
Abstract
More comprehensive modeling of psychopathology in youth is needed to facilitate a developmentally informed expansion of the Hierarchical Taxonomy of Psychopathology (HiTOP) model. In this study, we examined a symptom-level model of the structure of psychopathology in children and adolescents—most aged 11 to 17 years—bringing together data from large clinical, community, and representative samples (N = 18,290) covering nearly all major forms of mental disorders and related content domains (e.g., aggression). The resulting hierarchical and dimensional model was based on the points of convergence among three statistical approaches and included 15 narrow dimensions nested under four broad dimensions of (a) internalizing, (b) externalizing, (c) eating pathology, and (d) uncontrollable worry, obsessions, and compulsions. We position these findings within the context of the existing literature and articulate implications for future research. Ultimately, these findings add to the rapidly growing literature on the structure of psychopathology in youth and move a step closer toward quantifying (dis)continuities in psychopathology’s structure across the life span.
Understanding and accurately classifying psychopathology is a fundamental challenge in the field of mental health. In particular, there is a growing body of research on the development of alternatives to traditional categorical diagnostic systems such as the Diagnostic and Statistical Manual of Mental Disorders (DSM) and the International Classification of Diseases (ICD). One such alternative is the Hierarchical Taxonomy of Psychopathology (HiTOP; Kotov et al., 2017), a model of broad and narrow dimensions of psychopathology organized in a hierarchical framework (see Fig. 1a) based on patterns of covariation among individuals’ experiences of symptoms and syndromes. HiTOP dimensions aim to provide a more nuanced and dimensional depiction of psychopathology compared with the DSM and ICD, allowing for the examination of both shared and distinct features across a broad range of phenomena.
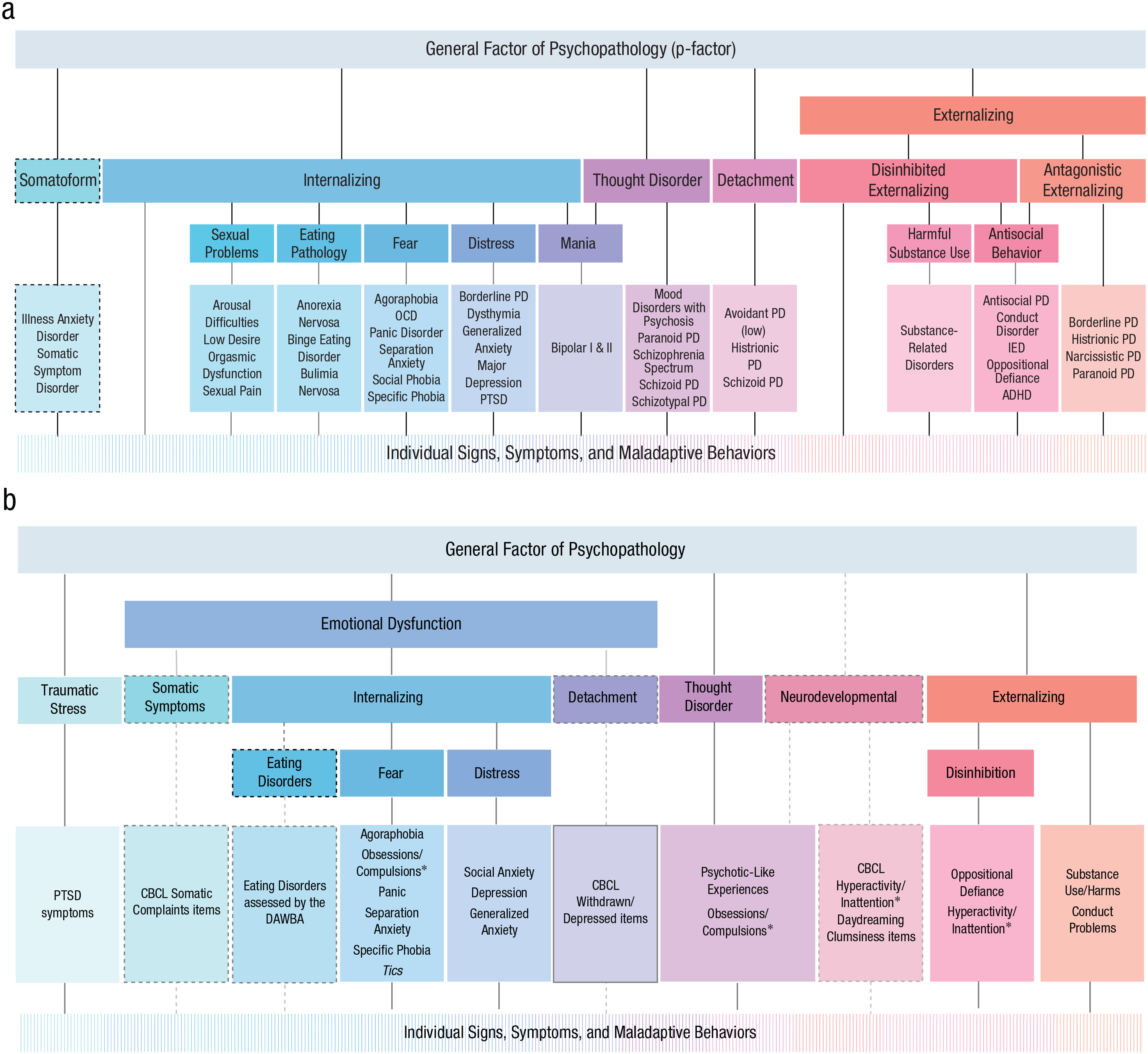
(a) An adaptation of the Hierarchical Taxonomy of Psychopathology (see https://osf.io/rscqf), emphasizing the placement of disorders and related constructs in the adult-psychopathology literature. Dashed lines indicate dimensions or relationships included as provisional aspects of the framework. (b) A hierarchical model summarizing the literature reviewed here on the structure of psychopathology in youth. Dashed lines indicate constructs included based on evidence from only a single study (specific measures used in the relevant study are listed for these constructs), and “Tics” is in italics for the same reason; other elements were evident in two or more studies. Obsessions/compulsions and hyperactivity/inattention are marked with an asterisk to highlight that they are listed twice in the figure. ADHD = attention-deficit/hyperactivity disorder; CBCL = Child Behaviour Checklist; DAWBA = Development and Wellbeing Assessment; IED = intermittent explosive disorder; OCD = obsessive compulsive disorder; PD = personality disorder; PTSD = posttraumatic stress disorder.
At the core of the HiTOP model are the internalizing and externalizing dimensions, which were studied long before HiTOP, beginning with the trailblazing research on empirically derived models of youth psychopathology (Achenbach, 1966). Achenbach and colleagues’ body of research in youth populations formed the foundation on which the HiTOP framework was built (e.g., Krueger, 1999). Nevertheless, the predominant focus in HiTOP on the classification of adult psychopathology has led to a disconnect with the youth-psychopathology literature despite clear parallels and some evidence for continuity in the structures that emerge across the life span (e.g., Forbes et al., 2016; Tackett & Hallquist, 2022). Indeed, beyond internalizing and externalizing, less is known about the metastructure of psychopathology in youth. Tackett and Hallquist (2022) recently called for developmental taxonomic work, particularly on more comprehensive models of psychopathology in youth, to facilitate a developmentally informed expansion of HiTOP as a path to more productive research on the etiology and course of mental illness. This goal is particularly important in the context of the rising prevalence of mental disorders in young people (e.g., Australian Bureau of Statistics, 2020–2021) and slow progress in improving treatment outcomes (e.g., Jorm et al., 2017).
Existing research through a HiTOP lens in youth usually relies on confirmatory factor analyses (CFAs) of internalizing and externalizing disorders (e.g., Etkin et al., 2020; Guy et al., 2022)—many alongside a general factor of psychopathology (or “p factor” in Caspi et al., 2014; e.g., Avinun et al., 2022; Choate et al., 2023; Mann et al., 2020)—and often adopts DSM-defined constructs (e.g., Mann et al., 2020; Vine et al., 2020). These types of studies have typically found dimensions of internalizing and externalizing and a general factor of psychopathology that align with findings in adult samples, but new approaches to provide stronger tests of the HiTOP structure are needed. For example, a subset of studies has used exploratory analyses, modeled individual items (as opposed to items bound within subscales or disorders), and/or included broader content coverage of psychopathology phenomena beyond internalizing and externalizing. Each of these approaches deepens the understanding of the structure of psychopathology in youth because they allow the resulting model to depart from prespecified subscale or disorder domains and flesh out associations that go beyond the core internalizing and externalizing dimensions. We turn now to review studies that have taken these approaches to modeling the dimensional structure of psychopathology in youth; Figure 1b shows a summary of how these results fit together into an overarching structure.
Exploratory, Item-Level, and/or Broad Content Coverage Studies
In early work, Lahey et al. (2004) conducted exploratory factor analyses of items designed to assess symptoms of a variety of diagnoses in children and adolescents aged 4 to 17 years based on the fourth edition of the DSM. They found a tiered, hierarchical structure that contained an internalizing dimension with narrower fear and distress dimensions nested under it and an externalizing dimension with narrower conduct problems, oppositional defiance, hyperactivity, and inattention dimensions nested under it (see also Lahey et al., 2008). Analyses of broader item sets have identified additional dimensions. For example, in their exploratory factor analyses of items on the Child Behavior Checklist (CBCL) in children aged 9 to 10 years, Michelini et al. (2019) found that the single factor at the top of the hierarchy split into (a) a broad internalizing dimension that comprised narrower dimensions that reflected somatic symptoms, detachment, and a narrower internalizing dimension (e.g., fears, worries, guilt, and a negative self-concept); (b) an externalizing dimension; and (c) a neurodevelopmental dimension that largely comprised attention-deficit/hyperactivity disorder (ADHD) symptoms—hyperactivity, impulsivity, inattention—with some representation of other symptoms reflecting obsessions and compulsions, strange ideas and behavior, and related behaviors (e.g., clumsiness). A CFA of a similar CBCL item set in clinically referred children and adolescents age 4 to 18 years included a similar broad internalizing dimension (labeled “emotional dysfunction” in the HiTOP literature; Watson et al., 2022) that comprised somatic, detachment, and core internalizing items—as well as dimensions of externalizing, thought problems, attention problems, and a general factor of psychopathology (Haltigan et al., 2018). In contrast with Michelini et al., Haltigan et al. (2018) assigned the attention problems and thought problems scales on an a priori basis (see Ivanova et al., 2015) to separate factors reflecting their namesakes, precluding their assembly into a neurodevelopmental dimension as in Michelini et al.
In addition, several studies have supported a thought-disorder dimension as distinct from internalizing and externalizing in youth. Laceulle et al. (2015) used CFA to model subscales from a variety of self-report measures in high school students. Along with a general factor of psychopathology and narrower factors of internalizing and externalizing, they found a thought-disorder dimension that comprised obsessions, compulsions, and psychotic-like experiences. This combination of obsessions, compulsions, and psychotic-like experiences forming a thought-disorder dimension was replicated in St Clair et al. (2017) and is similar to the thought-disorder dimension in He and Li (2021) that comprised DSM diagnoses of obsessive compulsive disorder (OCD) and psychosis together with manic episodes. Other confirmatory item-level analyses in youth have also found internalizing, externalizing, and thought-disorder (or psychotic-like experiences) dimensions along with general factors of psychopathology (Afzali et al., 2018; Carragher et al., 2016; Sunderland et al., 2021).
Adding to the breadth of coverage of these studies, Lynch et al. (2024) included measures of alcohol use and alcohol-related harms. Their confirmatory item-level analyses found four narrower dimensions of fear, distress, alcohol use and harms, and conduct problems under a higher-order general factor of psychopathology. Two studies also found some evidence for an independent traumatic-stress dimension capturing responses to trauma (Haahr-Pedersen et al., 2024; Hyland et al., 2022). Finally, confirmatory studies of DSM-defined constructs have included additional constructs, such as substance use aside from alcohol use under externalizing (Castellanos-Ryan et al., 2016; Sunderland et al., 2021), eating pathology under internalizing (Castellanos-Ryan et al., 2016), and vocal and motor tics under internalizing (Watts et al., 2019).
Together, each of these studies has contributed to the understanding of an overarching structure of psychopathology in youth, and a summary of how these results fit together (Fig. 1b) closely resembles the organization of the HiTOP model (Fig. 1a). However, each piece of this puzzle is based on a relatively narrow sampling of domains of psychopathology, which limits confidence in the overarching structure because each set of results is inherently bound to and limited by the pool of constructs being analyzed. For example, if there are no core indicators of thought disorder in a study (e.g., psychotic-like experiences), then other symptoms that may be related to thought disorder do not have the option to adhere to that construct. For example, in Watts et al. (2019), vocal and motor tics had only internalizing and externalizing spectra as potential higher-order constructs to load on, which does not provide a strong test of where vocal and motor tics might belong when the full breadth of psychopathology is modeled. Modeling sufficiently diverse markers of psychopathology simultaneously may well lead to substantial differences in the structure by providing the opportunity to test for convergence, divergence, and cross-loadings of items in each of the dimensions that emerge. From a HiTOP perspective, the strongest evidence that can come from a single study for adding to or changing the official model will come from a latent-variable approach in a large sample with sufficient breadth of measurement to capture the constructs of interest (Forbes et al., 2024).
The Present Study
Thus, in the present study, we adopted an exploratory, symptom-level approach to elucidating a hierarchical and dimensional structure of psychopathology in youth, harmonizing data across six samples—spanning large clinical, community, and representative samples of children and adolescents—that assess numerous common and uncommon symptom domains. This approach affords greater breadth of content coverage than any existing study, including more than double the maximum number of items included in other studies and more than double the maximum sample size. Analyzing these data can therefore provide a useful step forward in the understanding of the structure of psychopathology in youth and toward a revision of the HiTOP model that applies across the life span (Tackett & Hallquist, 2022).
Transparency and Openness
These analyses were exploratory, based on analyses of existing data rather than new data collection, and were not preregistered. A preregistered analytic plan failed spectacularly in just about every way possible but is available at https://osf.io/5ptsn/. For a full account of the planned, attempted, and failed analyses along with full details on coding, cleaning, and merging of data sets, see the Supplemental Material available online. The data in the form of the observed and model-implied pooled correlation matrices are also available at https://osf.io/5ptsn/. All primary studies received ethics approval from one or more Australian human research ethics bodies and were conducted in accordance with the World Medical Association Declaration of Helsinki (World Medical Association, 2013).
Method
Participants
We harmonized self-reported symptoms of psychopathology across six samples of children and adolescents, including participants from four high school cohorts, a nationally representative cohort, and a treatment-seeking sample, with a requirement of at least one valid response in the item set to be included in the analyses (N = 18,290; for an overview of the sample demographics, see Table 1). Note that in Australia, high school spans Grades 7 through 12.
Overview of Demographics for the Six Subsamples and Total Sample (N = 18,290)
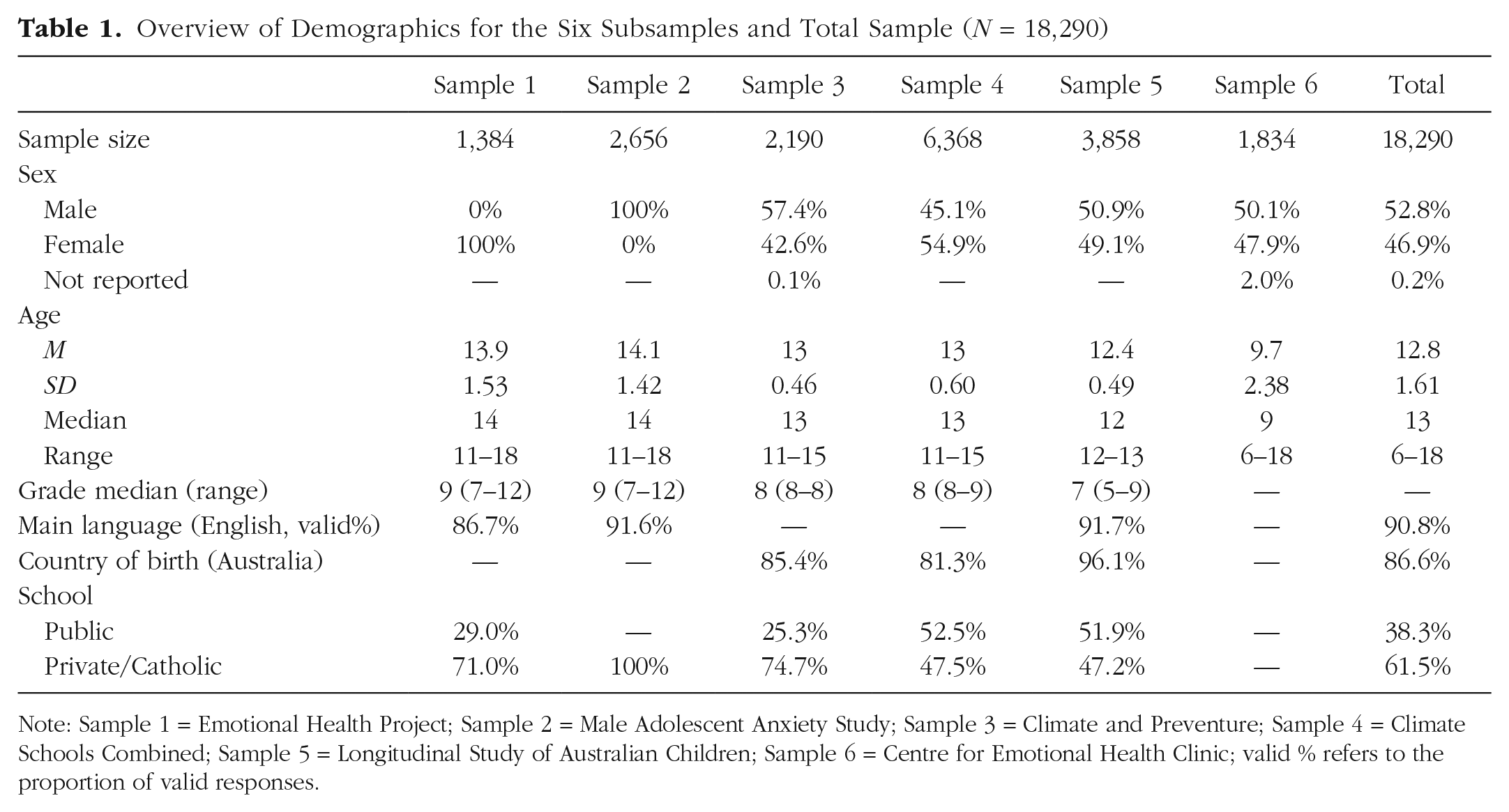
Note: Sample 1 = Emotional Health Project; Sample 2 = Male Adolescent Anxiety Study; Sample 3 = Climate and Preventure; Sample 4 = Climate Schools Combined; Sample 5 = Longitudinal Study of Australian Children; Sample 6 = Centre for Emotional Health Clinic; valid % refers to the proportion of valid responses.
The Emotional Health Project (Sample 1; e.g., Schneider et al., 2017) included participants (n = 1,384) recruited from two independent girls’ high schools in Sydney, Australia. The study was approved by Macquarie University Human Research Ethics Committee and the New South Wales Department of Education and Training. Passive consent was obtained from parents of study children in Years 7 to 10 and from study children directly for children in Years 11 and 12. All study children also provided verbal consent. The schools participated in a larger longitudinal study of the development and prevention of anxiety and depression in adolescent girls, which included a universal intervention and up to nine waves of data collection over 5 years. Data included here are drawn from baseline assessment of symptoms of psychopathology.
The Male Adolescent Anxiety Study (Sample 2; e.g., Schneider et al., 2017) included participants (n = 2,656) recruited from four Catholic boys’ high schools in Sydney, Australia. The study was approved by Macquarie University Human Research Ethics Committee, Sydney Catholic Education Office, and Armidale Catholic Schools Office. Like for Sample 1, passive consent was obtained from parents of study children in Years 7 to 10 and from study children directly for children in Years 11 and 12. All study children also provided verbal consent. Students participated in a larger longitudinal study composed of up to four waves of data collection over 10 months. This study included a universal program aimed at increasing help seeking and decreasing stigma for anxiety. Data included here are drawn from baseline assessments of symptoms of psychopathology.
The Climate and Preventure study (Sample 3; Newton et al., 2012) included participants (n = 2,190) from 26 Australian high schools, beginning in 2012 and following students for 7 years. The study was approved by the New South Wales, Queensland and Western Australian Departments of Education and Training, Curtin University, Queensland University of Technology Human Research Ethics Committee, University of Sydney, and University of New South Wales. All parents and children provided written consent. Schools in the study were randomly assigned to receive a universal substance-use intervention, a selective substance-use intervention for high-risk students, both interventions, or health education as usual. Data included here are from the baseline assessment of students’ self-reported psychopathology and substance use.
The CLIMATE Schools Combined study (Sample 4; Teesson et al., 2014) included participants (n = 6,368) from 71 Australian high schools, beginning in 2014 and following students for 7 years. The study was approved by the University of New South Wales Human Ethics Committee, Sydney Catholic Education Office, and New South Wales Department of Education and Training. All parents and children provided written consent. Schools in the study were randomly assigned to receive a universal substance-use-prevention intervention, a universal mental-health-prevention intervention, both interventions, or health education as usual. Data included here are from the baseline assessment of students’ self-reported psychopathology and substance use.
The Longitudinal Study of Australian Children (Sample 5; Soloff et al., 2005) is a nationally representative longitudinal cohort study of Australian children led by the Australian Institute of Family Studies to track children’s development. The study was approved by the Australian Institute of Family Studies Ethics Committee, and all parents and children provided written consent. The study commenced in 2004 and follows two cohorts of 5,000 children with data collection every 2 years. Data included in the present study are drawn from the child self-report interview and audio computer-assisted self-interview, drawing from the participants in the older cohort of children at Wave 5 (n = 3,858; 79.4% retention from baseline).
A clinical sample of participants was drawn from intake assessments of participants completing outpatient or online treatments (n = 1,834) at the Centre for Emotional Health Clinic at Macquarie University, Sydney, Australia, from 2000 to 2022 (Sample 6; e.g., Hudson et al., 2009, 2013, 2023; McLellan et al., 2024; Rapee et al., 2013, 2017, 2022; Schniering et al., 2022). Data collection was approved by the Macquarie University Human Research Ethics Committee, all parents provided written consent, and children provided written or verbal consent. During the initial screening, participants were required to report anxiety in at least one situation before progressing to the next stages of assessment. Data included here are from the questionnaires completed before the diagnostic interview and any subsequent treatment.
Measures
Each of the studies assessed a broader variety of constructs than those being analyzed here and were not conducted to fulfill the aims of the present study. The measures in each study were subset here to focus on self-reported symptoms of psychopathology, excluding measures of other domains (e.g., knowledge and attitudes about alcohol, self-efficacy, peer pressure, metacognitions, adaptive coping). The final data set contained 288 symptoms that altogether measured 254 symptom constructs spanning common and uncommon psychopathology, including distress, depression, hopelessness, specific worries, generalized anxiety, separation anxiety, panic, agoraphobia, physical-injury fears, social anxiety, obsessions and compulsions, hallucinatory experiences and delusional beliefs, eating pathology, body image, impulsivity, anger, aggression, bullying behaviors, antisocial behaviors, alcohol use and harms, other substance use, and other general symptoms of psychopathology (e.g., trouble sleeping or paying attention, withdrawal, and avoidance). For the measures included in each sample and the items assessed in each sample, with the respective sample size for each item, see Tables S1a and S1b in the Supplemental Material. We include a brief summary of the measures here.
Distress
The six-item Kessler Psychological Distress scale assesses global, nonspecific psychological distress in the past 4 weeks, drawing from depressive and anxiety-related symptoms (e.g., “nervous?”; Kessler et al., 2010). Items were rated on a frequency scale from none of the time (0) to all of the time (4). Furthermore, we included 19 items from the item pool used to develop the Brief Emotional Distress Scale for Youth (Spence & Rapee, 2022; e.g., “I feel really alone”) that were nonoverlapping with the Spence Children’s Anxiety Scale (included as indices of anxiety below). These items were rated on a frequency scale from never (0) to always (3).
Depression
The 13-item Short Mood and Feelings Questionnaire (Angold et al., 1995) assesses the severity of depressive symptoms over the past 2 weeks (e.g., “I felt miserable or unhappy”). Items were rated on a severity scale from not true (0) to true (2). The eight-item Patient Health Questionnaire (Johnson et al., 2002) also assessed frequency of depression symptoms over the past 2 weeks (e.g., “Feeling down, depressed, irritable or hopeless”). Items were rated from not at all (0) to nearly every day (3). Finally, the Depression subscale of the Brief Symptom Inventory (Derogatis, 1993) assessed frequency of depression symptoms over the past 6 months (e.g., “Feeling hopeless about the future”), which were rated from not at all (0) to often (4).
Worry
Twelve items from the Penn State Worry Questionnaire for Children (Chorpita et al., 1997) were included to assess self-reported excessive and uncontrollable worry (e.g., “My worries really bother me”) and rated from not at all true (0) to always true (3). A list of 10 specific worries adapted from the Children’s Worries and Concerns Scale (Tucci et al., 2007) were also assessed (e.g., “How worried are you about the environment?”) and rated from not at all worried (1) to very worried (4).
Anxiety
The 38 items from the Spence Children’s Anxiety Scale (Spence, 1998) that assess frequency of anxiety symptoms (e.g., “I feel scared if I have to sleep on my own”) were rated from never (0) to always (3). This measure includes items that span social anxiety, separation anxiety, generalized anxiety, panic, agoraphobia, obsessions and compulsions, and physical-injury-related anxiety. The three-item Mini-Social Phobia Inventory (Connor et al., 2001) was included to assess social anxiety (e.g., “I avoid activities). Items were rated from not at all (0) to extremely (4). Furthermore, the Generalized Anxiety Disorder 7-item scale (Spitzer et al., 2006) assessed symptoms of generalized anxiety over the past 2 weeks (e.g., “Feeling nervous, anxious, or on edge”) that were rated from not at all (0) to nearly every day (3). Finally, the anxiety subscale of the Brief Symptom Inventory (Derogatis, 1993) was assessed over the past 6 months (e.g., “spells of terror or panic”); items were rated from not at all (0) to often (4).
Obsessions and compulsions
The 22 items assessing symptoms of obsessions and compulsions from the Child Obsessive Compulsive Inventory (Shafran et al., 2003) were included to assess severity of symptoms (e.g., “I spend far too much time washing my hands over and over again” and “I can’t stop thinking upsetting thoughts about an accident”), rated from not at all (0) to a lot (2).
Hallucinatory experiences and delusional beliefs
Nine questions that assessed hallucinatory experiences and delusional beliefs over the past 6 months (e.g., “Have other people ever read your thoughts?”), adapted in part from the Diagnostic Interview Schedule (Costello et al., 1982), were rated from not true (0) to certainly true (2).
Eating pathology
The child version of the 26-item Eating Attitudes Test (Maloney et al., 1988) assessed disordered-eating attitudes and behaviors (e.g., “I vomit after I have eaten”). Items were rated from never (0) to always (6).
Body-image concerns
A screening question from the Body Dysmorphic Disorder Questionnaire–Adolescents (Phillips, 2005) was included, asking “Are you very worried about how you look?,” with a yes/no (1/0) response option.
Impulsivity
The five-item impulsivity scale of the Substance Use Risk Profile Scale (Woicik et al., 2009) was included (e.g., “I usually act without stopping to think”); items were rated from strongly disagree (0) to strongly agree (3).
Anger
Ten items from the Multidimensional School Anger Inventory (Furlong et al., 2002) assessed frequency of destructive experiences of anger at school (e.g., “If I get mad, I’ll throw a tantrum”). Items were rated on a 4-point Likert scale from never (0) to always (3).
Aggression and bullying
The 23-item Reactive-Proactive Aggression Questionnaire (Raine et al., 2006) assessed frequency of both reactive and proactive aggression in the past 6 months (e.g., “Yelled at others when they have annoyed you” and “Hurt others to win a game,” respectively); items were rated from never (0) to often (2). Furthermore, the eight cyberbullying items from the Online Friends Cyberbullying measure (Leung & McBride-Chang, 2013) were included to assess cyberbullying behaviors over the past 3 months (e.g., “I gossip or say mean things about others in online games/on the internet”). Items were rated from strongly disagree (1) to strongly agree (5). Finally, four items from the Revised Olweus Bully/Victim Scale (Olweus, 1996) measuring frequency of bullying perpetration in the past 6 six months (e.g., “I kicked, pushed, shoved, or locked another student indoors”) were rated from none (0) to several times a week (4).
Antisocial behavior
A list of 17 antisocial behaviors (e.g., “In the last 12 months have you stolen something from a shop?”) was adapted from the Self-Report Delinquency Scale (Moffitt & Silva, 1988), and frequency of behaviors was rated over the past 12 months from not at all (0) to five or more times (5).
Patterns of alcohol use
Items assessing quantity and frequency of alcohol use over the past 6 or 12 months, depending on the sample (e.g., “How often did you have a standard alcoholic drink of any kind in the past 6 months?”), were adapted from McBride et al. (2004) and rated from never (0) to daily or almost daily (6). Other items assessing alcohol use included questions about quantity of alcohol consumption (e.g., number of alcohol drinks in the past week) and asking binary yes (1) or no (0) questions about alcohol use.
Alcohol-related consequences and alcohol use disorder
An alcohol and lifestyle questionnaire included eight items from the Rutgers Alcohol Problems Index (RAPI; White & Labouvie, 1989) that assessed alcohol-related consequences common among adolescents over the past 6 months (e.g., “How many times have you got into fights, or acted bad or did mean thing as a consequence of drinking alcohol?”). Items were rated on a 5-point scale from never (0) to more than 10 times (4). Furthermore, 51 items adapted from the Diagnostic Interview Schedule for Children (DISC; Shaffer et al., 2000) were included to assess past-year alcohol use disorder (e.g., “Did you spend a lot of time drinking?” and “When you didn’t drink or when you cut down in the last year, did you feel bad or feel sick?”). Items were rated on a yes (1)/no (0) scale. Because of low endorsement rates, RAPI items were collapsed into a single maximum score on alcohol-related harms (RAPI) variable, and DISC items were collapsed into a single any alcohol use disorder symptoms (DISC) variable, as described below.
Patterns of other substance use
We included seven items assessing use of cannabis, tobacco, inhalants, and other substance use in the past 6 to 12 months; responses were yes (1) or no (0).
Broad symptom measures
Fourteen items from the Strengths and Difficulties Questionnaire (Goodman et al., 1998) assessing emotional symptoms, conduct problems, hyperactivity/inattention, and some peer problems over the past 6 months (e.g., “I am usually on my own,” “I generally play along or keep to myself”) were included and rated from not true (0) to certainly true (2). In addition, nine items from the Pediatric Quality of Life inventory (Varni et al., 2001) assessing varied symptoms of psychopathology over the past month (e.g., “I feel angry” and “I hurt or ache”) were included and rated from never a problem (0) to almost always a problem (4).
Sleep
Sleep quantity (“During the last month, do you think you usually got enough sleep?”) was rated from plenty (1) to not nearly enough (4), and sleep quality (“During the last month, how well do you feel you have slept in general?”) was rated from very well (1) to very badly (4).
Data harmonization and analysis
Data coding
Data harmonization and analysis unfolded over multiple steps with the aim of combining the six subsamples into a single large data set for analysis. First, we developed an analytic plan that ultimately failed because of the number of subsamples and patterns of missingness that we combined, and the number of items we included. For a complete and transparent description of all planned, attempted, and failed analyses along with full details on coding, cleaning, and merging of data sets, see the Supplemental Material.
The first stage of coding identified items with identical or highly similar content that came from different measures and subsamples. This step was conducted by two fourth-year undergraduate students (M. Twose and A. Barrett) who were trained and supervised by M. K. Forbes. Overall, in the final pool of items, 190 (66%) of the symptom constructs were measured in at least two of the studies. Identical items (n = 146)—measured using the same self-report scale in multiple studies—were merged into a single variable across subsamples. The remaining items deemed to be measuring the same constructs but with variations in wording and/or response scale were kept separate and used as trace items with tags (_t1, _t2, _t3, etc.) added to the variable labels to keep track of whether these items converged in their placement in the final structural model. In total, there were 61 trace items across the subsamples measuring 28 symptom constructs (i.e., there are 28 unique trace item tags: _t1 . . . _t28; see Table S2 in the Supplemental Material).
Measurement invariance
Before combining the subsamples, we conducted measurement-invariance analyses to examine the extent to which the subsamples were statistically comparable or structurally compatible. We focused on the three measures 1 selected a priori with the broadest coverage among the subsamples—the Strengths and Difficulties Questionnaire (n = 16,093; assessed in all six subsamples), the Short Mood and Feelings Questionnaire (n = 9,335; assessed in four of the six samples, spanning clinical and community participants), and the Spence Children’s Anxiety Scale (n = 5,872; assessed in three of the six samples, spanning clinical and community participants). In all cases, configural and metric invariance held between samples, as described in the Supplemental Material. The results indicated that there were mean differences between the samples, as expected (e.g., Marsh et al., 2018), but that factor loadings could be constrained to equality between groups without worsening model fit (i.e., the measures are assessing the same constructs in each sample). On the basis of these results, we proceeded with combining the subsamples for analysis.
Data harmonization
We dropped items with very low endorsement (> 95% endorsing “no” or “never”)—because of their lack of variability and to reduce sparse cells in the estimation of the correlation matrices—unless we could pool them with highly similar items (e.g., for the alcohol-related harms and alcohol use disorder symptoms described above). In addition, we excluded measures with very poor coverage (i.e., < 183 responses in total [< 1% of the final data set] or measures on unique constructs administered in only one of the single-sex school trials; for details, see the Supplemental Material).
We treated missing data as missing at random 2 (i.e., the six subsamples had varying levels of overlap in the measures that were included; see the Supplemental Material) and handled missingness with full information maximum likelihood. All subsequent analyses relied on a model-implied correlation matrix that we generated from a saturated exploratory factor analysis (i.e., approximately one factor for each item). To do so, we followed Mplus recommendations for highly complex models (i.e., geomin rotation and mean and variance adjusted unweighted least squares [ULSMV], suppressing the computation of standard errors and chi square; Muthén & Muthén, 2017). We used the resulting factor loadings, factor correlations, and residual variances to calculate the complete model-implied correlation matrix (λ × φ × t(λ) + ψ). Next, we reestimated this matrix using eigenvector smoothing and used it as the input for all subsequent analyses. The final 288 × 288 correlation matrix for analysis was highly correlated (ρ = .92) with the observed Spearman correlations computed from the raw data (for both correlation matrices, see the OSF page for the project at https://osf.io/5ptsn/).
Hierarchical modeling
Mirroring the analytic approach in Forbes et al. (2021), primary analyses delineated a symptom-level hierarchical model of the structure of psychopathology in youth. We used extended bass-ackward modeling (Forbes, 2023) to delineate a top-down hierarchical model based on oblique principal components. The traditional bass-ackward method (Goldberg, 2006) begins with one component at the first level of the hierarchy and then extracts two components on the second level, three on the third, and so on. The correlations between adjacent levels of the resulting components are examined to explicate a hierarchy in the traditional bass-ackward method. The extended bass-ackward approach modifies this traditional method by removing redundant components and probable artifacts from the bass-ackward solution and looking at the component correlations among all remaining components to elucidate a simpler yet more complete hierarchy. Forbes (2023) suggested using both r ≥ .9 and a congruence coefficient > .95 to establish redundancy between components, but we used a less stringent cutoff here—requiring only r ≥ .9—because the traditional bass-ackward solution included an intractable number of components (n = 171). This less stringent cutoff is consistent with Goldberg’s (2006) proposed approach for identifying components that perpetuate between levels of the hierarchy.
To cross-validate the narrower constructs at the bottom of the extended bass-ackward hierarchy, we used two clustering methods—iclust (Revelle, 1979) and Ward’s (1963) hierarchical agglomerative clustering—combining items into clusters only where the two methods agreed. We estimated the iclust solution based on rules that items/clusters were combined only if alpha and beta in the new cluster were both larger than the largest of the separate clusters, and beta was maintained ≥ 0.9 (i.e., ≥ 90% of the variance accounted for by a general factor within each cluster). Ward’s agglomerative hierarchical clustering relied on a Euclidean distance matrix from 1 – |ρ|, and we extracted clusters until the first orphan item emerged. These two largely overlapping clustering solutions were then concatenated into a merged cluster solution (i.e., items were included in a cluster only when both methods converged on that structure; otherwise. they were split into separate clusters) and further examined for convergence with the constructs at the lowest levels of the extended bass-ackward hierarchy. We compared the full Ward’s hierarchy with the upper levels of the extended bass-ackward hierarchy as a second test of convergence between methods, with a particular focus on understanding which aspects of the extended bass-ackward hierarchy did not replicate and thus were potentially artifactual (see Forbes, 2023). The points of convergence among these methods were used to identify the final hierarchical model, which is the focus of the results and discussion.
Results
Bass-ackward models
Parallel analysis suggested extracting up to 44 components, but only the first 19 components had at least three unique primary indicators ≥ .4 for each component. We therefore carried forward the first 19 levels of the hierarchy. For the component loadings for this level of the hierarchy, see Table S3 in the Supplemental Material; for a file with the component loadings for all other levels, see the OSF page for the project (https://osf.io/5ptsn/). The 19 components at the bottom of the hierarchy included dimensions of alcohol use and harms, impulsive anger, antagonism, positive psychosis (e.g., hallucinations, delusions), maladaptive responses to anger, eating pathology, substance use together with appearance concerns, specific worries, negative affect, internalizing, fear and separation anxiety, social anxiety, obsessions, uncontrollable worry, compulsions, distress, online bullying, and antisociality along with illicit substance use (see Table S3 in the Supplemental Material).
Importantly, most of these 19 components represented a mixture of subsamples and measures (see Table S3 in the Supplemental Material), indicating that the data harmonization did not simply recapitulate method artifacts in the structure. There were also a few instances in which the hierarchical structure produced components that did appear artifactual, containing only items from a single measure or a single sample. Specifically, the specific worries component reproduced the list of 10 specific worries adapted from the Children’s Worries and Concerns Scale measured only in Sample 5, the online bullying component reproduced the list of eight cyberbullying items from the Online Friends Cyberbullying measure included only in Sample 2, the positive psychosis component reproduces the nine DISC items assessing hallucinatory experiences and delusional beliefs included only in Sample 3, and the eating pathology component comprised only items from the Eating Attitudes Test (included in both Samples 1 and 2). Furthermore, for online bullying, it seems likely that the associations with other constructs were not well captured in the model-implied correlation matrix because this component was not related to any of the higher-order dimensions in the hierarchy; for the other three components described (specific worries, positive psychosis, and eating pathology), it appears more likely that these constructs emerged because of high levels of homogeneity or internal consistency among the items.
In the traditional bass-ackward version of the hierarchy (see Fig. S2 in the Supplemental Material), many of the lower-level components perpetuated across multiple levels of the hierarchy, which is one indication of their robustness. By contrast, above the seven-component level of the hierarchy, there were many redundant and artifactual components. In particular, there was marked instability in the composition and interpretation of the upper-level components, indicating what appear to be artifacts from forcing a structure with too few components (for discussion of each artifact, see the Supplemental Material). The exceptions in the upper levels of the hierarchy that had consistency across levels all perpetuated down to Level 7 (e.g., internalizing; uncontrollable worry, obsessions, and compulsions; externalizing; and eating pathology, described below). Even the highest-order components in the structure perpetuated through at least three levels of the hierarchy, indicating they did not capture broad overarching factors (e.g., a general factor of psychopathology). Together with the relatively low convergence in the upper levels of the clustering and bass-ackward solutions, this led us to take Level 7 as the top of the hierarchy in the extended bass-ackward approach. We removed all redundant and artifactual components as per the extended bass-ackward approach (Forbes, 2023). For descriptions of the artifacts in the traditional bass-ackward solution that were removed in the extended bass-ackward model (n = 14 [8.2%] of the 171 total components), see the Supplemental Material. The correlations among the remaining components were used to delineate a hierarchical structure, resulting in the full extended bass-ackward solution shown in Figure S3 in the Supplemental Material.
Hierarchical clustering
We used two clustering methods to identify and cross-validate narrow constructs at the bottom of the hierarchy: iclust and Ward’s agglomerative clustering. The iclust solution had 71 clusters, and the Ward’s agglomerative clustering hierarchy had 47 clusters. The solution based on the points of agreement between the two clustering methods (i.e., including items in a cluster only when both methods converged on that structure and otherwise splitting them into separate clusters) resulted in 79 total clusters. Table S3 in the Supplemental Material shows the full results for the three clustering solutions (i.e., based on iclust and Ward’s clustering alone and based on their combination), and Figure S1 in the Supplemental Material shows the full Ward’s hierarchy. Stopping rules for the Ward’s agglomerative clustering consistently indicated two or more clusters, further supporting the omission of a general factor of psychopathology.
Replication across methods
The 19 components at the bottom of the extended bass-ackward hierarchy had marked convergence with the clustering methods (see Table S3 in the Supplemental Material). Of the 79 clusters based on convergence between the iclust and Ward’s methods, five (6%) split across multiple components, three (4%) split with one or more items not loading ≥ .3 on any of the 19 components, and three (4%) split across multiple components and had one or more items not loading ≥ .3 on any component (these clusters are in bold and/or italics in Table S3 in the Supplemental Material). The large majority of clusters (86%) mapped directly onto the components at the bottom of the extended bass-ackward hierarchy.
Likewise, the upper levels of the extended bass-ackward and Ward’s clustering hierarchies also had marked convergence, as shown in Figures S1 and S3 in the Supplemental Material. We detail their patterns of convergence and divergence in the Supplemental Material. Briefly, both methods included similar broad externalizing; eating pathology; uncontrollable worry, obsessions, and compulsions; and internalizing constructs. Furthermore, the components that did not correlate with any of the higher-order components in the extended bass-ackward model tended to also be separate from other constructs in the clustering hierarchy. Finally, the trace items largely converged within broad domains of psychopathology (i.e., internalizing trace items were grouped together, and externalizing trace items were grouped together) with some exceptions, explored in more detail later.
Interpreting the final hierarchical structure
The final model based on convergence between Ward’s hierarchical clustering and the extended bass-ackward approach is captured in Figure 2 and organized around four broad domains. First, externalizing comprised narrower domains of impulsive anger, antagonism, positive psychosis, and maladaptive responses to anger. The items that cross-loaded among these narrower domains (see bold items in Fig. 2a) are consistent with an externalizing dimension pervading throughout the lower-order dimensions. The presence of the positive psychosis dimension here is somewhat unexpected but was consistent across methods. Second, the eating pathology dimension reflected an agglomeration dominated by eating-pathology symptoms alongside a mix of substance use and appearance concerns (Fig. 2a). Third, the uncontrollable worry, obsessions, and compulsions domain comprised obsessions and compulsions along with uncontrollable worrying; some items on the uncontrollable worry dimension also cross-loaded on the broad internalizing dimension (Fig. 2b). Finally, a broad internalizing domain comprised general internalizing-spectrum symptoms, a negative affect dimension, a negative self-concept dimension, and narrower dimensions of social anxiety, fear and separation anxiety, and specific worries (Fig. 2b). The internalizing-spectrum symptoms and negative-affect dimensions do not appear to differ substantively in content or breadth but, rather, seem to be primarily differentiating between two self-report measures (i.e., items from the Pediatric Quality of Life inventory and Brief Emotional Distress Scale for Youth, respectively; see Table S3 in the Supplemental Material). This distinction was retained in the final structure because of its methodological robustness across clustering and hierarchical modeling methods, but we do not believe it is likely to be particularly meaningful.
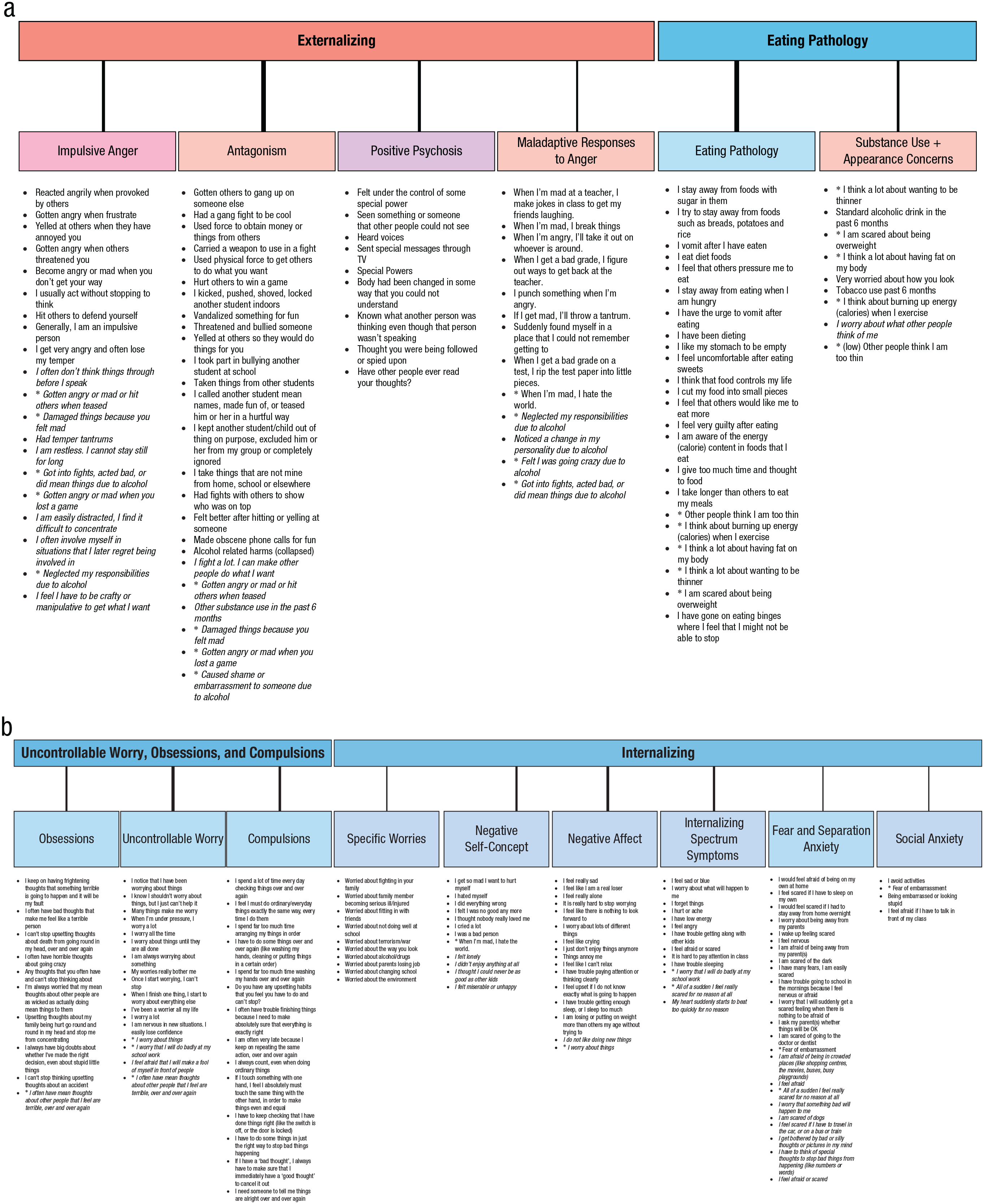
Two panels presenting a summary model of the convergence between the extended bass-ackward and hierarchical agglomerative cluster analysis solutions. (a) The dimensions under externalizing and eating pathology. (b) The dimensions under uncontrollable worry, obsessions, and compulsions and internalizing. The items listed under each dimension are sorted by the strength of their component loadings; items marked with an asterisk (*) cross-load on more than one component; italic items have a weak primary loading between .3 and .4. Line weights linking constructs correspond to the strength of the correlation between them. Dashed lines represent secondary correlations. A secondary correlation between obsessions and eating pathology is not shown because it spans Figure 1a and Figure 1b. Colors are selected to reflect the assignment of each domain in Figure 1b to compare what one might expect based on the literature with what was found here.
It is noteworthy that there was not compelling evidence for higher-order spectra above the four broad domains of externalizing; eating pathology; uncontrollable worry, obsessions, and compulsions; and internalizing. The one possible exception was some patterns of association among all higher-order spectra except externalizing, akin to emotional dysfunction in Figure 1b. For example, the lower-order dimensions under uncontrollable worry, obsessions, and compulsions all had secondary correlations with internalizing in the extended bass-ackward hierarchy; obsessions also had a secondary correlation with eating pathology. These three broad domains largely agglomerated in the (unreliable) upper levels of the clustering hierarchy and on the second tier of the traditional bass-ackward solution (see Figs. S1–S3 in the Supplemental Material), remaining distinct from externalizing. Items assessing anxiety were also spread across the three broad domains. For example, items assessing social anxiety loaded on narrow dimensions, including uncontrollable worry (“I feel afraid that I will make a fool of myself in front of people”), substance use and appearance concerns (“I worry about what other people think of me”), specific worries (“Worry about fitting in with friends”), and fear and separation anxiety (“Fear of embarrassment”) in addition to the relatively constricted social-anxiety dimension under internalizing (see Fig. 2). Items assessing worry did the same. These patterns are worth noting but were not robust enough to indicate the inclusion of a broad emotional dysfunction domain in the final structure.
In contrast with the anxiety items, other item-level cross-loadings generally reflected the broad domains shared by lower-order dimensions. Trace items further reinforced these patterns (for details on the trace items, see Fig. S1 and Table S2 in the Supplemental Material), indicating coherence between subsamples within the broad internalizing and externalizing domains in particular. Substance use trace items (see Table S2 in the Supplemental Material) were notably overrepresented in the components from the bass-ackward solution that were not included in the final structure, but the alcohol and tobacco use trace items did appear as part of the substance use and appearance concerns dimension, and the alcohol-related harms and illicit substance use trace items loaded on antagonism.
Discussion
In this study, we aimed to model the hierarchical and dimensional structure of a wide variety of psychopathology symptoms in a large sample of children and adolescents. The resulting model included four broad domains of internalizing; externalizing; eating pathology; and uncontrollable worry, obsessions, and compulsions with 15 narrower dimensions nested beneath them. Although our findings do not represent a definitive hierarchical and dimensional model of youth psychopathology, they add to the rapidly growing literature in several interesting ways. We turn now to interpret the results in the context of the extant literature.
Internalizing and externalizing
First, the internalizing and externalizing domains both represented familiar constructs from youth and adult literatures on the structure of psychopathology. That is, internalizing included items assessing worries, negative affect, negative self-concept, fear, separation anxiety, and social anxiety, and externalizing included impulsivity, anger, antagonism, and items assessing alcohol-related harms—both of which mirrored the placement of similar constructs in our synthesis of the existing youth literature and the HiTOP model (Fig. 1).
The internalizing dimensions also included the items assessing somatic symptoms, detachment, and inattention. The absence of a somatic-symptoms dimension (cf. Fig. 1b) is likely to be due in part to the sparse content coverage in the item pool, although somatic symptoms loading on a broad internalizing dimension—akin to emotional dysfunction in Figure 1b—is consistent with other studies’ findings (e.g., Achenbach, 2020; Haltigan et al., 2018; Michelini et al., 2019). Likewise, detachment items loading on this kind of broad internalizing dimension also mirrors prior work (e.g., Achenbach, 2020; Haltigan et al., 2018; Michelini et al., 2019). By contrast, inattention symptoms loading on internalizing departs from much of the existing youth literature in which ADHD symptoms often load on an externalizing dimension (e.g., Castellanos-Ryan et al., 2016; Haltigan et al., 2018; Lahey et al., 2004, 2008; for an exception, see Dominguez-Alvarez et al., in prep). Most of the studies that have included inattention under externalizing were confirmatory, so model misspecification considering hyperactivity and inattention as a single construct (reflecting ADHD) may be playing a role there. The relationship of inattention with internalizing found here does reflect the known association with internalizing psychopathology for symptoms such as difficulty concentrating and difficulty with school work (e.g., Schniering et al., 2023).
The absence of thought disorder
In addition to covering the expected domains, externalizing also included positive psychosis symptoms, which resulted in the absence of a thought-disorder domain in the final model. This was in contrast to other studies that have included assessment of psychosis-like experiences in youth (e.g., Afzali et al., 2018; Carragher et al., 2016; Laceulle et al., 2015). This association between externalizing and positive psychosis did not appear to be a method- or distribution-related artifact but notably departs from the existing youth literature and the HiTOP model (Fig. 1). Providing some support for the validity of this finding in youth, Michelini et al.’s (2019) neurodevelopmental factor was reminiscent of this mix of constructs with a combination of impulsivity and inattention items 3 along with thought-disorder items (e.g., strange ideas, strange behavior). Recent research in children and adolescents aged 9 to 13 years in the Adolescent Brain and Cognitive Development Study has also found a moderate association between prodromal schizophrenia symptoms and incipient alcohol use (Watts et al., 2021, 2024), the latter of which is typically regarded as an index of externalizing. Furthermore, Michelini et al. (2021) described mechanisms captured in the Research Domain Criteria social-processes and cognitive-systems domains shared by HiTOP thought-disorder and externalizing dimensions, perhaps supporting a stronger relationship than is captured in the current HiTOP model.
Alternatively, the absence of a thought-disorder domain in our final hierarchical model could be consistent with theories of p differentiation across development (i.e., that a general propensity to internalizing and externalizing psychopathology in childhood develops into distinct symptom domains only later in development; Murray et al., 2016) or due to lower prevalence of thought-disorder indicators in childhood and adolescence versus adulthood (e.g., Hare et al., 2010). In addition, the items measuring hallucinatory experiences and delusional beliefs measured here may be assessing nonpsychotic features in some cases (e.g., active imagination in childhood). Either way, the relatively low coverage of core thought-disorder indicators here with positive psychosis items assessed in only one of the subsamples is a limitation that should be addressed in future research; the inclusion of additional markers of thought disorder would help to clarify their placement in the metastructure of psychopathology.
Other domains that have sometimes been found to indicate a thought-disorder dimension—eating pathology, obsessions, and compulsions (e.g., Forbes et al., 2021)—were assessed across several subsamples we analyzed, but they did not converge with one another or with positive psychosis under externalizing. Instead, eating pathology and obsessions and compulsions formed distinct domains in the final model (Fig. 2b). These broad domains of (a) eating pathology and (b) uncontrollable worry, obsessions, and compulsions may be, in part, bloated specific factors that reflect the particularly detailed assessment of these constructs across our subsamples. Thus, if these two domains do indeed fall under a broader umbrella of internalizing, thought disorder, or both, the preponderance of items assessing these constructs might have contributed to the formation of broad components as well as their separation from other psychopathology domains too early in the clustering solutions.
Eating pathology
The eating pathology domain included all items designed to assess eating pathology in addition to a dimension of appearance concerns with two items assessing substance use—specifically, smoking and drinking—that appear to reflect image consciousness (cf. body-image and eating disorders). This latter association might represent an age-related effect reflecting lower prevalence of appearance concerns and substance use earlier in youth. Alternatively, if it reflects a substantive association relating to a desirable “image” associated with smoking or drinking, this may well be cohort-specific and change over time because alcohol and tobacco use in adolescence are becoming less common (e.g., Reitsma et al., 2021; Vashishtha et al., 2021). Alternatively, the relationship with maladaptive responses to anger seen in the extended bass-ackward results might suggest a deeper association with externalizing symptoms here (e.g., reflecting the relationship of binge eating and purging with disinhibition; Gilmartin et al., 2023; Kemps & Wilsdon, 2010; Pearson et al., 2015). Regardless, the associations between eating pathology, substance use, and traditional markers of externalizing psychopathology depart from some research that has examined the structure of psychopathology in youth (e.g., Castellanos-Ryan et al., 2016) and should be replicated and validated before it is considered for inclusion in formal models of youth psychopathology.
Uncontrollable worry, obsessions, and compulsions
The uncontrollable worry, obsessions, and compulsions domain was also broader than expected based on past research, combining general-anxiety-disorder-like uncontrollable worry with the OCD-related obsessions and compulsions items rather than with the core internalizing dimensions (e.g., specific worries and negative affect). This dimension might reflect the idea that general anxiety disorder and OCD diagnoses are similar in youth (Comer et al., 2004), that worry and ritualistic-behavior symptom components are closely related (Laing et al., 2009), and that obsessions, compulsions, and worrying share transdiagnostic processes, such as cognitive control (Fitzgerald et al., 2021) and intolerance of uncertainty (Gillett et al., 2018). As for the other novel dimensions, this dimension needs further testing before it is considered for inclusion in formal models of youth psychopathology.
Substance use and related harms
Many of the items assessing substance use and related harms were noteworthy in their absence from the final structure. Representation of these constructs was limited to the inclusion of two smoking and drinking items with image consciousness, a weak loading of one illicit substance use item on antagonism (consistent with rule-breaking behavior), and some alcohol-related harms items loading on externalizing and its subdimensions. Most items assessing alcohol and other substance use (cannabis, tobacco, inhalants) were not included in the final structure because of their weak associations with other constructs. Overall, substance use assessed separately from substance-use-related harms was not closely related to the externalizing dimensions, as would have been expected based on the existing youth literature and the HiTOP model (Fig. 1).
By contrast, the finding that alcohol-related harms were some of the strongest indicators for the higher-order externalizing component likely reflects the fact that harms were partly operationalized by social/interpersonal maladjustment (e.g., “caused shame or embarrassment to someone,” “got into fights, acted bad, or did mean things”) and irresponsibility (e.g., “neglected my responsibilities”; Martin et al., 2014; McDowell et al., 2019; Watts et al., 2023). These results are consistent with a burgeoning literature that suggests that the placement of harmful substance use in HiTOP, for example, is driven by a focus on substance-use-disorder diagnoses that heavily weight harms and impairment, pulling in variance related to externalizing (e.g., antagonism, rule breaking, irresponsibility; Martin et al., 2011; Watts et al., 2023). Parsing substance use per se from its potential downstream consequences (e.g., harms) may well be important for understanding where these constructs should be placed in an empirical hierarchical model of psychopathology for youth and in adulthood (Watts & Boness, 2022).
Limitations and future directions
The very large sample size and comprehensive breadth of assessment of psychopathology in this study are noteworthy strengths, but it is also important to keep the limitations of the study in mind when interpreting the results. For example, this study was based on analyses of existing self-report data that were not collected for the purpose of understanding the structure of psychopathology, and data harmonization was more difficult than we anticipated despite the substantial overlap in measurement across the subsamples.
Items were presented in blocks corresponding to the self-report measures they were a part of, and this is likely to have anchored items more strongly to constructs than if the items were presented in random order. Furthermore, there was much more detailed coverage of some constructs (e.g., negative affect, externalizing behaviors) than others (e.g., thought disorder, detachment, somatic symptoms), which is likely to have affected the dimensions that emerged—for example, with bloated specific factors in domains with detailed coverage and suppression of dimensions with insufficient coverage. Although method variance is an important threat to validity for structures that rely on items from multiple instruments and subsamples, we carefully considered interpretability and method variance at each interpretive step. We also used three different statistical methods (iclust, Ward’s clustering, and the extended bass-ackward approach) to identify the symptom-level hierarchical model indicated by their points of agreement and disagreement to reduce the likelihood of overinterpreting results idiosyncratic to a single statistical method. The close agreement among these methods increases our confidence in the results, as does the fact that most of the final hierarchical structure was made up of components that spanned instruments, time frames, and subsamples.
It remains unclear how robust the detailed levels of symptom-level models will be across measurement methods, among clinical versus community or representative samples, and in development across the life span. We found that trace items of similar symptoms measured in different samples loaded together within the internalizing and externalizing domains—indicating robustness at the level of broad spectra—but not within specific clusters or narrow components. Formally testing measurement invariance of the final hierarchical structure was not possible here but should be a focus of future research. More research is also needed that is tailor-built to answer questions such as whether a single structural model will be appropriate for the full age range of participants included here (6–18 years) and whether there is meaningful developmental discontinuity in the structure of psychopathology across the life span (e.g., Mann et al., 2020). More work is also needed to test the robustness of the structure among sociodemographic groups (e.g., racial-ethnic robustness; He & Li, 2021) and using multiinformant and multimethod approaches to assessing psychopathology. Research that is specifically designed to answer these questions can also ensure full coverage of youth psychopathology (e.g., although our item pool spanned nearly every construct in Fig. 1b, traumatic stress and tics were not covered). Furthermore, although core dimensions of psychopathology—such as fear, distress, and externalizing—have been found to show stable associations with normal personality across adolescence and adulthood (e.g., Levin-Aspenson et al., 2019), more work is needed to integrate personality pathology into the structure of youth psychopathology (Shields et al., 2021). Even if a robust and generalizable structure of psychopathology is found that applies to children and adolescents, it will be essential to test whether such a framework offers sufficient improvements over the status quo for clinical utility of assessment, diagnosis, prognosis, and treatment selection in youth before it is recommended for adoption in clinical practice.
Conclusion
Overall, this study adds to the growing literature on the structure of youth psychopathology using the biggest sample and broadest assessment of psychopathology to date. Our results reinforce some of the key structures in the extant literature (Fig. 1b) but raise questions about the placement of substance use and psychotic-like experiences as well as the organization of domains under traditional (i.e., narrow) and broad conceptualizations of internalizing. Furthermore, our structure largely converged with that of the adult literature (Fig. 1a), suggesting some compatibility in hierarchical models of psychopathology across the life span. Incorporating and testing these findings in future research will help iterate toward a clearer picture of a developmentally informed expansion of the HiTOP model.
Supplemental Material
sj-pdf-1-cpx-10.1177_21677026241257852 – Supplemental material for A Hierarchical Model of the Symptom-Level Structure of Psychopathology in Youth
Supplemental material, sj-pdf-1-cpx-10.1177_21677026241257852 for A Hierarchical Model of the Symptom-Level Structure of Psychopathology in Youth by Miriam K. Forbes, Ashley L. Watts, Maddison Twose, Angelique Barrett, Jennifer L. Hudson, Heidi J. Lyneham, Lauren McLellan, Nicola C. Newton, Gemma Sicouri, Cath Chapman, Anna McKinnon, Ronald M. Rapee, Tim Slade, Maree Teesson, Kristian Markon and Matthew Sunderland in Clinical Psychological Science
Footnotes
Acknowledgements
This article uses unit-record data from Growing Up in Australia: The Longitudinal Study of Australian Children (LSAC). LSAC was conducted by the Australian Government Department of Social Services (DSS). The findings and views reported in this article, however, are those of the author(s) and should not be attributed to the Australian Government, DSS, or any of DSS’s contractors or partners (http://dx.doi.org/10.26193/JOZW2U). The Climate and Preventure study was funded by the National Health and Medical Research Council (NHMRC; APP1004744, APP1124958). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. We acknowledge the study participants and all the research assistants who have worked across the study. The research team also acknowledges the assistance of the New South Wales Department of Education and Communities (SERAP 2011201) for access to their schools for this research. The Climate Schools Combined study was funded by NHMRC (APP1047291, APP1143555) and Australian Rotary Health. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. We acknowledge the schools, students, teachers and research assistants who were involved in this research. The research team also acknowledges the assistance of the New South Wales Department of Education and Communities (SERAP 2013054), the Western Australian Department of Education (D13/0475948), the Western Australian Catholic Education Office, the Brisbane Catholic Education Office, and Queensland Department of Education and Training for access to their schools for this research, NHMRC Fellowship funding (M. Teesson APP1870487), and NHMRC funding for the Centre of Research excellence in the Prevention and Early Intervention in Mental Health and Substance Use (APP1134909). The Centre for Emotional Health Clinic sample included data from trials funded by Australian Rotary Health, the NHMRC (e.g., APP1103611, APP382008, APP1027556), and the Australian Research Council (ARC; e.g., J. L. Hudson, FT120100217). The Emotional Health Project was funded by an ARC Linkage Grant (J. L. Hudson, R. M. Rapee, H. Dodd, C. Newall, T. Eley, LP130100576) and an ARC Future Fellowship (J. L. Hudson, FT120100217). The Male Adolescent Anxiety Project was funded by Beyondblue.
Transparency
Action Editor: Jennifer Lau
Editor: Jennifer L. Tackett
Author Contributions
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.