
Abstract
Sleep problems commonly co-occur alongside generalized and social anxiety, depression, and eating disorders in young people. Yet it is unclear if sleep disturbance conveys risk for these social-emotional disorders across early to middle adolescence and whether repetitive negative thinking (RNT) mediates this association. In this study, we examined longitudinal relationships between sleep (morning/eveningness, school-night sleep duration, and sleepiness), general and presleep RNT, and symptoms of generalized and social anxiety, depression, and eating disorders across 5 years. As part of the wider Risks to Adolescent Wellbeing Project, these constructs were assessed in a cohort of 528 youths over six annual waves of data collection, spanning ages 11 to 16. Cross-lagged panel models that examined direct, indirect, and bidirectional associations showed that worse adolescent sleep predicted increases in symptoms of generalized anxiety, social anxiety, depression, and eating disorders across each wave directly and indirectly through general and presleep RNT. Symptoms of social-emotional disorders did not predict worsening in sleep. Results suggest that sleep disturbance and RNT should be targeted simultaneously in the prevention and treatment of social-emotional disorders in adolescence, although limitations around the use of self-report and nondiagnostic symptom measures are noted.
Adolescence is a sensitive developmental period for the onset of psychopathology (Kessler et al., 2005), especially and predominantly social-emotional disorders, including generalized anxiety, social anxiety, depression, and disordered eating (Rapee et al., 2019). A recent conceptual model proposed that this group of disorders (i.e., social-emotional disorders) should be examined at the same time because they (a) all have an onset in adolescence; (b) share core features, such as negative affectivity, mood dysregulation, and concern about opinions/observations of others; and (c) share physical, cognitive, emotional, and social risk factors (for more detail, see Rapee et al., 2019). When experienced in adolescence, symptoms of these disorders are associated with significant burden (Klaufus et al., 2022) and adverse long-term outcomes, including worse educational outcomes, unemployment, and worse mental health and suicidality in adulthood (Clayborne et al., 2019; Johnson et al., 2018). Therefore, it is a priority to identify risk and protective factors for the onset of social-emotional disorders in adolescence so that more effective prevention and treatment approaches can be developed. Sleep disturbance and repetitive negative thinking (RNT; e.g., worry and rumination) have both been proposed as important transdiagnostic risk factors for the onset and maintenance of social-emotional disorders (Ehring & Watkins, 2008; Harvey et al., 2011). Yet the nature of the relationship (e.g., unidirectional, bidirectional) between sleep and symptoms of social-emotional disorders is relatively unknown across the course of early to middle adolescence, and it is unclear whether RNT mediates these relationships, as has been theorized (Akbar et al., 2022; Lovato & Gradisar, 2014).
Sleep Disturbance as a Risk Factor for Social-Emotional Disorders in Adolescence
Normative developmental changes in the circadian system and sleep homeostasis occur from the onset of puberty, resulting in major changes in sleep. Physiological rhythms related to alertness/sleepiness (i.e., melatonin and core body temperature) drift later, and sleep pressure (i.e., sleepiness) takes longer to build up across wakefulness (Crowley et al., 2014; Jenni et al., 2005). Consequently, maturation of these sleep processes commonly leads to an evening diurnal preference, later sleep timing, and sleep-onset difficulties (Gradisar et al., 2011). Furthermore, when paired with early school-start times, eveningness is associated with curtailed school-night sleep duration and daytime sleepiness (Crowley et al., 2018).
Sleep disturbance commonly co-occurs with social-emotional disorders in young people. In one study, 97% of children and adolescents (6–17 years) with a diagnosis of generalized anxiety and 90% of children and adolescents with social anxiety had at least one sleep-related problem (Alfano et al., 2007). Likewise, the vast majority (71%–92%) of adolescents diagnosed with a depressive disorder report sleep disturbances (Orchard et al., 2017; Reynolds et al., 2020). Sleep disturbance is also central to eating disorders; 43% of adolescents receiving treatment for an eating disorder meet diagnostic criteria for insomnia (i.e., 4 times what is seen in the general population; Hysing et al., 2022).
Beyond being just a symptom, there is growing longitudinal evidence, both from ecological momentary assessment studies across multiple days and cohort studies spanning many years, that sleep disturbance predicts increases in symptoms of anxiety, depression, and eating disorders (Cousins et al., 2011; Hafstad et al., 2013; Kortesoja et al., 2020; Lovato & Gradisar, 2014; Manasse et al., 2022; Peltz et al., 2017). Current evidence more strongly suggests that sleep disturbance predicts subsequent increases in anxiety (Willis & Gregory, 2015) and depression (Lovato & Gradisar, 2014) than the inverse (i.e., that anxiety and/or depression predict worsening of sleep), although there is a lack of research examining whether eating disorders predict changes in sleep.
In sum, sleep disturbance appears to be a robust risk factor for symptoms of social-emotional disorders in young people. However, the long time lags in existing longitudinal research limit understanding of the temporal features of this relationship and the potential role in the acceleration of disorder onset during adolescence (Rapee et al., 2019). For example, studies have examined early childhood sleep predicting adolescent eating-disorder symptoms (Hafstad et al., 2013) and adolescent sleep predicting depression and anxiety in early adulthood (Orchard et al., 2020). Understanding the relationship between sleep and mental-health symptoms during early to middle adolescence is important because this represents a developmental period that is associated with the sharpest increase in these disorders (Rapee et al., 2019).
RNT as a Mechanism Linking Sleep Disturbance With Social-Emotional Disorders in Adolescence
Although there is growing evidence for the importance of sleep as a risk factor for social-emotional disorders in adolescence, it is not yet clear exactly how sleep conveys risk. Although many pathways are likely implicated (e.g., executive dysfunction, social withdrawal, cognitive biases) and should be investigated (Blake et al., 2018), several theoretical and conceptual models point to RNT as a key mediator of this relationship (Akbar et al., 2022; Blake et al., 2018; Gradisar et al., 2022; Lovato & Gradisar, 2014).
In particular, in their model of sleep and depression, Lovato and Gradisar (2014) theorized that developmental changes in adolescent sleep, that is, the delay in circadian timing and slowed buildup of sleep pressure, lead to delayed sleep onset and sleep-onset difficulties. This means that many adolescents lie awake in quiet darkness, an environment conducive to RNT, until they are physiologically able to sleep. Research supports an association between later sleep timing and RNT in adolescents (Richardson & Gradisar, 2021; Stewart et al., 2021). In addition, bright-light therapy, a sleep intervention that advances sleep timing and reduces sleep-onset difficulties, has been shown to reduce RNT in adolescents and young adults (Richardson & Gradisar, 2021). Similarly to Lovato and Gradisar (2014), Akbar and colleagues (2022) theorized that sleep disturbance affects neural connectivity in the default mode network (a collection of brain regions implicated in mentation), which promotes RNT, and ultimately increases vulnerability for other forms of social-emotional disorders (i.e., generalized anxiety, social anxiety, eating disorders).
Several longitudinal studies have established RNT as a prospective risk factor for anxiety, depression, and eating disorders in young people (Raes et al., 2020; Sala et al., 2019; Spinhoven et al., 2018). Furthermore, prevention and treatment studies have suggested that improvement in symptoms of these disorders is at least partially driven by reductions in RNT (Bell et al., 2023; Topper et al., 2017). Although there is an absence of studies examining whether RNT mediates the relationship between sleep disturbance and symptoms of generalized anxiety, social anxiety, and eating disorders, there is evidence that catastrophic worry (a form of RNT) mediates the longitudinal relationship between sleep disturbance and symptoms of depression in older adolescents (16–18 years; Danielsson et al., 2013). There was no indication of moderation by gender, suggesting the relationships are equally strong for both girls and boys (Danielsson et al., 2013).
Although Danielsson et al.’s (2013) study provided important foundational evidence of a relationship between sleep, RNT, and depression, they assessed sleep problems with a single-item measure (i.e., “Do you sleep well?”). A previous study showed that a single self-report item (e.g., “Do you have a sleep problem?”) is not particularly sensitive for detecting adolescents with problematic sleep behaviors (e.g., gaining sufficient sleep; Short et al., 2013). Thus, replication using more robust measurement of sleep problems (i.e., that captures a range of more concrete problematic sleep behaviors, e.g., short sleep duration, evening diurnal preference, daytime sleepiness) is warranted. Furthermore, RNT was assessed using a general measure of RNT (e.g., “I cannot stop thinking about my symptoms/ problem”). However, theory specifically suggests that it is RNT in the presleep period that increases risk for depression (Lovato & Gradisar, 2014). Therefore, future research should test whether both presleep RNT and more general RNT mediate the relationship between sleep disturbance and symptoms of social-emotional disorders. Doing so would provide insight into whether such specificity in the theoretical model is needed.
Further evidence of the potential importance of RNT in explaining the association between sleep disturbance and social-emotional disorders comes from an intervention study with younger adolescents (ages 12–16) that found that RNT mediated the association between insomnia and depression at baseline (Li et al., 2023). The study also found that reductions in RNT throughout the course of the 6-week sleep intervention resulted in improvements in adolescents’ depressive symptoms. However, like the previous study (Danielsson et al., 2013), the study used a general measure of RNT, and it is not known whether these findings extend beyond depression to the other forms of social-emotional disorder (i.e., social and generalized anxiety, disordered eating).
A further methodological limitation of past research is that it has not considered the bidirectional relationships between sleep, RNT, and mental-health symptoms and that mediation has not yet been tested using a robust cross-lagged panel design (Danielsson et al., 2013). Cross-lagged panel designs are particularly useful in cases in which bidirectionality between constructs is possible. Indeed, RNT is a common feature of social-emotional disorders (Ehring, 2021), and cognitive arousal is known to interfere with sleep (Valck et al., 2004; Wuyts et al., 2012). Therefore, although sleep disturbance may give rise to RNT in adolescence and symptoms of social-emotional disorders, in turn, it is also possible that young people with higher symptoms of these disorders will experience RNT that interferes with their sleep. In this way, the relationship between sleep, RNT, and symptoms of generalized anxiety, social anxiety, depression, and/or eating disorders may form a mutually reinforcing cycle; however, this possibility needs testing.
One study that investigated sleep duration as a longitudinal mechanism linking rumination with depression and anxiety (combined) in 13- to 15-year-old adolescents found RNT and depression/anxiety were mutually reinforcing but that sleep duration did not mediate this relationship (Mazzer et al., 2019). Similar to the findings of Danielsson and colleagues (2013), gender did not moderate any of the longitudinal cross-lagged paths in the model between sleep duration, RNT, and depression/anxiety (Mazzer et al., 2019). Only hypothesized paths between the constructs of interest were specified, meaning that bidirectional relationships between sleep disturbance and depression/anxiety were not explored and RNT was not investigated as a mediator.
In sum, both sleep and RNT have emerged as important risk factors for generalized anxiety, social anxiety, depression, and eating disorders in adolescence, and theories have proposed that RNT may be a key mechanism linking sleep disturbance with these social-emotional disorders. Although there is emerging evidence to support RNT as a mediator of sleep problems and depression in both younger (12–16 years; Li et al., 2023) and older adolescents (16–18 years; Danielsson et al., 2013), relationships between sleep, RNT, and depressive symptoms are yet to be examined in a bidirectional longitudinal framework across the course of early to middle adolescence (which coincides with the rapid increase in onset of sleep and depressive disorders) or with other social-emotional disorders that also show a rapid increase in onset during adolescence (i.e., generalized anxiety, social anxiety, and eating disorders). Investigating this model across each social-emotional disorder separately has implications for understanding whether the proposed model is specific to depression (Lovato & Gradisar, 2014) or also applies to generalized anxiety, social anxiety, and/or eating disorders.
The Current Study
In the current study, we aimed to investigate RNT as a mechanism linking sleep disturbance (eveningness/short sleep duration/daytime sleepiness) with symptoms of generalized anxiety, social anxiety, depression, and eating disorders across the course of early to middle adolescence. To gain insight into whether presleep RNT is a specific risk factor, both presleep and general RNT were explored separately. Furthermore, to determine whether the model is specific to depression or generalizable to all social-emotion disorders, each disorder was also examined separately.
The study’s aims were achieved by accessing data collected as part of the larger Risks to Adolescent Wellbeing (RAW) Project and examining longitudinal associations between the constructs of interest using cross-lagged panel models across six annual waves of data collection, starting when participants were 10 to 12 years old. Given that the overarching study aimed to recruit participants at an age before widespread onset of social-emotional disorders and because a dimensional approach allows for investigation into the degree to which a disorder is manifested, symptoms (i.e., rather than diagnoses) of generalized anxiety, social anxiety, depression, and eating disorders were used. Because theory does not suggest differential relationships for boys and girls and empirical studies have not found evidence of longitudinal moderation by gender (Danielsson et al., 2013; Mazzer et al., 2019), gender was statistically controlled for but not examined as a moderator.
It was hypothesized that sleep disturbance would predict more RNT and higher symptoms of generalized anxiety, social anxiety, depression, and eating disorders over time and that RNT would mediate the relationship between sleep disturbance and symptoms of social-emotional disorders. In these mediation pathways, it was expected that associations between sleep disturbance and presleep RNT would be stronger than associations between sleep disturbance and general RNT (Lovato & Gradisar, 2014). Given past findings (Mazzer et al., 2019), it was expected that general RNT and symptoms of generalized anxiety, social anxiety, depression, and eating disorders would be mutually reinforcing over time. Because RNT is a feature of social-emotional disorders and interferes with sleep (Valck et al., 2004; Wuyts et al., 2012), it was also expected that RNT would mediate any relationships from symptoms of social-emotional disorders to the emergence of later sleep disturbance. Presleep RNT and sleep disturbance were also expected to be mutually reinforcing.
Transparency and Openness
Preregistration
This study was not preregistered.
Data, materials, code, and online resources
This study does not have ethical approval to share the de-identified data publicly. It is possible that other researchers may access the data, but this must occur by contacting the research team and providing appropriate justification. Furthermore, the Macquarie University Human Research Ethics Committee requires the researchers to gain and provide evidence of ethical approval before the data are released. Materials used in this study (e.g., questionnaires) are accessible via the references provided. Other resources are included in the Supplemental Material available online.
Reporting
We report how we determined our sample size, all data exclusions, all manipulations, and all measures relevant to this study.
Ethical approval
The Macquarie University Human Research Ethics Committee provided approval for the RAW Project (Project ID 1863).
Method
Participants
In all, 528 adolescents (age: M = 11.19 years, SD = 0.55, range = 10–12; 51% male) completed Wave 1 of the study, 498 (age: M = 12.19 years, SD = 0.53, range = 11–13; 52% male) completed measures in Wave 2, 478 (age: M = 13.20 years, SD = 0.53, range = 12–14; 52% male) completed measures in Wave 3, 437 (age: M = 14.25 years, SD = 0.56, range = 13–16; 52% male) in Wave 4, 422 (age: M = 15.24, SD = 0.57, range = 14–17; 51% male) completed measures in Wave 5, and 391 (age: M = 16.24 years, SD = 0.56, range = 15–18; 52% male) completed measures in Wave 6. Most participants were born in Australia (90%) and had a White background (82%). Approximately 21% of parents reported a gross household income under $100,000, 44% reported a household income between $100,000 and $200,000, and 34% reported a household income greater than $200,000 (all AUD). Participants were recruited by convenience sampling via advertisements placed in school newsletters, after-school care centers, sporting clubs, and medical centers and on local community Facebook pages in Sydney, Australia.
Procedures
Data for the current study came from a larger longitudinal study, the RAW Project, which aimed to identify and understand the psychological and social factors that positively and negatively influence social-emotional functioning throughout adolescence. For more about the project and related publications, see https://rawproject.com.au/. The Macquarie University Human Research Ethics Committee provided approval for the wider study. All parents provided informed consent for their child’s involvement, and all adolescent participants provided assent. Among other activities, each annual wave of data collection involved completion of an online questionnaire battery (Qualtrics).
Measures
Morningness/eveningness preference
Diurnal preference was assessed using the 10-item (e.g., “How alert [wide awake] are you in the first half hour you’re up?”) Children’s Morningness-Eveningness Scale (MESC; Carskadon et al., 1991). Total scores range from 10 to 43; lower scores indicate a greater eveningness diurnal preference. Reliability of the MESC was acceptable in each wave of the study (Wave 1: α = .79; Wave 2: α = .81; Wave 3: α = .83; Wave 4: α = .83; Wave 5: α = .85; Wave 6: α = .84).
School-night sleep duration
Adolescent self-reported sleep duration on school nights was assessed using a single item (i.e., “How many hours sleep do you usually get each night on a school night?”); participants selected the number of hours from a prefilled drop-down menu with whole numbers ranging from 0 to 12.
Daytime sleepiness
Daytime somnolence was measured using the eight-item (“Are you usually wide awake during the day?”) Pediatric Daytime Sleepiness Scale (PDSS; Drake et al., 2003). Total scores range from 0 to 32. Higher scores reflect greater daytime sleepiness; however, for longitudinal analyses, we reverse-scored the scale for consistency with the MESC, sleep-duration item, and PDSS so that higher scores indicate better adolescent sleep. The PDSS had acceptable reliability across all waves (Wave 1: α = .78; Wave 2: α = .81; Wave 3: α = .83; Wave 4: α = .86; Wave 5: α = .87; Wave 6: α = .86).
Presleep RNT
Presleep RNT was measured using five items (e.g., “I go to bed and replay the day’s events over and over in my mind”) from the cognitive/emotional subscale of the Adolescent Sleep Hygiene Scale (ASHS; Harsh et al., 2002). One item (“I check the clock several times during the night”) from the subscale was excluded for the purposes of this study because it better reflects clockwatching. The five items were averaged and reverse-coded to create a subscale score ranging from 1 to 6; higher scores indicate more presleep RNT. The presleep RNT scale had acceptable reliability across all waves (Wave 1: α = .75; Wave 2: α = .79; Wave 3: α = .84; Wave 4: α = .86; Wave 5: α = .86; Wave 6: α = .84).
General RNT
General transdiagnostic RNT was measured using four items (e.g., “When I have a problem I can’t get it out of my head”) from the Persistent and Intrusive Negative Thoughts Scale (PINTS; Magson et al., 2019). One item (“I lay awake at night thinking about things”) from the scale was excluded for the purposes of this study because it reflects sleep-related RNT. The four items were averaged to create a mean score ranging from 1 to 5; higher scores indicate more general RNT. The four-item PINTS had acceptable reliability across all waves (Wave 1: α = .86; Wave 2: α = .89; Wave 3: α = .92; Wave 4: α = .93; Wave 5: α = .93; Wave 6: α = .93).
Generalized- and social-anxiety symptoms
Symptoms of generalized anxiety (six items; e.g., “I worry something bad will happen to me”) and social anxiety (six items; e.g., “I worry what other people think of me”) were measured using the social-anxiety and generalized-anxiety subscales of the Spence Children’s Anxiety Scale–Child Report (SCAS-C; Spence, 1998). The items were summed to create a total score ranging from 0 to 18; higher scores indicate higher generalized and social anxiety. The generalized-anxiety subscale demonstrated acceptable reliability across each wave (Wave 1: α = .77; Wave 2: α = .81; Wave 3: α = .86; Wave 4: α = .86; Wave 5: α = .88; Wave 6: α = .87). The social-anxiety subscale also had acceptable reliability across all waves (Wave 1: α = .76; Wave 2: α = .78; Wave 3: α = .78; Wave 4: α = .82; Wave 5: α = .84; Wave 6: α = .84).
Depression symptoms
Symptoms of depression (e.g., “I felt miserable or unhappy”) were measured using the 13-item Short Mood and Feelings Questionnaire–Child Report (SMFQ-C; Angold et al., 1995). Total scores range from 0 to 26; higher scores reflect worse symptoms of depression. The SMFQ-C had acceptable reliability across all waves (Wave 1: α = .88; Wave 2: α = .89; Wave 3: α = .92; Wave 4: α = .94; Wave 5: α = .94; Wave 6: α = .93).
Eating-disorder symptoms
Eating-disorder symptoms (e.g., “I am scared about being overweight”) were measured using the 26-item Children’s Eating Attitude Test (ChEAT; Maloney et al., 1988). Total scores range from 0 to 78; higher scores indicate greater eating-disorder pathology. The ChEAT had acceptable reliability across all waves (Wave 1: α = .81; Wave 2: α = .84; Wave 3: α = .86; Wave 4: α = .89; Wave 5: α = .91; Wave 6: α = .91).
Statistical analyses
Data aggregation and preliminary analyses were conducted with IBM SPSS (Version 27.0). Descriptive statistics (estimated marginal means and standard errors) were reported from linear mixed models, which were conducted to investigate change in key variables over time. Associations between variables were examined using Pearson correlations.
Confirmatory factor analyses (CFAs), invariance testing, and longitudinal cross-lagged panel analyses were undertaken with Mplus (Version 8.5; Muthén & Muthén, 2015). The CFA was carried out to determine whether it was statistically appropriate to create latent factors with the sleep and RNT measures. Following this, invariance testing was undertaken to ensure that the latent factors were interpreted consistently by the participants over time and in the same way for both boys and girls. Latent factors were created for sleep, presleep RNT, and general RNT. Sleep was indicated by MESC total scores, school-night sleep duration, and reverse-coded PDSS total scores to create a robust multifactorial measurement of adolescent sleep. Presleep RNT was indicated by the five relevant items from the cognitive/emotional subscale of the ASHS. General RNT was indicated by the four nonsleep items of the PINTS. The SCAS generalized-anxiety subscale score, SCAS social-anxiety subscale score, SMFQ-C total score, and ChEAT total score were entered as observed variables because the large number of items in each are unsuitable for creating a single latent factor.
Separate longitudinal cross-lagged panel models were specified for presleep and general RNT and for generalized anxiety, social anxiety, depression, and eating disorder symptoms separately (i.e., eight models in total; for schematic representation, see Fig. 1). In each model, autoregressive paths for each variable were specified between consecutive waves and all cross-lagged paths between variables across consecutive waves (Wave 1 to Wave 2, Wave 2 to Wave 3 etc.). The observed psychological-symptom variable was correlated with the RNT and adolescent sleep latent factor within each wave. Error terms of latent indicators were also autocorrelated over time (i.e., ME1–ME6) except for the PDSS because including correlated error terms for the PDSS over time worsened the model fit and thus was omitted from the model. Child gender was added as a covariate for each autoregressive and cross-lagged path.
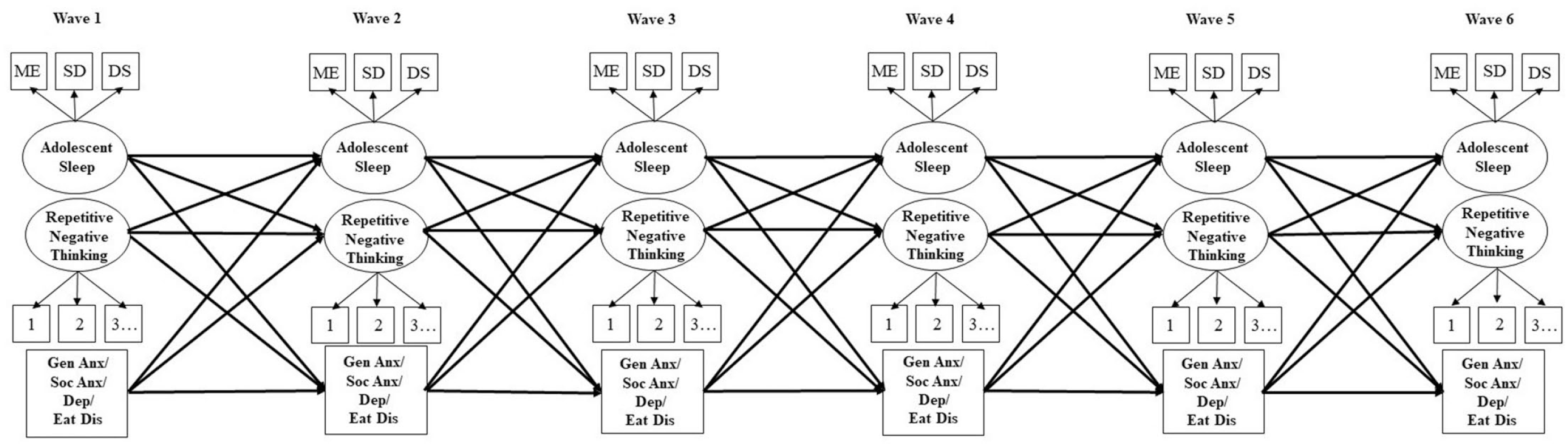
Schematic illustrating the autoregressive and cross-lagged paths specified in each statistical model. To avoid visual overcrowding concurrent associations between disorder symptoms and repetitive negative thinking/adolescent sleep within each wave and correlated error terms across waves, are not depicted.
All longitudinal mediation analyses were undertaken using the maximum likelihood estimator with 1,000 bootstraps. To investigate the pattern of missingness, a logistic regression was performed to assess whether baseline sample characteristics could predict whether participants dropped out or remained in the study until Wave 6 (Lu & Shelley, 2023). The full model containing all predictors (age, gender, sleep, RNT, symptoms of social-emotional disorders) was nonsignificant, χ2(11, 495) = 9.98, p = .532. The model as a whole explained little variance (2%–2.9%), and none of the individual predictors made a unique statistically significant contribution to the model (all ps ≥ .109). Thus, data were assumed to be missing at random and were handled using full information maximum likelihood in Mplus and linear mixed models in SPSS. For the current study, acceptable model fit was defined as comparative fit index (CFI) ≥ .90 and root mean square error of approximation (RMSEA) ≤ .08 (Chen, 2007). Measurement invariance was supported if the change in CFI value (ΔCFI) between the free and constrained model was ≤ .01 (Cheung & Rensvold, 2002).
The following cutoff values were used when interpreting small (0.03), medium (0.07), and large (0.12) effects in cross-lagged panel models (Orth et al., 2022). Correlation coefficients were interpreted with the following cutoff values for small (0.10), medium (0.30), and large (0.50) effects, and Cohen’s d was interpreted with the following cutoff values for very small (< 0.20), small (0.20), medium (0.50), and large (0.80) effects. To account for an article-wide 5% false-discovery rate, the Benjamini-Hochberg procedure (Benjamini & Hochberg, 1995) was applied. The adjusted critical alpha level was p < .044.
Results
Preliminary analyses
Estimated marginal means, standard errors, and range for each variable of interest are presented in Table 1, as are results from linear mixed models examining changes over time. There were significant main effects of time for all outcomes. Participants became increasingly evening orientated and obtained less sleep on school nights over time (small effect sizes were observed). Accordingly, there were very small increases in daytime sleepiness over time. Fluctuations in presleep and general RNT were typically very small, except for small increases in presleep RNT from Wave 4 to Wave 5 and small increases in general RNT from Wave 3 to Wave 4. There were small decreases in generalized anxiety from Wave 1 to Wave 2 and small increases from Wave 3 to Wave 4. There were very small to small increases in social anxiety and depressive symptoms each year from Wave 2 to Wave 5 and in eating-disorder symptoms from Wave 3 to Wave 5.
Descriptive Statistics (Estimated Marginal Means, Standard Errors, Range) and Change Over Time for Sleep, Repetitive Negative Thinking, and Symptoms of Social-Emotional Disorders From Wave 1 to Wave 6
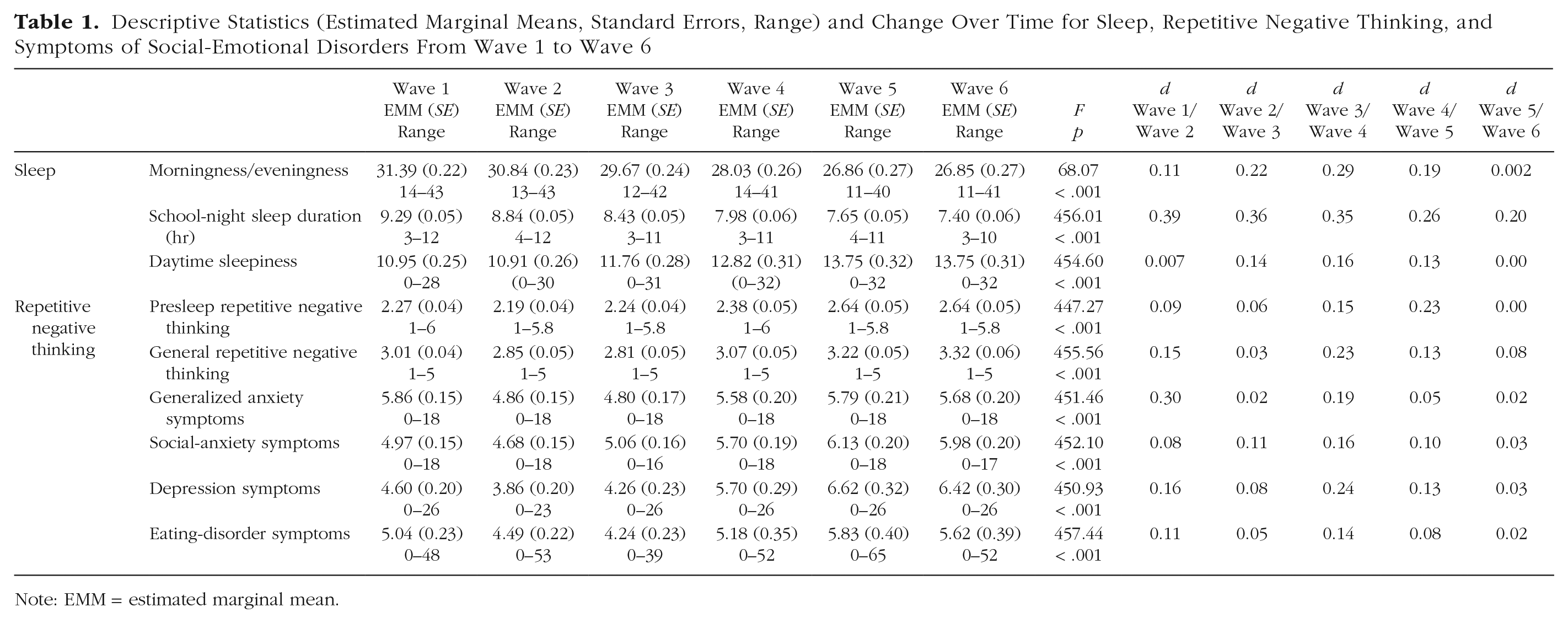
Note: EMM = estimated marginal mean.
Correlation coefficients are presented in Table 2. Within each wave, there were small to moderate correlations between morningness/eveningness, school-night sleep duration, daytime sleepiness, and RNT (presleep and general). There were also small to moderate correlations between sleep variables and psychological symptoms within each wave; the strength of the associations was strongest for daytime sleepiness. Finally, there were moderate to large intrawave correlations between RNT (presleep and general) and psychological symptoms.
Correlations Between Sleep, Repetitive Negative Thinking, and Symptoms of Social-Emotional Disorders From Wave 1 to Wave 6
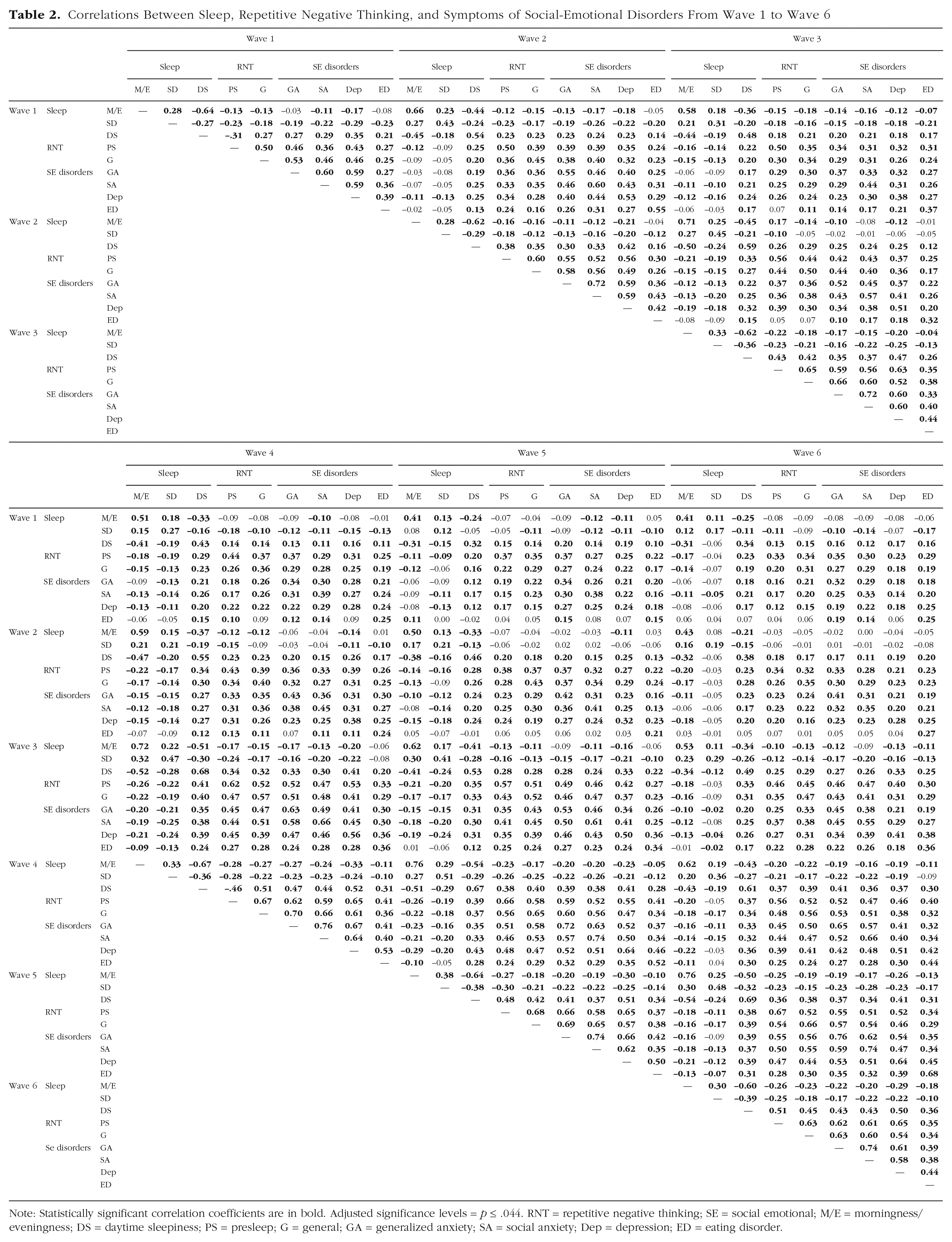
Note: Statistically significant correlation coefficients are in bold. Adjusted significance levels = p ≤ .044. RNT = repetitive negative thinking; SE = social emotional; M/E = morningness/eveningness; DS = daytime sleepiness; PS = presleep; G = general; GA = generalized anxiety; SA = social anxiety; Dep = depression; ED = eating disorder.
Measurement models and invariance testing
The six-wave CFA for the latent sleep factor produced a good fit to the data, χ2(N = 528) = 73.18, df = 75, CFI = 1.00, RMSEA = .000. The factor loadings were all positive and significant; daytime sleepiness loaded highest (0.80–0.83), followed by morningness/eveningness (0.74–0.82) and school-night sleep duration (0.35–0.47). Imposing equality constraints on the factor loadings across waves did not meaningfully change fit indices for the model (ΔCFI < .001), suggesting metric invariance over time. To determine whether the latent sleep factor was invariant for males and females, multigroup CFAs were run to assess configural (baseline), metric (factor loading), and scalar (intercept) invariance. The baseline model produced excellent fit, χ2(N = 528) = 145.20, df = 150, CFI = 1.00, RMSEA = .000, as did the metric model, χ2 = 166.96, df = 172, CFI = 1.00, RMSEA = .000, and scalar model, χ2 = 199.03, df = 184, CFI = .996, RMSEA = .018. Placing increasing constraints on the model parameters did not result in meaningful deterioration of the model fit when we compared the baseline model against the metric (ΔCFI < .001) and scalar (ΔCFI = .004) models; therefore, full invariance across gender was supported.
The six-wave CFA for the latent presleep RNT factor produced a good fit to the data, χ2(N = 528) = 600.68, df = 313, CFI = .949, RMSEA = .042. The factor loadings were all positive and significant. Imposing equality constraints on the factor loadings across waves did not meaningfully change fit indices for the model (ΔCFI < .001), suggesting metric invariance over time. To determine whether the latent presleep RNT factor was invariant for males and females, multigroup CFAs were run to assess configural (baseline), metric (factor loading), and scalar (intercept) invariance. The baseline model produced excellent fit, χ2(N = 528) = 994.76, df = 626, CFI = .932, RMSEA = .047, as did the metric model, χ2 = 1,030.82, df = 650, CFI = .929, RMSEA = .047, and scalar model, χ2 = 1,064.66, df = 674, CFI = .928, RMSEA = .047. Placing increasing constraints on the model parameters did not result in meaningful deterioration of the model fit when we compared the baseline model against the metric (ΔCFI = .003) and scalar (ΔCFI = .004) models; therefore, full invariance across gender was supported.
The six-wave CFA for the latent general RNT factor produced a good fit to the data, χ2(N = 528) = 191.49, df = 177, CFI = .998, RMSEA = .012. The factor loadings were all positive and significant. Imposing equality constraints on the factor loadings across waves did not meaningfully change fit indices for the model (ΔCFI < .001), suggesting metric invariance over time. To determine whether the latent general RNT factor was invariant for males and females, multigroup CFAs were run to assess configural (baseline), metric (factor loading), and scalar (intercept) invariance. The baseline model produced excellent fit, χ2(N = 528) = 402.72, df = 354, CFI = .993, RMSEA = .023, as did the metric model, χ2 = 418.86, df = 372, CFI = .993, RMSEA = .022, and scalar model, χ2 = 441.72, df = 390, CFI = .992, RMSEA = .022. Placing increasing constraints on the model parameters did not result in meaningful deterioration of the model fit when we compared the baseline model against the metric (ΔCFI < .001) and scalar (ΔCFI = .001) models; therefore, full invariance across gender was supported.
Longitudinal models
Generalized-anxiety symptoms
Presleep RNT
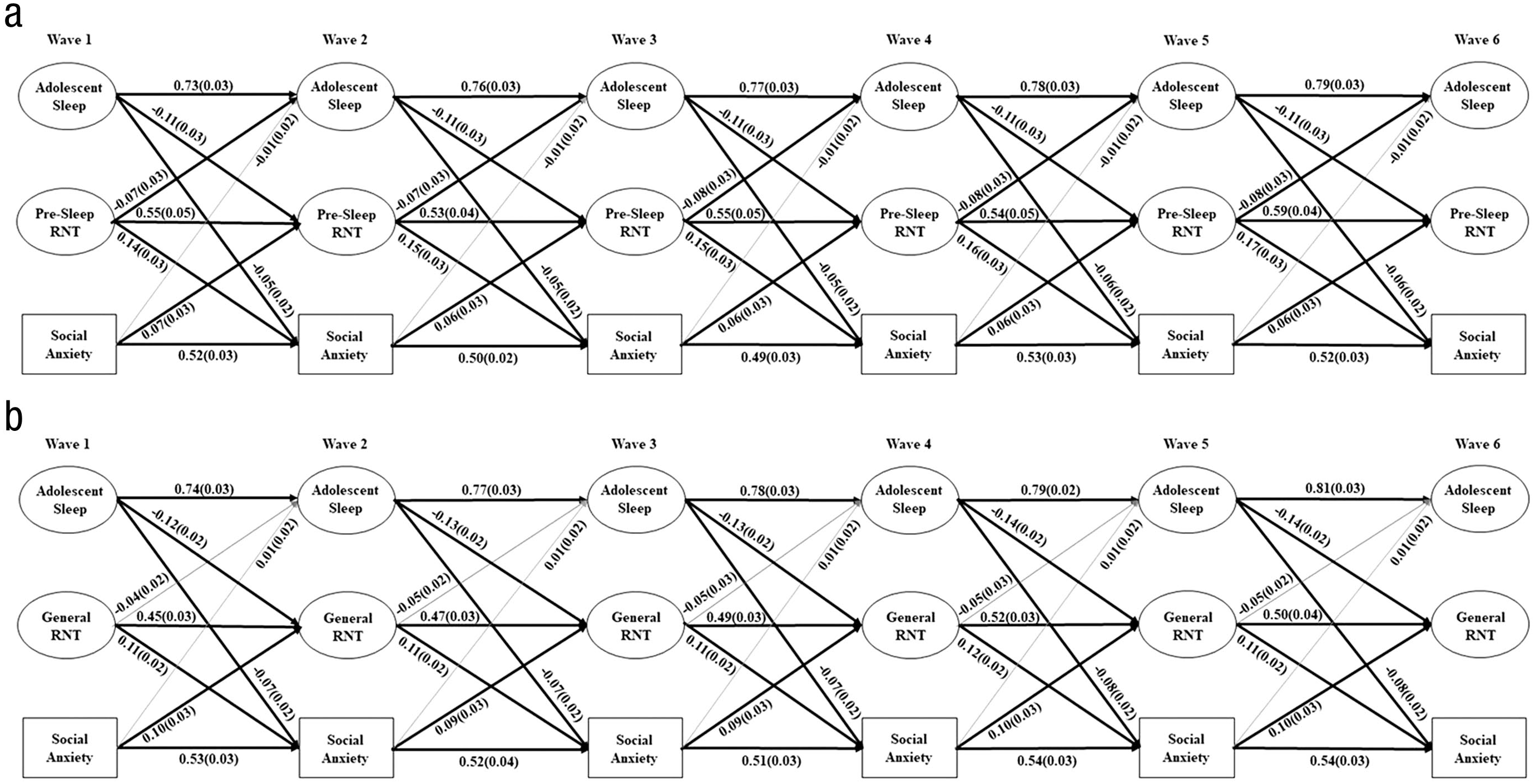
The model estimating the associations between the latent sleep factor, presleep RNT, and generalized-anxiety symptoms produced an acceptable fit to the data: χ2(N = 528) = 2,387.34, df = 1,336, CFI = .93, RMSEA = .039. The factor loadings were all positive and significant, ranging from 0.34 to 0.93. For all model results, see Table S1 in the Supplemental Material. For significant paths, see Figure 2a. As shown, there was a reciprocal association across all waves between sleep and presleep RNT; poor sleep predicted increases in presleep RNT 12 months later and vice versa. Both sleep and presleep predicted increases in generalized-anxiety symptoms over time, and generalized anxiety predicted increases in presleep RNT across all waves. However, the cross-lagged paths from generalized anxiety to sleep were nonsignificant. Estimates of the indirect paths from sleep to generalized anxiety indicated that presleep RNT partially mediated the association across all waves (Wave 1 to Wave 3: β = −0.02, SE = 0.004, p < .001; Wave 2 to Wave 4: β = −0.02, SE = 0.004, p < .001; Wave 3 to Wave 5: β = −0.02, SE = 0.004, p < .001; and Wave 4 to Wave 6: β = −0.02, SE = 0.004, p < .001). In contrast, the indirect path from generalized anxiety to adolescent sleep was not mediated by presleep RNT, from Wave 1 to Wave 3 (β = −0.01, SE = 0.006, p = .048), Wave 2 to Wave 4 (β = −0.01, SE = 0.006, p = .048), Wave 3 to Wave 5 (β = −0.01, SE = 0.006, p = .048), or Wave 4 to Wave 6 (β = −0.01, SE = 0.006, p = .048).
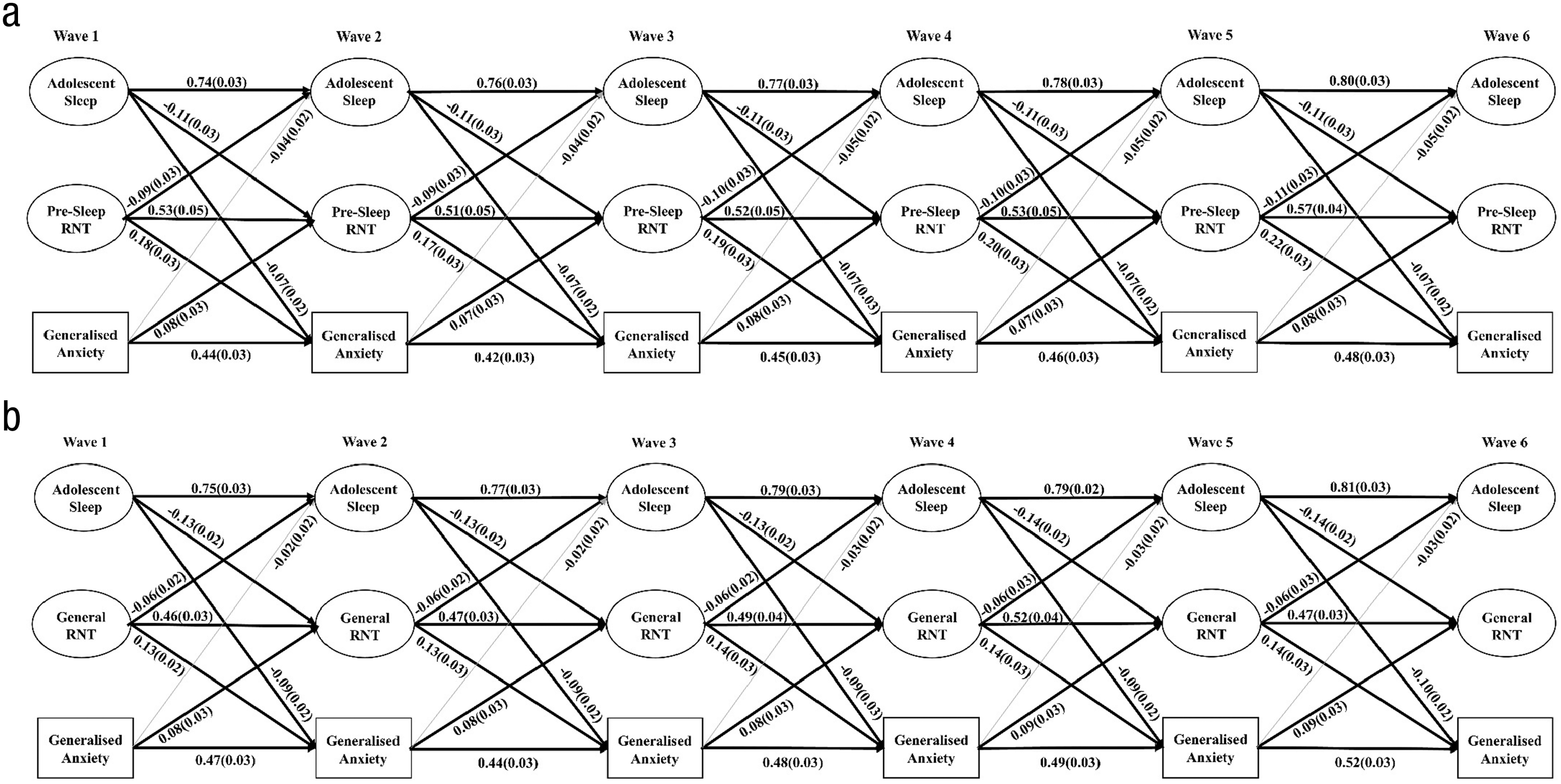
Schematic illustrating statistically significant relationships between (a) adolescent sleep, presleep repetitive negative thinking, and symptoms of generalized anxiety and (b) adolescent sleep, general repetitive negative thinking, and symptoms of generalized anxiety from Wave 1 to Wave 6. Solid black lines = significant paths; gray lines = nonsignificant paths. Standardized beta coefficients are presented with standard errors in parentheses.
Because presleep RNT predicted sleep, which, in turn, predicted symptoms of generalized anxiety, this mediation pathway was also explored. Estimates of the indirect paths from presleep RNT to generalized anxiety indicated that sleep partially mediated the association across all waves (Wave 1 to Wave 3: β = −0.006, SE = 0.003, p = .019; Wave 2 to Wave 4: β = −0.006, SE = 0.003, p = .020; Wave 3 to Wave 5: β = −0.007, SE = 0.003, p = .020; and Wave 4 to Wave 6: β = −0.007, SE = 0.003, p = .017).
General RNT
The model estimating the associations between the latent sleep factor, general RNT, and generalized-anxiety symptoms produced an acceptable fit to the data, χ2(N = 528) = 1,482.65, df = 1,043, CFI = .97, RMSEA = .028. All factor loadings were positive and significant, ranging from 0.34 to 0.92. As shown in Figure 2b and Table S2 (in the Supplemental Material), there were significant bidirectional associations between sleep and general RNT across all consecutive waves. Both sleep and general RNT significantly predicted levels of generalized anxiety across all waves, and generalized anxiety predicted higher general RNT 12 months later across each wave. There were no significant cross-lagged paths from generalized anxiety to sleep. The indirect path from sleep to generalized anxiety was partially mediated by general RNT from Wave 1 to Wave 3 (β = −0.01, SE = 0.003, p < .001), Wave 2 to Wave 4 (β = −0.01, SE = 0.004, p < .001), Wave 3 to Wave 5 (β = −0.01, SE = 0.004, p < .001), and Wave 4 to Wave 6 (β = −0.01, SE = 0.003, p < .001). In contrast, the indirect path from generalized anxiety to adolescent sleep was not mediated by general RNT from Wave 1 to Wave 3 (β = −0.008, SE = 0.004, p = .044), Wave 2 to Wave 4 (β = −0.008, SE = 0.004, p = .044), Wave 3 to Wave 5 (β = −0.008, SE = .004, p = .044), or Wave 4 to Wave 6 (β = −0.008, SE = 0.004, p = .044).
Because general RNT predicted sleep, which, in turn, predicted symptoms of generalized anxiety, this mediation pathway was also explored. Estimates of the indirect paths from general RNT to generalized anxiety indicated that sleep partially mediated the association across all waves (Wave 1 to Wave 3: β = 0.005, SE = 0.002, p = .021; Wave 2 to Wave 4: β = 0.005, SE = 0.002, p = .021; Wave 3 to Wave 5: β = 0.006, SE = 0.002, p = .021; and Wave 4 to Wave 6: β = 0.006, SE = 0.003, p = .021).
Social-anxiety symptoms
Presleep RNT
The model that included the latent sleep and presleep RNT factors and social-anxiety symptoms demonstrated acceptable model fit: χ2(N = 528) = 2,410.32, df = 1,336, CFI = .93, RMSEA = .039, and factor loading across all waves were significant, ranging from 0.34 to 0.93. Significant paths are depicted in Figure 3a; for standardized coefficients for all autoregressive and cross-lagged paths, see Table S3 in the Supplemental Material. Across all waves, worse adolescent sleep predicted increases in presleep RNT the subsequent year, which, in turn, predicted increases in symptoms of social anxiety. Adolescent sleep also directly predicted increases in social anxiety, and social anxiety predicted increases in presleep RNT. The relationship between sleep and presleep RNT was mutually reinforcing; presleep RNT also predicted worsening sleep over time. Symptoms of social anxiety did not directly predict adolescent sleep. The indirect path from adolescent sleep to social anxiety was partially mediated by presleep RNT from Wave 1 to Wave 3 (β = −0.012, SE = 0.003, p < .001), Wave 2 to Wave 4 (β = −0.012, SE = 0.003, p < .001), Wave 3 to Wave 5 (β = −0.012, SE = 0.003, p < .001), and Wave 4 to Wave 6 (β = −0.012, SE = 0.003, p < .001). In contrast, the indirect path from social anxiety to adolescent sleep was not mediated by presleep RNT from Wave 1 to Wave 3 (β = −0.005, SE = 0.003, p = .075), Wave 2 to Wave 4 (β = −0.005, SE = 0.003, p = .073), Wave 3 to Wave 5 (β = −0.005, SE = 0.003, p = .076), or Wave 4 to Wave 6 (β = −0.005, SE = 0.003, p = .076).
Schematic illustrating statistically significant relationships between (a) adolescent sleep, presleep repetitive negative thinking, and symptoms of social anxiety and (b) adolescent sleep, general repetitive negative thinking, and symptoms of social anxiety from Wave 1 to Wave 6. Solid black lines = significant paths; gray lines = nonsignificant paths. Standardized beta coefficients are presented with standard errors in parentheses.
Because presleep RNT predicted sleep, which, in turn, predicted symptoms of social anxiety, this mediation pathway was also explored. Estimates of the indirect paths from presleep RNT to generalized anxiety indicated that sleep did not mediate the association at any of the waves (Wave 1 to Wave 3: β = −0.004, SE = 0.002, p = .062; Wave 2 to Wave 4: β = −0.004, SE = 0.002, p = .066; Wave 3 to Wave 5: β = −0.004, SE = 0.002, p = .069; and Wave 4 to Wave 6: β = −0.004, SE = 0.002, p = .063).
General RNT
The model that included the latent sleep and general RNT factors and social-anxiety symptoms demonstrated acceptable model fit: χ2(N = 528) = 1,484.86, df = 1,043, CFI = .97, RMSEA = .028, and factor loadings across all waves were significant, ranging from 0.34 to 0.90. Significant paths are depicted in Figure 3b; for standardized coefficients for all autoregressive and cross-lagged paths, see Table S4 in the Supplemental Material. Across all waves, worse adolescent sleep predicted more general RNT, which, in turn, predicted increases in symptoms of social anxiety. Yet worse adolescent sleep also directly predicted increases in symptoms of social anxiety. The relationship between social anxiety and general RNT was mutually reinforcing; general RNT predicted worsened social anxiety, and social anxiety predicted increases in general RNT over time. All other cross-lagged paths in the model were nonsignificant. Neither social anxiety nor general RNT predicted adolescent sleep over time. The indirect path from adolescent sleep to social anxiety was partially mediated by general RNT from Wave 1 to Wave 3 (β = −0.01, SE = 0.002, p < .001), Wave 2 to Wave 4 (β = −0.01, SE = 0.002, p < .001), Wave 3 to Wave 5 (β = −0.01, SE = 0.002, p < .001), and Wave 4 to Wave 6 (β = −0.01, SE = 0.002, p < .001).
Depression symptoms
Presleep RNT
The model that included the latent sleep and presleep RNT factors and depressive symptoms demonstrated acceptable model fit: χ2(N = 528) = 2,564.42, df = 336, CFI = .92, RMSEA = .042, and factor loadings across all waves were significant, ranging from 0.34 to 0.92. Significant paths are depicted in Figure 4a; for standardized coefficients for all autoregressive and cross-lagged paths, see Table S5 in the Supplemental Material. Across all waves, worse adolescent sleep predicted increases in presleep RNT, which, in turn, predicted increases in symptoms of depression. Worse adolescent sleep was also directly related to worsening symptoms of depression, whereas worse depression predicted improvements in sleep over time. The relationship between sleep and presleep RNT was mutually reinforcing; presleep RNT also predicted worsening sleep over time. The relationship between depressive symptoms and presleep RNT was nonsignificant. The indirect path from adolescent sleep to depression was partially mediated by presleep RNT from Wave 1 to Wave 3 (β = −0.03, SE = 0.007, p < .001), Wave 2 to Wave 4 (β = −0.03, SE = 0.007, p < .001), Wave 3 to Wave 5 (β = −0.03, SE = 0.007, p < .001), and Wave 4 to Wave 6 (β = −0.03, SE = 0.007, p < .001).
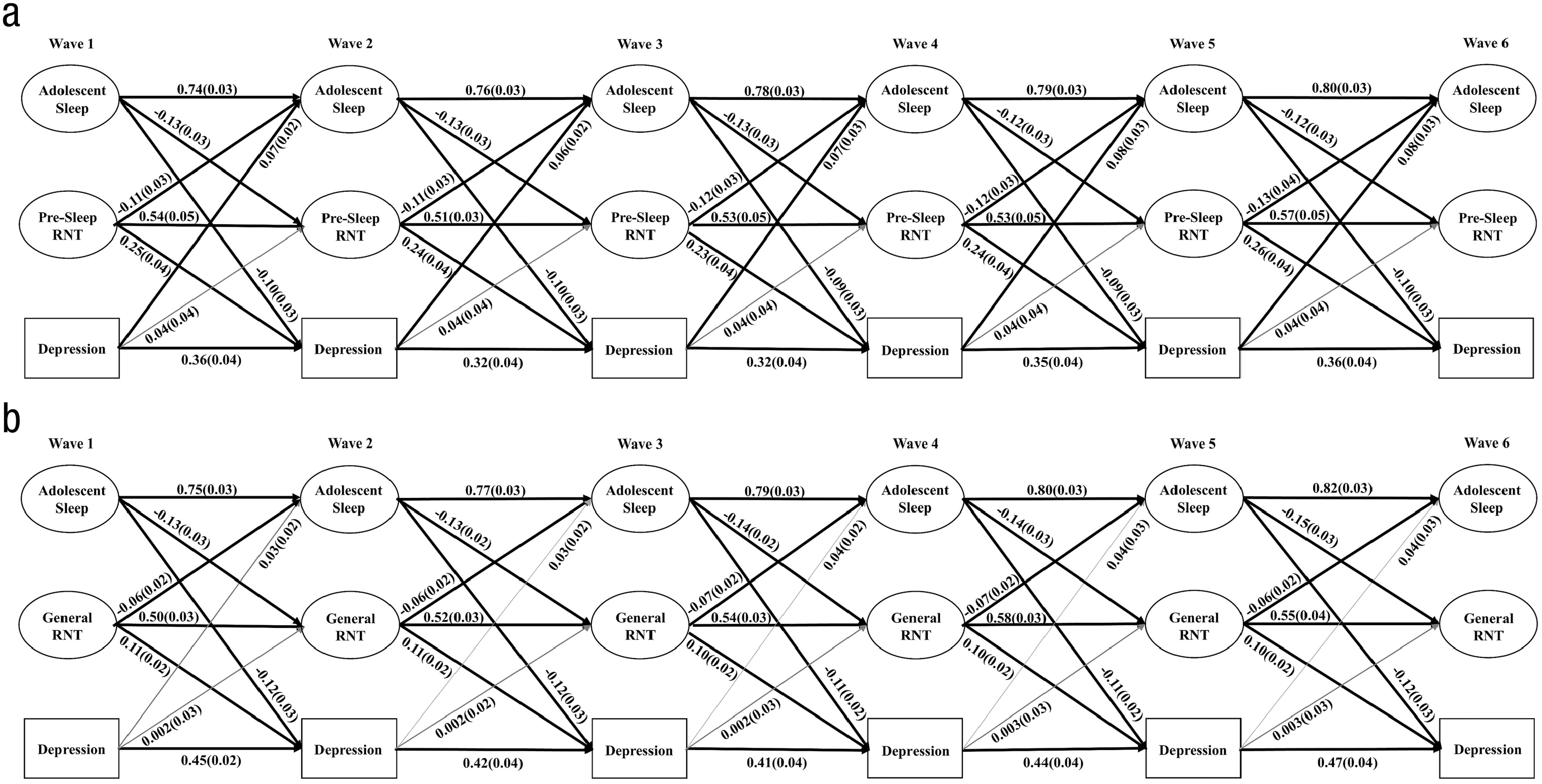
Schematic illustrating statistically significant relationships between (a) adolescent sleep, presleep repetitive negative thinking, and symptoms of depression and (b) adolescent sleep, general repetitive negative thinking, and symptoms of depression from Wave 1 to Wave 6. Solid black lines = significant paths; gray lines = nonsignificant paths. Standardized beta coefficients are presented with standard errors in parentheses.
Because presleep RNT predicted sleep, which, in turn, predicted symptoms of depression, this mediation pathway was also explored. Estimates of the indirect paths from presleep RNT to generalized anxiety indicated that sleep mediated the association across all waves (Wave 1 to Wave 3: β = −0.01, SE = 0.004, p = .006; Wave 2 to Wave 4: β = −0.01, SE = 0.004, p = .006; Wave 3 to Wave 5: β = −0.01, SE = 0.004, p = .006; and Wave 4 to Wave 6: β = −0.01, SE = 0.004, p = .005).
General RNT
The model that included the latent sleep and general RNT factors and depressive symptoms demonstrated acceptable model fit: χ2(N = 528) = 1,466.99, df = 1,043, CFI = .97, RMSEA = .028, and factor loadings across all waves were significant, ranging from 0.34 to 0.92. Significant paths are depicted in Figure 4b; for standardized coefficients for all autoregressive and cross-lagged paths, see Table S6 in the Supplemental Material. Across all waves, worse adolescent sleep predicted increases in general RNT, which, in turn, predicted increases in symptoms of depression. Worse adolescent sleep was also directly related to worsening symptoms of depression, whereas symptoms of depression did not predict changes in adolescent sleep or general RNT over time. The relationship between sleep and general RNT was mutually reinforcing; general RNT also predicted worsening sleep over time. The indirect path from adolescent sleep to depression was partially mediated by general RNT from Wave 1 to Wave 3 (β = −0.02, SE = 0.004, p < .001), Wave 2 to Wave 4 (β = −0.02, SE = 0.004, p < .001), Wave 3 to Wave 5 (β = −0.02, SE = 0.004, p < .001), and Wave 4 to Wave 6 (β = −0.02, SE = 0.004, p < .001).
Because general RNT predicted sleep, which, in turn, predicted symptoms of depression, this mediation pathway was also explored. Estimates of the indirect paths from general RNT to depression indicated that sleep partially mediated the association across all waves (Wave 1 to Wave 3: β = 0.007, SE = 0.003, p = .009; Wave 2 to Wave 4: β = 0.007, SE = 0.003, p = .008; Wave 3 to Wave 5: β = 0.007, SE = 0.003, p = .008; and Wave 4 to Wave 6: β = 0.008, SE = 0.003, p = .009).
Eating-disorder symptoms
Presleep RNT
The model that included the latent sleep and presleep RNT factors and eating-disorder symptoms demonstrated acceptable model fit: χ2(N = 528) = 2,485.10, df = 1,336, CFI = .92, RMSEA = .040, and factor loadings across all waves were significant, ranging from 0.34 to 0.93. Significant paths are depicted in Figure 5a; for standardized coefficients for all autoregressive and cross-lagged paths, see Table S7 in the Supplemental Material. Across all waves, worse adolescent sleep predicted more presleep RNT, which, in turn, predicted increases in eating-disorder symptoms. Worse adolescent sleep was also directly related to worsening eating-disorder symptoms, whereas eating-disorder symptoms did not predict changes in adolescent sleep or presleep RNT over time. The relationship between sleep and presleep RNT was mutually reinforcing; presleep RNT also predicted worsening sleep over time. The indirect path from adolescent sleep to eating-disorder symptoms was partially mediated by presleep RNT from Wave 1 to Wave 3 (β = −0.04, SE = 0.013, p = .001), Wave 2 to Wave 4 (β = −0.04, SE = 0.013, p = .001), Wave 3 to Wave 5 (β = −0.04, SE = 0.013, p = .001), and Wave 4 to Wave 6 (β = −0.04, SE = 0.013, p = .001).
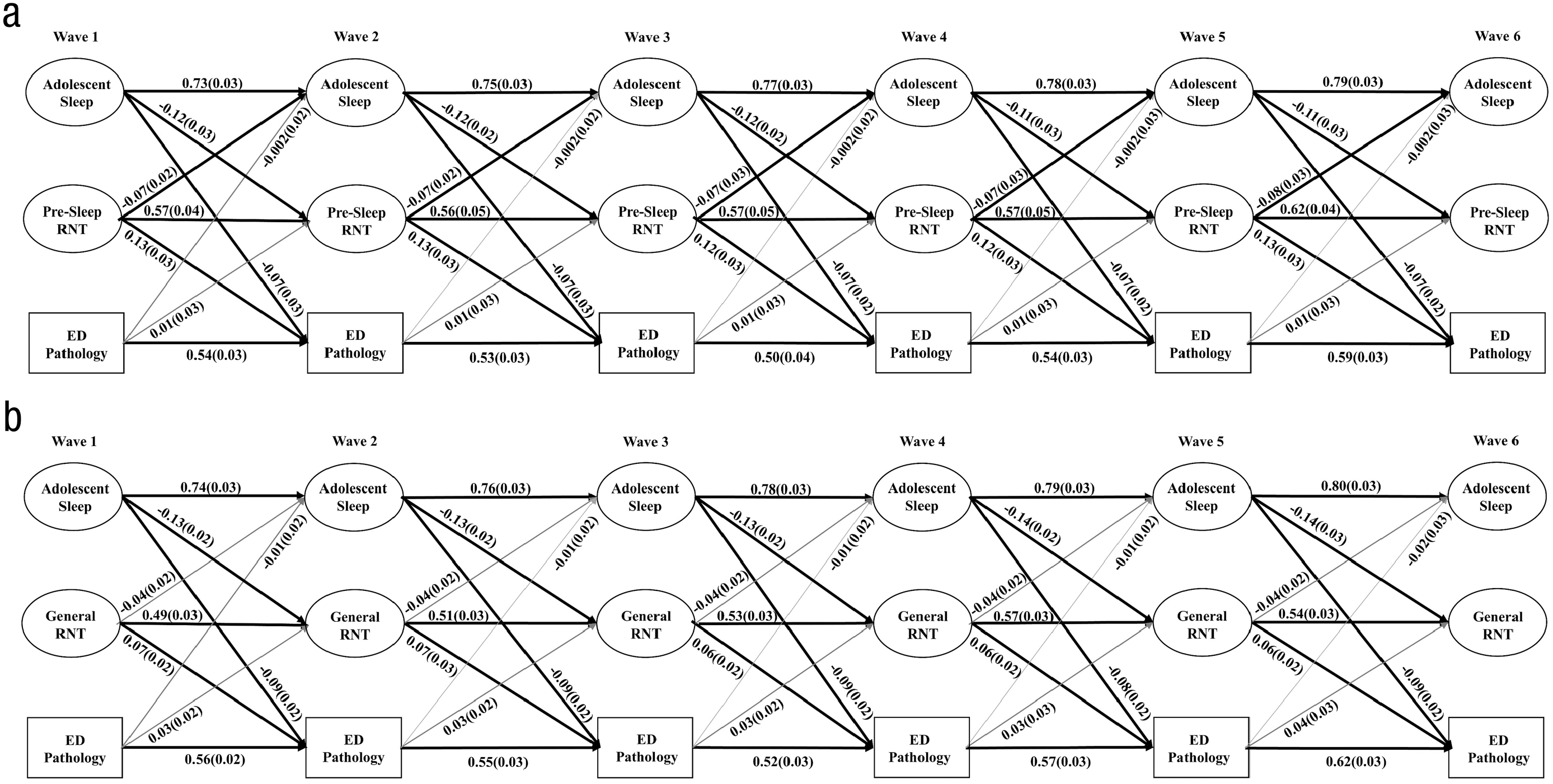
Schematic illustrating statistically significant relationships between (a) adolescent sleep, presleep repetitive negative thinking, and eating-disorder symptoms and (b) adolescent sleep, general repetitive negative thinking, and eating-disorder symptoms from Wave 1 to Wave 6. Solid black lines = significant paths; gray lines = nonsignificant paths. Standardized beta coefficients are presented with standard errors in parentheses.
Because presleep RNT predicted sleep, which, in turn, predicted eating-disorder symptoms, this mediation pathway was also explored. Estimates of the indirect paths from presleep RNT to eating-disorder symptoms indicated that sleep did not mediate the association at any of the waves (Wave 1 to Wave 3: β = −0.005, SE = 0.002, p = .052; Wave 2 to Wave 4: β = −0.004, SE = 0.002, p = .053; Wave 3 to Wave 5: β = −0.005, SE = 0.002, p = .058; and Wave 4 to Wave 6: β = −0.005, SE = 0.003, p = .056).
General RNT
The model that included the latent sleep and general RNT factors and eating-disorder symptoms demonstrated an acceptable model fit: χ2(N = 528) = 1,478.22, df = 1,043, CFI = .97, RMSEA = .028, and factor loadings across all waves were significant, ranging from 0.34 to 0.92. Significant paths are depicted in Figure 5b; for standardized coefficients for all autoregressive and cross-lagged paths, see Table S8 in the Supplemental Material. Across all waves, worse adolescent sleep predicted more general RNT, which, in turn, predicted increases in eating-disorder symptoms. Worse adolescent sleep was also directly related to worsening eating-disorder symptoms. In contrast, eating-disorder symptoms did not predict changes in adolescent sleep or general RNT over time, and general RNT did not predict changes in sleep. The indirect path from adolescent sleep to eating-disorder symptoms was partially mediated by general RNT from Wave 1 to Wave 3 (β = −0.03, SE = 0.009, p = .009), Wave 2 to Wave 4 (β = −0.03, SE = 0.009, p = .009), Wave 3 to Wave 5 (β = −0.03, SE = 0.009, p = .009), and Wave 4 to Wave 6 (β = −0.03, SE = 0.009, p = .009).
Discussion
In this six-wave longitudinal study, we investigated whether sleep disturbance (i.e., evening diurnal preference, shorter school-night sleep duration, daytime sleepiness) predicted increases in symptoms of generalized and social anxiety, depression, and eating disorders over 5 years, spanning early to middle adolescence. These disorders, referred to as “social-emotional disorders,” share common risk factors, and the incidence of these disorders sharply increases in adolescence (Rapee et al., 2019). To elucidate mechanisms linking sleep disturbance with increased risk for social-emotional disorders in adolescence, both presleep and general RNT were examined as separate mediators of this association.
Worse adolescent sleep in the current study was cross-sectionally associated with greater severity of generalized anxiety, social anxiety, depression, and eating-disorder symptoms. Supporting previous findings, we found that adolescent sleep disturbance was associated with both presleep and general RNT (Richardson & Gradisar, 2021) and that both forms of RNT were associated with symptoms of all four social-emotional disorders (Raes et al., 2020; Sala et al., 2019; Spinhoven et al., 2018).
Longitudinally, sleep disturbance consistently (i.e., across all waves and forms of social-emotional disorders) predicted increases in symptoms of generalized anxiety, social anxiety, depression, and eating disorders both directly and indirectly through presleep and general RNT. These results support prior longitudinal research, which suggests sleep disturbance in middle adolescence is a risk factor for anxiety and depression in older adolescence and young adulthood (Orchard et al., 2020). Yet the current study extends these findings by showing that sleep is a robust risk factor for anxiety and depression across the course of early to middle adolescence and furthermore, that sleep disturbance is also a risk factor for eating-disorder pathology across this developmental period (i.e., not just anxiety and depression).
The finding that RNT mediates the relationship between sleep disturbance and symptoms of social-emotional disorders in adolescence supports findings from Danielsson and colleagues (2013), who found that catastrophic worry (i.e., a form of RNT) mediates the relationship between sleep and depression in older adolescents (16–18 years old). However, again, the current study demonstrates that this pathway holds across early to middle adolescence and also applies to symptoms of generalized anxiety, social anxiety, and eating disorders. These findings support the conceptual model of social-emotional disorders (Rapee et al., 2019) by demonstrating that sleep disturbance and RNT are common risk factors for generalized anxiety, social anxiety, depression, and eating disorder in adolescence.
A strength of the current research is that sleep was comprehensively measured via a latent factor (i.e., rather than with a single item), making use of validated questionnaires. Furthermore, longitudinal models were analyzed using cross-lagged panel models, which specify relationships between all factors at each time point (i.e., rather than specifying only hypothesized paths). Thus, the current study provides the most robust evidence for RNT as a transdiagnostic mediator of the relationship between sleep disturbance and social-emotional disorders in young people to date.
Cross-lagged panel models also examine the possibility of bidirectionality. Although there is certainly evidence of bidirectionality between sleep and anxiety and depression (e.g., Kortesoja et al., 2020; Peltz et al., 2017), there was no evidence in the current study that symptoms of generalized anxiety, social anxiety, depression, or eating disorders predicted worsening of sleep over time either directly or indirectly through RNT. In fact, the model that examined presleep RNT and depression suggested that higher symptoms of depression predicted improvements in sleep over time. This might reflect the episodic nature of depression (i.e., improvements in sleep occur alongside improvements in or resolution of depression) or possibly that individuals high on depression tend to sleep longer (sleep duration was one of our three sleep indicators). Yet the same path did not emerge in the general RNT and depression model, which suggests this path was not stable or reliable. Thus, replication of this finding is needed.
The pattern of significant direct paths made it possible to test sleep as a mediator of the relationship between RNT and social-emotional disorders in six of the eight longitudinal models. Results suggested that sleep mediated the relationship between both presleep and general RNT and symptoms of generalized anxiety and depression but not social anxiety or eating disorders. These results support the notion that RNT may impair sleep over time and that sleep disturbance may increase risk for social-emotional disorders (Valck et al., 2004; Wuyts et al., 2012), yet there was more consistent evidence of RNT as a mediator rather than sleep.
Although the exact pattern of findings was not consistent across all models, there was evidence that RNT and sleep form a mutually reinforcing cycle and that generalized and social anxiety and RNT reinforce one another. In comparing the strength of beta weights, if their confidence intervals overlapped by less than 50%, differences can be considered statistically significant (Cumming, 2009). Accordingly, the paths from sleep to general RNT across all models was significantly stronger (i.e., medium to large) than the paths from general RNT to sleep (i.e., small to medium), although the paths between sleep and presleep RNT were not significantly different from one another. Furthermore, the paths from presleep RNT to symptoms of generalized anxiety and social anxiety were significantly stronger (i.e., large) than the paths from generalized/social anxiety to presleep RNT (i.e., small to medium), although the paths between generalized/social anxiety and general RNT were not significantly different. These findings suggest that targeting RNT may help to de-escalate the progression of sleep disturbance and generalized and social anxiety in adolescence. It was somewhat surprising that symptoms of depression and eating disorders did not predict increases in RNT over time. These results support previous findings that suggest RNT is an important risk factor (Raes et al., 2020; Sala et al., 2019; Spinhoven et al., 2018) and suggest that RNT may be a more robust predictor of depression and eating disorders than the inverse.
It is important to consider the size of the effects observed in the longitudinal models. Relationships from sleep to generalized anxiety, social anxiety, depression, and eating-disorder pathology were moderate in size, with large relationships from sleep to RNT. It was hypothesized that the relationship from sleep to presleep RNT would be stronger than the relationship from sleep to general RNT; however, there was little evidence of this (all paths βs ≈ 0.11–0.13). However, there was some evidence that the relationship from presleep RNT to symptoms of social-emotional disorders was stronger than from general RNT to symptoms of social-emotional disorders. This was particularly the case for depression, whereby the path coefficient for presleep RNT was double the coefficient for general RNT (β = 0.24 vs. β = 0.10, respectively). It should be acknowledged that all of the coefficients from RNT to symptoms of social-emotional disorders were moderate to large in size, suggesting both general and presleep RNT are important risk factors for social-emotional disorders. However, these results do suggest that presleep RNT may be a particularly robust risk factor for depression, supporting Lovato and Gradisar’s (2014) theoretical model.
Clinical implications
Given that results showed sleep disturbance predicted increases in generalized anxiety, social anxiety, depression, and eating-disorder pathology from early to middle adolescence, both directly and indirectly through RNT, the current study adds to the growing evidence base that highlights sleep as a robust risk/protective factor for mental health in adolescence (Blake & Allen, 2020). Thus, results support the inclusion of sleep strategies in mental-health prevention and intervention programs. There is a large body of evidence to suggest that nonpharmacological sleep interventions improve symptoms of depression and anxiety (Gee et al., 2019; Staines et al., 2021), including in young people (Blake & Allen, 2020) and across both clinical and nonclinical populations, suggesting sleep treatments can be used in both the prevention and alleviation of mental-health problems. Fortunately, nonpharmacological sleep interventions are becoming more accessible; a recent evaluation of Sleep Ninja, a digital sleep intervention based on cognitive-behavioral therapy for insomnia, in adolescents (12–16 years old) showed improvements in depression, which were mediated by improvements in insomnia (Werner-Seidler et al., 2023) and RNT (Li et al., 2023). Although there is a robust evidence base supporting the use of sleep treatments for depression and anxiety, the evidence base for eating disorders is much more limited. Yet results from the current study suggest that targeting sleep may reduce young people’s risk for eating-disorder symptoms, too.
Results from the current study also inform conceptualizations of how sleep conveys risk for social-emotional disorders in adolescence, which is likely to influence prevention and treatment approaches. RNT has been established as an important risk factor in its own right; yet results from the current study suggest that sleep disturbance may partly contribute to RNT and, in turn, symptoms of social-emotional disorders. In addition, RNT further contributes to worsening in sleep over time. Given that both sleep disturbance and RNT convey risk together, prevention and intervention approaches could aim to target both of these transdiagnostic processes to more effectively reduce the incidence of generalized anxiety, social anxiety, depression, and eating disorders in young people.
Limitations and future directions
Although the current study has several strengths, including the multicomponent measurement of sleep and six-wave longitudinal cross-lagged design, there are limitations to acknowledge. That is, all constructs were measured via self-report, which may have inflated the strength of associations (e.g., common-rater bias). Self-report measures of symptoms of social-emotional disorders are not diagnostic, and the ChEAT does not measure all symptoms of eating disorders. Furthermore, the sleep latent factor comprised only three sleep-related constructs, and operationalizing sleep through a latent factor prevented examination of the unique relationship between each sleep construct and RNT and social-emotional disorders. Future studies could include sleep diaries, which are less prone to cognitive (i.e., memory) biases, and objective means, such as actigraphy or wearable EEG devices. Sleep diaries and actigraphy could provide insight into specific sleep parameters linked with RNT and social-emotional disorders (e.g., wakefulness in bed, short sleep duration), whereas sleep EEG could allow evaluation of how developmental changes in sleep architecture (e.g., amount of deep and REM sleep) are linked to increased risk for social-emotional disorders (Blake et al., 2018; Marver & McGlinchey, 2020).
The current study spanned early to middle adolescence, so it is unclear whether these relationships hold in older adolescence and early adulthood. Although past research suggests adolescent sleep is a risk/protective factor for depression and anxiety in early adulthood (Orchard et al., 2020), future longitudinal research could aim to measure sleep, symptoms of social-emotional disorders, and candidate mechanisms across the entire course of adolescence and early adulthood. Furthermore, because of the overarching study design, there were 1-year lags between each follow-up. However, sleep, RNT, and symptoms of social-emotional disorders are likely to interact with one another across a shorter time scale, so future research might also like to use shorter lags between follow-ups or make use of other research designs (e.g., ecological momentary assessment).
Because sleep disturbance directly predicted increases in generalized anxiety, social anxiety, depression, and eating disorders even after accounting for the role of RNT, future research could aim to identify other mechanisms. Blake and colleagues (2018) proposed a large number of candidate mechanisms (e.g., cognitive style, executive dysfunction, emotion dysregulation, negative emotionality, social withdrawal and amotivation, hyperarousal, cognitive biases) linking insomnia with depression and anxiety in young people, yet further longitudinal and experimental studies are needed to fully understand how sleep conveys risk for social-emotional disorders in adolescence.
Conclusions
Results from the current study suggest sleep disturbance is a robust risk factor for symptoms of generalized anxiety, social anxiety, depression, and eating disorders in early to middle adolescence. Furthermore, sleep disturbance is likely to increase risk for social-emotional disorders partly because of increases in both general and presleep RNT. Inversely, there was no evidence that symptoms of generalized anxiety, social anxiety, depression, and eating disorders led to worsening of sleep. Findings support the use of nonpharmacological sleep interventions in the prevention and treatment of social-emotional disorders in adolescence.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026241230458 – Supplemental material for Repetitive Negative Thinking Mediates the Relationship Between Sleep Disturbance and Symptoms of Generalized Anxiety, Social Anxiety, Depression, and Eating Disorders in Adolescence: Findings From a 5-Year Longitudinal Study
Supplemental material, sj-docx-1-cpx-10.1177_21677026241230458 for Repetitive Negative Thinking Mediates the Relationship Between Sleep Disturbance and Symptoms of Generalized Anxiety, Social Anxiety, Depression, and Eating Disorders in Adolescence: Findings From a 5-Year Longitudinal Study by Cele Richardson, Natasha R. Magson, Ella Oar, Jasmine Fardouly, Carly Johnco, Justin Freeman and Ron M. Rapee in Clinical Psychological Science
Footnotes
Acknowledgements
The Risks to Adolescent Wellbeing Project team would like to thank our brilliant participants and all of the dedicated research assistants and interns who have worked on this project.
Transparency
Action Editor: Jennifer Lau
Editor: Jennifer L. Tackett
Author Contributions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.