
Abstract
Research suggests sex-related substance use can be conceptualized within the disinhibited externalizing spectrum of psychopathology. However, this research has generally excluded sexual-minority samples. In the current study, we examined the associations between the disinhibited externalizing spectrum and several sex-related substance use domains (i.e., heavy drinking and poppers [alkyl nitrite], cannabis, cocaine, and methamphetamine use) in a clinical sample (N = 254) of sexual-minority men. Disinhibited externalizing was significantly associated with reporting sex-related cannabis and methamphetamine use versus not and with frequency of sex-related alcohol and cocaine use. These results suggest few and generally weak associations—except for methamphetamine use—between the disinhibited externalizing spectrum and sex-related substance use. Implications for the applicability of dimensional models of psychopathology for sexual-minority populations, future directions for research on sexual behavior and substance use grounded in the specific sociocultural context in which sexual-minority men exist, and transdiagnostic interventions for sex-related substance use are discussed.
Keywords
Approximately 4.3 million American adults engage in sex-related alcohol use (Eaton et al., 2015). Similar nationally representative estimates of sex-related substance use among sexual-minority populations are nonexistent. However, several studies have documented high prevalence of substance use in the context of sex—sometimes termed “chemsex” (Bourne et al., 2014)—among sexual-minority men 1 (Bohn et al., 2020; Hegazi et al., 2017; Hibbert et al., 2019). Dimensional models of psychopathology—such as the Hierarchical Taxonomy of Psychopathology (HiTOP; Kotov et al., 2017)—are positioned to coalesce disparate findings about domain-specific forms of psychosocial dysfunction into a comprehensive metastructure (Conway et al., 2019) and are framed as particularly useful for understanding psychosocial health among sexual-minority populations (Eaton et al., 2021). Specifically, the disinhibited externalizing spectrum has been proposed as one way of conceptualizing underlying propensity for myriad forms of psychopathology 2 defined by low impulse control, disinhibition, and sensation seeking (Krueger et al., 2005, 2018). However, this empirical literature has excluded sexual-minority populations.
The goal of the current study is to examine how the disinhibited externalizing spectrum is associated with sex-related substance use among sexual-minority men. This is a unique sample and approach compared with prior research for the following reasons: (a) High-frequency sexual behavior is observed at high prevalence among sexual-minority men (Hibbert et al., 2019); (b) sexual behavior confers higher risk for negative health outcomes, including HIV transmission, among this population (Drückler et al., 2018; Pakianathan et al., 2018); and (c) substance use has previously been conceptualized within the externalizing spectrum among heterosexual populations (Rodriguez-Seijas et al., 2017).
Sex-Related Substance Use Among Sexual-Minority Men
Sex-related substance use has typically been studied by asking respondents about substance use either before or during sexual behavior; empirical evidence has documented high prevalence of sex-related substance use among sexual-minority men. For instance, among a large convenience sample (N = 1,649; 95% of the sample non-Hispanic White) of sexual-minority men in the UK, 41% reported engaging in past-year sex-related substance use (i.e., being under influence of or having taken substances just before or during sexual activity; Hibbert et al., 2019). Previous literature also suggests that sexual-minority men engage in sex-related substance use (i.e., reporting use of substances shortly before [Taggart et al., 2019] or during [Lawn et al., 2019] sex) at higher prevalence than heterosexual men. Data from the Global Drug Survey—an anonymous, Internet-based, self-selecting, cross-sectional survey of drug use behavior—documented disproportional engagement in sex-related substance use of 10.9% versus 1.3% for methamphetamine, 14.1% versus 10.1% for cocaine, and 19.4% versus 0.7% for alkyl nitrites (i.e., poppers) among gay respondents compared with heterosexual respondents, respectively (Lawn et al., 2019).
Sex-related substance use is associated with engagement in condomless anal sex and HIV/STI acquisition (Drückler et al., 2018; Pakianathan et al., 2018). Men who use methamphetamine often report using substances to increase sexual pleasure and doing so in settings in which they engage in sex with multiple sexual partners for several days at a time (Hammoud et al., 2020). Behaviorally, individuals using methamphetamine and other sex-related substances (e.g., GHB) are more likely to report a higher number of sexual partners and increased sexual risk, such as not using condoms (Colfax et al., 2004; Freeman et al., 2011; Halkitis et al., 2008; Koblin et al., 2003; Rawstorne et al., 2007), which suggests that there might be important intraindividual differences related to the type of substances used during sexual activity. It is estimated that 1 in 3 annual incident HIV seroconversions among sexual-minority men is associated with persistent methamphetamine use (Grov et al., 2020). And for men living with HIV, there is evidence that stimulants are associated with lower rates of viral suppression and faster HIV progression (Carrico et al., 2019; Miller et al., 2020). Therefore, the prevalence of sex-related substance use among sexual-minority men and its association with HIV acquisition makes it an important target for personal and public health.
Sex-Related Substance Use and the Disinhibited Externalizing Spectrum
Engagement in sexual behaviors that can lead to deleterious outcomes such as HIV/sexually transmitted infection (STI) acquisition and general substance use and personality domains such as sensation seeking, impulsivity, and disinhibition are interrelated (Allen & Walter, 2018; Hendershot et al., 2007; Hoyle et al., 2000; Krueger et al., 2005; Patrick et al., 2013; Rodriguez-Seijas et al., 2017). These personality traits further explain the associations between substance use and engagement in sexual behavior that can lead to HIV acquisition. For instance, associations with personality traits such as impulsivity, disinhibition, and sensation seeking explain relations between alcohol use and sexual behavior in both general (Justus et al., 2000) and sexual-minority (Kalichman et al., 1996) samples. The disinhibited externalizing spectrum accounts for comorbidity marked by impulsivity, sensation seeking, and disinhibition (Krueger et al., 2001, 2005; Rodriguez-Seijas et al., 2015). In theory, individuals higher on the latent disinhibited externalizing spectrum would exhibit more frequent—and potentially greater variety of—behavioral manifestations of this heightened propensity to disinhibition, sensation seeking, and impulsivity, including substance use and substance use in sexual contexts.
Sex-related substance use has been studied only once in relation to the externalizing spectrum. Greater sex-related alcohol and drug use (i.e., reporting greater frequency of alcohol and other drugs shortly before having sex) has been associated with higher externalizing levels (Rodriguez-Seijas et al., 2017). This association was stronger for sex-related drug use compared with alcohol use and showed important differences based on sex assigned at birth—women who reported regular sex-related alcohol use were higher on the externalizing factor than men who reported regular sex-related alcohol use. The externalizing factor shows differential associations with various substance use disorder diagnoses in the general population. For instance, alcohol dependence was associated with lower externalizing liability than cocaine dependence (Markon & Krueger, 2005). Finally, two previous studies documented higher externalizing levels among sexual-minority populations compared with heterosexual populations (Eaton, 2014; Rodriguez-Seijas, Eaton, & Pachankis, 2019). Sex-related substance use, therefore, may be another behavioral indicator of this underlying disinhibited externalizing liability that is particularly important to understand among sexual-minority men. It may even be the case that the type of substance used during sexual behavior may differentially reflect this propensity.
However, to date, several methodological limitations have impeded further understanding of associations between sex-related substance use and the disinhibited externalizing spectrum in general and among sexual-minority populations in particular. First, sex-related drug use, apart from alcohol, has not been examined as a behavioral indicator of the externalizing spectrum. Second, typical estimation of the externalizing factor relies on modeling the comorbidity of substance use disorder and antisocial personality disorder diagnoses as indicators (e.g., Markon & Krueger, 2005; Rodriguez-Seijas et al., 2017). It is unclear whether such estimation of the externalizing spectrum sufficiently indexes core processes of disinhibition rather than substance-use-specific variance. In addition, other evidence suggests that symptoms related to consequences of problematic substance use drive associations with the externalizing spectrum (Watts et al., 2022). Therefore, it would be particularly important to examine associations between sex-related substance use and the externalizing spectrum in a manner that minimizes the potential impact of both domains being confounded by common substance use variance. In that way, a better understanding of how the intraindividual propensity to disinhibited behavior is associated with sex-related substance use can be gleaned. Finally, there has been no research to explore associations between sex-related substance use and the disinhibited externalizing spectrum specifically among sexual-minority populations—for which sex-related substance use is more prevalent. For instance, results from one study documented higher prevalence of sex-related drug use among sexual-minority—particularly bisexual—individuals compared with heterosexuals (Taggart et al., 2019).
The extant literature on the interrelations among substance use, sexual behavior, and the disinhibited externalizing spectrum has developed without explicit attention to how these associations might manifest among subgroups of the population, such as sexual-minority men. In addition, previous evidence suggests there might be different associations between the disinhibited externalizing spectrum and specific forms of sex-related substance use in this population. Taken together, then (a) sexual-minority populations demonstrate higher mean externalizing levels, (b) previous research has documented elevated engagement in sex-related substance use among sexual-minority populations, (c) results from one study linked sex-related substance use to the externalizing spectrum among heterosexual individuals, and (d) transdiagnostic models such as the externalizing spectrum have been framed as particularly helpful for understanding psychosocial dysfunction among sexual-minority populations (Eaton et al., 2021). Despite these theoretical associations, no empirical studies of associations between the disinhibited externalizing spectrum and sex-related substance use outcomes among sexual-minority populations have been undertaken to date.
The Current Study
The goal of the current study, therefore, was to examine the associations between the disinhibited externalizing spectrum and sex-related substance use. To do so, we used data from a clinical research sample of young sexual-minority men. We examined how one measure of disinhibited externalizing, free of substance use variance, was associated with reports of engaging in sexual behavior while under the influence of alcohol, cannabis, poppers (alkyl nitrite), cocaine, and methamphetamine. We hypothesized that higher disinhibited externalizing would be cross-sectionally associated with greater frequency of engagement in sex-related substance use over the past 90 days. In addition, we also hypothesized that associations between sex-related substance use and the disinhibited externalizing spectrum would differ as a function of substance use domain.
For instance, we would expect to find low/no associations between use of poppers (alkyl nitrite) and the disinhibited externalizing spectrum given the relative high frequency and low risk profile of poppers use, compared with other substances, among sexual-minority men (Demant & Oviedo-Trespalacios, 2019). On the other hand, differential associations between the externalizing spectrum and other substance use domains in the general population (e.g., alcohol vs. cocaine; Markon & Krueger, 2005) suggest that the specific substance use domain itself might show distinct associations with the disinhibited externalizing spectrum. Furthermore, some specific substances are associated with particular detriment among sexual-minority men (e.g., methamphetamine; Hammoud et al., 2020), which might be reflective of higher associations between specific drug classes and the disinhibited externalizing spectrum. Therefore, we hypothesized that we would observe stronger associations between disinhibited externalizing and sex-related methamphetamine use compared with sex-related poppers use, for instance.
Transparency and Openness
All code for analyses conducted for this article are available at https://osf.io/ktrfz/?view_only=cdb3640f0ef044428fb0572e65236aa2. The study was approved by the Yale University and University of Miami Human Subjects Committees.
Method
Participants
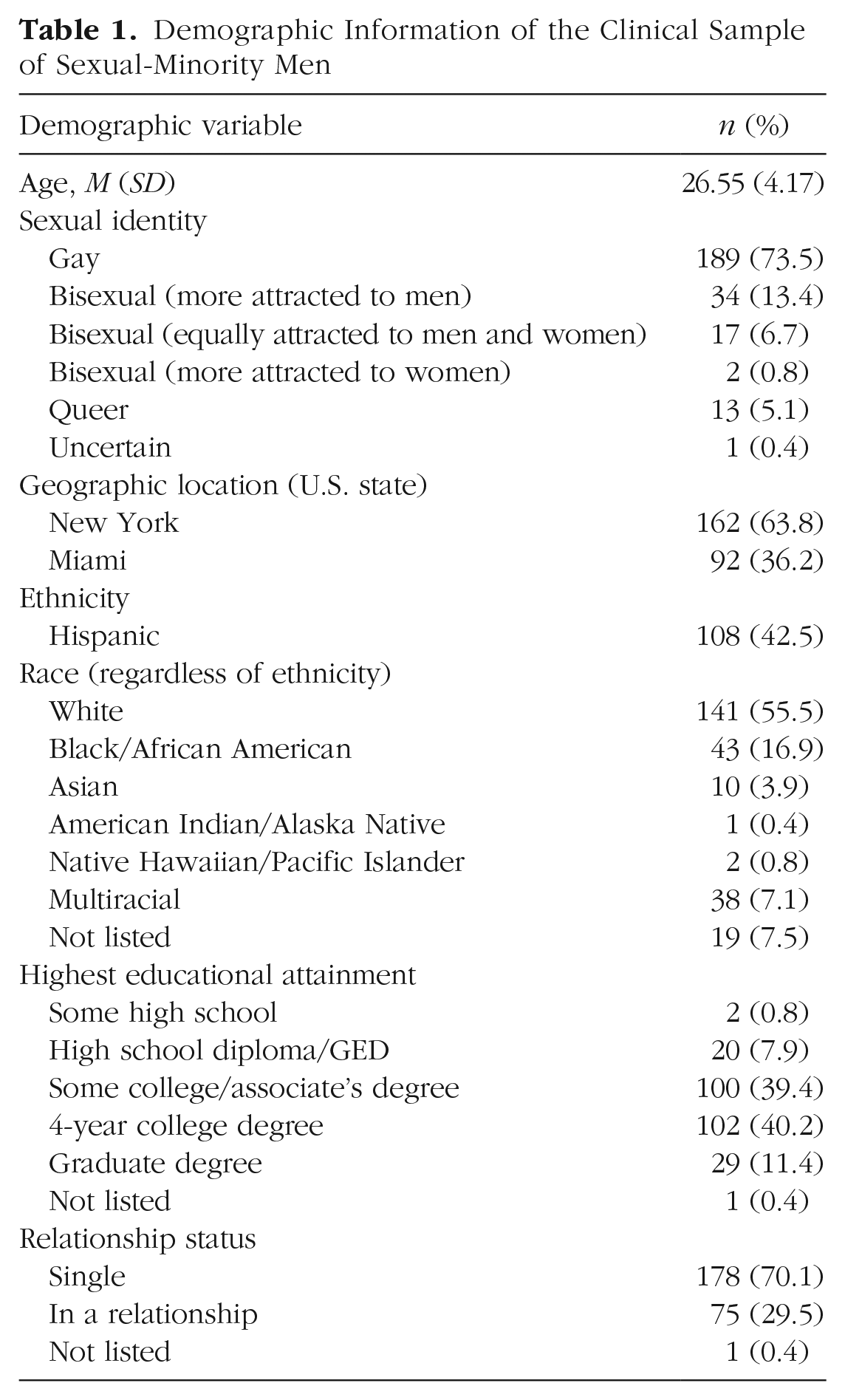
We used data from baseline assessments of young gay and bisexual men (N = 254) who were recruited as part of a treatment efficacy study (Pachankis et al., 2019). Participants were young gay and bisexual men between the ages of 18 and 35 who lived in New York City or Miami. Inclusion criteria for this study were (a) diagnosis of a current mood, disorder, and/or anxiety or trauma- or stress-related disorder; (b) HIV-negative serostatus; (c) not currently adherent to preexposure prophylaxis; (d) having engaged in condomless anal sex with someone living with HIV or unknown HIV serostatus in the past 90 days, unless the sex act was with an HIV+ main partner with known undetectable viral load; and (e) English-language proficiency. Demographic information about the sample is presented in Table 1. Note that although one of the study criteria was the presence of a mood/anxiety disorder, comorbid substance use disorder diagnoses were common among this sample. More than half (59.8%, n = 152) of participants met criteria for the diagnosis of at least one substance use disorder.
Demographic Information of the Clinical Sample of Sexual-Minority Men
Measures
Sex-related substance use
At their baseline assessment, participants completed a 90-day timeline follow-back indicating days in which they engaged in any sexual activity and/or used any substances. In the current study, we operationalized sex-related substance use as the number of times participants reported engaging in sexual activities while under the influence of substances in the past 90 days. Specifically, we investigated the following domains of sex-related substance use: (a) heavy drinking (defined as five or more standard alcoholic drinks), (b) cannabis use, (c) poppers (alkyl nitrite) use, (d) cocaine use, and (e) methamphetamine use. Low endorsement of other sex-related substance use domains (e.g., heroin, ketamine) precluded our examination of associations between use of these drugs and the disinhibited externalizing spectrum. We used count data of drug use days in each of these domains (i.e., the number of times an individual engaged in sex-related drug use for that substance domain over the 90-day period).
The externalizing spectrum
Externalizing was assessed using the general disinhibition scale (ESIDIS) of the Externalizing Spectrum Inventory-Brief Form (Patrick et al., 2013), which is a shorter version of the longer Externalizing Spectrum Inventory (ESI; Krueger et al., 2007). The ESIDIS consists of 20 items—two of which are reverse-scored—rated on a 4-point Likert-type scale (false, somewhat false, somewhat true, true). Sample items include “I have a hard time waiting patiently for things I want” and “I often get bored quickly and lose interest.” Scores are summed; higher scores indicate higher levels of externalizing. The ESIDIS items were intentionally created to exclude variance related to substance use, mental-disorder diagnoses, and aggression to avoid confounding (Patrick et al., 2013).
Analytic strategy
Analyses were conducted in MPlus (Version 8.6; Muthén & Muthén, 2017). First, we estimated a single-factor model from the ESIDIS items, treating items as ordered categorical with a weighted least squares estimator to facilitate conventionally described measurement model fit indices. Second, using a structural equation modeling framework, we regressed individual sex-related substance use items on the disinhibited externalizing factor to determine the extent to which externalizing was associated with sex-related substance use. We used a zero-inflated Poisson regression to accommodate the count nature of the sex-related substance use variables and the high preponderance of zeros in these data (i.e., the relative rarity of reporting sex-related substance use among this sample). The zero-inflated Poisson model permits separate parameterization of logistic regression and Poisson regression models simultaneously. Logistic regression models allow for exploration of associations between the externalizing spectrum and engagement in sex-related substance use of each specific domain. The Poisson regression models allow for exploration of associations between the externalizing spectrum and the frequency (i.e., count nature) of reported sex-related substance use. Results from the logistic regression portion represent the prediction of membership in the zero-generating process (i.e., not engaging in sex-related substance use) using the externalizing spectrum as the predictor. We present the inverse of these odds ratios (ORs) for ease of interpretation (i.e., ORs of engaging in sex-related substance use). We used a maximum likelihood estimator with robust standard errors for zero-inflated Poisson models.
Results
Clinical sample
ESIDIS measurement model
The single-factor ESIDIS provided acceptable fit to these data (comparative fit index [CFI] = .91, Tucker-Lewis index [TLI] = .90, root mean square error of approximation [RMSEA] = .08). Factor loadings are presented in Table 2.
Factor Loadings for ESIDIS Items From Single-Factor Model
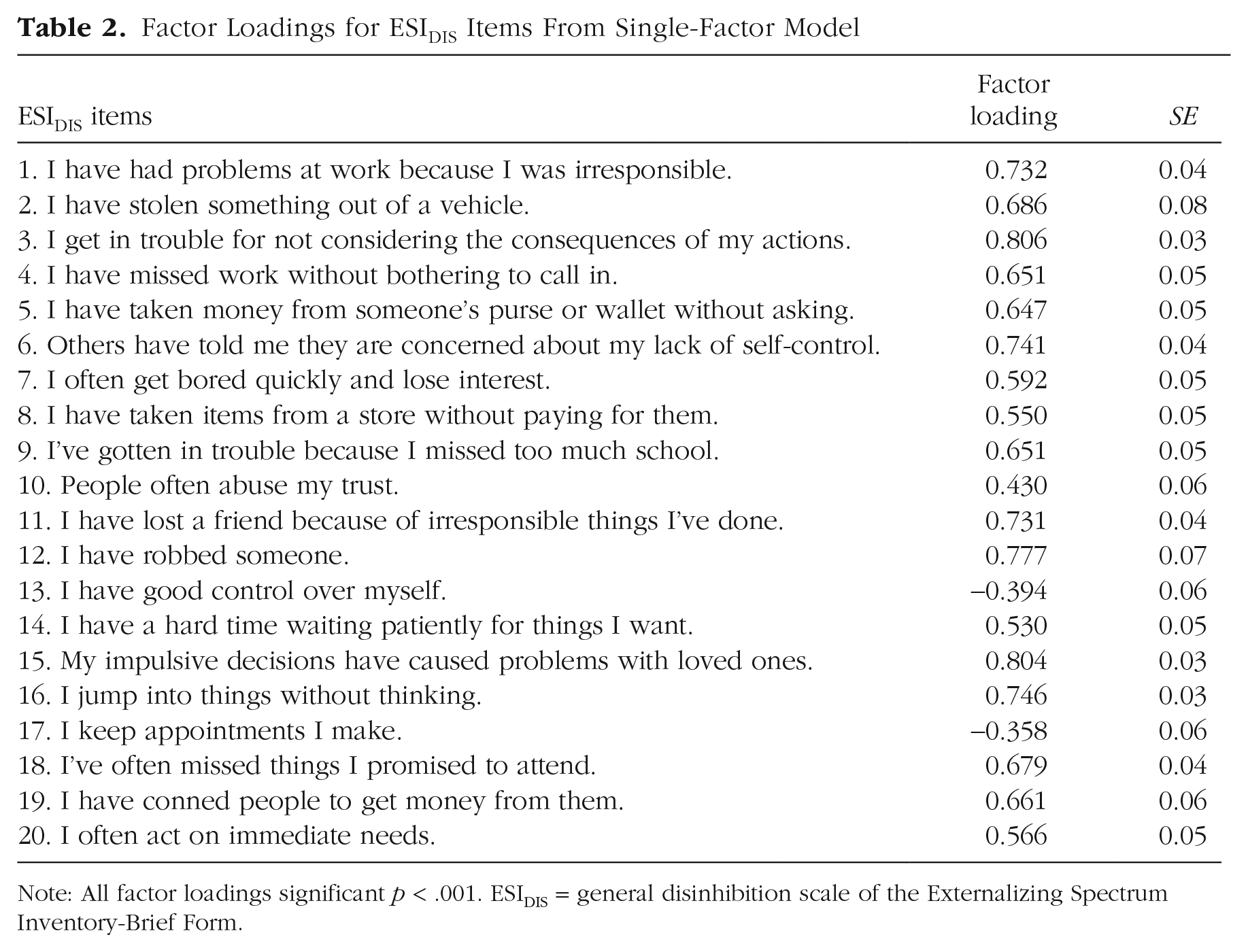
Note: All factor loadings significant p < .001. ESIDIS = general disinhibition scale of the Externalizing Spectrum Inventory-Brief Form.
Associations between ESIDIS and sex-related substance use
Results from zero-inflated Poisson models are presented in Table 3.
Associations Between ESIDIS and Sex-Related Substance Use Domains
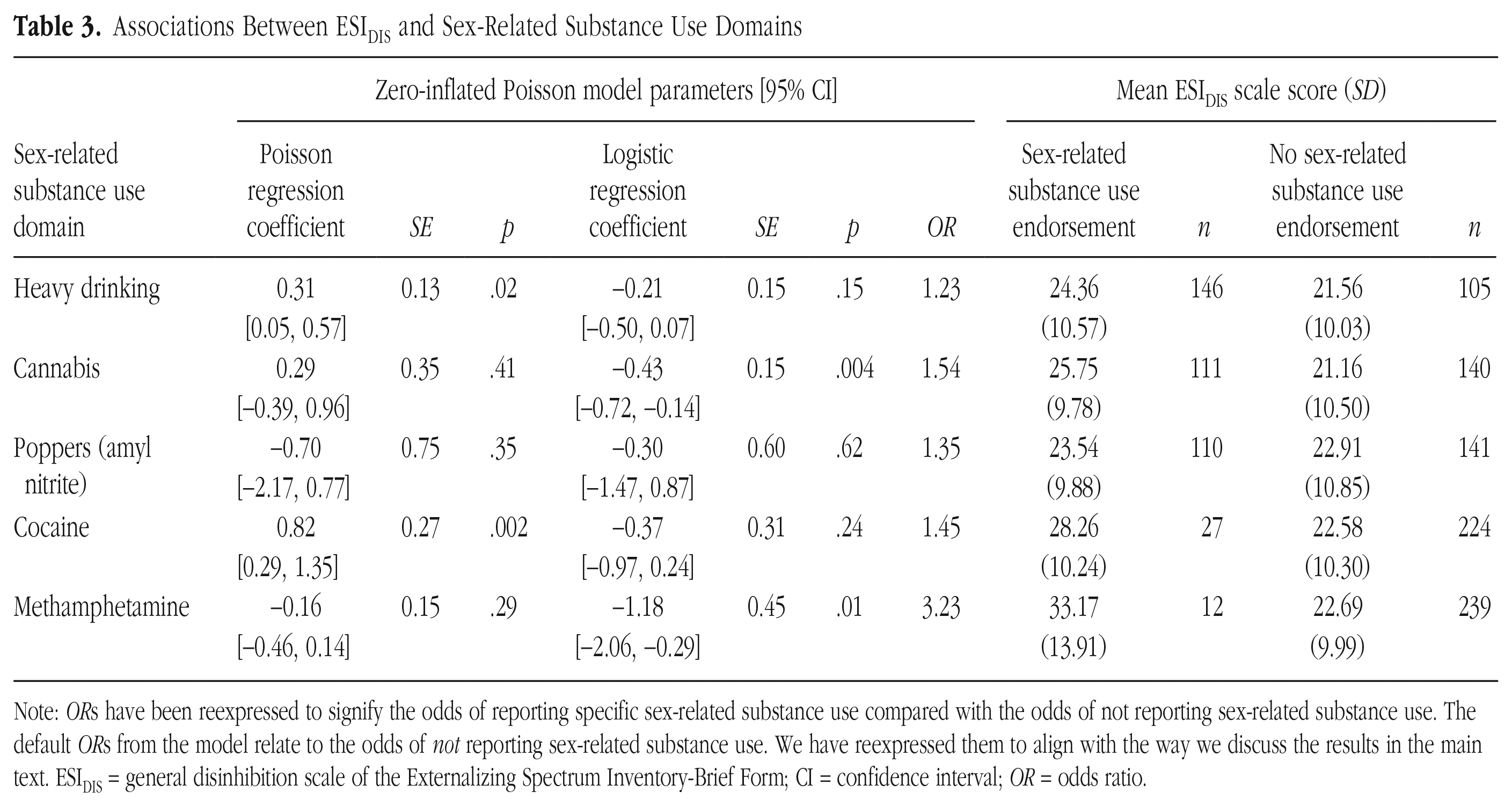
Note: ORs have been reexpressed to signify the odds of reporting specific sex-related substance use compared with the odds of not reporting sex-related substance use. The default ORs from the model relate to the odds of not reporting sex-related substance use. We have reexpressed them to align with the way we discuss the results in the main text. ESIDIS = general disinhibition scale of the Externalizing Spectrum Inventory-Brief Form; CI = confidence interval; OR = odds ratio.
Logistic model results
The ESIDIS factor was significantly associated with odds of reporting sex-related cannabis and methamphetamine use. That is, higher ESIDIS factor levels were associated with greater odds of reporting sex-related cannabis (OR = 1.54, p < .01) and methamphetamine use (OR = 3.23, p < .01). In other words, each unit increase in the disinhibited externalizing spectrum was associated with an increased odds of reporting sex-related cannabis and methamphetamine use of 1.54 and 3.23, respectively. ESIDIS scale score differences for individuals who did versus did not report sex-related substance use in any specific substance domain are presented in Table 3 and illustrated in Figure 1. The amount of variance explained by the externalizing spectrum in whether participants engaged in sex-related substance use for the various domains were as follows: heavy drinking: R2 = 1.3%; cannabis: R2 = 5.3%; poppers: R2 = 2.6%; cocaine: R2 = 3.9%; methamphetamine R2 = 29.6%.
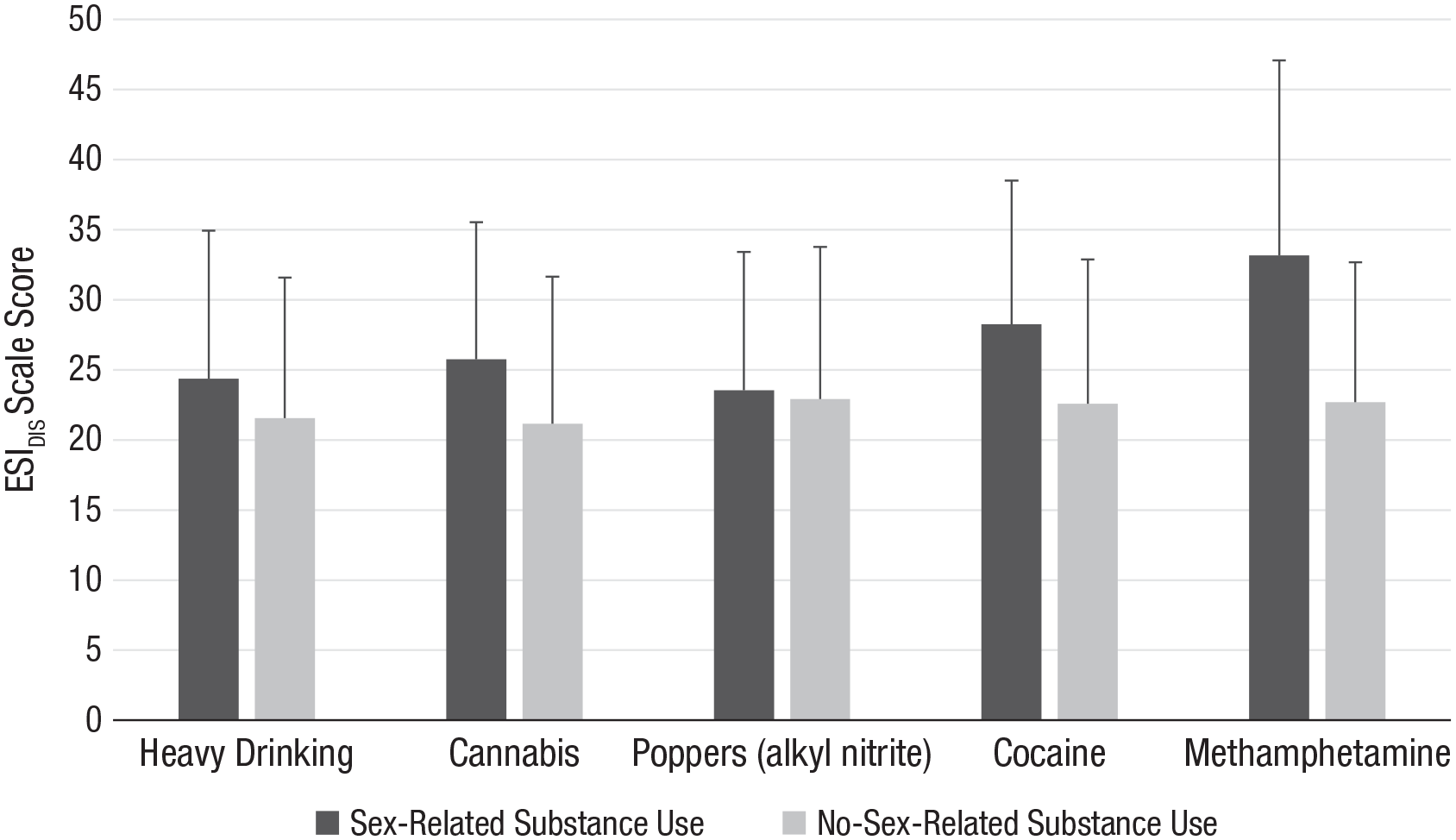
Mean scores for the general disinhibition scale of the Externalizing Spectrum Inventory-Brief Form among individuals who reported versus individuals who did not report sex-related substance use across various substance use domains.
Poisson-model results
The ESIDIS factor was significantly and positively associated with reported frequency of sex-related heavy drinking (b = 0.31, p < .05) and sex-related cocaine use (b = 0.82, p < .01). That is, each unit increase in the disinhibited externalizing spectrum level was associated with increased frequency of engaging in sex under the influence of heavy drinking and cocaine use of 1.36 and 2.27 times, respectively. The ESIDIS factor showed no significant associations with the frequency of reporting cannabis, poppers (alkyl nitrite), and methamphetamine use in this sample.
Discussion
We examined the extent to which the disinhibited externalizing spectrum was associated with different sex-related substance use domains among a clinical sample of young sexual-minority men. The disinhibited externalizing spectrum was associated with dichotomous sex-related cannabis and methamphetamine use but unrelated to the frequency with which individuals engaged in these behaviors. The disinhibited externalizing spectrum was, however, positively associated with greater frequency of sex-related alcohol and cocaine use but not dichotomous indicators of these behaviors. The relatively few associations between the disinhibited externalizing spectrum and various domains of sex-related substance use differed from our expectations based on the substance use literature in general, the sex-related substance use literature specifically, and the literature on the externalizing spectrum. Even when significant, there were very weak associations between the disinhibited externalizing spectrum and all sex-related substance use domains, with the exception of methamphetamine use. However, given the relatively small number of individuals who reported sex-related methamphetamine use, this result must be interpreted cautiously.
Sociocultural context, sex-related substance use, and the disinhibited externalizing spectrum
There were few and generally weak associations between various domains of sex-related substance use and the disinhibited externalizing spectrum for all substances except methamphetamine in our sample. Individuals who engaged in sex-related methamphetamine use reported higher externalizing levels than individuals who did not (see Fig. 1). However, among those users, individual differences in disinhibited externalizing levels were not associated with different frequencies of sex-related methamphetamine use. Although a minority of participants reported methamphetamine use in this study, methamphetamine use consistently emerges as a predictor of sexual behavior associated with detrimental outcomes among sexual-minority men across numerous studies. Nearly 2 decades of research have demonstrated the association between crystal methamphetamine use and HIV-transmission-risk behaviors, including condomless anal sex (Carrico et al., 2019; Grov et al., 2020; Hammoud et al., 2020; Mansergh et al., 2006; Miller et al., 2020). In addition, some research has linked the externalizing spectrum with HIV/STI acquisition among the general population (Latack et al., 2015). Our findings add to this literature, suggesting that intraindividual differences in disinhibited-externalizing-related pathology (i.e., sensation seeking, disinhibition, and impulsivity) predicts methamphetamine use versus not (i.e., the odds of reporting sex-related methamphetamine use). However, these results also show no associations between the disinhibited externalizing spectrum and how frequently one reports sex-related methamphetamine use.
Apart from sex-related methamphetamine use, when we observed significant associations between sex-related substance use and the disinhibited externalizing spectrum, the relatively small R2 values suggest that the majority of variance in sex-related substance use is largely independent of the disinhibited externalizing domain. These findings differed from our initial hypotheses. Further interpretation of these results requires several considerations, highlighting avenues for future inquiry. It is possible that higher prevalence of substance use among sexual-minority men might also partially explain the dearth of associations between sex-related substance use and the externalizing spectrum. At a structural level, bars and clubs—venues in which alcohol and drug use is relatively normative—are traditional “safe spaces” for sexual-minority men (Carpiano et al., 2011; Cochran et al., 2012; Grov, 2012). The result is an environment for increased substance use in social and sexual settings (Garcia et al., 2015). This comparatively normative nature of substance use among sexual-minority men might attenuate associations with the disinhibited externalizing spectrum—a domain characterized by psychopathology and maladaptive personality variables. In other words, because substance use may be more common among sexual-minority men, associations with individual differences in psychopathology dimensions may thus be weak, as found here.
Many of the measurements and criteria for diagnosis of problematic substance use have been normed on general-population (i.e., heterosexual rather than sexual minority) samples. Additional measurement studies are needed to identify appropriate reference values in sexual-minority men because there is evidence to suggest that subgroup-specific diagnostic rules for substance use disorder may be more optimal than “one-size-fits-all” approaches (Boness et al., 2020). Perhaps, for sexual-minority men, too, it is worth reviewing existing criteria for disorders and empirically evaluating the clinical utility of these measures for this specific population. In the context of the current study, it might be the case that merely engaging in nonmethamphetamine sex-related substance use among sexual-minority men is less indicative of dimensions of psychopathology than it is of group-specific behavioral norms. Future research can build on these results by incorporating measures of clinical impairment and distress beyond assessments of substance and sexual behaviors and the frequency of these behaviors. Such research would allow the field to separately assess dysfunction from behavior that can be attributed to population-specific contextual norms. Indeed, other research has shown that when impairment/distress is ignored, sexual-minority populations are more likely to meet diagnostic criteria for other forms of psychopathology—such as borderline personality disorder—but when impairment/distress is explicitly accounted for, criterion endorsement is reduced. This suggests that differences in certain behaviors and experiences considered maladaptive must be interpreted in light of their social context, which in this case means considering sex-related substance use in a population of sexual-minority men (Rodriguez-Seijas et al., 2021).
Transdiagnostic-psychopathology-research implications
Apart from normativity of sex-related substance use, it is also possible that sex-related substance use among sexual-minority men reflects broad dimensions of psychopathology apart from the disinhibited externalizing spectrum. Through a minority-stress lens, the sociocultural environment in which sexual-minority men exist might predispose them to use substances to manage emotional experiences both in general and in the context of sex (Burton et al., 2020; Halkitis et al., 2014; Pachankis et al., 2015). Indeed, some literature has demonstrated that among a majority (61%) sexual-minority male sample, there was no association between sex-related alcohol use and sensation seeking—one personality variable associated with the disinhibited externalizing spectrum—after accounting for the instrumental nature (i.e., to reduce anxiety) of sex-related alcohol use (Kalichman et al., 2002).
Sex-related alcohol and drug use among some sexual-minority men might be more a function of concerns about their sexual performance and managing the impression of their performance by their sexual partner (i.e., regulation of associated negative emotions) rather than an indicator of low impulse control. This hypothesis that sex-related substance use might be related to minority stress, internalized stigma or shame, or concerns about sexual performance among sexual-minority men resembles conceptualization of the negative urgency construct, defined as a tendency to commit rash or regrettable actions as a result of intense negative affect (Whiteside & Lynam, 2001). Empirical evidence demonstrates equivalent associations between negative urgency and both internalizing and externalizing spectra (Joyner et al., 2021). There is, therefore, a need for future research examining the extent to which behaviors such as sex-related substance use—or other indicators of broad transdiagnostic dimensions—are differentially related to various transdiagnostic factors among sexual-minority groups compared with heterosexual groups.
Therefore, these findings hold particular importance for transdiagnostic models of psychopathology such as the HiTOP (see Kotov et al., 2017, 2021), which seeks “to articulate a fully empirical classification of psychopathology” (Kotov et al., 2017, p. 85; Kotov et al., 2021). Despite this goal of articulating an entirely empirical system, the empirical evidence that has undergirded the HiTOP model to date overwhelmingly reflects heterosexual populations. Research specific to sexual-minority populations has applied parts of the HiTOP model in efforts to understand whether it is similar in sexual-minority populations. For instance, studies typically examine measurement invariance or compare group levels of HiTOP spectra (Eaton, 2014; Rodriguez-Seijas, Eaton, & Pachankis, 2019), finding higher levels of spectra such as externalizing among sexual-minority samples. Studies have also examined associations between minority stressors such as sexual-orientation-based discrimination (Eaton, 2014; Rodriguez-Seijas, Eaton, & Pachankis, 2019) and rejection sensitivity (Cohen et al., 2016). Similar to these studies, we also applied the disinhibited externalizing spectrum to sexual-minority populations. However, these results highlight the importance of adopting a more emic approach to articulating psychopathology, in which contextualized research is incorporated in the modeling, testing, and potential expansion of the (HiTOP) model.
The HiTOP model remains atheoretical regarding etiology of psychosocial dysfunction (DeYoung et al., 2021). However, assumptions of generalizability and universality of the model might be somewhat overstated. Indeed, that little research on the HiTOP model—from which the disinhibited externalizing spectrum is derived—has included sexual-minority participants or appreciated the sociocultural context in which sexual-minority participants exist makes it unclear whether the model is indeed applicable in the same way for sexual-minority populations as it might be for heterosexual populations. Recent scholarship has outlined how the conceptualization of personality pathology, to which the HiTOP domains bear striking resemblance (Markon, 2010; Wright et al., 2012), is misaligned with evidence-based ways of understanding the psychosocial needs of sexual- and gender-minority populations (Rodriguez-Seijas et al., 2022).
Taken together, then, these findings highlight the importance of understanding the sociocultural context and how it affects seemingly objective indicators of psychopathology. A future direction for the HiTOP consortium’s efforts at identifying generalizable transdiagnostic factors of psychopathology should be the incorporation of context in a more explicit manner in the HiTOP model. Given the relative infancy of the HiTOP consortium, incorporating contextual influences might be feasible and represents a particular advantage over other nosologies of psychopathology that overwhelmingly assume basic mechanistic attributions for psychopathology rather than being nuanced by social and structural contexts. This becomes even more important as the HiTOP consortium develops a self-report assessment tool (Simms et al., 2021). Without examination of how the measure performs among sexual and other minoritized populations, it will be unclear how such a measure may capture and parse psychopathology from potentially population-specific normative behavior.
This research then calls for (a) better understanding of the factors that affect for whom transdiagnostic models of psychopathology can be most useful and (b) explicit testing of these models among populations that are epistemically excluded from mainstream clinical psychology research; (c) testing of models should be conducted in a theory-driven manner rather than a decontextualized manner so that researchers can make meaningful interpretations of the data and translate findings related to nosology directly to clinical assessment and diagnosis.
Transdiagnostic-intervention implications
Although previous studies of the associations between sex-related substance use and the externalizing spectrum have suggested utility in the use of transdiagnostic interventions targeting the externalizing spectrum (e.g., Rodriguez-Seijas et al., 2017), the results from this study suggest caution in making such an assertion when it comes to interventions for sexual-minority men. An underlying assumption of this assertion is that behaviors that correspond with the disinhibited externalizing spectrum necessitate intervention efforts distinct from those associated with other psychopathology dimensions (e.g., the internalizing domain). For instance, for problems related to disinhibited externalizing, interventions focused on motivational techniques, mindfulness practice, and those fostering increased conscientiousness would be useful; exposure and response-prevention techniques would be recommended for problems related to the internalizing domain (Hopwood et al., 2020). Given our results, the former might be useful for individuals presenting with sex-related methamphetamine use. However, we cannot necessarily say the same for other sex-related substance use domains given these findings at this time.
The HiTOP model is increasingly positioned as useful for streamlining clinical assessment, conceptualization, and intervention (Conway et al., 2019; Ruggero et al., 2019). The assertions about its utility for streamlining intervention (e.g., Hopwood et al., 2020; Mullins-Sweatt et al., 2020; Ruggero et al., 2019) certainly help alleviate the separate problem/separate treatment path of psychosocial-intervention research. These transdiagnostic models have been positioned as particularly useful for sexual- and gender-minority populations, too (Eaton et al., 2021). However, our results highlight one gap in this literature domain. Specific behavioral signs and symptoms of psychopathology may not correspond with the same higher-order factors, subfactors, and/or spectra (see Kotov et al., 2017, Figure 2) across different, and particularly minoritized, populations (e.g., sexual-minority vs. heterosexual men in this case). Incorporating such nuance into dimensional psychopathology conceptualizations is particularly important to ensuring that such models, and their resultant intervention implications, are appropriate for epistemically excluded (Settles et al., 2020) populations such as sexual-minority men.
For example, sexual-minority men’s disproportionate risk of psychosocial problems is conceptualized as rooted in their distinct minority-stress experiences (e.g., Hatzenbuehler, 2009; Meyer, 1995). Lack of relevant sexual-health information (Kubicek et al., 2010), internalization of negative societal messages about same-sex sexual behavior (Herek, 2004; Jennings et al., 2022), and intraminority stress related to sexual behavior (Burton et al., 2020; Pachankis et al., 2020) leave sexual-minority men affected by sexual-health difficulties, including sex-related substance use. In one affirming intervention protocol for sexual-minority men (Pachankis et al., 2019, 2021), sexual behavior—such as sex-related substance use—is intervened on by first understanding minority-stress associations with the behavior (e.g., use of substances during sex to reduce anxiety associated with learned potential rejection) and subsequently engaging in behavioral experiments designed to reduce sex-related substance use as an emotion-driven behavior (e.g., having sex without using substances; Burton et al., 2019; Rodriguez-Seijas, Burton, & Pachankis, 2019). We mention these findings to illustrate how in the sexual-minority literature, sex-related substance use behavior and interventions to address it in therapy can perhaps be understood and treated in a manner more congruent with intervention foci for internalizing psychopathology. This represents a divergence from the conceptualization of sex-related substance use in the disinhibited externalizing domain, as indicated in the extant dimensional-psychopathology literature.
Therefore, we highlight the importance of a thorough understanding of the sociocultural context in which an individual exists when using transdiagnostic models—such as the disinhibited externalizing spectrum—for intervention purposes. Without doing so, clinicians might misattribute potentially normative and largely unproblematic behaviors (e.g., the use of poppers in sexual contexts among sexual-minority men) to intraindividual psychopathology processes (e.g., a propensity to act in impulsive, disinhibited manners).
Limitations
The study designs used here are cross-sectional, precluding conclusions about temporal and causal associations. Future research can benefit from investigating the predictive associations between the externalizing spectrum, other dimensional models of psychopathology, and sex-related substance use variables. Although we operationalize our populations of interest in terms of sexual identity, we do not mean to imply that gay or bisexual identity per se is associated with sex-related substance use. Instead, as discussed above, perhaps the specific sociocultural context in which sexual-minority men find themselves is responsible for the associations or general lack thereof found here. Sexual-orientation identity is used in this study as a proxy for myriad psychosocial processes, such as minority-stress experiences, that shape sexual-minority men’s psychosocial health. Future research is needed to extend the present findings to formally incorporate minority-stress processes in these models rather than using identity as proxy of such. We focused solely on reports of sex-related drug use behavior. Inclusion of other measures of distress/impairment and engagement in specific health-risk behaviors (e.g., HIV-transmission risk behavior) may better help delineate the nature of associations between sexual behavior, substance use, and the externalizing spectrum. Finally, we were not able to specify individuals’ reasons for engaging in sex-related substance use in either sample. It is possible that sex-related substance use might be a function of seeking substances to enhance arousal or performance or reduce anxiety around engagement in sexual activity. Conversely, it might also be a function of engagement in sexual behavior because of the disinhibition garnered from engaging in substance use. Future research would be tasked with exploring how motives for substance use in sexual contexts affects these findings.
Conclusion
In summary, our findings suggest few associations between sex-related substance use domains—with the exception of sex-related methamphetamine use—and the disinhibited externalizing spectrum among sexual-minority men. Because much of the research that has examined dimensional models of psychopathology used general-population samples (i.e., overwhelmingly heterosexual), it is unclear at this time how common psychosocial challenges among underrepresented groups, including sexual-minority men, might be accommodated in these structures. Future research that incorporates the impact of sociocultural context, particularly among groups underrepresented in the dimensional-psychopathology field, is needed to understand nuances of transdiagnostic models of psychopathology. In addition, intervention recommendations drawn from general-population psychopathology research might not apply to minoritized and underrepresented groups, including sexual-minority men.
Footnotes
Transparency
Action Editor: Steve S. Lee
Editor: Jennifer L. Tackett
Author Contributions