
Abstract
Estimates suggest that meditation use is comparable to mental-health-service access in the United States. Understanding meditation-related adverse effects (AEs) is therefore critical. We aimed to (a) estimate the incidence of meditation-related unusual experiences and AEs using different methods and (b) identify sociodemographic and health-related characteristics predicting their incidence. We conducted a cross-sectional, population-based survey of 886 U.S. adults (approximately representing population age, gender, and race/ethnicity) stratified by lifetime meditation experience and type. Of the participants, 96.6% reported an unusual experience, 58.4% reported an AE (Inventory of Meditation Experiences), 78.3% endorsed one or more items on the Meditation-Related Adverse Effects Scale, 31.4% endorsed experiencing a challenging/difficult/distressing experience, and 9.1% reported functional impairment because of AEs. In a robust multiple regression, psychological distress, psychoticism, unusual beliefs, and meditation-retreat participation were positively associated with unusual experiences and AEs. It is essential that (a) potential meditators are informed about possible experiences, (b) providers consider risk factors, and (c) AEs are routinely and actively monitored.
Meditation, in its many varied forms, is used as commonly as mental health promotion and management intervention in the United States (Davies et al., 2024; Terlizzi & Schiller, 2022). Given use by approximately 60.5 million people in 2022 (18.3% of the adult population; Davies et al., 2024), even low rates of potential harm could have huge individual and societal impacts. Although the field knows a considerable amount regarding the potential benefits of meditation, surprisingly little is known about adverse effects (AEs; Baer et al., 2019; Britton et al., 2021). Recent studies have suggested that meditation may lead to AEs and experiences of unusual psychological states; however, the research thus far has shortcomings around definitions and incidence rates that limit their reliability, interpretability, and applicability.
Meditation reflects a broad array of practices (Van Dam et al., 2018) used for a wide variety of purposes (Sedlmeier & Theumer, 2020). Much of what is known empirically about meditation comes from studies on mindfulness-based programs (see e.g., Van Dam et al., 2018), structured training programs that emphasize intensive meditation training, and experiential learning related to mindfulness (Crane et al., 2017). The broader set of practices spans an incredibly wide array of techniques, goals, and contextual factors (Matko et al., 2021). Relatedly, there are also therapeutic approaches that integrate concepts related to mindfulness and/or Buddhist philosophy but do not emphasize intensive meditation training (mindfulness-informed interventions; Shapero et al., 2018). Although differentiating meditation activities that are used clinically from those used for personal/spiritual growth is important (Van Dam et al., 2018), in this article, we largely focus on a generic definition of meditation, that is, those activities aimed at training attention and awareness in themselves and as oriented to thoughts, emotions, sensations, and more general concepts or ideas. The rationale for this generic approach is that it permits comparison with both population-level data in the United States as assessed by the U.S. Centers for Disease Control and Prevention every 5 years from 2002 to 2022 (see Davies et al., 2024) and with a considerable number of previous observational studies of meditation-related unusual experiences and AEs (Cebolla et al., 2017; Goldberg et al., 2022; Pauly et al., 2022; Schlosser et al., 2019; Vieten et al., 2018). The definition also permits comparison with therapeutic approaches that incorporate a broad variety of meditation techniques (although not most mindfulness-informed interventions).
Before any consideration of AEs, it is important to consider unusual or nonordinary experiences because these experiences sometimes contain AEs and more positive experiences (Lindahl et al., 2017). Although there is no common definition of unusual or nonordinary experiences, they are generally viewed as representing experiences or functions that stand out or are considered special or uncommon relative to what the individual thinks is ordinary or occurs in day-to-day experience (Taves et al., 2023). A key distinction lies in the specification that these are not necessarily frequent experiences for an individual within a relatively constrained time period (e.g., past week). Note that unusual/anomalous/nonordinary experiences may not be uncommon among the population during a protracted temporal period (e.g., past year or over lifetime), analogous to psychosis-like symptoms (occurring in as many as 28% to 44% of the population; Kendler et al., 1996; Peters et al., 1999). However, high frequency (Pechey & Halligan, 2012) and/or intense severity (Wright et al., 2024) is relatively uncommon, analogous to delusions/hallucinations among individuals with a diagnosable form of psychosis (Freeman, 2006).
In contrast to unusual experiences, there is a separate literature regarding unwanted effects that occur in response to treatment or intervention (see e.g., Klatte et al., 2023; Klein et al., 2024; Schermuly-Haupt et al., 2018). Ascertainment of causality is essential to the process; unwanted events that are not related to treatment or intervention may be related to the natural course of illness among an individual and/or attributable to factors other than the intervention (Britton et al., 2021; Schermuly-Haupt et al., 2018). Among the subset of unwanted effects that are treatment-related, side effects are unintended consequences and/or undisclosed potential outcomes (i.e., not included on “package insert” or treatment-overview documents) that are the result of correctly applied treatment. Note that those effects that are the result of incorrectly applied treatment are considered malpractice in clinical settings (Schermuly-Haupt et al., 2018).
AEs are those side effects that are negatively valenced or subjectively unpleasant, and resulting harm is defined as any kind of suffering (physical, psychological, social, etc.) or functional impairment (World Health Organization, 2010). Meditation-related AEs are reliably documented in historical sources (e.g., Ahn, 2021; Fisher, 2021; Sayadaw, 2016; Yates et al., 2017) and recent academic literature (for reviews, see Baer et al., 2019; Lindahl et al., 2021; Lustyk et al., 2009; Van Dam et al., 2018). Harms monitoring is largely geared toward clinical practice and trials, in circumstances in which an indicated treatment target is typically identified. The fact that meditation is used for a variety of purposes, including health/well-being promotion, managing/mitigating ill health, and personal/spiritual growth (see e.g., Sedlmeier & Theumer, 2020), potentially contributes to limited monitoring, which is required only in circumstances in which there is clinical/research governance oversight (e.g., by accreditation bodies, government agencies, or ethics committees). In many circumstances, only serious AEs (those AEs that are life-threatening, result in death, or lead to incapacitation) are required to be reported (Wong et al., 2018). Thus, it is challenging to get a reliable estimate of the prevalence of meditation-related AEs.
Meta-analytic estimates suggest overall meditation-related AE prevalence of 8.3% (Farias et al., 2020): 3.7% prevalence in experimental studies (including clinical trials) and 33.2% in observational studies (including retrospective assessments of large samples of meditators). However, there is considerable variation in how AEs are measured (for a detailed discussion, see e.g., Britton et al., 2021). The vast majority of clinical trials have used spontaneous reporting and/or reporting of serious AEs only (Wong et al., 2018). Evidence suggests that spontaneous reporting can yield significant underestimates of harms for a variety of reasons (Kramer, 1981). In contrast to the < 1% prevalence of AEs observed in a meta-analysis of mindfulness trials that largely used passive monitoring (Wong et al., 2018), active monitoring has resulted in documented AEs among as many as two-thirds of participants (Baer et al., 2021; Britton et al., 2021)—consistent with estimates in psychotherapy (Klein et al., 2024). Harms monitoring includes assessing deterioration of existing symptoms, emergence of new symptoms, and general deterioration, among other issues (see e.g., Linden, 2013). Symptomatic deterioration (one type of AE, distinct from emergence of new symptoms) has been shown to occur in 15% to 44% of participants in community offerings of mindfulness-based stress reduction (Hirshberg et al., 2022), although many have highlighted concerns that such a method can fail to capture the complex nature of treatment-related changes (potential improvements in some domains alongside deterioration in others) and entirely miss the emergence of new symptoms (see Britton et al., 2021; Dimidjian & Hollon, 2010; Van Dam & Galante, 2023). Thus, active monitoring of a variety of forms of harms is generally recommended (Linden & Schermuly-Haupt, 2014).
Even within this context, an additional consideration is whether questions are open-ended (asking participants to list/describe any AEs) or generic (asking a single question about potential distress, harms, etc.) or involve a specific checklist. Providing only an open-ended option is essentially akin to spontaneous reporting because it puts the onus on the participant to decide what might constitute a side effect, harm, or AE. Although generic questions are better than no monitoring at all, direct comparison of generic questions with checklists in general contexts indicates that the former underestimates AEs by significant amounts (Allen et al., 2018).
Prevalence notwithstanding, it is important to know whether AEs are expected or unexpected, how long they last, and the impact they have on an individual. AEs can vary in their frequency, duration, and impact. Both the duration of an AE and its impact on the individual’s everyday functioning are related to the level of harm (Britton et al., 2021), suggesting that even rare (i.e., infrequent and/or one time) events could result in significant harm. There is limited information available on the duration of AEs, suggesting that such events can last from a few seconds/minutes/hours to months or years (Britton et al., 2021; Goldberg et al., 2022; Lindahl et al., 2017). Note that there is no agreed minimal duration that results in an experience being relevant to the individual or treatment or to it potentially being harmful (Lineberry et al., 2016; World Health Organization, 2010).
Harm or functional impact is somewhat more challenging to quantify. Harm can be considered as any of the broad array of events that are considered AEs (e.g., deterioration of symptoms, emergence of new symptoms, interpersonal impairment; Lilienfeld, 2007; Linden & Schermuly-Haupt, 2014). However, assessment of functional impairment in mental health focuses on limitations to activities or behavior and restrictions on participation in life and society (Gold, 2014). Although formal assessment of domains of function is recommended, harm or functional impairment has largely been assessed in meditation-related AE monitoring by asking patients/participants directly about “harm” or impairment in “ability to function.” Harm was reported to occur in ≈3% of 157 participants undertaking an 8-week mindfulness-based program (Baer et al., 2021), whereas functional impairment was reported in ≈37% of 96 participants of a mindfulness-based cognitive-therapy-dismantling study (Britton et al., 2021) and 10.6% of a cross-sectional assessment of 434 mediators (Goldberg et al., 2022). The variability of these estimates highlights the need to provide more reliable estimates in a representative sample. However, few studies have examined representative samples or looked at meditation-related AEs in multiple ways in addition to measuring functional impairment and its duration.
Recently, Goldberg and colleagues (2022) found that 50% of 434 U.S. meditators endorsed one or more meditation-related AE (MRAE) items using a 10-item checklist (Britton et al., 2018), whereas 32.3% of their sample endorsed a single-item generic AE question (“I personally have had challenging, difficult, or distressing experiences as a result of my meditation practice”). The work by Goldberg and colleagues represents a significant advance in MRAE assessment. Despite the considerable value of recent work by Goldberg and colleagues, their sample comprised largely inexperienced mediators who were largely healthy (i.e., limited mental illness). In addition, although there are limited data on possible predictors of unusual experiences and AEs, the available data suggest that different subpopulations of meditators may experience different incidence rates (see e.g., Goldberg et al., 2022; Pauly et al., 2022; Schlosser et al., 2019); therefore, some of the variability in prevalence estimates may be explained by nonrepresentative surveys inadvertently sampling different subpopulations. For example, Goldberg and colleagues reported a single-item MRAE rate of 32.3% (50% rate using a multiitem checklist) among a sample of meditators, 60.1% of whom had 100 hr of practice or less and 6.9% of whom had attended a residential retreat. Two prior studies reported a single-item rate of 22% (Pauly et al., 2022) and 25.6% (Schlosser et al., 2019) among meditators, for whom 75% had a minimum approximate level of experience of 359 hr and 625 hr, respectively, and 57.4% and 63.5% of whom had attended a residential retreat, respectively. One possibility is that greater numbers of participants who experience significant AEs discontinue meditating than participants who do not experience significant AEs. As a direct result, estimates may vary when sampling largely newer meditators versus more experienced meditators.
To address the above limitations, we aimed to assess a broader set of unusual experiences and AEs in a larger sample that not only approximated the U.S. population but, more important, also approximated meditation type and experience distribution. Furthermore, we used a tool that has demonstrated initial psychometric validity (Van Dam et al., 2024). Finally, we measured sociodemographic and psychological characteristics for which there is suggestive evidence of predicting the risk of AEs (Goldberg et al., 2022).
In this study, we set out to answer two main questions:
Research Question 1: What is the incidence of (a) unusual experiences and (b) AEs in a representative sample of U.S. adult meditators?
Research Question 2: To what extent do sociodemographic, personality, meditation history, trauma history, mental health, and substance use predict meditation-related (a) AEs or (b) unusual experiences?
We had two a priori hypotheses related to question 1:
Hypothesis 1a: The rate of unusual experiences would not be significantly higher than the previously reported 88% in Vieten et al. (2018).
Hypothesis 1b: The incidence of AEs using an existing single-question tool asking about whether any AEs were experienced (generic AE) would not be significantly different to the previously reported 32.3% in Goldberg et al. (2022).
We then added the following hypotheses:
Hypothesis 1c: Rates of endorsement of any of the 14 MRAE items would not be significantly different to the previously reported 50% in Goldberg et al. (2022).
Hypothesis 1d: As measured by the Inventory of Meditation Experiences (IME), the rate of endorsing any of the items at slight or greater intensity and mild or greater unpleasantness would not be different to the previous AE incidence rate of 50% in Goldberg et al. (2022).
A priori, we predicted the following in relation to question 2:
Hypothesis 2a: Unusual beliefs, psychedelic use, meditation hours, and retreat attendance will predict unusual experiences.
Hypothesis 2b: Trauma history and psychological distress, added to the prior variables, will predict AEs.
Transparency and Openness
The study was preregistered at the following source before data collection: https://osf.io/r8beh. Data, materials, and code are available via the following link: https://osf.io/3mn9y/. We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study. All procedures were approved by the University of Melbourne Human Research Ethics Committee (No. 23969) and was conducted in accordance with provisions of the Declaration of Helsinki.
Method
This study comprised a cross-sectional survey, preregistered at osf.io/r8beh. Several modifications/deviations from the preregistration were made. (a) To improve manuscript clarity, preregistration Q4 (pertaining to varying estimates as a function of method) was added to preregistration Q1 (pertaining to incidence rates) to group them thematically, Hypothesis 1a became Hypothesis 1b and vice versa, and because we did not predefine our operationalization of AE for the multiple regression, we examined all three variations. (b) To improve manuscript accuracy, we used “adverse effects” (which typically refers to any undesired effect related to an intervention) instead of “adverse events” (which typically refers to a negative incident within the context of health-care provision or a clinical trial, arguably to which self-guided meditation does not apply) and “incidence” (which refers to the occurrence percentage or rate of an event in a given sample) instead of “prevalence” (which has a similar implication to incidence but typically reflects rates in a population). (c) To address utility concerns from statistical inference resulting from unexpected sample distributions, Bayesian analyses were added to explore support for the null in Hypothesis 1 because our originally proposed test (null-hypothesis chi-square test) is capable only of rejecting or not rejecting the null, and given the overwhelming number of participants who endorsed unusual experiences, number of unusual experiences replaced presence/absence of unusual experiences in multiple regression. Only 30 people did not endorse an unusual experience, and thus, a binary version of this variable was ascertained to provide extremely limited information. (d) Finally, to improve construct validity and align definitions with best practice, we used the 30-item IME instead of the less reliable 103 items originally asked (see Van Dam et al., 2024). Although the IME represents a psychometrically valid scale, the 103 original items do not possess established psychometric properties, and reliance on them may present fundamental concerns regarding construct validity. In addition, we reduced the threshold for defining AEs from modestly unpleasant to mildly unpleasant to better align our study with the standard definition of an AE (World Health Organization, 2010).
Sample-size determination
Assuming an incidence rate of 50% (as previously reported in Goldberg et al., 2022), which is also the standard recommendation for an unknown incidence rate, a sample of 1,067 would ensure the marginal error of the estimate does not exceed 3% with a confidence level of 95% (Naing et al., 2022). A sample size of 1,067 would permit 80% power to detect associations as small as r = .09. Thus, we aimed to recruit approximately 1,100 participants in total.
Participants
U.S. meditators ages 18 years or older with meditation experience were invited to a prescreening survey. Quotas were implemented to approximate National Health Interview Survey 2017 categories (mindfulness, mantra, spiritual; National Center for Health Statistics, 2018). Per definition provided by the National Health Interview Survey, participants were informed that mindfulness meditation was inclusive of Vipassana, Zen Buddhist meditation, mindfulness-based stress reduction, and mindfulness-based cognitive therapy; mantra meditation was inclusive of transcendental meditation, the relaxation response, and clinically standardized meditation; and spiritual meditation was inclusive of centering prayer and contemplative meditation. Each category was balanced across users with low (0–100 hr), medium (101–1,000 hr), and high (> 1,000 hr) estimated lifetime hours of meditation. A subset of invited participants (n = 1,262) completed the full survey (response rate = 70.58%), and a subset of those participants (n = 1,102) passed data checks (e.g., attention checks, completion time). We removed responses (n = 216) because of lack of response variability, excessive response variability, or being multivariate outliers, for a final sample of 886. All participants provided written informed consent. Study data were collected between August and September 2022.
Measures
Sociodemographics
Participants were asked to provide the year they were born and the highest level of education they completed from eight possible categories and to identify their religious or spiritual beliefs. The panel provider (Prolific) supplied data on age, gender, nationality/country of residence, education level, and employment status.
Mental-health diagnosis
Participants were asked if they had ever been formally diagnosed with a mental illness. They were also asked if their diagnosis was received before or after commencing meditation practice.
Substance use
We used a modified, shortened version of the Alcohol Smoking and Substance Involvement Screening Test (ASSIST; WHO ASSIST Working Group, 2002) in which participants were asked about lifetime exposure and past 12-month frequency of substance use. We included nine substance categories: tobacco, alcohol, cannabis, cocaine, amphetamines, inhalants, sedatives, hallucinogens, and opioids.
Psychedelics use
If participants indicated lifetime exposure to hallucinogens in the ASSIST question, they were asked a follow-up questionnaire from the National Survey on Drug Use and Health (Center for Behavioral Health Statistics and Quality, 2016) about lifetime classic psychedelic use, including ayahuasca, dimethyltryptamine, LSD, mescaline, PCP, peyote, psilocybin, and “other.”
Psychological distress
We used the Kessler Psychological Distress Scale (K10; Kessler et al., 2002), a 10-item questionnaire measuring psychological distress. Responses were made on a 5-point Likert scale ranging from 1 (none of the time) to 5 (all of the time). Total scores provide a clinical indication of the presence of low (score = 10–15), moderate (score = 16–21), high (score = 22–29), or very high (score = 30–50) levels of psychological distress and the likelihood of a mental disorder, ranging from likely well (score = 10–19), likely mild mental disorder (score = 20–24), likely moderate mental disorder (score = 25–29), and likely severe mental disorder (score = 30–50). Internal consistency was excellent: α = .94, ω = .93.
Trauma
The Primary Care PTSD Screen for DSM-5 (PC-PTSD-5; Prins et al., 2016) identifies probable posttraumatic stress disorder (PTSD) in primary-care settings. Lifetime exposure to traumatic events is assessed as a binary (yes/no) question. Affirmative responses result in an additional five binary (yes/no) items being presented, measuring past-month symptom severity. A total score of 4 or higher was used to indicate probable PTSD.
Unusual beliefs and experiences (unrelated to meditation)
Participants were prompted to answer eight items relating to the Unusual Beliefs and Experiences Subscale of the Personality Inventory of the DSM-5 (PID-UBE; Krueger et al., 2012). We selected this scale because it is a brief measure designed to measure the maladaptive personality trait of having unusual experiences, and it is plausible that meditation-related unusual experiences are underpinned by and/or like those occurring among individuals who have elevated schizotypy. Unusual beliefs and experiences (UBEs) are a common schizotypal characteristic (Crego & Widiger, 2017). Responses were made on a 4-point Likert scale ranging from very false or often false to very true or often true. Responses were averaged to generate a total score and a cutoff of 1.5 SD from normative data was used to indicate likely clinical significance (Miller et al., 2022). Internal consistency was good: α = .86, ω = .87.
Psychoticism
Participants answered the five items from the Psychoticism Inventory from the PID-5 Brief Form (PID-BF; Krueger et al., 2012), which measured the personality-trait domain of psychoticism. We selected this measure for much of the same reasons as the PID-UBE. Responses were made on five items using the same 4-point Likert scale as the PID-UBE and then averaged to generate a total score. A cutoff of 1.5 SD from normative data was used to indicate likely clinical significance (Miller et al., 2022). Internal consistency was acceptable: α = .78, ω = .79.
Meditation history
Participants were also asked the total number of days they had spent in meditation retreats, if their practice was aligned to a spiritual tradition, and the context of their meditation (e.g., unguided, guided by an app). We calculated estimated lifetime-meditation hours as a multiplier of self-reported regular years of practice, number of practices per week, number of sits per day, and approximate length of each sit (see e.g., Bowles et al., 2022), adjusting each variable by Winsorization as necessary. Because broad categories of practice (permitting comparison with population-level data; see e.g., Davies et al., 2024) were not especially detailed, we also asked participants to select any/all types of 14 different techniques that they used from a previously established list (Matko et al., 2021). For additional information, see the Supplemental Material available onlines.
IME
The IME (Van Dam et al., 2024) is a 30-item scale, designed to measure a variety of meditation-related experiences. Because this same data set was used to develop and validate the scale, participants were presented with 103 total items. Participants provide information regarding the intensity of experiences during or after meditation, prayer, or chanting. A 6-point Likert scale was presented as follows: 1 = no, not at all; 2 = so slight, cannot decide; 3 = slight; 4 = moderate; 5 = strong; 6 = extreme. Items endorsed as slight or above were further assessed for valence. To equate time required across participants, 50 pseudorandomly selected items (selecting first from those endorsed as slight or greater and then from those below slight) were presented for valence rating. Participants were asked to rate each item on a 7-point Likert scale: 1 = extremely unpleasant, 2 = modestly unpleasant, 3 = mildly unpleasant, 4 = neutral (neither pleasant nor unpleasant), 5 = mildly pleasant, 6 = modestly pleasant, 7 = extremely pleasant. Scores presented in the present analyses reflect the 30 items that provide evidence of psychometric validity. The IME has three subscales (enabling experiences, disabling experiences, and self/reality distortions), although endorsement of any item can be used to reflect an unusual experience or, if unpleasant, an AE. The scale has good psychometric properties, established on this same data set (Van Dam et al., 2024).
Meditation-related AEs
To contextualize responses relative to previous estimates (Goldberg et al., 2022), participants were also presented with a slightly modified version of the MRAE Scale (MRAES; Britton et al., 2018), reflecting the most common disabling symptoms endorsed among a qualitative survey of meditators (Lindahl et al., 2017). The items were slightly adapted from their original form (Britton et al., 2018) to expand on three double-barreled items (e.g., “I had trouble thinking clearly and/or making decisions”) using the same response format as unusual experiences listed above. Endorsement of any of the 14 items as slight or greater was interpreted as having had that experience. Note that this is a departure from prior versions of the scale, which have used a yes/no response format. Consistent with the design of the MRAES (Britton et al., 2018) and as used previously (Goldberg et al., 2022), the occurrence, severity, and length of functional impairment of AEs was then examined in three follow-up questions. We note here that severity and functional impairment were self-ascertained by participants. Internal consistency was excellent: α = .90, ω = .90.
Data handling and statistical analysis
Data used in this study were previously reported in an article regarding the psychometric properties of the IME (Van Dam et al., 2024). Only complete data sets were included in analyses except for valence ratings. Valence data were presumed to be randomly missing by design. Missing values for valence were estimated via multiple imputation by random forests.
As per preregistration, rates of unusual experiences (Research Question 1, Hypothesis 1a) and three variations of AE (Hypotheses 1b–1d) were compared with prior estimates via Fisher exact probability (chi-square) tests with continuity correction (Research Question 1: Hypotheses 1b and 1c). Rates of AE with functional impairment were also compared via chi-square test. To better adjudicate potential support for null hypotheses, Bayesian proportion tests (via BayesFirstAid package) were additionally undertaken.
Per preregistration (Research Question 2), regression was undertaken as standard multiple and/or logistic regression for continuous and categorical regression, respectively. Assessments of linearity, normality, homoscedasticity, independence, and multicollinearity were undertaken. Given deviations from normality, we used robust regression as implemented in the robustbase package. We computed an MM-type regression estimator, which implements a bi-square redescending score function (Koller & Stahel, 2011; Yohai, 1987). The approach permits weighting of cases to adjust for nonnormality. All analyses were conducted in R as implemented in RStudio.
We added a post hoc estimation of zero-order associations to allow direct comparison with prior work (Goldberg et al., 2022). We examined associations between predictor variables with one another and of predictor variables with outcomes measures. Associations between different variable types were of interest, and thus, different estimators were used (for details, see the Supplemental Material). Given the large number of correlations, we used the false-discovery rate (FDR; Benjamini & Hochberg, 1995) to correct for multiple comparisons. Odds ratios were converted to equivalent r values using the effectsize package for comparison with zero-order correlations.
Results
Participants
Sociodemographics
The sample was approximately comparable with the U.S. adult population on age, race, and gender (U.S. Census Bureau, 2020). Participants had a median age of 40 (M = 42.00, SD = 13.88; U.S. census median age = 38.8 years). The sample was 51.35% female (50.9% in 2020 U.S. census) and 71.51% White (aligned with 71.0% who endorsed White alone or in combination with other races in 2020 U.S. census). Most participants (60.61%) held a bachelor’s degree or higher (more than 39.4% in 2020 U.S. census). For additional details, see Table 1.
Sociodemographic Characteristics of Sample
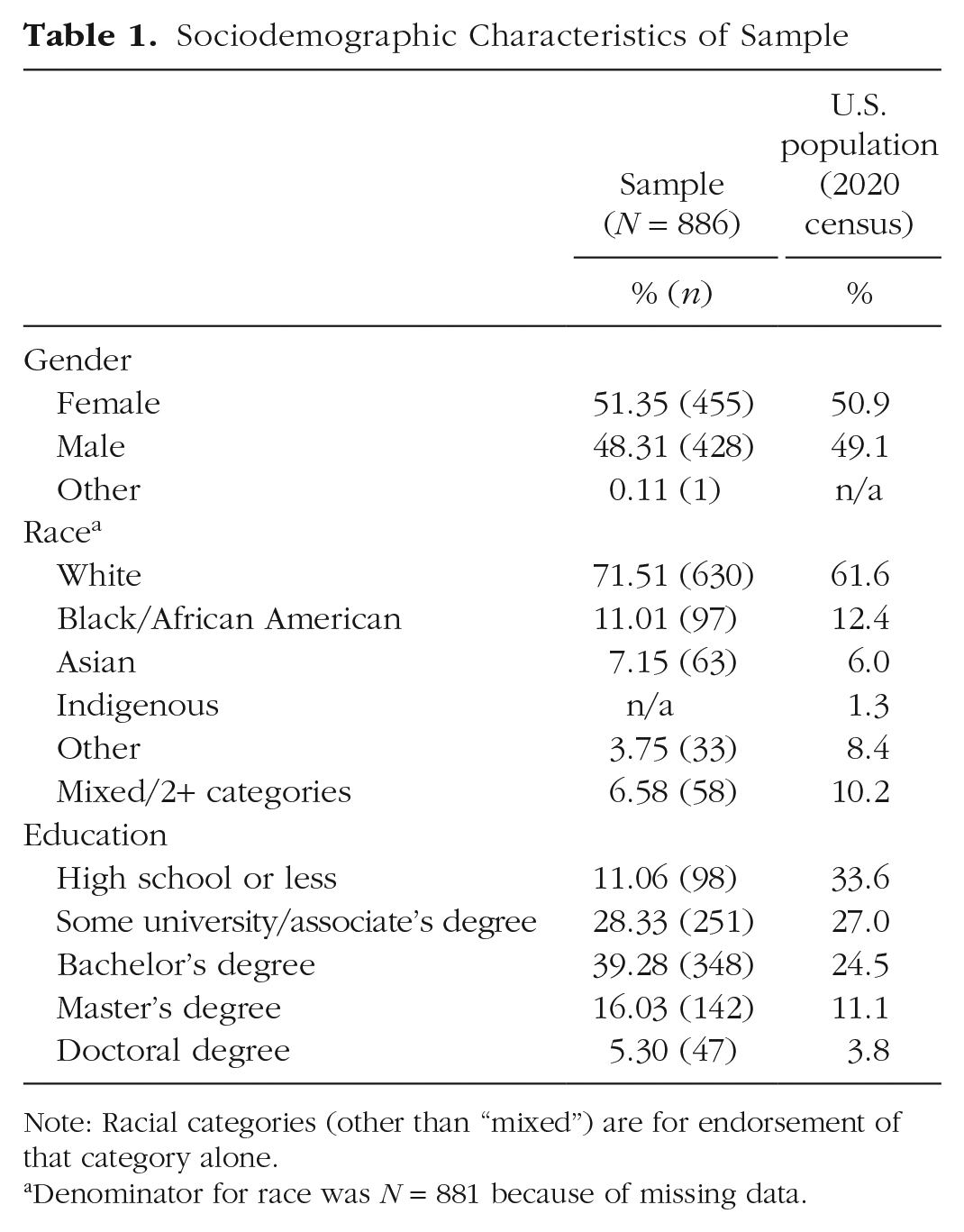
Note: Racial categories (other than “mixed”) are for endorsement of that category alone.
Denominator for race was N = 881 because of missing data.
Mental health
Participants were, on average, just below the cutoff for likely mild mental disorder (Kessler et al., 2002). The sample exhibited a high rate of likely mild mental disorder (42.78%, per K10) that matched self-reported mental-health diagnosis (see Table 2). Note that more conservative cutoffs have been suggested to provide a much higher accuracy in classifying mental disorders (Furukawa et al., 2003). If we consider only participants in the categories of moderate or severe, which others have suggested optimizes clinical relevance in a six-item version of the same scale (Prochaska et al., 2012), 24.26% of our sample would have a likely mental disorder (for participant characteristics by likely mental-disorder classification, see the Supplemental Material). Rates of psychoticism and UBEs were aligned with those of community samples (Miller et al., 2022).
Mental-Health Characteristics
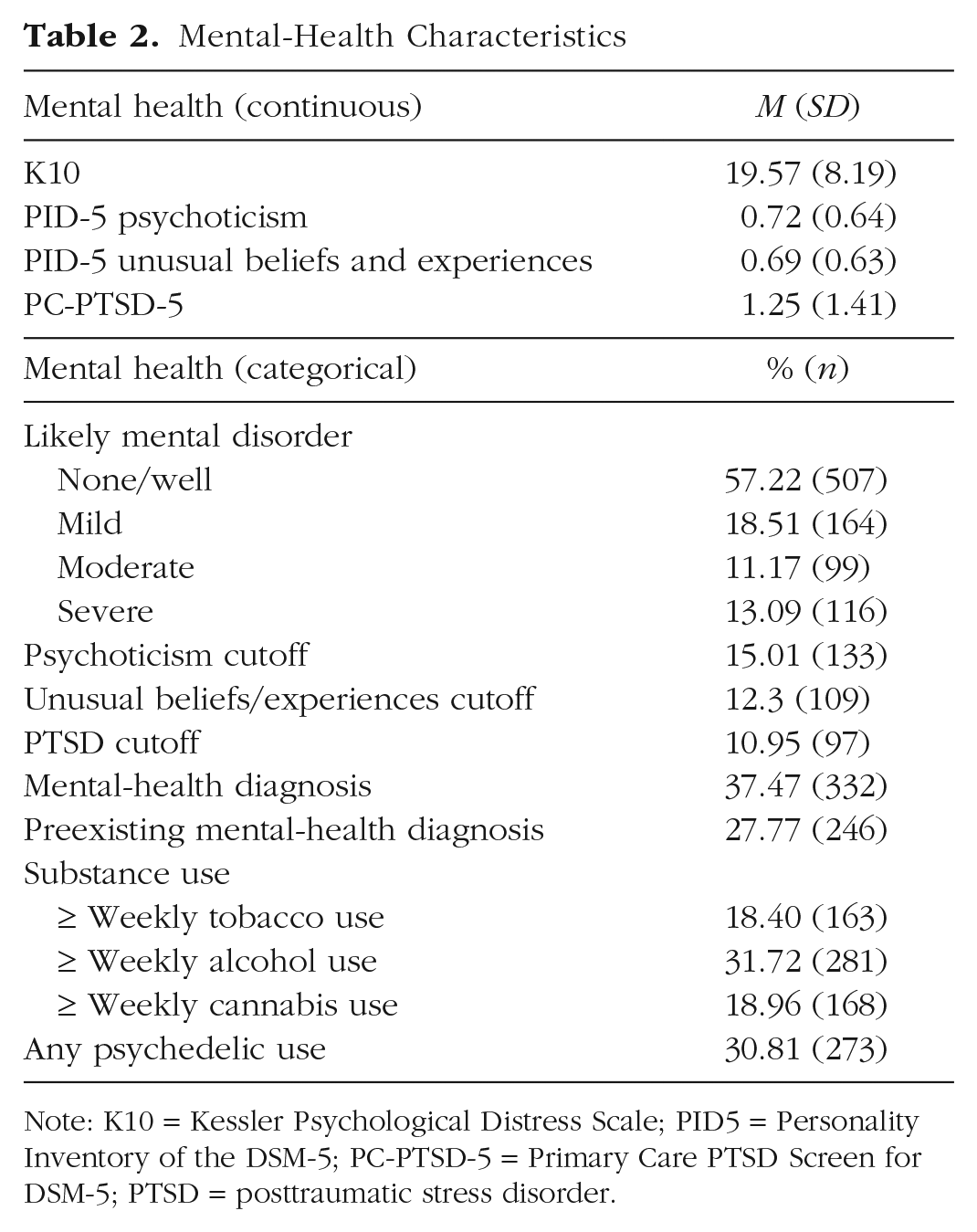
Note: K10 = Kessler Psychological Distress Scale; PID5 = Personality Inventory of the DSM-5; PC-PTSD-5 = Primary Care PTSD Screen for DSM-5; PTSD = posttraumatic stress disorder.
Meditation
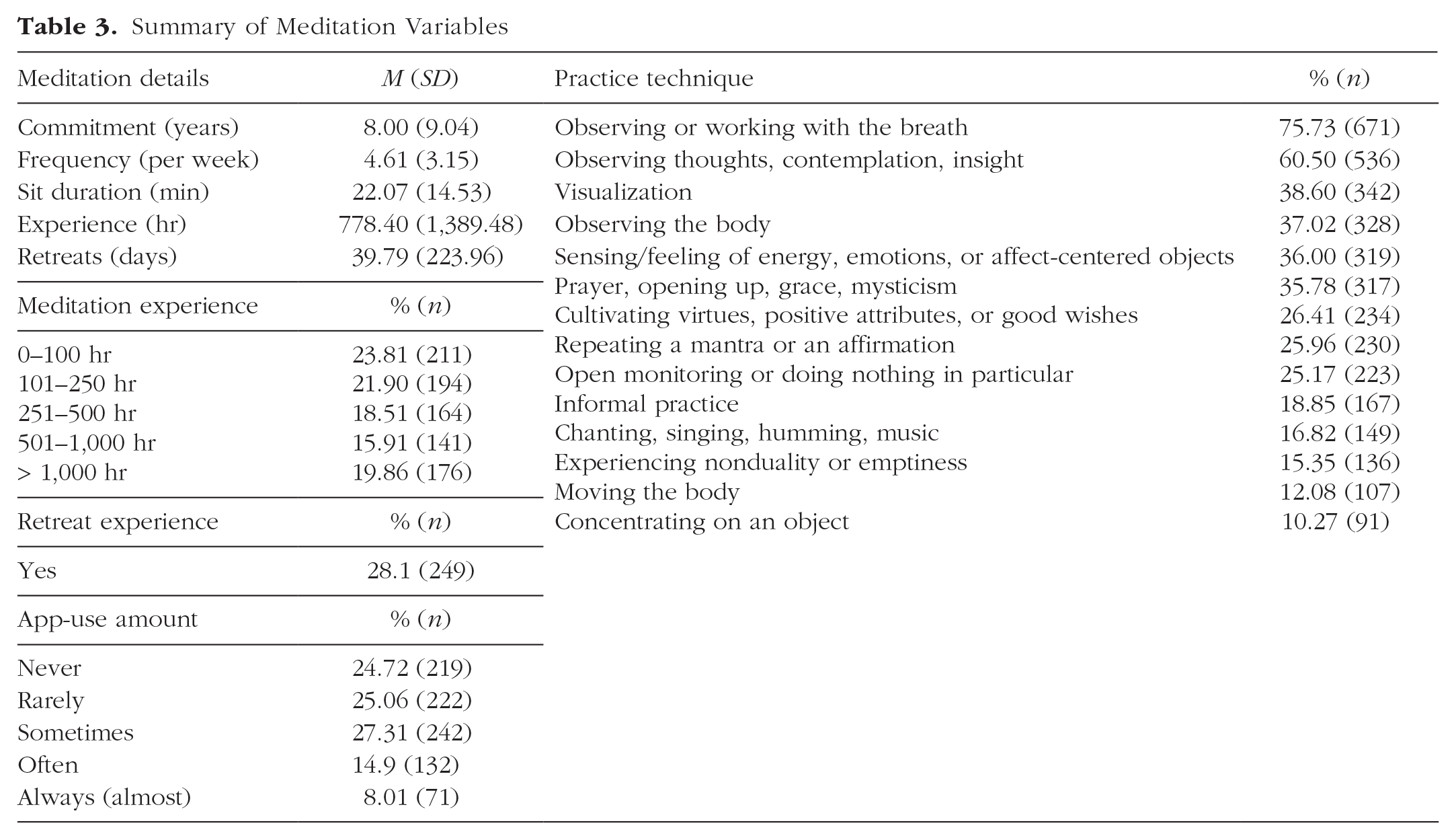
The sample comprised a majority of mindfulness meditators (52.71%), followed by spiritual meditators (35.10%) and mantra meditators (12.19%), which deviated from our targets but not recent data (Goldberg et al., 2022). Practice category and experience are reported in Table S1 in the Supplemental Material. For practice technique, see Table 3. Per estimated lifetime hours (i.e., the initial variable used for stratification), the sample reported a broad array of meditation experience: 38.37% were beginner, 38.83% were intermediate, and 22.80% were advanced practitioners. When using the detailed lifetime-hours estimate, the sample indicated 23.70% beginner practitioners, 56.43% intermediate practitioners, and 19.86% advanced practitioners. Assigned category (per estimated lifetime hours) and detailed lifetime-hours category were not significantly different, χ2(4) = 6.81, p = .146. For practice characteristics, see Table 3.
Summary of Meditation Variables
Incidence of unusual experiences
Inconsistent with our hypothesis (Hypothesis 1a), most participants (96.61%) experienced ≥ 1 unusual experiences, significantly higher than the previously reported rate of 88%, χ2(1) = 47.35, p < .001 (Vieten et al., 2018). Per Bayesian analyses, the 95% credible interval of the difference in posterior distributions was 0.064 to 0. 110, corresponding to a 99.99% probability of a substantial difference in the relative frequencies (0.01% probability of practical equivalence among the relative frequencies).
Incidence of AEs
Single-item generic question
Consistent with our preregistered hypothesis (Hypothesis 1b), the incidence rate of endorsing this item was 31.38%, which was not significantly different, χ2(1) = 0.07, p = .795, to the rate of 32.3% reported by Goldberg and colleagues (2022). Per Bayesian analyses, the 95% credible interval of the difference in posterior distributions was −0.062 to 0.043, corresponding to a 91.47% probability of practical equivalence among the relative frequencies (8.53% probability of a substantial difference in the relative frequencies). Among participants endorsing the generic AE question, 29.14% (n = 81; 9.14% of total sample) reported functional impairment. The percentage here (i.e., 9.14%) was not statistically different to the 10.6% rate previously reported, χ2(1) = 0.55, p = .457 (Goldberg et al., 2022). Among the subsample, 34 (12.23%) reported impairment lasting more than 1 day (3.84% of the overall sample); the proportion of the overall sample was statistically no different, χ2(1) = 2.64, p = .104, to the 5.99% reported by Goldberg et al.
MRAE
Inconsistent with our hypothesis (Hypothesis 1c), rates for endorsing at least one MRAES item (14 items; Britton et al., 2018) was 78.33%, which was significantly higher than the previously reported rate of 50%, χ2(1) = 108.01, p < .001 (Goldberg et al., 2022). Per Bayesian analyses, the 95% credible interval of the difference in posterior distributions was 0.230 to 0.340, corresponding to a > 99.99% probability of a substantial difference in the relative frequencies (< 0.1% probability of practical equivalence among the relative frequencies). Item-level incidence and scale incidence varied by intensity threshold (see Table S2 in the Supplemental Material).
Multiitem scale
Our hypothesis (Hypothesis 1d) of practical equivalence to previously reported incidence rates of AEs (50%) as defined by IME items was not supported. Of participants, 58.35% reported at least one AE as mildly unpleasant or worse (among 30 IME items), a significantly higher rate than the 50%, χ2(1) = 7.90, p = .005, of individuals endorsing any MRAE previously (Goldberg et al., 2022). Per Bayesian analyses, the 95% credible interval of the difference in posterior distributions was 0.026 to 0.140, corresponding to an 87.50% probability of a substantial difference in the relative frequencies (12.50% probability of practical equivalence among the relative frequencies). We considered the possibility that different intensity and unpleasantness thresholds might explain the variance in incidence rates using differing possible threshold combinations of the scale (see Table S3 in the Supplemental Material).
Predictors of unusual experiences and AEs
Sociodemographic variables
In robust multiple regression, only education was weakly positively associated with the endorsement of the generic AE question (see Table 4).
Robust Multiple Regression of Categorical Adverse Effects on Predictors in Full Sample (N = 886)
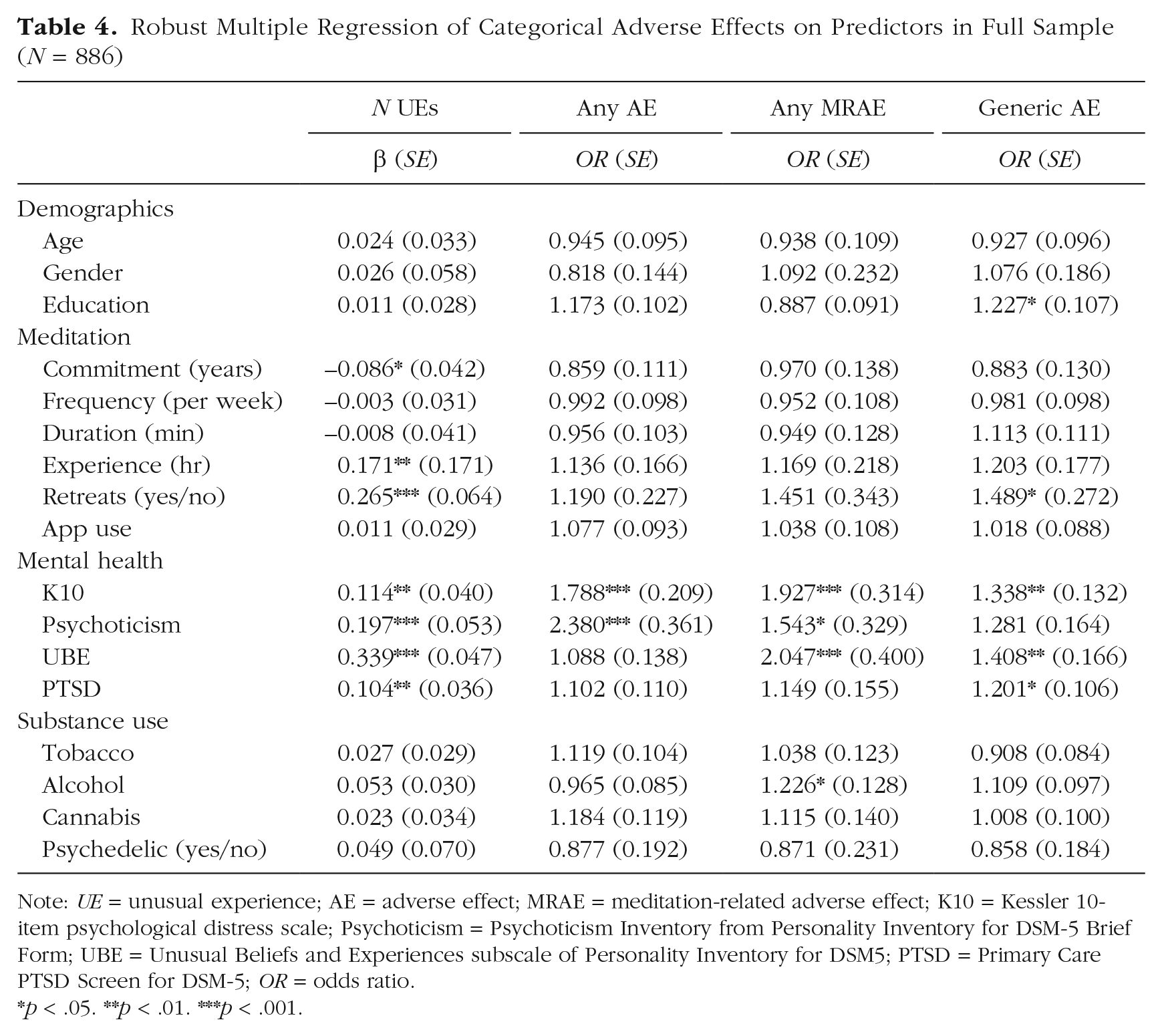
Note: UE = unusual experience; AE = adverse effect; MRAE = meditation-related adverse effect; K10 = Kessler 10-item psychological distress scale; Psychoticism = Psychoticism Inventory from Personality Inventory for DSM-5 Brief Form; UBE = Unusual Beliefs and Experiences subscale of Personality Inventory for DSM5; PTSD = Primary Care PTSD Screen for DSM-5; OR = odds ratio.
p < .05. **p < .01. ***p < .001.
Meditation variables
Consistent with our hypotheses, meditation experience and retreat attendance were significantly associated with unusual experiences (Hypothesis 2a). Inconsistent with our hypothesis (Hypothesis 2b), meditation experience was not robustly associated with AEs. Partially consistent with our hypothesis (Hypothesis 2b), meditation-retreat attendance was associated with the generic AE definition (see Table 4).
Mental-health and substance-use variables
Partially consistent with our hypotheses (Hypothesis 2a), the UBE scale was significantly associated with unusual experiences, whereas psychedelic use was not. Partially consistent with our hypotheses (Hypothesis 2a), psychological distress was robustly associated with all AE definitions, and UBE was associated with MRAE and generic AE definitions. Trauma was associated with the generic-AE definition. Psychedelic use was not associated with AE.
Post hoc examination of associations
Given prior work examining associations of various predictors with AEs (Goldberg et al., 2022), we computed zero-order associations and report the results alongside multiple regression results (see Table 5). Consistent with prior work, age was negatively associated with all definitions of AE and functional impairment and no longer significant when controlling for other variables. Years of practice but not lifetime-practice hours was significantly associated with AEs, in which prior data showed the opposite pattern (Goldberg et al., 2022). Neither variable was meaningful when controlling for other predictors. Note that in our data, lifetime-practice hours was significantly associated with functional impairment when accounting for other variables. Also departing from prior work, retreat experience was associated with AEs in our data. Retreat experience remained significant when controlling for other variables for two of our five AE definitions. Consistent with prior work, retreat experience was significantly associated with functional impairment. Finally, indicators of psychopathology were significantly associated with AEs and functional impairment, somewhat consistent with prior data. The association of psychopathology with functional impairment was no longer significant when controlling for other variables.
Standardized Zero-Order Association and Robust Multiple Regression Weights of Variables With Unusual and Adverse Effects
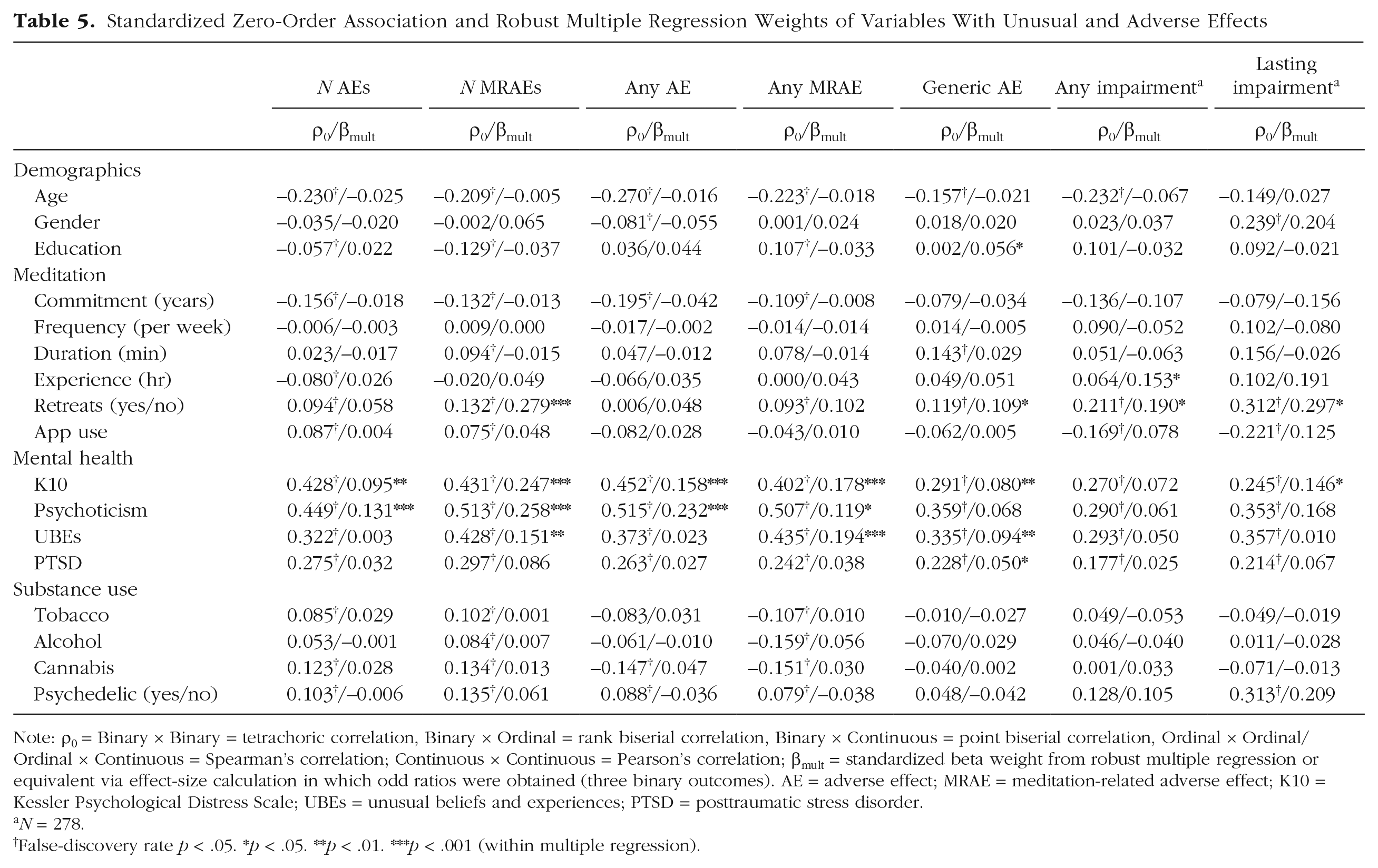
Note: = Binary × Binary = tetrachoric correlation, Binary × Ordinal = rank biserial correlation, Binary × Continuous = point biserial correlation, Ordinal × Ordinal/Ordinal × Continuous = Spearman’s correlation; Continuous × Continuous = Pearson’s correlation; = standardized beta weight from robust multiple regression or equivalent via effect-size calculation in which odd ratios were obtained (three binary outcomes). AE = adverse effect; MRAE = meditation-related adverse effect; K10 = Kessler Psychological Distress Scale; UBEs = unusual beliefs and experiences; PTSD = posttraumatic stress disorder.
N = 278.
False-discovery rate p < .05.
p < .05. **p < .01. ***p < .001 (within multiple regression).
Discussion
In this study, we report the assessment of unusual experiences and AEs in a large, representative sample of U.S. meditators who practice a variety of techniques with varying levels of experience. Surpassing high-incidence estimations in prior work (Vieten et al., 2018), unusual experiences occurred among almost every participant. Our analyses also indicated that the incidence of AEs exceeded common estimates (Farias et al., 2020; Pauly et al., 2022; Schlosser et al., 2019) and were similar to what recent work using similar methods has found (Britton et al., 2021; Goldberg et al., 2022): 58.4% of participants reported an AE per the IME (Van Dam et al., 2024), and 78.3% reported a clinically relevant symptom per the MRAES (Britton et al., 2018). Consistent with prior work that used generic single-item assessment (Cebolla et al., 2017; Pauly et al., 2022; Schlosser et al., 2019), 31.4% of participants endorsed a challenging, difficult, or distressing experience. Also consistent with prior work, the most reliable predictors of any unusual experiences or AEs were mental-health issues (Pauly et al., 2022). Again, consistent with some prior work (Schlosser et al., 2019), attendance at a residential meditation retreat was associated with endorsement of a single-item AE query and functional impairment. Psychopathology was robustly associated with AEs even when controlling for other variables. Our results provide an important indicator of the commonality of unusual experiences and AEs, indicators of how to improve assessment, and suggestions of who might be at greatest risk.
Varying definitions of AEs
We examined AEs in a number of different ways, including using the two definitions provided by the MRAES (Britton et al., 2018) and via the IME (Van Dam et al., 2024). Note that rates of an AE per IME items (58.4%) and modified MRAES items (78.3%) were both substantially higher than prior reports that used similar methodology (Goldberg et al., 2022) and well above prior reports that used generic single-item queries (e.g., Cebolla et al., 2017; Pauly et al., 2022; Schlosser et al., 2019). The rate of generic single-item query for AEs was consistent with work that used similar methods (31.4%; Goldberg et al., 2022) but somewhat higher than prior reports (e.g., Cebolla et al., 2017; Pauly et al., 2022; Schlosser et al., 2019). Prior work that examined AE reporting in general (Allen et al., 2018) and specifically in relation to meditation (Britton et al., 2021) suggests that symptom checklists are more sensitive than single-item queries. Data suggest that checklists remind participants of experiences that individuals may not otherwise have thought to report while also making the reporting process less effortful (Allen et al., 2013). In our analysis, the estimated rate per multiitem checklist was 86% higher than the rate estimated by single-item generic query. The discrepancies likely reflect that the MRAES checklist is composed of symptomatic experiences and has no valence threshold despite exhibiting variability in reported valence (see Van Dam et al., 2024), whereas an AE per the IME requires an intensity and a valence threshold. An additional consideration is that thresholds for endorsing yes/no items are known to be slightly higher than thresholds for moving a step on Likert-style response scales (see e.g., Batterham et al., 2018). Thus, present and previous results (Goldberg et al., 2022) are not necessarily at odds with one another but perhaps reflect different categories of experience that are increasingly serious. Indeed, only 9.14% of the total sample reported functional impairment, and only 6.6% reported strong-intensity experiences that were extremely unpleasant. Nonetheless, nearly 60% of individuals experienced AEs, and ≈10% experienced functional impairment. The incidence rates are significantly higher than meta-analytic estimates (8.3%; Farias et al., 2020) and large cross-sectional studies (≈25%; Cebolla et al., 2017; Pauly et al., 2022; Schlosser et al., 2019), but our primary definition of AEs is aligned with active multiitem assessment in clinical trials (Baer et al., 2021; Britton et al., 2021).
Functional impairment
Overall rates of functional impairment in prior studies are consistent with those estimated herein (9.14%). Baer and colleagues (2021) found that 12% of their sample described AEs as “quite a bit” or “extremely upsetting,” and Goldberg and colleagues (2022) observed that 10.6% of their sample reported functional impairment. Studies that have explicitly asked about lasting impact have found that participants are reluctant to indicate that meditation/mindfulness was harmful (≈5%; Baer et al., 2021) or that they were not glad that they had practiced (11.3%; Goldberg et al., 2022), although the former may be the result of participants trying to please the experimenters/teachers (see e.g., Britton et al., 2021). Still other studies have reported that participants who experience AEs may reappraise them as part of the therapeutic process (Hanssen et al., 2021). Although such an argument is not uncommon, we recommend caution; the adage that “it has to get worse before it gets better” has limited empirical support (see Lilienfeld, 2007). Moreover, individuals who experience AEs may discontinue the intervention/treatment before having an opportunity to “get better” (Klein et al., 2024). With 60.5 million Americans estimated to have engaged with meditation in 2022 (Davies et al., 2024), the possibility that ≈36.3 million people may be experiencing unexpected mild distress and ≈6.1 million of those people may be experiencing functional impairment warrants clear disclosure to practitioners and serious consideration among clinicians and researchers.
Establishing causality
A number of criteria are required to establish that a specific treatment/intervention has caused harm (see Britton et al., 2021). It is imperative to know whether the treatment has been correctly delivered; although a negative experience related to correct treatment is an AE, the same experience related to incorrect treatment is malpractice. Although mindfulness-based practices have established training protocols and ethical standards (e.g., Kenny et al., 2020), they are lacking for meditation more generally. This could be, in part, because meditation is often used in wellness settings, which do not have the same regulatory requirements as health settings. A direct result of the lack of guidelines is difficulty differentiating “correct” from “incorrect” treatment/instruction. Another issue is that individuals likely to use meditation may differ from the population in important ways that could put them at greater risk of problems in general and complications related to meditation specifically (see e.g., Davies et al., 2024). Multiple simultaneous lifestyle changes (of the kind associated with someone who may wish to take up meditation to address a problem) can make it difficult to tease out which change has led to harms and benefits. A specific outcome could be the result of meditation, some other change, or a combination of the two.
Despite these challenges, there is emerging evidence from randomized controlled trials that mindfulness meditation, even at mild doses such as those found in mindfulness-based stress-reduction courses, has a causal role in the incidence of unusual experiences, that is, altered states of consciousness consisting of disembodiment and unity experiences, for up to a year after randomization (Galante et al., 2024; Hanley et al., 2020). Moreover, meditation practice predicts spiritual, blissful, and unity experiences; insightfulness; disembodiment; and changed meanings in a dose-response fashion (Galante et al., 2024). Regarding AEs, best-practice examination of AEs in meditation suggests that there is a clear causal path to AEs (Britton et al., 2021). In any case, absence of evidence is not evidence of absence (Ioannidis et al., 2004), and the inability to disentangle causes contributing to AEs does not mean that providers need not warn practitioners about potential AEs or abstain from actively monitoring them.
Commonality of unusual experiences and AEs
Another important element to consider is when a potentially AE occurred and for how long it lasted. Estimates herein are related to lifetime experience of an unusual experience and/or AE in relation to meditation. The fact that such experiences may be common challenges the definition of these experiences. As noted in the introduction, it is important to distinguish between the percentage of the population that has ever experienced an unusual experience and/or AE and the percentage that experiences such events regularly or in a debilitating way. Because there is no commonly accepted duration that is associated with harm (Britton et al., 2021), it is important to be aware of any/all such experiences. Our estimates and those from prior work (Goldberg et al., 2022) suggest that as many as 10% of people may experience lasting negative effects. These effects, in particular, warrant further consideration. However, not all experiences are likely to be harmful or lead to lasting negative impact. It is possible that people who experience AEs may be able to reinterpret them (Hanssen et al., 2021) and/or come to view them as part of the process (Baer et al., 2021). However, acknowledging that such experiences are likely to occur (and better understanding for whom they are more likely to occur) is a critical part of informed consent and will help the field to follow best practice.
Predictors of AEs
Consistent with previous work (Goldberg et al., 2022; Pauly et al., 2022), mental-health symptoms/psychological distress during the past 30 days was the single most robust predictor of unusual events and adverse experiences. Personality tendencies toward psychoticism and unusual beliefs/experiences were among the second most robust predictors. It is not possible to differentiate whether mental-health symptoms/characteristics were a risk factor for AEs or a result of meditation-related AEs. In other words, it is possible that preexisting mental-health problems are a vulnerability for meditation-related AEs (see e.g., Pauly et al., 2022) and also that mental health worsens as a result of experiencing meditation-related AEs. Further prospective longitudinal work is needed to gain more insights into any potential causal relationships between these variables. Minimally, our findings lend credence to traditional warnings that meditation may be contraindicated for those with mental-health presentations unless delivered in a structured and supported way (Dobkin et al., 2012). Our findings also highlight the critical importance of monitoring for AEs for everyone in meditation programs, especially among individual who have mental-health issues, regardless of whether the programs are designed to address those issues.
Of additional note and consistent with some prior work (Lindahl et al., 2017; Schlosser et al., 2019), the most robust predictor of functional impairment was residential-retreat attendance, which was positively associated with AEs. The nature of our data means that we cannot specifically speak to the setting or configuration of retreats among our participants. Discussion of “set and setting”—a term typically associated with drug effects (Hartogsohn, 2017)—has started to gather momentum in meditation research (see e.g., Lindahl et al., 2021). More research is needed to understand what types of retreats are conducive to maximizing potential benefits and minimizing potential harms associated with meditation.
Beginning meditators may discontinue because of AEs
One particularly important note is that discrepant findings herein pertaining to rates of AEs and associations of AEs may reflect sample characteristics. Prior studies of meditators using large samples have estimated rates of AEs on the order of 25% (Cebolla et al., 2017; Pauly et al., 2022; Schlosser et al., 2019). Those studies have typically focused on individuals with an established meditation practice, as indicated by relatively high rates of regular practice and participation in meditation retreats. In contrast, the recent work by Goldberg and colleagues (2022) estimated an AE rate of 50%, but their sample largely comprised beginning meditators (majority of participants had fewer than 100 hr of practice, and very few attended a residential retreat). Our study enrolled a sample that was more representative of the population of U.S. meditators, capturing a range of practice type and experience levels. Note that years of practice showed negative zero-order correlations with several definitions of AE. Although these effects largely disappeared in multiple regressions, the result may suggest discontinuation of practice among beginning meditators who have AEs or fail to experience improvement. Only longitudinal work will be able to fully address this question.
Limitations and future directions
The method used to acquire our sample (online platform) is a limitation in that it may have biased our sample in ways that make it different to a broader population of meditators. Furthermore, our analyses were cross-sectional, limiting the ability to make any causal conclusions. The inability to make causal attributions is somewhat concerning because there are many factors contributing to unwanted treatment effects (Schermuly-Haupt et al., 2018). In addition, our sample comprised a very broad variety of meditation types—which is both a strength and a weakness. Our lack of ability to verify the type of practice undertaken (especially when it comes to retreats) means we cannot know definitively whether any particular type of meditation is more prone to result in AEs than any other (although for consideration of techniques associated with AEs, see Supplemental Material). However, the breadth of practice types means that we were able to estimate an incidence rate that is analogous to the broad array of meditative practices within the United States in particular. We also cannot say whether AEs are more or less common based on the set and setting of the practice. It is plausible that some practice types are more likely to lead to AEs than others or that AEs are relatively comparable but that having the support of a skilled teacher/instructor leads one to being able to manage any AEs and potentially even find a way to learn from them. We also note that our choice of measures for psychosis-proneness and unusual beliefs meant that we assessed these constructs more in relation to mental health than personality; assessing these constructs in alignment with broad personality tendencies (e.g., Farias et al., 2005) may have resulted in different associations to experiences.
Despite the limitations of the current work, the study has critical implications for unusual experiences and AEs in meditation. Meditation is commonly used to address mental-health concerns and indeed is used almost as commonly as mental-health services in the United States (Davies et al., 2024). Accordingly, rates of MRAEs (58.35% herein) are in line with the best available estimates for psychotherapy: 57.8% have reported at least one negative experience (i.e., resurfacing of unpleasant memories; Strauss et al., 2021), whereas 5.2% reported a lasting bad effect (Crawford et al., 2016; compared with 3.84% of meditators). Note, however, that people who pursue psychotherapy typically do so with the aim of managing their mental health and professional codes of ethics require informed consent. Because meditation is offered by a variety of individuals/organizations across a variety of unregulated settings, it is unclear to what extent people are informed of the possibility of unusual experiences and/or AEs. Given huge increases in the uptake of meditation (Davies et al., 2024), it is essential that more information is available to providers and consumers regarding potential benefits and harms such that they can make an informed choice regarding risk-benefit ratios.
Because meditation training programs are increasingly used to manage mental illness and/or promote mental health, it is also critical that the field better understand the relationship between preexisting vulnerabilities that may be exacerbated by meditation, factors that may relate to the onset of new problems, the number of individuals for whom deterioration may occur, and a host of other ways of consider potential harms (see e.g., Britton et al., 2021). A major first step is to synchronize the way in which harms are assessed and to ensure there is direct and structured assessment, especially in clinical trials of meditation. Although evidence increasingly suggests that structured meditation training programs may be helpful on average, so too, the evidence is clear that it will not be helpful for all and may even be harmful for some.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026241298269 – Supplemental material for Incidence and Predictors of Meditation-Related Unusual Experiences and Adverse Effects in a Representative Sample of Meditators in the United States
Supplemental material, sj-docx-1-cpx-10.1177_21677026241298269 for Incidence and Predictors of Meditation-Related Unusual Experiences and Adverse Effects in a Representative Sample of Meditators in the United States by Nicholas T. Van Dam, Jessica Targett, Jonathan N. Davies, Alex Burger and Julieta Galante in Clinical Psychological Science
Footnotes
Transparency
Action Editor: Vina Goghari
Editor: Jennifer L. Tackett
Author Contributions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.