
Abstract
Although emotion dysregulation has been robustly associated with posttraumatic stress disorder (PTSD), there is relatively little understanding of this process in refugees. Specifically, longitudinal methodology has not been used to examine the relationship between emotion dysregulation and PTSD among refugees. In this study, we investigated the temporal relationship between emotion dysregulation, postmigration stressors, and PTSD clusters (reexperiencing, avoidance, negative alterations in mood and cognition [NAMC], and hyperarousal) from the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders among a community sample of refugees (N = 1,081) over a 2-year period. Random intercept cross-lagged panel analysis found that emotion dysregulation was antecedent to within-persons increases in reexperiencing and NAMC symptoms over time and bidirectionally associated with hyperarousal and postmigration stressors. In addition, postmigration stressors were antecedent to within-persons increases in reexperiencing, avoidance, and NAMC and bidirectionally associated with hyperarousal symptoms. Findings provide novel evidence in support of postmigration stressors and emotion dysregulation as mechanisms maintaining PTSD and highlight the potential utility of tailoring interventions to address these factors.
Keywords
Humans are currently experiencing unprecedented levels of forced displacement globally, with over 100 million people forcibly displaced because of ongoing war and conflict (UNHCR, 2022). As the global population of refugees continues to rise, increased pressure is placed on the health-care systems of transit and host nations to support the mental-health needs of these populations. Refugees experience multiple, prolonged, and severe forms of traumatization and report elevated rates of psychiatric disorders (Blackmore et al., 2020; Bogic et al., 2015). In particular, refugees represent one of the largest at-risk groups for developing posttraumatic stress disorder (PTSD), with an estimated prevalence of 31.5% (Blackmore et al., 2020). In addition to their exposure to many traumatic events, the refugee experience is often characterized by the presence of ongoing stressors and living difficulties that occur in the postmigration environment, including economic hardship, visa and housing insecurity, discrimination, and family separation. The presence of these postmigration stressors has been found to uniquely predict PTSD over and above the influence of established predictors, such as cumulative trauma exposure (Li et al., 2016; Porter & Haslam, 2005), and may serve to further complicate the clinical presentation of traumatized refugees. Despite this, little research has explored the psychological mechanisms that might underpin the relationship between refugee experiences of trauma and stress and the development of PTSD. Supporting the mental health of refugees represents a significant global challenge to public health (Lindert et al., 2016) and highlights the critical need for targeted and efficient treatments. To meet this global challenge and develop effective interventions tailored to the specific needs of these populations, it is incumbent on clinical research to first understand the psychological mechanisms underpinning PTSD in refugees.
Emotion dysregulation is a promising candidate mechanism implicated in the development and maintenance of PTSD in refugees. Emotion dysregulation refers to an impaired capacity to monitor and modulate one’s emotional responses, such as having difficulties in implementing effective emotion-regulation strategies when distressed (Gratz & Roemer, 2004). Refugees may be a population especially likely to experience emotion dysregulation. In particular, prolonged trauma exposure, often composed of elements of deprivation, betrayal, and interpersonal trauma such as imprisonment, torture, and sexual assault, has been associated with disruptions to adaptive emotional processing and regulation (Liddell et al., 2022; Nickerson et al., 2016; Walsh et al., 2011). Once resettled, refugees then contend with pervasive postmigration stressors and trauma reminders, such as having family members missing or still residing in conflict-affected areas. These stressors have been shown to prompt repeated negative emotions and undermine psychological functioning (Li et al., 2016; Nickerson et al., 2010, 2019). Accordingly, difficulties in regulating one’s emotions may be especially relevant to the development of PTSD in refugees. This is consistent with both theoretical models of PTSD, which posit deficits in emotional processing and regulation as key mechanisms driving the emergence and maintenance of PTSD (Foa et al., 1989; McLean & Foa, 2017; Tull et al., 2020), and wider research that has found robust associations between emotion-regulation difficulties and PTSD (Seligowski et al., 2015; Tull et al., 2020).
In the refugee literature, there is emerging empirical evidence in support of emotion regulation as a psychological mechanism underpinning PTSD. For example, in a cross-sectional study, emotion-regulation difficulties were found to fully mediate the relationship between trauma exposure and PTSD (Nickerson et al., 2015). In a treatment study, Hinton et al. (2009) found that increases in emotion-regulation skills mediated reductions in PTSD symptom severity following culturally adapted cognitive behavior therapy. Likewise, the provision of an emotion-regulation skills-training program (Skills Training of Affect Regulation – A Culture-Sensitive Approach [STARC]) resulted in improvements in both emotion regulation and PTSD symptoms (Koch, Ehring, & Liedl, 2020). Together, these studies provide promising initial evidence that emotion regulation may be a key driver of PTSD symptoms in refugees.
To date, however, very little research (with either refugees or any trauma-affected population) has investigated the temporal relationships between emotion dysregulation and PTSD. One prospective study with 78 adolescents living in Boston at the time of the 2013 Boston Marathon terrorist attack found that greater use of rumination and catastrophizing emotion-regulation strategies before the attack predicted the onset of PTSD symptoms in the month following (Jenness et al., 2016). Likewise, Mayou et al. (2002) found that among 546 survivors of motor-vehicle accidents, greater use of rumination and thought suppression shortly following the accident predicted greater PTSD 3 years later. These studies corroborate that emotion dysregulation may both precede and maintain PTSD. However, the predominant use of cross-sectional designs in the refugee literature precludes the investigation of the direction of influence between emotion dysregulation and PTSD symptoms and means that the prevailing theory that emotion dysregulation is one mechanism underpinning PTSD has remained untested. Moreover, given that postmigration stressors have been shown to be independently associated with PTSD (Li et al., 2016; Nickerson et al., 2019), it may be the case that these ongoing stressors are undermining refugee mental health via disruptions to emotion regulation. Despite this, the temporal influence of postmigration stressors—a key characteristic of the refugee experience—on either emotion dysregulation or PTSD has also remained untested. Longitudinal research with refugees is critically needed to highlight key mechanisms through which to target PTSD and to pinpoint which components of PTSD symptoms are most central to initiating overall reductions in PTSD. Such insights have the potential to inform the development of tailored interventions to alleviate the psychological impact of persecution and displacement among refugees.
In the current study, we aimed to investigate the longitudinal relationship between postmigration stressors, emotion dysregulation, and PTSD symptoms among a large community sample of refugees in a naturalistic setting. Specifically, we aimed to explore the within-persons temporal dynamics between each of the PTSD clusters (reexperiencing, avoidance, alterations in mood and cognition [NAMC], and hyperarousal) from the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013), emotion dysregulation, and postmigration stressors to (a) pinpoint which aspects of PTSD symptoms are most strongly influenced by emotion dysregulation, (b) explore the contribution of postmigration stressors to the longitudinal course of PTSD and emotion dysregulation, and (c) investigate whether there is a cascade of influence between different PTSD clusters over time. Cluster-level investigation is especially useful when investigating PTSD given the enormous heterogeneity of presentations in PTSD (Galatzer-Levy & Bryant, 2013) and the distinctiveness of the PTSD symptom clusters (Yufik & Simms, 2010). Cross-sectional and clinical studies with refugees to date suggest that emotion dysregulation functions as a mechanism underpinning PTSD. However, whether all or specific PTSD clusters are driving this relationship remains unclear.
In this study, we predicted that emotion dysregulation would be most strongly associated with PTSD symptoms of avoidance, NAMC, and hyperarousal. This was based on research indicating that emotion dysregulation is characterized by reduced emotional awareness, heightened emotional reactivity, and a reduced capacity to self-regulate emotional responses, often characterized by a limited scope of emotion-regulation strategies and an overreliance on avoidance-based strategies, such as suppression (Gratz & Roemer, 2004; Gross & Jazaieri, 2014). Specifically, we hypothesized that greater emotion dysregulation would precede increases in avoidance, NAMC, and hyperarousal symptoms over time. Second, we predicted that postmigration stressors would be associated with both emotion dysregulation and all PTSD clusters. The association between postmigration stressors and emotion dysregulation was based on Gross’s (2015) extended process model of emotion regulation, which cites stressors as emotional triggers and thus, a means through which emotion-regulation resources can be depleted. The association between postmigration stressors and PTSD clusters was based on prior research that established the presence of these stressors as unique predictors of PTSD (Porter & Haslam, 2005). Finally, we hypothesized that hyperarousal symptoms would be associated with increases in all other PTSD symptom clusters, consistent with longitudinal research among other trauma-affected populations that found that hyperarousal symptoms were antecedent to increases in all other PTSD clusters (Doron-Lamarca et al., 2015; Marshall et al., 2006; Schell et al., 2004; Solomon et al., 2009).
Method
Participants
Participants were adult refugees and asylum seekers who had participated in the Refugee Adjustment Study—a longitudinal cohort study investigating predictors of refugee mental health and adjustment following resettlement in Australia (Liddell et al., 2021; Nickerson, Byrow, Hoffman, et al., 2022; Nickerson, Byrow, O’Donnell, et al., 2022; Nickerson et al., 2019). A total of 1,081 Arabic-, Farsi-, Tamil-, or English-speaking refugees and asylum seekers resettled in Australia completed the first time point of the study (T1). Of these, 1,041 (96.3%) participants completed the second time point (T2) 6 months following T1, 981 participants (90.7%) completed the third time point (T3) 6 months following T2, 931 participants (86.1%) completed the fourth time point (T4) 6 months following T3, and 889 participants (82.2%) completed the fifth time point (T5) 6 months following T4. These language groups were selected for this study because they represented more than 50% of successful refugee-status applications in Australia at the time of this study’s inception (Department of Immigration and Border Protection, 2014). Participants were recruited via multilingual advertisements at refugee support services and organizations, on social media platforms, in community newspapers, on community radio stations, and via snowball sampling, in line with recommendations for engaging difficult-to-access populations in research (Sadler et al., 2010).
The overall attrition rate was 17.8%. Correcting for multiple comparisons (Bonferroni, α = .05 / 9 = .006), we found no significant differences between participants who completed T5 and participants who did not in terms of baseline PTSD symptoms (M = 0.67 vs. 0.71), t(1013) = −0.68, p = .49; emotion dysregulation (M = 39.6 vs. 41.0), t(933) = −1.22, p = .22; postmigration stressors (M = 1.95 vs. 2.04), t(1003) = −1.40, p = .16; or diversity of trauma exposure (M = 4.1 vs. 4.9), t(318) = −2.47, p = .01. However, some significant differences in baseline demographic factors were present. Although there was no difference in education level, χ2(4) = 9.40, p = .05, participants with complete data were older (M = 38.8 vs. 35.8 years), t(369) = 3.57, p < .001, and had spent less time resettled in Australia (M = 1.8 vs. 2.7 years), t(308) = −6.62, p < .001. In addition, a greater proportion of females had complete data (397 complete, 66 incomplete) compared with males (456 complete, 159 incomplete), χ2(1) = 21.52, p < .001, and a greater proportion of Arabic-speaking participants had complete data (618 complete, 119 incomplete) compared with the other language groups (Farsi: 130 complete, 56 incomplete; Tamil: 34 complete, 20 incomplete; English: 73 complete, 31 incomplete), χ2(3) = 38.63, p < .001.
Measures
Measures used in the Refugee Adjustment Study (for a list of all questionnaires administered, see Table S1 in the Supplemental Material available online) were provided in Arabic, Farsi, Tamil, or English. Non-English versions were translated and blind back translated using “gold-standard” procedures (Bracken & Barona, 1991). Minor discrepancies that emerged from this process were resolved by the research team in consultation with accredited interpreters and cultural experts. To verify the reliability of the translated versions of each questionnaire, the internal consistency of each scale was additionally computed per language group. Internal consistency estimates (α) ranged from .720 to .951 and are presented in Table S2 in the Supplemental Material.
Exposure to potentially traumatic events
The 16-item Harvard Trauma Questionnaire (HTQ; Mollica et al., 1992) was used at T1 to index exposure to different types of traumatic events commonly experienced by refugees. Participants reported whether they had experienced, witnessed, or learned about each potentially traumatic event (PTE). A total count of the number of different types of PTEs that each participant had experienced and/or witnessed was derived for the present study.
Postmigration stressors
The 25-item Post-Migration Living Difficulties (PMLD) Checklist (Silove et al., 1998; Steel et al., 1999) was used to index exposure to different types of postmigration stressors. The scale, developed specifically for refugees in a resettlement context, measures common living difficulties in the areas of employment, immigration, housing, income, access to health services, social integration, and family separation. Participants rated each living difficulty on a 5-point scale (1 = was not a problem/did not happen, 5 = a very serious problem). At T1, living difficulties were rated over the past 12 months. All subsequent administrations of the scale (T2–T5) asked participants to rate their level of living difficulties over the past 6 months (i.e., over the period since the previous measurement occasion). A mean score was calculated for the present study. Internal consistency for this scale was α = .94 (T1), α = .94 (T2), α = .95 (T3), α = .95 (T4), and α = .95 (T5).
PTSD symptoms
The 16-item Posttraumatic Diagnostic Scale for DSM-IV (PDS; Foa et al., 1997) was used to measure PTSD symptom severity. Because our study commenced before the publication of the DSM-5 (American Psychiatric Association, 2013) version of the PDS, we adapted the original scale to include four additional items to reflect the new DSM-5 PTSD criteria: persistent negative beliefs, distorted blame of self or others, persistent negative emotional state, and risk-taking behavior. Participants rated on a 4-point scale (0 = not at all/only once, 3 = 5+ times a week/almost always) how often each symptom bothered them over the past month. To calculate probable PTSD diagnosis (Foa et al., 1997), symptoms were considered to be present if they were rated as 1 (once a week/at least once in a while) or higher. In addition, a mean score of PTSD symptom severity for each cluster (reexperiencing, avoidance, NAMC, and hyperarousal) was calculated. Internal consistency for these subscales were as follows: reexperiencing: α = .92 (T1), α = .94 (T2), α = .94 (T3), α = .94 (T4), α = .95 (T5); avoidance (split-half reliability, Spearman-Brown corrected): α = .83 (T1), α = .82 (T2), α = .86 (T3), α = .85 (T4), α = .88 (T5); NAMC: α = .90 (T1), α = .92 (T2), α = .92 (T3), α = .92 (T4), α = .93 (T5); hyperarousal: α = .89 (T1), α = .89 (T2), α = .90 (T3), α = .90 (T4), α = .90 (T3).
Emotion dysregulation
The Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004) was used to measure emotion dysregulation. In the current study, we used a shortened 18-item version of the original 36-item self-report scale to reduce assessment burden. Furthermore, we adapted some of the original items that required reverse-scoring to ensure that all items were phrased in the same direction, where higher scores reflected greater difficulties in emotion regulation (e.g., “I pay attention to how I feel” was reworded to “I do not pay attention to how I feel”). The decision to reword reverse-scored items was based on cross-cultural research demonstrating poor internal consistency among reverse-scored items (Nickerson et al., 2015; Schlechter et al., 2021). This scale has previously been validated for use with refugees (Doolan et al., 2017). Response options ranged from 1 (almost never, 0%–10%) to 5 (almost always, 91%–100%) such that higher scores reflected greater emotion dysregulation. The internal consistency for this scale was α = .94 (T1), α = .95 (T2), α = .95 (T3), α = .95 (T4), and α = .95 (T3).
Procedure
Baseline data (T1) were collected between April 2015 and January 2018. Following time points (T2–T5) were then administered at 6-month intervals. Prospective participants who had registered their interest in the study online were first screened by telephone to determine eligibility (refugee or asylum-seeker background residing in Australian community, arrival in Australia in or after January 2011, age 18+ years, literate in Arabic, Farsi, Tamil, or English). Eligible participants then completed the survey online via a personalized link to the KeySurvey platform or, for those without Internet or technology access, by returning a paper version of the survey in the post. Six months following each participant’s T1 completion date, participants were sent the T2 survey. Likewise, 6 months following T2 completion, participants received the T3 survey, and so on such that T1 through T5 were completed over a 2-year period. Participants received an $AUD25 shopping voucher after the completion of each time point. This study was performed in line with the principles of the Declaration of Helsinki. Ethics approval for the project was provided by the University of New South Wales Human Research Ethics Committee (HC14106).
Data analysis
Planned analysis
Random intercept cross-lagged panel analysis (Hamaker et al., 2015) was conducted using Mplus (Version 8; Muthén & Muthén, 2019) to test the within-persons temporal relationships and between-persons associations between emotion dysregulation, postmigration stressors, reexperiencing, avoidance, NAMC, and hyperarousal across the five time points. A schematic representation of the variables used in the random intercept cross-lagged model is presented in Figure 1. Random intercept cross-lagged panel models (RI-CLPMs) parse out the variance in the observed scores into within- and between-persons components. Traditional approaches to modeling longitudinal data, such as cross-lagged panel models (CLPMs), have been criticized for confounding between-persons associations (i.e., stable between-persons differences, such as individual differences in levels of PTSD symptoms) with within-persons change over time (Hamaker et al., 2015). Accordingly, by partitioning the within- and between-persons variance, RI-CLPMs offer more precise estimates of within-persons temporal dynamics. Random intercepts (RI.PMLD, RI.Reexperiencing, RI.Avoidance, RI.NAMC, RI.Hyperarousal. and RI.DERS) are specified for each variable (PMLD1–PMLD5, Reexperiencing1–Reexperiencing5, Avoidance1–Avoidance5, NAMC1– NAMC5, Hyperarousal1–Hyperarousal5, and DERS1–DERS5). In this way, the random intercepts capture a participant’s time-invariant deviations from the grand mean of the observed variables (postmigration stressors, emotion dysregulation, and PTSD symptoms) to account for stable differences between participants. The remaining within-persons components (wPMLD1–wPMLD5, wReexperiencing1–wReexperiencing5, wAvoidance1–wAvoidance5, wNAMC1–wNAMC5, wHyperarousal1–wHyperarousal5, and wDERS1–wDERS5) thus reflect the differences between a participant’s observed measurement and their expected score (derived from the grand mean and random intercepts) for each variable at a given time point. The within-persons portion of the RI-CLPM estimates (a) autoregressive effects, where within-persons components are regressed on themselves to account for the persistence of each variable over time, and (b) cross-lagged effects, where within-persons components are regressed on each other to test how one’s level of a particular variable at one time point (e.g., emotion dysregulation at T1) predicts changes in the other variables at the next time point (i.e., reexperiencing at T2). Given the aims of the current study, we were particularly interested in exploring potential cross-lagged effects.
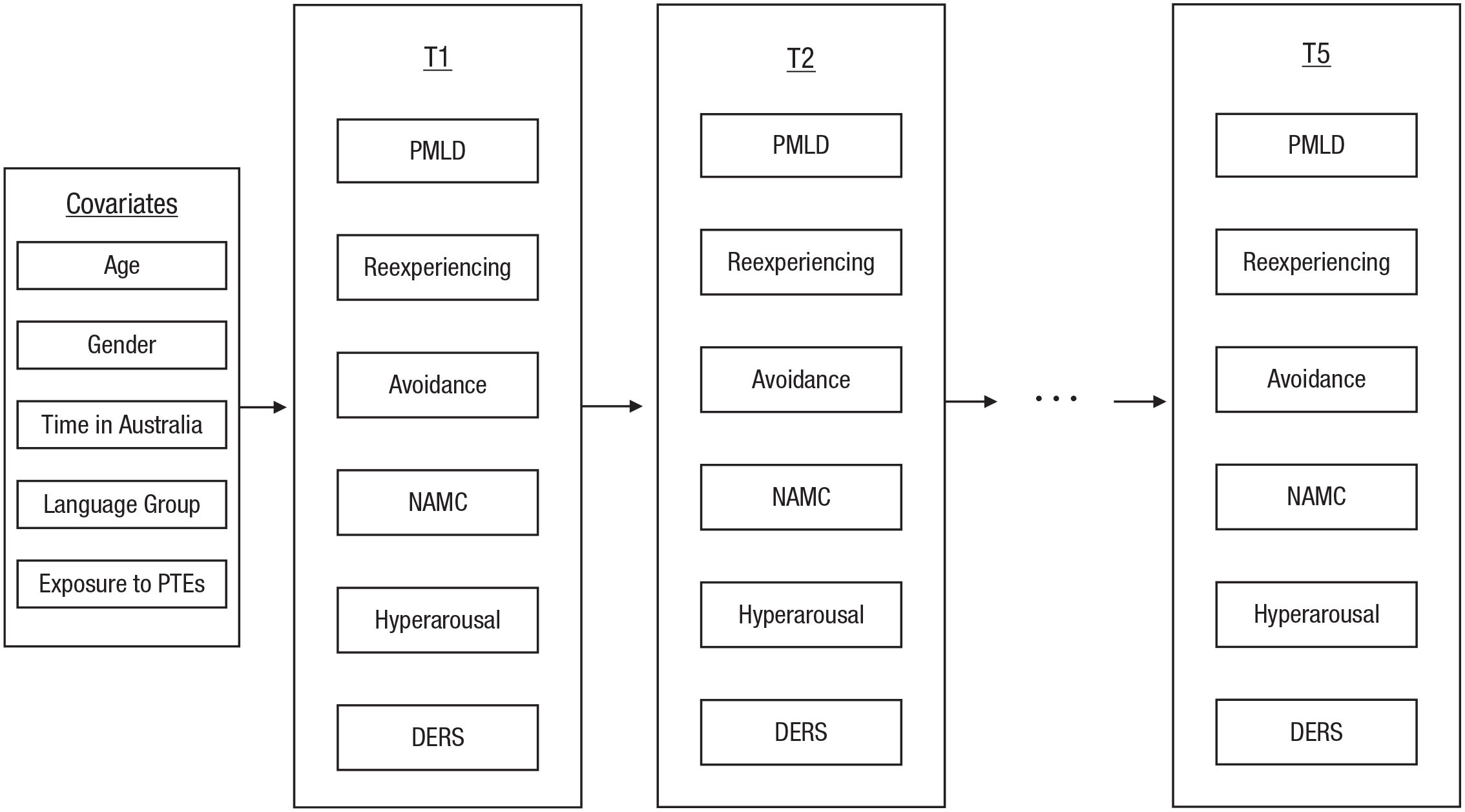
Schematic representation of Time 1 (T1) through Time 5 (T5) variables used in the random intercept cross-lagged model (RI-CLPM). Note that although observed scores are illustrated above, RI-CLPM generates latent variables of T1 through T5 observed scores (including between-persons random intercepts and within-persons deviations). PTEs = potentially traumatic events; PMLD = postmigration living difficulties; NAMC = negative alterations in mood and cognition; DERS = Difficulties in Emotion Regulation Scale.
RI-CLPM specifications followed that of Hamaker et al. (2015). Missing data were handled using full information maximum likelihood estimation. Random intercepts (RI.PMLD, RI.Reexperiencing, RI.Avoidance, RI.NAMC, RI.Hyperarousal, and RI.DERS) were specified in MPlus by creating latent variables with the repeated measures for each variable (PMLD1–PMLD5, Reexperiencing1–Reexperiencing5, Avoidance1–Avoidance5, NAMC1–NAMC5, Hyperarousal1–Hyperarousal5, and DERS1–DERS5) as its indicators. All factor loadings were fixed to 1. We specified that all random intercepts were correlated. Within-persons components (wPMLD1–wPMLD5, wReexperiencing1–wReexperiencing5, wAvoidance1–wAvoidance5, wNAMC1–wNAMC5, wHyperarousal1–wHyperarousal5, and wDERS1–wDERS5) were created by specifying a latent variable for each measurement occasion and fixing factor loadings to 1. Measurement-error variances were constrained to 0. Specific structural relations between the within-persons components were specified to investigate the temporal dynamics between postmigration stressors, emotion dysregulation, and PTSD symptoms; these included estimating autoregressive paths, cross-lagged effects, and the covariance between within-persons’ components (at T1) and residuals of the within-persons components (at the subsequent time points). In line with recent recommendations and prior studies (Mulder, 2022; Mulder & Hamaker, 2021; Orth et al., 2021; Sewall et al., 2022), autoregressive and cross-lagged paths were constrained to equality. This approach was informed by three factors: (a) The time intervals between each measurement occasion were equal (6 months), (b) we did not expect to observe systematic differences between the time points, and (c) constraining pathways is recommended for complex models to increase their stability and interpretability. Model fit was evaluated in line with recommendations in which a comparative fit index (CFI) greater than .95, Tucker-Lewis index (TLI) greater than .95, standardized root mean square residual (SRMR) less than .08, and root mean square error of approximation (RMSEA) less than .06 were considered to indicate good fit (Hu & Bentler, 1999).
As a final step and to control for the effects of key demographic variables on the within-persons dynamic effects, covariates (age, gender, time resettled in Australia, exposure to PTEs, and language group) were specified as predictors of each random intercept. Continuous covariates were mean-centered. Missing data rates among the covariates ranged from 0% to 4.2%.
Post hoc analyses
In addition to the main RI-CLPM analysis (detailed above), which used the total score of the DERS to index overall emotion dysregulation, we ran exploratory analyses to investigate whether each of the six DERS subscales yielded differential temporal relationships with PMLD and PTSD symptom clusters. These analyses were conducted post hoc in response to reviewer and editorial feedback. A single RI-CLPM, comprising PMLD, the four PTSD clusters, and the six DERS subscales (i.e., Nonacceptance, Goals, Impulsivity, Awareness, Strategies, and Clarity) was too complex to yield stable results. Consequently, we constructed six separate RI-CLPMs (each with the same predictors—PMLD and the four PTSD clusters—but with a different DERS subscale in each model) to compare the pattern of findings from each of these models with the planned model that used the DERS total score. The specifications of these exploratory RI-CLPMs were identical to the data-analytic procedure detailed above for the planned analysis. For instance, all models included the same covariates, and the autoregressive and cross-lagged paths across the five time points were constrained to equality. Because each DERS subscale model yielded a very similar pattern of results to the planned DERS total model, in this article, we focus solely on outlining and discussing the findings from the planned analysis. Findings from the post hoc analyses are available in Appendix C in the Supplemental Material.
Results
Sample characteristics
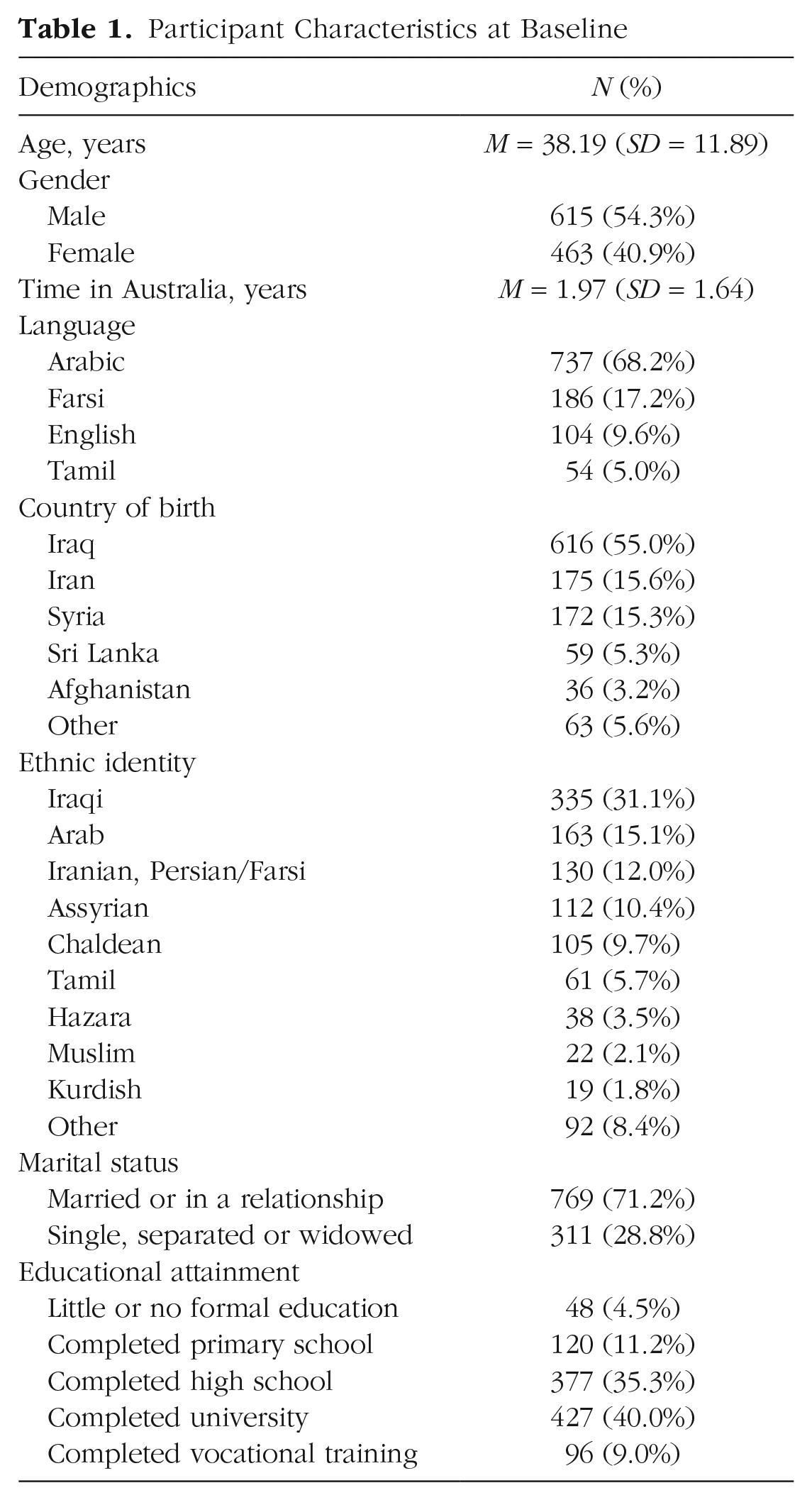
Demographic characteristics of the sample at baseline (T1) are presented in Table 1. At baseline, participants reported being exposed to a mean of 4.24 (SD = 4.43) different types of PTEs. Seven hundred sixty-nine participants (71.6%) reported that they had experienced or witnessed at least one type of PTE. The frequency and percentage of participants who were exposed to each type of PTE are presented in Table S4 in the Supplemental Material. Mean PTSD symptom severity was 13.59 (SD = 14.08, range = 0–60). Consistent with recent prevalence estimates among refugee community samples (Blackmore et al., 2020; Henkelmann et al., 2020), we found that approximately one third of our sample (337 participants; 35.6%) met criteria for a probable DSM-5 (American Psychiatric Association, 2013) PTSD diagnosis at T1.
Participant Characteristics at Baseline
Preliminary analyses
The means and standard deviations of and correlations between PTSD symptom clusters, emotion dysregulation, and postmigration stressors for each time point are presented in Tables S5 and S6 in the Supplemental Material. All variables yielded significant and positive bivariate correlations at each time point.
Random intercept cross-lagged panel analysis
Model fit
Goodness-of-fit indices for our RI-CLPM were as follows: CFI = .991, TLI = .988, SRMR = .020, and RMSEA = .023 (90% confidence interval = [.020, .026]). Our model had excellent fit according to the CFI, TLI, SRMR, and RMSEA criteria.
Between-persons correlations
All between-persons components of the model (random intercepts) yielded significant variance, indicating the presence of stable between-persons differences in levels of postmigration stressors, emotion dysregulation, and PTSD symptom clusters. In addition, all random intercepts were positively and significantly correlated (see Table S7 in the Supplemental Material).
Within-persons temporal dynamics between PTSD symptoms clusters, emotion dysregulation, and postmigration stressors
The standardized and unstandardized autoregressive effects and cross-lagged effects are presented in Table 2. The correlations between the within-persons components are presented in Table S7 in the Supplemental Material. For ease of interpretation, Figure 2 shows the standardized cross-lagged effects of emotion dysregulation and postmigration stressors on PTSD symptom clusters, and Figure 3 shows the standardized cross-lagged effects among the PTSD symptom clusters.
Random Intercept Cross-Lagged Model: Unstandardized and Standardized Within-Persons Autoregressive Effects and Cross-Lagged Paths
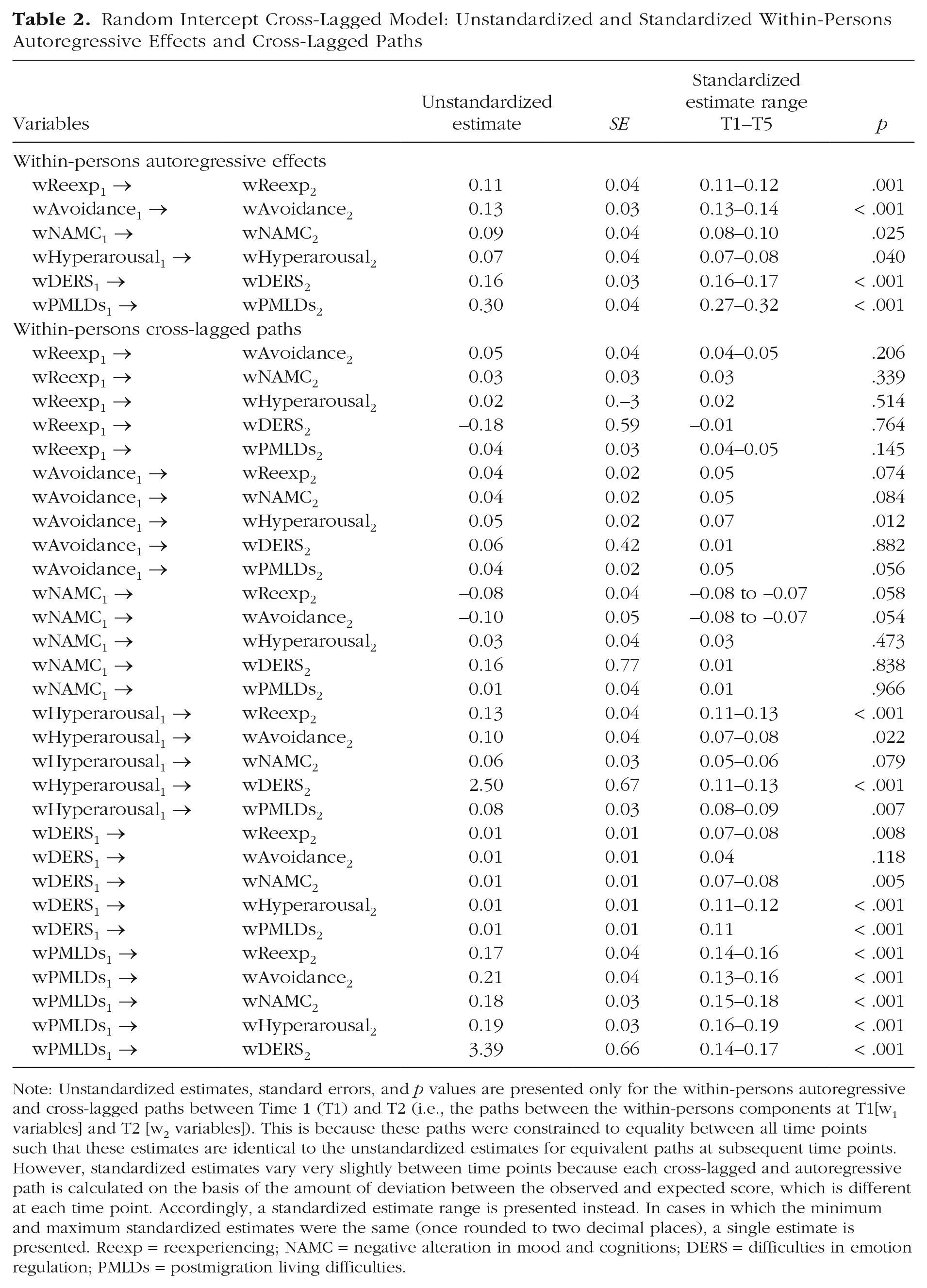
Note: Unstandardized estimates, standard errors, and p values are presented only for the within-persons autoregressive and cross-lagged paths between Time 1 (T1) and T2 (i.e., the paths between the within-persons components at T1[w1 variables] and T2 [w2 variables]). This is because these paths were constrained to equality between all time points such that these estimates are identical to the unstandardized estimates for equivalent paths at subsequent time points. However, standardized estimates vary very slightly between time points because each cross-lagged and autoregressive path is calculated on the basis of the amount of deviation between the observed and expected score, which is different at each time point. Accordingly, a standardized estimate range is presented instead. In cases in which the minimum and maximum standardized estimates were the same (once rounded to two decimal places), a single estimate is presented. Reexp = reexperiencing; NAMC = negative alteration in mood and cognitions; DERS = difficulties in emotion regulation; PMLDs = postmigration living difficulties.
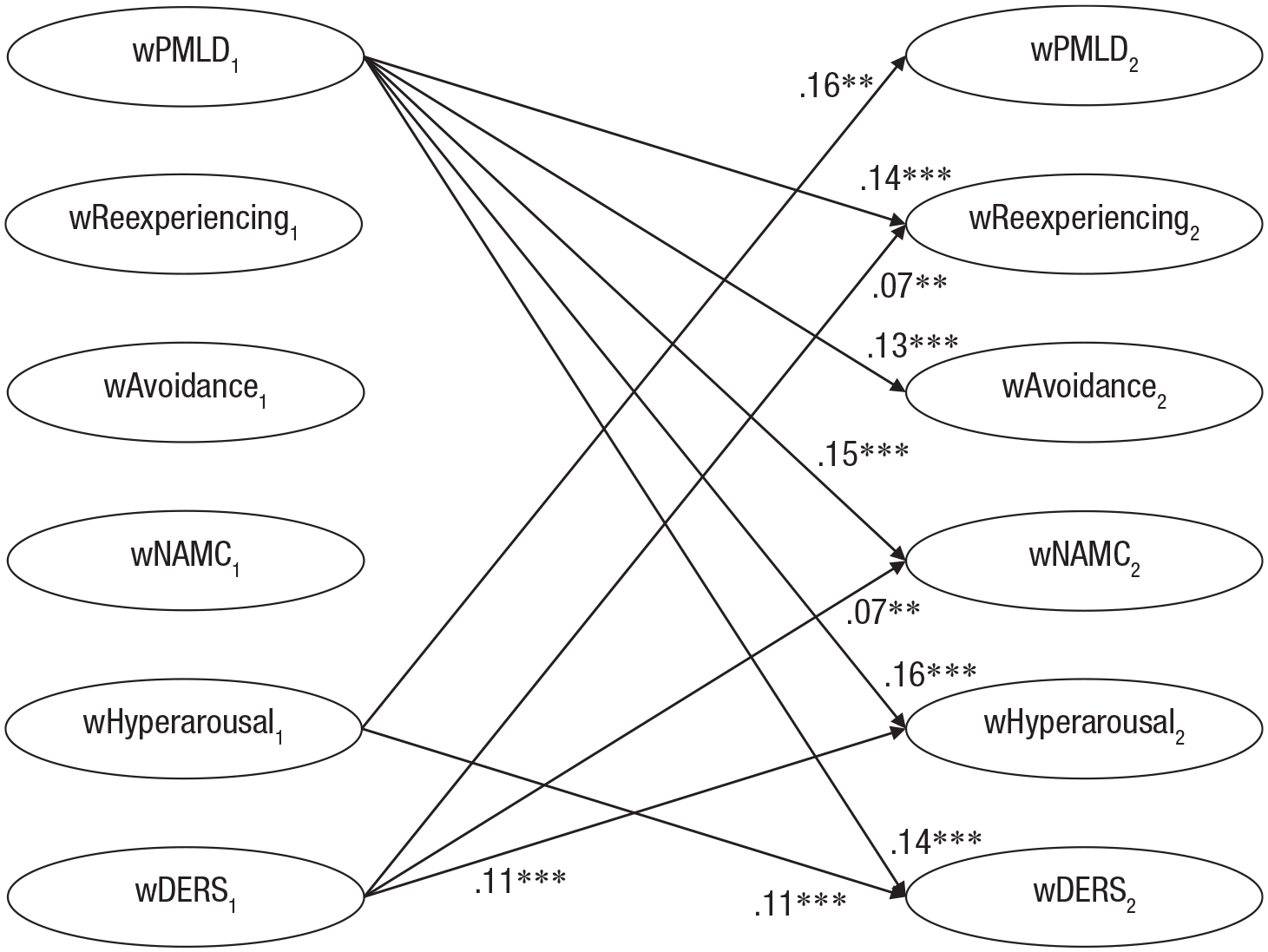
Temporal influence of emotion dysregulation and postmigration stress over time: standardized cross-lagged effects. Only significant paths are shown. For ease of interpretation, only the significant within-persons cross-lagged paths are shown. (Because the model was constrained, estimates of the standardized cross-lagged effects from T1 [T1] to T2 are very similar to those from T2 to T3, T3 to T4, and T4 to T5.) PMLD = postmigration living difficulties; NAMC = negative alterations in mood and cognition; DERS = Difficulties in Emotion Regulation Scale. Asterisks indicate significant paths (*p < .05, **p < .01, ***p < .001).
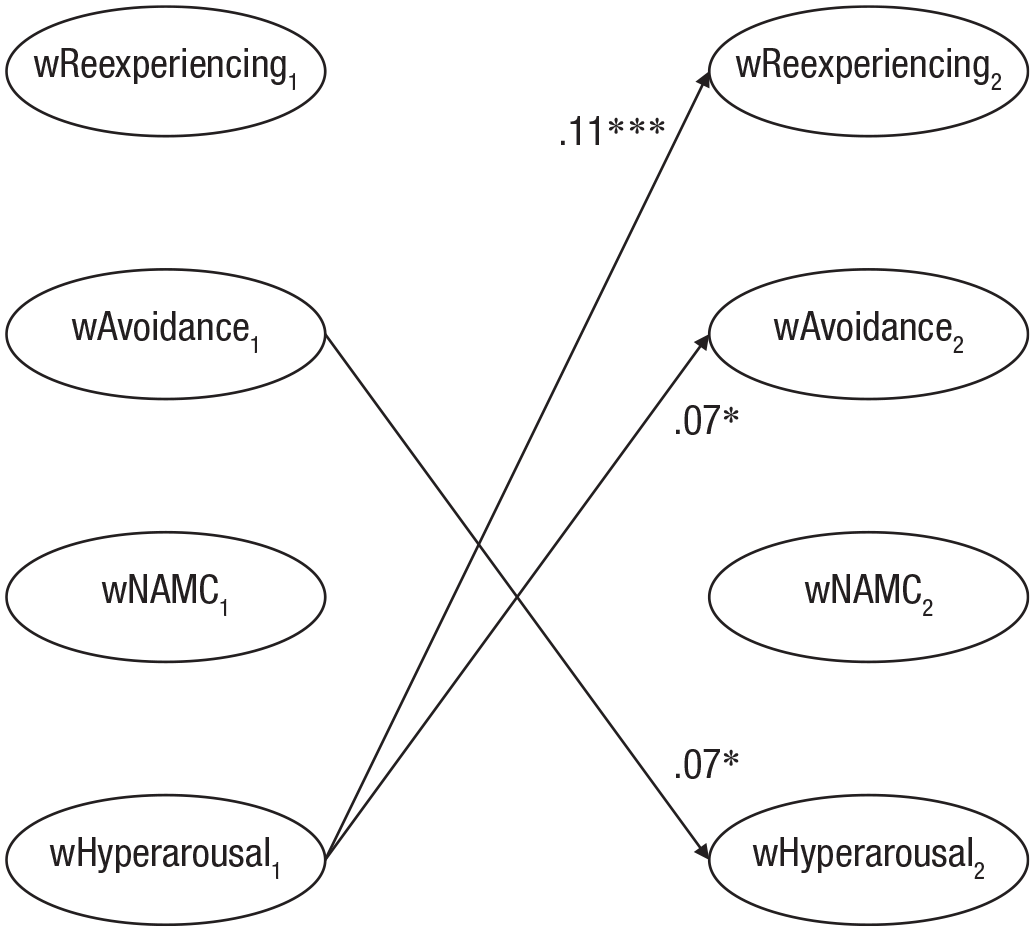
Temporal associations among the posttraumatic stress disorder (PTSD) symptom clusters over time: standardized cross-lagged effects. For ease of interpretation, only the significant within-persons cross-lagged paths are shown. (Because the model was constrained, estimates of the standardized cross-lagged effects from Time 1 [T1] to T2 are very similar to those from T2 to T3, T3 to T4 and T4 to T5.) NAMC = negative alterations in mood and cognition. Asterisks indicate significant paths (*p < .05, **p < .01, ***p < .001).
Regarding the longitudinal influence of emotion dysregulation, in line with our hypothesis, emotion dysregulation was temporally associated with NAMC and hyperarousal symptoms. However, contrary to our hypothesis, emotion dysregulation was also temporally associated with reexperiencing symptoms, although there was no significant longitudinal association between emotion dysregulation and avoidance symptoms. Emotion dysregulation had an antecedent temporal influence on reexperiencing and NAMC symptoms over time. Specifically, elevated levels of emotion dysregulation, relative to a participant’s typical level of emotion dysregulation, predicted greater increases in both reexperiencing and NAMC symptom severity at the subsequent time point. In addition, emotion dysregulation was bidirectionally associated with hyperarousal symptoms such that elevated levels of emotion dysregulation predicted increases in hyperarousal symptom severity at the subsequent time point and vice versa.
Regarding the longitudinal influence of postmigration stressors, as hypothesized, postmigration stressors were associated with all other variables. First, postmigration stressors were bidirectionally associated with emotion dysregulation and hyperarousal symptoms. Second, postmigration stressors were antecedent to increases in reexperiencing, avoidance, and NAMC symptoms.
Within-persons temporal associations among PTSD symptoms clusters
In partial support of our hypothesis, hyperarousal symptoms were temporally related to reexperiencing and avoidance symptoms. Specifically, hyperarousal symptoms were antecedent to increases in reexperiencing symptoms over time and bidirectionally associated with avoidance symptoms. No other significant cross-lagged effects between the PTSD symptom clusters emerged.
Associations between demographic factors, refugee experiences, and exposure to PTEs
The covariate paths (i.e., predictors of stable between-persons differences in overall levels of emotion dysregulation, postmigration stressors, and PTSD symptom clusters) are presented in Table S8 in the Supplemental Material. Being female, having spent a greater time in Australia, being exposed to more types of PTEs, and being from a Farsi-speaking or English-speaking background (compared with an Arabic-speaking background) was associated with greater overall emotion dysregulation. Elevated overall levels of postmigration stressors were predicted by having spent more time living in Australia, being exposed to more types of PTEs, and being from a Farsi-speaking background (compared with an Arabic-speaking background). Being female, having spent more time living in Australia, and greater exposure to more types of PTEs were associated with greater overall reexperiencing, avoidance, NAMC, and hyperarousal symptoms. In addition, participants from English-speaking backgrounds were more likely to have elevated overall avoidance symptoms.
Discussion
In the current study, we aimed to investigate the within-persons temporal relationships between emotion dysregulation, postmigration stressors, and PTSD symptoms among a community sample of refugees. In partial support of our hypothesis, emotion dysregulation was temporally associated with some PTSD symptom clusters. As hypothesized, we found that elevated levels of emotion dysregulation were antecedent to increases in NAMC symptoms and bidirectionally associated with increases in hyperarousal symptoms. In addition, elevated levels of emotion dysregulation preceded subsequent increases in reexperiencing symptoms. Contrary to our hypothesis, we did not find a significant association between emotion dysregulation and symptoms of avoidance over time. These findings largely accord with prior research showing an association between emotion regulation and PTSD in refugees (Hinton et al., 2009; Koch, Ehring, & Liedl, 2020; Nickerson et al., 2015) and extend this research to more precisely identify which aspects of PTSD symptoms are particularly driving this effect (i.e., reexperiencing, NAMC, and hyperarousal symptoms). Furthermore, our findings provide insight into the direction of influence between these factors, indicating that emotion dysregulation precedes but is not preceded by increases in reexperiencing and NAMC symptoms, whereas emotion dysregulation is reciprocally associated with hyperarousal symptoms. The particular relevance of emotion dysregulation to reexperiencing, NAMC, and hyperarousal symptoms aligns with theoretical models of emotion dysregulation. Quintessentially, emotion dysregulation is characterized by a heightened sensitivity and reactivity to emotional triggers combined with a diminished capacity to adaptively self-regulate in response to these triggers (Gratz & Roemer, 2004; Gross & Jazaieri, 2014). Accordingly, elevated levels of emotion dysregulation would precipitate increases in PTSD symptoms that result from heightened sensitivity and reactivity to emotional triggers. For instance, greater levels of emotion dysregulation may amplify an individual’s reactivity to trauma-related reminders, thus increasing the severity of reexperiencing symptoms such as intrusive memories and psychological and physiological reactivity to internal and external cues resembling past trauma. Likewise, increases in emotion dysregulation may serve to intensify an individual’s reactivity to diffuse emotional stressors, thus increasing the severity of hyperarousal symptoms such as hypervigilance, startle response, irritability, and concentration difficulties. In turn, this chronic state of hyperarousal may serve to deplete emotion-regulation resources and precipitate greater subsequent dysregulation. Relatedly, emotion dysregulation would also necessarily precipitate PTSD symptoms that result from a limited repertoire of effective emotion-regulation strategies (e.g., NAMC symptoms such as persistent negative emotional state, anhedonia/behavioral inhibition, social disconnection, diminished positive affect, and exaggerated negative thinking). Accordingly, these symptom profiles may be especially salient to the presentation of PTSD in refugees, and thus it may be valuable to tailor existing first-line PTSD treatments, which have traditionally focused on reexperiencing and avoidance symptoms (Phoenix Australia, 2020), to additionally target symptoms of NAMC and hyperarousal. For instance, our findings suggest that emotion-regulation capacity building may be a fruitful way to facilitate reductions in these PTSD symptoms among refugees.
However, it was somewhat surprising that avoidance symptoms were not associated with emotion dysregulation longitudinally. Indeed, a prior meta-analysis found large effect sizes for the association between PTSD symptoms and avoidance-based emotion-regulation strategies, including thought suppression and experiential avoidance (Seligowski et al., 2015). However, note that engagement in avoidance-based strategies is not universally maladaptive (Bonanno et al., 1995; Park, 2010) and thus may not necessarily always be associated with emotion dysregulation. Furthermore, because the participants in our study had been resettled in Australia for a mean of 2 years, it is likely for most participants that it had been many years since their trauma exposure. Many of our participants were likely experiencing long-term PTSD symptoms, and thus, avoidance may have been so well integrated into their daily behaviors that participants did not identify it as avoidance. Indeed, prior longitudinal research on PTSD has found that avoidance symptoms were particularly prominent in influencing the development of PTSD but not its maintenance (Creamer et al., 2004; O’Donnell et al., 2007). Finally, our finding may be the result of methodological differences between our study and prior research on emotion regulation and PTSD. First, although prior research has generally used a unitary construct for PTSD (typically a total symptom severity score), we explored PTSD on a cluster level, which tested the influence of avoidance symptoms over and above that of other PTSD symptoms. Second, rather than measuring participants’ engagement in specific emotion-regulation strategies, such as thought suppression, we used the DERS (Gratz & Roemer, 2004) to index overall emotion dysregulation, which instead assessed key functional processes underpinning emotion dysregulation, such as a lack of emotional awareness, emotional clarity, or ability to use emotion-regulation strategies when distressed. Although these factors may account for our finding, it would be nonetheless valuable for our study to be replicated with other refugee populations.
Another key finding of the present study was that postmigration stressors had a diffuse and deleterious influence on the longitudinal course of both emotion dysregulation and PTSD symptoms. As hypothesized, postmigration stressors and emotion dysregulation were temporally associated. Specifically, this relationship was bidirectional such that increased exposure to postmigration stressors predicted subsequent increases in emotion dysregulation and vice versa. Moreover, elevated exposure to postmigration stressors was antecedent to increases in reexperiencing, avoidance, and NAMC symptoms and reciprocally associated with increases in hyperarousal symptoms. This finding accords with prior cross-sectional research that has found an independent association between postmigration stressors and PTSD symptoms (Li et al., 2016; Nickerson et al., 2019) and theoretical models of emotion regulation that cite the role of stressors (i.e., emotional triggers) in depleting emotion-regulation resources (Gross, 2015). Our findings can be interpreted using Sheppes and Gross’s (2011) timing hypothesis, which argues that as emotions become more intense, emotion-regulation strategies become more effortful and less effective. In this way, unrelenting postmigration stressors may be especially insidious because they make negative emotions more diffuse and attempts at emotion regulation less successful. The present study extends prior research to show that the deleterious effect of ongoing stressors on PTSD occurred via a direct exacerbation of each PTSD clusters and an exacerbation in emotion dysregulation. These findings provide novel longitudinal evidence in support of a vicious cycle between contemporary stressors, emotion dysregulation, and PTSD symptoms that serve to maintain a chronic course of PTSD in refugees. In light of these findings, a valuable future line of inquiry would be to test for a possible interaction effect between emotion dysregulation and postmigration stressors on PTSD symptoms. Although psychological interventions may aid in increasing an individual’s capacity to cope with postmigration stressors, our finding points to the additional utility of case-management support and structural interventions that might be able to directly ameliorate these stressors by expanding the scope of refugee host nation service provision and welfare schemes to aid in the resettlement process.
The final key finding of the present study was that hyperarousal symptoms were central to the longitudinal course of PTSD in refugees. In partial support of our hypothesis, hyperarousal symptoms were temporally associated with all other PTSD symptom clusters, except for NAMC. Specifically, we found that hyperarousal symptoms were antecedent to increases in reexperiencing symptoms over time and was reciprocally associated with avoidance symptoms. This pattern of results is similar to prior longitudinal studies of PTSD symptoms that found that hyperarousal symptoms were antecedent to all other PTSD clusters (Doron-Lamarca et al., 2015; Marshall et al., 2006; Schell et al., 2004; Solomon et al., 2009). In fact, the centrality of hyperarousal symptoms to the longitudinal course of PTSD appears to be a robust finding that has persisted across both the fourth and fifth editions of the DSM conceptualizations of PTSD clusters and different trauma-affected populations, including survivors of community violence (Marshall et al., 2006; Schell et al., 2004) and military samples in Israel (Solomon et al., 2009) and America (Doron-Lamarca et al., 2015). The central influence of hyperarousal symptoms to the development of PTSD may be explained by evidence suggesting that the presence of physiological indictors of arousal immediately following trauma exposure predicts the subsequent onset of PTSD (Coronas et al., 2011; Suendermann et al., 2010). However, contrary to prior studies, increases in hyperarousal symptoms did not predict subsequent increases in NAMC symptoms, and more broadly, we found relatively fewer significant cross-lagged paths between the PTSD symptoms clusters. This may be due to a methodological difference between our study, which employed an RI-CLPM to explore within-persons temporal dynamics, and prior investigations, which employed CLPMs to explore between-persons temporal associations. The analytic approach used in past studies did not control for stable trait-like differences between participants (i.e., the fact that participants likely differed in their average levels of PTSD symptoms, which may have caused temporal relationships to be overstated; Hamaker et al., 2015). Further investigations of PTSD symptoms using RI-CLPMs are needed to verify this possibility and replicate our findings. Notwithstanding this, our findings suggest that hyperarousal symptoms are an important clinical target in PTSD treatment with refugees.
A number of limitations are noteworthy. First, there are some limitations to the generalizability of our findings to wider refugee populations. When conducting research with communities that are hard to reach, methodological adaptations are required to make research participation more accessible and less burdensome (Sadler et al., 2010). Participants in the current study were mostly recruited via snowball sampling. In addition, because the study was conducted online, participants were required to be literate in either Arabic, Farsi, Tamil, or English. As a result of the sampling procedures and eligibility requirements, findings from our convenience sample may not be generalizable to all members of the Australian refugee community. Furthermore, our findings provide insight into the longitudinal course of PTSD in a community sample of refugees and thus may not be generalizable to clinical or treatment-seeking samples. In addition, because participants had been resettled in Australia for a mean of 2 years, our findings provide insights into the psychological factors associated with the maintenance and chronic course of PTSD and may not generalize to the experiences of refugees immediately following resettlement. Future research investigating the temporal dynamics of emotion dysregulation, postmigration stress, and PTSD among clinical samples and in the acute stages of resettlement is warranted. Second, the measurement of PTSD and emotion dysregulation could be improved. The current study used self-report scales to assess PTSD symptom severity and emotion dysregulation. Although these scales are well validated and have previously been used with cross-cultural refugee samples (Doolan et al., 2017; Koch, Liedl, & Ehring, 2020; Specker & Nickerson, 2019), clinician-administered scales provide a more rigorous assessment of psychological constructs, such as PTSD. Regarding emotion dysregulation, the DERS total score, rather than each of the DERS subscales, was used. Although the current study adopted a more parsimonious approach by using the DERS total score, we note that the scale authors (Gratz & Roemer, 2004) suggested that a subscale-level analysis may be more informative. Although this analysis was too statistically complex to undertake in the current study, future investigations that isolate the specific components of emotion dysregulation that may be especially salient to its relationship with PTSD symptoms are warranted. Furthermore, because emotion dysregulation is a multidimensional construct, the inclusion of behavioral (Specker & Nickerson, 2023), physiological (Spiller et al., 2019), and neurological (Liddell et al., 2022) indices of emotion dysregulation would provide a more comprehensive assessment. Third, although the current study was based on Gratz and Roemer’s (2004) integrative conceptualization of emotion-regulation difficulties, other aspects of emotion regulation that may be relevant to PTSD, such as the use of adaptive or maladaptive emotion-regulation strategies (Gross & Jazaieri, 2014; Seligowski et al., 2015) and emotion-regulation flexibility (Aldao et al., 2015; Fine et al., 2021; Levy-Gigi et al., 2016), were not measured in the present study. This would be a valuable avenue for future research. Finally, emotion dysregulation has been proposed as a transdiagnostic factor underpinning multiple forms of psychopathology in refugees (Koch, Liedl, & Ehring, 2020) and other populations (Aldao et al., 2010). Future research would greatly benefit from exploring the impact of emotion dysregulation on the longitudinal course of different dimensions of psychopathology using transdiagnostic frameworks such as the Hierarchical Taxonomy of Psychopathology (Kotov et al., 2017).
Findings from the present study have several potential clinical implications. First, our study provides novel evidence in support of emotion dysregulation as a mechanism underpinning the maintenance of PTSD in refugees. We found that emotion dysregulation particularly undermines a refugee’s capacity to manage reexperiencing, NAMC, and hyperarousal symptoms and that elevated hyperarousal symptoms worsen emotion dysregulation over time. Given this finding and that hyperarousal was additionally found to be a key driver of most PTSD clusters over time, targeting emotion dysregulation in treatment with refugees may be an effective way to initiate reductions in PTSD. Second, our findings highlight ways in which existing PTSD treatments can be augmented for the specific needs of refugees. For instance, these results suggest that treatment gains may be optimized by concurrently or sequentially providing both exposure-based therapy and emotion-regulation skills training. Moreover, given the extraordinary heterogeneity in PTSD presentations and the emergence of multiple treatments for refugees, including both PTSD-specific (e.g., narrative exposure therapy) and transdiagnostic interventions (e.g., Problem Management Plus, STARC), our findings highlight avenues for personalizing treatment for refugees by pairing a treatment or a combination of treatments to the specific presentation of an individual. Finally, our finding that greater postmigration stressors had a deleterious impact on all PTSD clusters and emotion dysregulation strongly suggests that the contemporary environment and living conditions for refugees have a substantial impact on long-term psychological functioning. Consequently, our findings suggest that addressing and ultimately reducing key postmigration stressors may be an effective and efficient way to alleviate the mental-health burden of PTSD in refugees. For instance, valuable targets for policy and service provision in the refugee sector could include greater access to relevant services and the provision of secure visas and schemes that facilitate financial security, host-language acquisition, and family reunification. Although tentative, the findings from the present study offer compelling evidence in support of both psychological and structural interventions in addressing PTSD in refugees.
Findings from the present study highlight the temporal impact of emotion dysregulation and postmigration stressors on the longitudinal course of PTSD symptoms among individuals from a refugee background. In particular, these results provide novel evidence in support of emotion dysregulation as a psychological mechanism underpinning PTSD in refugees and emphasize the impact of contemporary stressors in exacerbating the mental-health burden experienced by refugees. Our findings suggest that interventions seeking to promote psychological recovery among refugees may benefit from considering both clinical targets, such as emotion dysregulation, and sociological factors, such as postmigration living difficulties.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026231164393 – Supplemental material for The Longitudinal Association Between Posttraumatic Stress Disorder, Emotion Dysregulation, and Postmigration Stressors Among Refugees
Supplemental material, sj-docx-1-cpx-10.1177_21677026231164393 for The Longitudinal Association Between Posttraumatic Stress Disorder, Emotion Dysregulation, and Postmigration Stressors Among Refugees by Philippa Specker, Belinda J. Liddell, Meaghan O’Donnell, Richard A. Bryant, Vicki Mau, Tadgh McMahon, Yulisha Byrow and Angela Nickerson in Clinical Psychological Science
Footnotes
Acknowledgements
We gratefully acknowledge the contribution of participants in this study and thank refugee settlement and counseling services in Australia for their assistance in study recruitment. We acknowledge the contribution of the Australian Red Cross and Settlement Services International to this study. We also acknowledge the contributions of Rosanna Pajak and Susan Li to study conception and data collection, Zachary Steel and David Berle to study conception, and Stephanie Murphy, Natalie Mastrogiovanni, Candy Liu, Amber Hamilton, Savannah Minihan, Joel Hoffman, Lillian Le, Shraddha Kashyap, Ola Ahmed, Jessica Cheung, Miriam Den, and Emma Doolan to data collection in this study. The data set generated and analyzed in the present study is available from the corresponding author on reasonable request. Analysis code has been provided in the Supplemental Material available online. Translated versions of the questionnaires used in the current study are available from the senior author on reasonable request.
Transparency
Action Editor: Kelsie T. Forbush
Editor: Jennifer L. Tackett
Author Contribution(s)
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.