
Abstract
Pediatric burn injuries are a global health concern that significantly impacts children’s well-being. Few cost-effective psychosocial interventions currently exist that focus on bolstering resilience in pediatric burn survivors and their surrounding support systems, specifically in resource-constrained contexts. Therefore, this study sought to explore caregivers’ perceptions of an existing resilience-themed multimedia psychosocial intervention aimed at child burn survivors. This qualitative study’s design was exploratory and utilized face-to-face, semistructured interviews. The caregivers of 13 child burn survivors were recruited from the Red Cross War Memorial Children’s Hospital, South Africa. Thematic analysis yielded four themes revealing some key caregiver perceptions of the burn recovery video: (1) acceptance of burn injury promotes psychological recovery; (2) hope matters; (3) emotional support matters in all contexts; and (4) resilience matters, but… The themes echoed the resilience literature and emphasized the importance of support from all systems, including professional, and peer and familial groups, in postburn recovery. They also identified areas not usually foregrounded, such as the social contexts which may mitigate against resilience. Caregivers distilled some key aspects of resilience from the multimedia intervention and through this felt encouraged about the recovery process. The findings highlight the importance and utility of resilience-orientated multimedia and complementary interventions in pediatric postburn care.
Implications for Impact Statement
The study’s findings highlight the importance of incorporating resilience strengthening into postburn recovery as well as the need for complementary interventions to support pediatric burn care. Importantly, the study findings caution against social contexts which may undermine resilience and postburn recovery.
The study’s findings highlight the importance of incorporating resilience strengthening into postburn recovery as well as the need for complementary interventions to support pediatric burn care. Importantly, the study findings caution against social contexts which may undermine resilience and postburn recovery.
Pediatric burn injuries are a global health concern (World Health Organization [WHO], 2018) that result in around 2.5 burn deaths per 100, 000 population, but this is much higher in Sub-Saharan Africa, at 4.5 burn deaths per 100, 000 (Sengoelge et al., 2017). These injuries occur in the context of increasingly limited health resources globally (Riley & Freeman, 2019), especially in resource-constrained contexts like South Africa, with an increase in the burden of care for caregivers and other social and health support systems involved in pediatric care.
There are significant psychological outcomes that may follow pediatric burn injuries, ranging from common mental health diagnoses such as depression, anxiety and posttraumatic stress reactions, as well as impacts on other aspects of psychological well-being, such as self-esteem and self-concept (Woolard et al., 2021). Caregivers themselves face significant and multiple psychological challenges after a child sustains a burn injury. Studies have shown that caregivers tend to report incidents of depression, anxiety, emotional distress and feelings of guilt following the injury (Bakker et al., 2013; Bronner et al., 2010), with up to 47% of parents developing posttraumatic stress disorder (PTSD) (Hall et al., 2006). According to Rencken et al. (2021), the primary challenges caregivers face consist of stigma, difficulty accepting their caregiving role, a decline in personal relationships, the financial and emotional consequences of being unable to return to work, and difficulties managing long-term aftercare at the hospital outpatient clinic.
Psychological support for both children and families is vital to enhance better treatment and recovery outcomes (Van Niekerk et al., 2020; Woolard et al., 2021). Effective pediatric burn care necessitates interventions from multiple systems associated with children, including caregivers (Ohgi & Gu, 2013; Van Niekerk et al., 2020), professional health staff (Hornsby et al., 2020; Woolard et al., 2021), school facilitators (Christiansen et al., 2007; Rosenberg et al., 2006), and groups addressing peer reintegration challenges due to stigma and bullying concerns (Van Niekerk et al., 2020; Woolard et al., 2023). The effective utilization of these systems is crucial to facilitate children’s psychosocial rehabilitation (Van Niekerk et al., 2020). However, global changes in health care, like budget cuts (Druery et al., 2017; Rencken et al., 2021), place a greater burden of care on all pediatric care systems (Rencken et al., 2021; Thomson et al., 2015). Providing optimal health care for pediatric burn injuries in this context faces significant challenges. Medical care is sometimes compromised (Allorto et al., 2023; Van Niekerk et al., 2020) and psychological interventions are sometimes seen as a luxury (Rencken et al., 2021).
A recent systematic review (Hornsby et al., 2020) is indicative of the paucity and range of available psychological interventions for children. They identified a total of only 27 eligible studies, which were grouped into three categories, namely, distraction studies, residential boot camps, and other psychological interventions. There were only four studies in the latter category (two categorized as cognitive behavior therapy (CBT) and two categorized as parent group counselling). While the study attested to the efficacy of distraction studies for pain management and reducing anxiety, it also pointed to the promise of the latter two categories as well as highlighted the need for interventions that target other psychological sequelae. As the studies indicate, the focus on coping strategies and reducing psychological distress is effective and can even bolster resilience (Patel et al., 2022; Woolard et al., 2021). However, it remains unclear whether these interventions are explicitly guided by a resilience framework, a promising conceptualization from which to inform recovery interventions (Kornhaber et al., 2016). Resilience has commonly been described as the ability to bounce back after a traumatic injury (Smith et al., 2010). Social ecological resilience perspectives underscore the importance of both individual and contextual factors like social support to fostering resilience (Foster et al., 2019). Importantly, these perspectives highlight the potential to strengthen the interaction between individuals and their environment, modify risk and protective processes, and provide resources that can support positive adaptation and wellbeing for caregivers and families dealing with the aftermath of the traumatic event.
While there is still limited data on the efficacy of resilience-informed burn recovery interventions, the evidence from incorporating resilience in postburn recovery seems promising. In their systematic review of posttraumatic growth (PTG) and resilience after burn injury, Woolard et al. (2022) suggest that while factors such as age and total burn surface area (TBSA) mediate resilience and PTG, adaptive coping mechanisms and social support are strongly associated with these outcomes. The study highlights that resilience-informed interventions should focus on social support, coping styles, and deliberate positive introspection (Woolard et al., 2022). Similarly, in an integrative study of the role of resilience in burn recovery, Kornhaber et al. (2016) identified three key themes, namely, relational strengths, positive coping, and resistance to trauma symptoms. Interventions incorporating these components show promise (Wickens et al., 2024), including those targeted at families (Asefnia et al., 2025; Sveen et al., 2017), with a recent randomized control study (Hosseini et al., 2025) showing significant differences in maternal resilience after exposure to a resilience building intervention.
Support systems, especially those comprising caregivers, are critically important for child burn recovery and responsible for providing proper burn treatment, facilitating aftercare, and providing comfort during hospitalization (Van Niekerk et al., 2017). While many caregivers may demonstrate resilience and adjust well following their child’s burn injury (Quezada et al., 2016; Woolard et al., 2021), they also face numerous obstacles to the provision of support, especially in low-income contexts, such as competing domestic, family, and work expectations, that may impact childcare, supervision, and support (Van Niekerk et al., 2017). Therefore, the access of caregivers to a range of support networks, including immediate family members, local communities, and professional support systems are all crucial to enable their support of the injured child (Rencken et al., 2021; Van Niekerk et al., 2017), especially in resource-constrained contexts. There is an apparent lack of any complementary resilience informed interventions that could potentially be utilized with multiple support systems involved in pediatric care, despite the call for this by Woolard et al. (2022). Furthermore, cost-effective and accessible interventions are a priority in pediatric care and needed to significantly increase its reach and impact among burn survivors (Jefferis et al., 2019).
The intervention utilized in the current study was developed to address this gap. It was created by Ashley van Niekerk., who is Director of the SAMRC-Unisa Violence, Injury and Social Asymmetries Research Unit, and has led several psycho-social and public health studies into child burns, their causation and the opportunities and barriers to prevention (Van Niekerk, 2022). The intervention is a roughly 3-minute animation video that is narrated in English and portrays a story of psychosocial resilience and positive recovery after a burn injury, from the perspective of an adolescent boy’s experiences a few years ago. It combines psycho-educational and supportive messages to instill hope and mobilize support in both burn survivors and others affected, including friends, teachers, health professionals, parents, and caregivers (van Niekerk et al., 2020). There are four key aspects to this intervention, namely, that it is a (1) multimedia intervention, (2) it uses animation in depicting the different support systems for a child recovering from a burn injury, (3) it highlights how these support systems can be harnessed to facilitate recovery, and (4) it foregrounds resilience. Resilience is portrayed in various ways with the primary narrative showing how a child burn survivor overcomes challenges through support, to success as a youth some years later. Positive portrayals of support and positive outcomes are portrayed in different postburn scenarios.
The aim of the video is thus to support the early recovery of child burn survivors and their caregivers by focusing on cultivating hope and activating social support, drawing from ecologically oriented definition of resilience (Ungar, 2013). It was designed as a complementary, cost-effective, resilience informed intervention that could be used by multiple child support systems, especially in resource-constrained contexts.
The purpose of the current study was to understand how this intervention, aimed at child burn survivors and their surrounding support systems, including families, peers and professionals, was experienced specifically from the caregiver’s perspective. We focused on caregivers’ general perceptions of this multimedia intervention and not its potential impact on resilience or its efficacy. Specifically, we explored the extent to which the resilience messages that were integrated into the intervention were experienced by them. Two other studies that are part of our research have similarly focused on other pediatric care systems, specifically involving nurses (Matsana, 2023) and teachers (Wilson, 2023). The aim of this line of research is to assess perceptions of the intervention’s acceptability, relevance, and potential utilization in pediatric burn care.
The present study’s objectives include the following: (1) to explore the perceptions of a multimedia intervention from caregivers currently accessing postburn care in a public hospital, and (2) to explore whether caregivers distilled messages of psychosocial resilience from the video clip, as a way of informing future interventions in postburn recovery.
Methods
Design
This study was grounded within a qualitative approach, using semistructured individual interviews with caregivers.
Sampling
Participants were recruited at the Red Cross War Memorial Children’s Hospital, the largest dedicated pediatric hospital in South Africa, situated in Cape Town. The study made use of convenience sampling to select participants who were the primary caregivers of a child who had sustained a burn injury and were seeking postburn outpatient treatment at the hospital. This typically ranges from 4 weeks up to 2 years and includes both medical as well as allied health services. Inclusion criteria included being the primary caregiver for a child burn survivor younger than 13 years, aligning with the hospital’s policy of only admitting children up to the age of 12 (Red Cross War Memorial Children’s Hospital Outpatients Department Booklet, 2014). Since the study assessed caregiver perceptions of the intervention, criteria like severity of the burn injury, length of time since the injury, and the presence of either psychological symptoms or resilience were not screened. While it was a convenience sample, only caregivers currently accessing postburn rehabilitation support were chosen to create sample homogeneity. Their proximity to the burn events would also facilitate potentially richer data. An additional consideration was the recruitment of caregivers from resource-constrained contexts, as this group remains an important target for the intervention. The Red Cross War Memorial Children’s Hospital is a public facility that traditionally serves low socio-economic families from Cape Town and beyond who do not have private health insurance. Affluent families are far more likely to access burns treatment in the private health care system.
Selection Procedures
Participants were recruited during their follow-up appointments at the outpatient burn clinic with the assistance of the nurse on duty. The nurse approached caregivers who were waiting to see the outpatient hospital staff. The recruitment rate was 87.5% (16 were approached and 14 agreed to participate). One declined due to having another ill child in their care when approached, and one other caregiver declined participation without elaborating further. Once their availability was confirmed and after a briefing on the study and informed consent, the participants were requested to watch the multimedia intervention video and immediately thereafter to participate in an interview (for additional details about this video, please see van Niekerk et al., 2020; the video may be viewed at https://youtube/7m0YVtpVePo).
Demographics
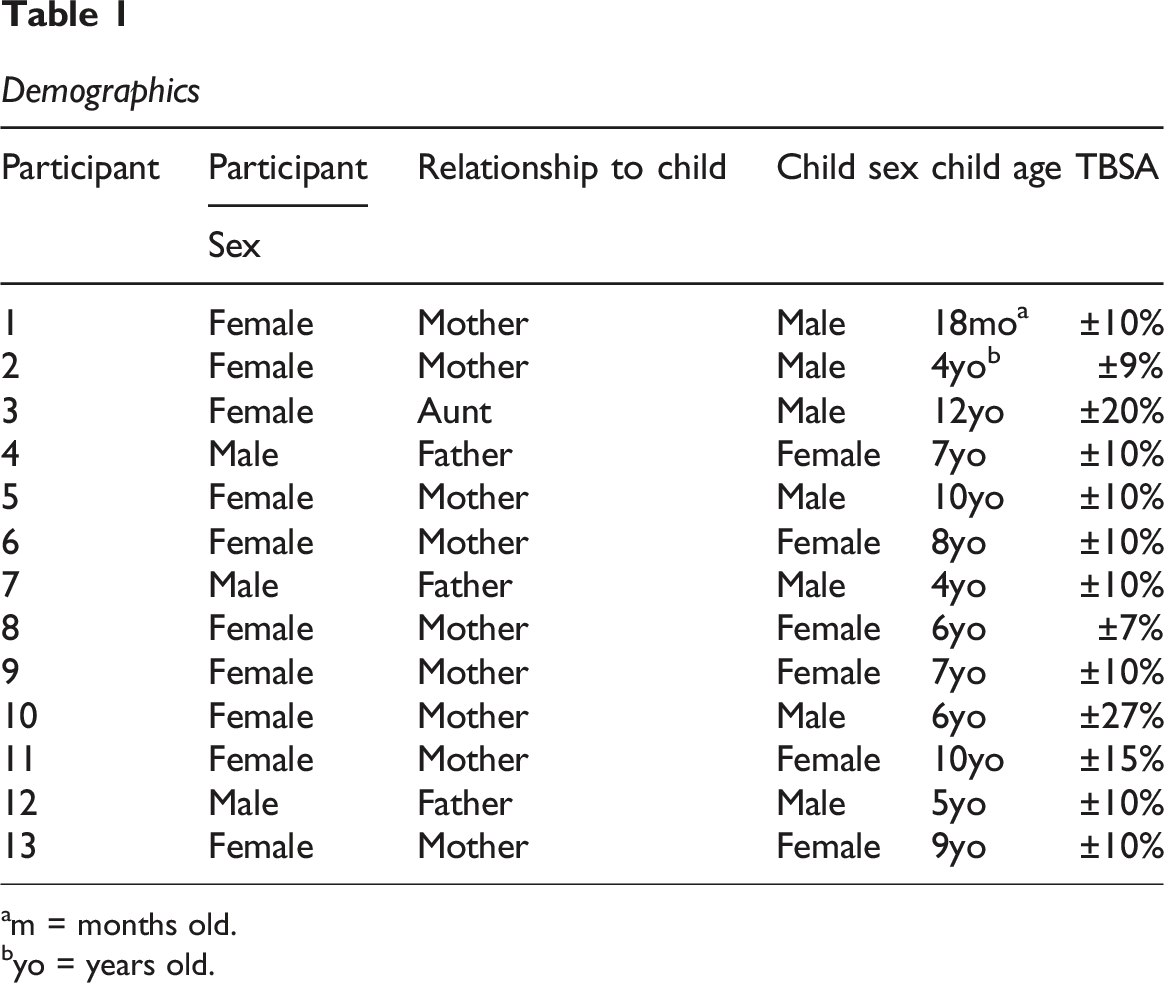
am = months old.
byo = years old.
Saturation
Sample sizes are not without debate; there is widespread contention as to the ideal qualitative sample size (Vasileiou et al., 2018). In settling on our ideal participant sample, we were guided by theoretical and data saturation (Saunders et al., 2018). We initially aimed for at least 15 participants in keeping with Vasileiou et al.’s (2018) view of an acceptable sample size. However, by interview 13, no new codes or themes seemed to be emerging, and it was felt that the data was rich enough for analysis.
Data Collection
Interviews were conducted in English and Afrikaans. While Afrikaans speaking participants were able to communicate in English they were also allowed to communicate in Afrikaans when the primary interviewer discerned the need. For the Afrikaans participants, interviews were either a combination of English and Afrikaans or primarily in Afrikaans.
To increase rigor, the interview guide was finalized after mock interviews with a caregiver and a student volunteer. The interview guide (see Appendix 1) was devised to facilitate both general perceptions of the intervention as well as the extent to which embedded resilience messages could be identified in the intervention. The exploration of the resilience messages proceeded by first focusing on unsolicited participant responses, before specific prompting. Data was collected by the first author (Wayne van Tonder) through face-to-face interviews which were audio-recorded and transcribed verbatim by Wayne van Tonder and checked by Rashid Ahmed, Ashley van Niekerk, Brendon D. Faroa, and Toughiedah Basadien.
Trustworthiness and Reflexivity
We ensured trustworthiness of the data through four criteria: credibility, transferability, dependability, and confirmability (Shenton, 2004). Credibility (Lincoln & Guba, 1985) was achieved through carefully documenting data collection processes and experiences accurately. This involved continuously checking and re-checking the data for inconsistencies and the researcher asking participants clarifying questions throughout all interviews to ensure that the researcher correctly captured the essence of what participants were saying.
In terms of transferability, caregivers currently accessing treatment may be better informants, given their more immediate immersion in their child’s and family’s needs and experiences during postburn recovery and care. For the purpose of dependability, the researcher (Wayne van Tonder) who conducted the interview field notes were read by the rest of the team (Rashid Ahmed, Ashley van Niekerk, Brendon D. Faroa & Toughiedah Basadien) to review these independently for interpretations, manage or eliminate bias, and to enhance further credibility and dependability as noted by Stahl and King (2020). Confirmability, which deals with how unbiased a researcher remains throughout a study (Korstjens & Moser, 2018), was upheld via an audit trail in this research study using field notes, team debriefing meetings, and journaled thoughts about the research process. Immediately after an interview or in some cases after two or three interviews, Wayne van Tonder sent his transcriptions to Rashid Ahmed. These were checked by Rashid Ahmed and feedback given before proceeding to the next set of interviews. The aim was to guide and enhance the process of data collection.
Reflexivity is understood in the current study as the practice through which qualitative researchers can critically self-appraise their feelings, reactions, preferences, beliefs, and ideological stances (Berger, 2015). The research team included a public health professor with a clinical psychology background and experience in burn prevention research (AVN), a psychology professor with a clinical psychology background and experience in resilience studies (RA), and three research psychology postgraduates (a PhD psychology candidate, BDF, and two recent MA graduates, TB and WvT, with this publication based on WvT’s MA thesis). The team’s self-appraisal included considerations of issues like gender, body differences and “race”*(see footnote at the end), including considerations relating to culture and contexts like religion. All authors shared a commitment to the transformation of health care service provision in South Africa. Regular debriefing meetings were also held during the data collection phase between the first and second author. All aspects mentioned above, including emotional challenges faced by caregivers, were discussed to assess their impact on the participants and the findings and interpretation.
Data Analysis
Interviews were transcribed and coded. For Afrikaans speaking participants, the data was first translated into English before coding. In the process of coding, researcher Wayne van Tonder developed a codebook. There was only a single coder, the first author, who developed codes, by reading through the transcripts. These were developed by reading each transcript and selecting a short phrase that summarized the essence of extract. These codes reviewed, but not revised by the second author, who also advised on possible themes. Once themes were developed along with suitable quotes these were then reviewed by all team members. The final themes and quotes were finalized by the first and second authors. The researchers were guided by Braun and Clarke’s (2012) approach to codebook thematic analysis (Roberts et al., 2019) to guide their interpretation of the meanings of the text. The rigor of this study was enhanced in various ways which included incorporating detailed process notes, cross-checking both the data and themes by the other team members together with feedback on transcriptions from the researchers involved in the study.
Ethical Considerations
This study received ethics approval from the University of the Western Cape (BM20821), by the University of Cape Town (HREC:332/2021) and from Red Cross War Memorial Children’s Hospital Research Review Committee (RCC/WC_202106_053). All participants were offered information sheets regarding the aims and objectives of this study, including matters relating to privacy and confidentiality. The South African Protection of Personal Information Act of 2013 (POPIA) was clarified in relation to privacy and access to their individual particulars and these were honored accordingly. Informed consent forms were explained and signed before interviews commenced. The participants were informed that participation was voluntary and that they were free to withdraw from this study at any point without consequence. All transcripts and coded data were de-identified.
Results
Four main themes were generated from the data, highlighting the caregivers’ key experiences and impressions distilled from the video clip: (1) acceptance of burn injury promotes psychosocial recovery; (2) hope matters; (3) emotional support matters in all contexts; and (4) resilience matters, but….
Acceptance of Burn Injury Promotes Psychological Recovery
The first theme that emerged encapsulated caregiver reflections on the importance of accepting a burn injury as seen in the video. They reflected on the portrayal of acceptance in the video, and it resonated with their own experience of negotiating acceptance both for themselves and their children. They emphasized acceptance as a process rather than an event and the importance of support in facilitating acceptance in the burn survivor. Acceptance was described as both an internal process as well as a complex relationship between this internal process, external support and resilience.
Participants highlighted both the magnitude of the task, as well as the struggle in negotiating this for both the child and the caregiver. Participant 13 [Female, Mother] expressed this as: It may seem that it’s impossible, but it’s possible. Because if you accept it, yes, I have [a] burn, I’m here now, I’m in this thing, but now, let me just take it as if I am not in this pain. Inside, you become something if you just like wash… like don’t pin [make it out to be] it as though it’s nothing, yes, there is something, but take it easy… take it like, yes, I’m going to pass this [sic].
Drawing on her own experience participant 11 [Female, Mother] expressed it as: “So I saw that he was not accepting himself so I tried to told him that no, it’s you…this happened to you and now accept yourself because I accept you, because I am your mum…and you will be fine.”
In the complex relationship between acceptance as an internal process, the importance of support and resilience outcomes was best captured by the quotes below. Participant 13 [Female, Mother] reflected: It’s tragic that the kid burnt but after that he had to accept the scar and people have to accept him with the scar and that is why he moved on with his life and [be]came a schoolteacher and helped kids you see [sic].
Participant 11 [Female, Mother] expressed this relationship even more explicitly: “you will not come out [out of the tough situation such as a burn injury] because [you] can’t go alone without [another] person to support you. You can’t do nothing you have to get another hand to help your hand to go through.”
Hope Matters
Hope remains one of the most important dimensions of resilience, and this emerged in the majority of participant responses about the intervention, with some also referring to their own narratives of hope. The power of hope as a transformational belief system facilitating positive outcomes in the future was evident as the quotes illustrate. Participant 4 [Male, Father] expressed: “When the mother come visited in the hospital…Then she told the boy that, he must not worry. Everything’s gonna be fine,” and participant 6 [Female, Mother] expressed this more generally as:…“because if you hope that things are going to turn out better …if you have hope in yourselves, I think you will come out.” [sic]
Participant 13 [Female, Mother] continued in a similar vein, but also linked hope to specific outcomes associated with burn injuries such as acceptance and reintegration: Hope is… actually something you believe in… you are hoping that people will accept you… so if the hope is there meaning that you believe it, people will accept the way you are…hope is actually the believing thing…I can fit back into the world and that my friends will still accept me and my people will still accept me when I go back to work… but I believe hope will come.
Like acceptance, participants also commented on how hope is both an internal quality as well as a process facilitated by support systems as the quotes illustrate. Participant 2 [Female, Mother] echoed, “The message of hope is that this young guy… he didn’t know how to face things… he didn’t have hope, but then after his mom spoke to him, then he had hope… He was strong.” Similarly, participant 11 [Female, Mother], expressed it as follows: When I saw that woman [in the video clip], she encouraged …[her] son… she gave him that hope… [s]he gave him ah… there’s a bright future in front of him… and she told him he’s not gonna lose… she told him he’s going to be okay, and she gave him that… it’s not the end of the world.[sic]
The quotes capture the transformational power of hope, but simultaneously emphasize social support in cultivating hope. One interesting observation about this was that even though hope was portrayed in multiple contexts in the video, the majority of participants focused on the maternal support system as the primary source of hope, as the quotes above illustrate.
Another important finding was the extent to which hope was spiritually located for some of the participants. This is revealing since this aspect is neither portrayed in the intervention, nor specifically elicited during the interviews. Participant 13 [Female, Mother] expressed it clearly as: “I can say first from God, if you believe in God, it’s only Him who can give you hope, even though sometimes you feel like He answers so- so… but the hope is from God…, and participant 9 [Female, Mother] highlighted the importance of prayer in cultivating hope: “because I pray a lot… I pray a lot so… after every time I feel like down I’m asking myself if she got burnt and hurt more than this?.. I just draw my strength from God.”
Emotional Support Matters in All Contexts
Support remains the single most important factor in facilitating resilience, and all the participants responded to the various portrayals of support in the intervention. Not surprisingly the participants underscored the importance of relationship support. Caregivers noted from the video the importance of caregivers and significant others as well as professionals from the hospital and school settings offering this kind of support, often in “mirroring” the positive during difficult times. Participant 3 [Female, Aunt] reflected: He [boy in the video clip] thought all was lost when he saw his face. When he saw his scar and he was concentrating on this scar, but he didn’t concentrate on what his life can be. So that is when his mother said to him that he is still the same person.
Similarly, the emotionally supportive role that friends played in the video clip was also observed by the caregivers, with participant 6 [Female, Mother] observing: Friends is also very important… because children love to play, so in the video clip I saw the friend that he have also support him…and help him go through with …. to help him to expose himself and go out with a friend… because of his friend he could get through the situation.
The importance of relationship support was reaffirmed by drawing on their own experiences. Participant 5 [Female, Mother] shared her daughter’s experiences of the support she had received from her friends: Oh no, it’s massive for her. It’s [peer support] absolutely massive for her… especially on the physical aspect because she is a girl also… you know, so if girls want to look pretty, or walk a certain way ya so… but when her friends have that ‘no, that looks nice’ or ‘oh, that looks cool’ because they are that supportive it’s really important for her because it boosts her confidence… because then for her it’s like ‘it’s fine, there’s nothing wrong with me.
While the importance of the relational support from caregivers and friends is to be expected, the extent to which this expectation also emerged for professional staff was striking. Caregivers strongly echoed the need for emotional support in the professional systems interacting with the child. For example, caregivers recognized the importance of the emotional support that schoolteachers can offer children living with burn injuries. Participant 3 [Female, Aunt] observed: So I think that is when he, he received the support at school where acceptance is, then is really the order of the day. So I think there is also where he realized that he is still the same person… And that is when he was resilient. [sic]
Similarly, the importance of emotional support was also observed in how professional medical staff were depicted in the video clip; participant 13 [Female, Mother] reflected: The caring of the nurses and the staff and the way they help the kid; he was actually feeling very safe because he knows the people help him and do want to help him and not just because it’s their job, but because they have a heart of helping kids… that’s the part that stands out for me.
Similarly, some caregivers shared how they personally experienced emotional support from the medical staff with their own children. Participant 8 [Female, Mother] reflected on her experience with both the nursing staff and treating physician: “Like the doctor that did the thing on her foot, the gentleness, like it’s not just a matter of ‘ag you’re a burns patient, carry on with life … even with the nurses, the absolute care of ‘don’t worry, we’ve got you.”
Similarly, drawing on her own experience, participant 8 [Female, Mother] highlighted the totality of the care required, encompassing both professional and emotional support: “The absolute care of you know… like [interactions from nurses] playing with her… you don’t want to just ‘ah let’s do this quickly’… the playing, the gentle talking, it was very important for her.” [sic]
For participant 11 [Female, Mother], the totality of this care included even material support: “Even the time I was here at hospital one of the doctors from ICU he gave me hundred rand [local currency] to get home, to buy food, a bread at home….”
Resilience Matters, but…
Despite caregivers feeling generally positive about the video clip, some caregivers felt that some aspects of the animation were portrayed too idealistically. One of the themes that emerged here was the extent to which the type of support that was being portrayed in the video did not reflect what they experienced in everyday life.
In drawing from their own experiences, participants questioned whether the portrayal of support depicted in the intervention was possible. Participant 10 [Female, Mother], for example, reported on the limitations of support from the schooling system. Participant 10 [Female, Mother] expressed her concern about the failure of the school to protect her child: “Every time she goes to school, she comes telling me that there is a child teasing her in class or even outside … there’s not really support [sic]. Participant 3 [Female, Aunt] continued in a similar vein, expressing her concern about the failure of peer support: “Even children can be very nasty. They look at you, they know you didn’t look like that, but still they will make fun of you.”
Participant 11 [Female, Mother] questioned the decision of the school to refer her child to a school for learners with special education needs, instead of providing the necessary support at the current school: “One of the teachers ask me why you don’t go to social worker to ask him to find a special school for him because the hands is not gonna work….” [sic]
What was also interesting was the extent to which limitations in the capacity to offer support extended to their own capacity as caregivers and the context they found themselves in; participant 3 [Female, Aunt] said: In his case there was no mother, there’s no father, cause both is now passed on. Okay, the aunties and uncles is there but, you know you are in a working environment, you are at your work, you are not at his bedside because you can’t be there all the time.
Probably the most telling though was from Participant 1 [Female, Mother] who through reflecting on the support offered by the schooling system in the intervention, questioned the capacity of professional support systems like schools to support burn injury survivors. The quote illustrates the apparent contradiction between the need for the supportive situations portrayed in the intervention and the extent to which these could in reality help facilitate change: But what about the school? … like they all need to be onboard… they all need to know how to treat someone that looks different… that has been through a traumatic experience … it’s difficult to get that kind of message out… because it’s no point watching this video and the child goes to school and has got an abusive teacher, like a verbally abusive teacher… the child is gonna… ya, it’s not going to work. [sic]
Discussion
The findings not only support and amplify some of the dimensions associated with resilience, but also help qualify and locate these in context. The literature confirms the difficult and complex process of acceptance. Self-acceptance is a crucial step to take for burn survivors (Kornhaber et al., 2014) and the acceptance of the event can bolster burn survivor’s resilience (Bailey et al., 2015). Importantly, social acceptance, especially by significant others, may protect or at least partially buffer against the impact of stigmatization (Armstrong-James et al., 2018; Ross et al., 2021). However, as the findings underscore, acceptance, like resilience, is best understood as a complex relationship between internal processes and the surrounding support systems that can be mobilized to facilitate positive outcomes.
The importance of the transformative power of hope in recovery was highlighted. Participants commented on both the portrayals of hope in the intervention, as well as their own accounts of negotiating hope in their own postburn recovery process, echoing what is reported in the literature. Hope, as a dimension of psychosocial resilience, has been described as encompassing a range of attributes that include the perceptions and expectations that individuals may have, as well as adaptive behaviors which include how they cope, solve problems, and how well they can adjust after a traumatic experience (Krause & Edles, 2014). Hope has also been identified as a specific enabler of psychosocial recovery (Van Niekerk et al., 2020). This suggests that when hope is present, positive psychological outcomes are likely to increase for individuals with injuries (Brazeau & Davis, 2018).
Importantly, several caregivers located hope in a spiritual higher power despite this dimension not being portrayed in the video clip. This is aligned to previous research that highlighted the importance of both spirituality and religion in postburn recovery (Dekel & Van Niekerk, 2018; Jibeen et al., 2018). Spiritual and religious beliefs may be an important counter to the despair associated with illness (Espedal, 2021), and may contribute to psycho-spiritual growth in burn survivors (Jibeen et al., 2018).
Social support remains one of the most consistent findings associated with resilience (Dykes, 2016; Neill et al., 2022) and the current findings highlight the importance of this dimension. The findings also accentuate the importance of support systems like schooling and health but also foreground the importance of emotional support. Studies suggest that even though re-entering the school environment is crucial for on-going scholastic success, psychological preparatory work needs to be done because of the nature and likely impact of the burn injury (Pan et al., 2018). For instance, not only do children living with burn injuries have to contend with their friends staring at their injuries or even being stigmatized because of it (Lehna, 2013), they may also experience similar challenges in the school setting (Kazis et al., 2016). Similarly, emotional support offered by medical staff also remains pivotal for postburn recovery. Despite burn injuries being physical in nature, these can have significant negative psychological outcomes. Medical staff, such as nurses and doctors, should not only provide physical care but emotional support too (Butler, 2013). Such dual support is reported to bolster the psychosocial resilience in burn survivors (Van Niekerk et al., 2020).
The caregiver’s support of the child itself is a pivotal source of psychological recovery for pediatric burn survivors, and the findings clearly indicate this. Caregivers can bolster resilience in their child through being present during medical procedures (Piira et al., 2005). The physical presence of caregivers during painful procedures, such as wound care, was shown to reassure children and deepen the sense of trust in their caregivers (Egberts et al., 2018). Furthermore, caregivers who show unconditional emotional support may also help their child feel reassured of the future regardless of their injury (Van Niekerk et al., 2020). The observation that the portrayal of maternal support most resonated with the participants may have to do with gender socialization and the social demographics of childcare in low-income contexts like South Africa. In South Africa, the maternal support system is crucial in the aftermath of burn injuries, often bearing the ongoing burden of care, and reflective of a societal structure where caregiving is primarily viewed as a maternal responsibility (Mayer & Barnard, 2015). Burn injuries disproportionately affect people from lower socioeconomic backgrounds, with single mothers leading a large number of households (Govender et al., 2020). This demographic trend highlights the South African societal expectation that women take on the role of caregivers, regardless of personal cost or broader societal implications (Mayer & Barnard, 2015).
The findings also highlight the importance of relationship support more broadly. The literature reports that family and friends’ presence, emotional support, and practical assistance are crucial for children’s psychosocial recovery after burn injury. Supporting the child in the hospital, helping with chores, and offering emotional comfort assists them in healing (Harrison et al., 2021; Rencken et al., 2021). For example, in KwaZulu-Natal, the involvement of extended family and friends was found to be crucial in easing the transition back into daily life after discharge. By fostering normalcy and acceptance, these support networks assist in reducing burn-related stigma and social isolation (Rencken et al., 2021).
The extent to which resilience was located in context, both in terms of its portrayal in the intervention but also in their own narratives of resilience, was clear from the findings. They point to the fact that support may not materialize in contexts like the schooling system, and that the burden of care, especially for caregivers, may intensify. Caregivers have to negotiate domestic and other workloads and seeing to the needs of their children (Lernevall et al., 2021), a burden more likely to be carried by a maternal care system.
Deepening global inequality and associated austerity measures in systems like health and education (Druery et al., 2017; Rencken et al., 2021) has constrained the capacities of health, social, and education systems to provide the kind of support needed for children, especially in impoverished settings. The study findings highlight both the capacity of caregivers, friends, and professionals to provide the kind of support that may be needed for burn survivors, but also the challenges associated with providing this. Budget cuts and reduced funding have affected these systems’ capacities to provide comprehensive care and rehabilitation services (Druery et al., 2017; Rencken et al., 2021). The impact on these systems, through reduced resources, limit caregivers and burn survivors’ access to critical clinical care and support services and exacerbates the recovery process in the complex medical and social landscapes of postburn recovery (Rencken et al., 2021; Thomson et al., 2015).
While the resonance with the messages of resilience point to the potential utility of this intervention, further research is needed on the utilization of the intervention by the intended audience. While there was a strong resonance with the messages of hope in the video the extent to which this portrayal can facilitate hope needs investigation. Similarly, the psychoeducational message that support matters may need to be complemented by further engagement on how this support can and should be activated especially in resource-constrained contexts. Finally, the extent to which the idealistic portrayals may serve as a potential barrier to facilitating resilience also needs to be considered.
Findings Summary
While focus of the study was on caregiver perceptions of the acceptability, relevance and potential utility of the intervention, it was the participant’s ability to draw from and reflect on their own experiences that contributed to the richness of the data. The findings offer rich insight into a resilience informed approach to postburn recovery. They amplify and extend the importance of crucial resilience dimensions such as acceptance and hope, and underscore both the complexity of these processes, as well as the relational nature of these constructs. These were discussed as both internal dimensions as well as relational dimensions amenable to support and intervention as highlighted in the social ecological definitions of resilience. This aligns to one of the most consistent findings from the resilience literature, that is, the importance of mobilizing support systems, with the findings underscoring the importance of both relationship and professional support.
The findings have important implications for informing recovery interventions. While this was not an efficacy study, the findings point to the potential utility of incorporating resilience into future interventions for postburn recovery, drawing on the dimensions identified above. For pediatric care, the findings underscored the importance of activating support systems for children, both relational and professional to facilitate psychological processes like acceptance and hope. While individual interventions remain important in postburn recovery, the findings highlight the role of mobilizing broader support systems in postburn recovery and the importance of complementary, accessible psycho-social interventions.
The participants’ narratives strongly connected the multimedia portrayals with their own experiences as caregivers. The portrayals of dimensions like hope and support in particular resonated strongly with their own experiences and beliefs in the importance of these dimensions. It appears as if the intervention afforded an opportunity to reflect on resilience (including their own) within their unique contexts, pointing to the potential utility of the intervention.
Finally, while resilience messages were identified and resonated with the participants’ experiences, these also pointed to systemic constraints in facilitating resilience. These highlight a potential gulf between the desirability and utility of support and the capacity of these systems to provide it in the current global context. The findings highlighted the challenges often faced by support systems, especially in resource-constrained contexts. The qualifications to support that emerged in caregiver contexts like single parent families, and in public systems like schools, suggest that resilience-informed interventions may have to incorporate appraisals of the capacity of support systems to facilitate the resilience of affected individuals and families.
The clinical care and research implications of these findings are enormous and some are considered here briefly. The majority of resilience research is focused on aspects like protective factors and positive psychology, often without a corresponding focus on the complex interaction between risk, protective factors or resilience building, and outcomes. In terms of developing interventions, it suggests that the extent to which risk counters protective factors is crucial, and the need to address risk more directly may also be necessary. In our daily clinical work, it means assessing for and building on resilience, whilst simultaneously foregrounding risk. This implies cultivating hope in context and guarding against idealistic or overly positive messages of hope. In terms of support, it implies an awareness of the gulf between the necessity of support and the capacity to provide support, and the extent to which risk is omnipresent, especially in resource-constrained contexts.
The findings are a stark and daily reminder that the quality of our health care provision alone may not be enough. We need to work even more effectively in a multidisciplinary way, and sometimes even out of our professional comfort zones, to activate and utilize multiple support systems especially outside of the burn care setting and into the daily lives of the burn survivor. Long-term we need to transform health care so it can be both ameliorative and transformative (Prilleltensky, 2014).
Limitations
The potential bias that emerges from convenience sampling must be noted. For example, the time from the injury to the interview was not recorded, and given the potentially wide window period for postburn care, this may obscure the differences in caregiver interpretations of resilience responses as a result of the different phases of recovery and the accuracy of memory recall (Van Niekerk et al., 2020). Furthermore, while the relative homogeneity of the group enhanced the richness of the data, nonprobability sampling has selection bias and includes strong assumptions about sample-population similarity, which makes generalizations risky (Vinther-Larsen et al., 2010). South Africa is a multilingual country and while English is the universal language of communication, native language fluency is limited and impacts on research (Ngcobo et al., 2021). In our study, while attempts were made to accommodate this, it remains a limitation both in terms of the data collection and losses in translation, but also the English language of the multimedia intervention. As the current study was not conceptualized as an efficacy study, a crucial issue for future research is to separate the specificity of interventions (like the attempt at resilience building in the current intervention or even techniques like CBT) from general characteristics (like relationship building) that are also associated with positive outcomes. Furthermore, the focus of this study on perceptions of resilience in the intervention did not incorporate an appraisal of more general intervention limitations including on aspects such as the chosen content or the form of the intervention. Similarly, while there was resonance with the resilience messages in the intervention, further research is needed to assess the utility and efficacy of the depicted strategies and intervention.
Conclusion
The extent to which caregivers confirmed the importance of self and social acceptance, hope and psychosocial support in the multimedia intervention has important implications for interventions for postburn recovery, survivors and their families. It underscores the importance of these dimensions and their integration in supportive interventions. However, the findings also question the promise and the possibilities offered by resilience informed interventions, and contexts that may mitigate against resilience. One of the earlier calls in the resilience literature (Seccombe, 2002) remains pertinent here. We need to both facilitate resilience as well as transform conditions like structural inequality that undermine resilience. Prilleltensky’s (2014), call to question our roles and responsibilities, so that our work can be both ameliorative and transformative, remains challenging in the current context, but possible if we draw from this understanding of resilience.
Supplemental Material
Supplemental Material - Caregiver Perceptions of a Psychosocially Orientated Resilience-Themed Multimedia Burn Intervention
Supplemental Material for Caregiver Perceptions of a Psychosocially Orientated Resilience-Themed Multimedia Burn Intervention by Wayne van Tonder, Rashid Ahmed, Toughiedah Basadien, Brendon Duran Faroa, Ashley van Niekerk in Clinical Practice in Pediatric Psychology.
Footnotes
Acknowledgements
The authors wish to express their sincere gratitude to Dr. Gary Dos Passos and the dedicated team at the Burns Clinic at the Red Cross War Memorial Children's Hospital for their exceptional support and cooperation throughout the data collection process.Above all, the authors extend their deepest thanks to every participant who took part in this study. Your willingness to contribute so openly and generously made this research possible, and your courage and trust are profoundly appreciated. This work would not have been possible without you. The authors also gratefully acknowledge the University of the Western Cape, the University of South Africa, the South African Medical Research Council, and the National Research Foundation for their valued support.
Consent to Participate
Informed consent was obtained from all participants involved in the study. The use of racial terminology is being problematized here, as is often done in the South African context, given the historical legacy of Apartheid.
Author Contributions
Conceptualization: W.v.T, R.A, B.D.F., and A.v.N.; methodology: W.v.T, R.A, B.D.F., and A.v.N; formal analysis and writing—original draft: W.v.T; writing—review and editing: W.v.T, R.A, T.B, B.D.F., and A.v.N; supervision, “lead”: R.A and “supporting”: B.D.F., T.B, and A.v.N.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research reported in this publication was supported by the University of South Africa, National Research Foundation, and the South African Medical Research Council.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this article cannot be shared publicly due to ethical/privacy reasons. The data will be shared on reasonable request to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.