
Abstract
In a recent call to action, we described pressing issues in the health-service-psychology (HSP) internship from the perspective of interns. In our article, we sought to initiate a dialogue that would include trainees and bring about concrete changes. The commentaries on our article are a testament to the readiness of the field to engage in such a dialogue, and we applaud the actionable recommendations that they make. In our response to these commentaries, we seek to move the conversation further forward. We observe two themes that cut across these responses: the impetus to gather novel data on training (the “need to know”) and the importance of taking action (the “need to act”). We emphasize that in new efforts to gather data and take policy-level action, the inclusion of trainee stakeholders (as well as others involved in and affected by HSP training) is a crucial ingredient for sustainable and equitable change.
Keywords
In 2022, Clinical Psychological Science published our article, “Systemic Challenges in Internship Training for Health-Service Psychology: A Call to Action From Trainee Stakeholders” (Palitsky et al., 2022). As a group of 23 interns, we sought to add previously absent trainee perspectives to the ongoing, field-wide discussions about the future of the health-service-psychology (HSP) internship. The central argument of our article was that trainee stakeholders needed to be included in decision-making about the HSP internship to identify and address systemic problems in HSP training. We made 24 recommendations on the basis of the challenges that we observed and suggested a set of “questions for collaborative inquiry” that training programs might use, together with trainees, to navigate their responses to these challenges. The publication and reception of our article and the four thoughtful commentaries published in response are clear indicators of the readiness to include trainees in conversations about the future of training in the field.
Each of the four commentaries (Atkins & Mehta, 2024; Galán et al., 2024; Gee & Shackman, 2024; Knowles et al., 2024) addressed the interconnected and multifaceted challenges in HSP training, providing valuable insights and actionable strategies for change. Although we cannot respond to each point raised in the commentaries here, we focus on two overarching themes relevant to the larger discussions on HSP training that we consistently observed in the commentaries. We label the first theme the “need to know,” which reflects the many calls for additional data on HSP training to produce evidence-informed changes in the field. Then, we address the second theme—the “need to act”—which reflects the mounting, field-wide impetus to begin materially addressing the challenges in the field. Across both themes, trainee inclusion remains critical for ensuring that the next actions we take as a field support equitable and sustainable HSP training.
Given that the original authors are no longer interns (importantly, some of us are new clinical training faculty), we are joined by two current interns who have added important perspectives on current experiences of internship. Nevertheless, as Galán et al. (2024) noted, it is important to bear in mind the broader communities and still-unrepresented individuals affected by HSP and to strive to include them in ongoing work.
Need to Know: Calls for More and Better Data in HSP Training
Resistance [to making changes in HSP training] may be related to specific assumptions or beliefs about what constitutes “good clinical training” and optimal methods for learning. However, many of these beliefs may actually represent speculation from more privileged individuals who are drawing from their own prior experiences and what worked for them in the past. (Galán et al., 2024, p. 181)
Several commentaries urged for quality data in the field of HSP training, and we strongly support these calls. Our original article’s discussion of data collection was primarily restricted to recommending (a) feedback solicitation from trainees and (b) a forum for trainees to hold internships accountable through publicly available ratings (Recommendations 20 and 24; Palitsky et al., 2022). The commentaries made meaningful additions over and above our initial recommendations. HSP is an evidence-based discipline; accordingly, data should inform the design and implementation of HSP training. Galán et al. (2024) noted that embedded practices in HSP internship are often based on assumptions about training in the absence of data. Such tacit and unfounded beliefs (e.g., that difficult training means rigorous training) can be offset by “new data streams for recursive refinement” (Gee & Shackman, 2024, p. 176) in clinical training.
Gee and Shackman’s (2024) commentary provides a well-rounded account of ways to enhance the data-collection streams in HSP training. They highlighted the importance of trainee anonymity, of collecting (and acting on) data at local and national levels, and of including trainees in the development of feedback mechanisms. Furthermore, they pointed to the importance of longitudinal data collection, a recommendation also made by Galán et al. (2024), which can help to answer quality and equity questions (e.g., In what ways are characteristics such as gender, race, number of dependents, or financial savings during internship linked with the career trajectories of trainees?). Galán et al. also emphasized that patients and other consumers of HSP must figure prominently in the research that informs training recommendations, a suggestion with which we concur. For instance, they expanded on our recommendations for improving telehealth (and telehealth access) in training: “Better understanding how telehealth can be adapted to meet the specific needs of historically marginalized populations is critical before we can draw definitive conclusions about the circumstances under which trainees should be allowed to provide telehealth services” (Galán et al., 2024, p. 182). These recommendations provide excellent starting points for collecting information about HSP training that equitably reflects the needs and experiences of all major stakeholders in training: training programs, trainees, and the individuals whom health-service training systems aspire to serve.
Balancing Knowledge With Action
Given the emergent emphasis on collecting new data about clinical training, we highlight two priorities that we hope will be considered in discussions about the need for more data. First, it is crucial to ensure that newly collected data are actually representative of trainees with diverse experiences. Disparities in data often reflect societal gradients in privilege (Diebold, 2022), potentially skewing representation toward better-resourced programs and trainees (e.g., Which institutions are designing the studies on HSP training?). “Certain data are also difficult to obtain or interpret accurately, whether because of the positionality and power dynamics inherent to research with trainees, or because of imprecise fits between units of analysis and the problems we are attempting to solve” (p. 3). Lived experiences, such as ones we described (Palitsky et al., 2022), can nevertheless signal the existence of urgent issues. In one example from our article, also noted by Atkins and Mehta (2024), an intern coauthor had to take multiple jobs during internship to support their family, a situation that is disturbing but not shocking in light of already available information about internship salaries. The question remains, however: Whose lived experiences inform the narratives of clinical training?
Therefore, the second priority is that the improved collection of data should be part of a broader response that includes prompt and attentive alleviation of known problems rather than deferring action on the basis of needing more data. Although a new study about the prevalence of intern moonlighting may be illuminating, it would be misguided to wait for such a study before increasing interns’ salaries. The field knows this problem is occurring (without formal data collection), and it should act now. 1 When collection of novel empirical data is not practical or expedient, we also suggest that turning to established theoretical frameworks may help guide effective action locally and field-wide. For example, in our call to action (Palitsky et al., 2022), we applied the exchange-boundary framework (Watson & Foster-Fishman, 2013) 2 to understand the barriers and possible solutions to collaborative decision-making in HSP training. Interdisciplinary analyses grounded in feminist theory (Sharma, 2019), anti-racism (Diffey & Mignone, 2017), and decolonial theory (Cullen et al., 2020), which have been developed through decades of rigorous research on difficult-to-address problems, can be vital frameworks for action. Critically, nonaction in and of itself constitutes a response. The rationale for such a response is not based on data but, rather, on entrenched structures that constitute the training environment. When invited to the table, trainees have voiced that waiting for action is untenable.
Need to Act: The Time for Change Is Now
The field is in a moment of unique opportunity to consider changes—large and small—to the HSP internship. If interns are included as stakeholders in these efforts, the primary aim of our article (Palitsky et al., 2022) will have been achieved. The commentaries also provide many important proposals for concrete change, which we examine in this section.
One eminently actionable step is to make feedback count more for training programs. As we mentioned in our article and as emphasized by Gee and Shackman (2024), publicly visible feedback that is recognized by training institutions (and perhaps even included in their directory listings) can provide a powerful incentive for training sites and a direct way to include interns in power-sharing. Just as interns should be involved in the development of feedback mechanisms, they should also influence the interpretation and dissemination of the feedback results (providing a crucial and context-sensitive way of protecting them from the repercussions of negative feedback). As noted by Gee and Shackman, inviting trainees to serve and vote as members of accreditation, guideline-setting agencies, and professional organizations is a very important and achievable step. Feedback from trainees is not only a data-collection strategy but also a way to empower interns.
Importantly, strategies for involving trainees in HSP-training decisions do not need to be led by training programs and can be enacted by clinical-science forums and organizations. For example, academic journals may add weight to trainee perspectives by soliciting special issues on training that include trainee coauthors (a practice exemplified by the journal Translational Issues in Psychological Science, published in collaboration with the American Psychological Association of Graduate Students [APAGS]; Weiss, 2021). Organizations such as the Association for Psychological Science (APS) can also ensure the involvement of trainees in different aspects of HSP training by codifying collaborative trainee-stakeholder models into their standards. As Atkins and Mehta (2024) noted, “[APS-affiliated] Psychological Clinical Science Accreditation System (PCSAS) has yet to identify internship standards after more than a decade into its formation” (p. 172) despite early calls to do so (Atkins et al., 2014). Establishing such standards is imperative.
Balancing Action With Knowledge: Reflections on a Postdoctoral Internship
A core issue noted by all commentaries is that although internship is a required part of doctoral training, it is only loosely connected with interns’ doctoral programs. Perhaps the most prominent large-scale solution recommended in the commentaries was a transition to a postdoctoral internship (i.e., internship would begin after completion of the doctorate). This idea has been raised recurrently over the years (Berenbaum et al., 2021) and was advocated by Knowles et al. (2024), Galán et al. (2024), and Gee and Shackman (2024). On the other hand, Atkins and Mehta (2024) recommended strengthening ties between internships and graduate programs. We, much like the authors of the commentaries, are not uniformly in opposition or in favor of a shift toward postdoctoral internships. Although Galán et al. interpreted our article as “predicated on” a predoctoral model of internship (p. 182), we wish to clarify that we wrote about internship in the only way we have experienced it and not as an argument for retaining the predoctoral model.
Advocates of the postdoctoral internship anticipate many potential benefits of its adoption. Knowles et al. (2024) recommended a transition to postdoctoral internship as a high-impact initiative that would prevent programs from selectively deciding which recommendations for action in HSP training to take up. If its proponents’ best intentions are realized, these benefits would indeed address a number of our recommendations (Palitsky et al., 2022), including improved understanding of the status and roles of interns (Recommendations 1–3), elimination of redundant training, excessive focus on training hours and improved choice in training (Recommendations 4, 6), improved pay and benefits for interns (Recommendations 14–16), elimination of tuition and fees for interns still in their graduate programs, and greater parity with the physician model of training (e.g., formalizing “interns/internship” as “residents/residency”). However, these are potential strengths, and—as with the other recommended changes—a shift as large as a transition to postdoctoral internship should be carefully evaluated to constitute a real improvement for trainees.
We emphasize that each of the recommendations we made in the initial article (Palitsky et al., 2022) remains relevant, and if a transition to postdoctoral internship occurs, sustained quality-improvement initiatives aligned with our recommendations are still needed. It remains unclear to what extent these recommendations would be effected in a transition to postdoctoral internship. For example, it is not guaranteed that a postdoctoral internship would shift training benchmarks from clinical hours to competencies (Recommendation 4), that trainee approval would be sought when training aims change (Recommendation 7), or that trainees would have broad representation in the infrastructure of training (Recommendations 20–24). These recommendations would still need to be pursued, and we do not believe that the only choice is between cherry-picking solutions or adopting one singular, sweeping change. To address the many issues that require consensus, we recommend dedicated forums for discussion and dialogue to identify criteria that would need to be met to justify such a change, which should meaningfully include trainee stakeholders.
If we are to achieve a trainee-stakeholder model in HSP training, perhaps the most integral question is whether postdoctoral interns would, in fact, have more voice in training. Galán et al. (2024) stated that “As postdoctoral fellows, interns could play a critical role in the evolution of internships.” (p. 183). However, the postdoctoral role is notoriously exploitative (Greenberg, 2003), particularly of women, BIPOC (Black, Indigenous, and other people of color) individuals, international workers, and underserved populations (Ålund et al., 2020; Bodin et al., 2018; Ding, 2021; Karalis Noel et al., 2022). Many of this article’s authors have now completed postdoctoral fellowships, and we cannot in confidence state that we have had greater opportunities for input into our own training during our fellowships than we had during internship (some authors have; some have not). Postdoctoral internship may be a deferral, rather than a solution, to solving the existing problems with the HSP internship as long as postdoctoral fellows also lack real influence on training.
Discussion
More and better data are important, but in the absence of meaningful power-sharing, trainee concerns and suggestions can easily be ignored. (Gee & Shackman, 2024, p. 177)
There are clear tensions in our responses to these commentaries: We urge for better data on HSP training, but we also advocate against waiting for the data to come in. We call for action now, yet we hesitate at big changes such as postdoctoral internship. To help manage these tensions, we return to the trainee-stakeholder and collaborative approaches that we advocated in our article (Palitsky et al., 2022) and this commentary. We introduce a simple heuristic: Are trainees included or excluded? The application of this heuristic to the need to know and the need to act is illustrated in Figure 1. For example, data collection is an important tool for representing the impacts of policies on trainees, clients, and others with a stake in HSP training as long as the data reflect and represent their experiences. Importantly, data should not be made to stand in the place of trainees or act as a barrier to their inclusion. Specific kinds of data gathered on behalf of trainees should not be required to legitimate trainee concerns. Likewise, concerted action is needed in response to the serious challenges of HSP internship. When trainees are included collaboratively, the field begins to directly address problems in training. However, when large-scale changes are made on the administrative level on behalf of trainees without including them, it is easy to make oversights, even with the best of intentions. In the impetus for greater knowledge and effective action to improve HSP training, trainee inclusion is key.
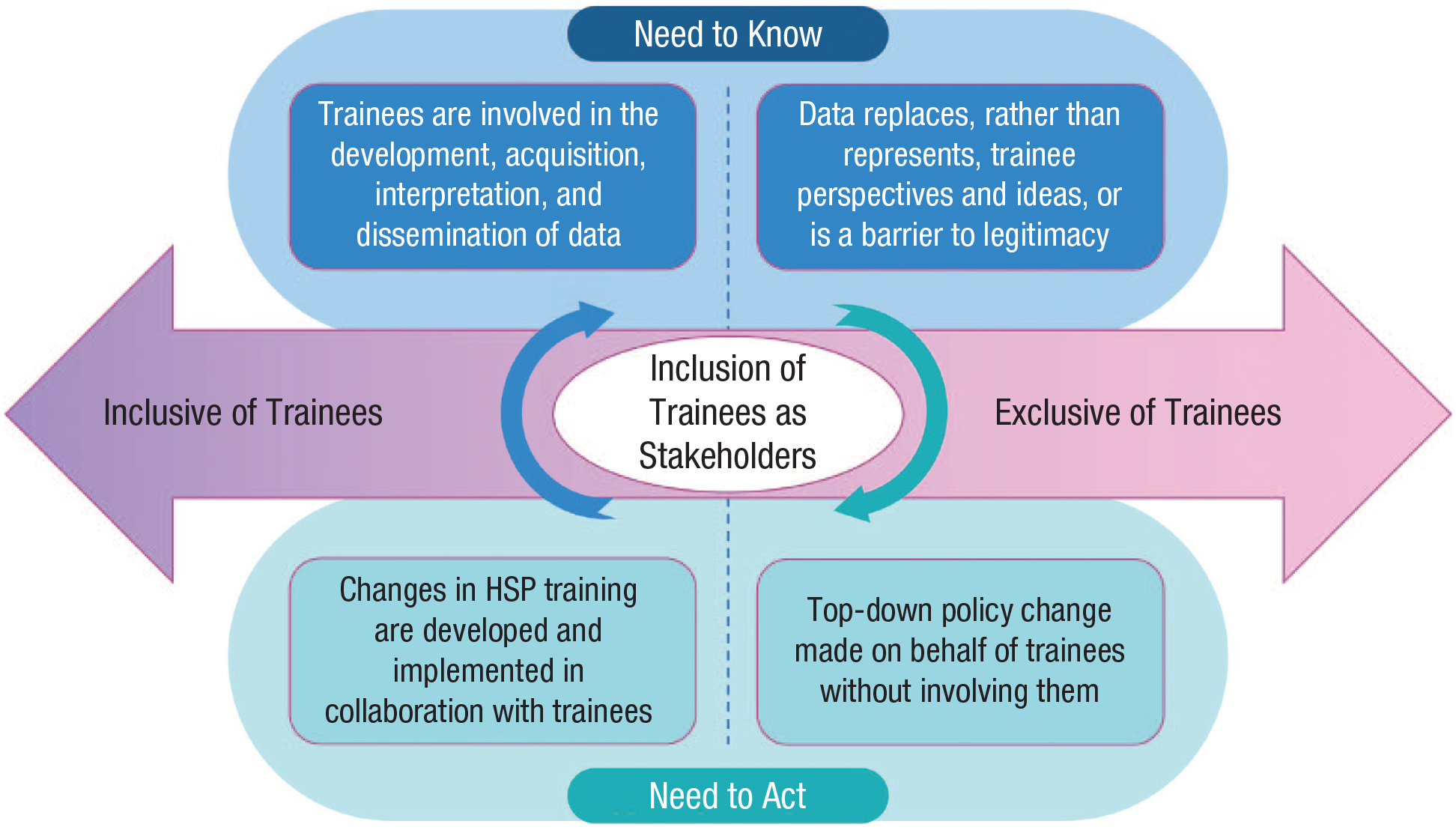
The importance of trainee inclusion for knowledge and action in HSP internship.
In that spirit, we recapitulate that deliberate efforts to develop new policies that support trainees across the field are needed now. We concur with Atkins and Mehta (2024) that guidelines for internship from APS are long past due. Even provisional guidelines, perhaps published as the summary statement from a nationwide meeting, would represent a visible benchmark that can be followed with action from PCSAS and other training entities. Training agencies and entities in clinical, counseling, and school psychology, including PhD and PsyD programs, would be important collaborator-stakeholders in such an effort. There are already existing initiatives moving in this direction in HSP, such as recent efforts by the Coalition for Advancement and Application of Psychological Science, which includes members of many professional societies and organizations instrumental in training (e.g., Park & Stewart, 2022). “Boulder 2.0” has also become an increasingly popular idea, which may be realized in planned meetings such as the Summit on Clinical Science Training (Academy of Psychological Clinical Science, 2023). We call for trainees, including especially trainees of historically marginalized positionalities, to be included as partners in these next steps for training reform. In addition to these top-down change strategies, individual programs can make meaningful changes that are locally responsive while advocating for larger systematic national changes rather than waiting for them to occur from the top-down, as exemplified by Atkins and Mehta (2024).
Note that articles such as ours (Palitsky et al., 2022) may be helpful for beginning to explore issues relevant to interns, but reading the experiences of a group of interns who are not local stakeholders to a given program is not a suitable substitute for including local interns. We do not write on behalf of all trainees in this commentary and speak only from our own experiences and understandings of clinical training. Although there were many voices included in our initial article (Palitsky et al., 2022) and the commentary responses, many perspectives remain unrepresented. At the same time, our assessment points to the importance of action because the cost of inaction is an untenable status quo. In the responses the field takes to the many calls for action in HSP training, including trainees as stakeholders will be vital for an equitable and sustainable future.
Footnotes
Transparency
Action Editor: Jennifer L. Tackett
Editor: Jennifer L. Tackett
Author Contribution(s)
M. R. Anderson, A. Athey, M. A. Brodt, J. A. Coffino, A. Egbert, E. S. Hallowell, J. T. Fox-Fuller, G. T. Han, M.-A. Hartmann, C. Herbitter, M. Herrera Legon, C. Hughes, N. C. Jao, M. T. Kassel, T.-A. P. Le, H. F. Levin-Aspenson, G. López, M. R. Maroney, M. Medrano, and M. L. Rogers share equal authorship.