
Abstract
In this study, we link long-term vulnerability to psychopathology to short-term dynamics between sleep satisfaction and eight daytime psychiatric symptoms. A total of 122 young adults (age: M = 23.9 years; 43% female) from the Tracking Adolescents’ Individual Lives Survey cohort reported nightly sleep satisfaction and daily symptom severity for 6 months using electronic diaries. The severity of internalizing, externalizing, attention-deficit/hyperactivity-disorder (ADHD), and autism-spectrum-disorder (ASD) problems was assessed across 15 years before the diary study. Mixed-effect models showed that lower sleep satisfaction predicted more severe next-day apathy, worry, impatience, irritability, resistance to change, and sensory sensitivity, and there were stronger effects in participants with a history of internalizing and ASD problems. Reverse associations were weaker and symptom-specific such that some daytime symptoms predicted lower next-night sleep satisfaction primarily in participants with a history of ADHD and ASD problems. These findings highlight bidirectional daily associations between sleep and mental health, particularly in individuals with enduring psychiatric vulnerability.
Keywords
Chronic sleep problems affect up to a quarter of the general population (Kocevska et al., 2021) and frequently accompany common mental disorders, such as mood and anxiety disorders (Sivertsen et al., 2021), in some cases even being included as part of their diagnostic criteria as “sleep disturbance” or “insomnia” in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2013). Sleep problems that start in childhood often persist (Fernandez-Mendoza et al., 2022) and can predict a higher risk and severity of psychiatric conditions during adolescence and early adulthood (Lam & Lam, 2021; Mah & Larkings, 2021; Scott et al., 2021). The role of sleep in mental health is supported by multiple observational studies consistently linking sleep problems with stable internalizing, externalizing, and neurodevelopmental traits (Hertenstein et al., 2023; Mijnster et al., 2024; Quach et al., 2018; Sarsembayeva et al., 2024). Beyond the average severity of sleep problems, intraindividual variability, or irregularity, in sleep behaviors can have equally disruptive effects because it has been linked to depression, anxiety, and lower subjective well-being (Lemola et al., 2013; Slavish et al., 2019; Windred et al., 2024). Therefore, the coexistence of sleep problems with psychopathology amplifies the adverse health outcomes and health-care costs associated with mental and sleep disorders worldwide (Chattu et al., 2018; GBD 2019 Mental Disorders Collaborators, 2022; Streatfeild et al., 2021).
The association between sleep problems and psychopathology is commonly conceptualized in models that view insomnia as a 24-hr hyperarousal disorder rather than a purely nocturnal disturbance (Palagini et al., 2023). According to these frameworks, sleep plays a central role in emotional and cognitive regulation, and insufficient or nonrestorative sleep may impair overnight adaptation to stress, resulting in heightened emotional reactivity and reduced regulatory capacity during the following day, which can manifest as various daytime psychiatric symptoms (Palagini et al., 2023). Importantly, the same psychiatric symptoms can also serve as sources of arousal, which are not limited to affective symptoms (e.g., worry) but may also include heightened sensory sensitivity, cognitive activation, or behavioral dysregulation, which are characteristic of neurodevelopmental symptom profiles. These symptoms may interfere with sleep initiation and continuity by sustaining arousal, consistent with stress-arousal models of sleep disturbance (Palagini et al., 2023). These reciprocal processes are embedded in diathesis-stress frameworks, such as the 3P (predisposing, precipitating, and perpetuating) model (Spielman et al., 1987), which emphasize how stable vulnerabilities (e.g., psychopathology) can interact with short-term precipitating factors (e.g., acute stress) to sustain maladaptive sleep-symptom cycles. Together, these perspectives highlight sleep-psychopathology associations as dynamic, bidirectional processes that may vary across individuals and symptom domains.
These theoretical frameworks imply that sleep-psychopathology associations should be observable in everyday behavior as systematic covariation between sleep experiences and psychiatric symptoms. At the behavioral level, such associations can manifest both as stable between-persons differences (i.e., when people with poor sleep generally report more symptoms of psychopathology) and as within-persons fluctuations (i.e., when people sleep worse than usual, they will also report more severe psychiatric symptoms on the next day). The within-persons level is particularly relevant for studying dynamic processes because it captures how day-to-day variations in sleep relate to subsequent changes in mental health in the same individual (Hamaker, 2012). This distinction can be examined using experience-sampling methods (ESMs) and daily diary designs, which repeatedly assess sleep and mental health in daily life (Kouros & El-Sheikh, 2014; Lenneis et al., 2024; Shen et al., 2021). Using such approaches, researchers of multiple studies have demonstrated bidirectional day-to-day associations between poor sleep and mood (Das-Friebel et al., 2020; Dong et al., 2023; Hachenberger et al., 2023; Harris et al., 2022; Kouros & El-Sheikh, 2014; Kouros et al., 2022; Lenneis et al., 2024; Newman et al., 2022; O’Leary et al., 2016; Patapoff et al., 2022; Ratcliff et al., 2014; Song et al., 2023; Takano et al., 2013; Totterdell et al., 1994; Triantafillou et al., 2019), and a smaller set of studies found that poorer sleep can predict increases in daily worry and stress (Menghini et al., 2022; Peltz, 2020; Peng et al., 2024; Werner et al., 2024; Wu & Cronin-Golomb, 2019). In support of these findings, experimental data further confirmed that disrupted or insufficient sleep can impair emotion regulation and heighten stress sensitivity (Minkel et al., 2014; Tomaso et al., 2021), providing a plausible pathway from poor sleep to worse psychiatric symptoms. In turn, some psychiatric symptoms—such as worry, stress, and sensory overstimulation—can potentially interfere with sleep initiation and continuity, as demonstrated by their between-persons-level associations (Benítez-Agudelo et al., 2025; Costa-López et al., 2024; Mische Lawson et al., 2022), but the evidence of such short-term (within-persons) associations is lacking. Furthermore, potentially distinct daily associations with other psychiatric symptoms—particularly symptoms of autism spectrum disorder (ASD), attention-deficit/hyperactivity disorder (ADHD), and externalizing disorders—remain unexplored despite some research suggesting that poor sleep may precede broader behavioral problems in children with ADHD (Sidol et al., 2023) or externalizing problems (McQuillan et al., 2023).
In addition, the strength of these within-persons associations may considerably vary across individuals such that a night of poor sleep may lead to mild adverse effects on mental health for some and pronounced deterioration for others (Fuligni et al., 2019). Indeed, people differ in their vulnerability to detrimental effects of sleep problems on psychopathology, such as demonstrated by the stronger effect of sleep duration on daily mood in adolescents with internalizing problems (Fuligni et al., 2019). Likewise, the day-to-day effect of sleep on affect may be stronger in people with depression and anxiety (Cousins et al., 2011). However, another study showed the opposite direction such that affect was a stronger predictor of sleep quality in children with externalizing problems (Evans et al., 2024). Although such studies are scarce and the effect direction remains unclear, it could be that individuals vulnerable to psychopathology may show systematically different daily dynamics between daily sleep and mental health compared with individuals without such vulnerability. Thus, examining psychopathology as a moderator of within-persons associations offers a way to connect long-term vulnerabilities with short-term processes, which may give insight into the mechanisms of recurrence and/or increases in the severity of psychiatric conditions among individuals with long-term vulnerability.
Taken together, we propose that there is a need for studies that examine sleep-symptom associations at both within- and between-persons levels, include a broader range of psychiatric symptoms, consider variability in sleep problems, and analyze both directions of influence—acknowledging that sleep is not only a precursor but also a consequence of psychiatric symptoms. Addressing these questions at the daily level requires measurement of short-term fluctuations in sleep problems while allowing repeated assessment in everyday life. In this context, sleep satisfaction provides a pragmatic, integrative indicator of perceived sleep quality on a given night, reflecting the cumulative impact of multiple sleep characteristics (e.g., difficulties with initiating/maintaining sleep, sleep duration) without requiring detailed assessment of each component.
In this 6-month daily diary study, we therefore investigated the bidirectional associations between nightly sleep satisfaction and a wide range of psychiatric symptoms (apathy, worry, impatience, irritability, impulsivity, hyperactivity, resistance to change, and sensory sensitivity). In addition, mean sleep satisfaction over 6 months and variability in sleep satisfaction were examined, the latter capturing instability in sleep regulation. We hypothesized the following:
Hypothesis 1: All psychiatric symptoms will be more severe in individuals with lower average sleep satisfaction and will be associated with greater variability in sleep satisfaction on the between-persons level.
Hypothesis 2: There will be bidirectional day-to-day associations between nights with lower-rated sleep satisfaction and more severe psychiatric symptoms on the within-persons level.
Hypothesis 3: These effects will be stronger on apathy and worry in participants with a history of more severe internalizing problems, impatience and irritability in participants with a history of externalizing problems, impulsivity and hyperactivity in participants with a history of ADHD problems, and resistance to change and sensory sensitivity in participants with a history of ASD problems.
In this study, we aimed to clarify the day-to-day interplay between sleep satisfaction and psychiatric symptoms and potential implications for identifying symptom-specific treatment targets.
Transparency and Openness
Preregistration
This study was not preregistered.
Data, materials, code, and online resources
The code for reproducing the analyses in R and the corresponding output are available online on the OSF (https://osf.io/8xkd4/files/osfstorage). The data from the Tracking Adolescents’ Individual Lives Survey (TRAILS) study can be made available on request; the conditions are outlined on the website (https://www.trails.nl/en/researchers/working-with-trails).
Reporting
We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study.
Ethical approval
Informed consent was obtained from all participants of the TRAILS cohort and TRAILS (TRacking Adolescents Individual Lives Survey) TRANS-ID Transitions in Depression) substudy before enrollment. Both studies were approved by the standing Ethics Committee, in accordance with the 1964 Declaration of Helsinki. No additional procedures were required for the current study.
Method
Sample
The data came from TRAILS (Huisman et al., 2008), an ongoing, multidisciplinary cohort study of psychological, social, and physical development of adolescents and young adults in the northern Netherlands. The study started in 2000 and included a general-population cohort and a clinical cohort. Only data from the clinical cohort were used for the current study. It included 543 participants (34% female, 98% Dutch ethnicity) who were referred to outpatient child psychiatric services at least once before the age of 11 years and who are therefore vulnerable (at risk) to mental disorders later in life (Girela-Serrano et al., 2024). All participants were approximately the same age (10–12 years) when the study started in September 2004 and were assessed every 2 to 3 years until the age of 25 to 26 years via questionnaires, interviews, tests, and physical measurements. For more detailed information, see the TRAILS cohort-profile publications (Huisman et al., 2008; Oldehinkel et al., 2015; Ormel et al., 2012).
Around the age of 24 years, participants of the TRAILS clinical cohort were invited to a daily diary study that aimed to prospectively monitor sudden transitions in psychopathology (TRAILS TRANS-ID; Schreuder et al., 2020). Out of 443 eligible participants, 134 (30%) were enrolled, out of whom one dropped out after the baseline interview and 11 more dropped out during the diary period, resulting in 122 participants who completed the study. Both TRAILS and TRAILS TRANS-ID were approved by the Dutch Central Committee on Research Involving Human Subjects, and all participants gave written informed consent before enrollment. TRAILS TRANS-ID participants were not significantly different from individuals who participated in the contemporary (fifth) assessment wave of the TRAILS clinical cohort in terms of personality, socioeconomic status, and physical- and mental-health problems (Schreuder et al., 2023). TRAILS TRANS-ID comprised 6 months of daily diary assessments (183 consecutive days). Participants completed a brief electronic questionnaire every evening, accessed via a link sent by text message to their mobile phone at a fixed time chosen by the participant. Diaries assessed experiences during the past day and were completed once per day, with 24 hr between assessments. If a diary was not completed within 30 min, an automated reminder was sent, after which participants had an additional 2.5 hr to respond. Participants received regular contact from the research team during the diary period to resolve technical issues and support adherence. After completing the study, participants received a financial compensation (a higher amount with higher compliance) and an overview of their own data. Compliance in the TRAILS TRANS-ID study was high (approximately 88% of diaries completed), and perceived burden was low. A detailed description and validation of the diary procedure have been published previously (Schreuder et al., 2020, 2023).
Both the general TRAILS and TRANS-ID studies were conducted in accordance with the Declaration of Helsinki and approved by the relevant medical ethics committees; a written informed consent was obtained from each parent/participant at every assessment wave.
Measurements
Demographic and health characteristics
Self-reported demographic data retrieved from the fifth measurement wave of TRAILS were used for sample description. Education status (“Are you studying at the moment?”) was classified as not studying or studying in secondary or higher education. Employment (“Did you have paid work in the last month?”) was classified as not employed or employed. Marital status (“What is your marital status?”) was classified as married/in a relationship or single. In addition, participants rated their overall physical health in the previous month on a Likert scale that ranged between 1 (bad) and 4 (good) points.
History of psychopathology
The severity of problems in four domains of psychopathology (internalizing, externalizing, ADHD, and ASD problems) was assessed at five consecutive measurement waves of TRAILS over the period of 12 to 13 years before the diary study. Subscales of the Youth Self-Report (YSR; Waves 1–3; Achenbach, 2001) and Adult Self-Report (ASR; Waves 4 and 5; Achenbach & Rescorla, 2003) were used to assess the severity of internalizing problems, comprising signs of depression, anxiety, and somatic symptoms (31 items), and externalizing problems, comprising questions about aggressive and delinquent behavior (32 items). The severity of ADHD problems was parent-reported using subscales of the parent-reported Children’s Behavior Questionnaire (seven items; C. A. Hartman et al., 2006) and Adult Behavior Checklist (13 items; Achenbach & Rescorla, 2003). ASD problems were parent-reported using four subscales of the Children’s Social Behavior Questionnaire (CSBQ; 30 items; C. A. Hartman et al., 2006) that specify four problem dimensions: Reduced Contact, Reduced Social Insight, Insistence on Sameness, and Sensory Stimulation and Motor Stereotypes. The subscales Orientation Problems and Violations of Social Conventions were excluded because of their associations with ADHD and externalizing problems, respectively, and hence, lower specificity for ASD (Groen et al., 2024). The response scale for all items was a Likert scale ranging from 0 (not at all) to 2 (often), except for CSBQ, which ranged from 0 to 3. Total scores for each domain of psychopathology per measurement wave were estimated as a mean of these item scores. Participants’ history of problems in different domains of psychopathology was calculated as the mean of the scores across five assessment waves (point range = 0–2) separately for each of the four domains of psychopathology.
Daily sleep satisfaction and psychiatric symptoms
Every evening at a fixed time chosen by the participant for a period of 183 consecutive days, participants answered diary questions regarding their experiences in the last 24 hr. Diary questions were designed to include common symptoms of psychiatric disorders based on earlier ambulatory assessments, diary protocols, and existing standardized questionnaires. The final selection of questions included 58 symptoms rated on a visual analogue scale that ranged from 0 (not at all true) to 100 (very true). All included items covered multiple diagnostic categories and were sufficiently distinct from each other, expected to vary day to day, and easy to understand, as tested in a pilot study of 12 adolescents (Schreuder et al., 2020). Diary items were validated by qualitatively assessing the consistency of their interpretation by the first 60 participants during the interviews at baseline and after the diary period. For the current study, we selected nine diary items: one that assessed sleep satisfaction (“I slept well”) and eight others that matched four specific domains of psychopathology (Table 1). The latter items were chosen based on (a) their correlations with the psychiatric domains of interest (Schreuder et al., 2020) so that they could be grouped as more specific to four domains of psychopathology and (b) high within-persons variability so that they were useful to assess on a daily basis.
Diary Items That Describe Daily Symptoms in the Corresponding Domains of Psychopathology

Variables used in the additional analyses
Standard deviations from participants’ mean sleep satisfaction across 6 months were calculated to reflect sleep-satisfaction variability; higher values indicate more variable (i.e., inconsistent from day to day) sleep satisfaction.
History of sleep problems was assessed using the item “I have problems with sleeping” from YSR (Waves 1–3) and ASR (Waves 4 and 5), averaged across five waves in the same way as history of psychopathology. Participants’ history of sleep problems was classified as “high” if their scores exceeded the sample’s average (≥ 0.5 points).
Self-rated history of ADHD problems was assessed similarly to the parent-rated version using the scores from YSR (seven items) and ranged between 0 and 2.
Concurrent psychopathology was calculated by averaging the scores on different domains of psychopathology assessed during a standardized clinical interview (mini-SCAN (Schedules for Clinical Assessments in Neuropsychiatry); Nienhuis et al., 2010) at the start of the diary study. Item scores varied between 0 and 2, corresponding to absent, subclinical, and clinical symptoms, respectively. Item scores for different diagnostic categories were averaged as means to reflect the severity of concurrent internalizing (mean score on the items for generalized anxiety and depression), externalizing (approximated from the items for oppositional defiant disorder), ADHD, and ASD problems.
Statistical analyses
Daily associations between sleep satisfaction and next-day psychiatric symptoms were analyzed using linear mixed-effects models, which can separate the variability in the outcome because of between-persons and within-persons differences. These analyses were conducted in R (Version 4.5.2; R Core Team, 2017) using the package lme4 (Bates et al., 2015). The script with the full output is available on the OSF (https://osf.io/8xkd4/files/osfstorage).
Before the analysis, daily ratings of sleep satisfaction were centered around each participant’s mean score to reflect daily deviations in the ratings from the participant’s average daily sleep satisfaction. Mean levels of sleep satisfaction, sleep-satisfaction variability (i.e., within-persons standard deviations), and all psychopathology scores were centered around the sample mean to reflect the deviations from the sample’s average. Data from all participants were used in the analysis, but the analyses excluded observations that were incomplete on at least one variable required for the main analyses; this limitation guaranteed that the analytical sample remained the same for each analysis and preserved the direct comparability of the study results. Pearson’s correlation coefficients (r) were estimated to measure correlations between the item scores and scores on psychopathology.
For each of the eight outcomes (i.e., daily symptoms), a separate set of linear mixed models was fit by consecutively adding the predictors and random effects (see the script for exact model specifications). Model fit was tested based on differences in maximum-likelihood indices using analysis of variance. Fixed effects included the effects of participants’ day-to-day and average sleep satisfaction and their interactions with each score for history of psychopathology (separate models per domain of psychopathology, including internalizing, externalizing, ADHD, and ASD problems). Additional predictors included the scores on the corresponding symptom from one day earlier to account for possible autocorrelation in the outcome variable (i.e., the case when symptom severity at one moment is predictive of its severity at the subsequent assessment), and the time period was counted in days from the start to the end of the study to account for possible effects of time itself on changes in the outcome (i.e., time trends). Random intercepts and slopes (i.e., effects of daily sleep satisfaction and time) were added in all models to acknowledge that participants may differ in the severity of daily psychiatric symptoms (the intercept) and how symptoms were affected by time trends and sleep (random slopes).
To test whether the severity of the psychiatric symptoms would predict next-night sleep satisfaction in reverse, we fit similar mixed models that included sleep satisfaction as the outcome predicted by symptom severity from the day before (centered within persons), average symptom severity (centered between persons), sleep satisfaction from the night before (i.e., autocorrelation), and time. The Johnson-Neyman procedure was used to determine the range (at −1 SD, the mean, and +1 SD) of psychopathology severity for which the association between sleep satisfaction and symptom severity differed from zero.
Additional (post hoc) analyses were used to investigate whether the effects of daily and average sleep satisfaction would differ (a) with the addition of the effects of sleep-satisfaction variability to test whether it can be a stronger predictor of psychiatric symptoms than mean sleep satisfaction, (b) in participants with a history of more severe sleep problems to determine if sleep satisfaction has (a stronger) effect in those more likely to have a sleep disorder, (c) with the replacement of parent-rated with self-rated history of ADHD problems to investigate which version has a stronger moderating effect, and (d) with the replacement of a history of psychopathology with the severity of concurrent psychopathology to determine whether present psychiatric problems may have a stronger moderating effect than psychiatric problems averaged across 15 years.
We regarded the associations as statistically significant if p values (computed following the Satterthwaite’s procedure) were smaller than .05 after correcting for multiple testing using the false-discovery-rate (Benjamini & Hochberg, 1995) procedure. Magnitude of effects was judged based on the standardized regression coefficients (i.e., the expected difference in the outcome standard-deviation units between individuals that differ by 1 SD in the predictor), which were acquired from the model output using the misty package (Yanagida, 2025). Unless stated otherwise, effects described in the text refer to standardized regression coefficients (β), and the tables present original model estimates. The proportion of total variance in the outcome that is accounted for by clustering because of repeated measurements in individuals was indicated by the intraclass correlation coefficient (ICC).
Results
Characteristics of the study sample and correlations between the variables
The analytical sample included all participants who completed the diary study (N = 122) and had complete data on all variables required for the analyses (i.e., diary data and psychopathology), resulting in 17,620 observations (M = 144 per participant). Participants completed, on average, 88% of all prompted daily diaries (SD = 0.10, range = 0.54–1.00), calculated as the number of completed diaries divided by the number of daily prompts sent during the study period.
For demographic and general-health characteristics, see Table 2. For variation in diary item ratings across days (within persons) and across individuals (between persons), see Table S1 in the Supplemental Material available online. For correlations between psychiatric symptoms, sleep satisfaction, and psychopathology, see Figure S1 in the Supplemental Material.
Demographic and Physical- and Mental-Health Characteristics of the Study Sample Before the TRAILS TRANS-ID Substudy

Note: For continuous variables, the estimates are the mean ± standard deviation and minimum/maximum (in brackets). For categorical variables, the estimates are the absolute number of participants and their proportion in the whole sample (in parentheses). TRAILS = Tracking Adolescents’ Individual Lives Survey.
Daily associations between sleep satisfaction and psychiatric symptoms
Model-fit comparison
Although we initially specified random slopes for time and daily sleep satisfaction, convergence problems led us to use random-intercept-only models for inference (https://osf.io/8xkd4/files/osfstorage). In all models, a substantial proportion of variance was attributed to within-persons clustering (ICCs = 0.4–0.7; Table 3).
Associations Between Sleep Satisfaction and Next-Day Psychiatric Symptoms Adjusted for Symptom Severity and the Period of the Study

Note: The regression coefficients in the table are derived from the original models. Standardized regression coefficients are presented in the text (see Results). Statistically significant p-values are highlighted in bold. CI = confidence interval.
General associations between sleep satisfaction and daily psychiatric symptoms
For all psychiatric symptoms, higher symptom severity on the previous day was significantly associated with more severe symptoms on the next day (Table 3).
Time was significantly associated with symptom severity for most psychiatric symptoms, except for resistance to change and sensory sensitivity. Closer to the end of the study period, the severity of most symptoms somewhat decreased, but these differences were very small, with a decrease of up to 3 points (on the scale 0–100) on average during the whole study period (Table 3).
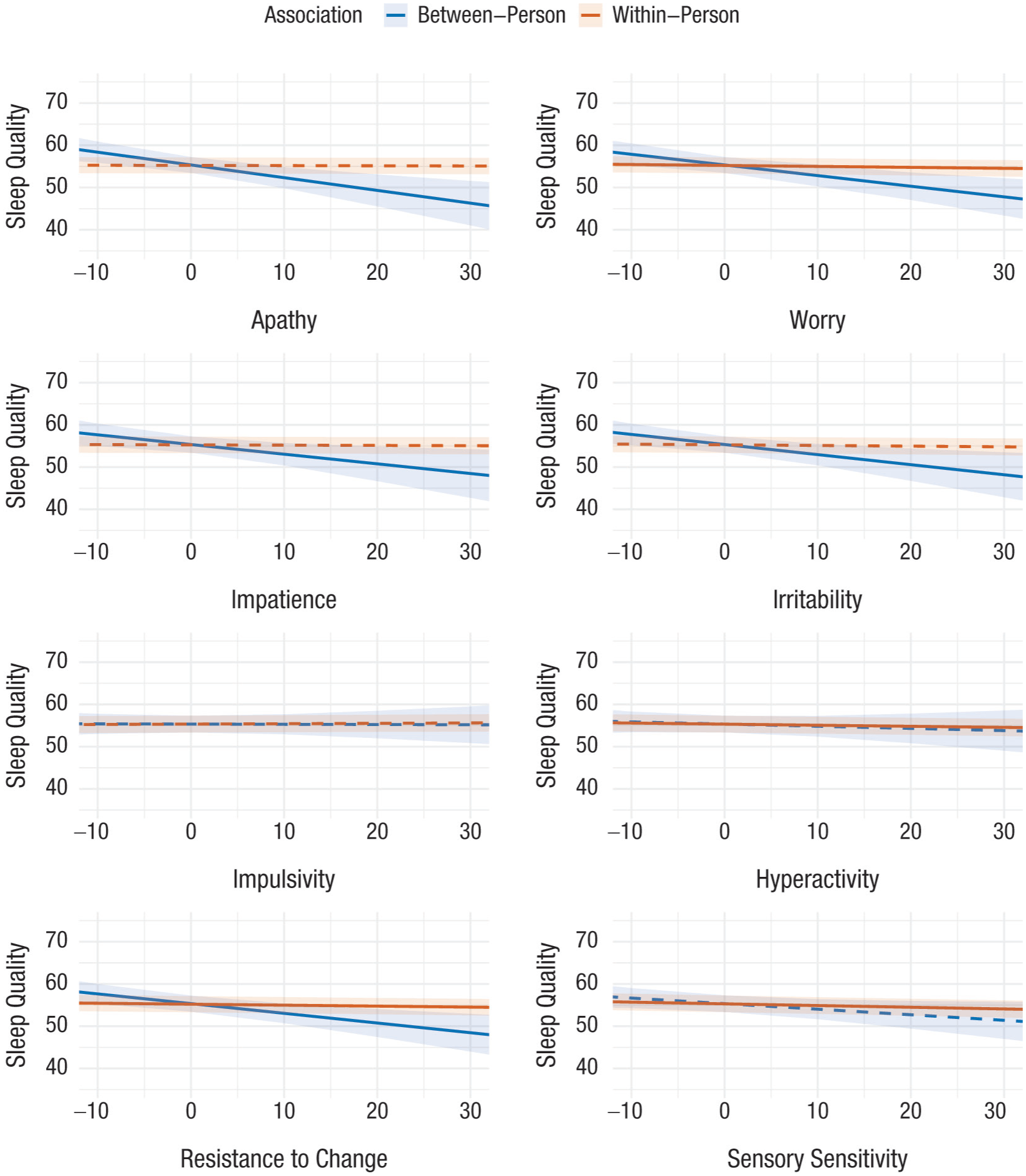
On the within-persons level (Fig. 1, in red), higher daily sleep satisfaction was significantly associated with less severe next-day symptoms of internalizing problems, that is, apathy (β = −0.10; p < .01) and worry (β = −0.09; p < .01); symptoms of externalizing problems, that is, impatience (β = −0.08; p < .01) and irritability (β = −0.11; p < .01); and symptoms of ASD, that is, resistance to change (β = −0.13; p < .01) and sensory sensitivity (β = −0.12; p < .01); but not symptoms of ADHD, that is, impulsivity and hyperactivity (Table 3). Thus, on days when a person slept 1 SD better than their own usual sleep quality, the severity of their daytime symptoms was on average around 0.1 SD lower than their usual symptom severity.

Associations between daily sleep satisfaction and next-day severity of psychiatric symptoms. Scores are centered around each participant’s mean for daily sleep satisfaction and around the sample’s mean for average sleep satisfaction. Lines show the predicted severity of psychiatric symptoms (on a 0–100 scale) depending on sleep-satisfaction ratings, with 95% confidence intervals (ribbons around the lines). Daily (within-persons) associations are indicated in red, and average (between-persons) associations are indicated in blue. Dashed lines present predicted values for the associations that were not statistically significant.
On the between-persons level (Fig. 1, in blue), higher average sleep satisfaction was significantly associated with less severe average apathy (β = −0.26; p < .01), worry (β = −0.24; p < .01), impatience (β = −0.18; p = .01), irritability (β = −0.21; p = .01), and resistance to change (β = −0.25; p < .01), but not impulsivity, hyperactivity, and sensory sensitivity (full model output including original unstandardized estimates can be found in Table 3).
Associations between sleep satisfaction and daily psychiatric symptoms in participants with a history of psychopathology
Regarding moderation by history of psychopathology (Fig. 2), history of more severe internalizing problems significantly strengthened the effects of daily sleep satisfaction on the next-day apathy (β = −0.02; p = .03), worry (β = −0.02; p < .01), impatience (β = −0.03; p < .01), resistance to change (β = −0.03; p < .01) and sensory sensitivity (β = −0.04; p < .01). In individuals with a history of severe internalizing problems, conditional effects of daily sleep satisfaction varied between β = −0.16 and β = −0.11, which were around 1.5 to 2 times stronger than the effects in participants with a history of mild internalizing problems. History of more severe externalizing problems strengthened the effects of daily sleep satisfaction on next-day apathy (β = −0.02; p = .01) but weakened its effect on the next-day hyperactivity (β = 0.02; p < .01) up to the point that the effect of sleep quality on hyperactivity was statistically significant only in individuals with mild externalizing problems (conditional β = −0.03; p < .01). History of more severe ADHD problems strengthened the effects of daily sleep satisfaction on the next-day apathy (β = −0.02; p = .01), irritability (β = −0.02; p < .01), hyperactivity (β = −0.02; p < .01), and sensory sensitivity (β = −0.03; p < .01), so that in participants with severe ADHD problems, the effects were around 1.5 times stronger than for participants with mild ADHD problems. For hyperactivity in particular, the effect of sleep satisfaction was significantly negative only in participants with very severe ADHD problems (conditional β = −0.02; p < .01). History of more severe ASD problems strengthened the effects of daily sleep satisfaction on the next-day irritability (β = −0.05; p < .01), hyperactivity (β = −0.02; p = .02), resistance to change (β = −0.04; p < .01), and sensory sensitivity (β = −0.06; p < .01), so that the effects of daily sleep satisfaction were 2 to 3 times stronger in participants with a history of severe compared with participants with mild ASD problems. Likewise, as for history of ADHD, the effect of sleep satisfaction on hyperactivity was statistically significant only in participants with very severe ASD problems (conditional β = −0.03; p = .01).

Associations between daily sleep satisfaction and next-day psychiatric symptoms in participants with a history of four different types of psychopathology. Scores on daily sleep satisfaction are centered around each participant’s mean. Lines show the predicted severity of psychiatric symptoms (on a 0–100 scale) depending on daily sleep satisfaction ratings, with 95% confidence intervals (ribbons around the lines). Color of the line corresponds to the severity of psychopathology (according to the legend). Dashed lines present predicted values for the associations that were not statistically significant.
History of psychopathology did not moderate the effects of average sleep satisfaction on any daily symptoms. Full output of the models can be found in Tables S2 to S5 in the Supplemental Material.
Reverse associations: psychiatric symptoms as predictors of next night’s sleep satisfaction
Regarding the reverse associations (Table 4), more severe apathy predicted significantly lower next-night sleep satisfaction in participants with a history of severe ADHD (conditional β = −0.11; p < .01 for participants with +1 SD or greater ADHD severity) and ASD problems (β = −0.07; p < .01). More severe daytime worry predicted lower next-night sleep satisfaction (β = −0.02; p < .01), and this effect was not significantly moderated by history of psychopathology. More severe irritability predicted lower next-night sleep satisfaction in participants with a history of severe ADHD (β = −0.07; p < .01) and ASD problems (β = −0.06; p < .01). The main effect of impulsivity on next-night sleep satisfaction was not statistically significant, except for subgroups with a history of no to mild internalizing problems and severe ADHD problems, in which higher impulsivity predicted significantly higher next-night sleep satisfaction (conditional β = 0.03; p < .01 and β = 0.02; p = .01, respectively). More severe hyperactivity predicted lower next-night sleep satisfaction (β = −0.02; p < .01), particularly strongly in participants with a history of severe internalizing problems (β = −0.04; p < .01). Resistance to change predicted lower next-night sleep satisfaction (β = −0.02; p < .01), particularly strongly in participants with a history of severe ADHD (β = −0.05; p < .01) and ASD problems (β = −0.05; p < .01) and mild internalizing problems (β = −0.03; p < .01). More severe sensory sensitivity predicted lower next-night sleep satisfaction (β = −0.03; p < .01), particularly strongly in participants with a history of severe ADHD (β = −0.06; p < .01) and ASD problems (β = −0.06; p < .01) and mild externalizing problems (β = −0.06; p < .01).
Associations Between Daytime Psychiatric Symptoms and Next-Night Sleep Satisfaction Adjusted for Symptom Severity and the Period of the Study

Note: The regression coefficients in the table are derived from the original models. Standardized regression coefficients are presented in the text (see Results). Statistically significant p-values are highlighted in bold. CI = 95% confidence interval.
Impatience was not associated with next-night sleep satisfaction. All associations are visualized in Figures 3 and 4. For full model output, see the online supplement on the Open Science Framework.
Daily associations between daily severity of psychiatric symptoms and next-night sleep satisfaction. Scores are centered around each participant’s mean for daily symptom severity and around the sample’s mean for average symptom severity. Lines represent the predicted next-day sleep satisfaction depending on the daily severity of psychiatric symptoms (on a 0–100 scale), with 95% confidence intervals (ribbons around the lines). Daily (within-persons) associations are indicated in red, and average (between-persons) associations are indicated in blue. Dashed lines present predicted values for the associations that were not statistically significant.

Daily associations between daily severity of psychiatric symptoms and next-night sleep satisfaction depending on the history of four types of psychopathology. Scores on daily symptom severity are centered around each participant’s mean. Colored lines represent model-predicted next-day sleep satisfaction depending on the daily severity of psychiatric symptoms (on a 0–100 scale) in particupants with different history of psychopathology, with 95% confidence intervals (ribbons around the lines). Color of the line corresponds to the severity of psychopathology (according to the legend), and dashed lines present the moderation effects of psychopathology that were not statistically significant.
Additional analyses
The effects of sleep-satisfaction variability were not statistically significant in the models without a history of psychopathology. In participants with a history of mild ASD problems, greater sleep variability was associated with more severe average levels of irritability (conditional β = −0.31, p = .01), resistance to change (β = −0.35, p < .01), and sensory sensitivity (β = −0.24, p = .01).
In participants with a history of more severe sleep problems (N = 50), daily associations with sleep were only slightly stronger, and the effects of sleep satisfaction on hyperactivity and impulsivity were also absent.
Similar to a history of parent-rated ADHD problems, a history of self-rated ADHD problems strengthened the effect of daily sleep satisfaction on apathy (β = −0.02, p = .04) and sensory sensitivity (β = −0.02, p = .03), but it did not strengthen the effect on irritability and even weakened the effects of daily sleep satisfaction on impatience (β = 0.02, p = .04) and hyperactivity (β = 0.02, p = .02).
Unlike a history of internalizing problems, concurrent internalizing problems strengthened the effect of daily sleep satisfaction only on the next-day sensory sensitivity (β = −0.03, p < .01) but not other symptoms. Unlike a history of externalizing problems, concurrent externalizing problems strengthened the effects of daily sleep satisfaction not only on apathy (β = −0.04, p < .01) but also on irritability (β = −0.05, p < .01), resistance to change (β = −0.02, p < .01), and sensory sensitivity (β = −0.04, p < .01) and had no effect on hyperactivity. Unlike a history of ADHD problems, concurrent ADHD problems did not strengthen the effects of daily sleep satisfaction on hyperactivity but did strengthen the effect of daily sleep satisfaction on apathy (β = −0.03, p < .01), irritability (β = −0.03, p < .01), and sensory sensitivity (β = −0.02, p < .01). Unlike a history of ASD problems, concurrent ASD problems did not strengthen the effects of daily sleep satisfaction on hyperactivity but did so for apathy (β = −0.03, p < .01) in addition to the similarly stronger effects on irritability (β = −0.04, p < .01), resistance to change (β = −0.04, p < .01), and sensory sensitivity (β = −0.05, p < .01). These associations are visualized in Figure S3 in the Supplemental Material.
For the full output of additional analyses, see the supplementary materials on the OSF.
Discussion
Summary of the findings and implications
Using the data from a 6-month-long daily diary study of 122 at-risk young adults (TRAILS TRANS-ID), we investigated reciprocal associations between nighttime sleep satisfaction and the severity of eight daytime psychiatric symptoms in participants with different histories of psychopathology. Our findings demonstrated that the associations between sleep satisfaction and next-day symptoms were generally stronger (β ≈ 0.10) and more widespread across symptom domains than reverse associations between symptoms and next-night sleep satisfaction (typical β ≈ 0.02). Furthermore, far fewer symptoms significantly preceded lower sleep satisfaction, and these effects were often confined to individuals with a history of specific psychopathology, such as severe ADHD and ASD problems. This asymmetry suggests that although bidirectional associations exist, poor sleep may represent a more consistent short-term risk factor or early indicator of next-day symptom worsening than vice versa.
Contrary to our initial hypothesis, within-persons associations between daily sleep satisfaction and psychiatric symptoms were not restricted to the matching domains of psychopathology. Higher sleep satisfaction was linked to lower next-day severity of most psychiatric symptoms, including those linked to poor sleep in earlier diary-based studies (e.g., worry and irritability; Meigs et al., 2024; Menghini et al., 2022; Narmandakh et al., 2021; Newman et al., 2022; Peng et al., 2024) and those for which prior evidence has so far been scarce (e.g., apathy, resistance to change, sensory sensitivity). Although the absolute changes in symptom severity following a night of worse sleep were modest in magnitude on average (which is typical for short-term within-persons processes; Fraser et al., 2025), these effects were substantially stronger in participants with a history of severe psychopathology, particularly internalizing and ASD problems. This pattern suggests that daily sleep disturbances may be particularly consequential for people with enduring psychiatric vulnerabilities.
The reverse within-persons associations were more selective. Only a subset of psychiatric symptoms predicted lower next-night sleep satisfaction, and these effects were often confined to participants with a history of specific psychopathology. Worry predicted lower next-night sleep satisfaction, consistent with earlier ESM research (Meigs et al., 2024; Menghini et al., 2022; Narmandakh et al., 2021) and likely serving as a common manifestation of presleep hyperarousal (Dressle & Riemann, 2023). In contrast, several other symptoms predicted lower sleep satisfaction primarily in participants with a history of neurodevelopmental problems (ADHD and ASD), including apathy, irritability, resistance to change, sensory sensitivity, and hyperactivity. This clustering indicates that in neurodevelopmental subgroups, daytime symptoms may more readily translate into an evening state of hyperarousal that interferes with sleep initiation and continuity. Together, these findings indicate that bidirectional associations between perceived sleep and daily symptoms can depend on the broader psychiatric vulnerability that underlies these symptoms.
Between-persons associations largely agreed with the within-persons pattern: Higher average sleep satisfaction was associated with lower average apathy, worry, impatience, irritability, and resistance to change, resembling associations reported in earlier cross-sectional studies (Alqahtani et al., 2022; Alwhaibi & Al Aloola, 2023; Balter et al., 2025; Costa-López et al., 2023; A. G. Hartman et al., 2022; Hong et al., 2022; Jurgelis et al., 2022; Karlovich et al., 2023; Manelis-Baram et al., 2022; Palmer et al., 2023; Whiting et al., 2023). However, these associations were not moderated by history of psychopathology, suggesting that people with more severe psychopathology may not necessarily have consistently poorer sleep satisfaction but, rather, be more sensitive to short-term sleep problems. Clinically, this distinction matters because it implies that vulnerability may be expressed more in reactivity to poor sleep rather than in stable co-occurrence of sleep problems and symptoms, and it provides one explanation for why daily sleep-focused interventions might be particularly beneficial in high-risk groups even when their average sleep satisfaction is not markedly reduced.
A notable discrepancy was observed in the effects of mean sleep satisfaction and sleep-satisfaction variability in people with different histories of ASD problems: Higher mean sleep satisfaction was linked to lower average severity of irritability, resistance to change, and sensory sensitivity, particularly strongly in participants with more severe ASD problems, whereas higher sleep-satisfaction variability predicted lower average severity of these symptoms in individuals with a history of no to mild ASD problems. This discrepancy suggests that in neurotypical people, sleep-satisfaction variability may be a more relevant aspect of sleep health than mean sleep satisfaction. Overall, the discrepancies found between the effects of average and variable sleep satisfaction emphasize the need to distinguish the role of individual sleep characteristics when studying daily symptoms and potential mechanisms behind these associations. Because variability could be examined only at the between-persons level, these findings primarily inform individual differences rather than within-persons mechanisms and should be interpreted cautiously with respect to therapeutic targets. Nevertheless, they may help identify subgroups for whom sleep irregularity is a more reliable marker of psychiatric vulnerability.
In partial agreement with our hypotheses, this study demonstrated that a history of psychopathology can strengthen the associations between daily sleep satisfaction and some psychiatric symptoms, but these effects were not restricted to symptoms in the matching domains: For example, internalizing problems strengthened the associations not only with apathy and worry but also with resistance to change and sensory sensitivity. Furthermore, the strongest and most consistent moderation effects were observed for internalizing and ASD problems rather than externalizing or ADHD problems, suggesting that the associations between sleep satisfaction and next-day symptoms may be particularly relevant when the psychiatric vulnerability is predominantly characterized by heightened arousal, emotional reactivity, and sensory dysregulation. In addition, the specificity of reverse associations to people with a history of ADHD and ASD problems suggests diverse mechanisms maintaining poor sleep across domains of psychopathology such that neurodevelopmental traits are more likely to lower the threshold at which daytime dysregulation translates into sleep-disrupting arousal.
The associations with sleep satisfaction for hyperactivity and impulsivity deviated from the general trend observed for other symptoms. Because hyperactivity and impulsivity are listed as behavioral consequences of poor sleep in the criteria of insomnia disorder (Riemann et al., 2022), we expected a negative correlation between sleep satisfaction and these symptoms in all participants. However, sleep satisfaction was associated with the next-day hyperactivity only in participants with a history of severe ADHD and ASD problems, supporting the association observed between actigraphy-based sleep parameters and hyperactivity in children with ASD in prior research (Bangerter et al., 2020). In reverse, hyperactivity was a rather stable predictor of next-night sleep satisfaction in participants with different histories of psychopathology, albeit somewhat stronger in participants with a history of severe internalizing problems. Furthermore, sleep satisfaction did not predict next-day impulsivity, and the reverse association contradicted the general trend for other symptoms: Higher impulsivity predicted higher next-night sleep satisfaction, specifically in participants with a history of no to mild internalizing problems but moderate to severe ADHD problems. Given the small effect sizes and psychopathology-specific nature of these results, strong mechanistic conclusions would be premature. One possible explanation is that in neurodevelopmental conditions, hyperactivity reflects presleep cognitive or physical hyperarousal that directly interferes with sleep initiation (Dressle & Riemann, 2023), whereas in internalizing disorders, a comparable arousal state may be experienced primarily as worry. In contrast, impulsivity in people with severe ADHD problems and no/mild internalizing problems (i.e., lower than usual depression and anxiety) may reflect other phenomena leading to more positive sleep-satisfaction ratings, such as cognitive disinhibition and hypomania associated with decreased sleep need and higher sleep efficiency (Asaad & Rasas, 2013; Patapoff et al., 2022). However, these interpretations remain highly speculative and underscore the need for replication and future studies that differentiate how specific symptoms affect various dimensions of sleep health.
The patterns from this observational study should be interpreted as reflecting short-term dynamics rather than definitive causal pathways, and extensive further research is required to determine the exact causal pathways underlying the complex relationships between sleep behavior and mental health. If follow-up research indeed confirms that the associations found in this study reflect causal pathways, we would be able to conclude that sleep satisfaction may serve different roles depending on the direction of effects. When poorer sleep precedes increases in psychiatric symptoms, as observed in people with internalizing problems, sleep may represent a promising target for interventions striving to alleviate the burden of mental illness. Conversely, when changes in sleep satisfaction primarily follow symptom fluctuations, as observed in people with a history of more severe ADHD and ASD problems, poor sleep may be better understood as a consequence of psychiatric symptoms rather than a causal driver. In these cases, approaches aimed at improving sleep may yield greater benefits when they also address accompanying psychiatric symptoms. The findings further suggest that long-term psychiatric vulnerabilities may shape individual sensitivity to short-term sleep problems, potentially through sustained differences in stress reactivity and emotion regulation. From a clinical perspective, this implies that day-to-day sleep disturbances may be especially detrimental for people with prior or ongoing mental-health problems and emphasizes the importance of identifying subgroups that may be particularly sensitive to sleep-related interventions.
Strengths and limitations
The intensive longitudinal design of TRAILS TRANS-ID allowed the study of within- and between-persons effects of sleep satisfaction on a variety of psychiatric symptoms during a long (half a year) period of extensive daily assessments of 122 young adults. Unlike previous ESM studies of the effects of sleep that focused on mood and anxiety (Harris et al., 2022; Lenneis et al., 2024; O’Leary et al., 2016; Patapoff et al., 2022; Peng et al., 2024; Ratcliff et al., 2014; Takano et al., 2013; Totterdell et al., 1994; Triantafillou et al., 2019; Werner et al., 2024), in this study, we investigated the effects of sleep satisfaction on symptoms that have been studied rarely or not at all, including apathy, irritability, impatience, hyperactivity, impulsivity, resistance to change, and sensory sensitivity. In addition, these diary data could be complemented with a comprehensive history of psychopathology experienced by each participant across five TRAILS assessment waves (in the age period between 11 and 25 years), which was used to determine whether associations between sleep satisfaction and daily symptoms were stronger in participants with a history of problems in four different domains of psychopathology.
Several limitations require caution when interpreting the findings. First, although sleep parameters should ideally be assessed on waking (Mulligan et al., 2019), sleep satisfaction in this study was assessed simultaneously with psychiatric symptoms in the evening, so the responses were more prone to recall bias. Although changes in sleep-satisfaction ratings throughout the day may not be affected by mood (Tang et al., 2023), lower sleep-satisfaction ratings were linked to more negative appraisal of daytime events (Song et al., 2024), which in our study, may have inflated the strength of the daily associations between sleep satisfaction and affect-dependent symptoms, such as apathy and worry. Second, diary responses about daily experiences highly depend on each participant’s interpretation of the questions, so the same items could be understood as signs of different psychiatric symptoms. For example, the item “I was unable to sit still” could be interpreted as restlessness associated with both ADHD and anxiety. However, the dynamic nature and less widespread use of momentary data complicate the assessment of validity and reliability of single items used in diary studies, and unlike for multiitem questionnaires, there are no standardized and widely accepted methodologies (Dejonckheere et al., 2022). Third, the study was well powered to detect within-persons associations, but the relatively modest sample size of N = 122 limits the power for detecting small between-persons effects, meaning that null or weak between-persons effects should be interpreted with caution; however, our results are in line with the findings of earlier cross-sectional studies on larger samples (Ghani et al., 2022; Hong et al., 2022). Finally, our study was exploratory, and more research is needed to validate our findings and complement them, such as investigating the effects of other domains of sleep health on everyday psychiatric symptoms and the effects of sleep satisfaction on other psychiatric symptoms.
Conclusions
Results of this study demonstrated that on a daily basis, individuals with lower perceived sleep satisfaction tend to experience a constellation of various psychiatric symptoms during the day, including apathy, worry, irritability, impatience, resistance to change, and sensory sensitivity. On the other hand, the reverse associations demonstrate that psychiatric symptoms can differentially predict lower next-night sleep satisfaction, although these effects are weaker and more symptom- and psychopathology-specific. Furthermore, day-to-day associations between sleep satisfaction and psychiatric symptoms can depend strongly on the personal history of psychopathology, especially internalizing and neurodevelopmental problems. Altogether, these findings underline the crucial role of healthy sleep in daily mental well-being across multiple psychiatric domains, particularly in individuals more vulnerable to psychopathology.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026261444282 – Supplemental material for Daily Associations Between Sleep Satisfaction and Psychiatric Symptoms in Young Adults at Risk of Psychopathology
Supplemental material, sj-docx-1-cpx-10.1177_21677026261444282 for Daily Associations Between Sleep Satisfaction and Psychiatric Symptoms in Young Adults at Risk of Psychopathology by Dina Sarsembayeva, Catharina A. Hartman and Marieke J. Schreuder in Clinical Psychological Science
Footnotes
Transparency
Action Editor: Jennifer L. Tackett
Editor: Jennifer L. Tackett
Author Contributions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.