
Abstract
The field of mental-health care continues to face the challenge of translating conceptual approaches into the idiographic reality of everyday clinical practice. For any framework to be both meaningful and useful to individual cases, it must account for the contextual, interconnected, temporal, and granular nature of such problems and prioritize clinical utility by design. In this narrative review, we aim to bridge this gap by proposing a workable framework building on these premises. Our proposal centers on the concept of “problem-sustaining patterns,” which aligns with the ongoing trend toward complexity thinking while offering sufficient clinical utility in practice. We advocate for a collaborative approach in which professionals and help-seeking individuals co-construct these models. Furthermore, we discuss the need for new digital tools to facilitate the procedural steps while also enabling development of generative models as clinical decision-making support tools, which could significantly enhance the feasibility of embracing complexity in clinical practice.
Keywords
A diagnosis is a prerequisite for adequate treatment of mental-health problems. Diagnostics involves the process of examining the nature and possible causes of a mental-health problem, which, in turn, forms the foundation for making informed predictions about treatment outcomes and long-term prognosis. Errors in the diagnostic process may introduce a risk of unnecessary suffering and increase the likelihood of unfavorable clinical outcomes (National Academies of Sciences, Engineering, and Medicine [NASEM], 2015). For these reasons, a dedicated focus on diagnostics is paramount in the delivery of mental-health care.
Diagnoses serve multiple purposes in clinical practice (Perkins et al., 2018). Ideally, a diagnosis provides a parsimonious description of a mental-health problem that improves communication and enables shared understanding between professionals and help-seeking individuals. Furthermore, a diagnosis should provide the basis for treatment selection, symptom monitoring, and recovery evaluation (Luteijn et al., 2019; NASEM, 2015). A diagnosis also carries a profound experiential impact on those individuals who receive it because it influences their own understanding of the problem and shapes their treatment expectations (Perkins et al., 2018). Taken together, these functions underscore the continuing importance of diagnosis throughout an individual’s entire care trajectory.
The way in which diagnoses are formulated often depends on the setting or clinical orientation that is being practiced. A diagnosis derived from psychological assessment typically entails a broad and structured inventory of clinically relevant features (Bornstein, 2017; Luteijn et al., 2019), whereas a psychiatric diagnosis emphasizes pathological conditions manifested in both physical and behavioral aspects of human functioning (Hengeveld et al., 2019). Diagnostic formulations can also be adapted to specific therapeutic approaches, such as case formulations in cognitive-behavioral therapy (CBT; Beck et al., 1979; Persons, 2006) or schema-focused formulations in schema therapy (Young et al., 2003).
Empirical Diagnostic Practice
Regardless of which approach or formulation method is used, a diagnosis is essentially construed as a clinically meaningful model of the mental-health problem. Constructing such a model necessarily involves an empirical process guided by an iterative diagnostic-reasoning cycle. This cycle bears much resemblance to the scientific method used in research, albeit applied at the individual level (Luteijn et al., 2019). Thus, the empirical part of the diagnostic practice can be broken down into separate phases that are recurrently revisited, that is, (a) observation, (b) induction, (c) deduction, (d) testing, and (e) evaluation (see Fig. 1; de Groot, 1961/1994).
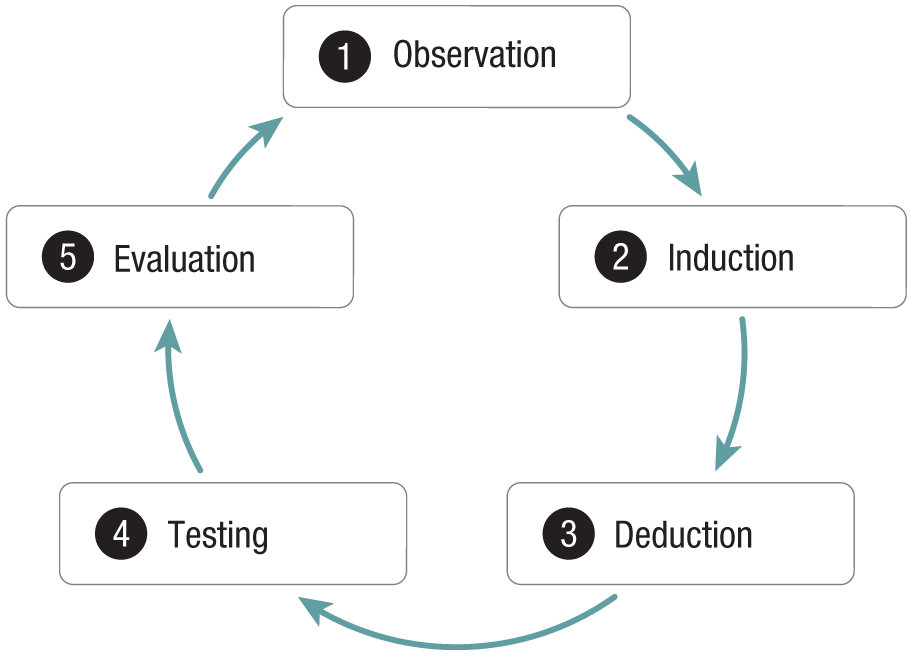
Illustration of the empirical diagnostic cycle, representing an iterative framework to refine the understanding of a mental health problem (de Groot, 1961/1994).
In practice, clinicians (implicitly) progress through this cycle by using their clinical observations to induce a broader conceptualization of what could be the problem and then deduce hypotheses from that conceptualization. Subsequently, these hypotheses are tested with appropriate instruments, the results of which are evaluated to either confirm or reject each hypothesis. As these evaluations feed back into the observation phase, the cycle repeats itself until sufficient evidence has accumulated to support a diagnosis of the mental-health problem. This iterative strategy makes the diagnostic practice inherently self-correcting, allowing for an optimal model to grow from repeated conjectures and refutations (Popper, 1959).
However, a crucial point to make here is that the efficacy of this empirical cycle is contingent on the assumption that one’s generic conceptualization of mental-health problems is sufficiently valid to serve as a solid foundation for generating adequate hypotheses in individual cases. In other words, the empirical cycle requires a well-defined understanding of what mental-health problems are and how they should be described in which it is presupposed that the unraveling of general features of mental-health problems is clinically relevant to every individual case. Despite decades of research and discussion, this presupposition is still challenged, as becomes apparent by ongoing and fundamental debates in the field (e.g., Eaton et al., 2023; Glas, 2019; Hyman, 2021; Kendler, 2016; Stein et al., 2024).
Consequently, a translational gap persists between findings produced through application of the empirical cycle in routine diagnostic practices and the needs of professionals and help-seeking individuals. This gap contributes to a variety of downstream challenges in the delivery of mental-health care, including inefficient care trajectories that result in prolonged treatment periods for help-seeking individuals. As demand for mental-health services continues to rise (ten Have et al., 2023), these inefficiencies place an additional burden on mental-health-care systems, which further compromises care quality and accessibility. Addressing these challenges requires strengthening the foundation of diagnostic practices, including the conceptual frameworks that underpin them, such that they sufficiently resonate with individual cases in routine care.
Present Article
In this article, we seek to address the aforementioned translational gap by presenting a narrative review of conceptual approaches to mental-health problems. From these insights, we propose a workable framework aligned with the needs of individual cases in clinical practice. Recognizing that any conceptual framework is a general approach by nature and that a gap with individual cases is an inherent feature of reality (Glas, 2019), our goal is not to eliminate it completely. Rather, we aim to provide clinicians and help-seeking individuals with the conceptual tools necessary to manage this gap effectively, allowing them to collaboratively generate diagnostic models that are meaningful and uniquely relevant to the individual. In doing so, this work aims to improve routine diagnostic practices and, ultimately, the delivery of mental-health care in clinical settings.
Our review proceeds as follows. First, we discuss conventional taxonomic approaches and the limitations they encounter when applied to individual cases. We then elaborate on the premises that conceptual frameworks must address to ensure clinical relevance. In light of these, we review the ongoing trend toward complex-systems thinking, noting that although many frameworks in this direction respond to these premises, most do not prioritize clinical utility. Building on these insights, we propose a framework centered on the concept of “problem-sustaining patterns” (Voerman et al., 2025). We suggest adopting an inferential strategy to collaboratively construct such models in practice and to augment this process with a Bayesian framework. We subsequently outline the procedural steps to effectuate this approach in practice and discuss the use of digital resources to support implementation. This includes exploring pathways for advanced clinical-decision support, such as generative modeling, which could significantly enhance the feasibility of embracing complexity in routine diagnostics. We discuss challenges and future directions in the final section of the article.
Taxonomical Approaches
The field of mental-health care has long been shaped by taxonomical frameworks for conceptualizing psychopathology. These frameworks have profoundly influenced how people think and talk about mental-health problems across clinical, research, and public domains. In this section, we briefly discuss traditional and emerging taxonomical frameworks and highlight inherent limitations that challenge their applicability in clinical practice.
Classification systems
Taxonomical approaches in mental-health care are exemplified by classification systems such as the International Classification of Diseases (World Health Organization [WHO], 2022) and the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association [APA], 2022), which categorize psychiatric phenomena and underpin these with concrete diagnostic criteria. Their adoption has become widespread in both research and practice (Shorter, 2013, 2015) given that diagnostic criteria improved communication about mental-health problems and provided clear targets for empirical research, pharmaceutical development and policymaking (Strand, 2011). It was initially assumed that the validity of these demarcations (i.e., “mental disorders”) would be confirmed through empirical research into their presumed neurobiological underpinnings (Spitzer et al., 1978; Spitzer & Fleiss, 1974). However, extensive efforts to identify reliable biomarkers have not produced sufficiently robust findings for clinical use (Abi-Dargham et al., 2023; Abi-Dargham & Horga, 2016), leaving the foundational validity of psychiatric categories unsubstantiated (Jablensky, 2016).
A clear manifestation of this lack of validity is the observed heterogeneity of symptom expression both between (Allsopp et al., 2019; Forbes et al., 2024) and within traditional psychiatric disorders (e.g., Fried & Nesse, 2015; Galatzer-Levy & Bryant, 2013). Moreover, individuals often meet the criteria for multiple disorders simultaneously (Kessler et al., 2005; Newman et al., 1998), especially when their mental-health problems are considered over an extended period of time (Caspi et al., 2020; Plana-Ripoll et al., 2019). These heterogeneity and comorbidity issues contribute to overdiagnosis and underdiagnosis of psychiatric disorders in clinical practice (Zimmerman, 2016) and limit the ability to effectively predict treatment outcomes (Eaton et al., 2013; Kim & Eaton, 2015; Kim et al., 2021; Krueger et al., 2018). Consequently, there is little optimism that continued research in the categorical paradigm will ever convincingly establish the validity of conventional psychiatric constructs (Hyman, 2010, 2021; Insel et al., 2010; Jablensky, 2016).
Alternative frameworks
Recognizing these limitations, various initiatives have been seeking to move toward more dimensional approaches, which are presumed to offer greater predictive validity (Krueger et al., 2018; Markon et al., 2011). The Research Domain Criteria (RDoC) project (Insel et al., 2010) is one such alternative, which argues that the absence of physiological indicators in standard diagnostic criteria undermines their ability to reliably validate psychiatric constructs (Cuthbert, 2014; Cuthbert & Insel, 2013). In response, RDoC proposes a framework that organizes aspects of mental health across multiple domains of neurobehavioral functioning (Cuthbert, 2014; Pacheco et al., 2022) and provides “units of analysis” to measure these dimensionally, ranging from molecular and genetic data to behavioral observations and self-report measures (Morris et al., 2022; Sanislow et al., 2022).
Another alternative framework is the Hierarchical Taxonomy of Psychopathology (HiTOP), introduced by Kotov et al. (2017), which seeks to disentangle the latent structure of psychopathology using statistical techniques, such as cluster and factor analyses (Forbes et al., 2021; Kotov et al., 2022; Krueger et al., 2018; Ruggero et al., 2019). This effort has resulted in a hierarchically organized framework that includes multiple levels of covarying transdiagnostic factors (Kotov et al., 2021). Mental-health problems are characterized as unique scoring profiles across all dimensions (Kotov et al., 2022; Ruggero et al., 2019), which effectively accounts for the heterogeneity and comorbidity issues of categorical approaches (Forbes et al., 2021).
Other alternative diagnostic frameworks have adopted hybrid approaches that combine dimensional and categorical perspectives to preserve some of the practical benefits of categorical systems. For example, the Alternative Model for Personality Disorders (APA, 2022) defines personality pathology based on impairments in personality functioning (Criterion A) and the presence of maladaptive personality traits (Criterion B; Zimmermann et al., 2019) and offers dimensional indices to assess both. Subsequently, algorithmic methods can map these dimensional profiles onto specific personality-disorder categories (Waugh et al., 2017). Research demonstrates that this dual approach effectively addresses heterogeneity and comorbidity issues without compromising clinical utility (Bach & Tracy, 2022; Weekers et al., 2024).
Another hybrid approach is clinical staging (McGorry et al., 2006; McGorry & Mei, 2021), which focuses on capturing the dynamic and heterogeneous progression of mental-health problems (Clarke et al., 2025). This framework refines diagnoses by mapping disorders along a continuum reflecting their progression, prototyped from at risk (Stage 0) to treatment resistance (Stage 4; Dwyer et al., 2025). Clinical staging is considered hybrid because it acknowledges the transdiagnostic and dimensional nature of mental-disorder progression while superimposing a categorical, stage-based framework to support clinical decision-making (Dwyer et al., 2025; McGorry & Mei, 2021).
Limitations of taxonomical approaches
The frameworks discussed above are taxonomical in the sense that they seek to understand mental-health problems by either reducing such phenomena into generalized (categorical) abstractions or decomposing them into discrete, measurable constructs. Although such strategies are useful for classification, they are inherently limited to describing observable characteristics of mental-health problems at the “nomothetic” level, thus providing group-level information only. This limitation poses significant challenges when applying such frameworks to individual clinical cases in everyday practice, that is, at the “idiographic” level.
One limitation is the increased risk of “reification,” in which individuals mistakenly treat group-level constructs as real things (Hyman, 2010; Voerman et al., 2025) and presuppose that the construct itself causes their mental-health problem (e.g., “I am sad because of my depression”). Closely related is the tendency toward a reductionist fallacy (te Meerman et al., 2022) that assumes that a mental-health problem can be universally explained by a small set of underlying (latent) features. Such reductionism tends to obscure contextual influences that cannot be reduced to single (hidden) causes, such as the social environment or living conditions. Finally, taxonomical approaches typically avoid making etiological claims because mental-health problems often emerge from complex, interacting pathways characterized by both multifinality and equifinality (Nolen-Hoeksema & Watkins, 2011). Yet such etiological information is often important for developing tailored intervention strategies (Wittchen & Beesdo-Baum, 2018).
Taken together, these limitations emphasize how taxonomical approaches fail to capture the unique features of mental-health problems such that hypotheses derived from these conceptual frameworks often lack clinical relevance at the level of individual cases. To address this, there is a growing consensus that new conceptual frameworks are needed that move beyond traditional taxonomies and explicitly allow modeling of individual variability (e.g., Borsboom et al., 2022; Fried, 2022; Wright & Woods, 2020). By offering more personalized understandings, such models are expected to hold greater promise for aligning with the idiographic nature of diagnostic practices (Köhne, 2020), ultimately providing a better fit for the needs of both practitioners and help-seeking individuals.
Premises for Effective Translation
As the field moves toward developing new conceptual frameworks to better meet the needs of individuals and professionals in mental-health care, establishing foundational premises to achieve this becomes essential. At the very least, these premises should capture the nature of mental-health problems in ways that resonate with individual experiences while aligning with professional demands. To this end, we posit five such premises, encouraging frameworks to sufficiently address the contextual, connected, temporal, and granular nature of mental-health problems and incorporate clinical utility by design. We briefly elaborate on each of these in the following subsections.
The premise of contextuality
Mental-health problems are recognized to be shaped and influenced by the broader context that surrounds the individual (Kirkbride et al., 2024). Although external, such influences are often intrinsic to the manifestation of individual mental-health problems (Gómez-Carrillo & Kirmayer, 2023). In this regard, “contextuality” refers to influences beyond the intrapsychological domain, which may be physical, such as the body (e.g., Turner et al., 2006); social, such as the family situation (e.g., Lereya et al., 2015; J. Wang et al., 2007); or demographic, such as neighborhood adversity (e.g., Baranyi et al., 2021; Kivimäki et al., 2020).
Contextual factors contribute to the onset, incidence, persistence, and expression of mental-health problems (Bruffaerts et al., 2010; Kessler et al., 2010). Changes in context can cause mental-health problems to intensify or resolve entirely. Furthermore, contextual influences take various forms, including acute events (e.g., an accident), situational stressors (e.g., workplace conflict), or chronic conditions (e.g., living in poverty). Because identical contextual factors can affect each person in different ways, their impact can be meaningfully understood only at the individual level. A useful conceptual framework must therefore account for this person-specific variability to maintain clinical relevance.
The premise of connectivity
A meaningful understanding of mental-health problems further requires identifying not only which internal or external factors influence the problem but also how they do so. This premise serves to emphasize the necessity of adopting an interaction-dominant perspective to understand how mental-health problems manifest in individual cases (Hasselman, 2023). The term “connectivity” refers to the degree of interconnectedness between all involved factors (Turnbull et al., 2018) that collectively constitute the mental-health problem. In this view, the significance of any single factor to the problem should be judged by its interactions with other relevant factors (Epskamp et al., 2018; McNally, 2021).
Furthermore, the nature of these interactions can differ in many ways. They can be linear or nonlinear, reciprocal or asymmetric (directed), or reinforcing or inhibiting, and such characteristics may evolve over time. Multiple interactions can create feedback loops, generating cyclical processes that contribute to the self-organizing and self-regulating behavior of mental-health problems (Kauffman, 1993). Such dynamic connectivity allows mental-health problems to adapt or stabilize in response to disruptions, aligning with an ecological-systems perspective to mental-health problems and emphasizing systemic tendencies to maintain equilibrium or homeostasis (Goekoop & de Kleijn, 2021a; Gómez-Carrillo & Kirmayer, 2023).
The premise of temporality
As interactions inherently unfold over time, conceptual frameworks must account for the temporal characteristics of mental-health problems to provide a comprehensive understanding. In this regard, “temporality” refers to dynamic features, such as changes in the frequency of associated symptoms, including their duration, stability, or likelihood of recurrence, which are often clinically informative to individual cases (Olthof, Hasselman, Aas, et al., 2023). Innovations such as ecological momentary assessment (EMA) have enabled ways to capture temporal dynamics by repeatedly collecting real-time data from individuals in their natural environments (Shiffman et al., 2008). EMA findings have challenged the traditional assumption of gradual and linear change (Hayes et al., 2007), revealing instead that changes in mental health can occur suddenly and unexpectedly (Olthof, Hasselman, Aas, et al., 2023; Wichers et al., 2019).
Furthermore, EMA research shows that mental states operate across a wide spectrum of temporal frequencies (Lunansky et al., 2020). For instance, an emotion such as anger may change rapidly over seconds but can also display stable patterns across longer time frames, such as months. By monitoring such patterns, EMA studies have revealed complex temporal patterns that emerge from complex interactions (Bringmann et al., 2013; van de Leemput et al., 2014), such as power-law frequency spectra (Goekoop & de Kleijn, 2023), bursting, hysteresis (Cramer et al., 2016), attractor dynamics (Olthof, Hasselman, Oude Maatman, et al., 2023), and tipping points (Scheffer et al., 2009; Wichers et al., 2019). Recognizing and modeling these temporal dynamics provides deeper understanding of how mental-health problems develop, persist, and potentially resolve. Therefore, conceptual frameworks must find ways to meaningfully accommodate for such temporal information in individual cases.
The premise of granularity
The concept of “granularity” refers to the level of detail at which features of a mental-health problem are being evaluated; high granularity corresponds to a finer level of detail, and low granularity corresponds to a broader, more aggregated level of detail. In clinical psychology, this notion typically pertains to the degree of abstraction in psychological constructs (Forbes et al., 2021). For example, basic emotions, such as “sadness” or “fear,” are generally considered elementary in the sense that decomposing them does not offer any additive clinical meaning, whereas more complex traits, such as “antagonism” or “conscientiousness,” are viewed as aggregated constituents of such elements. These distinctions are intuitive to clinicians (e.g., to distinguish between “syndromes” and “personality traits”) and therefore considered important when modeling for mental-health problems (Wright & Hopwood, 2022). However, how psychological concepts at varying levels of granularity exactly relate to one another is often unclear and remains poorly understood (Eronen, 2021).
Granularity applies to both spatial and temporal dimensions of mental-health problems. Spatial granularity relates to the multilevel organization of the problem, ranging from discrete symptoms and experiences to broader traits; temporal granularity concerns the pace of change, from rapid moment-to-moment shifts to slow, long-term developments. Both spatial and temporal dimensions are often interdependent in terms of granularity given that constructs of low spatial granularity tend to exhibit slow temporal changes and those with high spatial granularity may vary quickly (Lunansky et al., 2020). This relationship underpins attractor dynamics, in which systems tend to gravitate toward specific configurations over time (Olthof, Hasselman, Oude Maatman, et al., 2023). Such characteristic states can be understood as constitutive elements that combine to form higher-order attractors within a hierarchy of part-whole relationships that extends across spatiotemporal scales (i.e., a mereology). Attending to granularity enables more precise and scalable models of mental-health problems that better reflect the layered, dynamic structure of psychological phenomena.
The premise of clinical utility
Although the previous premises focus primarily on the conceptual nature of mental-health problems, any framework must demonstrate practical utility to effectively translate to clinical settings (Beutler & Howard, 1998; First, 2005; First et al., 2004; Mullins-Sweatt & Widiger, 2009). Definitions of “clinical utility” generally trace back to the work of First et al. (2004), although its meaning depends much on the perspective of different stakeholders ((Smart, 2006). Clinical utility is most commonly assessed from the clinician’s standpoint. The WHO operationalizes clinical utility in terms of three criteria (Keeley et al., 2016; Reed, 2010; Roberts et al., 2012). First, a conceptual framework must establish a shared language to describe mental-health problems. Second, it must be applicable and easy to use across different settings and stages of care. Third, it must support clinical decision-making (First, 2005; First et al., 2004).
From a management and policy perspective, clinical utility also involves a framework’s ability to aid in the allocation of health-care resources by differentiating levels of need for care (First, 2010; Mullins-Sweatt et al., 2016; Reed et al., 2018). Furthermore, to achieve clinical utility, conceptual frameworks must be able to describe mental-health problems in ways that are representative, relevant, and meaningful to the individual seeking help (Perkins et al., 2018; Weekers et al., 2021). Without attention to such personal relevance, even the most advanced conceptual frameworks risk remaining detached from the idiographic reality they aim to improve. To prevent this, the development of conceptual frameworks should prioritize clinical utility from the very beginning.
Embracing complexity
When the premises of contextuality, connectivity, temporality, and granularity are jointly considered, it becomes apparent that they encourage conceptual frameworks to embrace rather than reduce the inherent complexity of mental-health problems. More specifically, they advocate for a complex, dynamic, and multilevel systems-based view. A systems-oriented approach to mental-health problems is not entirely new and can be traced back to the biopsychosocial model introduced by George Engel (Engel, 1977, 1980; Lehman et al., 2017). This early integrative approach continues to resonate with many practicing clinicians who work holistically in pragmatic ways. However, the biopsychosocial model has also faced criticism for its lack of conceptual precision and operational guidance (Bolton & Gillet, 2019; Ghaemi, 2009). This inadequate account of clinical utility has consequently prevented its systematic implementation as a diagnostic and decision-making tool in everyday clinical practice.
Nevertheless, advances in network science and dynamic-systems modeling have made it increasingly feasible to work with complexity in meaningful ways. In fact, complex systems are now studied and applied across a wide range of disciplines, including meteorology, economics, and computer science (Barabási, 2012). These developments offer promising foundations for building frameworks based on complexity science while remaining clinically applicable. Accordingly, growing consensus in the field suggests that adopting a complex-dynamic-systems-based approach represents a logical and necessary step forward (e.g., Borsboom et al., 2022; Fried & Robinaugh, 2020; Hayes & Andrews, 2020).
Complex-Dynamic-Systems Approaches
The shift toward complex-systems thinking represents a growing trend in mental-health research. Numerous initiatives have emerged that aim to develop and operationalize conceptual frameworks grounded in complex-dynamic-systems theory. In this section, we discuss several noteworthy developments that have been influential in shaping this shift, which include the network approach, active inference, and enactivism.
Network approach
The network approach, pioneered by Borsboom (2008), posits that psychopathological symptoms are not passive indicators of a latent construct (i.e., “a mental disorder”) but rather active agents that influence each other directly within a causal system (Borsboom, 2017; Borsboom et al., 2019; Cramer et al., 2016; Robinaugh et al., 2020; Roefs et al., 2022). These systems can be modeled as symptom networks, in which the state of every symptom continuously fluctuates on a spectrum of activity. Activation of one symptom in the network (e.g., anxiety) may trigger activation of other connected symptoms (e.g., concentration problems or fatigue) and potentially lead to a cascading effect activating the entire network that may persist even after the initial stressor is gone (Cramer et al., 2016). Sustained activation then becomes an emergent property of the network, which, according to the network approach, represents what is traditionally perceived as a mental disorder (Borsboom, 2017).
Arguably, the network approach is the most operationalized complex-dynamic-systems approach in the field of mental-health research. It has offered new methodologies and an extensive library of tools that allow for the statistical estimation of these networks. When applied to data gathered using EMA (Epskamp, 2020), such tools allow for the visualization of symptoms as nodes (dots) and the causal relationships between them as edges (lines; Borsboom & Cramer, 2013; Epskamp et al., 2012). These visualizations make complex phenomena easier to interpret and open up innovative avenues in research on mental-health problems that build on the principles of network science (Bringmann et al., 2013; McNally, 2021).
Active inference
Active inference had its origin in neurocognitive sciences, where it emerged as a theory to understand brain function (Friston, 2010; Friston et al., 2017; Parr et al., 2022). It particularly addresses how the brain infers a reliable understanding of the external world from the noisy electrical signals it receives from its sensory organs (Clark, 2013). Active inference leans heavily on predictive-processing theory, which posits that the brain actively generates predictions of the external world and simulates what it would perceive if these predictions were correct (Hodson et al., 2024). Any discrepancy between sensory input (i.e., what is perceived) and the internal predictive model (i.e., what is expected) is known as the “prediction error.” Organisms continuously work to suppress prediction errors to minimize surprise (Clark, 2018), thereby driving them toward stable, low-energy states, such as homeostasis (Goekoop & de Kleijn, 2021a; Pezzulo et al., 2015).
Active inference suggests that there are two primary options to minimize prediction errors (Friston, 2010; Parr & Friston, 2019). The first option is to update the internal predictive model such that the incoming information again matches the prediction (i.e., “belief updating” or “learning”). The second option is to perform an action to influence the environment and thereby alter the sensory input until it matches the internal prediction (Parr et al., 2022). Active inference is mathematically formalized using approximate Bayesian inference (Smith et al., 2022). It is suggested that the brain adopts these processes through hierarchical predictive coding, in which higher levels of the hierarchy represent more abstract and temporally extended predictions or goals (Clark, 2018; Goekoop & de Kleijn, 2023; Parr & Friston, 2018).
The principles of active inference can be applied to psychiatry to understand and describe mental-health problems (Goekoop & de Kleijn, 2021a, 2021b, 2023). From this perspective, such problems arise when a person persistently fails to minimize prediction errors and therefore cannot form an accurate model of a situation. These inaccurate models produce maladaptive actions, which, in turn, create problematic situations that are also misinterpreted, thus reinforcing a cycle in which poor understanding yields poor outcomes. Such vicious cycles self-organize as regularities in the dynamics between individuals and their environment and disrupt individuals’ ability to achieve personal or social goals. Over time, these cycles may interfere with basic (homeostatic) needs, producing a state of “disorder as instability.” Because this process involves continuous subject-environment interactions, both the individual and the surrounding (social) context may be the owner of the disorder that ensues.
Enactivism
Another influential viewpoint in the domain of complex-systems thinking is enactivism, which originated from cognitive science and philosophy (Thompson, 2007; Varela et al., 1991) and goes beyond the idea that mental processes are primarily the result of neural computations done by the brain (McGann et al., 2013). Central to this viewpoint is the characterization of organisms as autonomous systems that are self-producing, self-maintaining, adaptive, and situated in a particular environment (Di Paolo, 2005). Systems and environments mutually define one another and coevolve through continuous interaction over time (Thompson, 2007; Varela et al., 1991). According to enactivism, mental processes are fundamentally “enacted” through this dynamic coupling of brain–body–environment systems (McGann et al., 2013). This is often articulated through the “4E-approach,” which holds that mental processes are embodied, embedded, enacted, and extended (Newen et al., 2018).
An important concept in enactivism is “sense-making,” which relates to how organisms actively generate values and meaning through evaluating their interactions with the world in ways that are affective and grounded in their lived, embodied experiences (De Haan, 2020; Di Paolo, 2005; Thompson, 2007; Thompson & Stapleton, 2009). An extension of this notion is “participatory sense-making,” which describes how understanding emerges and transforms through the mutual engagement of individuals in ongoing, dynamic social interactions (De Jaegher & Di Paolo, 2007). Enactivist frameworks often draw on language from dynamical-systems theory to model such complex interactions (Gallagher, 2017).
Understanding mental-health problems in an enactivist framework requires addressing the integration problem, which concerns how diverse biopsychosocial factors dynamically couple to produce and maintain such problems (De Haan, 2020; Gallagher, 2022). Enactive interpretations have been proposed for various conventional psychiatric phenomena (e.g., De Jaegher, 2013; Gipps, 2020; Glas, 2020). A general framework was offered by Nielsen and Ward (2018), who suggested that mental-health problems can be understood as recognizable patterns of dysfunctional behavior across individuals in which dysfunctional behavior is defined as a stable pattern in the brain-body-environment system of individuals that runs counter to their values (Nielsen & Ward, 2018, p. 812). De Haan (2020) addressed the integration problem by introducing an existential dimension alongside the biopsychosocial ones, referring to the human capacity to relate to themselves through reflexive stance-taking. By integrating all four dimensions into an enactive framework, De Haan suggested that mental-health problems can be understood as structurally disordered patterns in “existentialized” sense-making.
The need for clinical utility
Complex-dynamic-systems approaches to mental-health problems rapidly evolve (Stein et al., 2024), and our coverage of this literature is by no means exhaustive. Many adjacent frameworks exist, such as ecological psychology (e.g., Lobo et al., 2018), complex adaptive systems (e.g., Olthof, Hasselman, Oude Maatman, et al., 2023), or cybernetic theory (e.g., DeYoung & Krueger, 2018). Moreover, complex-systems approaches continue to develop in both conceptual and methodological ways. For example, recent proposals seek to improve the network approach by integrating environmental factors to account for contextuality (e.g., de Boer et al., 2021; Lunansky et al., 2021) or adopting multilayered approaches to address varying levels of granularity (e.g., Brooks et al., 2020; Lunansky et al., 2020). This broader movement toward systems thinking is also accompanied by ongoing philosophical debate. Enactivism, for instance, encompasses a range of distinct viewpoints (Ward et al., 2017), and competing enactive frameworks for psychiatry remain critically discussed (e.g., De Haan, 2021; Nielsen, 2021). Furthermore, the question of whether enactivism and active inference are truly compatible with one another is much debated in the literature (e.g., Di Paolo et al., 2022; Gallagher, 2023; Ramstead et al., 2020).
Nevertheless, the growing interest in complex-systems thinking in the field of mental-health research stands in stark contrast to the degree to which these approaches are adopted in clinical practice. This likely stems from the fact that most of these frameworks have been developed without clinical utility as a primary goal (Russell, 2023). For example, person-specific networks of mental-health problems are generally inferred from EMA data (Bringmann, 2024), but collecting such data is time-consuming to carry out in practical settings and requires a prior understanding of the mental-health problem to be meaningful (De Smet et al., 2024). Moreover, even when properly quantified, networks are difficult to interpret and translate into actionable interventions, which impedes their usefulness in clinical decision-making (Bastiaansen et al., 2020; von Klipstein et al., 2020). The same critique applies to advanced conceptual frameworks, such as enactivism and active inference, which may be philosophically expansive but remain practically underspecified (e.g., Glas, 2020). As argued by Russell (2023), the ontological openness of such frameworks enables broad theorizing but leaves clinicians with little guidance and introduces normative ambiguity at the point of care. Moving forward, any of these conceptual frameworks must find ways to offer sufficient clinical utility in practical settings to translate meaningfully to individual cases.
Translation Into Clinical Practice
In the preceding sections, we established that for a diagnostic model to be effective, it must be able to account for the complex, contextual, temporal, and granular nature of mental-health problems in individual cases. Although advanced frameworks, such as network theory, active inference, and enactivism, address most of these premises, their development did not prioritize clinical utility from the beginning. As a result, the gap between theory and practice remains. In this section, we seek to bridge that gap by translating these theoretical advances into a practical diagnostic framework, for which we turn to the concept of problem-sustaining patterns. We discuss the implications of adopting this concept in empirical diagnostic practices and outline the procedural steps necessary for its assessment in clinical settings.
Problem-sustaining patterns
The concept of problem-sustaining patterns, as proposed by Voerman et al. (2025), seeks to understand mental-health problems in a revised way that resonates with the ongoing trend toward complex-dynamic-systems thinking yet is intended to offer clinical utility in practice. Voerman and colleagues formally defined a problem-sustaining pattern as “a pattern of dynamic interaction between biological, psychological, and/or social factors that persistently or recurrently counteracts or undermines everyday problem-solving activities.” Its ontology expands on the notion of “real patterns,” which posits that patterns are observable regularities in a complex system, much like a tornado is an observable regularity in a complex weather system (Dennett, 1991). Although the number of interactions in a complex system can be innumerable, a problem-sustaining pattern conceptually offers an objectifiable claim about what maintains the entire system in a suboptimal state, thus filtering out those interactions that significantly contribute to the mental-health problem.
This pattern-based conceptualization naturally aligns with the premises outlined previously. That is, its ontological emphasis on interactions inherently relates to the premise of connectivity, and its occurrence across different domains (e.g., physical, psychological, or social) addresses the contextuality premise. Furthermore, a problem-sustaining pattern is not a singular event but a dynamic phenomenon characterized by repetitive interactions that unfold over time, thus accounting for the premise of temporality. These interactions can occur at various levels of granularity in which, for instance, environmental conditions, psychological experiences, and neurobiological factors are all seen as influencing one another.
Most importantly, the concept of problem-sustaining patterns is designed to offer clinical utility. The notion of “patterns” creates a shared language for communication about mental-health problems that resonates to various stakeholders in practice (Voerman et al., 2025). This terminology also aligns with various established formulation-based therapeutic approaches that incorporate some form of pattern identification, including functional analysis in CBT (Beck et al., 1979; Persons, 2006) or schemas in schema therapy (Young et al., 2003). From the help-seeking individual’s perspective, this approach is inherently personalized, offering a meaningful framework to understand the individual’s unique problem. Furthermore, the “sustaining” aspect of the concept (i.e., the inability to escape the pattern by oneself) naturally signals a need for professional support (Bakker, 2019). Finally, once formalized, a problem-sustaining pattern outlines the interactions that contribute to the problem, revealing specific mechanisms that can be targeted by interventions, which aids in clinical decision-making.
Implications for empirical practice
Implementing problem-sustaining patterns as a conceptual framework requires a reorientation in clinical-diagnostic practice. Whereas traditional diagnostic approaches tend to focus on identifying the causal origins of a mental-health problem, this framework instead seeks to understand the dynamic interactions between biopsychosocial factors that collectively perpetuate the problem. Consequently, the empirical practice places less emphasis on deductive reasoning and hypothesis testing and more on broad observation, inductive reasoning, and pattern recognition. In this form, the empirical process is better characterized as an “inference to the best explanation” (Harman, 1965) in which the aim is to construct the most coherent and plausible explanation of the mental-health problem based on all available information and is continuously refined as new information emerges.
Although this shift may appear subtle, it carries significant procedural implications. Importantly, it introduces a “hermeneutic component” into the empirical practice such that it must be interpreted which factors and interactions, among the many possibilities, are most relevant and meaningful to an individual’s problem-sustaining pattern. This “judgment of relevance” feeds back into the iterative empirical-diagnostic practice. Although this approach relies on skilled judgment to some extent, it does not imply arbitrariness. Rather, judgments should remain grounded in clinical theory, empirical evidence, and professional expertise, all of which are considered alongside the individual’s lived experience. Ideally, this process results in a formalized problem-sustaining pattern that represents the most plausible and clinically useful explanation of an individual’s mental-health problem.
A Bayesian framework
In practice, this approach explicitly takes a clinical starting point. Van den Bergh et al. (2024) underscored this necessity by demonstrating that the majority of factors included in individual case formulations (i.e., problem-sustaining patterns) are largely unique. However, this uniqueness also complicates judgment of relevance because of the sheer number and diversity of potentially interacting biopsychosocial factors. For example, financial stress may appear as a risk factor, but its relevance depends entirely on how it interacts with other factors in the context of the individual’s mental-health problem. Without a structured method, this complexity may be overwhelming, creating a risk that the diagnostic process becomes overly dependent on intuition.
To address these challenges, the diagnostic practice of “inference to the best explanation” can be augmented by probabilistic reasoning in a Bayesian framework (Henderson, 2014; see Fig. 2). This approach allows for the integration of established nomothetic knowledge as prior expectations, which can be updated as idiographic information is gathered (Tiemens et al., 2020). Such integration can occur implicitly, as when clinicians naturally draw on internalized nomothetic knowledge from clinical experience and literature. However, this integration of nomothetic knowledge can also be made explicit through systematic information gathering across cases. Van den Bergh et al. (2024) demonstrated qualitatively that despite individual uniqueness, overarching themes emerge across personalized models. By collecting data systematically, such overarching information can be operationalized as nomothetic priors in a Bayesian framework, representing population-level expectations (Tiemens et al., 2020)
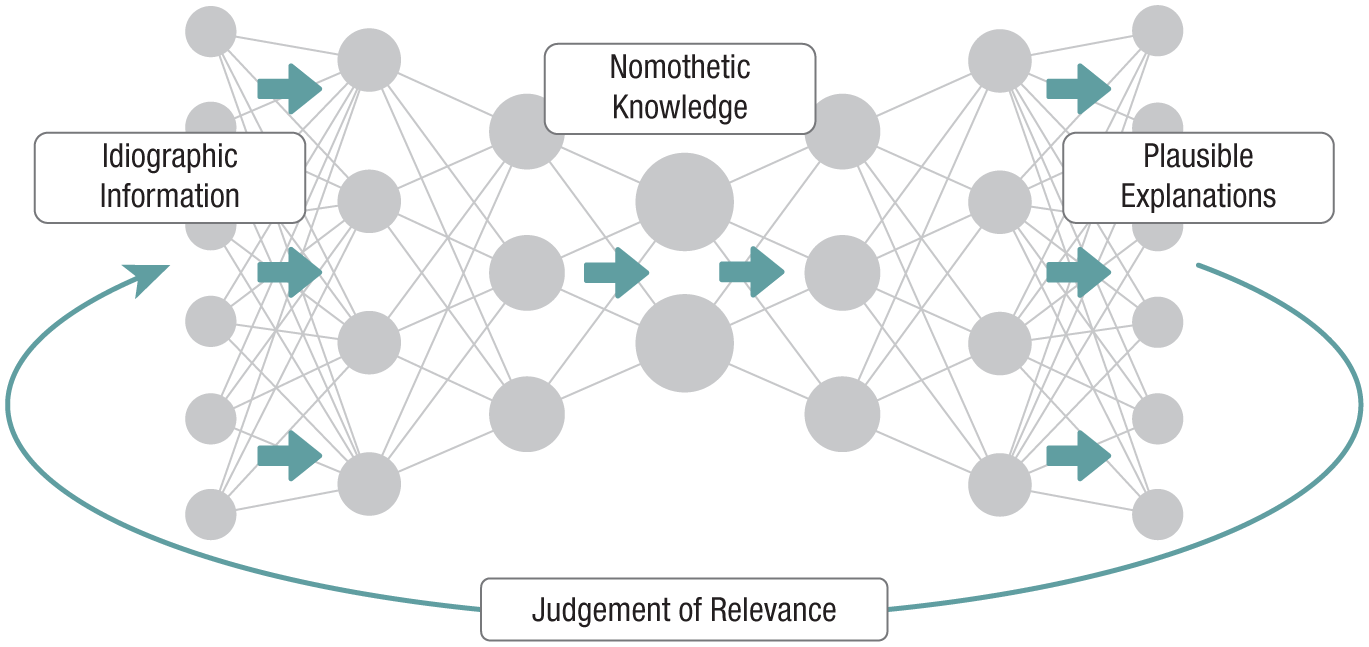
Illustration of how the diagnostic approach follows an “inference to the best explanation,” augmented by a Bayesian framework. Arrows indicate the flow of information. In this framework, idiographic information (e.g., observations, self-reports) is integrated with nomothetic knowledge to produce plausible explanations for the individual’s mental-health problem. Explanations are evaluated for relevance and meaning through collaborative dialogue between the clinician and the individual and iteratively refined until they converge on a formalized problem-sustaining pattern.
In both its implicit and explicit forms, Bayesian reasoning provides a structured procedure for identifying which information is likely to be relevant to the problem. Nevertheless, probabilistic estimates alone will not be sufficient. Gathered information must still be interpreted in terms of its relevance and meaning for the individual case. In practice, this requires a collaborative process between clinician and the help-seeking individual in which they jointly reflect on the information and judge its significance. The outcome is a formalized problem-sustaining pattern that represents a shared understanding of what best explains the mental-health problem and may serve as the basis for developing an appropriate intervention strategy.
Assessment in clinical practice
An explicit operationalization of a Bayesian framework in clinical practice requires that problem-sustaining patterns be clearly defined and formalized to enable probabilistic inference based on structured information. This can be achieved by visualizing the pattern as a graph in which relevant factors are represented as nodes and their interactions as connecting edges. The collaborative procedural approach then consists of three stages. It begins with the identification of relevant factors (the nodes), followed by an exploration of interactions between these factors (the edges) to form the pattern. Finally, the resulting formalization provides a concrete foundation for shared clinical decision-making. In the following subsections, we elaborate on each of these stages.
Factor identification
The procedure of factor identification is illustrated in Figure 3. This phase benefits from a comprehensive yet structured information-gathering strategy designed to broadly capture a range of biopsychosocial factors that potentially contribute to the individual’s mental-health problem. This strategy must be grounded in the premises outlined previously to adequately account for the complexity of such problems. Accordingly, it must consider the broader context of the individual (e.g., living conditions, life events, and social factors), address temporal dimensions (e.g., ontogenetic development, recent changes), and account for multiple levels of granularity (e.g., transient states, stable traits). Information must be drawn from multiple sources to enhance reliability and validity of this strategy (Bornstein, 2017), including clinical interviews, standardized assessments, observations, self-report measures, medical records, and input from significant others.
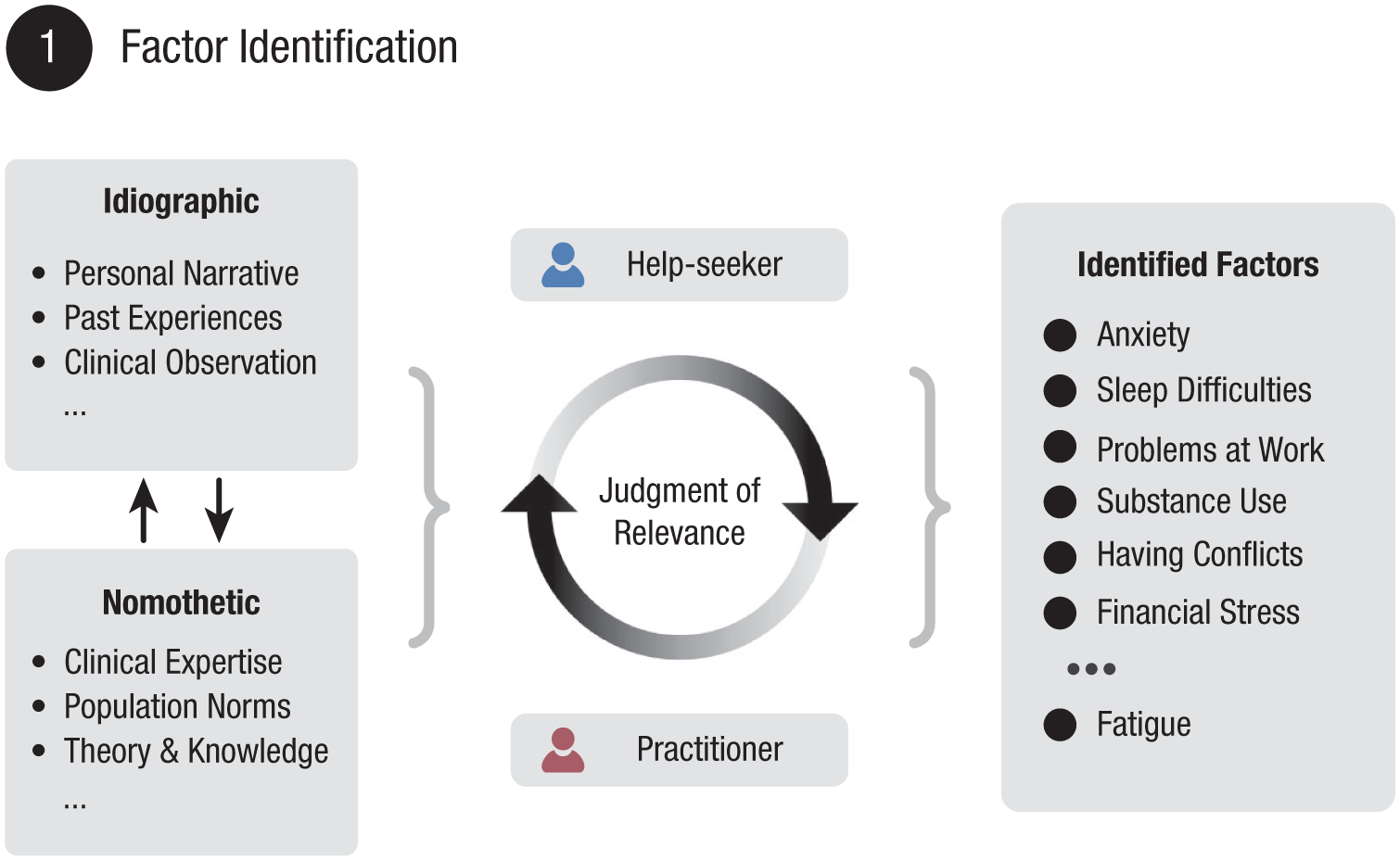
Illustration of the factor identification stage. Factor identification requires a comprehensive information-gathering strategy that incorporates diverse sources. This approach integrates both idiographic and nomothetic information in a Bayesian framework to identify potential contributing factors. The help-seeking individual and practitioner engage in collaborative dialogue to assess the relevance of each factor to the specific mental-health problem. This process culminates in a provisional working list of factors that contribute to the problem-sustaining pattern.
Gathered idiographic information is then synthesized by evaluating it against the backdrop of broader nomothetic knowledge, applying the principles of Bayesian inference. This occurs through a collaborative dialogical process in which the clinician and individual jointly make judgments of relevance regarding which factors are most meaningful. The phase concludes with a provisional working list of the most plausible biopsychosocial factors. This list provides the optimally informed foundation for formulating the problem-sustaining pattern in the subsequent steps.
Pattern exploration
Interactions between identified factors need to be explored to formalize a problem-sustaining pattern (illustrated in Fig. 4). Existing network approaches often attempt to model such interactions statistically using time-series data, assuming that a change in one factor followed by changes in another indicates a causal link (Epskamp et al., 2018; Robinaugh et al., 2020; Roefs et al., 2022). Although time series are informative, such approaches primarily reflect strong correlations rather than establish true causality (Bringmann, 2021). To address this, researchers have suggested incorporating qualitative methods, such as “perceived causal relations” (Deserno et al., 2020; Frewen et al., 2012). This method invites the clinician and the individual to collaboratively identify causal links based on lived experience and clinical expertise, resulting in more contextually relevant and meaningful connections (e.g., Burger et al., 2023; Klintwall et al., 2021).
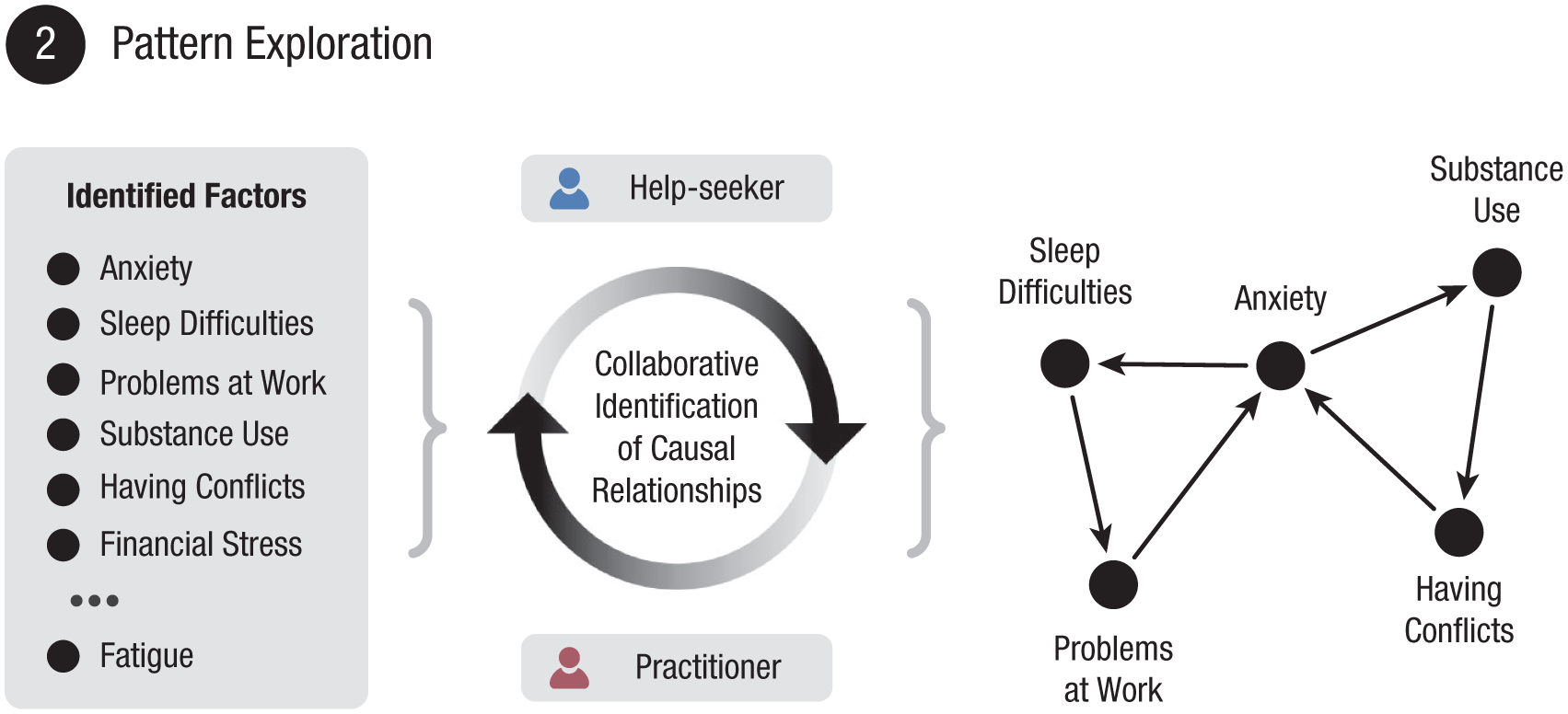
Illustration of the pattern-exploration stage. The provisional list of identified factors is used as a starting point. Through collaborative dialogue, the help-seeking individual and the individual’s practitioner map perceived causal relationships between factors in a dynamic process. The procedure results in a visualized problem-sustaining pattern. The self-sustaining nature of the problem is reflected by a feedback loop, formed by the directed arrows. This illustration demonstrates a relatively simple example of a pattern. In reality, patterns can be much more complex.
In practice, it would already be sufficient to identify directional relationships between factors to formulate a problem-sustaining pattern. However, such relationships can also be modeled in more complex ways. For example, other approaches additionally assess the strength or the positive/negative nature of such relations (e.g., Klintwall et al., 2021; Schiepek et al., 2015). Such extra detail can be valuable and informative to individual cases and would be compatible with our framework. Nevertheless, we encourage using such extensions only when their adoption is demonstrably feasible, meaningful, and useful in clinical practice.
The mapping of causal relations is a dynamic process in which new factors may emerge or may be left omitted through collaborative dialogue. This process is fundamentally shaped by the relational dynamics between the practitioner and the help-seeking individual. The result is a visualized problem-sustaining pattern that represents a shared understanding of the mental-health problem in question. Consequently, this diagnostic procedure must be flexible to tailor the pattern to the specific needs of the individual case. Although such adaptability is important, the procedure also benefits from a basic protocol and practical guidelines to ensure conceptual consistency and quality across cases. Although development of protocols and formal guidelines lies beyond the scope of this article, one such guideline may be, for example, a requirement that feedback loops are derivable from directed interactions to explain the sustainment of the pattern.
Clinical decision-making
Once a problem-sustaining pattern is collaboratively formulated and agreed on, it can serve as a practical map for identifying how to intervene (Voerman et al., 2025). This procedure (illustrated in Fig. 5) should be grounded in shared decision-making involving the help-seeking individual, the practitioner, and when appropriate, other stakeholders. Commonly used treatment techniques in mental-health care, such as CBT, eye movement desensitization and reprocessing, or exposure therapy, are designed to target particular mechanisms underlying mental-health problems. Over the past decade, the field of clinical psychology has established substantial evidence and knowledge regarding which interventions are effective for which mechanisms based on both empirical research and clinical expertise. This knowledge does not need to be abandoned when problem-sustaining patterns are used as diagnostic models for clinical decision-making. Rather, a visualized pattern could potentially provide a more refined representation of precisely those mechanisms that require intervention. In this way, problem-sustaining patterns may enhance clinical utility by supporting more targeted, mechanism-informed decision-making.
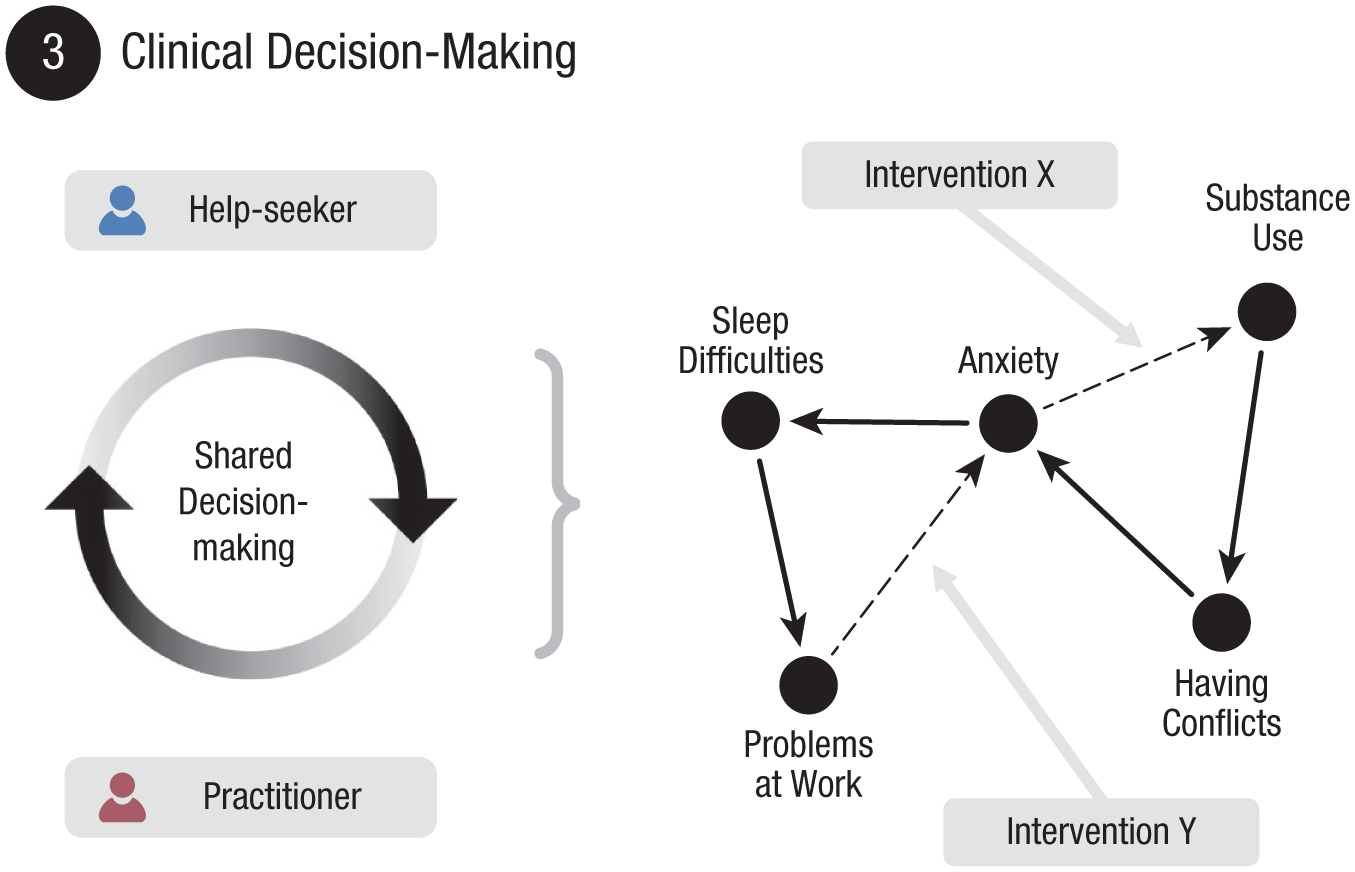
Illustration of the clinical decision-making stage. The formalized problem-sustaining pattern serves as a practical map for intervention planning. Through a process of shared decision-making, the clinician and help-seeking individual use this map to identify interactions in the pattern that are promising to target for change. Based on this, interventions can be selected aimed at disrupting problem-sustaining feedback loops.
Tools for Implementation
Most existing diagnostic tools in mental-health care have been developed in the context of taxonomical conceptualizations, which does not align with the empirical practice we proposed in the previous section. Therefore, to successfully implement a framework centered on problem-sustaining patterns, new tools will be necessary that support the procedural steps of factor identification, pattern exploration, and clinical decision-making.
Digital tools and resources
A shift toward inferential (Bayesian) reasoning in diagnostic practices introduces substantial information-processing demands, which can be effectively managed through the strategic use of digital resources (Stein et al., 2022). Integration of a digital infrastructure has become feasible and advantageous given the increasing ubiquity of digital tools in clinical practice (Torous et al., 2016). Such an infrastructure can reduce the logistical burden of collecting, storing, sharing, modifying, and analyzing information, thereby streamlining the procedural steps of our proposed framework.
To support the factor-identification process, digital tools must enable systematic gathering of biopsychosocial information in both structured and unstructured formats. Structured information can be obtained from self-report questionnaires, screening tools, rating scales, and checklists. Unstructured inputs may include narrative accounts, open-ended questions, clinical notes, or transcribed interviews, which can capture experiential and contextual nuances often missed by structured formats. Accessibility and efficiency of information gathering can be increased using digital means (Bond et al., 2023) while also allowing for advanced techniques, such as automated scoring and adaptive testing (Cella et al., 2007).
To facilitate pattern exploration, clinicians and individuals need a tool that enables them to visually connect identified relevant factors. Although this can be done using analog methods (e.g., on a whiteboard), digital tools offer the advantage of allowing users to dynamically adjust nodes and edges in real time. This enables a more interactive and collaborative experience, which better aligns with the empirical practice of iterative refinement we propose. That is, problem-sustaining patterns can be adapted as new idiographic insights emerge through collaborative clinical dialogue. In addition, digital interfaces make it possible to preserve patterns as structured data assets by storing nodes and edges as vectorized representations.
When using a dedicated digital infrastructure, clinicians can combine all gathered information into a digital case record, integrating structured assessments, unstructured narratives, and vectorized patterns into a single multimodal data object for each individual case. Aggregating these data objects across multiple cases creates a nomothetic source of information, from which base rates and population-based estimates can be derived, thereby informing priors for Bayesian inference. Such large-scale data sets open new pathways to support clinical decision-making through advanced computational analyses, including big-data analysis (Rutledge et al., 2019), precision psychiatry (Chen et al., 2022), and digital phenotyping (Insel, 2018; Montag & Baumeister, 2023). In this regard, machine-learning techniques are particularly promising because they offer a powerful approach to effectively deal with highly complex information.
Generative modeling
Generative modeling is a class of machine learning aimed at understanding how (clinical) observations are produced by latent factors such that new data can be simulated or generated based on this understanding (Moor et al., 2023; Torous & Blease, 2024). Generative models have gained public attention through large language models, which power chatbots that generate coherent conversational responses by predicting next words in a sequence. However, a variety of generative modeling techniques exists, including autoregressive models, variational autoencoders (Kingma & Welling, 2019), generative adversarial networks (Goodfellow et al., 2020), and other frameworks that model joint probability distributions (Bond-Taylor et al., 2022).
A key advantage of generative modeling is the capacity to simultaneously deal with different types of data from multiple sources (Haines et al., 2023). In mental-health care, this may include information from questionnaires, clinical interviews, medical records, wearables, and narrative transcripts (Moor et al., 2023; Sezgin & McKay, 2024). By jointly considering these data types, a generative model can detect underlying patterns and relationships that single-source analyses might miss and generate tailored insights or hypotheses that could support clinical decision-making in individual cases.
The field of mental-health care increasingly recognizes the potential of generative modeling, and many applications have emerged into various clinical domains, including diagnostics, monitoring, and interventions (Cruz-Gonzalez et al., 2025). Although such applications are promising, empirical evaluation of their clinical effectiveness is still in an early stage (Hua et al., 2025; L. Wang et al., 2025), and implementation faces many significant challenges with respect to ethics, privacy, reliability, and efficacy that need to be resolved (Saeidnia et al., 2024; Torous & Blease, 2024). Importantly, a foundational limitation of many current efforts is that generative models are often trained on data structured by traditional diagnostic taxonomies. As a result, their output remains confined to the conceptual constraints of those very frameworks.
Implementation in our framework
Generative modeling provides a natural extension to the Bayesian framework described earlier (see Fig. 2) because Bayesian methods align closely with the underlying philosophy of generative models (Haines et al., 2023). A generative model learns from multiple clinical cases to derive nomothetic priors and combines those priors with idiographic input to infer probable latent mechanisms that explain an individual’s mental-health problem. Based on this understanding, the model can generate personalized hypotheses about relevant factors or interactions that contribute to a problem-sustaining pattern. In this way, generative modeling has the potential to enhance feasibility of navigating complexity in clinical practice.
In our proposed diagnostic approach, a generative model may serve as a clinical decision-making support tool throughout the procedure (illustrated in Fig. 6). More specifically, the model could support the factor-identification phase by suggesting plausible biological, psychological, or social factors for the individual case. During pattern exploration, the model could propose nodes (factors) and edges (interactions), aiding clinicians and help-seeking individuals in their effort to cocreate a problem-sustaining pattern. In the clinical-decision-making phase, the generative model may suggest interventions targeted at certain aspects of the problem-sustaining pattern, supported by evidence from similar cases.
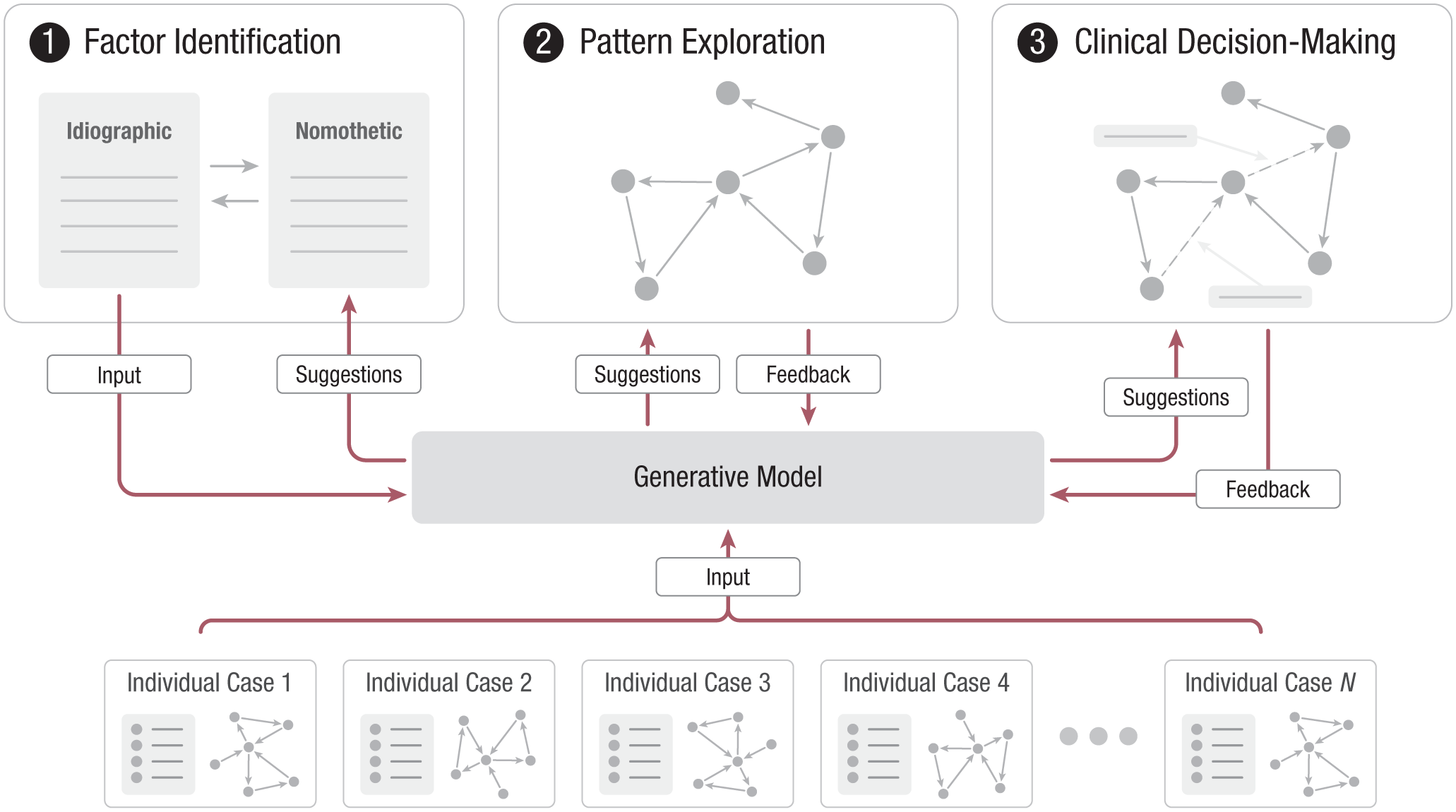
Illustration of how a generative model serves as a dynamic decision-support tool throughout the diagnostic procedure. (Top) Procedural steps of the active idiographic case. (Bottom) Nomothetic pool of aggregated individual cases in which each case contains all individually collected diagnostic information, including its finalized pattern. The generative model integrates two inputs, idiographic information from the individual clinical case and nomothetic priors from the knowledge base, to generate plausible, tailored hypotheses. These are offered as suggestions in every procedural step and may be accepted or rejected, constituting a natural feedback loop to the model. Completed idiographic cases are added to the aggregated pool, allowing continuous refinement of nomothetic priors and progressive improvement of the model’s ability to generate plausible hypotheses.
In every procedural step, however, the model’s suggestions must still be judged for relevance through collaborative dialogue between the clinician and the individual. Suggestions may be used, adjusted, or disregarded during the diagnostic process. This “human-in-the-loop” approach is imperative given that relevant diagnostic information often emerges through clinical dialogue, which cannot be captured by data alone. Generative models should thus be viewed as complementary tools (Guo et al., 2024; Sun et al., 2025) rather than replacements for clinical expertise. Therefore, a blended approach remains preferable in which a generative model may act as a third source of expertise to assist in the diagnostic process alongside the expertise of the clinician and the lived experience of the individual struggling with a mental-health problem.
Discussion
The field of mental-health care continues to face the challenge of translating conceptual approaches into the idiographic reality of everyday clinical practice. For any framework to be both meaningful and useful, it must account for the inherent complexity of mental-health problems while offering sufficient clinical utility. In this narrative review, we have argued that by conceptualizing mental-health problems as problem-sustaining patterns, it becomes possible to design a diagnostic framework that is grounded in complexity science yet remains feasible for routine application. This approach builds on a Bayesian framework to support clinical reasoning and can be enhanced with digital tools to systematically guide the diagnostic process.
The novelty of our proposed framework does not lie in a radical paradigm shift away from established clinical intuition. In fact, many practitioners already pragmatically engage in holistic approaches to understand the biopsychosocial factors maintaining an individual’s mental-health problems. The distinct contribution of our framework lies in the formal integration of this complex-systems thinking into the initial diagnostic-assessment phase. By structuring this process at the very beginning of individual care trajectories, the aim is to improve overall efficiency and effectiveness in the delivery of mental-health care.
Commitment to complexity
Complex-dynamic-systems-based approaches to mental-health problems often make operational concessions that compromise their commitment to complexity (Epskamp & Isvoranu, 2022). In this regard, Hasselman (2023) made a distinction between “weak” and “strong” commitments to complexity. Frameworks having a weak commitment typically use complexity as a guiding metaphor while continuing to rely on conventional methods and statistical analyses to address this. In contrast, strong commitments treat complexity as a foundational principle, requiring new methods that are idiographic, dynamic, and sensitive to nonlinear interactions over time. In light of this distinction, our proposed framework principally aligns with a strong commitment to complexity by adopting an interaction-dominant causal ontological concept (i.e., problem-sustaining patterns) to address mental-health problems. However, operational concessions have to be made nonetheless, although not in a methodological sense that would dilute the framework’s conceptual integrity of embracing complexity. Rather, concessions must be made purely to ensure that the approach is feasible and holds genuine utility daily practice.
Accordingly, the framework presented here is intentionally pragmatic. It provides a structured yet flexible procedure for integrating complexity thinking into routine diagnostic practice, which is achieved by mapping directional relations among relevant biopsychosocial factors and identifying problem-sustaining feedback loops. Although this approach to complexity is straightforward, it can serve as a foundation for more advanced modeling of complex phenomena. This may include, for example, mapping of multiscale interactions (e.g., Hasselman, 2023), quantifying and weighting of pattern components (e.g., Klintwall et al., 2021), or further assessing of dynamical and temporal properties (e.g., Olthof, Hasselman, Aas, et al., 2023). However, future work will be needed to empirically evaluate whether such extensions are feasible and interpretable and add meaningful clinical value. We recommend adopting them only when they demonstrably improve clinical utility.
Framework evaluation
Although we contend that our proposed framework offers meaningful improvements to diagnostic practices in mental-health care, demonstrating this empirically will not be straightforward. This difficulty stems largely from the empirical reorientation in our framework toward inference to the best explanation. In this view, the outcome of a diagnostic procedure is not a deduced model of the problem but must instead be construed as a hypothesis that best explains the observations. Hypotheses must be falsifiable to hold empirical value (Popper, 1959), which means that a problem-sustaining pattern must be structured in a way that allows for the possibility of being proven wrong. However, this poses a challenge because problem-sustaining patterns are dynamic and flexible by nature, which makes it difficult to define clear empirical criteria by which they could be falsified.
One way to address this challenge is to evaluate a diagnostic model by its predictive capacity using a Bayesian approach rather than seeking definitive falsification (Villarreal et al., 2023; Wagenmakers et al., 2018). That is, when an individual’s problem-sustaining pattern accurately predicts that a certain intervention leads to a meaningful improvement in mental health, then our confidence in the pattern’s validity as a diagnostic model increases. However, to demonstrate whether our proposed framework offers an improvement over other existing diagnostic practices, this evaluative strategy must be implemented on a much broader scale. Specifically, the concept of problem-sustaining patterns must be adopted in every stage of the mental-health-care system to enable systematic testing of clinical utility and predictive performance. Although this level of implementation is theoretically possible, the scale and complexity of such effort present considerable challenges in practice.
Ethical responsibility
The utility and meaningfulness of generative models for clinical decision-making in individual cases heavily depends on the quality and representativeness of the data on which they are trained. Any biases in these data can propagate throughout the model and result in structurally biased predictions and suggestions. This problem is commonly described as “garbage in, garbage out” and underscores the ethical responsibility to carefully manage development of such models and continuously verify that model-informed clinical decisions are not harmful to help-seeking individuals.
Recent calls in mental-health research have emphasized the need for more representative and ecologically valid data to address these risks of bias (Torous et al., 2023). In our proposed framework, this involves gathering information during initial diagnostic assessments in authentic clinical environments, where the need for professional support is most acute. It would be important to focus on a maximally heterogeneous population of help-seeking individuals to ensure applicability of the model in every case. Because our framework relies on digital tools to gather idiographic information and build a nomothetic knowledge base, special care must be taken to avoid excluding individuals who may have limited access to digital technologies or be less comfortable using them.
Even with such measures in place, however, generative models continue to remain a “black box” in nature. Without clear interpretability and external validation, they risk obscuring rather than clarifying clinical reasoning (Guo et al., 2024). Our framework addresses this to some degree by making a human-in-the-loop approach explicit, in which model suggestions are collaboratively considered and may be rejected when inappropriate. This prevents outputs of the model from becoming authoritative in decision-making (Sun et al., 2025) while also creating a natural feedback loop through which the generative model can learn from such rejections and improve over time. Nevertheless, integration of generative models in mental-health care remains to be done meticulously and must be guided by transparent, iterative research to ensure that their use in clinical practice is safe and ethically responsible.
Future directions
Translating the proposed diagnostic framework into clinical practice requires future work to concentrate on its formal implementation, the development of a digital infrastructure, and empirical evaluation of its effectiveness as a diagnostic practice. Given the framework’s emphasis on collaborative dialogue, establishing clear protocols and minimum quality standards will be important to prevent inconsistent or ad hoc implementation in practical settings. Future research should prioritize integrating these developments into actual clinical workflows to ensure clinical utility and generate ecologically valid data for ongoing refinement.
Various promising initiatives are developing protocols for clinical practice that adopt complex-systems or pattern-based conceptualizations, although most of these efforts do so in the context of therapeutic intervention rather than routine initial diagnostic assessment (e.g., Bakker, 2019; Burger et al., 2020; Hofmann & Hayes, 2019; Schiepek et al., 2015). A complementary effort is the Patterns of Life Project (Patterns of Life, n.d.), which seeks to specifically operationalize the concept of problem-sustaining patterns into routine diagnostic workflows by applying the procedural steps outlined here. Nevertheless, any tools, protocols, and models emerging from such initiatives will demand ongoing monitoring, empirical validation, utility testing, and ethical evaluation. Therefore, future research will be necessary to determine whether an approach using problem-sustaining patterns as diagnostic models provides a meaningful improvement over existing practices and whether it can reliably support clinicians in delivering more context-sensitive, personalized assessments.
Conclusion
A dedicated focus on diagnostics is fundamental for improving the delivery of mental-health care. This requires the use of conceptual frameworks that capture the complexity of mental-health problems in individual cases while offering sufficient clinical utility in practice. In this review, we have used the concept of problem-sustaining patterns to propose such a framework. By using an inferential, collaborative approach supplemented with a Bayesian framework, clinicians can integrate nomothetic knowledge with an individual’s unique life experience. Formalizing this assessment method early in the care pathway can lay the groundwork for advanced techniques that can address complexity and support clinical decision-making. This makes embracing complexity in clinical practice a feasible reality, promising to significantly improve the effectiveness, efficiency, and personalization of mental-health care.
Footnotes
Transparency
Action Editor: Pim Cuijpers
Editor: Jennifer L. Tackett
Author Contributions