
Abstract
The well-documented between-individuals correlation between anxiety and depression cannot address within-individuals questions, such as whether targeting depression subsequently alleviates anxiety comorbidity. Recent studies have demonstrated the importance of focusing on within-individuals processes to provide evidence-based guidelines to commonly encountered questions in clinical practice. This study examined the within-patient effect of reduction in depression on subsequent reduction in anxiety during a treatment targeting depression, as well as the potential variability in this effect between patients. Data from a randomized controlled trial of more than 3,220 observations nested within 100 patients treated for depression were used. Findings indicate that at the sample level, targeting depression reduced depression, which, in turn, predicted a subsequent reduction in anxiety. Although no qualitatively distinct subgroups emerged, quantitative differences between individuals were found. The pretreatment interplay between depression and anxiety explains heterogeneity between individuals. The findings have implications for personalizing depression treatment to address comorbidities.
To personalize treatment effectively, it is essential to transform comorbidity from a source of noise into a valuable factor that guides treatment personalization. The most common comorbidity is the co-occurrence of depressive and anxiety disorders (Kaufman & Charney, 2000; Kroenke et al., 2007); studies have indicated that comorbidity rates may be as high as 75% to 81% (Lamers et al., 2011). Understanding this comorbidity can help determine whether treating depression can lead to reductions not only in depression but also in anxiety, a critical question in clinical practice. This question concerns within-individuals processes, which cannot be adequately addressed by examining between-individuals comorbidity (Fisher et al., 2017; Zilcha-Mano, 2021). Between-individuals effects assess the overall efficacy of treatment across individuals, determining whether a treatment targeting depression also reduces anxiety across a group. However, this approach does not capture the specific processes driving change within each individual. By contrast, within-individuals effects examine the temporal relationship between depression and anxiety reductions within an individual, helping to determine if treating depression may lead to subsequent anxiety reduction. Without within-patients analysis, one cannot establish whether changes in anxiety are directly related to changes in depression or if they occur independently. Disentangling these effects is crucial for tailoring personalized treatment strategies in clinical practice. The limited research available on the within-individuals associations between anxiety and depression during treatment for depression suggests potential between-individuals variability (Cusack et al., 2024; Wright et al., 2014). The present study investigated whether reductions in depression predict subsequent reductions in anxiety at the within-individuals level (Aim 1) and explored potential between-individuals variabilities in this effect (Aim 2) to inform personalization approaches.
Because treatments are effective for only about 50% of individuals (Cuijpers et al., 2024), there has been a growing interest in personalized-treatment approaches (Cohen et al., 2021). Such approaches can be especially effective when they transform the complexity of individual differences from noise into valuable information, making it possible to identify the most effective interventions for each individual. An important source of complexity in mental-health diagnosis is high comorbidity, especially between anxiety and depression. A global survey (Kessler et al., 2015) found that 45.7% of individuals with lifetime major depressive disorder (MDD) also had a history of one or more anxiety disorders. In addition, 41.6% of individuals with 12-month major depression had an anxiety disorder in the same period (Kessler et al., 2015). Likewise, studies have indicated that 53% of patients with major depression experience significant anxiety (Fava et al., 2004) and that patients participating in clinical trials for anxiety disorders exhibit mild to moderate depression (Cuijpers et al., 2016). Findings further suggest that depression and anxiety share common neural alterations that are related to aberrant emotion processing, as manifested in alterations in the salience, reward, and lateral orbital nonreward networks (McTeague et al., 2020), and that individuals with comorbid depression and anxiety have a unique signature of neural alterations (Zilcha-Mano et al., 2020). The high comorbidity between depression and anxiety results in a more adverse course of psychopathology (Lamers et al., 2011), worse prognosis, and less effective treatments (Dold et al., 2017; Ter Meulen et al., 2021).
A critical question in the research on treatment for MDD is whether treating depression may not only reduce depression but, subsequently, also alleviate anxiety. This question concerns within-individuals processes taking place between depression and anxiety and cannot be answered based on research focusing on between-individuals differences. Accumulating studies suggest that it is not possible to infer from between-individuals effects to within-individuals effects (Hamaker, 2023). That is, the findings that individuals with MDD are also likely to suffer from anxiety do not imply that treating depression will result in a subsequent reduction of anxiety as well.
The vast majority of studies examining the association between depression and anxiety have been conducted at the between-individuals level, meaning they cannot explain within-individuals processes. These studies provide valuable insights for clinical guidelines. For example, meta-analyses comparing the effects of treatments targeting anxiety disorders with those targeting depression suggest that treatments for anxiety disorders have a moderate to large effect on depressive symptoms. However, treatments targeting depression generally show larger effects in reducing depression, particularly within-groups effect sizes (Cuijpers et al., 2016). Likewise, treatments for depression may result in reductions not only in depressive symptoms but also in anxiety (Stein et al., 2021). Yet between-patients analyses leave open the question of which within-patients process underlies the between-patients findings that targeting one symptom is associated with reducing another—specifically, whether targeting depression facilitates a within-individuals process in which reductions in depression lead to subsequent reductions in anxiety. Recently, there has been growing interest in understanding the within-individuals association between depression and anxiety (Wright & Woods, 2020). Emerging evidence suggests that individuals with depression often experience co-occurring anxiety (Cusack et al., 2024), especially during certain stages of treatment (Wright et al., 2014). However, it remains unclear whether reducing depression through targeted treatment predicts a subsequent decrease in anxiety. The first aim of the present study was to address this question. At the sample level, it is hypothesized that effective treatment reducing depression will also result in subsequent reductions in anxiety.
Another open question in the literature concerns the potential variability in the within-individuals association between depression and anxiety (Cusack et al., 2024). Potential individual differences in the within-individuals association between depression and anxiety, as identified based on data-analytic approaches, may indicate qualitatively distinct subpopulations of patients or quantitative individual variation within a continuous spectrum. Qualitative differences may manifest in distinct subgroups of individuals showing certain patterns of association, whereas quantitative ones may refer to different magnitudes of association. Regarding qualitative differences between individuals, it is unknown whether distinct subgroups of individuals show distinct patterns of association. Although some studies have suggested that the within-individuals association between depression and anxiety is positive (Wright et al., 2014), there have been sporadic indications that for different individuals, the effect may even move in opposite directions. For example, in a case study, Fisher and Boswell (2016) identified an individual with a mixed diagnosis of anxiety and depression displaying a negative within-individuals association between depression and anxiety. It is unclear whether these sporadic indications represent a distinct and meaningful subgroup within the population of patients with comorbidities. Aim 2a of the present study was to use a data-analytic approach to explore potential qualitative differences between individuals.
Regarding quantitative differences between individuals, the question is whether there are individual differences between patients in the magnitudes of the within-individuals association, that is, whether individuals differ in the extent to which a reduction in depression is associated with a reduction in anxiety. If quantitative differences are found, identifying their source can be instrumental in personalizing treatment. One such source of potential variability is the pretreatment interplay between anxiety and depression. Although in psychotherapy research patients’ pretreatment condition is commonly evaluated as a snapshot, psychopathology research documents dynamic patterns of mental health (Zilcha-Mano, 2024). Findings suggest that emotions (Jacobson et al., 2023), including depression (Fisher et al., 2017; Fried, 2017; van Eeden et al., 2019), vary within persons over time. Aim 2b of the present study was to explore quantitative differences between individuals by testing the potential moderating effect of the pretreatment interplay between anxiety and depression on the effect of changes in depression on subsequent changes in anxiety.
The overarching goal of the present study was to examine the within-patient effect of changes in depression on subsequent changes in anxiety during the treatment of depression, as well as the potential variability in this association between patients. The study had two main aims: Aim 1 was to examine the within-patient effect of changes in depression on subsequent changes in anxiety in a treatment targeting depression, and Aim 2 was to use data-analytic approaches to explore potential qualitative and quantitative differences in this association between patients. Specifically, the study aimed to (a) identify any qualitative variability between patients to determine whether more than one distinct subgroup characterizes the sample, and (b) assess the quantitative variability by examining how the pretreatment interplay between anxiety and depression affects the strength of this association.
Method
Open Data, Open Materials, Open Code, or Preregistration
The analysis code appears online. The main analyses of the trial were preregistered before recruiting the first patient. The informed-consent form signed by the participants stated that their data would be kept strictly confidential. The data are currently not available because sharing them requires obtaining the consent of participants and approval from the Ethics Committee. The sample size determination, all data exclusions, all manipulations, and all measures are reported in the study protocol (Zilcha-Mano et al., 2018).
Study Design and Participants
The sample included 100 individuals with MDD participating in a randomized controlled trial (RCT; Zilcha-Mano et al., 2021). The patients’ demographic and clinical characteristics are presented in Table S1 in the Supplemental Material available online. The inclusion criteria were (a) current MDD diagnosis using structured clinical interviews for the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2013), with scores above 14 on the 17-item measurement of high risk of suicide or self-harm (Hamilton Rating Scale for Depression [HRSD]; Hamilton, 1967) at two evaluations 1 week apart, and current MDD based on the Mini-International Neuropsychiatric Interview (Sheehan et al., 1998); (b) if on medication, patients’ dosage had to be stable for at least 3 months before the start of the study, and patients were asked to maintain stable dosage for the duration of treatment; (c) age between 18 and 60 years; (d) Hebrew language fluency; and (e) written informed consent. Exclusion criteria were (a) current high risk of suicide or self-harm (HRSD suicide item > 2); (b) current substance abuse disorder; (c) current or past schizophrenia, psychosis, bipolar disorder, or severe eating disorder, requiring medical monitoring; (d) history of organic mental disease; and (e) currently in psychotherapy. Like other RCTs for MDD and as a priori hypothesized, no differences were found between treatments in their efficacy. The trial protocol (Zilcha-Mano et al., 2018) and main outcome (Zilcha-Mano et al., 2021) provide further details about the trial. All procedures were approved by the institutional review board, and participants signed informed-consent forms.
Treatments
All participants received a short-term treatment targeting depression in one of two forms: supportive-expressive treatment (SET) or supportive treatment (ST). Although both treatments targeted the same mechanism underlying the depressive symptoms—maladaptive interpersonal repetitive tendencies—one did so through the use of interpretations (SET), and the other did so through the use of supportive techniques (SE).
Measures
Severity of depressive symptoms and severity of anxiety were measured using the Beck Depression Inventory (BDI-21; Beck et al., 1996) and the Beck Anxiety Inventory (BAI-21; Beck & Steer, 1990), respectively. The BDI-21 and BAI-21 were chosen because (a) both were administered repeatedly and on the same schedule: weekly, throughout the course of treatment (16 weeks) and twice at baseline; and (b) both were measured in the same manner, by self-report (unlike semistructured interviews, such as the HRSD).
Overview of Statistical Analyses
Within-individuals association between reduction in depression and subsequent reduction in anxiety
To test the within-individuals association between reduction in depression and subsequent reduction in anxiety, multilevel model was used with observations over time nested within patients nested within therapists. Analyses were conducted in R using the nlme package. The outcome variable was reduction in anxiety (from session T + 1 to T + 2). The predictor of interest was the prior reduction in depression (from session T to T + 1). To account for potential autoregressive effects, the following variables were controlled for: the previous level of anxiety (at session T + 1) and the previous reduction in anxiety (from session T to T+1).
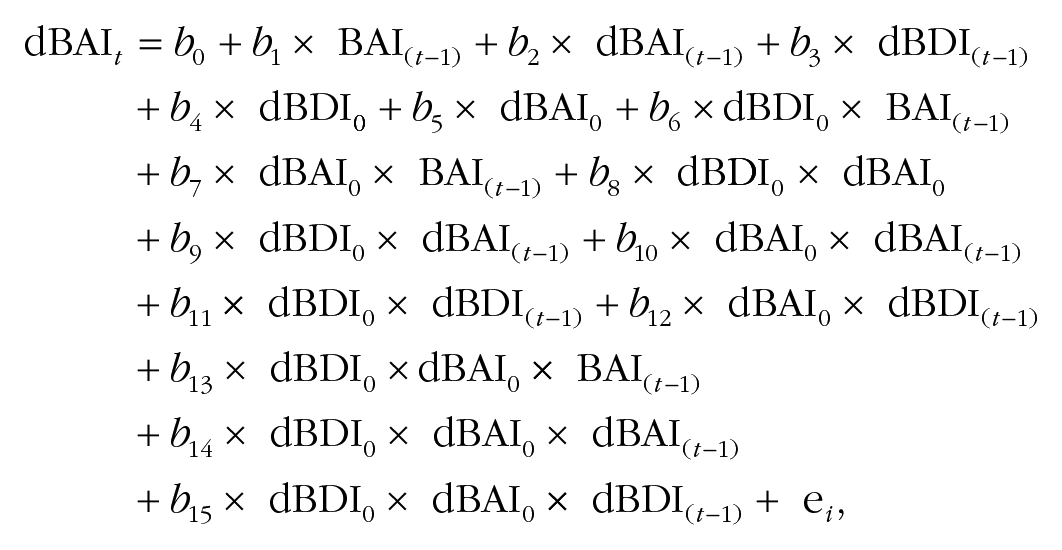
The equation was as follows:

where dBAI it is the change in anxiety between sessions t and t – 1; BAIi(t–1) is the anxiety at session t – 1, t = 3, . . ., 16, for subject i; dBAIi(t–1) is the change in anxiety between sessions t – 1 and t – 2; dBDIi(t–1) is the change in depression between sessions t – 1 and t – 2; and γ1i, γ2i, and γ3i are their coefficients, respectively, for the subject i, assumed to be random effects of a normal distribution and to be independent of error eit, which also has a normal distribution.
Exploring between-individuals variability in the depression-anxiety effect
Qualitatively distinct subpopulations
To explore potentially distinct subpopulations in the sample for whom qualitatively distinct effects of changes in depression on subsequent changes in anxiety exist, data-driven cluster-analysis approaches were used. Two approaches were implemented independently: (a) applying separate models for each individual and then implementing a cluster-analysis approach on the estimated coefficients and (b) applying a model to the entire sample that assumes clustering in the distribution of the parameters using the mclust package in R.
Quantitatively different magnitudes
To explore potentially quantitatively different magnitudes of the distinct effect of changes in depression on changes in anxiety, the focus of inquiry was the pretreatment interplay between them. The model described above was used and added a three-way interaction of the moderating effect of the interaction between pretreatment changes in depression and pretreatment changes in anxiety on the association between reduction in depression (from session T to T + 1) on subsequent reduction in anxiety (from session T to T + 1). The pretreatment change refers to the change between the two pretreatment assessments. Positive values refer to an increase from one point to the next, and negative values refer to a decrease. As has been done in the original model, to account for potential autoregressive effects, I controlled for the following variables: the previous level of anxiety (at session T + 1) and the previous reduction in anxiety (from session T to T + 1). The models accounted for all the lower-order interactions and main effects of the three-way interaction of interest. To explore the meaning of the estimated interaction, a heat map was used. The equation was as follows:
where dBAI0 and dBDI0 are the pretreatment changes in anxiety and depression. In this model, random effects were not included because the sample size did not enable this complexity.
Sensitivity analysis
(a) Given that analyses were conducted on RCT data, the analyses were repeated while controlling for the effect of the treatment condition. (b) The analyses were also repeated using structural equation modeling with the lavaan package in R. A random-intercept model was included, incorporating the effects of prior changes in anxiety to predict subsequent changes. In addition, the model included the previous level of anxiety and prior changes in depression. To address endogeneity, as recommended by Gistelinck et al. (2021), the correlation between the random intercept and the initial changes in anxiety was also accounted for.
Results
Within-Individuals Association Between Reduction in Depression and Subsequent Reduction in Anxiety
As reported in Table 1 (Model 1), findings suggest that the predictor of interest, changes in depression (from session T to T + 1), significantly predicted a subsequent reduction in the dependent variable, anxiety (from session T + 1 to T + 2). Specifically, greater reduction in depression predicted greater subsequent reduction in anxiety. This effect contributed significant unique variance above the variance explained by the autoregressive effects, which were also significant.
Within-Individuals Association Between Reduction in Depression and Subsequent Reduction in Anxiety (Model 1) and Between-Individuals Differences in the Magnitude of This Association as the Result of the Pretreatment Interplay Between Depression and Anxiety (Model 2)

Note: Partial η2 was calculated by the effectsize package of R. BAI = Beck Anxiety Inventory; BDI = Beck Depression Inventory; d = delta.
Exploring Between-Individuals Variability in the Depression-Anxiety Effect
Qualitatively distinct subpopulations
The two approaches that were implemented demonstrated convergent findings according to which distinct subpopulations of the effect of changes in depression on subsequent changes in anxiety were not found in the sample. Specifically, the distribution of the individual coefficients estimated in the first approach was single-mode shaped (rather than bimodal and above), as shown in Figure 1. Using the lccm procedure in the second approach with two clusters resulted in a degenerated clustering in which one cluster had only two members.
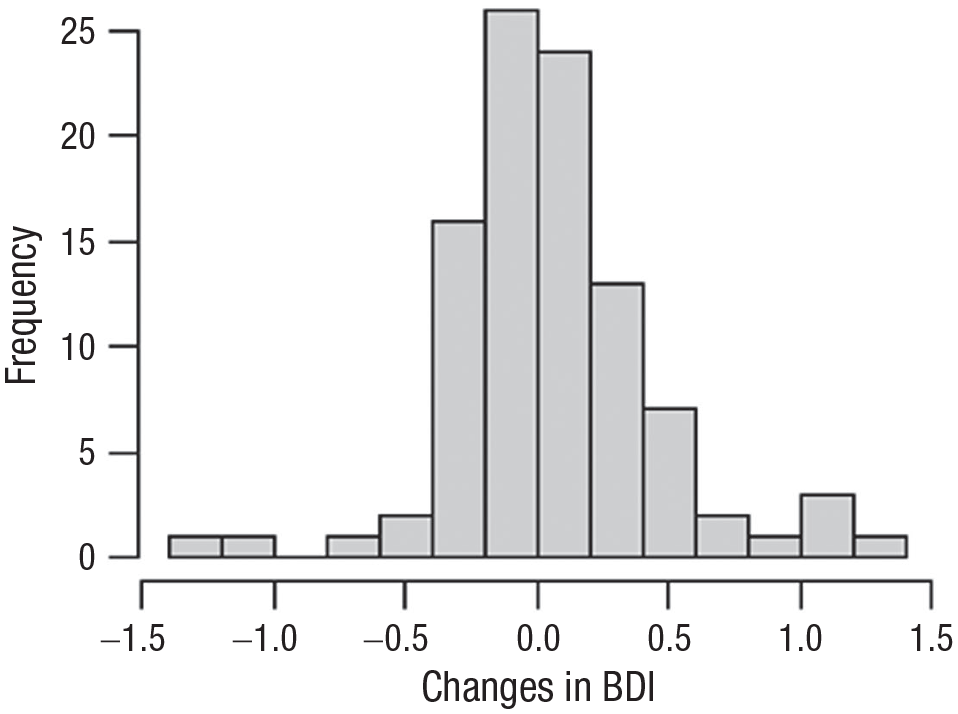
Distribution of individual estimated coefficients.
Quantitatively different magnitudes
As shown in Table 1 (Model 2), the three-way interaction of interest was significant. The heat map suggests that for individuals who showed a pretreatment increase in depression and a decrease in anxiety, a greater reduction in depression was associated with a greater subsequent reduction in anxiety (Fig. 2). This effect contributed a significant unique variance above the variance explained by the autoregressive effects.
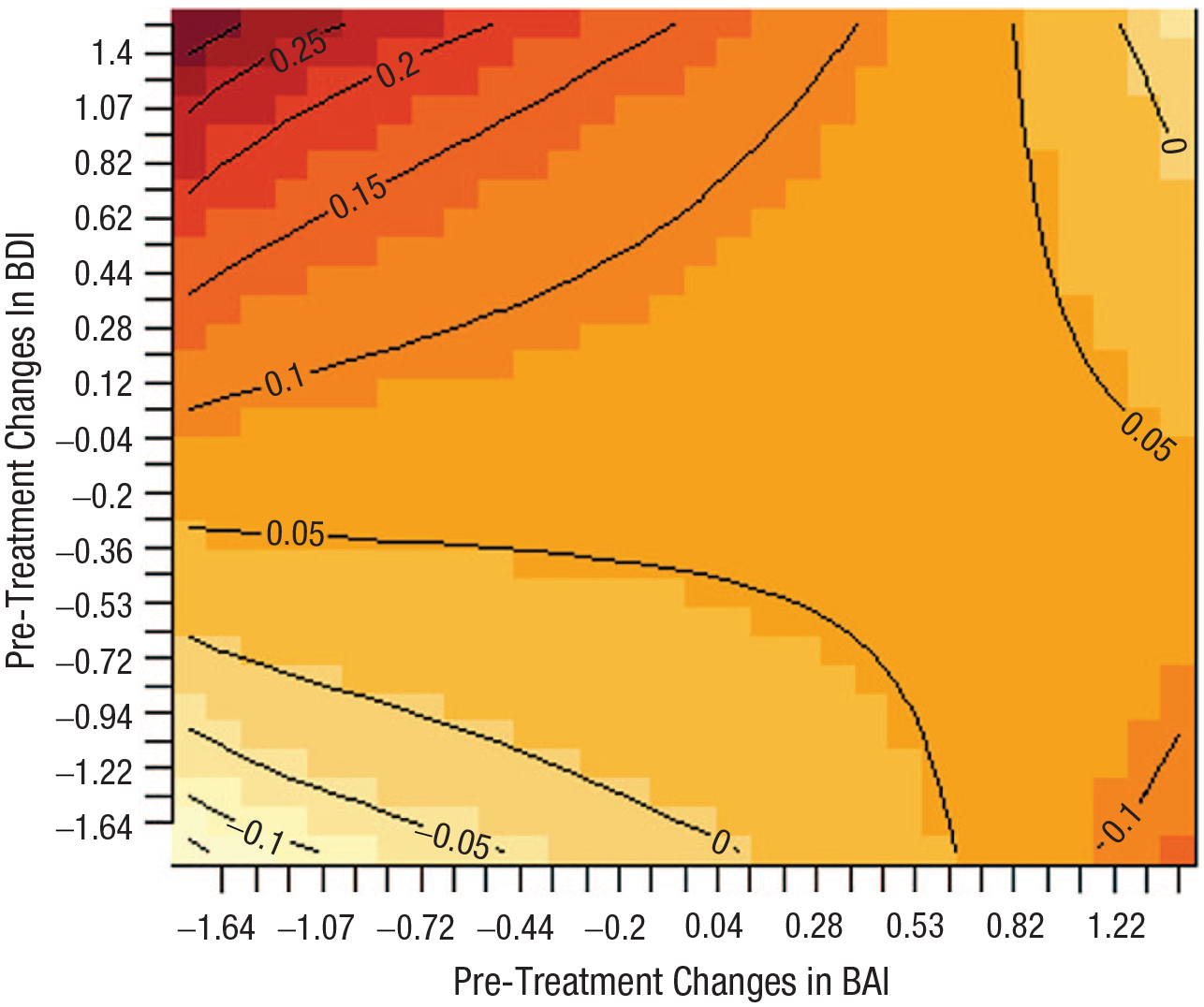
Heat map of the estimated moderating effect of the pretreatment interaction between depression and anxiety on the association between reduction in depression and subsequent reduction in anxiety.
Sensitivity analysis
(a) Findings remained the same when controlling for the potential effect of treatment conditions (see Table S2 in the Supplemental Material). (b) The structural equation modeling analysis results closely mirrored those obtained from multilevel modeling; the structural equation model suggested an even stronger predictive value of depression reduction for subsequent anxiety reduction (see Table S3 and Fig. S1 in the Supplemental Material). This replication further reinforces the robustness of the findings.
Discussion
Comorbidity of depression and anxiety disorders is the rule, not the exception (Kessler et al., 2015). This study examined whether reducing depression through targeted treatment also leads to a subsequent reduction in anxiety and applied data-analytic approaches to explore qualitative and quantitative differences between individuals in this within-individual process, aiming to inform future personalized treatment approaches. Findings suggest that a reduction in depression following treatment targeting depression results not only in a reduction in depressive symptoms but also in a subsequent reduction in anxiety. That is, when targeting depression, a prior reduction in depression repeatedly predicts a subsequent reduction in anxiety over the course of treatment. Although qualitatively distinct subpopulations with unique within-individuals effects were not found, quantitative differences were observed between individuals such that the pretreatment interplay between depression and anxiety predicted the magnitude of the within-individuals effect. These findings attest to the potential of personalizing treatments based on the quantitative differences in within-individuals depression-anxiety associations.
Comorbidity between depression and anxiety complicates psychopathology, treatment course, and prognosis (Ter Meulen et al., 2021). This proof of concept provides a blueprint for addressing some of the most common questions in clinical practice: What should be the therapeutic priority given the large comorbidity between depression and anxiety? Would treating depression result in subsequent improvement in anxiety? The findings suggest that at the sample level, targeting depression results in subsequent anxiety reduction as well. Although this effect was observed at the sample level, it is important to know whether different patients show different patterns of this within-individuals effect to guide treatment personalization. For patients showing a pretreatment increase in depression and a decrease in anxiety, a greater reduction in depression during treatment was associated with a greater subsequent reduction in anxiety. This suggests that for individuals exhibiting the pretreatment dynamic identified in this study, targeting depression may effectively address both disorders, but for individuals who do not display this particular dynamic, additional or alternative treatments might be required.
Understanding within-patients processes is crucial for shedding light on therapeutic mechanisms (Zilcha-Mano, 2021). Although between-patients effects address efficacy (e.g., Does treatment for depression also reduce anxiety?), these effects can occur under various scenarios, such as independent reduction in depression and anxiety because of different mechanisms within the treatment. By contrast, within-patients effects zoom in on the mechanisms of change, examining whether reducing depression in an individual predicts a subsequent reduction in anxiety. The findings further suggest that in individuals characterized by a pretreatment interplay between depression and anxiety, targeting depression may initiate a within-individuals process that leads to subsequent changes in anxiety as well because of their interconnected nature. Importantly, the literature shows that findings from between- and within-patients levels cannot be inferred from one another without making unrealistic assumptions (Fisher et al., 2018; Hamaker, 2012; Molenaar, 2004). Moreover, applying the same moderators to these different levels can yield contradictory results (Zilcha-Mano & Webb, 2024). This study aligns with the growing call to integrate analyses of within-patients mechanisms with the exploration of individual differences (Borsboom & Haslbeck, 2024).
The focus on between-individuals heterogeneity in within-individuals processes holds great potential for personalized treatment. Such heterogeneity can serve the development of personalized actionable information on how to address comorbidity most effectively in clinical work. Although these findings need to be replicated with larger samples and more frequent measurements of depression and anxiety before and during treatment (Bringmann et al., 2023), they suggest that understanding the pretreatment interplay between depression and anxiety is critical for elucidating whether treating depression is sufficient for reducing both depression and anxiety. The pretreatment interplay may provide insight into the individual-specific pathophysiology, which may then be directly targeted in treatment (Zilcha-Mano, 2024). Future studies should examine the mechanisms explaining this effect. One post hoc explanation is that the mechanism underlying this finding is the distinct pathophysiology of individuals with comorbid depression and anxiety. Individuals whose psychopathology is marked by the specific interplay between anxiety and depression—a profile showing an increase in depression and a decrease in anxiety—may benefit most from treatments that prioritize addressing depression because this approach could alleviate both their depressive and anxious symptoms. Another possible post hoc explanation of this finding is that the mechanism underlying it is an expectancy effect concerning impending treatment (Constantino et al., 2018) such that expecting treatment, some individuals may show a reduction in their worries but sink deeper into depression. For these individuals, targeting depression may be sufficient to induce meaningful changes in anxiety as well.
The two most important limitations of the current work are the sample size and the limited number of assessments, especially before treatment. Although the weekly assessments during treatment provided a relatively strong power for investigating within-individuals processes (16 time points per patient with a very small percentage of missingness), the pretreatment assessments were more limited. The pretreatment assessments enabled proof-of-concept appreciation of the importance of observing the dynamics of depression before the start of treatment. To fully leverage the potential utility of understanding the pretreatment interplay, it is necessary to collect a sufficient number of observations to capture the full dynamic patterns of depression and anxiety before treatment begins and the interplay between them (Bringmann et al., 2023). Identifying the pretreatment dynamic patterns of the individual’s psychopathology has the potential to help tailor the treatment to match the full richness of every individual and achieve more effective outcomes (Cohen et al., 2021; Zilcha-Mano, 2024). Future studies should explore the optimal duration and frequency of pretreatment measurements (Zilcha-Mano, 2024).
The question of whether anxiety and depression are distinct diagnoses is beyond the scope of this work. Yet the observed heterogeneity in how individuals respond to treatment suggests that different mechanisms may be at play for different individuals. The p-factor approach, which focuses on shared underlying factors across psychopathologies (Böhnke & Croudace, 2015; Caspi & Moffitt, 2018; Lahey et al., 2012), may appear at odds with these findings, but they can also complement each other. The findings identify subpopulations for which a mono-treatment approach, potentially targeting common underlying mechanisms, may reduce symptoms of both depression and anxiety, minimizing the need for multiple treatments. This study may contribute to the p-factor literature, which focuses mainly on between-individuals variances (Watts et al., 2024), by adding a deeper understanding of individual differences in within-individuals processes. It suggests that for a subpopulation of individuals, providing a single treatment that targets one of the disorders can be effective for both, whereas for others, it may not be.
Future studies are needed to examine whether these findings can be replicated across diverse populations, types of treatment, and analytic models. As in any psychotherapy (vs. experimental) study, it is challenging to completely disentangle the various contributing components. Although the level of treatment adherence in the current RCT was high (Zilcha-Mano et al., 2021), it cannot be completely ruled out that therapists may have made some minor adjustments in their therapeutic work to respond not only to patients’ depression but also to their level of anxiety (e.g., addressing anxious ruminations when working on mechanisms contributing to depression). In the present study, the two treatments designed to reduce depression did not yield distinct patterns of results. However, using treatments that specifically target depression, anxiety, or a combination of both (Wright et al., 2014) may yield different results. That is, in this study, we focused on whether reducing depression through targeted treatment also reduces anxiety, and thus, treatments targeting depression were used. An equally important question for future research is whether reducing anxiety through targeted treatment will similarly reduce depression. It will also be informative to explore the two directions of effects within the same individuals receiving transdiagnostic treatments that include distinct modules targeting each condition. Additionally, this study examined the within-individual association between anxiety and depression. Future research should complement these findings by investigating the interplay between the specific symptoms that constitute each diagnosis (Beard et al., 2016).
This study serves as a proof of concept for addressing some common clinical questions regarding therapeutic priorities. If replicated, the findings indicate that treatments targeting depression (e.g., SE, behavioral activation, and cognitive restructuring) not only reduce depression but may also subsequently reduce anxiety even without directly targeting it. This effect is particularly notable in individuals sharing similar pretreatment patterns of interplay between depression and anxiety. This finding is instrumental because a frequent clinical question is whether treating one mental-health disorder in individuals with comorbidities can also treat co-occurring disorders. This knowledge can inform personalized strategies to address comorbidities in individuals with MDD: Although some patients may benefit from treatments targeting depression, others with a specific pretreatment profile of anxiety-depression dynamics may require targeted interventions addressing either anxiety alone or both conditions to achieve optimal outcomes.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026241301056 – Supplemental material for Is Targeting Depression Sufficient to Alleviate Anxiety Comorbidity? Exploring Between-Individuals Heterogeneity in Within-Individuals Processes
Supplemental material, sj-docx-1-cpx-10.1177_21677026241301056 for Is Targeting Depression Sufficient to Alleviate Anxiety Comorbidity? Exploring Between-Individuals Heterogeneity in Within-Individuals Processes by Sigal Zilcha-Mano in Clinical Psychological Science
Supplemental Material
sj-jpg-1-cpx-10.1177_21677026241301056 – Supplemental material for Is Targeting Depression Sufficient to Alleviate Anxiety Comorbidity? Exploring Between-Individuals Heterogeneity in Within-Individuals Processes
Supplemental material, sj-jpg-1-cpx-10.1177_21677026241301056 for Is Targeting Depression Sufficient to Alleviate Anxiety Comorbidity? Exploring Between-Individuals Heterogeneity in Within-Individuals Processes by Sigal Zilcha-Mano in Clinical Psychological Science
Footnotes
Acknowledgements
I extend sincere gratitude to Laura Bringmann for her invaluable consultation and insights.
Transparency
Action Editor: Pim Cuijpers
Editor: Jennifer L. Tackett
Author Contributions
Sigal Zilcha-Mano: Conceptualization; Data curation; Formal analysis; Funding acquisition; Methodology; Validation; Visualization; Writing – original draft.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.