
Abstract
Dissociation has long been thought to regulate distressing emotions. However, empirical findings are mixed. To test the purported regulatory effects of dissociation, we examined 88 participants with borderline personality disorder, posttraumatic stress disorder, and/or derealization/depersonalization disorder who experienced frequent dissociation. Specifically, we collected dense experience-sampling and continuous electrocardiogram data 1 week in daily life and additional electrodermal data, blood pressure, and salivary cortisol data during the Trier Social Stress Test. Results from dynamic-structural-equation and latent-change-score models showed a strong contemporaneous link between negative affect and dissociation in both daily life and the laboratory. However, we found no reduction in negative affect following dissociation and no consistent alteration in physiological responses during or after dissociation. These findings challenge traditional views of the emotion-regulatory functions of dissociation, highlighting the maladaptive nature of recurrent dissociation.
Keywords
Dissociation is a widespread phenomenon with profound implications for mental health (White et al., 2022). One comprehensive conceptualization of dissociation defines dissociation as a state of involuntary disruption or discontinuity in the normal integration of one or more mental capacities, such as sensation, perception, affect, thought, and memory (World Health Organization, 2022). However, an ongoing debate regarding the scope of the dissociation construct (Loewenstein, 2018) recognizes that differences exist within its broader definitions (Holmes et al., 2005; Nijenhuis et al., 2010; Spitzer et al., 2006). Common dissociative experiences include alterations in perception of the external world (derealization) and gaps in normally accessible aspects of awareness (gaps in awareness; Macia et al., 2022).
These experiences are not normally distributed across the general population—most adults experience little to no dissociation (Cˇernis et al., 2021; Ellickson-Larew et al., 2020; Heekerens et al., 2024; Macia et al., 2022). However, dissociation is frequently reported in clinical populations. A systematic review identified dissociative disorders, posttraumatic stress disorder (PTSD), and borderline personality disorder (BPD) as the primary categories in which these experiences are most pronounced (Lyssenko et al., 2018). Although many studies have focused on dissociation within specific diagnostic groups, previous research suggests that dissociation can be thought of as a transdiagnostic symptom, broadly related to psychopathology rather than specific disorders (Ellickson-Larew et al., 2020). A transdiagnostic approach is advantageous in its ability to investigate shared underlying dissociative processes across psychopathology (Conway et al., 2021) while still acknowledging that dissociative symptoms can have different etiological origins, some of which are disorder specific (i.e., traumatic experiences; Lynn et al., 2022).
Like many psychological states, dissociation has attracted functional explanations (Cardeña, 1994; Gershuny & Thayer, 1999). A functional explanation outlines the purpose or consequences that a particular response or experience is meant to achieve within a given environment. Theories generally assume adaptive functions because those should be favored by evolutionary processes. Researchers who believe that dissociative experiences are adaptive highlight two key functions: reducing distressing feelings (Dalenberg et al., 2012; Lanius et al., 2018; Saini et al., 2022; Sierra & Berrios, 1998; Steinberg, 2023; van der Kolk, 1987; Vancappel & El-Hage, 2023) and dampening physiological reactivity to prepare the body for immobilization (Hagenaars et al., 2014; Kozlowska et al., 2015; Lanius et al., 2018; Schauer & Elbert, 2010). In this study, we aim to empirically test these hypotheses, beginning with a review of the existing evidence.
Evidence for Dissociation’s Role in Regulating Negative Affect
Cross-sectional survey studies typically find strong associations between dissociation and indicators of ill-being, such as depression states, anxiety states, and negative affectivity, across diagnostic categories (for reviews, see Carlson et al., 2012; Krause-Utz et al., 2021; Lanius et al., 2018; Lynn et al., 2019). Furthermore, studies using multiple daily assessments have found positive within-persons associations between state dissociation and negative affect in patients with BPD (Stiglmayr et al., 2008), PTSD (Carlson et al., 2016), and depressive disorders (Heekerens et al., 2024). In addition, laboratory studies have shown increased state dissociation during or shortly after exposure to various stressors, such as personalized stressful narratives in BPD (Chung et al., 2020); arousal induced by the hyperventilation-provocation test in distressed individuals without a current diagnosis (Nixon & Bryant, 2006); fear induced by carbon-dioxide inhalation in panic disorder (Rassovsky & Kushner, 2003); psychosocial stress in BPD, PTSD, and major depressive disorder (Graumann et al., 2023; Zaba et al., 2015); and trauma scripts in PTSD (Danböck et al., 2024). This line of evidence further demonstrates that dissociation is closely related to negative affect.
Establishing an emotion-regulation function for dissociation also involves showing a reduction in negative affect shortly after dissociation, for which there is currently limited evidence. One study using multiple daily assessments showed that affective valence improved following dissociation for some participants with BPD but not depressive disorders (Heekerens et al., 2024). However, effects varied across participants and, on average, did not reach statistical significance, warranting further investigation. In laboratory settings, increases in dissociative experiences generally coincide with increases in negative affect in patients with BPD, PTSD, or major depressive disorder (Graumann et al., 2023). To our knowledge, few studies have conducted a fine-grained temporal analysis examining how variations in dissociative experiences during stress tests influence subsequent changes in negative affect. From an emotion-regulation perspective, individuals who exhibit earlier and more pronounced dissociation should experience a less intense increase in negative affect because dissociation may partially shield them from distressing experiences.
Evidence for Dissociation’s Role in Altering Physiological Reactivity
Findings on the association between dissociation and physiological reactivity are currently not consistently aligned (for reviews, see Beutler et al., 2022; Boulet et al., 2022; Roydeva & Reinders, 2021). For example, some studies have linked changes in acute dissociation with simultaneous decreases in heart rate (HR) and increases in high-frequency HR variability (HF-HRV) in PTSD (Danböck et al., 2024; Hauschildt et al., 2011), BPD (Krause-Utz et al., 2019), and depersonalization/derealization disorder (Schoenberg et al., 2012). However, other studies have found the opposite effect in major depressive disorder (Bob et al., 2009) or no significant effect in BPD (Ebner-Priemer et al., 2005), PTSD (Seligowski et al., 2019), distressed individuals without a diagnosis (Powers et al., 2021), and dissociative disorders (Schäflein et al., 2018). Some evidence suggests a nonlinear relationship between changes in HR and concurrent changes in dissociation in PTSD (Danböck et al., 2024). In addition, one study demonstrated higher nonspecific skin-conductance responses in relation to increases in dissociation in PTSD (Danböck et al., 2024), whereas other studies did not find this effect, potentially because of a lack of statistical power (Bichescu-Burian et al., 2017; Schmahl et al., 2004; Vermes et al., 2020). Regarding salivary cortisol, which is a marker for hypothalamic-pituitary-adrenal-axis reactivity, one study showed a blunted response for higher increases in dissociation during stress in a nonclinical sample (Morgan et al., 2001), whereas other studies found a positive association between dissociation and cortisol during stress in students (Giesbrecht et al., 2007) and military personnel (Morgan et al., 2004). In addition, past studies have reported conflicting findings on the relationship between dissociation and blood pressure; some showed an increase in individuals with dissociative disorders (Reinders et al., 2006), and others showed a decrease (Owens et al., 2015).
Despite frequent laboratory investigations, there is currently only one study that provided evidence on the contemporaneous relationships between dissociation and physiological parameters outside the laboratory. Beutler-Traktovenko et al. (2025) investigated the relationships between experiences of depersonalization and derealization with HR changes in 49 female inpatients with PTSD and found no significant correlation between dissociative episodes and HR changes. However, the study’s controlled hospital environment may limit its generalizability to daily life, highlighting the need for further research in more naturalistic settings.
Thus, there is currently limited direct evidence to inform whether physiological reactivity is reduced shortly after dissociation. The reason for this is that few studies have performed fine-grained temporal analyses to examine how variations in dissociative experiences during stress tests influence subsequent changes in physiological reactivity (Danböck et al., 2024, is one of the few that has done so). From an emotion-regulation perspective, individuals who exhibit earlier and more pronounced dissociation should experience a less intense physiological reaction because dissociation may partially shield them from distressing experiences.
The Present Research
The goal of this study is to investigate the emotion-regulation function of dissociation. Dissociation, defined as a mental state, was assessed through two dissociative experiences that relate to alterations in perception of the external world (derealization) and gaps in normally accessible aspects of awareness (gaps in awareness; Carlson et al., 2016; Stiglmayr et al., 2003). This study comprises two parts. We hypothesized that negative affect and physiological reactivity closely relate to dissociation and decrease shortly after dissociation both in daily life (Part 1) and in the laboratory (Part 2). These a priori hypotheses were preregistered (Heekerens et al., 2023). To test these hypotheses, in Part 1, we used dense experience sampling and electrocardiogram (ECG) data over 1 week in a transdiagnostic clinical sample. Part 2 involves a controlled lab-based stress paradigm with the same participants, adding measures of cardiovascular function, electrodermal activity, and cortisol levels. Dynamic-structural-equation models (DSEMs) and latent-change-score (LCS) models were employed to explore the temporal dynamics between affective, physiological, and dissociative states. By exploring the relationships between dissociative, affective, and physiological states, we aim to better understand whether—and under what circumstances—dissociation can be beneficial.
Methods
Transparency and openness
Preregistration
The daily life and laboratory parts of this study were preregistered (https://pubmed.ncbi.nlm.nih.gov/37287088/).
Data, materials, code, and online resources
Statistical code is available at https://osf.io/x4wa6/. After an initial embargo period, data will be made available at https://zenodo.org/records/15265833. A detailed laboratory protocol is available at https://doi.org/10.17504/protocols.io.e6nvwj85zlmk/v3.
Reporting
We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study. Additional material is available in the Supplemental Material available online.
Ethical approval
The process of the study was approved by the institutional review board of Charité – Universitätsmedizin Berlin (EA4_062_22).
Participants
Participants were included if they reported recurrent dissociative symptoms in the past week, evidenced by a total score of at least 20 on the Dissociative Symptoms Scale or at least 5 on the brief version’s items for derealization or gaps in awareness (Carlson et al., 2018; Macia et al., 2022). A total of 88 participants were recruited, as shown in the flowchart (Fig. S1 in the Supplemental Material). The sample comprises 38 persons with BPD, 21 persons with PTSD, 25 persons with both BPD and PTSD, and four persons with depersonalization/derealization disorder. Participants’ mean age was 30.32 years (SD = 8.59, range = 19–53), and there were 78 females. For demographic characteristics of participants, including self-reported ethnicity, see Table S1 in the Supplemental Material. For comorbid diagnoses, see Table S2 in the Supplemental Material. The gender distribution in our study aligns with previous research on dissociation in clinical samples (Al-Shamali et al., 2022). The high comorbidity rates of BPD and PTSD are consistent with past findings (Scheiderer et al., 2015). All participants were living in Germany at the time of the study and were consecutively enrolled from Charité – Universitätsmedizin Berlin between June 2023 and July 2024. We excluded participants who were currently hospitalized to investigate dissociation and affect in natural, everyday environments. All participants signed informed-consent forms before the study.
Participants were diagnosed with the German versions of the Structured Clinical Interviews for DSM-5 Clinical Version (Beesdo-Baum et al., 2019a), Personality Disorders (Beesdo-Baum et al., 2019b), and Dissociative Symptoms and Disorders (Steinberg, 2023) by J. B. Heekerens. Participants were excluded if they met criteria from the fifth edition of the Diagnostic and Statistical Manual for Mental Disorders (American Psychiatric Association, (2013) for bipolar disorder or any psychotic disorder in the past year or if they had a current severe major depressive episode, anorexia nervosa, severe alcohol use disorder, or any moderate to severe substance use disorder, except nicotine and caffeine, in the past 3 months.
Procedure
All eligible participants completed a set of self-report questionnaires (Heekerens et al., 2023; see Supplementary Methods in the Supplemental Material). For Part 1, they then downloaded two apps to their smartphones: m-path for receiving experience-sampling prompts and Multi Vital Monitor for connecting to the portable ECG recorders. Instructions were provided for using and charging the ECG recorder, which participants wore for 7 consecutive days following the diagnostic interviews. During this period, participants regularly responded to prompts on their smartphones. To assess self-reported affective and dissociative states, participants received 12 audio prompts daily between 9:00 a.m. and 9:00 p.m. for 1 week, totaling 84 prompts. Four prompts were sent within three random 60-min intervals each day (morning, afternoon, evening). Participants had up to 4 min to respond, ensuring evenly spaced time lags of approximately 15 min between prompts. In addition, participants received prompts daily at 9:00 a.m. and 9:00 p.m. At 9:00 a.m., they reported on nightly sleep disturbances, and at 9:00 p.m., they reported on daily stress, anxiety, depression, and social isolation. At the end of each 60-min interval, participants were asked about recent situations and activities, such as perceived social rejection, task-related stress, exercise, and positive social events. All questions are documented in the study protocol (Heekerens et al., 2023).
Afterward, for Part 2, participants underwent the Trier Social Stress Test (TSST; Kirschbaum et al., 1993; Linares et al., 2020), which was shown to effectively induce dissociation in a previous study (Graumann et al., 2023). The TSST had three phases. In the first phase, participants were asked to prepare a speech for 5 min. In the second phase, participants delivered the speech for 5 min in front of two judges (one male and one female), who were trained to respond in a discouraging way and take long pauses. In the third phase, participants were asked to perform mental arithmetic (1,022 – 13) in front of the judges for 5 min. Participants were asked on eight occasions to first report their levels of affect and dissociation. This was immediately followed by measuring their blood pressure and collecting a salivary sample on eight occasions (Fig. S2 in the Supplemental Material). HR, electrodermal activity, and respiratory rate were measured continuously. A laboratory protocol is available at dx.doi.org/10.17504/protocols.io.e6nvwj85zlmk/v3.
Self-report measures
In Parts 1 and 2, momentary affect was assessed using items from a validated measure designed to reliably capture within-persons variability (Wilhelm & Schoebi, 2007). Participants were asked to indicate their levels of arousal using two bipolar items (“relaxed-tense” | “entspannt-angespannt” and “agitated-calm” | “unruhig-ruhig”) and valence using two bipolar items (“bad-good” | “unwohl-wohl” and “content-discontent” | “zufrieden-unzufrieden”). The items used a slider from the starting position 0 to a maximum of 6. Before analysis, we recoded the second item in each dimension. Thus, higher arousal scores indicate feeling more tense and agitated, and higher valence scores indicate feeling more content and good. In daily life (Part 1), coefficient alpha for within-persons reliability for arousal was estimated at .82, 95% [CI] = [.81, .83], and for valence at .82, 95% CI = [.81, .83] (Tables S3 and S4 in the Supplemental Material; Lai, 2021). Across the eight assessments in the laboratory (Part 2), within-persons reliability for arousal was .81, 95% CI = [.78, .84], and for valence, it was .77, 95% CI = [.74, .81].
In Parts 1 and 2, momentary dissociation was assessed using the brief version’s items for derealization or gaps in awareness of the Dissociative Symptoms Scale (Macia et al., 2022). Participants were asked to answer two items indicating momentary derealization (“At the moment, things around me seem strange or unreal” | “Im Moment wirken die Dinge um mich herum fremd oder unwirklich” and “At the moment, I feel like I am in a movie – like nothing that is happening is real” | “Im Moment fühle ich mich wie in einem Film – alles, was passiert, wirkt unwirklich”) and two items indicating gaps in awareness (“At the moment, I realize I am not paying attention to what is going on around me” | “Im Moment merke ich nicht, was um mich herum vorgeht” and “At the moment, I am so focused on something going on in my mind that I lose track of what is happening around me” | “Im Moment bin ich so in meine Gedanken vertieft, dass ich nicht mitbekomme, was geschieht”). The items used a slider from the starting position 0 to a maximum of 4. In daily life (Part 1), coefficient alpha for within-persons reliability for derealization was estimated at .82, 95% CI = [.82, .83], and for gaps in awareness, it was at .79, 95% CI = [.78, .80] in the 1-week assessment in daily life (Tables S3 and S4 in the Supplemental Material). Across the eight assessments in the laboratory (Part 2), within-persons reliability for derealization was .80, 95% CI = [.77, .83], and for gaps in awareness, it was .69, 95% CI = [.63, .74].
Cardiac and respiratory assessments
In Parts 1 and 2, ECG recordings were sampled with a frequency of 128 Hz using portable three-lead recorders developed by Vivalink (Campbell, CA, USA). The wireless recorders were placed below the left collarbone on the chest. We used HR to indicate combined changes in cardiac sympathetic and parasympathetic activity and a cardiac chronotropic biological rhythm (respiratory sinus arrhythmia [RSA]) to indicate changes in parasympathetic activity. We used a frequency-domain metric, HF-HRV, and a time-domain metric, root mean square of successive differences (RMSSD), to indicate RSA. Following conventions, we used 5-min recordings covering the time immediately before participants submitted self-reports to calculate mean HR, HF-HRV, and RMSSD. We selected recordings taken before the self-report to minimize confounding effects because focusing on the prompt’s content could shift attention and potentially alter both dissociative experiences and associated physiological states. We report HR and HF-HRV in daily life (Part 1) and the laboratory (Part 2) in the main text. To reduce complexity, RMSSD for daily life data are reported in the Supplemental Material.
Data were preprocessed in two steps. First, we automatically detected artifacts from a time series consisting of differences between successive R-wave peaks (R-R intervals) using Kubios software (Kubios Oy, Kuopio, Finland). Second, we visually inspected the automatically cleaned ECG signal and manually corrected it, including the removal of all remaining artifacts. The average percentage of corrected beats across all 5-min recordings was 1.35% (SD = 2.19%) in daily life (Part 1) and 0.45% (SD = 1.07%) in the laboratory (Part 2). Afterward, Kubios software was used to detect R waves in the ECG to calculate consecutive R-R intervals. RMSSD reflects the root mean square of successive differences between R-R intervals. The HF-HRV parameter was indexed by calculating the absolute power (in ms2) of the high-frequency or respiratory band (0.15–0.40 Hz), reflecting parasympathetic (or vagal) influence on the heart. Because changes in respiration behavior affect the phenomenon of HF-HRV, we statistically adjusted for parallel-changes respiratory rate by regressing out respiratory effects on HF-HRV in our analyses (Quigley et al., 2024). The respiratory rate was estimated from the HR variability spectrum and measured in the range of 5 to 35 breaths per minute (brpm). HR was measured in the range of 40 to 300 beats per minute (bpm). The Vivalink ECG monitor also assesses movement using a 5 Hz three-axis accelerometer. We statistically adjusted for changes in corecorded physical activity by regressing out these effects on HR, HF-HRV, and RMSSD in our analyses (Quigley et al., 2024).
Blood-pressure assessments
Blood pressure was measured eight times using a blood-pressure cuff developed by iHealth (San Jose, CA, USA). The cuff was placed on the participant’s nondominant upper arm (brachial artery) at the height of the heart (as recommended by Berntson et al., 2017). Blood pressure was measured in units of millimeters of mercury (mmHg). We computed mean arterial pressure based on the highest blood pressure seen at systole (SBP; range = 60–260 mmHg) and the lowest seen in diastole (DBP; range = 40–199 mmHg) using the formula 1/3 × SBP + 2/3 × DBP.
Electrodermal assessment
Electrodermal activity was sampled using a textile band worn on the nondominant wrist with electrodes placed on the skin developed by Empatica Inc. (EmbracePlus; Picard et al., 2016). Although some studies found that electrodermal measures based on the recordings of wrist-worn devices only moderately correlate with measures obtained from traditional palmar devices, wrist-worn devices have been shown to successfully detect intraindividual differences in arousal levels across a variety of contexts, including clinical applications (Dawson et al., 2017; Kleiman et al., 2022). Skin-conductance level (SCL) was measured in units of microsiemens (μS) and in the range of 2 to 100 μS. The sampling rate is 4 Hz, meeting minimum requirements (Silva et al., 2023). Following our approach for ECG recordings, we used 5-min recordings immediately before the eight occasions participants submitted self-reports to calculate mean SCLs. We statistically adjusted for changes in corecorded external skin temperature at the recording site by regressing out these effects on SCLs in our analyses (Dawson et al., 2017).
Salivary cortisol
To assess salivary cortisol, we used cellulose pledges developed by Sarstedt AG (Salivette), placed in plastic carriers designed for low-temperature storage. After data collection, the samples were frozen on the same day and stored at −80 °C until biochemical analyses were performed at Charité – Universitätsmedizin Berlin, Germany.
Statistical analysis
We used Mplus (Version 8.11; Muthén & Muthén, 2025) and R (Version 4.4.3; R Development Core Team, 2025) for our analyses. We report a priori power analyses and handling of missing data in the Supplementary Methods in the Supplemental Material.
Part 1: main analysis of daily life data
Data were analyzed using DSEMs (Asparouhov et al., 2018). The approach separates interindividual between-persons differences (trait levels) from within-persons fluctuations around this value and allows investigation of interindividual differences in autoregressive and cross-lagged associations. DSEMs are implemented within a Bayesian framework, and parameters are estimated using a Markov chain Monte Carlo procedure. When reporting point estimates from DSEM analyses, we also provide 95% credibility intervals for context. We also report values for region of practical equivalence (ROPE). The ROPE is a predefined range of parameter values considered practically equivalent to a null value for an applied purpose. For the hypothesized cross-lagged relationships (Heekerens et al., 2023), we used a lower bound of −0.05 for expected negative effects and an upper bound of 0.05 for expected positive effects, reflecting directional hypotheses. For contemporaneous relationships, we employed a symmetric ROPE range of −0.05 to 0.05. We selected ROPE with bound of −0.05 and 0.05 because it reflects half the width of Cohen’s (1988) “small” effect (r = ±.10), and effects within this range explain ≤.25% of variance, rendering them practically negligible. Our thresholds are conservative because these effects are well below the typical range of meaningful correlations found in, for example, HRV research (Quintana, 2017). The ROPE uses Bayesian estimation to decide whether to accept or reject the null value by comparing the entire highest density interval (HDI) of the posterior distribution with the predefined ROPE. All our analyses used 89% HDIs, following the recommendations of Kruschke and Liddell (2018), and were implemented via the R package bayestestR (Version 0.15.2.3; Makowski et al., 2019). For reliability analyses, we use a maximum likelihood estimator and report 95% confidence intervals (CI). All models, except those estimating intraclass correlations, included autocorrelations of order 1 (AR[1]) at the within-persons level. Models used to estimate cross-lagged relations additionally include person-specific random innovation variances (also called “dynamic errors”). In these models, if appropriate, covariations between the variances of random innovations were allowed. All models used latent variables to account for measurement error when evaluating self-reported measures. Within-persons standardized results were based on the Mplus default procedure (Schuurman et al., 2016). Varying time intervals between assessments were accounted for by inserting missing data for omitted prompts (Asparouhov et al., 2018). Convergence was assumed if the potential scale-reduction factor fell below 1.10 (1.05 for hypothesis tests) for all parameters, using at least 5,000 iterations (20,000 iterations for hypothesis tests) and a thinning interval of 10 with the default Gibbs sampler for Markov chain Monte Carlo. All models used the Mplus default diffuse priors. According to scale-reduction factor values and visual inspection of trace plots, parameters for all models converged well. Before our calculations, we log-transformed HF-HRV values to achieve normalization. After transformation, the data exhibited near-normal distribution characteristics, with a skewness of −0.333 and kurtosis of 0.278.
Our analyses were performed in several steps. First, we ran univariate models to calculate intraclass correlations and latent means (trait levels; Tables S3 and S4 in the Supplemental Material). Second, we included predictor variables between levels to explore relations between latent means and exogenous variables (e.g., Patient Health Questionnaire–8 depression scores; Tables S3 and S4 in the Supplemental Material). Third, we included predictor variables within levels to explore relations between within-levels fluctuations and contextual variables (e.g., sleep disturbances, physical activity; Table S5 in the Supplemental Material). Fourth, we calculated bivariate models to investigate the contemporaneous within-persons relations between pairs of repeatedly assessed variables (Tables S3 and S4 in the Supplemental Material). Fifth, to test our hypotheses, we included cross-lagged associations at the within-persons level (Tables 2 and 3; for full results, see Tables S6 and S7 in the Supplemental Material). Cross-lagged effects focus on how one variable (e.g., derealization) at an earlier time predicts another variable (e.g., affective arousal) at a later time while accounting for the stability of both variables over time. Sixth, we examined differences between participants across diagnostic categories in these associations by including between-levels predictors (Table S8 in the Supplemental Material). Seventh, we repeated our hypothesis tests using two-part models that divided the dissociation variables into an observed binary (0 = no dissociation, 1 = dissociation) variable and a latent variable for positive dissociation values (dissociation > 1; Tables S9 and S10 in the Supplemental Material). Finally, we conducted additional tests for cardiac outcomes, incorporating quadratic terms to assess nonlinear relationships in dissociation’s contemporaneous and cross-lagged effects. These analyses are further described in the Supplementary Results in the Supplemental Material.
Part 2: main analysis of laboratory data
Data were analyzed using LCS models (McArdle, 2009). This approach provides a flexible framework for examining processes that change over time, specifically enabling analysis of how changes in two constructs relate over time. We opted for this approach over preregistered cross-lagged panel models because LCS explicitly models change, better suited to this study. All models include first-order autocorrelations (AR[1]) at the within-persons level and use latent variables to account for measurement errors in self-reported measures. When reporting point estimates from LCS analyses, we also provide 95% CI for context. All analyses employ robust maximum likelihood estimation to accommodate nonnormal distributions, particularly in dissociation indicators. We adopted a frequentist approach in Part 2 to leverage well-established procedures for model comparisons and streamline computational demands. We introduced a “phantom” variable—a latent variable without observable indicators—between the second baseline assessment (0) and the first assessment during the TSST (+10) to account for the unequal time interval between these measurements (Fig. S2 in the Supplemental Material; Voelkle & Oud, 2015). Model selection during model comparisons was based on the Bayesian information criterion (BIC), favoring the model with the lowest BIC value, provided there was no substantial reduction in model fit as indicated by a decline in comparative fit index (CFI; ΔCFI ≥ −.010) and/or an increase in root mean square error of approximation (RMSEA; ΔRMSEA ≥ .015; Chen, 2007; Usami et al., 2016). We chose BIC as the criterion because it penalizes model complexity, which aligns with our goal of efficiently describing change trajectories (Vrieze, 2012). Following Klopack et al. (2019), we considered the fit of our LCS models acceptable when CFI ≥ .95 and RMSEA < .08 (but for a nuanced discussion on the use of fixed cutoff values, see Groskurth et al., 2024). Before our calculations, we log-transformed several values to achieve normalization. After transformation, the data exhibited near-normal distribution characteristics across the eight time points in the laboratory session for HR (average skewness = −0.062; average kurtosis = −0.509) and RMSSD (average skewness = −0.085; average kurtosis = 0.840). However, moderate nonnormality remained for HF-HRV (average skewness = −0.547; average kurtosis = 1.940) and SCLs (average skewness = −1.59; average kurtosis = 3.40).
Our analyses were performed in several steps. First, we ran univariate latent state models to calculate (latent) means across time (Table S11 in the Supplemental Material). Second, we ran bivariate latent state models to calculate (latent) correlations between dissociation measures and all other repeatedly assessed outcomes across the eight measurement occasions (Table S12 in the Supplemental Material). We also explored quadratic correlations, incorporating quadratic terms to assess nonlinear relationships (e.g., Danböck et al., 2024). The results of these analyses are detailed in the Supplementary Results in the Supplemental Material. Third, we explored the functional form of the univariate change across time for each of our outcomes because the application of LCS modeling depends on accurately modeling changes over time, and more complex statistical models generally provide greater flexibility in describing these change patterns. We focused on five measurement occasions at the start and during the TSST because this time frame captured the most significant changes (Fig. 1; Table S11 in the Supplemental Material). One of the most flexible approaches is the dual-change-score model, which incorporates two distinct components: a proportional change component that depends on scores from the previous time point and a constant-change component that is additive. In other words, the model separates the global change process from the more localized, time point to time point deviations from that overall trajectory. In our univariate analysis, we compared three models for each of our outcomes: one with only a proportional-change component, one with only a constant-change component, and the dual-change-score model, which includes both. Fourth, we calculated bivariate LCS models to determine whether there are significant average changes in our outcomes over time and to examine how changes in dissociation relate to changes in other repeatedly assessed outcomes (Tables 4 and 5). In all bivariate models, the functional change form and the starting points of the proportional- and/or constant-change factors were fixed to a priori values based on results from the univariate models. The bivariate models include either derealization or gaps in awareness as indicators of changes in dissociation across time. In addition, the models incorporate a second outcome of interest (e.g., affective arousal or HR), enabling the investigation of cross-domain couplings. These couplings reflect the extent to which changes in one construct (e.g., derealization) are influenced by the initial level in another construct (e.g., affective arousal or HR). We compared four models for each pair of outcomes: one without coupling effects, one in which only changes in dissociation influence subsequent changes in the other construct, one in which only changes in the other construct influence subsequent changes in dissociation, and one with full coupling effects between both constructs (Table S13 in the Supplemental Material; Klopack et al., 2019). Fifth, we included predictor variables at the between-persons level to explore the relationship between univariate slope factors for changes during the TSST and diagnostic status (Table S14 in the Supplemental Material).
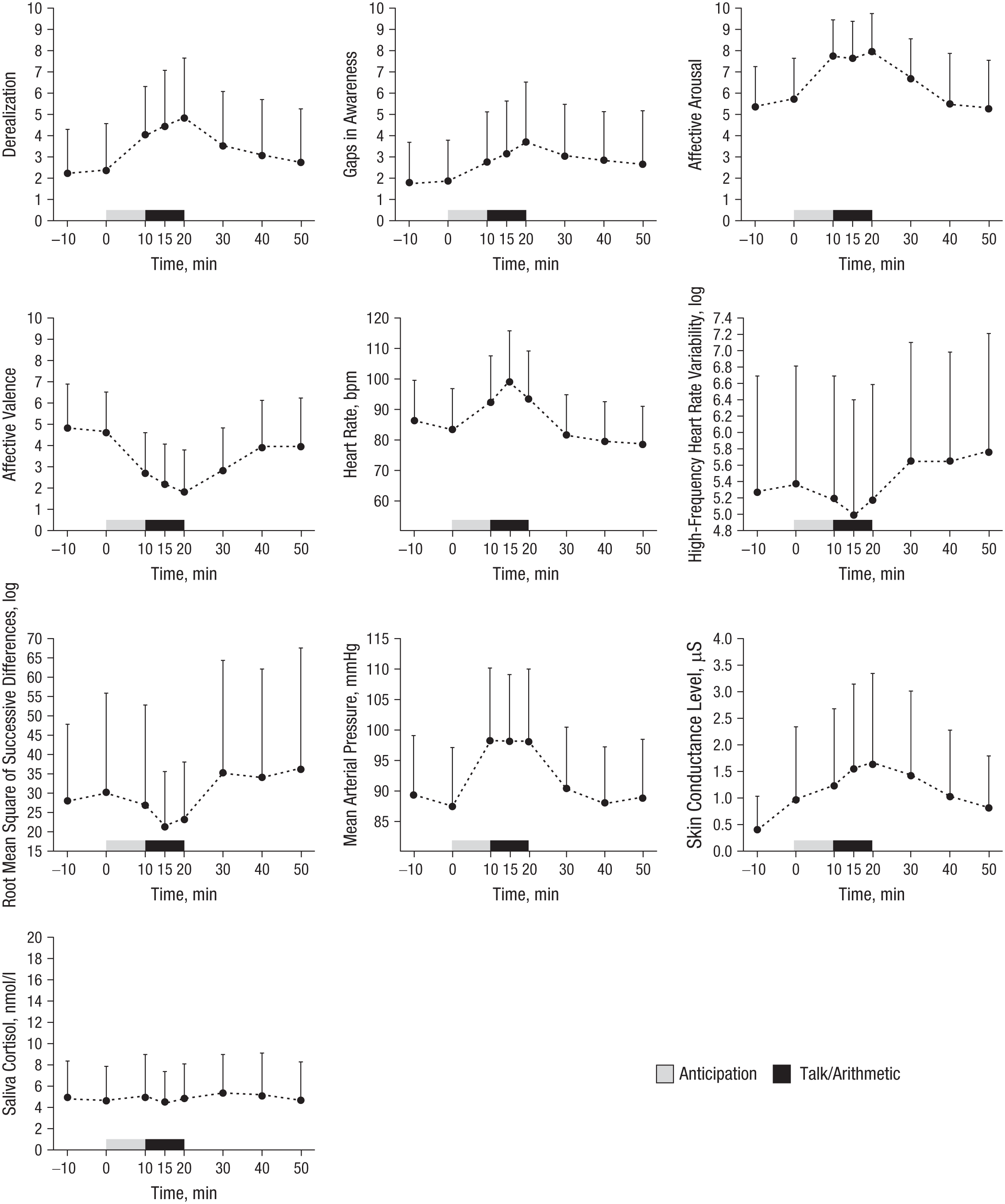
Mean changes in self-reported dissociation and affect and cardiac, blood-pressure, electrodermal, and salivary-cortisol response to the Trier Social Stress Test (TSST).
Measurement-invariance testing
The application of LCS modeling relies on the assumption of metric measurement invariance (Millsap, 2011). To evaluate this assumption, in a first step, we fitted models indicating configural invariance in which the general measurement structure is set to be equal across time (i.e., the same item loadings on the same factors across time) but the intercepts, factor loadings, and residual variances are freely estimated. In the next step, we fitted models to test for scalar invariance, in which both the intercepts and factor loadings were constrained to remain equal across time points. By comparing the fit of the configural and scalar models, we found that metric-invariance models were preferred for our repeatedly assessed self-report constructs. Details are provided in the Supplementary Results in the Supplemental Material.
Results
Main results are summarized in Table 1. To test our hypotheses in daily life (Part 1), we investigated the average standardized contemporaneous relationships between dissociative states and affective and cardiac states (Tables S3 and S4 in the Supplemental Material) and the average standardized cross-lagged relationships between these states (Tables 2 and 3). Estimates varied across individuals, as shown in Figures S3 through S5 in the Supplemental Material. To test our hypotheses in the laboratory (Part 2), we explored the average standardized contemporaneous relationships between the changes in dissociative states and affective and physiological states and the average coupling effects between these states (Tables 4 and 5).
Overview of Temporal Relations Between Dissociative, Affective, and Physiological States

Note: We present a summary of the contemporaneous and cross-lagged standardized relationships between dissociation and affective and physiological measures in daily life and the laboratory. Upward arrows indicate significant positive relationships, downward arrows indicate significant negative relationships, and left-right arrows represent nonsignificant relationships. Gaps = gaps in awareness; RMSSD = root mean square of the successive differences between heart beats; HF-HRV = high-frequency heart rate variability; bpm = beats per minute; mmHg = millimeters of mercury; μS = microsiemens; nmol/l = nanomoles per liter.
Results of the Dynamic-Structural-Equation Models of the Relations Between Affective and Dissociative States

Note: All parameters denote posterior medians. Parameters relevant to our hypothesis tests are in bold. The 95% CIs denote Bayesian credibility intervals.
p < .05.
Results of the Dynamic-Structural-Equation Models of the Relations Between Cardiac and Dissociative States

Note: All parameters denote posterior medians. Parameters relevant to our hypothesis tests are in bold. The 95% CIs denote Bayesian credibility intervals.
p < .05.
Results of the Bivariate Dual Latent-Change-Score Models of the Relations Between Affective and Dissociative States (N = 88)

Note: We show maximum likelihood robust estimates and fully standardized correlation coefficients. Estimates relevant to our hypothesis tests are in bold. Affective states of arousal and valence were assessed on scales from 0 to 6, and dissociative states of derealization and gaps in awareness were assessed on scales from 0 to 4. All models include latent variables measured with two indicators each. CI = confidence interval;
p < .05.
Results of the Bivariate Dual Latent-Change-Score Models of the Relations Between Physiological and Dissociative States (N = 87)

Note: We show maximum likelihood robust estimates and fully standardized correlation coefficients. Estimates relevant to our hypothesis tests are in bold. Dissociative states of derealization and gaps in awareness were assessed on scales from 0 to 4. All models include latent variables measured with two indicators each. Several physiological outcomes were log-transformed to achieve normalization. Heart rate is measured in beats per minute. Mean arterial pressure is reported in millimeters of mercury, skin-conductance level is reported in microsiemens, and salivary cortisol levels are reported in nanomoles per liter. CI = confidence interval;
p < .05.
Part 1: evidence from daily life
Preliminary analysis
The average number of answered prompts was 75.94 out of 84 (SD = 8.96, 90.41%) in daily life (Part 1). Because ratings were mandatory, participants answered all items if they responded to the prompts. Multilevel models showed that most variance in dissociative experiences in daily life was due to within-persons fluctuations rather than stable differences between persons; intraclass correlations were .41, 95% CI = [.30, .54], for derealization and .42, 95% CI = [.34, .51], for gaps in awareness (Tables S3 and S4 in the Supplemental Material). Latent means were 1.15, 95% CI = [1.02, 1.29], SD = 0.59 for derealization and 1.07, 95% CI = [0.94, 1.21], SD = 0.58 for gaps in awareness on scales from 0 to 4, indicating significant dissociation levels throughout the study week. Participants reported no derealization on average in 29.13 out of 84 occasions (SD = 19.85; 34.68%,) and no gaps in awareness on 26.71 occasions (SD = 20.53; 31.78%), suggesting floor effects. The average number of 5-min segments before prompts with available ECG data was 77.27 out of 84 (SD = 14.44; 91.99%) in daily life (Part 1). In addition, we observed significant within-persons fluctuations in the affective states (arousal and valence) and cardiac states (HR and HF-HRV; Tables S3 and S4 in the Supplemental Material). At the same time, dissociative, affective, and cardiac variables also showed substantial between-persons differences. We report the influence of baseline variables (e.g., questionnaire responses and diagnosis) on mean dissociation levels in Tables S3, S4, and S8 in the Supplemental Material and the influence of context variables and physical activity on current dissociation levels in Table S5 in the Supplemental Material. To test our hypotheses, we calculated contemporaneous and cross-lagged relationships between affective, cardiac, and dissociative states.
Contemporaneous links between dissociation, affect, and cardiac states
Dissociation ↔ affect
As shown in Table S3 in the Supplemental Material, the standardized relationships were 0.53, 95% CI = [0.50, 0.56], ROPE = 0.00%, between arousal and derealization, and 0.46, 95% CI = [0.42, 0.48], ROPE = 0.00%, for gaps in awareness (for credibility intervals, see Table S4 in the Supplemental Material). This indicates that dissociation at a given moment was positively related to arousal. Specifically, the estimate means that at time points at which arousal is 1 person-specific SD higher, derealization (or gaps in awareness) is, on average, 0.53 (or 0.46) of 1 person-specific SD higher. The ROPE values of 0.00% suggest that the null hypothesis of no practically relevant contemporaneous relationships between arousal and dissociation can be rejected with a reasonable degree of confidence. The relationship was significant and positive for 74 out of 87 participants for derealization and 60 out of 86 participants for gaps in awareness (for between-persons variation, see Fig. S3). Significant individual-level relationships suggest that for these participants, arousal and dissociation were consistently correlated at corresponding time points across the 1-week study period. Results in Table S8 in the Supplemental Material suggest that participants who were diagnosed with BPD reported significantly weaker relationships between arousal and gaps in awareness than participants diagnosed only with PTSD or depersonalization/derealization disorder. The standardized relationships were −0.55, 95% CI = [−0.58, −0.52], ROPE = 0.00%, between valence and derealization and −0.51, 95% CI = [−0.55, −0.48], ROPE = 0.00%, for gaps in awareness (Tables S3 and S4 in the Supplemental Material). This indicates that dissociation at a given moment was negatively related to valence (i.e., participants reported less pleasant affect). The relationship was significant and negative for 72 out of 87 participants for derealization and 68 out of 86 participants for gaps in awareness (Fig. S3 in the Supplemental Material). Results in Table S8 in the Supplemental Material suggest that participants who were diagnosed with BPD reported significantly weaker relationships between valence and gaps in awareness than participants diagnosed only with PTSD or depersonalization/derealization disorder.
Dissociation ↔ cardiac states
As shown in Table S3 in the Supplemental Material, the standardized relationships were 0.10, 95% CI = [0.06, 0.14], ROPE = 0.00%, between HR and derealization, and 0.10, 95% CI = [0.06, 0.15], ROPE = 0.00%, for gaps in awareness (for credibility intervals, see Table S4 in the Supplemental Material). This indicates that dissociation at a given moment was positively related to HR. The relationship was positive for 71 (18 significant) out of 86 participants for derealization and 63 (nine significant) out of 85 participants for gaps in awareness (for between-persons variation, see Fig. S3 in the Supplemental Material). One participant showed a significant negative relationship for derealization. Results in Table S8 in the Supplemental Material suggest that participants who were diagnosed with BPD reported significantly weaker relationships between HR and dissociation than participants diagnosed only with PTSD or depersonalization/derealization disorder. For HF-HRV, the contemporaneous relationships were −0.03, CI = [−0.07, 0.00], ROPE = 88.87%, for derealization and −0.01, CI = [−0.05, 0.03], ROPE = 99.80% for gaps in awareness (Tables S3 and S4 in the Supplemental Material). This indicates that dissociation at a given moment was not significantly related to HF-HRV. The ROPE values, which range between 0.00% and 100.00%, suggest that the null hypothesis of no practically relevant contemporaneous relationships between HF-HRV and arousal cannot be confidently accepted because some uncertainty remains in this conclusion. The relationship was negative for 64 (one significant) out of 86 participants for derealization and 50 (zero significant) out of 85 participants for gaps in awareness (Fig. S3 in the Supplemental Material). These results suggest that on average, HR was positively correlated with dissociation in daily life, and the relationships between dissociation and HF-HRV remained inconclusive.
Cross-lagged links between dissociation, affect, and cardiac states
Affect → dissociation
As shown in Table 2, the standardized relationships were 0.09, 95% CI = [0.07, 0.13], ROPE = 0.00%, between arousal and subsequent derealization and 0.07, 95% CI = [0.04, 0.11], ROPE = 11.13%, for subsequent gaps in awareness. This indicates that arousal at a given moment was positively related to dissociation approximately 15 min later. Specifically, the estimates mean that when arousal increased by 1 person-specific SD, derealization (or gaps in awareness), on average, increased by 0.09 (or 0.07) of 1 person-specific SD. The relationship was positive for 61 (13 significant) out of 87 participants for derealization and 67 (10 significant) out of 86 participants for gaps in awareness (for between-persons variation, see Fig. S4 in the Supplemental Material). The relationships were −0.07, 95% CI = [−0.10, −0.03], ROPE = 10.95%, between valence and subsequent derealization and −0.08, 95% CI = [−0.10, −0.05], ROPE = 0.00%, for subsequent gaps in awareness. This indicates that valence at a given moment was negatively related to dissociation approximately 15 min later (i.e., less pleasant affect predicted later dissociation). The relationship was negative for 68 (four significant) out of 87 participants for derealization and 83 (10 significant) out of 86 participants for gaps in awareness (for between-persons variation, see Fig. S4 in the Supplemental Material). The analysis revealed distinct ROPE percentages across tested relationships. The 0.00% ROPE values suggest strong evidence against the null hypothesis, demonstrating a practically relevant positive relationship between arousal and subsequent derealization and a practically relevant negative relationship between valence and subsequent gaps in awareness. ROPE values above zero indicate remaining uncertainty regarding the relationships between arousal and subsequent awareness gaps and valence and subsequent derealization. Results in Table S8 in the Supplemental Material suggest that participants who were diagnosed with both BPD and PTSD reported significantly stronger negative relationships between valence and subsequent derealization than participants diagnosed only with PTSD or depersonalization/derealization disorder, accounting for some of the between-persons variability in the results.
Cardiac states → dissociation
As shown in Table 3, the standardized relationships were 0.03, 95% CI = [0.01, 0.05], ROPE = 100.00%, between HR and subsequent derealization and 0.02, 95% CI = [−0.01, 0.03], ROPE = 100.00%, for subsequent gaps in awareness. This indicates that based on the 95% CIs, HR at a given moment was positively related to derealization (but not gaps in awareness) approximately 15 min later. The ROPE values indicate that both effects were practically zero, providing strong evidence in favor of the null hypothesis that there is no practically meaningful relationship. The relationship was positive for 63 (zero significant) out of 86 participants for derealization (for between-persons variation, see Fig. S5 in the Supplemental Material). There was insufficient between-persons variation to estimate random effects for gaps in awareness. The standardized cross-lagged relationships were −0.03, 95% CI = [−0.04, −0.01], ROPE = 100.00%, between HF-HRV and subsequent derealization and −0.04, 95% CI = [−0.06, −0.01], ROPE = 100.00%, for subsequent gaps in awareness. This indicates that based on the 95% CIs, HF-HRV at a given moment was negatively related to derealization and gaps in awareness approximately 15 min later. The ROPE values indicate that both effects were practically zero, providing strong evidence in favor of the null hypothesis that there is no practically meaningful relationship. The relationship was positive for 23 (two significant) out of 86 participants for derealization and 23 (two significant) out of 85 participants for gaps in awareness (for between-persons variation, see Fig. S5 in the Supplemental Material). Note that unstandardized parameter estimates did not reach significance in any of the models, and additional analyses using RMSSD instead of HF-HRV did not replicate the significant standardized results.
Dissociation → affect
As shown in Table 2, the standardized relationships were 0.03, 95% CI = [0.00, 0.06], ROPE = 100.00%, between derealization and subsequent arousal and 0.06, 95% CI = [0.03, 0.09], ROPE = 100.00%, for gaps in awareness. This indicates that based on the 95% CIs, gaps in awareness (but not derealization) at a given moment were positively related to arousal approximately 15 min later. The relationship was positive for 61 (three significant) out of 87 participants for derealization and 67 (seven significant) out of 86 participants for gaps in awareness (for between-persons variation, see Fig. S4 in the Supplemental Material). The ROPE values indicate that both effects were practically zero, providing strong evidence in favor of the null hypothesis that there is no practically meaningful relationship. The relationships were 0.01, 95% CI = [−0.02, 0.04], ROPE = 100.00%, between valence and subsequent derealization and −0.03, 95% CI = [−0.05, 0.01], ROPE = 100.00%, for subsequent gaps in awareness. This indicates that dissociation at a given moment was not significantly related to valence approximately 15 min later. Again, the ROPE values indicate that both effects were practically zero, providing strong evidence in favor of the null hypothesis that there is no practically meaningful relationship. The relationship was negative for derealization in 31 (two significant) out of 87 participants and significantly positive in one participant (for between-persons variation, see Fig. S4 in the Supplemental Material). In summary, we can confidently conclude that there is no practically relevant relationship between dissociation and subsequent reduction in negative affect (i.e., we rejected the expected emotion-regulation function of dissociation).
Dissociation → cardiac state
As shown in Table 3, the standardized relationships were 0.03, 95% CI = [0.01, 0.05], ROPE = 100.00%, between derealization and subsequent HR and 0.02, 95% CI = [−0.01, 0.03], ROPE = 100.00%, for gaps in awareness. This indicates that based on the 95% CIs, gaps in awareness (but not derealization) at a given moment were positively related to HR approximately15 min later. Note that unstandardized parameter estimates for this relation did not reach significance, and additional analyses using RMSSD instead of HF-HRV did not replicate the significant standardized result. In addition, the ROPE values indicate that both effects were practically zero, providing strong evidence in favor of the null hypothesis that there is no practically meaningful relationship. The relationship was positive for 63 (zero significant) out of 86 participants for derealization and 62 (zero significant) out of 85 participants for gaps in awareness (for between-persons variation, see Fig. S5 in the Supplemental Material). The relationships were −0.01, 95% CI = [−0.03, 0.02], ROPE = 100.00%, between HF-HRV and subsequent derealization and 0.01, 95% CI = [−0.02, 0.03], ROPE = 100.00%, for subsequent gaps in awareness. This indicates that dissociation at a given moment was not significantly related to HF-HRV approximately 15 min later. Again, the ROPE values indicate that both effects were practically zero, providing strong evidence in favor of the null hypothesis that there is no practically meaningful relationship. The relationship for gaps in awareness was positive for 40 (two significant) out of 86 participants for derealization and 52 (two significant) out of 85 participants for gaps in awareness (for between-persons variation, see Fig. S5 in the Supplemental Material). In summary, we can confidently conclude that there is no practically relevant relationship between dissociation and subsequent reduction in cardiac reactivity (i.e., we rejected the expected emotion-regulation function of dissociation).
Part 1: results summary
Results indicate significant positive contemporaneous relationships between dissociation with both increased negative affect and elevated HR, although no such relationship was observed with HF-HRV. In addition, negative affect consistently predicted subsequent increases in dissociation approximately 15 min later. Across analyses, our findings consistently show no evidence supporting the notion that dissociation leads to reduced negative affect or diminished cardiac reactivity.
Part 2: evidence from the laboratory
Preliminary analysis
The average number of answered prompts was 7.74 out of 8 (SD = 0.78; 96.73%) in the laboratory (Part 2). Because ratings were mandatory, participants answered all items if they responded to the prompts. The average number of 5-min segments before prompts with available ECG data was 7.74 out of 8 (SD = 1.03; 96.73%); for electrodermal data, it was 7.36 out of 8 prompts (SD = 2.17; 92.05%); for blood pressure, it was 7.73 out of 8 (SD = 0.83; 96.58%); and for salivary cortisol, it was 7.64 out of 8 (SD = 1.55; 95.45%). Descriptive results indicate that dissociative experiences increased during the TSST and that derealization increased more than gaps in awareness (Fig. 1; for latent means across time, see Table S11 in the Supplemental Material). In addition, affective arousal increased, negative valence decreased, HR increased, HF-HRV decreased, blood pressure increased, and SCL increased. Peak reactivity in HR, HF-HRV, and blood pressure occurred before peaks in self-reports and SCL. The cortisol response was blunted (for comparisons, see Zorn et al., 2017). For contemporaneous relations between dissociation facets and all other repeatedly assessed outcomes, see Table S12 in the Supplemental Material.
The slope factors reported in Tables 4 and 5 show that changes in all self-report and physiological measures during the stress test were significant. These estimates are derived from the bivariate LCS models described in the fourth step of our analysis plan, as detailed in the Method section. For example, the slope factor for derealization was estimated at 0.23, 95% CI = [0.17, 0.30], indicating that on average, derealization was predicted to increase steadily by 0.23 points on a scale from 0 to 4 every 5 min, starting from the beginning of the stress test (0 min in Fig. 1) until its conclusion (20 min in Fig. 1). The associated factor variance of 0.56, 95% CI = [0.24, 0.78], revealed significant between-persons variation in this change, and some participants exhibited slower or faster increases or in rare cases, a decline in dissociation (Fig. S6 in the Supplemental Material). These differences were not explained by diagnostic categories (Table S12 in the Supplemental Material). We tested our hypotheses by investigating contemporaneous changes in dissociation, affective, and physiological states and coupling (cross-lagged) effects for these relationships. The investigation of contemporaneous changes between two variables examines whether changes in both variables (e.g., derealization and affective arousal) are predicted to occur simultaneously during the stress test. In contrast, the analysis of coupling (cross-lagged) effects explores whether the level of dissociation at one time point predicts changes in other variables at subsequent time points. From an emotion-regulation perspective, higher levels of dissociation would be expected to predict blunted affective and physiological responses, manifesting as reduced subsequent changes in these outcomes.
Contemporaneous changes in dissociation, affect, and cardiac states
Dissociation ↔ affect
As shown in Table 4, the standardized relationships between slope factors during the laboratory stress induction were 0.47, 95% CI = [0.24, 0.70], between changes in arousal and derealization and 0.13, 95% CI = [−0.18, 0.44], for gaps in awareness. For changes in valence, the relationships were −0.68, 95% CI = [−1.00, −0.36], with derealization and −0.34, 95% CI = [−0.76, 0.09], for gaps in awareness. This shows that on average, increases in arousal and decreases in valence coincided with increases in derealization but not gaps in awareness.
Dissociation ↔ cardiac state
As shown in Table 5, the relationships were −0.30, 95% CI = [−0.78, 0.18], between changes in HR and derealization and −0.19, 95% CI = [−0.64, 0.27], for gaps in awareness. For HF-HRV, the relationships were 0.48, 95% CI = [−0.25, 1.21], for derealization and 0.37, 95% CI = [−0.26, 1.00], for gaps in awareness. This shows that increases in HR and decreases in HF-HRV did not coincide with changes in dissociation. Figure 1 and Table S11 in the Supplemental Material show that average increases in cardiac parameters precede increases in dissociation, reaching maximum levels approximately one measurement interval (around 5 min) earlier.
Dissociation ↔ blood pressure
The relationships were 0.24, 95% CI = [−0.13, 0.61], between changes in mean arterial pressure and derealization and 0.22, 95% CI = [−0.10, 0.54], for gaps in awareness. This shows that increases in blood pressure did not coincide with changes in dissociation. Figure 1 and Table S11 in the Supplemental Material show that blood pressure increases during the TSST preparation phase and then levels off throughout the remainder of the stress test, whereas dissociation levels steadily rise.
Dissociation ↔ SCL
The relationships were −0.05, 95% CI = [−0.38, 0.28], between changes in SCL and derealization and −0.06, 95% CI = [−0.43, 0.31], for gaps in awareness. This shows that increases in electrodermal activity did not coincide with changes in dissociation, although on average, SCL and dissociation reach peak levels at approximately the same time (Fig. 1, Table S11 in the Supplemental Material).
Dissociation ↔ salivary cortisol
The relationships were −0.31, 95% CI = [−0.68, 0.06], between changes in salivary cortisol and derealization and −0.03, 95% CI = [−0.40, 0.33], for gaps in awareness. As shown in Figure 1 and Table S11 in the Supplemental Material, salivary cortisol levels began to rise approximately 15 min to 20 min after the onset of the stressor. This delay reflects the time required for cortisol to reach detectable levels in saliva following activation of the hypothalamic pituitary adrenal axis. Our results show that increases in salivary cortisol levels did not coincide with changes in dissociation 15 min to 20 min earlier.
Coupling effects in dissociation and affect, dissociation, and cardiac states
To investigate coupling (cross-lagged) effects, we compared models including these effects with models not including them. Results revealed no significant coupling effects between increases in dissociation and changes in affective or physiological states (Table S13 in the Supplemental Material). This shows that dissociation scores did not influence the subsequent change in affective and physiological states during the stress test or vice versa. For example, the level of derealization at the beginning of the speech task did not influence the increase in affective arousal during the 5-min speech task or affect the decrease in affective valence, the rise in HR, the reduction in HF-HRV, or any other changes in physiological parameters. The same held true for gaps in awareness and other phases of the stress test.
Part 2: results summary
Results indicate significant increases in dissociation during the laboratory stress test. Elevated negative affect aligned temporally with heightened derealization but not with gaps in awareness. We found no significant relationships between dissociation and concurrent changes in cardiovascular activity (HR, HF-HRV, RMSSD, blood pressure), electrodermal response (SCLl), or neuroendocrine response (salivary cortisol). In addition, we consistently found no evidence supporting the notion that dissociation leads to reduced negative affect or diminished physiological reactivity approximately 5 min to 10 min later.
Discussion
To our knowledge, this is the first study to investigate two potential adaptive functions of dissociation—reducing negative affect and altering physiological reactivity—using comprehensive experience-sampling and physiological data in a transdiagnostic sample of individuals with high levels of dissociation both in daily life and in the laboratory.
Limited evidence for emotion-regulation functions of dissociation
We found that two facets of dissociation—derealization and gaps in awareness—appear to be consistently associated with elevated levels of negative affect in daily life. In the laboratory, increases in derealization coincided with increases in negative affect. These findings are consistent with past studies in daily life (Carlson et al., 2016; Heekerens et al., 2024; Stiglmayr et al., 2008) and in the laboratory (Danböck et al., 2024; Graumann et al., 2023). We also replicated findings from a previous study indicating that for some patients—particularly individuals with comorbid BPD and PTSD—increases in negative affect consistently precede episodes of dissociation in daily life (Heekerens et al., 2024). This demonstrates that negative affect serves dual roles as both a correlate of dissociative experiences and a proximal antecedent.
In addition, we found little evidence that dissociation reduces negative affect in either daily life or laboratory settings (i.e., our results do not support the notion that dissociation serves as an effective emotional-regulation mechanism; e.g., van der Kolk, 1987; Vancappel & El-Hage, 2023). Indeed, we found no evidence of any practically meaningful changes in affect following dissociation. In some individuals, negative affect consistently worsened after dissociation in daily life, particularly in the gaps in awareness facet. However, results varied between persons given that individual participants showed reduced affective arousal or improved affective valence following experiences of derealization (Heekerens et al., 2024). This variability underscores the importance of considering individual patterns in the temporal relationship between dissociation and subsequent affective states.
The contemporaneous links between dissociation and physiological outcomes were variable in both daily life and the laboratory, which aligns with the current literature (Beutler et al., 2022; Boulet et al., 2022; Roydeva & Reinders, 2021). In daily life, dissociation was consistently positively correlated with increased HR at the same measurement occasion in several individuals, particularly individuals with PTSD (Beutler-Traktovenko et al., 2025). In the laboratory, peak responses in cardiac parameters, on average, occurred before peak dissociation levels, and no significant lagged associations were found (i.e., changes in cardiac parameters did not predict changes in dissociation). In daily life, HR and HF-HRV did not consistently change before increased dissociative states. This pattern does not align with participants’ self-reported increases in affective arousal preceding dissociation. These findings suggest that increased cardiac reactivity may play a role as a correlate of dissociative experiences but not a proximal antecedent, questioning the hypothesis that dissociation may be triggered by an autonomic stress response and highlighting the role of subjective changes in affective arousal (Boulet et al., 2022). In the laboratory, we also observed a blunted cortisol response, which is in line with research into hypothalamic-pituitary-adrenal-axis function under acute stress in PTSD (Metz et al., 2020; von Majewski et al., 2023), dissociative disorders (Simeon et al., 2007), and patients with substance use disorder who report heightened levels of PTSD symptoms (Dixon-Gordon et al., 2013).
In addition, we found no consistent pattern of reduced cardiac reactivity following dissociation in daily life (i.e., our results do not support the notion that dissociation is followed by states of cardiac hypoarousal; e.g., Schauer & Elbert, 2010). Increases in dissociation during the laboratory stressor also had no significant effect on subsequent cardiac states, SCL, blood pressure, or salivary cortisol levels. In line with previous findings, these results challenge the theorized model of physiological hypoarousal following dissociation (Beutler-Traktovenko et al., 2025).
Implications for functional accounts of dissociation
Our results address the notion that dissociation serves as a broad and involuntary coping (“defense”) response to perceived threats (Dalenberg et al., 2012; Saini et al., 2022). We provide evidence against the view that recurrent dissociative states effectively regulate negative emotions across various everyday situations or during acute social-evaluation-based stress responses in the laboratory (Steinberg, 2023; van der Kolk, 1987; Vancappel & El-Hage, 2023). Instead, although we did not find such an effect across all individuals, our observation that negative affect consistently worsened following dissociation for a few participants in daily life resembles patterns seen in maladaptive regulation strategies, such as rumination (Blanke et al., 2022). This maladaptive pattern was more pronounced for gaps in awareness than for derealization, suggesting that different facets of dissociation may serve distinct functions (Holmes et al., 2005). Furthermore, the between-persons variation in these effects indicates that dissociation may act as an effective form of emotion regulation for some individuals and remained maladaptive or insignificant for most others. This variability should be further considered in assessment tools for dissociative disorders (Steinberg, 2023), therapy models across therapeutic orientations (e.g., van der Kolk, 1987; Vancappel & El-Hage, 2023), and neurobiological models (Lanius et al., 2018; Sierra & Berrios, 1998).
Our findings provide little support for the idea that recurrent dissociation is broadly linked to reduced physiological reactivity leading to immobilization (Hagenaars et al., 2014; Kozlowska et al., 2015; Schauer & Elbert, 2010). Current models posit the perception of an imminent threat initially causes increases in negative affect, followed by behaviors that protect the organism from perceived or anticipated danger (fight or flight). If active defense is impossible, the mind is believed to gradually disconnect from its immediate surroundings (derealization) and to shut down mental processes (gaps in one’s awareness) that may hinder survival (faint or freeze). At this stage, arousal is theorized to decrease, resulting in emotional numbing and physiological shutdown. However, consistent with findings from a previous ecological-momentary-assessment study conducted in patients with PTSD in a hospital setting (Beutler-Traktovenko et al., 2025), we found no evidence supporting a reduction in autonomic reactivity during or shortly after dissociation. Instead, although we did not observe this effect in all individuals, a few participants exhibited further increases in HR in daily life, suggesting a pattern of autonomic escalation rather than shutdown. This finding should be considered when further developing models of the association between dissociation and physiological responses. These associations may vary depending on the context (e.g., dissociation during a stressful social interaction in adulthood vs. dissociation during childhood abuse), the individual’s state (e.g., lower vs. higher levels of dissociation), and stable between-persons differences (e.g., current level of psychopathology).
Limitations and future directions
Our study is the first to test fine-grained hypotheses regarding the temporal relationships between dissociation, affect, and physiological reactivity in both daily life and the laboratory. We used a study designed to detect effects predicted by current emotion-regulation theories of dissociation and a sample size guided by a priori power analyses. The use of identical measurement tools across contexts and comparable data analyses is a strength of this study. Because we do not find evidence for hypothesized effects, our Bayesian analysis approach, applied to the daily life data, is particularly effective in providing evidence for the null hypothesis through the reported ROPE values. However, our study also has several limitations.
First, we used a transdiagnostic approach, including participants from three diagnostic categories commonly associated with dissociation. The advantage of a transdiagnostic approach lies in its ability to investigate shared underlying dissociative processes across different diagnostic groups. However, it can also limit statistical power to detect potential disorder-specific effects. For example, only four participants had a primary diagnosis of depersonalization/derealization disorder. Future studies could aim to recruit larger transdiagnostic samples that include enough participants in different diagnostic groups to inform both shared underlying processes and diagnostic specific effects. Furthermore, our sample comes from a single study site located in Germany, a Western country. This limits the generalizability of our findings, and further studies are encouraged to explore the temporal dynamics of dissociation in more diverse samples.
Second, although we differentiate different aspects of dissociation and affect and report multiple indicators of physiological reactivity, our study is still limited by the selection of a finite number of measures of dissociative, affective, and physiological states. For example, we assessed two different but related aspects of dissociation: derealization and gaps in awareness (Carlson et al., 2018; World Health Organization, 2022). However, other aspects of dissociation, such as depersonalization, could not be included because of concerns about participant burden (for multifaceted measures, see Carlson et al., 2018; Cˇernis et al., 2021). Because we found some differences between derealization and gaps in awareness, future studies are needed to explore whether temporal dynamics differ in, for example, depersonalization. Likewise, although we assessed two common dimensions of affect (arousal and valence), we did not examine other dimensions, such as wakefulness (Wilhelm & Schoebi, 2007). Furthermore, we used consistent 5-min segments to analyze ECG data in both daily life and the laboratory, facilitating comparability. Different results may be obtained with finer-grained segments (e.g., 1 min or 30 s), which could be explored in future studies. In addition, future laboratory studies could investigate a broader range of physiological outcomes using measures of endocrine activity, such as oxytocin, adrenaline/noradrenaline, and testosterone/estrogen (Boulet et al., 2022). The results from our measure of SCLs could be validated against “gold-standard” assessments (Dawson et al., 2017). Studies in daily life could include ecological momentary measures of SCLs, blood pressure, and salivary cortisol. Furthermore, employing mobile electroencephalography would be of particular interest (Roydeva & Reinders, 2021).
Third, we combined ecological-momentary-assessment and laboratory methods to explore the temporal relationships between dissociation and affect, leveraging the unique strengths of each approach while mitigating their limitations. However, our investigations may still bias the processes being studied. For example, in ecological momentary assessment, we used audible beeps to enhance compliance while trying to ensure they were not so loud that they might reduce dissociative states given that loud sounds have been used to counter dissociation therapeutically. This approach yielded high compliance rates (> 90%) and occasional reports of intense dissociation, indicating minimal interference with the process being studied.
Fourth, although we observed similar levels of derealization and gaps in awareness in daily life, our laboratory stressor induced stronger derealization than gaps in awareness. Future research should investigate whether this difference stems from the social-evaluative nature of the stressor and aim to identify stressors that more effectively evoke gaps in awareness and other aspects of dissociation (for dissociation-induction strategies, see Brake et al., 2024; Leonard et al., 1999). Some procedures for inducing mild dissociation, such as the spiral staring task (Holmes et al., 2004), may also be feasible for administration outside the laboratory. For example, these could be implemented as an experimental manipulation embedded within an ecological-momentary-assessment study.
Fifth, although we achieved excellent compliance rates (> 90%) in this study, we were unable to fully ascertain the reasons for the missing data. For example, participants may have been unable to respond to prompts during periods of particularly intense distress and/or dissociation, raising the possibility that dissociation serves an emotion-regulation function only at higher levels. However, we collected numerous instances of dissociation at the extreme end of our scale, and these results do not support such a function. In addition, participants were considerably stressed and dissociated during the laboratory stress test, and we found no evidence of an emotion-regulation function in that context either.
Conclusion
We investigated the emotion-regulation functions of dissociation in a sample of individuals who experience frequent and intense dissociation in both daily life and the laboratory. Across contexts, we found that dissociation is closely associated with negative affect. However, we found little evidence that negative affect or physiological reactivity decrease shortly after dissociation, challenging emotion-regulation accounts of dissociation. Instead, our results underscore the maladaptive properties of dissociation.
Supplemental Material
sj-pdf-1-cpx-10.1177_21677026251396803 – Supplemental material for Does Dissociation Have an Emotion-Regulation Function? Evidence From Daily Life and the Laboratory
Supplemental material, sj-pdf-1-cpx-10.1177_21677026251396803 for Does Dissociation Have an Emotion-Regulation Function? Evidence From Daily Life and the Laboratory by Johannes B. Heekerens, James J. Gross, Sylvia D. Kreibig, Hannah L. Ober, Randy Eichentopf, Theresa Dittrich, Julia G. Lebovitz, Julian Hellmann-Regen, Katja Wingenfeld and Stefan Roepke in Clinical Psychological Science
Footnotes
Acknowledgements
We thank Matthias Hoheisel, Christian Otte, and Stefanie Koglin for their assistance during data collection; Nikolaus Kleindienst for providing the German translation of the Dissociative Symptoms Scale; Michael Eid, Jana Holtmann, and Mario Lawes for their feedback on the statistical-modeling approach; Maya-Elena Ienascu, Dunja Shalan, and Martin Tegtmeyer for their assistance during data collection and support in data cleaning; Marie Barthauer, Livia Graumann, Julia Jäger, and Tizian Rademacher; Laura Renée Lipka, Catarina Rosada, and all other colleagues from Charité – Universitätsmedizin Berlin for their help in administering the Trier Social Stress Test; Miles Edward Lucas for his help with the tables; and the study participants for their time completing the study.
Transparency
Action Editor: Vina Goghari
Editor: Jennifer L. Tackett
Author Contributions
K. Wingenfeld and S. Roepke contributed equally.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.