer (Y.B.) resolved any disagreements.
Statistical Analysis
Based on the normalization method, cues, action following a cue, action without a cue, and action following protocol were divided into time frames and are reported by means and standard deviations (standard deviations were not calculated for the veteran paramedic since the data include a single simulation). Time frames were divided into the three MCI management phases: (1) evaluation and triage, (2) treatment and preparedness for evacuation, and (3) evacuation according to casualty priority. Matplotlib and Statistics Python packages were used for statistical analysis and graphing.
Results
The data for this study included two data-sets, the first of paramedic students, which was presented in Perry, Jaffe & Bitan (2022a) and included eight simulations with an
Interaction Sub-Category Division.

Paramedic Students’ Decision-Making Analysis
Both the overall number of cues and the overall number of actions increased towards the treatment phase, reaching mean peaks of 4.98%±1.36% and 6.14%±2.04%, respectively, and decreased as the second phase unfolded. As the third phase began, overall actions and cues peaked at mean values of 4.73%±2.05% and 6.95%±2.32%, respectively. The actions following the protocol were at their peaks at initiation of the simulations, at 2.65%±1.33%, and decreased as the simulations proceeded. In contrast, actions without a cue increased as the simulations unfolded and peaked in the 80%–90% time frame, at 2.57%±1.60%. The number of responses following cue maintained similar trends as actions and cues, at 5.24%±1.79% in the 30%–40% time frame, and at 4.38%±3.09% in the 80%–90% time frame. Cues without a response increased toward the 40%–50% (1.39%±1.40%) time frame and maintained similar trends to the end of the simulations. Figure 2 represents the average percentage (black bars) across the different MCI phases.
Veteran Paramedic Decision-Making Analysis
Although this part of the data is based on a small sample, these preliminary results present different patterns. Both actions and cues show a similar trend over the simulation timeline. Both increased toward the end of the first phase peaking at the 40%–50% time frame with 10.52% and 3.15, respectively. From the 50%–60% time frame, both gradually increased until the end of the simulation. Actions without a cue maintain a similar trend as the actions, peaking at the end of the second phase with 6.31% and the 40%–50% time frame with 7.89%, and gradually increasing from the 50%–60% time frame until the end of the simulation. Responses to cues peaked at 40%–50% with 2.63% and maintained a similar trend until the end of the simulation. Actions following the protocol are mostly dominant in the first phase, reaching a peak at the 10%-20% time frame with 6.84%. Cues without responses maintain a similar trend over the simulation timeline, ranging from 0% to 0.52%. Figure 2 represents the average percentage (grey bars) across the different MCI phases.
Discussion
This study’s results reveal the difference between the decision-making process of paramedic students and veteran paramedics (Figure 1). Two main findings may shed light on these differences. First, for paramedic students, the triggers for most actions are cues received from team leaders and EMS team members. Thus, the commander utilized the cues to manage the MCI that fits System 1. For the veteran paramedic, most actions were initiated without a preliminary cue, indicating that fewer cues were required to manage the MCI, which fits System 2. In addition, the veteran paramedic was able to shift between MCI phases more quickly than the paramedic students.
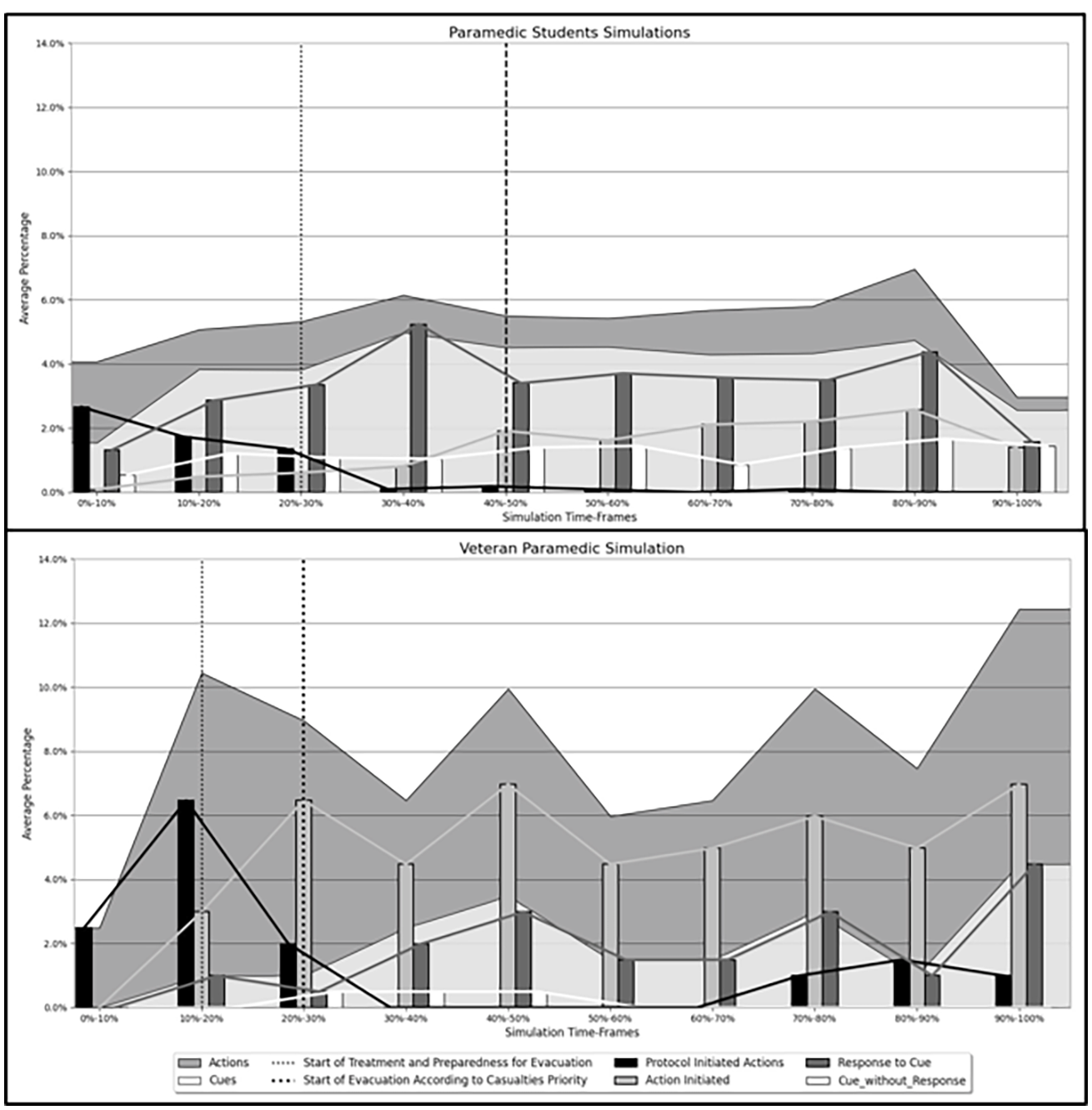
Paramedic Students’ (Top Graph) and Veteran Paramedic’s (Bottom Graph) Decision Making.
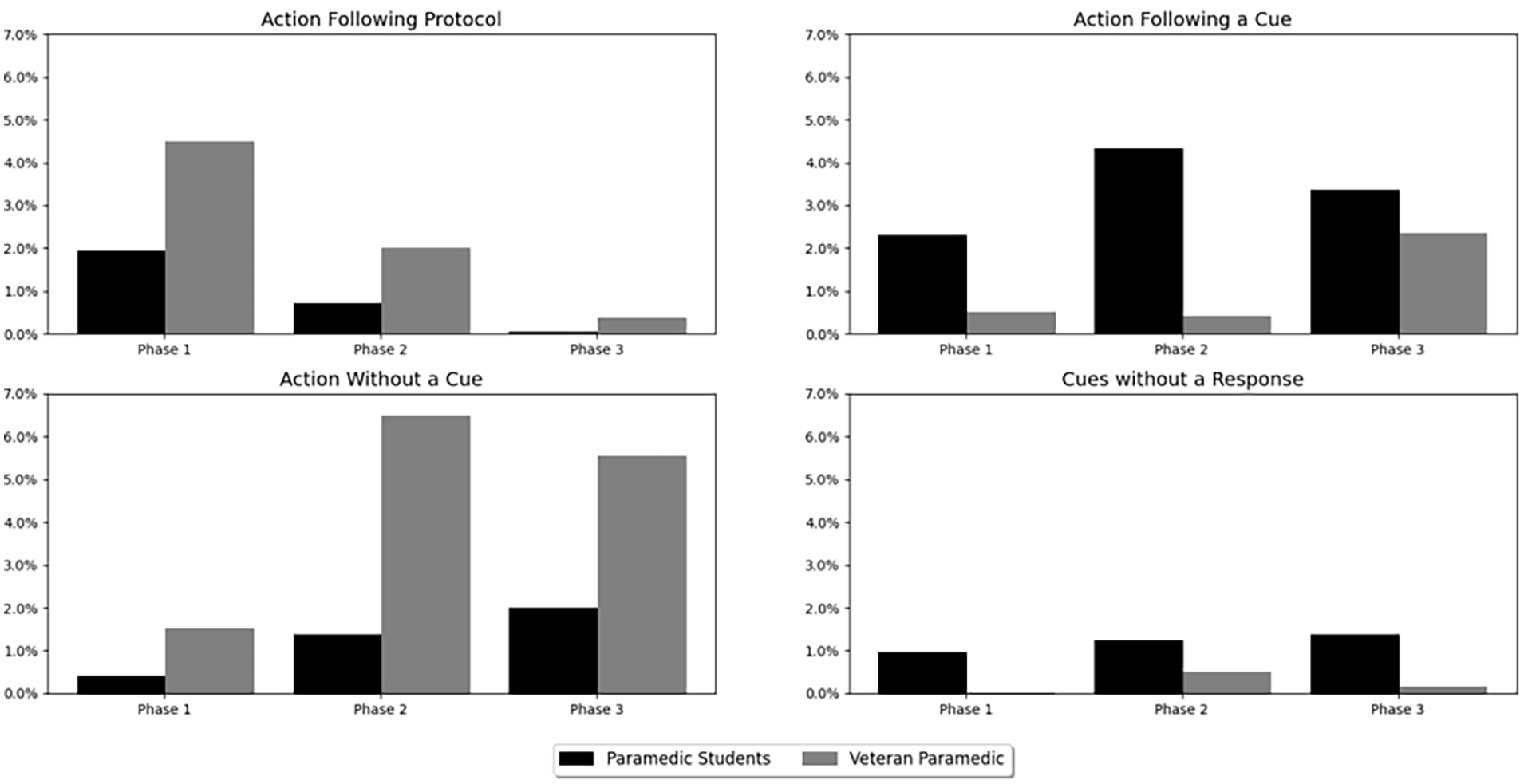
Paramedic Students’ and Veteran Paramedic’s Average Percentage Actions Following Protocol, Action Following a Cue, Action Without a Cue, and Cues Without Response.
These findings align with previous results indicating that expert paramedics operate more strategically than novice paramedics (Smith et al., 2013). In terms of Situational Awareness (Endsley, 1995, 2021) and the Recognition Primed Decision-Making framework (G. Klein, 1999; G. A. Klein, Calderwood, & Macgregor, 1989), it can be assumed that the experience of the commander allows projection generation (i.e., Situational Awareness Level-3) or to integrate and follow only the required information on the time to shift between phases.
The second finding is that the veteran commander utilized the MCI protocol and then shifted to initiated actions versus the paramedic students who utilized the protocol, but then waited for cues to arrive before making a response. As mentioned above, it can be assumed that the expertise of the expert allowed him to recognize the situation easily and to recall what possible actions can be performed to manage the MCI. Similar findings were reported by Berndt & Herczeg (2019), in which experienced MCI commanders demonstrated better situational awareness than preliminary leaders with no experience.
An additional finding is the number of cues without a response. For paramedic students, there is a consistent trend of receiving cues without a response in contrast to the veteran paramedic, in which there were almost no cues without a response. If a cue did not yield a response, it might indicate that it was ignored or did not perceive. The ability to ignore a cue was observed as an advantage of experts to ignore cues that are not relevant to the problem at hand (G. Klein, Pliske, Crandall, & Woods, 2005). A cue that was not perceived could be due to working memory limitations - number of stored items (Wickens, Helton, Hollands, & Banbury, 2021) or items decay (Brown, 1958; Peterson & Peterson, 1959), lack of required encoded knowledge in the long-term memory (Barsalou, 2008, 2010), or high mental workload (Wickens, 2002, 2008).
Lastly, there is a difference in the quantities of the actions and cues. While the action and cue trends are similar, the quantities differ. The veteran paramedic simulation included more actions than the paramedic students’ simulations. This could be explained by the complexity of the MCI (i.e., the number of casualties in the MCI) (Busby & Witucki-Brown, 2011). Since there were more casualties, it is safe to assume that more information must be controlled, resulting in more procedures and actions that needed to be performed.
This study’s contribution in evaluating the differences between novice and expert commander decision-making can serve as a paradigm for researchers, trainees, and instructors to assess current decision-making skills and the required level of decision-making skills (i.e., how experts make decisions while managing an MCI). Instructors should utilize this study’s results as a benchmark for their trainees’ decision-making and to strive for expert decision-making at the end of a qualification or operational training.
Like any study, the analysis method used in this study has limitations. In our simulation, information exchanges were mostly verbal, aside from a few cases where interactions were tagged as responses to visual input (e.g., the commander pointed to specific casualties and asked the team to evacuate them). The assumption that there could have been cases where verbal interactions, combined with visual inputs, led to a response should be considered. Thus, the assumption that commanders acquire visual data should be considered and reviewed in post-simulation interviews. An additional limitation is the sample size of the veteran paramedic simulation, which due to logistics and administrative challenges included only one simulation. Lastly, the method made it difficult to differentiate between a cue that was not perceived or was ignored. Post-simulation interviews or questionnaires could shed light on the reason for cues without a response. Future studies should be based on more experienced MCI simulations to further explore the differences between novice and expert MCI commanders.
Footnotes
Acknowledgements
This study was conducted as part of SimReC - The research center for simulation in healthcare at Ben-Gurion University of the Negev. The contribution of Heli Bergman and Michal Hergas to the manuscript is acknowledged with gratitude.