
Abstract
In this meta-analysis, we synthesized existing research on perseverative negative thinking, self-control, and executive functioning to better define their etiologic role in symptoms of depression and anxiety. After a review of leading models of perseverative negative thinking, self-control, executive functioning, and depressive and anxious symptoms, the relevant associations were meta-analyzed as reported in cross-sectional and longitudinal studies. A total of 223 studies met the inclusion criteria, providing 239 independent samples (28 of which provided longitudinal data), N = 50,987. According to both longitudinal and cross-sectional path analyses, self-control deficits predict depression and anxiety symptoms, and these symptoms then predict perseverative negative thinking. In the present research synthesis, we identified evidence that reduced self-control predicts increases in depressive and anxious symptoms, which, in turn, lead to perseverative negative thinking. All in all, this finding suggests an opportunity to treat depression and anxiety through training of self-control and emotional-regulation strategies.
Even though thinking about negative aspects of the past and the future can help people learn from their experiences and prepare for the future, the role of these thoughts is complex. On the one hand, these thoughts may interfere with people’s ability to reach their goals and make them feel dejected because of that. On the other hand, these thoughts may be the result of not reaching important goals and cause feelings of depression or anxiety. So what comes first in the path to these distressing symptoms? What role do regulatory deficits and thinking patterns play in depressive and anxious symptoms? Attempting to answer these questions can help better understand the psychological processes implicated in symptoms of anxiety and depression and ultimately improve psychological interventions.
Past research has examined whether difficulties inhibiting one’s thoughts or actions (i.e., deficits in self-control and executive functioning; e.g., Joormann, 2006) are associated with ruminating about the past or worrying about the future (i.e., perseverative negative thinking): For example, difficulties regulating one’s thoughts may make it hard to disengage from negative thoughts such as “I am a failure.” However, no empirical research synthesis has considered how self-control or executive function and perseverative negative thinking operate in relation to symptoms of depression and anxiety. In this article, we endeavored to fill this gap by using meta-analytic techniques to examine the links among perseverative negative thinking, self-control and executive functioning, and symptoms of depression and anxiety. In doing so, we examined cross-sectional and longitudinal data from all relevant research.
Understanding the Interplay Between Perseverative Negative Thinking, Self-Control, and Depression and Anxiety Symptoms
Depression symptoms are uniquely characterized by low positive affect (e.g., behavioral withdrawal and anhedonia; Clark & Watson, 1991), whereas anxiety symptoms are distinguished by hyperarousal (e.g., heart racing and trouble relaxing; Sharp et al., 2015). Although depression and anxiety are distinct, they also overlap, having high comorbidity and related symptoms (Craske et al., 2009). Structural analyses have indicated that generalized anxiety disorder (GAD) and major depression correlate closely, and although many researchers distinguish them (Watson, 2009), the two conditions can be considered part of a category of distress disorders rather than separate entities (Clark & Watson, 2006). We believe that the same logic applies to combining anxiety and depression symptoms. 1
Perseverative negative thinking is found in both rumination about past events, occurring most prominently in depression (Nolen-Hoeksema et al., 2008), and worrying about future events, occurring most prominently in GAD (Borkovec et al., 1983). Rumination and worry differ in their temporal orientation and content (Davey et al., 1992; Hur et al., 2019) but are similar in that both are verbal in nature, are difficult to control, and focus negatively on the self (Ruscio et al., 2011). The relation between rumination and worry is complex, and the two can be considered as separate constructs. We consider them together here given their similarity as a form of perseverative thinking. 2
Our central question is how perseverative negative thinking and self-control or executive functioning are positioned in relation to anxiety and depression symptoms. Self-control is typically defined as a general capacity to regulate behavior by inhibiting behavioral, cognitive, or emotional impulses (Baumeister & Heatherton, 1996; Carver & Scheier, 2011; Tangney et al., 2004). Studies of self-control have traditionally used behavioral-choice tasks (e.g., choosing between healthy or unhealthy but delicious snacks; Baumeister et al., 1998) or questionnaires (e.g., the Brief Self-Control Scale; Tangney et al., 2004).
In conceptualizing executive functioning, we adopt the position of Zhou et al. (2012), who defined executive functioning as a domain-general resource for goal pursuit that involves the ability to control attention, cognition, emotion, and behavior. Studies of executive functioning have traditionally used cognitive-performance tasks (e.g., the Stroop task) assessing the momentary capacity for (a) inhibition or reactive control of thoughts, emotion, or behavior (Braver, 2012); (b) shifting or switching; (c) updating of working memory (Miyake et al., 2000); (d) sustained attention; and (e) affective disengagement (Ochsner & Gross, 2005), although inhibition is assumed to play a central role in all of these subprocesses (Miyake & Friedman, 2012). Defined in this way, self-control and executive functioning partially overlap because both describe the deployment of attentional resources in the service of goal pursuit (Beaver et al., 2007; Munakata et al., 2011).
Self-control and executive functioning have therefore both been defined as the capacity to override impulses, and both are assumed to rely on inhibition as their central component (Baumeister & Heatherton, 1996; Carver & Scheier, 2011; Miyake & Friedman, 2012; Saunders et al., 2018; Scherbaum et al., 2018). Because of the overlap between self-control and executive functioning as forms of impulse control, we include them both as traits related to inhibiting perseverative negative thinking. Various models have assumed that self-control relies on executive functions (Hofmann et al., 2009; Nigg, 2017; Robinson et al., 2010) or that it is itself an executive function (Beaver et al., 2007). However, self-control is a trait often linked to motivated, self-regulatory goals, whereas executive functioning comprises the capacity of the central executive to perform the task at hand (Hofmann, 2017). In addition, previous meta-analyses have found weak relationships between self-control and executive functioning (see Table S3 in the Supplemental Material available online), leading us to consider them as separate constructs.
Although depression and anxiety symptoms are linked to the common, transdiagnostic process of perseverative negative thinking (for meta-analytic reviews, see Aldao et al., 2010; Olatunji et al., 2010, 2013), their relations to self-control or executive functioning are far from obvious. For example, perseverative thinking has been thought of as a risk factor, clinical feature, and consequence of anxiety and depression. However, self-control has not been adequately studied in relation to perseverative negative thinking and depressive and anxious symptoms. Accordingly, in this article, we tested different models of the relations among depression and anxiety symptoms, self-control or executive functioning, and perseverative negative thinking. However, we do not consider these models to be mutually exclusive. The first model implies that rumination or worry decreases self-control or executive functioning, which, in turn, increases depression and anxiety symptoms. The second model assumes that decreases in self-control or executive functioning increase perseverative negative thinking, which, in turn, increases depression and anxiety symptoms. The third model implies that deficits in self-control or executive functioning increase symptoms of depression and anxiety, which then increase perseverative negative thinking. Finally, the fourth model implies that perseverative negative thinking increases symptoms of depression and anxiety, which ultimately decreases self-control or executive functioning.
Adjudicating between these four potential models is of essence for the development of theory, research, and practice. Although all the models consist of the same constructs, their distinct arrangements have important implications for the processes that maintain symptoms of depression and anxiety. If, for instance, the first model had the strongest support, researchers and practitioners could then focus on decreasing rumination or worry as a means for increasing self-control or executive functioning, which could ultimately reduce depressive and anxious symptoms. If the third model were most heavily supported, one could conclude that lower self-control or executive functioning triggers anxiety and depression symptoms and thus constitutes a risk factor for anxiety and depression. If two models with different directions were plausible (e.g., perseverative thinking predicting anxiety/depression in one model and anxiety/depression predicting perseverative thinking in another), a bidirectional relation is a definite possibility.
Potential pathways
The first model (Fig. 1a), which has never been assessed meta-analytically, links rumination or worry to decreases in self-control or executive functioning, which are then linked to increased depression and anxiety symptoms. This pathway describes how engaging in repeated negative thoughts may use up attentional resources needed to control depression and anxiety symptoms. As self-control or executive functioning is depleted, perseverative negative thinking ends up increasing the risk for depressive or anxious symptoms. Experiments manipulating rumination have shown negative impacts on self-control or executive functioning (Watkins & Brown, 2002), thus giving credence to Eysenck and Calvo’s (1992; see also Eysenck et al., 2007) processing-efficiency premise that worry exhausts cognitive resources otherwise available for executive functioning (Watkins & Brown, 2002). The notion also dovetails well with the strength model of self-control in which depletion in one area can have ripple effects in other areas (Baumeister et al., 2007; Muraven & Baumeister, 2000; for the limitations of this model, see Vohs et al., 2021).
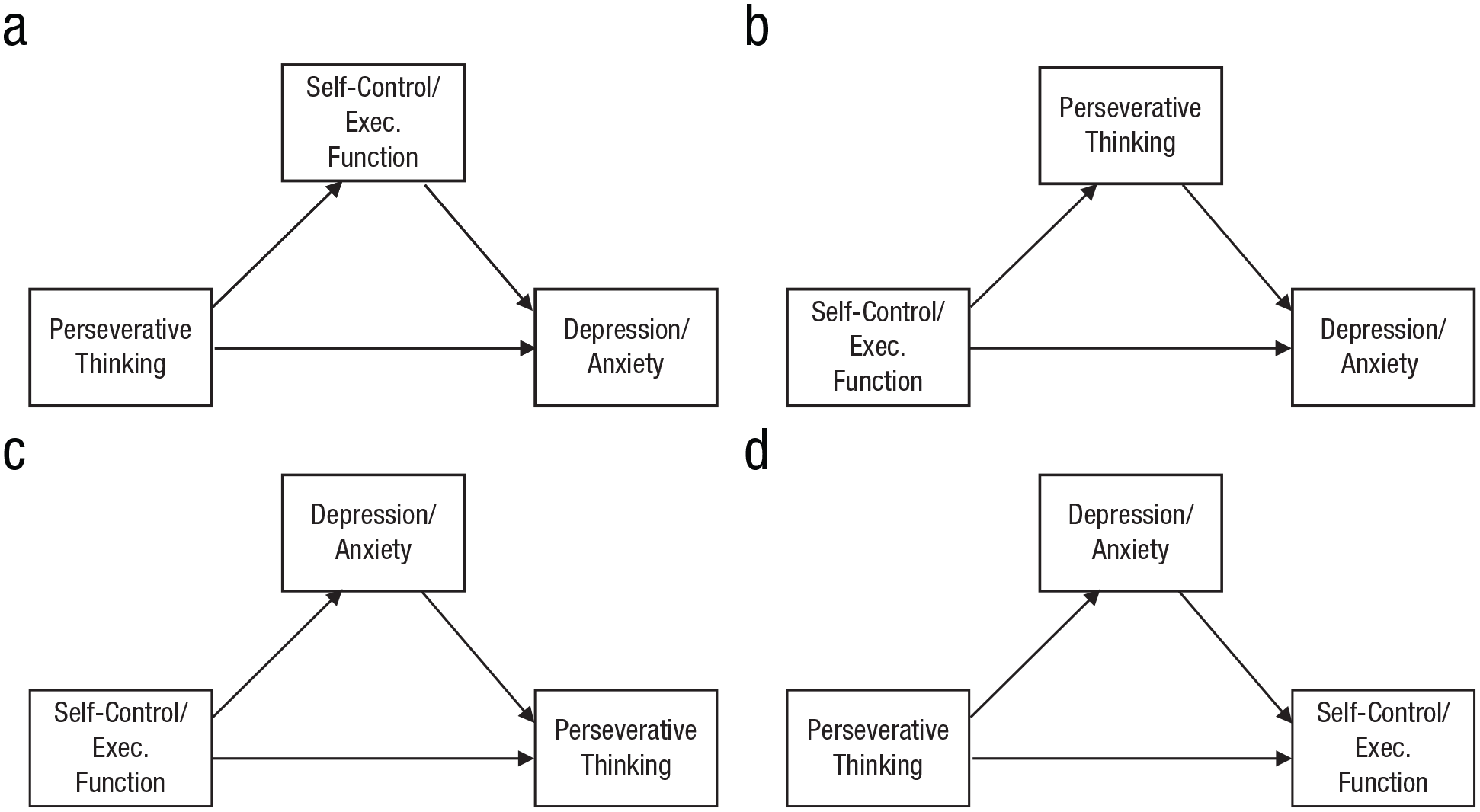
Mediation pathways of the four models tested. (a) Perseverative thinking leads to deficits in self-control/executive functioning, which increases depressive and anxious symptoms; (b) Self-control/executive functioning deficits increase persevrative thinking, which increases depressive and anxious symptoms; (c) Self-control/executive functioning deficits increase depressive and anxious symptoms, which increase perseverative thinking; (d) Perseverative thinking increases depressive and anxious symptoms, which undermine self-control/executive functioning.
The second half of the pathway in Figure 1a is supported by evidence that impaired attentional disengagement predicts depressive and anxious symptoms (Derryberry & Reed, 2002; Vălenaş et al., 2017). This process has been described by Rehm (1977) and Kuhl and Helle (1986), who pointed to the inability to disengage from irrelevant or unattainable goals as a cause of the development and maintenance of depression, and Hammen (2006; Snyder et al., 2019), who pointed to anxiety and depression increasing stressful life events that, in turn, maintain the symptoms. More concretely, past research has shown that multiple domains of executive functioning, including working-memory updating, inhibition, and shifting (Bora et al., 2013; McDermott & Ebmeier, 2009; Rock et al., 2014; Shi et al., 2019; Snyder, 2013), are impaired in depressed (vs. nondepressed) individuals.
The second model (Fig. 1b), which also has not been evaluated in any past meta-analysis, assumes that decreases in self-control or executive functioning increase perseverative negative thinking, which, in turn, heightens depression and anxiety symptoms. This sequence assumes that deficits in executive functioning make it difficult to disengage from negative thoughts, thereby increasing risk for depression or anxiety symptoms (Koster et al., 2011), often because of the inability to attain goals (see Martin & Tesser, 1996). This pathway is empirically consistent with associations between rumination and executive functioning (e.g., inability to inhibit unwanted material, Yang et al., 2016; shift away from negative thoughts, De Lissnyder et al., 2012; or manipulation of cognitive load, Joormann et al., 2011). However, past meta-analyses have yielded inconsistent relations between executive functioning and perseverative negative thinking. One found effects for shifting but not updating (Vălenaş & Szentágotai-Tătar, 2017), another found effects for inhibition but not updating (Yang et al., 2016), and yet another found effects only for updating (Zetsche et al., 2018).
The second half of this pathway, linking perseverative negative thinking to symptoms of anxiety and depression, has ample support in the literature. Rumination can lead to depression by increasing the salience of negative events, interfering with problem-solving, reducing self-efficacy, and exaggerating the severity of negative events (Bower, 1981; Lyubomirsky & Nolen-Hoeksema, 1995). Although this pathway has not been verified for anxiety, empirical studies have confirmed that self-control or executive functioning influences depression via changes in perseverative negative thinking (e.g., DeJong et al., 2019; Sanchez-Lopez et al., 2019). Critically, this pathway has yet to be analyzed meta-analytically, and we assessed it in relation to both depression and anxiety symptoms.
In addition to the models in Figures 1a and 1b, other relations among these variables are possible. For example, our third model (see Fig. 1c) assumes that impaired self-control or executive functioning gives rise to symptoms of depression and anxiety, which, in turn, produce worry or rumination. The few studies that examined preclinical levels of executive functioning have found that executive-functioning deficits predicted symptoms of depression and anxiety (as described in Fig. 1c) rather than the reverse (Allott et al., 2016; Ronold et al., 2020). Depression has been described as an evolutionary adaptation that triggers perseverative thinking to arrive at a solution of difficult challenges even if the pattern has maladaptive consequences (Hollon et al., 2021; see also Schwarz & Clore, 1988). Individually, a single successful episode of rumination may foster a habitual pattern of rumination each time negative feelings arise (Watkins & Nolen-Hoeksema, 2014).
A fourth possible pathway (see Fig. 1d), which to date has not been evaluated meta-analytically, considers how perseverative negative thinking spurs on depressive and anxious symptoms and how these symptoms, in turn, stifle self-control and executive functioning. Rehm’s (1977) theory of depression characterizes depressive symptoms as a deficiency across several domains of executive control. As previously mentioned, there is also evidence that impaired attentional disengagement predicts symptoms of depression and anxiety (Derryberry & Reed, 2002; Vălenaş et al., 2017). Regarding the second half of this pathway, quantitative and qualitative reviews have found that relative to healthy control subjects, depressed individuals demonstrate deficiencies in working memory, shifting, and inhibition (Hammar & Ardal, 2009; Snyder, 2013).
The present study
In this meta-analysis, we synthesized all relevant research to examine the pathways in Figure 1, the generalizability of these relations for the different operationalizations of self-control and executive functioning (e.g., questionnaires vs. tasks), and the effect of possible inclusion biases in the literature, surpassing prior reviews in several important ways. First, although past research syntheses have supported the existence of associations among self-control or executive functioning, perseverative negative thinking, and symptoms of depression and anxiety, most studies have focused on just two of these constructs without examining the full process, and none have looked at both the cross-sectional and longitudinal evidence. Second, and perhaps more important, our synthesis could shed light on contradictory results from previous bivariate meta-analyses linking rumination and executive functioning (e.g., Vălenaş & Szentágotai-Tătar, 2017; Yang et al., 2016; Zetsche et al., 2018). We also examined moderators, including variation in tasks, item overlap between questionnaires, and self-report bias, and corrected associations for lack of measurement reliability and publication bias. Our analysis more than doubled the number of studies of this issue synthesized so far (k = 239 andN = 50,987 vs. k < 109 and N < 7,000 in the largest prior syntheses), allowing for a more comprehensive examination of the literature that can reconcile prior conflicting results. Finally, we made all data publicly available to enable other researchers to test other models of interest.
Transparency and Openness
Details on how we determined our sample size, our inclusion and exclusion criteria, all measures used in the study, and analysis scripts are available on OSF (https://osf.io/vaedn/?view_only=f6006490adae475ca2f7dac50be4d336).
Method
Systematic search
We conducted a computerized search of APA PsycINFO, PubMed, and Web of Science on February 18, 2022. Our search terms consisted of keywords representing the following variables: self-control, executive functioning, perseverative negative thinking, and psychopathology. After duplicates were removed, the search yielded 3,993 reports, which were published between 1976 and 2022. To supplement these database searches, we sent requests to email lists of relevant professional societies seeking published or unpublished data sets and searched the citations of influential articles. These strategies, respectively, yielded six and 97 potentially eligible records.
Inclusion criteria and selection of studies
For the criteria we used to determine the inclusion and exclusion of reports from our analysis, see Figure S17 in the Supplemental Material. To ensure that our associations could be validly estimated within the same samples, reports were included if they allowed us to extract (a) the correlation between self-control or executive functioning and perseverative negative thinking and (b) the correlation between self-control or executive functioning and symptoms of depression or anxiety. Thus, they must contain at least one measure of self-control or executive functioning, one measure of perseverative negative thinking, and one measure of depression or anxiety. We excluded reports that used measures not in accordance with our definitions of the constructs, studies relying only on biological or neural measures of executive functioning, or studies in which measures were obtained only after an experimental induction. For a list of all measures that were contained in the final sample of studies, see Table S1 in the Supplemental Material; for descriptions and sample items of the most common measures, see Table S2 in the Supplemental Material. Reports were excluded if they did not provide quantifiable information or appropriate statistics to calculate the two target correlations. In cases in which a report did not include the necessary statistics, missing data were requested from authors via email. Based on these selection criteria, of the 3,993 reports initially considered for inclusion in this meta-analysis, 223 met our inclusion criteria, providing k = 239 statistically independent groups (for samples, Ns, and effect sizes, see Tables S4 and S5 in the Supplemental Material).
We assigned a quality rating to each study (M = 6.83, SD = 1.15) by coding the following characteristics: (a) reporting of exclusion criteria, (b) sensitivity analyses with excluded data, (c) a sample size equal to or greater than 60 people, (d) valid measurement of the dependent variable, (e) whether the study was longitudinal, (f) whether attrition was under 20% (for longitudinal studies), (g) a continuous independent variable, (h) a continuous dependent variable, (i) no conflict of interest, (j) preregistration, and (k) reported reliability of measures (see Table S5 in the Supplemental Material). We selected these characteristics based on recommendations from Drukker et al. (2021) for evaluating study quality in psychology. Each characteristic counted for 1 quality point.
Our target effect size was the Pearson correlation. To average correlations in data preparation and in the univariate analyses, we converted them to the Fisher’s Z scale for analysis and back-transformed them back to Pearson correlations for ease of interpretation in our report (Rosenthal, 1994). The structural equation models were conducted based on Pearson correlations.
Several approximations were made in calculating our effect-size statistic. First, conversion from a t or F value, where one variable was conceptualized as dichotomous, to a Pearson correlation, where both variables were conceptualized as continuous, assumes that the dichotomized variable has an underlying continuous distribution. Second, if a study incorporated more than one measure as an index of the constructs identified in our meta-analysis (e.g., two depression questionnaires), we assumed homogeneity and averaged the correlations (Borenstein et al., 2009). In addition, we examined these measures separately in supplementary analyses (see the Supplemental Material). Furthermore, we coded study characteristics related to the general study context, publication details, sample, measurement, and other specifications (see Table S4 in the Supplemental Material).
To assess interrater reliability, three independent pairs of coders were trained to code all study characteristics. Across the 21 continuous variables used in our analyses, we achieved an average interrater reliability of intraclass correlation coefficient = .97, whereas across the 23 categorical variables, we achieved an average interrater reliability of κ = .76, 90% agreement (based on k = 23 samples). In addition, each effect size in the final sample was obtained by two independent coders. Throughout the coding process, disagreements and questions were resolved by discussion and further examination of the studies.
Statistical analyses
Univariate meta-analyses were conducted using the metafor package (Viechtbauer, 2010). To test the indirect effect pathways, we used meta-analytic, two-stage structural equation modeling (Cheung, 2015). This multivariate technique accounts for shared variance among correlation coefficients that are assessed in the same samples and was therefore more appropriate than univariate meta-analysis. Data analysis was conducted in R using the metaSEM package (Cheung, 2015), and the effect sizes were weighted by the inverse of their asymptotic covariance matrix. The procedure consisted of two steps. In the first step, the correlation matrices of the individual studies were pooled together. Because of the large heterogeneity of methodology and sample and verification of significant random heterogeneities, we used a random-effects model. In the second stage, we used the pooled correlation matrix to fit and compare path models.
The disadvantage of fitting an indirect-effects model to our data is that the model is fully identified because three path coefficients are estimated from three correlations. This limitation makes it impossible to calculate goodness-of-fit indices and thereby compare the different hypothesized indirect-effect pathways. To address this limitation, we also ran sequential models in which the direct effect was removed. For example, we tested a model in which perseverative negative thinking predicted self-control and self-control predicted symptoms of depression or anxiety without a pathway from perseverative thinking to depression or anxiety symptoms. These sequential models yielded similar results but allowed us to inspect goodness-of-fit indices as well.
First, in the subsample of longitudinal data, we analyzed the association between any two variables (e.g., self-control at Time 1 and symptoms of depression and anxiety symptoms at Time 2) while controlling for baseline associations. Specifically, we calculated partial correlations that controlled for the baseline associations with the Time 2 variable (e.g., controlling for the association of Time 1 self-control or executive functioning with Time 1 depression and anxiety symptoms and the autocorrelation of Time 1 and Time 2 depression and anxiety symptoms). Next, to evaluate the models using the longitudinal partial correlations, we conducted multivariate, meta-analytic structural equation modeling as described above. To check those models in a larger sample, we then tested the same models in the full sample of cross-sectional data. Finally, we examined a variety of moderators with the cross-sectional data, which had greater statistical power.
Results
Characteristics of the included studies
A total of k = 239 independent samples across 223 reports (N = 50,987) were included in the cross-sectional analysis, and k = 28 independent samples (N = 4,168) were included in the longitudinal analysis (see Table 1). Dates of publication ranged from 2002 to 2022; most reports were published in the last 5 years on the basis of studies conducted in the United States, Canada, and the UK (57%) or other European countries (29%). Of the samples in our analyses, 31% stated that they included clinically diagnosed (14% of all participants) adults between 18 and 65 years years old (89%; weighted age across all studies: M = 29.50 years, SD = 15.91, total range = 7–97), with a preponderance of women (across all participants: M = 66%, SD = 48%). We define “clinically diagnosed” as having a current diagnosis resulting from a diagnostic interview. Samples frequently included more than 100 participants (50%), and the majority included participants with a college degree or currently enrolled in college (91% of studies for which these data were available, 76% of the participants). Race and ethnicity data were mostly unreported, but the available data indicated that most participants were White.
Partial Correlations From Longitudinal Studies
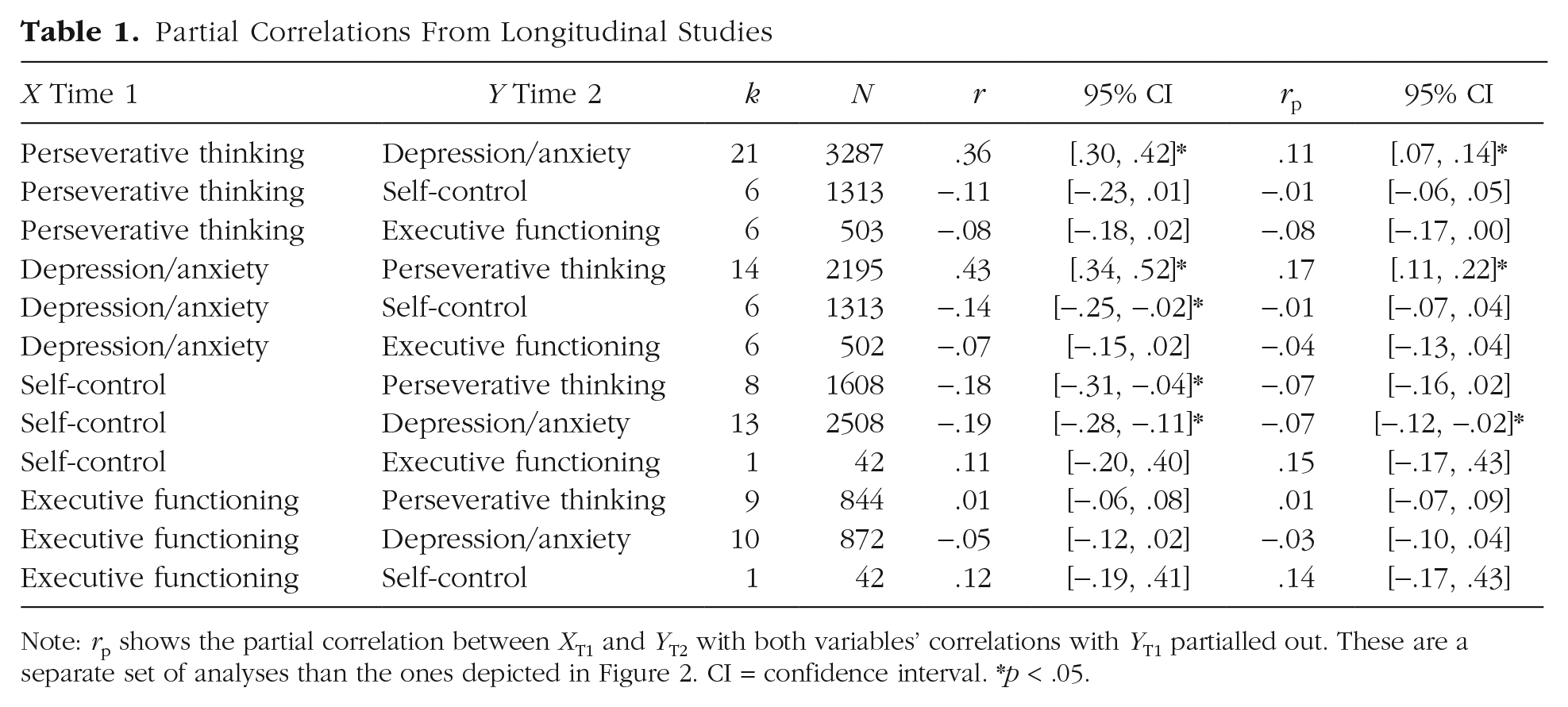
Note: rp shows the partial correlation between XT1 and YT2 with both variables’ correlations with YT1 partialled out. These are a separate set of analyses than the ones depicted in Figure 2. CI = confidence interval. *p < .05.
Longitudinal associations
Univariate partial correlations
We first calculated partial correlations controlling for the baseline values of the variables. For example, when correlating Time 1 self-control with Time 2 depression symptoms, we controlled for both the baseline correlation of Time 1 self-control and Time 1 depression symptoms and for the Time 1–Time 2 autocorrelation of depression symptoms over time (Table 1). The partial longitudinal effects of executive functioning with either depression or anxiety symptoms or perseverative negative thinking were almost nonexistent, |rps| = .01–.08 (all ns). In the following section, we therefore focus on only associations with self-control.
Perseverative negative thinking was prospectively related to increased depression and anxiety symptoms, rp = .11, but depression and anxiety symptoms were also prospectively related to perseverative negative thinking, rp = .17. Although these associations imply a bidirectional relation, the prospective effect of depression and anxiety on perseverative negative thinking was significantly stronger than the effect of perseverative negative thinking on depression and anxiety symptoms, z = 2.14, p = .03. The other prospective partial correlation that reached significance was an effect of self-control on symptoms of depression and anxiety, rp = −.07. These partial correlations thus supported a model in which deficits in self-control predict increased symptoms of depression and anxiety and these symptoms then predict increased rumination and worry.
Structural equation modeling
In addition to obtaining partial correlations, we formally tested our different predictions using meta-analytic structural equation modeling. We used Time 1 data for the predictor and Time 2 data for the mediator and the outcome (Fig. 2; for associations between Time 1 mediator and Time 2 outcome, see partial correlations in Table 1). Results indicated support for the model in which impaired self-control is prospectively associated with perseverative negative thinking and thereby with depression or anxiety (Fig. 2b1) and the model in which impaired self-control is prospectively associated with depression and anxiety and thereby with perseverative negative thinking (Fig. 2c1). In contrast, the models with executive functioning (see Figs. 2a2, 2b2, 2c2, and 2d2) had inadequate fit, as did the models in which perseverative negative thinking reduces either self-control or depressive and anxious symptoms (Figs. 2a1 and 2d1).
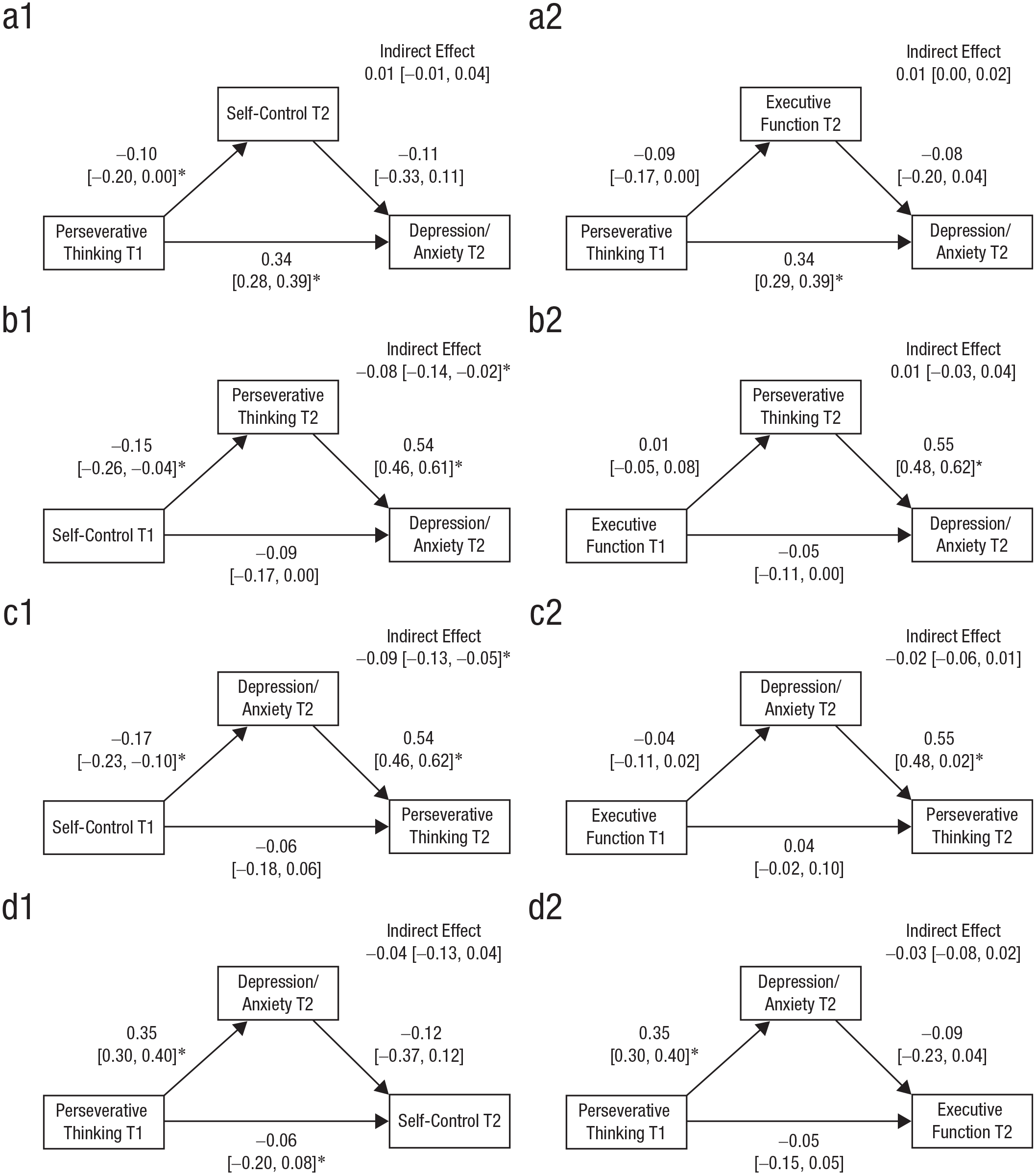
Longitudinal mediation pathways for the indirect pathways. (a1) Perseverative thinking at T1 predicting depression/anxiety at T2 via self-control at T2. (a2) Perseverative thinking at T1 predicting depression/anxiety at T2 via executive function at T2. (b1) Self-control at T1 predicting depression/anxiety at T2 via perseverative thinking at T2. (b2) Executive function at T1 predicting depression/anxiety at T2 via perseverative thinking at T2. (c1) Self-control at T1 predicting perseverative thinking at T2 via depression/anxiety at T2. (c2) Executive function at T1 predicting perseverative thinking at T2 via depression/anxiety at T2. (d1) Perseverative thinking at T1 predicting self-control at T2 via depression/anxiety at T2. (d2) Perseverative thinking at T1 predicting executive function at T2 via depression/anxiety at T2. Values represent standardized path coefficients; 95% likelihood-based confidence intervals are in brackets. The models are based on k = 20 to 25 studies and N = 2,485 to 3,942 participants. *p < .05.
Cross-sectional associations
The longitudinal subsample allowed us to obtain insights of high methodological quality but without high statistical power to conduct meaningful moderation analyses because splitting the data by a moderator would have resulted in too few studies being meta-analyzed. To address this shortcoming, we extended the previous analyses using the cross-sectional database, which contains the largest number of studies ever synthesized in this domain (k = 238 studies). For the simple correlations between all the constructs, all of which had high heterogeneity, see Table S12 in the Supplemental Material. As in the longitudinal analyses, perseverative negative thinking and symptoms of depression or anxiety were strongly associated, r = .51. In addition, self-control was associated with perseverative negative thinking (r = −.21) and symptoms of depression or anxiety (r = −.26), as was executive functioning, albeit more weakly (rs = −.07 in both cases). Supporting the aforementioned differences between self-control and executive functioning, we found that their intercorrelation was very small, r = .06.
Next, we compared the four mediation pathways in Figure 1. Like in the longitudinal analyses, we found support for the model in which self-control predicts more perseverative negative thinking and, finally, symptoms of depression or anxiety (see Fig. 3b1). Both the indirect and direct effects of self-control on symptoms of depression and anxiety were significant, and 37% of the total effect of self-control on depression and anxiety symptoms was mediated by perseverative negative thinking. Examining these pathways in purely sequential models suggested that the data fit the model in Figure 3b1 well (root mean square errors of approximation ≤ .04, standardized root mean square residuals ≤ .08, Tucker-Lewis indexes ≥ .91, supporting a link from self-control to perseverative negative thinking to symptoms of depression or anxiety (see Table S14 in the Supplemental Material). The comparable models using executive functioning instead of self-control showed similar results, albeit coefficients were much smaller in size (Fig. 3b2).
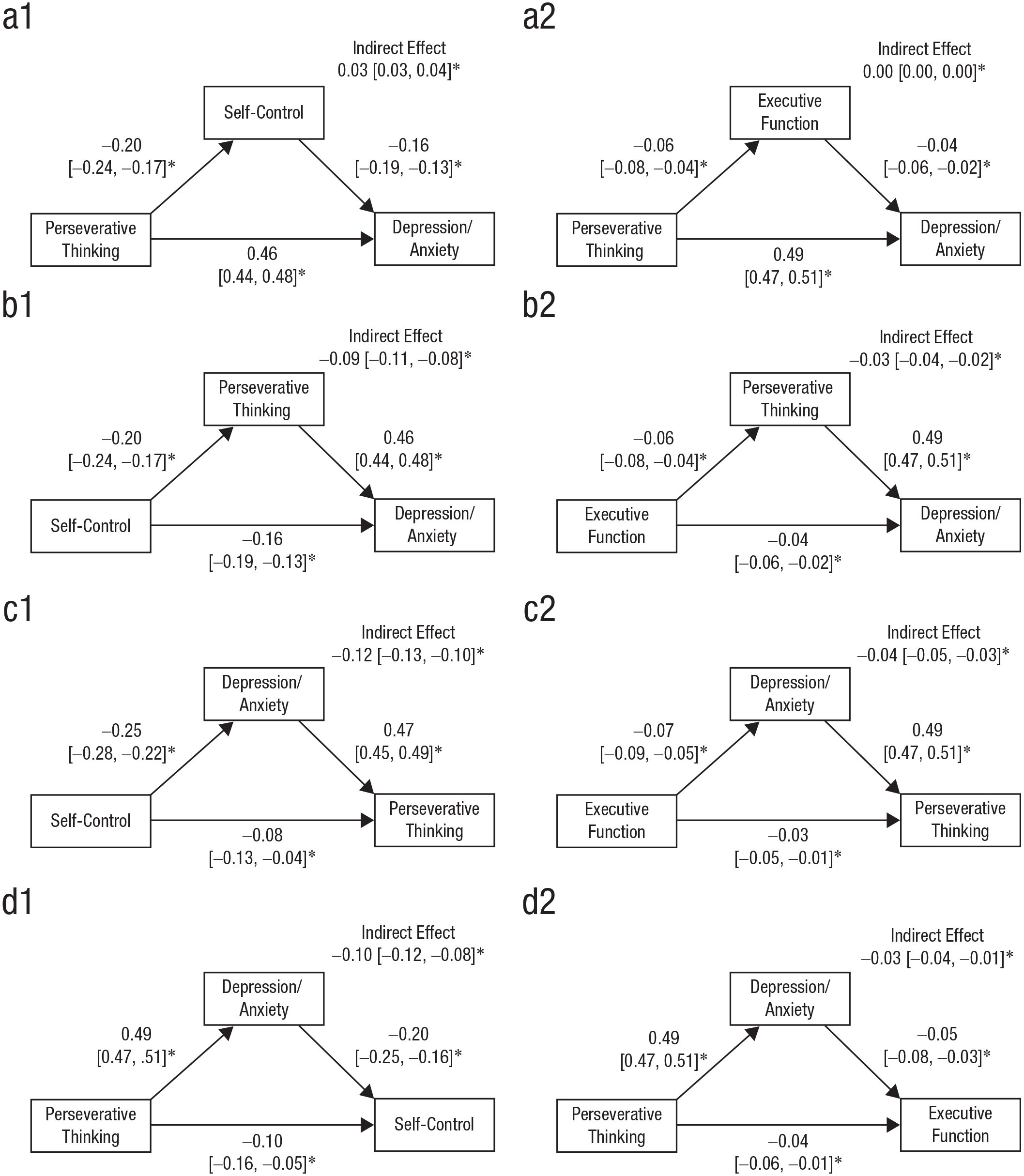
Cross-sectional mediation pathways for self-control (a1, b1, c1, d1; N = 48,572, k = 224), executive functioning (a2, b2, c2, d2; N = 48,532, k = 232), perseverative negative thinking, and symptoms of depression and anxiety. (a1) Perseverative thinking predicting depression/anxiety via self-control. (a2) Perseverative thinking predicting depression/anxiety via executive function. (b1) Self-control predicting depression/anxiety via perseverative thinking. (b2) Executive function predicting depression/anxiety via perseverative thinking. (c1) Self-control predicting perseverative thinking via depression/anxiety. (c2) Executive function predicting perseverative thinking via depression/anxiety. (d1) Perseverative thinking predicting self-control via depression/anxiety. (d2) Perseverative thinking predicting executive function via depression/anxiety. Values represent standardized path coefficients; 95% likelihood-based confidence intervals are in brackets. EF = executive functioning. *p < .05.
As with the longitudinal models, the cross-sectional ones also revealed support for the model in which self-control influences symptoms of depression and anxiety, which, in turn, influence perseverative negative thinking (see Fig. 3c1). About 57% of the total association between self-control and perseverative thinking was actually explained by symptoms of depression or anxiety. Results were similar when using executive functioning instead of self-control, although the coefficients were smaller (Fig. 3c2).
Moderators
One of the most striking findings of both our longitudinal and our cross-sectional analyses was that the models that were supported for self-control were either weakly or not at all supported for executive functioning. We thus examined whether characteristics of the executive-functioning tasks themselves, characteristics of self-report questionnaires, and characteristics of the samples could account for the differences across measures of self-control and executive functioning. For these analyses, see Tables S6 to S9 in the Supplemental Material. The moderator analyses showed that out of various possible executive-functioning tasks, the negative-affective-priming task had higher correlations with depression than the others, r = −.15 (vs. r = −.07 overall).
Alternatively, the discrepancy between self-control and executive functioning could stem from the content of self-control questionnaires overlapping with the content of rumination or worry questionnaires rather than a substantive association. We examined this issue by conducting separate analyses for different self-control measures and found that measures of emotional regulation (r = −.12) were less strongly correlated with rumination than measures of cognitive regulation (r = −.30; see Table S7 in the Supplemental Material). If not item overlap, self-report bias may selectively inflate associations with self-control questionnaires. We examined 18 articles containing observer ratings of depression or anxiety symptoms and self-report measures and found little evidence of self-report bias. There were no statistically significant differences of correlations of observer-reported versus self-reported symptoms of depression and anxiety with negative perseverative thinking or with executive-functioning tasks (see Table S13 in the Supplemental Material). We thus concluded that the small associations we found with executive functioning are unlikely to be driven by specifics of the measures.
More generally, our results may be explained by characteristics of the samples in the studies, such as clinical diagnosis (or lack thereof), gender composition, and publication status. Our moderation analyses showed that average sample age affected associations (see Table S9 in the Supplemental Material) but still did not account for the lower correlations with executive functioning (r = −.06 at age 20 to r = −.13 at age 60). We found that clinical status significantly weakens the relationship between self-control and depression/anxiety relative to nonclinical or mixed samples. We also found some effect of the gap between Time 1 and Time 2 for longitudinal studies, although these did not meaningfully change the results (see Table S9 in the Supplemental Material). Quality rating also significantly moderated the relationship between perseverative negative thinking and symptoms of depression and anxiety, suggesting that higher quality studies show a weaker relationship between these two variables (see Table S9 in the Supplemental Material). We also considered potential measurement unreliability in the tasks. Table S10 in the Supplemental Material shows how measurement error reduced effect sizes, exemplified by correlations among color-word Stroop scores, rumination, and depression when correcting for different reliability estimates. However, even after correcting for imperfect measurement, correlations with executive functioning remained small.
Finally, we assessed whether publication bias contributed to our results. We examined funnel plots, conducted trim-and-fill analyses, calculated a random-effects version of Egger’s regression test (Egger et al., 1997), and tested whether results from published articles were systematically larger than those from unpublished articles. These tests showed no difference in significance for any of our associations of interest (see Table S11 in the Supplemental Material). In sum, neither characteristics of the tasks, questionnaires, and samples nor issues of measurement quality or publication bias could account for why associations with executive functioning were so much smaller than expected, and these associations remained small (≤ −.15) even after adjusting for moderators.
Discussion
The overarching goal of this meta-analysis was to synthesize research on the direct and indirect effects of self-control, executive functioning, and perseverative negative thinking on symptoms of depression or anxiety. Specifically, in this meta-analysis, we attempted to answer the following question: Which of the models in Figure 1 are supported by longitudinal and cross-sectional data, and do these models work the same for self-control and executive functioning? We found that three models were moderately supported (Models B–D) and that one was not supported (Model A). The supported models include the one in which self-control deficits predict first symptoms of depression and anxiety and then perseverative negative thinking (Model C), the one in which self-control deficits predict first perseverative negative thinking and then symptoms of depression and anxiety (Model B), and the one in which perseverative negative thinking predicts first symptoms of depression and anxiety and then self-control deficits (Model D). Taken together, these results suggest a possible bidirectional relation between symptoms of depression and anxiety and perseverative negative thinking. The unsupported model was the one in which perseverative negative thinking first predicts self-control or executive-functioning deficits and then symptoms of depression and anxiety. Furthermore, we found that the three supported models, Models B through D, were supported for self-control but not for executive functioning. This discrepancy between self-control and executive functioning remained even after accounting for various moderators, and the associations between executive functioning and depression and anxiety symptoms remained very small throughout. The overall findings from this meta-analysis, which is the most comprehensive conducted on this topic, are summarized in Table 2. Table 2 also lists the limitations of the evidence so far, which should guide future research.
Summary of Findings
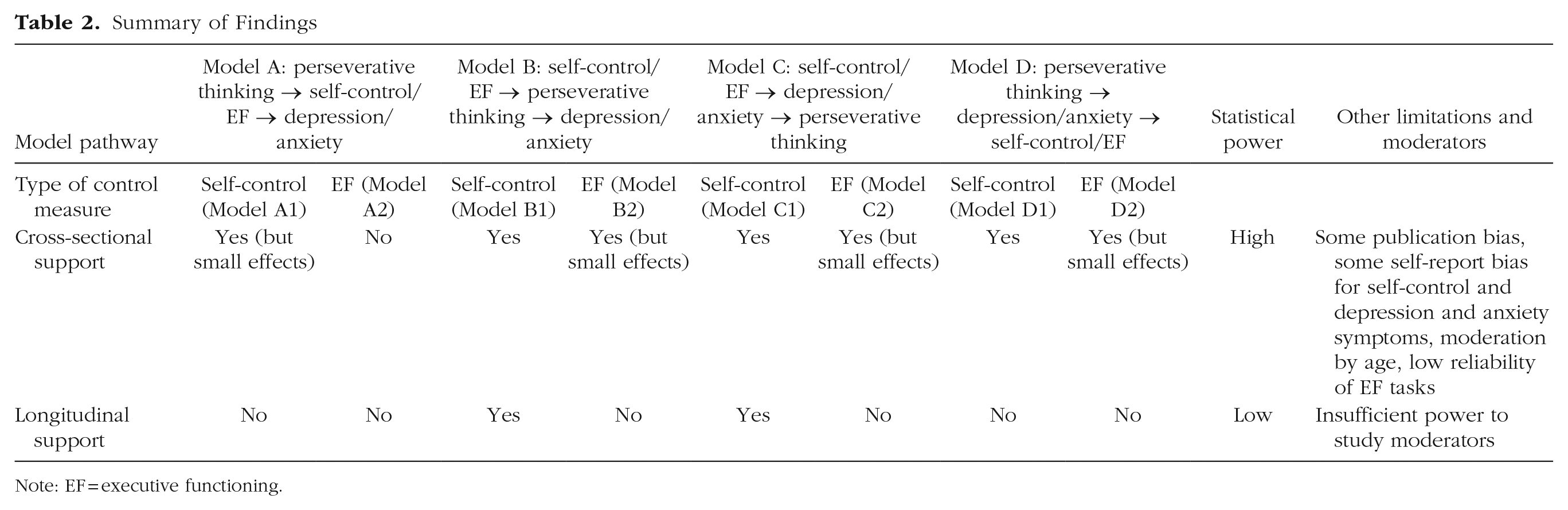
Note: EF = executive functioning.
Some previous bivariate meta-analyses have found stronger associations of executive functioning with rumination, depression, or anxiety compared with our synthesis. Considering the correlation between depression symptoms and executive functioning, three meta-analyses that compared people with diagnosed major depressive disorder and nonclinical control subjects found estimates between r = −.21 and r = −.28 (Bora et al., 2013; Rock et al., 2014; Snyder, 2013), and one very small meta-analysis of studies with patients with major depressive disorder found r = −.32 (McDermott & Ebmeier, 2009). Crucially, however, these studies all examined groups at the extreme ends of the psychopathology spectrum rather than using the full variation along this spectrum. The same applies to a meta-analysis comparing participants with diagnosed obsessive compulsive disorder with nonclinical control subjects, rs = −.18 to −.33 (Snyder, Kaiser, et al., 2015). In contrast, two meta-analyses that used correlations across the whole spectrum found markedly smaller effects, including our own, r = −.07 for both depression and anxiety, and Zetsche et al.’s (2018) meta-analysis, which found only r = −.03 for depression and r = −.04 for anxiety. A potential outlier to this pattern is a meta-analysis that used both extreme-group comparisons and full-spectrum correlations, r = −.19 for anxiety (Shi et al., 2019). Even though our own results showed no difference between samples with more versus fewer formally diagnosed participants, we observe a large difference between prior meta-analyses relying only on samples of formally diagnosed participants and those relying on mixed samples.
It is possible that the small impairments in executive functioning, which are typical in predominantly healthy or subsyndromal samples, are too small to have strong effects on mental health but that they begin to disproportionately affect mental health once they become noticeable enough to cause problems in daily life. For instance, we found a moderation by age such that executive-functioning difficulties are increasingly related to the risk of perseverative negative thinking later in the life span. This possibility would be in accordance with stress-generation theory (Hammen, 2006; Snyder et al., 2019), which proposes that executive-functioning impairments influence depression or anxiety because they increase stress for the individual, an effect that strengthens over time. This possibility would also dovetail with findings that many executive-functioning tasks are subject to ceiling effects (Snyder, Miyake, & Hankin, 2015) because they were initially developed to detect severe neuropsychological issues (e.g., dementia) and lack sensitivity in less severely affected populations. Nevertheless, we once again point out that 27% of our samples and 14% of all participants in our sample were also clinically diagnosed (typically with major depressive disorder), and yet those groups did not yield any stronger results than nonclinical samples.
It is also possible that publication bias increased the estimates of previous meta-analyses. Our study included a comparatively large proportion of unpublished data (9% of articles) and data from articles not focused on the issues at hand. Even based on this broad sample of reports, we found evidence that null results were underreported. In particular, the association between executive functioning and symptoms of depression or anxiety disappeared entirely after correcting for publication bias using the trim-and-fill procedure. Other associations, however, were robust.
Limitations
Our meta-analysis was limited by the availability of data from the literature. Our highest powered analyses relied on cross-sectional data, and our longitudinal analyses could examine only two time points, so future studies with more complex designs are needed. Furthermore, our results are limited by the correlational nature of the literature. Indirect-effect models are best suited for causal associations, and ascriptions of causality require covariation, temporal precedence, and exclusion of alternative explanations (e.g., Shadish et al., 2002). Correlational analyses cannot prove causality, particularly for trait-level data and in a domain in which associations arise naturally rather than from experimental manipulations or other external shocks. We were also limited by incomplete demographic information in much of our sample data, particularly for race and ethnicity. The existing data, however, served to establish (a) covariation between the variables, based on cross-sectional analyses with larger samples than any previous reviews had examined; (b) temporal precedence between the variables, based on longitudinal analyses with a much smaller sample; and (c) exclusion of several alternative explanations, based on moderator analyses and robustness checks, focusing especially on how self-control and executive functioning were operationalized.
Clinical implications
Traditionally, rumination has been implicated in the development and maintenance of depression (Nolen-Hoeksema et al., 2008), whereas worry has been implicated in the development and maintenance of anxiety (Borkovec et al., 1983). Accordingly, we found that the relations between disorder-specific types of perseverative negative thinking and their associated symptoms (rumination and depression; worry and anxiety) were strong. However, the associations between worry and depression and between rumination and anxiety were almost equally strong, supporting the idea of perseverative negative thinking as a transdiagnostic process with a common core (Harvey, 2004; Hur et al., 2019).
Overall, our results provide evidence of etiological factors that may inform psychological interventions designed to treat depression and anxiety. In addition to our findings from cross-sectional and longitudinal correlational data, experimental work has supported directional effects of self-control and executive functioning on perseverative negative thinking and symptoms of depression and anxiety. For example, Bomyea and Amir (2011) found that training undergraduates on an inhibitory-control task led to fewer intrusions in a postintervention thought-suppression task. Other reviews have found that cognitive-control training (Koster et al., 2017) or attention-bias training (Hakamata et al., 2010) sometimes reduces depression and anxiety symptoms, which is consistent with our longitudinal finding that self-control prospectively predicts depression and anxiety symptoms.
Our results, however, suggest that broad traits as measured by self-control questionnaires are a more promising predictor of changes in depression or anxiety symptoms than highly specific executive-functioning tasks. Furthermore, it is possible that cognitive remediation treatment may be helpful in severe, treatment-resistant cases of depression and anxiety, in which cognitive impairments may be sufficiently intense to interfere with treatment efficacy (for a review, see Porter et al., 2013; although, see Elgamal et al., 2007, for null results, and Diamond & Ling, 2016, for a critique). Nevertheless, further research should identify the strengths of such effects and the mechanisms through which such improvement might occur. Our results from the model in which impaired control predicts first perseverative thinking and then predicts depression or anxiety symptoms suggest that a reduction in perseverative negative thinking is a likely candidate for one of these mechanisms.
The generalizability of our findings to different cultural groups and high-risk groups must also be examined given that our results are based largely on U.S. and West European student samples without clinical levels of depression or anxiety. We encourage future researchers to include information on race and ethnicity in their studies to enable meta-analytic testing of group differences. Future studies should also investigate under which conditions executive-functioning training does and does not transfer to improvements in well-being to evaluate the potential for treatment options. Averaged across studies, our review does not suggest a uniformly high potential for task-based training. In contrast, interventions that are broader in scope and train metastrategies to deal with life challenges instead of focusing on one or two specific computerized tasks may hold more promise, based on our finding that broader questionnaire measures of self-control were more strongly correlated with symptoms in all analyses.
Conclusion
This meta-analysis contributes to the literature by clarifying the nature of the associations between self-control, executive functioning, perseverative negative thinking, and symptoms of depression and anxiety using both longitudinal and cross-sectional data. Through the first longitudinal meta-analysis and the most extensive cross-sectional meta-analysis of this literature, we found cross-sectional evidence that decreases in self-control are associated with increased perseverative thinking and therefore depression and anxiety symptoms, and decreases in self-control are associated with increased depression and anxiety symptoms and therefore increased perseverative thinking. Furthermore, we found some evidence that perseverative negative thinking causes symptoms of depression and anxiety, thereby causing deficits in self-control.
Furthermore, measures of self-control and of executive functioning showed limited convergent validity and very different patterns of associations. Whereas self-control deficits were associated with moderately higher rumination, worry, depression, and anxiety symptoms, executive functioning had only small associations with these experiences. We therefore conclude that self-control questionnaires and executive-functioning tasks probably assess fundamentally different processes. We hope that the next decade will bring clarity to how affective experiences and affective disorders color people’s thinking about the world (Bless & Fiedler, 2006; Forgas, 1995; Schwarz & Clore, 1988). This possibility aligns well with the current research on the regulation of emotion rather than the regulation of thought (Cisler et al., 2010; Farb et al., 2012; Gotlib & Joormann, 2010) and is a promising avenue toward ameliorating depression and anxiety.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026251344172 – Supplemental material for Perseverative Negative Thinking, Self-Control, and Executive Functioning in Symptoms of Depression and Anxiety: A Comprehensive Meta-Analysis of Competing Models
Supplemental material, sj-docx-1-cpx-10.1177_21677026251344172 for Perseverative Negative Thinking, Self-Control, and Executive Functioning in Symptoms of Depression and Anxiety: A Comprehensive Meta-Analysis of Competing Models by Janet M. Lopez, Sophie Lohmann, Yara Mekawi, Colleen Hughes, Aashna Sunderrajan, Chinmayi Tengshe, Aishwarya Rajesh and Dolores Albarracín in Clinical Psychological Science
Footnotes
Acknowledgements
We are grateful to Dianne L. Chambless for her comments on the coding scheme and the manuscript. Prior versions of these analyses were presented at the 89th meeting of the Midwestern Psychological Association, the 28th meeting of the Association for Psychological Science, and the 17th meeting of the Society for Personality and Social Psychology.
Transparency
Action Editor: DeMond M. Grant
Editor: Jennifer L. Tackatt
Author Contributions
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.