
Abstract
Caring for a person with dementia (PWD) can produce declines in caregivers’ emotional well-being and physical functioning, which could result from disruptions in the emotional linkage between PWDs and caregivers. We examined the effects of interpersonal linkage in emotional behaviors on emotional well-being and physical functioning in caregivers and control partners. Forty-five PWD–caregiver dyads and 12 control dyads had a 10-min unrehearsed conflict conversation in the laboratory. We quantified positive and negative emotional linkage as the covariation between objectively coded positive and negative emotional behaviors during the conversation. Caregivers and one partner in the control dyads completed questionnaires concerning their emotional well-being and physical functioning. We found that lower positive emotional linkage was associated with lower emotional well-being in caregivers and control partners. We did not find similar effects with negative emotional linkage or for physical functioning. We offer possible explanations for these findings and implications for assessing caregiver risk.
As the aging population continues to grow, the number of persons with dementia (PWDs) and the number of family caregivers are rising dramatically. Dementias are progressive, debilitating conditions that cause profound changes in cognitive, social, emotional, and physical functioning. Providing care for a loved one with dementia can be a meaningful part of family life (Quinn & Toms, 2019; Shim et al., 2013). However, caregiving can also be highly burdensome, leading to declines in caregivers’ emotional well-being and physical functioning (Schulz et al., 2020). Declines in caregiver emotional well-being and physical functioning may further lead to greater mortality for PWDs (Lwi et al., 2017). Therefore, there is an urgent need to identify risk factors for adverse outcomes in family caregivers.
Factors Contributing to Adverse Caregiver Outcomes
Because dementias can produce impairment in multiple aspects of PWDs’ functioning, changes in emotional functioning may be particularly challenging for family caregivers, even more so than declines in cognitive functioning (Ornstein & Gaugler, 2012; Schulz et al., 1995). Our previous work has examined PWDs’ emotional functioning and found that caregivers had lower emotional well-being when they were caring for PWDs who were impaired in the ability to (a) generate appropriate emotional responses (Chen, Wells, et al., 2017; Lwi et al., 2018), (b) adjust emotional responses to meet situational demands (Otero & Levenson, 2017), and (c) identify emotions in others (Brown et al., 2018). We have also examined caregivers’ emotional functioning and found that poorer caregiver emotion regulation and greater reactivity to others’ distress were associated with caregivers having more anxiety and depressive symptoms (Hua et al., 2021; Wells et al., 2020). Dementia may also disrupt the emotional connection between PWDs and their caregivers; however, whether and how these disruptions influence caregivers’ emotional well-being and physical functioning has not been determined.
Emotional Linkage, Emotional Well-Being, and Physical Functioning
Emotional linkage is an important aspect of emotional connection. It refers to the degree to which two individuals’ emotions, either positive or negative, change in coordinated ways during dyadic interactions. For example, people’s positive emotions can become linked when laughing at the same humorous event or when one person shares a proud experience and the other person expresses affection. On the other hand, people’s negative emotions can become linked when one person expresses anger and the other person also expresses anger or another negative emotion at the same time. Past research that has quantified emotional linkage in this way among married couples has found a robust association between higher negative emotional linkage and adverse outcomes across various aspects of mental and physical health (for a review of couple relationships and health, see Kiecolt-Glaser & Wilson, 2017). In a recent longitudinal study with neurotypical dyads discussing a relational conflict, we (Wells et al., 2022) found that lower positive emotional linkage, indexed by less simultaneous experiences and expressions of positive emotions, predicted less favorable trajectories of health and shorter longevity in spouses.
Emotions are short-lived phenomena that can produce changes in multiple response systems, including physiological responses, subjective experiences, and expressive behaviors (Levenson, 2014; Levenson et al., 2016). Therefore, emotional linkage may occur in any of these response systems. Note that even within the same affective valence, emotional linkage in dyads can occur in two distinct forms. The emotions of two individuals can be “in-phase” linked, meaning that their emotions increase together and decrease together. On the other hand, a dyad’s emotions can be “anti-phase” linked, meaning that as one person’s emotions increase, the other person’s emotions decrease (Reed et al., 2013). Although most past research on emotional linkage has not distinguished between these two forms of linkage, those that distinguished them have found that different forms of linkage may reflect different psychosocial processes (Chen, Brown et al., 2021; Reed et al., 2013). For example, in-phase linkage tends to occur when one person socially influences another, whereas anti-phase linkage tends to occur during turn-taking (Reed et al., 2013). Of direct relevance to the present study, in a recent study in which physiological linkage between PWDs and their caregivers during daily interactions was investigated, we (Chen, Casey, et al., 2022) found that lower in-phase linkage, but not anti-phase linkage, was associated with greater severity of anxiety symptoms in caregivers.
Altered Emotional Linkage Between PWDs and Caregivers
Dementia produces profound damage to the PWD’s brain (Seeley et al., 2009; Zhou & Seeley, 2014) and a wide range of impairments, including those in the emotional domain (Levenson et al., 2014). Given the important social role of emotions, it is likely that these impairments lead to altered emotional linkage between PWDs and their caregivers (Pressman et al., 2018). For example, PWDs’ inability to understand and anticipate caregivers’ emotions (Chen, Hua, et al., 2022; Goodkind et al., 2015) may reduce the dyad’s positive emotional linkage. In addition, PWDs’ inability to recognize and regulate their own emotions (Chen, Lwi et al., 2017; Otero & Levenson, 2019) may increase the dyad’s negative emotional linkage.
Altered emotional linkage between PWDs and caregivers may negatively affect caregivers’ emotional well-being and physical functioning. In the above-mentioned study of PWD–caregiver physiological linkage (Chen, Casey, et al., 2022), we examined linkage in somatic activity, which often increased during moments when dyads exhibited shared emotional behaviors (Chen, Brown, et al., 2021). We found that lower PWD–caregiver linkage in somatic activity was associated with greater severity of caregiver anxiety symptoms. In addition, emotional linkage among loved ones, particularly when the emotions are positive, is typically considered a key element or manifestation of high relationship quality and interpersonal connectedness (Brown & Fredrickson, 2021; Fredrickson, 2016). Past caregiver research has used questionnaires and analyzed the frequency of using “we-ness” language during dyadic interactions to quantify dyads’ relationship quality and interpersonal connectedness, respectively. These studies found that dementia caregivers’ worse relationship quality (Mahoney et al., 2005; Seider et al., 2009) and lower interpersonal connectedness (Connelly et al., 2020) with the PWDs were both associated with more anxiety and depressive symptoms and experiencing more burden and strain in the caregivers.
The Present Study
In the present study, we examined whether lower emotional linkage between PWDs and their caregivers is associated with lower caregiver emotional well-being and physical functioning. We focused on spousal caregivers because they have frequent and intimate interactions with PWDs and may be more vulnerable to disrupted emotional linkage with PWDs than other kinds of caregivers (e.g., paid formal caregivers). Participants included PWDs, their spousal caregivers, and a group of healthy control (HC) participants and their spousal partners (referred to as “HC partners”). The inclusion of HC dyads enabled us to (a) determine the degree to which PWDs’ emotional linkage with their caregivers differs from neurotypical couples and (b) increase the range and variety of emotional linkage in study participants. The approach of including HC dyads has previously been used in studies of caregiver health (Brown et al., 2018; Chen, Wells, et al., 2017; Hua et al., 2019).
We focused on two major dimensional groupings of emotions—positive valence and negative valence—reflecting a distinction commonly found in the literature (Chen, Brown, et al., 2021; Fredrickson, 1998). We focused on linkage in emotional behaviors and quantified emotional linkage as the covariation of PWDs’ and caregivers’ objectively coded positive or negative expressive emotional behaviors. In dementia, damage to the brain and associated memory and/or language impairments typically undermine the accuracy of PWD self-report (Chen, Hua, et al., 2021; Chen, Lwi, et al., 2017; Levenson, 2007). By focusing on expressive emotional behaviors, rather than self-reported emotional experiences, we were able to quantify PWD–caregiver emotional linkage in a more objective and accurate manner. We focused on emotional linkage during a 10-min conversation in our laboratory about an area of relationship conflict. Previous research has demonstrated that couples typically exhibit a mixture of positive and negative emotions during discussions of relationship conflicts (Chen, Brown, et al., 2021; Levenson & Gottman, 1983). This type of conversation provided an ideal context to examine systematically the association between positive versus negative emotional linkage and caregivers’ well-being and physical functioning.
We hypothesized that lower positive and higher negative emotional linkage, particularly the in-phase linkage, would be associated with lower emotional well-being and worse physical functioning among the caregivers and HC partners. In preliminary analyses, we also compared PWDs with different dementia diagnoses with each other and with HCs to determine whether emotional linkage would differ among PWD-caregiver dyads and/or against neurotypical couples.
Data, Materials, Code, and Online Resources
Data and syntax (IBM SPSS, MATLAB) supporting our analyses are available at OSF (https://osf.io/gtbmr/?view_only=41a1a85223b5441ca2011c6ba43eadb3). The SPSS syntax is also shown in Syntax 1 through 3 in the Supplemental Material available online.
Method
Participants
Participants included 45 PWDs with either behavioral variant frontotemporal dementia (bvFTD; n = 23) or Alzheimer’s disease (AD; n = 22) and their spousal caregivers (n = 45). BvFTD is typically associated with greater social and emotional impairments than AD (Levenson et al., 2014). Therefore, including PWDs with both types of dementias helps increase the range and variety of PWDs’ emotional dysfunctions and therefore the emotional linkage with their caregivers. PWDs were recruited from the Memory and Aging Center (MAC) at the University of California, San Francisco (UCSF) for a collaborative research project conducted by the MAC and the Berkeley Psychophysiology Laboratory at the University of California, Berkeley (UCB). At UCSF, PWDs were assessed via neurological, neuropsychological, and neuroimaging testing and diagnosed using current research criteria for bvFTD (Rascovsky et al., 2011) and AD (McKhann et al., 2011). To further increase possible range of linkage, a comparison group of neurologically HCs (n = 14) and their spousal partners (n = 14) were recruited from the community.
Procedure
All participants first visited UCSF, where they completed detailed clinical interviews, a neurological examination, and a functional assessment. Within 4 and 12 months following the UCSF visit, respectively, PWD–caregiver dyads and control dyads visited UCB for a comprehensive daylong assessment of emotional functioning (Levenson, 2007). Informed consent was obtained upon arrival. All procedures were approved by the UCB Institutional Review Boards.
In the current study, we focused on a conflict conversation task during the UCB visit. In this task, the dyad sat facing each other in comfortable chairs in a laboratory room. A trained experimenter first interviewed the dyad to identify an area of unresolved conflict (e.g., communication, home improvements). The experimenter then left the room, and the dyad sat quietly for 5 min and then engaged in a 10-min unrehearsed conversation about the chosen topic. Each participant’s face and upper torso were recorded continuously using two remote-controlled video cameras that were partially concealed behind darkened glass.
Between the UCSF and UCB visits, caregivers completed questionnaires about their own emotional well-being and physical functioning and the quality of their relationship with the PWDs. For HC dyads, we randomly assigned one member of each dyad to answer the questionnaires. This person is referred to as “HC partner” or simply “partner” in this article.
Measures
Positive and negative emotional behaviors
Positive and negative emotional behaviors for each participant were coded by a team of trained coders who were blind to the research hypotheses using the Specific Affect Coding System (SPAFF; Coan & Gottman, 2007). SPAFF uses verbal content, voice tone, context, facial expression, gestures, and body movement to code emotional behaviors. For speakers, positive emotional codes include joy, humor, affection, interest, and validation; negative emotional codes include contempt, disgust, defensiveness, belligerence, domineering, anger, whining, sadness, fear/tension, and stonewalling. For listeners, emotional codes are positive emotion, negative emotion, and stonewalling. For both speaker and listener behaviors, the coders first identified the specific seconds during which a SPAFF-coded behavior started and ended and then determined the intensity of the behavior: 1 = low intensity, 2 = high intensity. Next, for each SPAFF code, we computed a second-by-second time series over the conversation using a 3-point scale in which 0 indicated that the code was absent, 1 indicated that the code was present at low intensity, and 2 indicated that the code was present at high intensity. To allow for assessment of interrater reliability, 47% of all conversations were coded by two coders. Cohen’s κ was computed for each participant to control for agreement by chance alone. The overall κ for second-by-second SPAFF coding was moderate, at .66, and overall agreement was high, at 78%.
Next, separately for each participant, we computed a second-by-second time series of positive emotional behaviors using binary scores in which 1 indicated the presence and 0 indicated the absence of any positive emotional behaviors for a given second (Fig. 1a). We collapsed the low- and high-intensity levels into a single binary score because theories have suggested that even small amounts of positive emotional behaviors benefit relationship quality and health (Fredrickson, 2016; Wells et al., 2022). Thus, in this study, we focused on presence versus absence rather than low intensity versus high intensity. Using the same method, we also computed a second-by-second time series of negative emotional behaviors. We have used the same approach previously in PWD–caregiver and neurotypical dyads (Chen, Brown, et al., 2021; Wells et al., 2022). To ensure our results based on the binary scores were robust, we also analyzed scores that included the intensity information. More specifically, in these additional analyses, emotional behaviors were scored on a scale of 0 to 2 in which 0 indicated absence, 1 indicated low intensity, and 2 indicated high intensity. Findings from these additional analyses are presented below in Robustness of Findings.
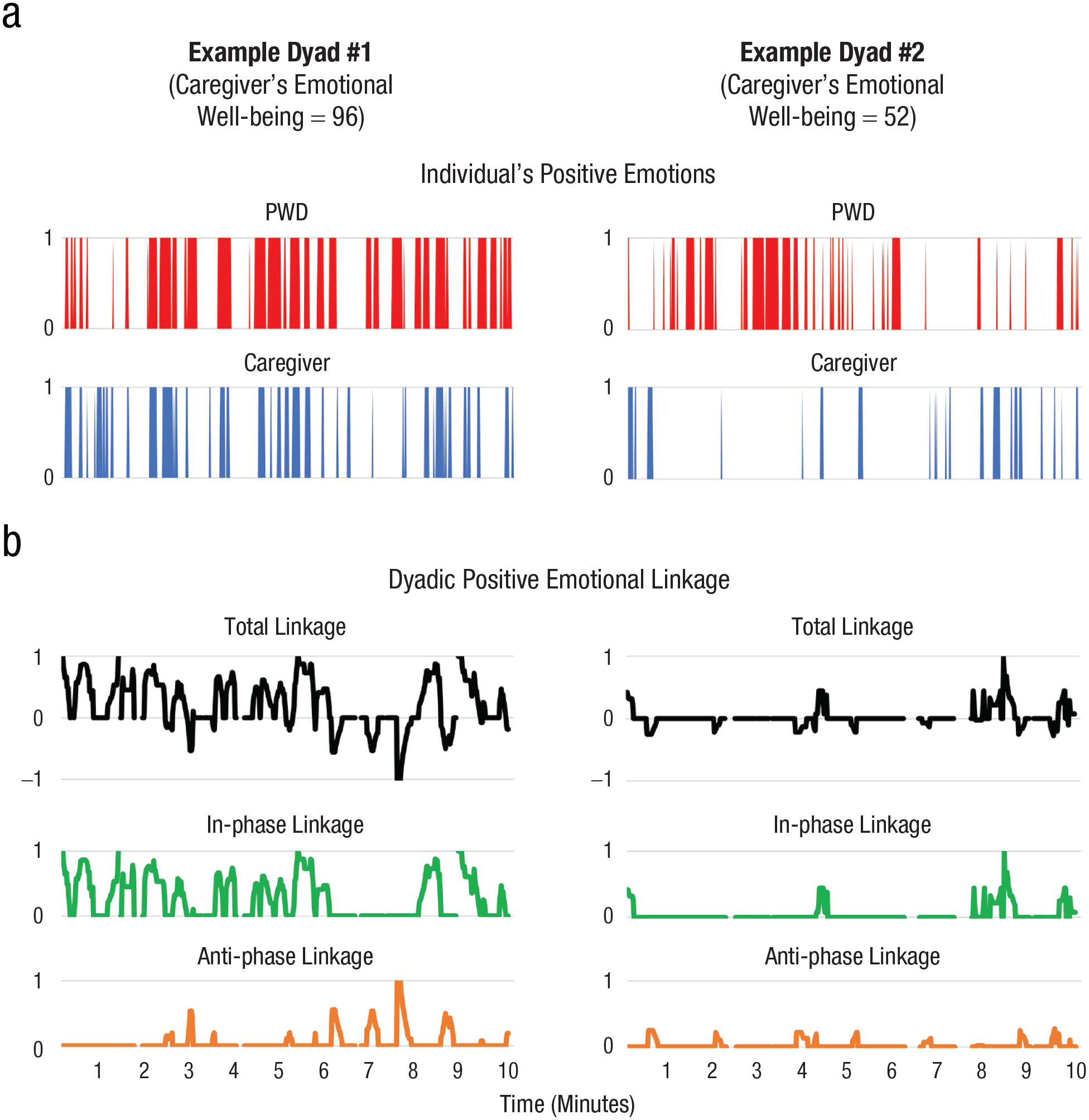
Illustration of (a) individual-level positive emotional behaviors and (b) dyadic positive emotional linkage (including total, in-phase, and anti-phase linkage) using example data from two study dyads. The dyad on the left had a relatively high positive emotional linkage (in-phase = 0.28, anti-phase = 0.06), and the caregiver had relatively higher emotional well-being (score = 96). In contrast, the dyad on the right had a relatively low positive emotional linkage (in-phase = 0.04, anti-phase = 0.02), and the caregiver reported relatively lower emotional well-being (score = 52).
For each participant, we also computed the total positive emotional behaviors and total negative emotional behaviors by summing the number of seconds that the participant expressed each type of emotional behavior during the conversation, respectively. These scores were entered as covariates to ensure that our findings were specific to the dyadic level of “emotional linkage,” rather than simply driven by the amount of emotional behaviors at the individual level.
Positive and negative emotional linkage
Using each dyad’s positive and negative emotional behavior time-series data, positive and negative emotional linkage were computed on a second-by-second basis. Specifically, separately for positive and negative emotional behaviors, we used a “rolling window” approach (Chen, Brown, et al., 2021; Gates et al., 2015) and computed Spearman correlations, centered on each second of the conversation, between the dyad’s emotional behaviors during successive 15-s windows. The computation of Spearman correlations advanced one second at a time. This time series is referred to as “total linkage.” Because the total-linkage scores were based on correlations, they ranged from +1 to −1; positive values reflect in-phase values, and negative values reflect anti-phase linkage (see below for details; Fig. 1b).
We selected 15 s as our time window because it is long enough to provide sufficient variation to compute correlations but not too long to obscure any short-lasting changes in linkage. The same approach has been used in previous research that studied physiological linkage in neurotypical dyads (Chen, Brown, et al., 2021; Marci & Orr, 2006). In the current study, we also performed sensitivity analyses and observed very similar effects when different time windows were used. Results from these sensitivity analyses are presented in Robustness of Findings.
Spearman correlations require both variables to have some variability, that is, to not be constant. During dyadic interactions, there may be no coded positive or negative emotional behaviors for an individual for 15 s or longer. In addition, a person may have a single emotion code assigned for all 15 s. Therefore, using a similar approach as in our previous work (Chen, Casey, et al., 2022), (a) we assigned a value of 0 as the linkage score if one member of the dyad had no variability and the other had some variability in emotional behaviors within the 15-s time period, and (b) we did not compute a linkage score when both members of the dyad had no variability in emotional behaviors within the 15-s time period.
The total linkage time series computed in this way can contain both in-phase (values between 0 and +1) and anti-phase (values between 0 and −1) linkage. To further differentiate these two forms of linkage, we computed a time series of in-phase linkage and a time series of anti-phase linkage using a similar approach as that in our previous research (Chen, Brown, et al., 2021; Chen, Casey, et al., 2022). For each second of the in-phase linkage time series, we either entered the correlation coefficient from the relevant total linkage time series if it was positive or entered a 0 if the correlation was 0 or negative. Likewise, for each second of the anti-phase linkage time series, we either entered the relevant total linkage correlation coefficient if it was negative or entered 0 if it was 0 or positive. Before statistical analyses, correlations in the anti-phase linkage time series were multiplied by −1 so that higher positive values reflect higher linkage. Finally, to provide summary measures for use in subsequent analyses, the in-phase and anti-phase linkage correlations for each 15-s time window during the entire conversation were averaged for each dyad.
Caregiver emotional well-being and physical functioning
Emotional well-being and physical functioning of caregivers and HC partners were assessed using the emotional well-being and physical-functioning subscales, respectively, of the Medical Outcomes Study 36-Item Short Form (SF-36) Survey (Ware & Sherbourne, 1992). The SF-36 is a well-validated (e.g., reliability coefficient for the questionnaire > 0.75; Brazier et al., 1992) self-report questionnaire that includes a five-item emotional well-being subscale (e.g., “Have you been a happy person?”) and a 10-item physical-functioning subscale (e.g., “Does your health now limit you in vigorous activities, such as running, lifting heavy objects, participating in strenuous sports?”). For the complete list of items, see Table S1 in the Supplemental Material. Item scores were reversed as appropriate such that higher scores indicated higher emotional well-being and better physical functioning. The mean score for each subscale was computed by averaging all corresponding item scores.
PWD dementia severity
To ensure that our findings did not simply reflect individual differences in PWDs’ dementia severity, we included the Clinical Dementia Rating (CDR; Morris, 1993) as a covariate. The CDR consists of a semistructured interview with caregivers (and HC partners) regarding functional abilities of the PWDs (and HC participants). The CDR yields two scores: (a) total score (CDR-total), which ranges from 0 to 3 (0 = normal, 0.5 = very mild, 1 = mild, 2 = moderate, 3 = severe), and (b) sum of boxes score (CDR-box), which ranges from 0 to 18 such that higher values indicate greater severity. Data analyses used CDR-box because it is continuous and has a greater range, making it more sensitive to variations in dementia severity.
Relationship quality
Relationship quality of PWD–caregiver and HC dyads was included as a potential covariate because past research has revealed its associations with (a) emotions during dyadic interactions (Brown et al., 2021; Levenson & Gottman, 1983) and (b) well-being and health of the dyads (Kiecolt-Glaser & Wilson, 2017). Caregivers and HC partners rated their relationship quality with the PWDs and HC participants using the Marital Adjustment Test (Locke & Wallace, 1959). The test consisted of 15 items (e.g., “Do you confide in your mate?”). Weighted mean scores of all items were computed (the weighting of each item was determined by the ratio of the maximum score for each item to the entire test; for more details about the weighting and the related SPSS scripts, see Table S2 and Syntax 2 in the Supplemental Material), and a higher value indicated higher relationship quality. To ensure our results based on weighted mean scores were robust, we also analyzed the data after imputing total scores based on the proportion of items answered (out of total items of the test) and found very similar results (see Tables S3 and S4 in the Supplemental Material).
Results
Preliminary analyses
Preliminary analyses were performed to help us determine our sample size, data exclusions, manipulations, measures, and covariates in the study.
For emotional well-being, physical-functioning, and relationship-quality questionnaires administered to caregivers and HC partners, we set a 20% cutoff for each as the acceptable rate for missing data. Sensitivity analyses revealed that our primary findings remained robust when different cutoffs were used (see Robustness of Findings). A preliminary review of our data set revealed that two HC partners had more than 20% data missing for emotional well-being or physical functioning. Because these two variables are our primary dependent variables, these two HC dyads were excluded from all remaining data analyses. This resulted in a final sample of 57 dyads (23 bvFTD, 22 AD, 12 HC) in our data analyses. Demographics and descriptive statistics for this final sample are presented in Table 1.
Descriptive Statistics and Bivariate Correlations With Primary Independent (Emotional Linkage) and Dependent (Caregiver/Partner Emotional Well-Being and Physical Functioning) Variables for Demographic and Functional Information
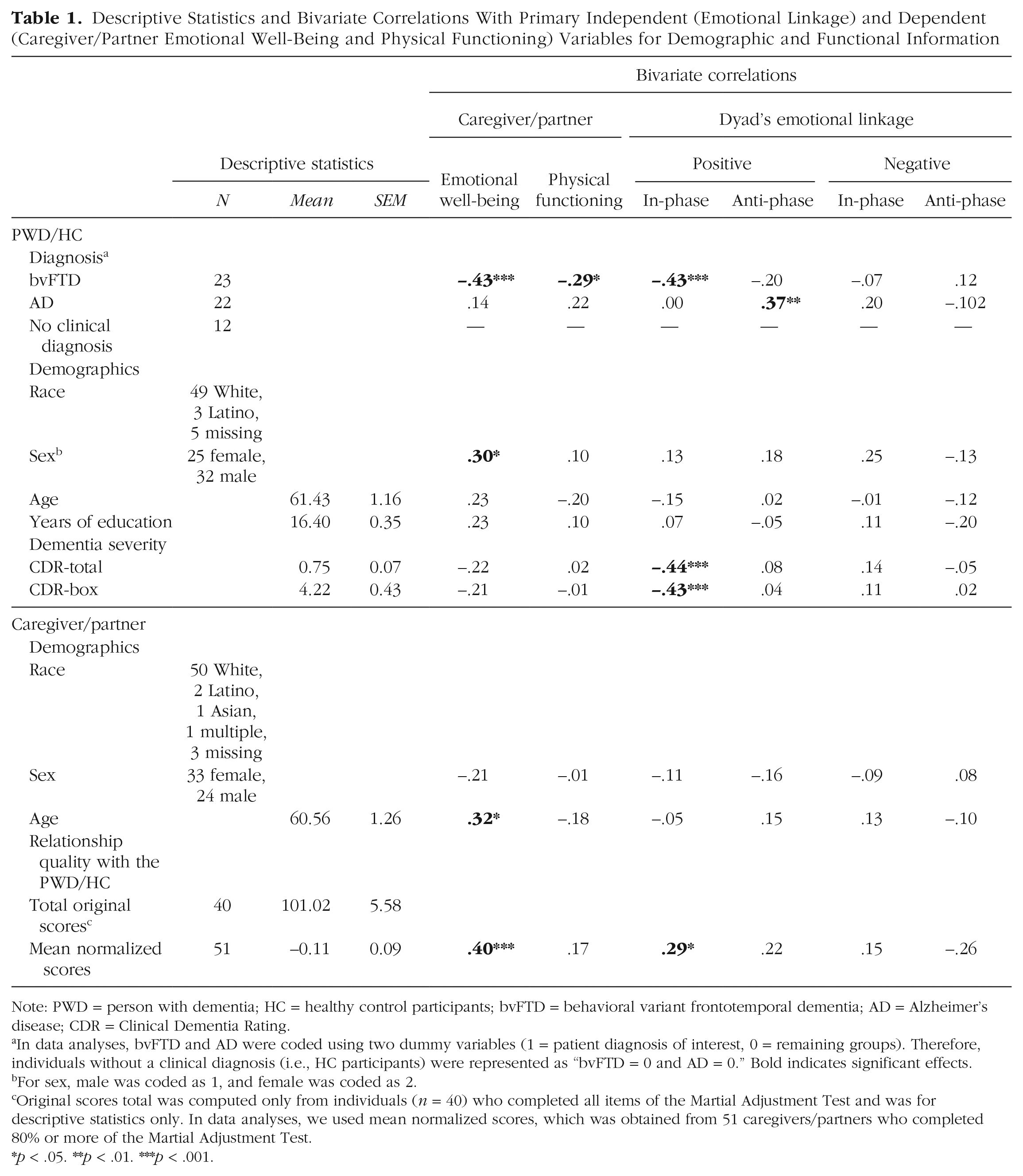
Note: PWD = person with dementia; HC = healthy control participants; bvFTD = behavioral variant frontotemporal dementia; AD = Alzheimer’s disease; CDR = Clinical Dementia Rating.
In data analyses, bvFTD and AD were coded using two dummy variables (1 = patient diagnosis of interest, 0 = remaining groups). Therefore, individuals without a clinical diagnosis (i.e., HC participants) were represented as “bvFTD = 0 and AD = 0.” Bold indicates significant effects.
For sex, male was coded as 1, and female was coded as 2.
Original scores total was computed only from individuals (n = 40) who completed all items of the Martial Adjustment Test and was for descriptive statistics only. In data analyses, we used mean normalized scores, which was obtained from 51 caregivers/partners who completed 80% or more of the Martial Adjustment Test.
p < .05. **p < .01. ***p < .001.
Regarding covariates, our preliminary data examination identified six additional caregivers (one bvFTD, four AD, one HC) with more than 20% data missing for relationship quality. These dyads were included in all data analyses except those that included relationship quality. No other covariates were missing.
To determine whether any differences emerged between the three groups of dyads (bvFTD, AD and HC dyads), we performed four one-way analyses of variance, separately for each linkage measure (i.e., in-phase positive, anti-phase positive, in-phase negative, and anti-phase negative emotional linkage). The analyses revealed a significant group effect for in-phase positive emotional linkage (F = 12.43, η2 = .32, p < .001). Post hoc t tests with Bonferroni corrections for multiple comparisons revealed that bvFTD and AD dyads both had a significantly lower in-phase positive emotional linkage than HC dyads (p < .001 and p = .006, respectively). Analyses also revealed a significant group effect for anti-phase positive emotional linkage (F = 4.41, η2 = .14, p = .017) with higher levels in the AD than bvFTD (p = .044) and HC dyads (p = .048). No group effects were found for in-phase or anti-phase negative emotional linkage (Fs < 1.37, ps > .26). These results are presented in Figure S1 in the Supplemental Material.
We used Pearson’s (for continuous variables) and point biserial (for continuous with binary variables) correlations to identify possible demographic and functional covariates for primary data analyses. For sex, we coded male as 1 and female as 2. For each PWD diagnosis, we created two diagnostic dummy variables (1 = diagnosis of interest, 0 = remaining groups). Variables that significantly correlated with our primary dependent (i.e., caregiver emotional well-being and physical functioning) or independent variables (i.e., in-phase and anti-phase positive and negative emotional linkage) were entered as covariates in the corresponding analyses. For example, to evaluate the association between positive in-phase emotional linkage and caregiver emotional well-being, we included PWD sex, bvFTD diagnosis, dementia severity, caregiver age, and the dyad’s relationship quality because these variables were significantly correlated with either positive in-phase emotional linkage, caregiver emotional well-being, or both (ps < .042; see Table 1).
Primary analyses
Emotional linkage and caregiver emotional well-being
To test the hypothesis that lower positive and higher negative emotional linkage would be associated with lower caregiver/partner emotional well-being, we conducted four Pearson’s correlations for emotional linkage (separately for each linkage measure) and caregiver/partner emotional well-being. Results revealed that lower in-phase positive emotional linkage was associated with lower caregiver/partner emotional well-being, r = .38, p = .003 (Table 2).
Results of Primary Analyses (N = 57): Bivariate Pearson’s Correlations Between Primary Independent (Emotional Linkage) and Dependent (Caregiver/Partner Emotional Well-Being and Physical Functioning) Variables
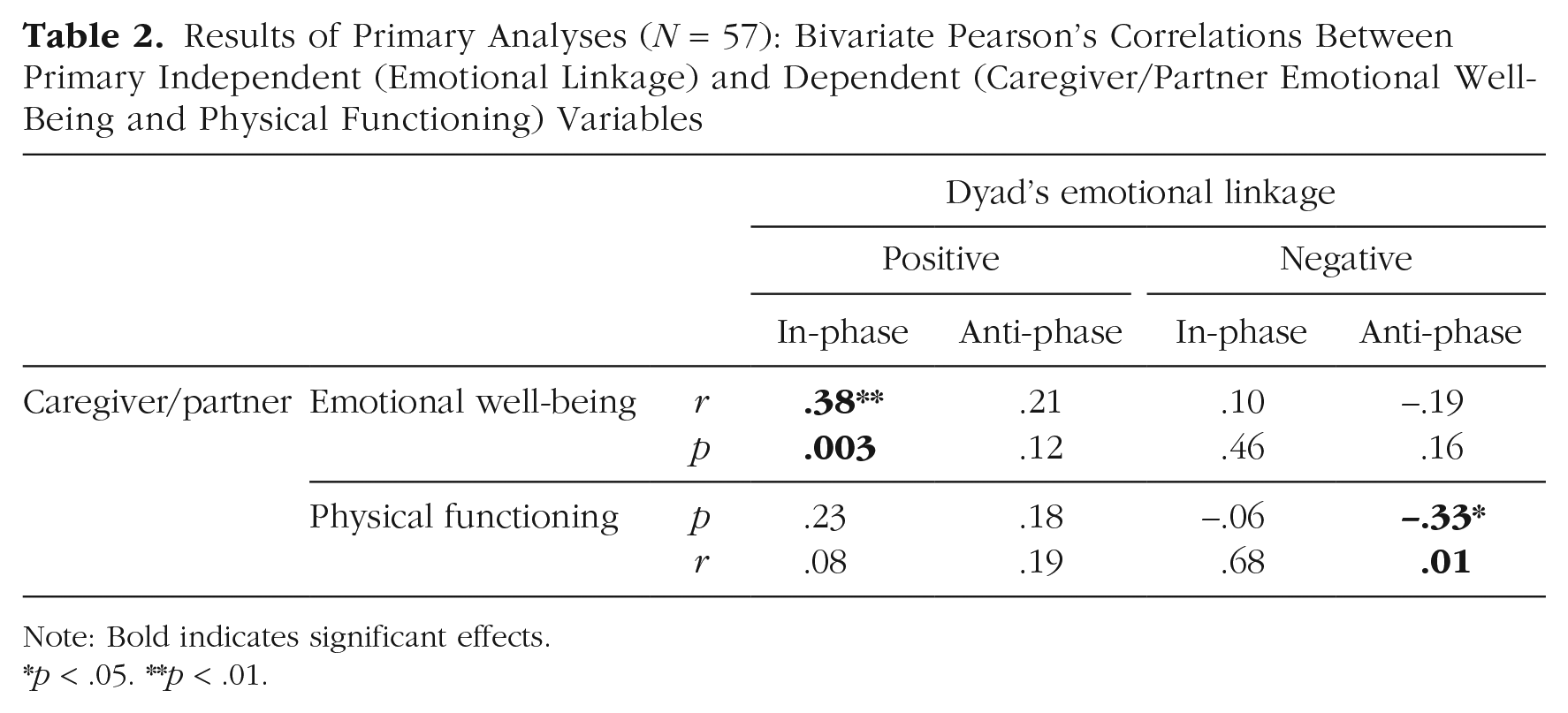
Note: Bold indicates significant effects.
p < .05. **p < .01.
To ensure that these findings were specific to the dyadic levels and did not simply reflect disease-related emotional changes at individual levels (e.g., diagnosis of AD was associated with greater PWD total positive emotional behaviors, r = .31, p = .017; see Table S5 in the Supplemental Material), we followed up the above findings with a linear multiple regression in which total positive emotional behaviors of the PWD/HC, of the caregiver/partner, and in-phase positive emotional linkage of the dyad were entered as independent variables; caregiver/partner emotional well-being was the dependent variable (Table 3). We found that the association between lower in-phase positive emotional linkage and lower caregiver/partner emotional well-being remained significant when adjusted for individual-level total positive emotional behaviors (β = 0.33, p = .011).
Results of Primary Analyses (N = 57): Two Follow-Up Regression Analyses (Adjusting for Individual-Level Emotional Behaviors) to Determine Effect Specificity to the Dyadic Levels (for Significant Effects Reported in Table 2)
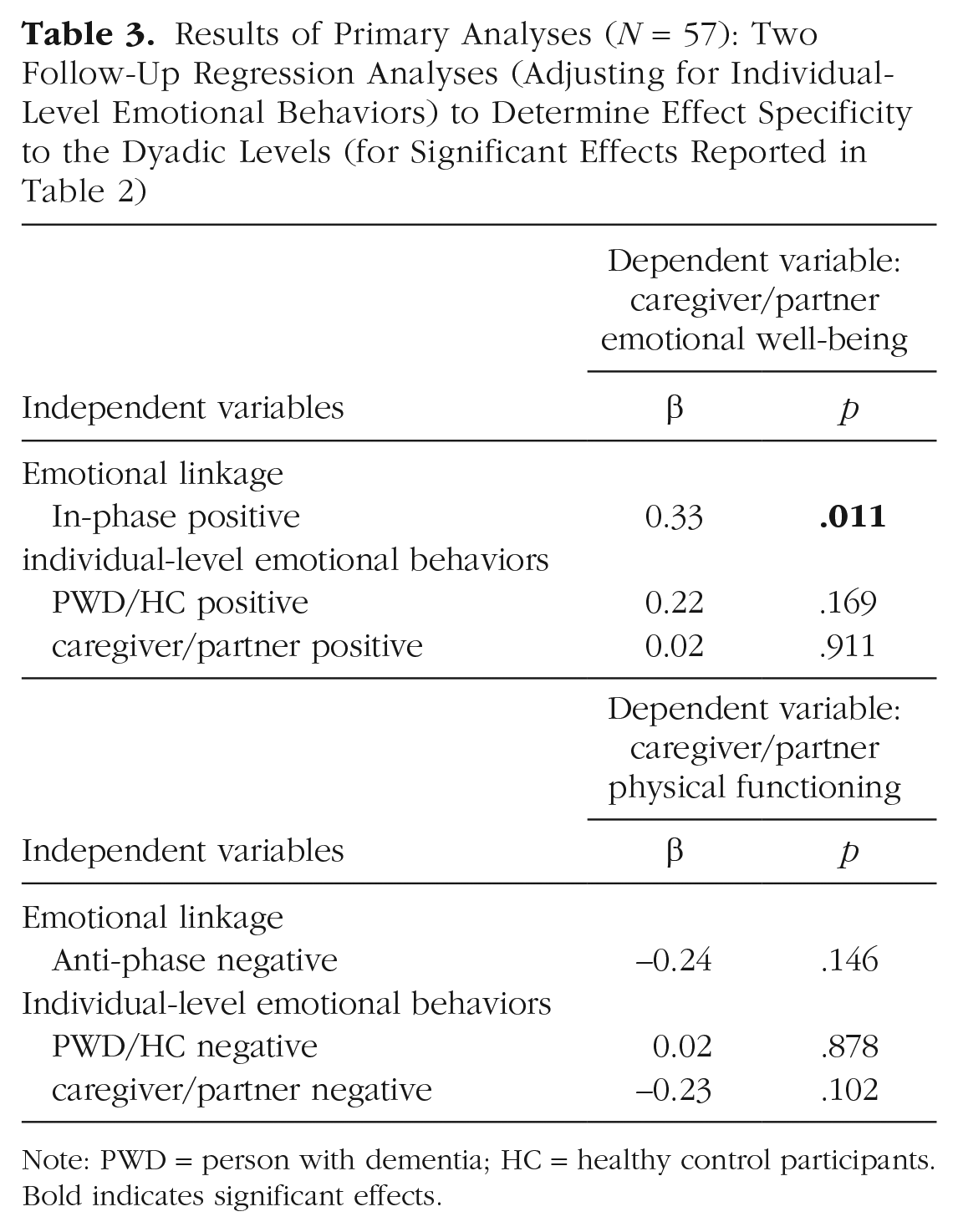
Note: PWD = person with dementia; HC = healthy control participants. Bold indicates significant effects.
Emotional linkage and caregiver physical functioning
To test the hypothesis that lower positive and higher negative emotional linkage would be associated with lower caregiver/partner physical functioning, we conducted similar Pearson’s correlations as described above. We found that higher anti-phase negative emotional linkage was associated with worse caregiver/partner physical functioning (r = −.33, p = .013; Table 2). However, in the follow-up regression analysis adjusted for individual-level total negative emotional behaviors, this association became statistically insignificant (β = −0.24, p = .146; Table 3).
Because our primary analyses revealed significant and uniquely “dyadic-level” effects only for the association between lower in-phase positive emotional linkage and lower caregiver/partner emotional well-being, we focused on this association in the analyses reported below.
Robustness of findings
To ensure our findings did not simply reflect individual differences in demographic variables and PWD dementia severity, we conducted a linear multiple regression (Table 4) to examine the association between lower in-phase positive emotional linkage and lower caregiver/partner emotional well-being while adjusting for all five covariates identified in the preliminary analyses reported in Table 1 (i.e., PWD/HC sex, diagnosis, dementia severity, caregiver/partner age, and relationship quality). Results still indicated a significant association between lower in-phase positive emotional linkage and lower caregiver/partner emotional well-being (β = 0.30, p = .045).
Effect Robustness (N = 51): A Regression Analysis to Determine the Associations Between Lower In-Phase Positive Emotional Linkage and Lower Caregiver Emotional Well-Being While Adjusting for Covariates
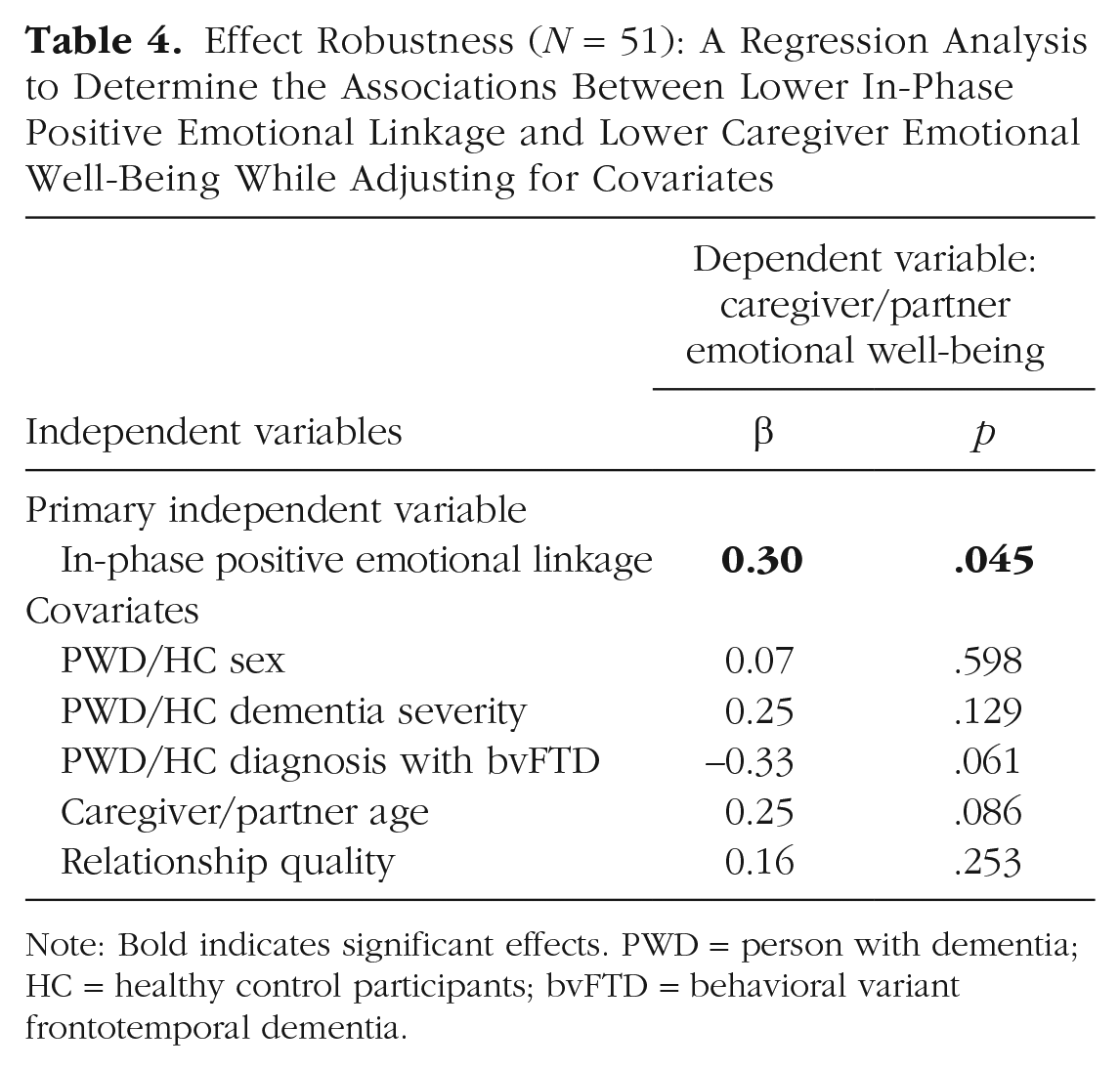
Note: Bold indicates significant effects. PWD = person with dementia; HC = healthy control participants; bvFTD = behavioral variant frontotemporal dementia.
In our primary analyses, the four linkage measures were evaluated separately for their associations with caregiver outcomes. To ensure the above-reported findings were specific to in-phase positive emotional linkage, we conducted a linear multiple regression in which all four linkage measures were entered as independent variables and caregiver emotional well-being was the dependent variable. Results indicated that only lower in-phase positive emotional linkage was significantly associated with lower caregiver emotional well-being (β = 0.39, p = .002; see Table S6 in the Supplemental Material).
To ensure our findings based on analyzing the 15-s windows were robust, we repeated our primary analysis (Pearson’s correlation) using shorter or longer time windows (e.g., 10 s and 20 s). To ensure our findings based on converted binary emotion scores were robust, we repeated our primary analysis using raw emotion scores. To ensure findings based on the 20% cutoff for acceptable questionnaire missing data were robust (which resulted in n = 57 dyads), we repeated our primary analysis using lower or higher cutoffs (e.g., 0% and 30%; corresponding ns = 55 and 58 dyads, respectively). All of these additional analyses revealed a significant association between lower in-phase positive emotional linkage and lower caregiver/partner emotional well-being (rs > .36, ps < .01; see Tables S7–S9 in the Supplemental Material).
Finally, 12 control dyads were included in our data analyses. To ensure our findings would be robust when considering only PWD–caregiver dyads, we repeated our primary analyses with only the 45 PWD–caregiver dyads. These analyses still revealed a significant association between lower in-phase positive emotional linkage and lower caregiver emotional well-being (r = .37, p = .01; see Table S10 in the Supplemental Material).
Exploratory Analysis 1: unique value of laboratory assessment of positive emotional linkage
Our preliminary analyses revealed that the dyad’s worse relationship quality, assessed using a well-established questionnaire, was significantly associated with (a) dyads’ lower positive emotional linkage and (b) lower emotional well-being of the caregivers/HC partners. These results raise an important question: whether there is any unique or incremental value of assessing positive emotional linkage in the laboratory compared with assessing the dyad’s relationship quality using questionnaires in predicting or explaining emotional well-being in caregivers and HC partners.
To answer this question, we performed a hierarchical linear multiple regression in which relationship quality, in-phase positive emotional linkage, and a set of covariates that were significantly correlated with caregiver emotional well-being (i.e., PWD/HC sex, bvFTD diagnosis, and caregiver/partner age, based on preliminary analyses reported in Table 1) were sequentially entered as independent variables in Steps 1, 2, and 3, respectively, and caregiver/partner emotional well-being was the dependent variable. This analysis revealed that although lower relationship quality alone was significantly associated with lower caregiver/partner emotional well-being (β = 0.40, p = .003) in Step 1, adding in-phase positive emotional linkage as an additional independent variable in Step 2 improved the model by accounting for significantly more variance in caregiver/partner emotional well-being (∆R2 = .08, p = .032). When the analysis was adjusted for covariates in Step 3, only lower in-phase positive emotional linkage (β = 0.30, p = .045) but not worse relationship quality (β = 0.16, p = .253) was significantly associated with lower caregiver/partner emotional well-being (Table 5).
Results of Exploratory Analysis (N = 51): A Regression Analysis to Examine the Unique, Incremental Value of Laboratory Assessment of In-Phase Positive Emotional Linkage to Questionnaire Assessment of Relationship Quality in Explaining Caregiving/Partner Emotional Well-Being
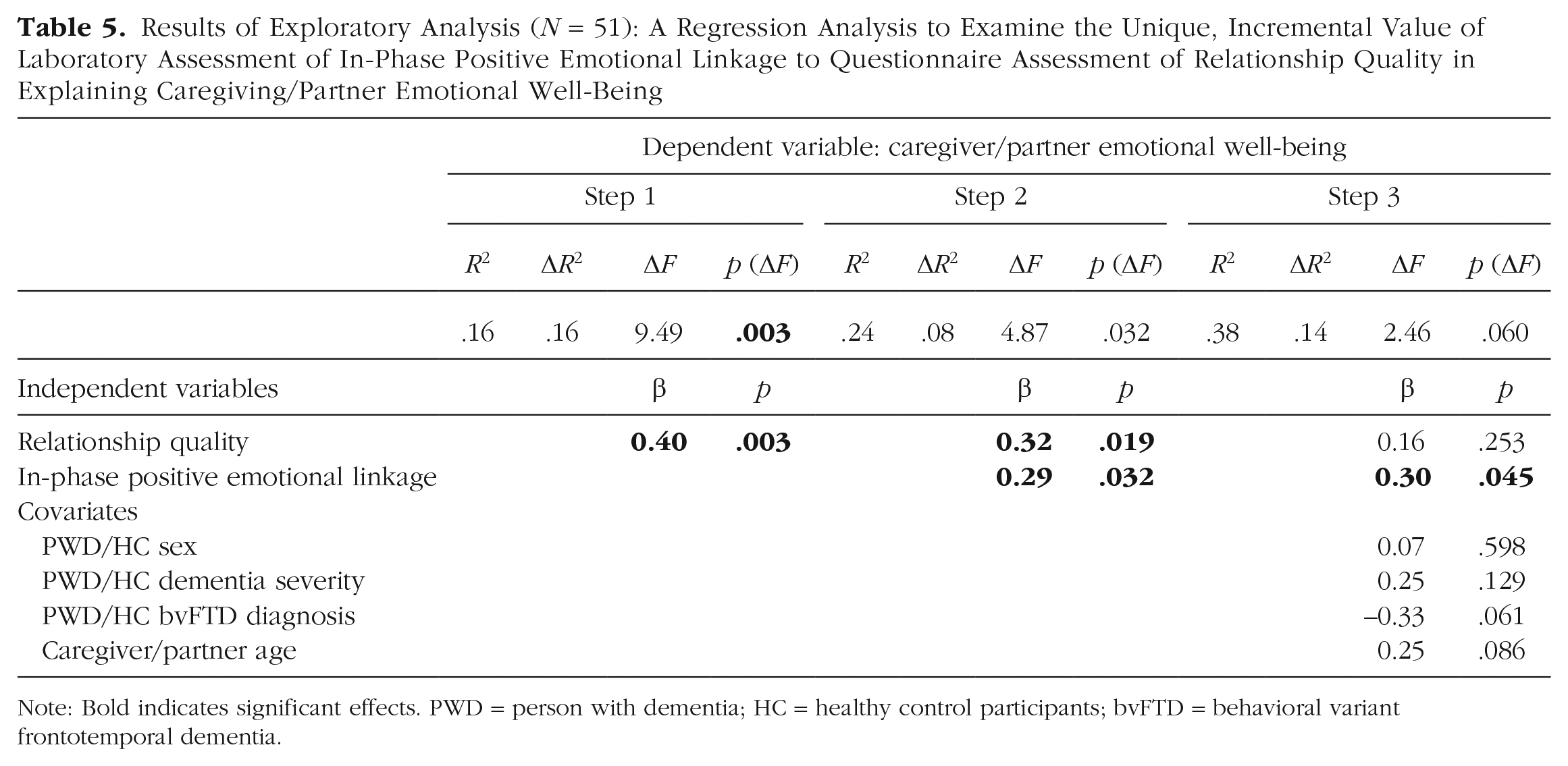
Note: Bold indicates significant effects. PWD = person with dementia; HC = healthy control participants; bvFTD = behavioral variant frontotemporal dementia.
Exploratory Analysis 2: lower positive emotional linkage as an explanation for lower emotional well-being in bvFTD caregivers
Our preliminary analyses also revealed that (a) having a diagnosis of bvFTD was associated with lower emotional well-being in caregivers/partners and (b) bvFTD dyads had significantly lower in-phase positive emotional linkage than AD and HC dyads. These results raise the question of whether lower in-phase positive emotional linkage explains bvFTD caregivers’ lower emotional well-being compared with caregivers or partners whose loved one does not have bvFTD.
To answer this question, we performed a mediation analysis using IBM SPSS PROCESS (Version 3.4.1) with default parameters (Hayes, 2013). In this analysis, the diagnosis of bvFTD was the independent variable (1 = bvFTD, 0 = otherwise), caregiver/partner emotional well-being was the dependent variable, and in-phase positive emotional linkage was a mediator. Note that AD caregivers and HC partners were grouped together in this analysis because an independent sample t test did not reveal a significant difference in their emotional well-being (p = .35).
The mediation analysis revealed that bvFTD caregivers (n = 23) had lower emotional well-being than AD caregivers and HC partners (n = 34), c = −0.87, p < .001, and this effect was partially mediated (c′ = −0.66, p = .02) by bvFTD caregivers’ lower positive emotional linkage with the PWDs (standard indirect effect = −0.21, 95% confidence interval = [−0.46, −0.02], accounting for 24% of the total effect; see Fig. 2). These effects remained robust when the analysis was adjusted for PWD dementia severity, sex, and caregiver age (see Fig. S2 in the Supplemental Material).
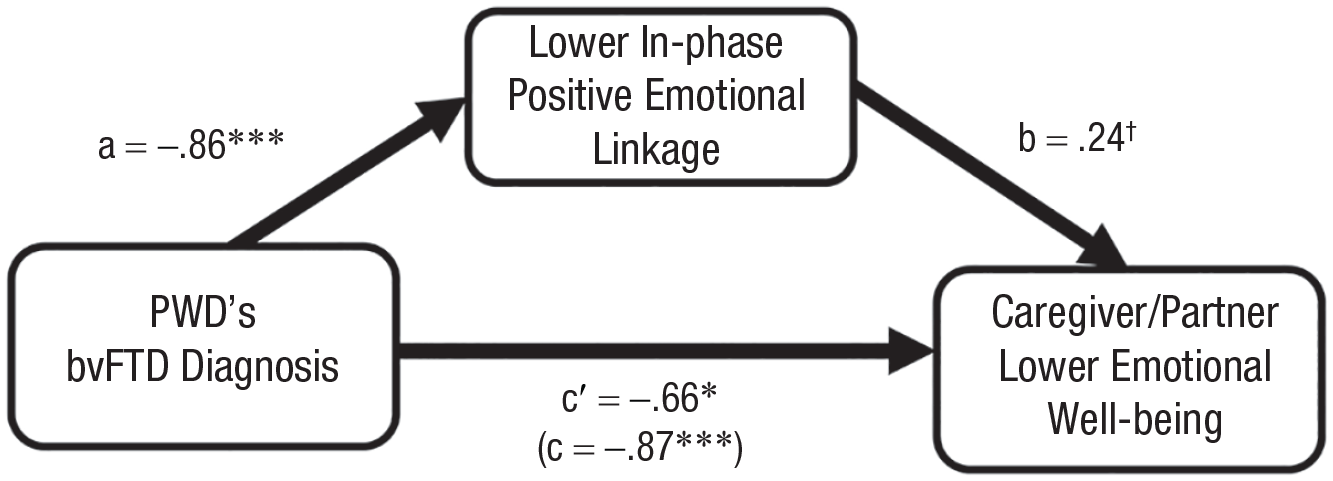
Results of exploratory mediation analysis (N = 57). Lower in-phase positive emotional linkage as a mediator for the effects of lower emotional well-being in bvFTD caregivers, n = 23 (vs. AD caregivers and HC partners, n = 34). Standardized indirect effect = −0.21, 95% confidence interval = [−0.46, −0.02], accounting for 24% of the total effect. bvFTD = behavioral-variant frontotemporal dementia; AD = Alzheimer’s disease; HC = healthy control participants. †p < .10. *p < .05. ***p < .001.
Discussion
In this study, we systematically examined the in-phase and anti-phase forms of linkage in positive and negative emotional behaviors in PWD–caregiver and HC dyads during a 10-min conflict conversation in the laboratory. Even when adjusting for participant emotional behaviors at the individual levels, we found that lower in-phase positive emotional linkage was associated with lower caregiver/partner emotional well-being. No similar effect was found for anti-phase positive emotional linkage or either form of negative emotional linkage. We also did not find similar effects for caregiver/partner physical functioning. In exploratory analyses, we found that our laboratory assessment of emotional linkage provided additional explanatory power for caregiver/partner emotional well-being—independent of questionnaire assessments of the dyad’s relationship quality. In addition, exploratory mediation analyses revealed that lower emotional well-being in bvFTD caregivers compared with AD caregivers and HC partners was partially explained by bvFTD caregivers’ lower positive emotional linkage to the PWDs under their care.
Positive emotional linkage, emotional well-being, and physical functioning
Caregiver/partner emotional well-being
Our finding of an association between lower dyadic in-phase positive emotional linkage and lower caregiver/partner emotional well-being is consistent with the literature on married neurotypical couples (Kiecolt-Glaser & Wilson, 2017; Wells et al., 2022). For example, we recently reported that neurotypical individuals in couples who had fewer simultaneous positive emotions (measured across multiple response systems) during dyadic interactions in the laboratory had a steeper decline in health in the following 13 years and less longevity over the following 30 years (Wells et al., 2022). More broadly, our findings are consistent with results from developmental studies that have found lower positive emotional linkage between parents and children to be associated with worse health and more problem behaviors in the children (Feldman, 2012; Lunkenheimer et al., 2020). Extending these previous findings, our study is the first to our knowledge to demonstrate (a) the association between lower positive emotional linkage and lower emotional well-being in the context of dementia and family caregiving; (b) the specificity of these effects, given that only the dyadic-level in-phase positive emotional linkage, rather than other dyadic- or individual-level emotional measures, was associated with caregiver emotional well-being; and (c) that lower positive emotional linkage helps explain bvFTD caregivers’ lower emotional well-being compared with AD caregivers and neurotypical partners.
Several mechanisms may account for the association between lower positive emotional linkage and lower caregiver/partner emotional well-being. First, positive emotions have been shown to speed recovery from negative emotions (Fredrickson et al., 2000; Fredrickson & Levenson, 1998), broaden awareness of self and others, and build new thoughts and actions including prosocial behaviors (Aknin et al., 2018; Fredrickson et al., 2008). When PWDs and their caregivers face a conflict, not linking to each other’s positive emotions (e.g., not showing shared laughter, interests, or affections) may preclude both the PWDs and caregivers from down-regulating their own negative emotions, empathizing with each other’s negative emotions, or developing and implementing prosocial solutions that are mutually beneficial. Second, recent theories and findings suggest that positive emotional linkage promotes social bonds and attachment formation (Feldman, 2017; Kurtz & Algoe, 2017). Therefore, reduced in-phase positive emotional linkage may result from and/or lead to caregivers’ interpersonal distancing and insecure attachment to PWDs. Future research should investigate whether these potential mechanisms explain our findings of an association between lower linkage in positive emotions and lower caregiver emotional well-being.
Our analyses did not reveal an association between lower anti-phase positive emotional linkage and lower caregiver emotional well-being. This result is consistent with our previous findings that anti-phase physiological linkage tends to be less sensitive to relationship quality and mental health than in-phase physiological linkage (Chen, Brown, et al., 2021; Chen, Casey, et al., 2022). We suspect this may reflect our approach that collapses the 15 emotional behaviors coded by SPAFF into two dimensional emotional categories. Even within the same affective valence, the time course for each emotional behavior to occur and alternate between partners may differ (e.g., laughter/humor is associated with a sharper onset and faster contagion/alternation between partners than affection; Bachorowski & Owren, 2001; Provine, 1992). Therefore, collapsing multiple emotional behaviors into two larger categories and thereafter computing linkage scores using the same set of temporal parameters (e.g., 15-s time window) may attenuate the hypothesized association between lower anti-phase emotional linkage and lower caregiver emotional well-being.
Our findings also revealed important differences related to PWD diagnosis. We found that PWDs with AD had (a) more total positive emotional behaviors (see Table S5 in the Supplemental Material) and (b) higher anti-phase positive emotional linkage with their partners compared with PWDs with bvFTD and HCs (see Fig. S1 in the Supplemental Material). Previous studies have found that PWDs with AD have increased experience of certain positive emotions that are incongruent with the socioemotional context (Chen, Hua, et al., 2021; Chen, Lwi, et al., 2017). In addition, previous studies have found increased emotional contagion in AD in which individuals with AD show greater frequency in echoing emotions of others during social interactions (e.g., Sturm et al., 2013; Sturm & Levenson, 2019). We suspect that some AD caregivers may feel confused by PWDs’ positive emotions when these emotions are out of context. Caregivers may also view PWDs’ increased echoing of positive emotions as a warning sign of disease worsening. This may also help explain the nonsignificant results regarding our hypothesized association between lower anti-phase positive emotional linkage and lower caregiver emotional well-being.
Caregiver/partner physical functioning
Although in the expected direction, the effects for the association between lower in-phase positive emotional linkage and lower caregiver physical functioning was not statistically significant. We suspect that the impact of reduced PWD–caregiver positive emotional linkage on caregiver physical functioning may take longer time to develop than on caregiver emotional well-being. In a 20-year longitudinal study, we (Haase et al., 2016) found that links between negative emotional behaviors and physical health problems in neurotypical couples appeared only after more than a decade. Future research will benefit from using longitudinal research designs with repeated assessments of key PWD, caregiver, and dyadic variables over time to address these issues.
Negative emotional linkage, emotional well-being, and physical functioning
We hypothesized that higher negative emotional linkage would also be associated with lower caregiver/partner emotional well-being and physical functioning. We did not observe such effects when the analyses were adjusted for negative emotional behaviors at the individual level. As is often the case with research with PWDs, our sample size was small, which limited our power to detect small-sized effects. In addition, although negative emotional linkage is typically viewed as harmful, some instances of negative emotional linkage, such as sharing a partner’s distress, may be beneficial. Supporting this idea, Haase et al. (2012) found that during late adulthood, a person’s experience of sadness is associated with his or her own better satisfaction with life and a higher ratio of dispositional positive to negative affect. Future studies are needed to differentiate the associations between linkage in specific negative emotions (e.g., anger, fear, sadness) and caregiver health outcomes.
The value added of laboratory assessment of positive emotional linkage
The associations between worse relationship quality and lower emotional well-being have been well recognized in the literature (Kiecolt-Glaser & Wilson, 2017). Extending this previous work, we found in our analyses that adding laboratory assessment of positive emotional linkage offers additional explanatory power for caregiver/partner emotional well-being. When positive emotional linkage and relationship quality were entered simultaneously as independent variables, both were significantly associated with caregiver/partner emotional well-being. These findings suggest that lower positive emotional linkage was not simply a reflection of the dyad’s worse relationship quality. Rather, they may reflect additional aspects of dyadic interpersonal processes not captured by the relationship-quality questionnaires. Moreover, when controlling for PWD dementia severity and caregiver/partner age, we found that the association between relationship quality and caregiver/partner emotional well-being became statistically insignificant, whereas the association with positive emotional linkage remained significant. These findings underscore the value of laboratory assessments for providing an arguably more objective (i.e., less biased by age, functional declines, and social desirability) and more targeted (i.e., observing behaviors that occur during dyadic interactions) measure for studying emotional and social changes in aging couples, including PWD–caregiver dyads.
Strengths and limitations
There are several strengths of our study. First, by studying emotional linkage during naturalistic dyadic interactions, we increased the ecological validity of our findings (given that most emotions occur in interpersonal situations; Levenson, 1999). Second, we demonstrated the added value of using laboratory assessments of emotional linkage, finding that they accounted for additional variance in caregiver emotional well-being independent of what would have been obtained when solely relying on questionnaire measures of relationship quality. Third, we evaluated emotions at both the individual and dyadic levels and found that the observed effects were specific to the dyadic emotional measures. Fourth, we evaluated emotions by comparing four forms of emotional linkage and two different caregiver outcomes. Fifth, we included dyads in which the PWD was diagnosed with either AD or bvFTD and HC dyads, which enabled us to examine diagnosis-specific findings. Finally, sixth, we established the robustness of our findings by rejecting several alternative explanations including PWD dementia diagnosis, severity, and caregiver/partner age.
Our study has several limitations. First, we focused on emotions and linkage during a conflict conversation and thus do not know if findings would generalize to other conversational topics and other contexts. Second, we quantified emotions and emotional linkage using objectively coded emotional behaviors and cannot know if our findings would generalize to other important aspects of human emotions (e.g., subjective experience, physiology). Third, we focused on spousal caregivers and cannot know if our findings would generalize to other kinds of caregivers (e.g., adult children, friends). Fourth, we focused on linkage in two major dimensional groupings of emotions (i.e., positive and negative emotions), and it is not clear if our findings would generalize to linkage in specific emotions (e.g., linkage in humor or affection; linkage in positive emotions with high vs. low arousal). Fifth, we focused on the mean levels of emotional linkage over the entire conversation, which limits inferences about temporal dynamics (e.g., dyads shifting from negative to positive emotional linkage over the course of the conversation) and directional influences (e.g., when emotions were linked, whether the caregiver’s emotions preceded or followed those of the PWD) in relation to caregiver outcomes. Sixth, our cross-sectional design limits inferences about the directional influences between lower emotional linkage and lower caregiver emotional well-being and our ability to assess longer-term caregiver outcomes. Finally, seventh, our sample size is relatively small (53 dyads with all measures available; four with all measures except relationship quality) and unbalanced between groups (i.e., 12 control, 23 bvFTD, and 22 AD dyads); thus, future studies with a larger and more balanced sample size will be needed to confirm the robustness of the observed effects.
Conclusion
The current study is the first to our knowledge to demonstrate an association between lower PWD–caregiver positive emotional linkage and lower caregiver emotional well-being. These findings have important implications to health outcomes in PWDs and caregivers—in the literature, lower caregiver emotional well-being has been linked to health worsening in caregivers (Schulz et al., 2020) and shorter longevity of PWDs (Lwi et al., 2017). Our findings underscore the promise of laboratory assessments of emotional linkage between PWDs and caregivers for understanding caregiver emotional well-being. Given the enormous and growing number of PWDs and spousal caregivers worldwide and projections that this number will increase dramatically in the near future (Alzheimer’s Association, 2023), recognizing dyadic factors that are associated with lower caregiver emotional well-being and physical functioning can help inform future interventions that target these interpersonal processes (Bannon et al., 2022) to help protect from adverse health outcomes in caregivers and the people in their care.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026231214530 – Supplemental material for Interpersonal Linkage in Positive and Negative Emotional Behaviors, Emotional Well-Being, and Physical Functioning in Dementia Caregivers
Supplemental material, sj-docx-1-cpx-10.1177_21677026231214530 for Interpersonal Linkage in Positive and Negative Emotional Behaviors, Emotional Well-Being, and Physical Functioning in Dementia Caregivers by Kuan-Hua Chen, Jennifer Merrilees, Casey L. Brown, Claire Yee, Anna Sapozhnikova, Jenna L. Wells, Emilio Ferrer, Peter S. Pressman, Barbara L. Fredrickson and Robert W. Levenson in Clinical Psychological Science
Footnotes
Acknowledgements
We thank Scott Newton and Kia Nesmith for their assistance with subject recruitment, Deepak Paul for helping with data management and technical support, all research assistants for their help with data collection and behavioral coding (Samuel Gong, Cheuk Hei Cheng, and Adokole Otonwa), and Enna Chen for proofreading. We also thank all the persons with dementia and caregivers who donated their time so generously to participate in this research.
Transparency
Action Editor: Vina Goghari
Editor: Jennifer L. Tackett
Author Contributions
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.