
Abstract
The COVID-19 pandemic resulted in drastic disruptions to lives and possible pernicious impacts on mental health, including suicidality. Understanding these relations, as well as impacts on at-risk populations, is essential. The present study examined changes in daily behaviors and cognitions after the implementation of physical/social distancing mandates in individuals with symptoms of suicide crisis syndrome (SCS) and/or suicidal ideation. Adults (N = 5,528) across 10 countries completed online self-report measures. There were significant main effects of time and various configurations of interactions between time, SCS, and suicidal ideation in predicting behaviors (outdoor and social engagements) and cognitions (thoughts about health, finances, and living situation). Cross-culturally, individuals with more severe SCS symptoms generally had the largest changes in behaviors and cognitions, though this effect was not replicated across all countries. Overall, these findings highlight the implications of the potentially mutually exacerbating influences of routine disruptions and suicide risk and the importance of examining associations cross-culturally.
The COVID-19 pandemic introduced unprecedented challenges to social and economic structures across the globe, consequently upending the lives of billions of people. Since the declaration of the public health emergency in the beginning of 2020, more than 90 countries and territories have imposed lockdowns and restrictions to varying degrees. For instance, from March through May 2020, the United States saw the issuance of mandatory stay-at-home orders in 42 states, resulting in a decreased median population movement across the nation (Moreland et al., 2020). These stay-at-home orders included a shift to virtual learning, decreased public transportation services, and the closing of businesses that were deemed nonessential on the basis of individual state guidelines. In China, stringent regulations prohibited transport across cities, banned private vehicles from roads, and limited outings from one’s home (Koh, 2020). In December 2020, Colombia’s government permitted its citizens to leave their homes only on certain days, based on the last number of their identification numbers (Alsema, 2020). Meanwhile, many countries across Europe and Asia, including the United Kingdom, The Netherlands, France, and Israel, entered their second or third lockdowns in February 2021, shutting down schools and nonessential businesses alongside the implementation of nationwide curfews (Buchholz, 2021). These safety measures have reshaped daily life for billions of people worldwide, as financial strain, social isolation, and health concerns have been exacerbated by the pandemic.
Although mass quarantines at such a historic level have rarely occurred, disruptions to daily life more broadly, including isolation, restricted social interactions, and financial changes, have been commonly viewed as contributory factors to mental health concerns. For instance, social isolation has been linked to myriad physical and mental health concerns, including depression, poor sleep quality, impaired executive functioning, poor cardiovascular functioning, and impaired immunity (Hawkley & Capitanio, 2015), as well as increased mortality rates from all causes (Holt-Lunstad et al., 2015), including suicide (Van Orden et al., 2010). Likewise, financial stressors have been linked to increased inflammation (Sturgeon et al., 2016), poorer physical health (Ahnquist et al., 2012), and greater psychological distress (Myers, 2000), including suicidal thoughts and behaviors (Van Orden et al., 2010). More recently, initial studies examining the psychosocial impact of the COVID-19 pandemic have highlighted upsurges in depression, anxiety, sleep disturbances, and acute posttraumatic stress symptoms cross-nationally (Casagrande et al., 2020; Odriozola-González et al., 2020; Sun et al., 2021; J. Zhu et al., 2021; S. Zhu et al., 2020). Potential mechanisms underlying the relationships between COVID-19-related life disruptions (e.g., lockdowns) and aggravated mental health concerns include constriction of social interactions and social support, which have been significantly related to stress coping and largely achieved through face-to-face exchanges (Ono et al., 2011; Usher et al., 2020); increases in physical inactivity, which have been associated with loneliness, sadness, and anxiety (Werneck et al., 2021); and excessive worries about potential infection and/or financial losses (Brooks et al., 2020; Mimoun et al., 2020). Thus, it is plausible that populations at higher risk of experiencing financial or health-related distress may be more susceptible to pandemic-induced psychological distress.
As hypothesized early in the pandemic (Gunnell et al., 2020; Reger et al., 2020) and supported by preliminary emerging data (Bray et al., 2021; Fortgang et al., 2021; Gunnell et al., 2020, though see also Pirkis et al., 2021), individuals may also be at elevated risk for suicide-related symptoms and outcomes during and following pandemic-related life disruptions (e.g., lockdowns, social isolation, financial stress), including both explicit suicidal ideation and more indirect indicators of suicide risk. Such indirect indicators may include suicide crisis syndrome (SCS; Galynker, 2017), an acute, time-limited cognitive-affective mental state that is characterized by intense and persistent feelings of entrapment, affective disturbances, loss of cognitive control, hyperarousal, and social withdrawal and that has accumulated empirical support as a predictor of prospective, short-term suicidal behavior (Barzilay et al., 2020; Bloch-Elkouby et al., 2020; Galynker et al., 2017; Yaseen et al., 2019). Notably, SCS does not include suicidal ideation or intent as a core feature, overcoming issues related to the nondisclosure of suicidality (Berman, 2018; Podlogar et al., 2016) and allowing for the comparison of risk among individuals who explicitly disclose suicidal ideation and those who exhibit acute risk factors for suicide yet deny experiencing suicidal ideation. Previous research has indicated that stressful life events (including routine disruptions) are associated with both suicidal ideation (Howarth et al., 2020) and SCS (Bloch-Elkouby et al., 2020; Cohen et al., 2018, 2019).
In the context of the COVID-19 pandemic, lockdowns issued across the world may have led to changes in individuals’ thoughts and behaviors, such as decreases in outdoor and social activities as well as increases in worries about health, finances, and living situations. Such disruptions to routines, especially when mandated by external events and mandates occurring in the broader environment (e.g., spread of the virus, government mandates), may have resulted in increases in entrapment and social withdrawal, two symptoms of SCS that have been linked to suicidal ideation and behavior (Robins, 1981; Taylor et al., 2011), as people were limited in their ability to leave their homes and engage with others face to face. Indeed, previous research has linked quarantine-induced confinement, loss of daily routine, and decreases in both physical and interpersonal connections to an elevated sense of social isolation and distress (Brooks et al., 2020). Another possible explanatory factor is ruminative thinking, defined as a tendency to perseverate repeatedly and passively on one’s distress (Nolen-Hoeksema, 1991). Ruminative thinking, included as a core feature of SCS (Schuck et al., 2019) and identified as a risk factor for suicidal ideation and behaviors (Rogers & Joiner, 2017), may have been exacerbated during the pandemic because of excessive worries about health and financial situations. Notably, recent articles have proposed that the continuous exposure to the pandemic and pandemic-related information may lead to increased ruminative thinking and fear of COVID-19, thereby resulting in deteriorations in mental well-being (Satici et al., 2022; Ye et al., 2020). It is therefore possible that both lockdown-induced restrictions and increased rumination on these changes could contribute to poorer mental health outcomes, including SCS and suicidal ideation.
Our aims in the present study were twofold. First, we examined self-reported changes in individuals’ typical patterns of cognitions and behaviors over time, specifically from the year prior to the implementation of stay-at-home orders (i.e., “past year”) to the time period following the execution of these policies on a global scale (i.e., “since the stay-at-home orders”). Our second goal was to determine whether changes in cognitions and behaviors differed across individuals with varying severity of symptoms of SCS and/or suicidal ideation in a large community-based sample of adults across 10 participating countries. We accordingly made two hypotheses. The first was that, consistent with recent research, there would be significant changes in daily cognitions and behaviors after the implementation of stay-at-home orders. Our second hypothesis was that individuals with more severe suicide-related symptoms (i.e., SCS and/or suicidal ideation) would exhibit greater changes in daily cognitions and behaviors than those without these symptoms. We made no a priori hypotheses regarding potential differences between individuals presenting with SCS symptoms versus suicidal ideation, given a lack of previous research in this domain. Finally, in addition to examining overall effects in the entire sample, we tested models in each country to determine whether there were differences in the magnitudes of these effects across countries. We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study.
Method
Participants and procedures
Participants were 5,528 adults (age: M = 30.99 years, SD = 12.44, range = 18–89) who were recruited across 10 countries (Brazil: n = 127; Canada: n = 65; Germany: n = 532; India: n = 302; Israel: n = 195; Poland: n = 309; Russia: n = 561; South Korea: n = 1,043; Turkey: n = 424; and the United States: n = 1,970) to complete an anonymous battery of self-report measures online. Inclusion criteria included (a) being 18 years or older and (b) residing in the country of interest during the COVID-19 pandemic; there were no specific exclusion criteria. The majority of participants self-identified as cisgender women and as single/never married, and most had completed college/university. Detailed sociodemographic breakdowns for each country can be found in Table 1; racial/ethnic options differed by country and can be found in Table S1 in the Supplemental Material available online. Results of an a priori power analysis indicated that a sample size of 220 or higher was needed to achieve power of .80 to detect small to moderate two-way interaction effects with an alpha of .05 using mixed-model analyses.
Sociodemographic Characteristics of All Participants, Stratified by Country
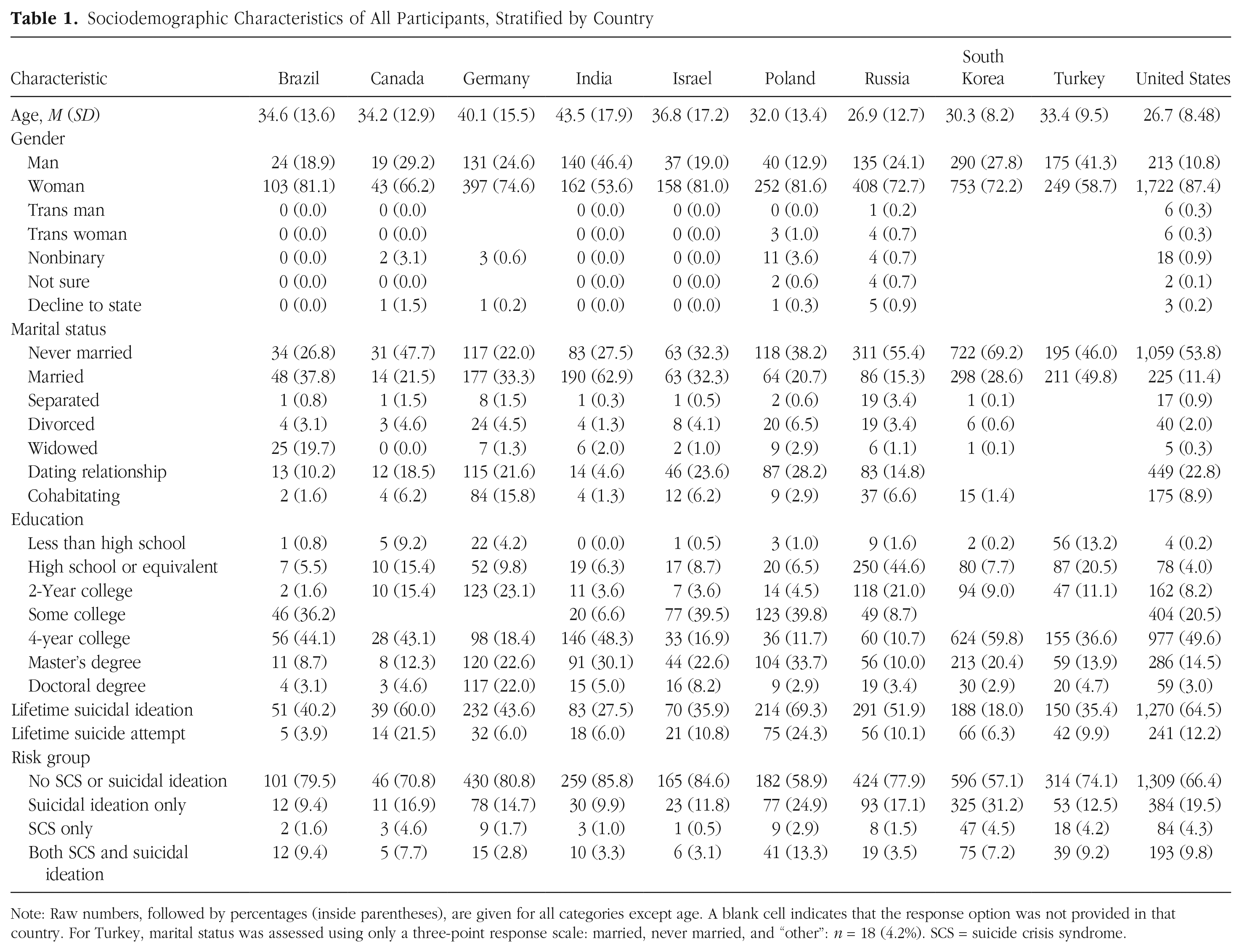
Note: Raw numbers, followed by percentages (inside parentheses), are given for all categories except age. A blank cell indicates that the response option was not provided in that country. For Turkey, marital status was assessed using only a three-point response scale: married, never married, and “other”: n = 18 (4.2%). SCS = suicide crisis syndrome.
Recruitment took place on various social media platforms and included both paid advertisements and individual postings. Prospective participants were directed to the study through an anonymous link to a secure online platform (Qualtrics); separate links were created for each country on the basis of primary language (or languages) spoken. Turkey additionally allowed for the distribution of paper copies of the study that were later manually entered into the survey platform. All participants provided electronic or written informed consent prior to completing the battery of self-report measures. Monetary compensation was offered in South Korea for the completion of the study, whereas participants in the U.S. sample were able to enter a raffle for compensation. Compensation was not offered in any other country. All study procedures were approved by the relevant institutional review boards or institutional ethics committees from the affiliated institutions of all principal investigators. Data collection took place from June 2020 to January 2021; specific dates for each country are included in the Supplemental Material.
Prior to the beginning of data collection, all study measures were translated into local languages across all countries through an iterative process, guided by steps outlined by Sousa and Rojjanasrirat (2011). Study measures underwent forward and blind backward translation by two independent bilingual coders; in some cases, two independent blind back translations were conducted, and these versions were compared and synthesized. Following these translations, several consensus meetings were held to discuss disagreements and finalize language translations for inclusion in each country’s study protocol.
Measures
Changes in behaviors and cognitions
Two sets of eight items, which were developed for the purposes of the present study, were administered to participants to measure the extent to which pandemic-related factors have influenced their daily lives. Specifically, these item sets contained differing stems to assess different time frames (i.e., “In the past year . . .” vs. “Since the stay-at-home order . . .”). Participants rated how often they engaged in each behavior/cognition during the specified time frame on a 5-point scale ranging from 1 (Never) to 5 (Always). Items specifically assessed time spent going outside, engaging in outdoor activities, engaging in social interactions, having face-to-face social interactions, thinking about one’s health, thinking about the health of a loved one, thinking about one’s financial situation, and thinking about one’s living situation.
Columbia—Suicide Severity Rating Scale Screener
The five-item screener version of the Columbia—Suicide Severity Rating Scale (C-SSRS; Posner et al., 2011) was administered to assess the presence and severity of participants’ past-month suicidal ideation and behaviors. Five binary (i.e., yes/no) items, with increasing severity, were used to assess suicidal ideation; higher summed scores were reflective of greater severity of suicidal ideation. The C-SSRS has demonstrated adequate reliability and convergent, discriminant, and criterion validity in previous research across populations (Gutierrez et al., 2019; Posner et al., 2011).
Suicide Crisis Inventory–2
The Suicide Crisis Inventory–2 (SCI-2; Bloch-Elkouby et al., 2021) is a 61-item self-report scale updated from the original Suicide Crisis Inventory (Galynker et al., 2017). The SCI-2 assesses the presence and severity of SCS symptoms, including entrapment, affective disturbances, loss of cognitive control, hyperarousal, and social withdrawal. Participants rated the intensity of each symptom based on their worst feelings over the last several days on a 5-point scale ranging from 0 (Not at all) to 4 (Extremely). The SCI-2 has demonstrated strong internal consistency, convergent and discriminant validity, and predictive validity in relation to suicide attempts in past research (Bloch-Elkouby et al., 2021). In the present study, internal consistency was very high (α = .98).
Data-analysis strategy
Descriptive statistics were first computed to examine each COVID-related cognition/behavior variable. Next, because our outcome variables were single items rated on 5-point Likert scales, we tested assumptions that model residuals would be normally distributed through examination of quantile-quantile (Q-Q) plots (Chambers et al., 2017) and Shapiro-Wilk tests (Shapiro & Wilk, 1965). In all cases, assumptions of normality were not met, so these cognitions and behaviors (i.e., outcome variables) were treated as ordinal in all subsequent analyses. Accordingly, cumulative link mixed models (Bürkner & Vuorre, 2019), which are designed to handle ordered yet noncontinuous response data, were then computed using the ordinal (Christensen, 2019) package to examine changes in each cognition/behavior over time (i.e., past year vs. since the stay-at-home order), as moderated by SCS symptom severity and suicidal ideation severity. Specifically, the main effects and interaction of time (0 = past year, 1 = since stay-at-home order), SCS symptoms, and suicidal ideation severity were entered as fixed predictors, whereas each cognition/behavior was entered as an outcome variable in separate models. Pairwise comparisons within significant interaction effects were examined using the emmeans package (Lenth, 2021) and plotted using the emmip() function. Random intercepts were modeled such that time points were nested within individual participants, which were nested within countries, to account for nonindependence of observations across these three levels. Age and gender identity were included as covariates in all models to account for the potential influence of these sociodemographic characteristics. All continuous variables were centered/standardized prior to inclusion in models to facilitate interpretation. Nagelkerke pseudo-R2 values are reported for each model compared with the baseline model.
All models were first conducted using the full sample but then refitted across individual countries separately to examine potentially differential cross-national effects. Importantly, only countries with a sample size large enough to allow us to detect small to moderate two-way interaction effects (i.e., n = 220 or higher) were included in country-specific analyses (i.e., Brazil, Canada, and Israel were not analyzed separately). Because of the large number of statistical tests conducted, alpha for all cumulative link mixed models was set to .01, and the Holm-Bonferroni correction was used for all pairwise comparisons to adjust for Type I error rate.
Missing data, which ranged from 0.0% to 3.5% missing across individual variables, were handled using listwise deletion. However, Little’s (1988) test indicated that data were not missing completely at random, χ2(365) = 1,048, p < .001. Instead, data were missing at random. Therefore, we conducted sensitivity analyses and estimated each model with multiple imputation with 10 imputed data sets using the MICE package (van Buuren & Groothuis-Oudshoorn, 2011). Pooled estimates, standard errors, p values, and confidence intervals were nearly equivalent to those calculated using the listwise-deletion approach. 1 Given the similarity of these estimates, as well as the complexity of the models combining cumulative linked mixed modeling and multiple imputation—which posed challenges for estimating marginal means and slopes—listwise-deletion results were retained and are reported in the text and tables.
Results
Means and standard deviations for each COVID-related behavior and cognition are listed in Table S2 in the Supplemental Material. For all primary analyses, full regression models, including main effects, interaction effects, and 99% confidence intervals, are presented in Tables 2 and 3 (outdoor behaviors), Tables 4 and 5 (social behaviors), Tables 6 and 7 (health-related cognitions), and Tables 8 and 9 (other cognitions) for the overall sample. Simple slopes of models with significant interaction effects in the full sample are included in Tables S3 through S6 in the Supplemental Material, and plots decomposing selected interactions can be found in Figures S1, S2, and S3 in the Supplemental Material. Regression models within each individual country can be found in Tables S7 through S14 in the Supplemental Material.
Fixed Effects From Cumulative Link Mixed Models Examining Changes in Outdoor Behaviors in the Full Sample
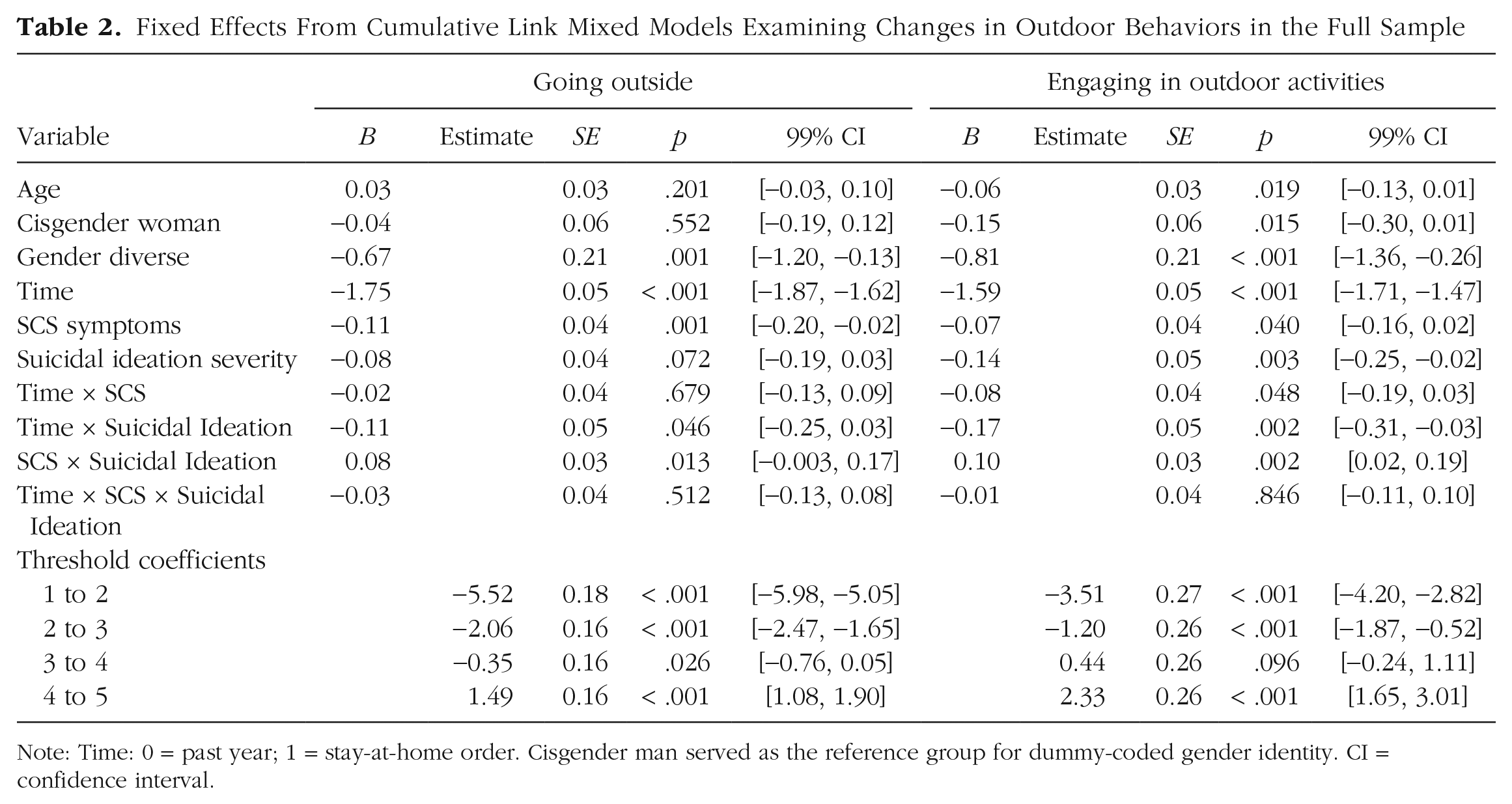
Note: Time: 0 = past year; 1 = stay-at-home order. Cisgender man served as the reference group for dummy-coded gender identity. CI = confidence interval.
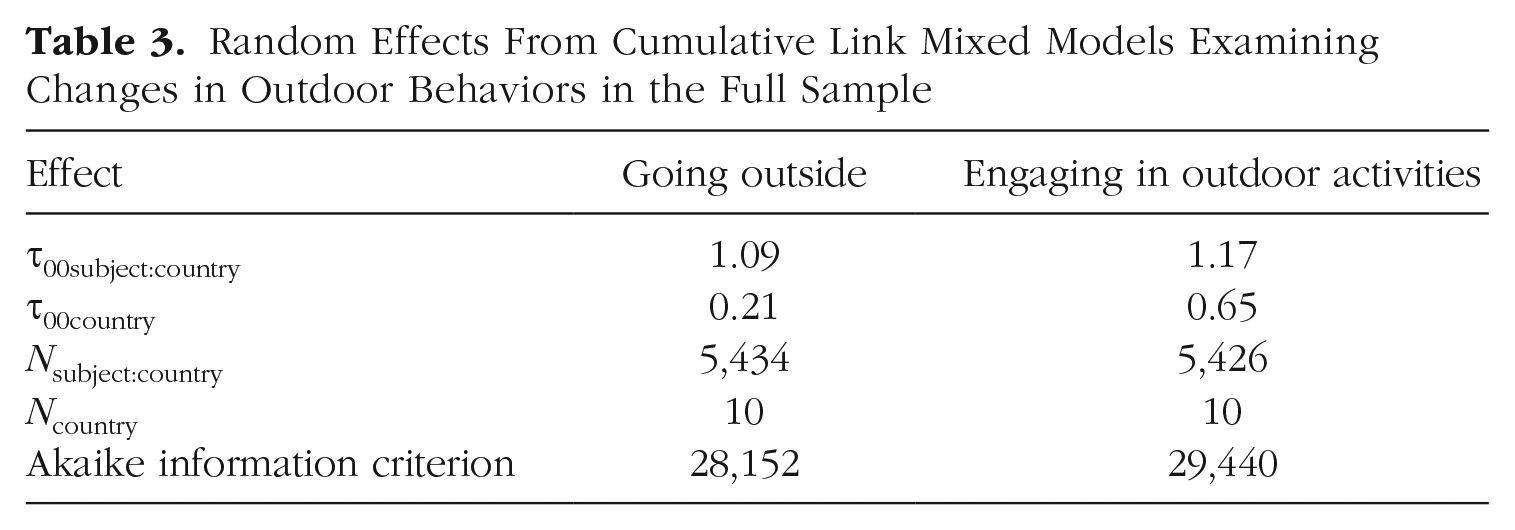
Random Effects From Cumulative Link Mixed Models Examining Changes in Outdoor Behaviors in the Full Sample
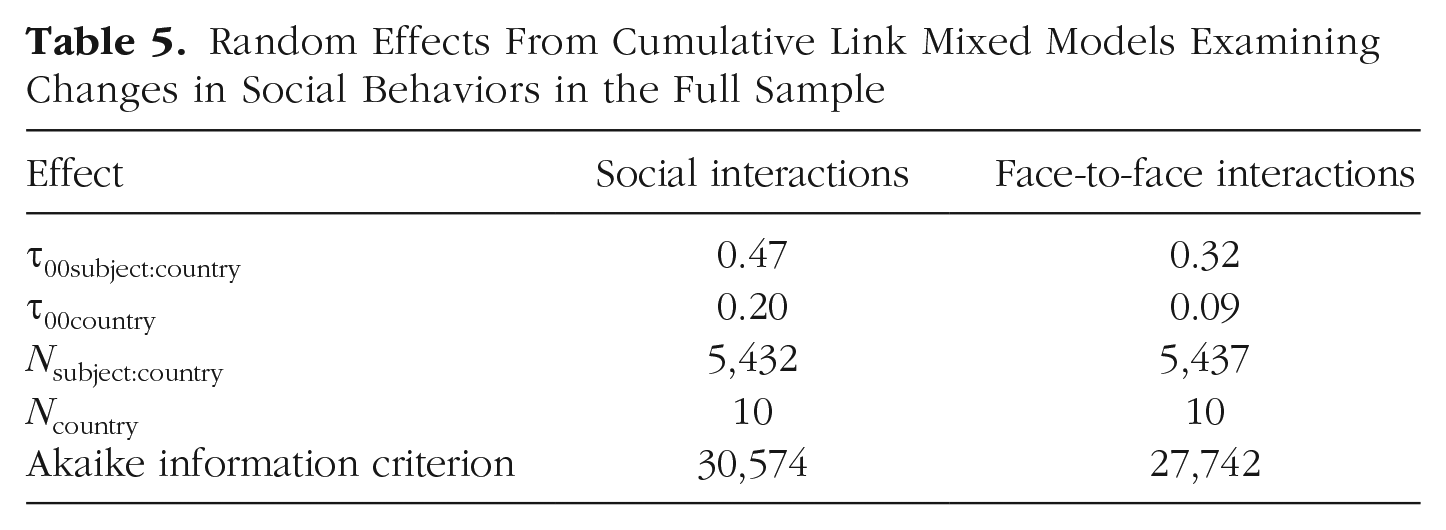
Fixed Effects From Cumulative Link Mixed Models Examining Changes in Social Behaviors in the Full Sample
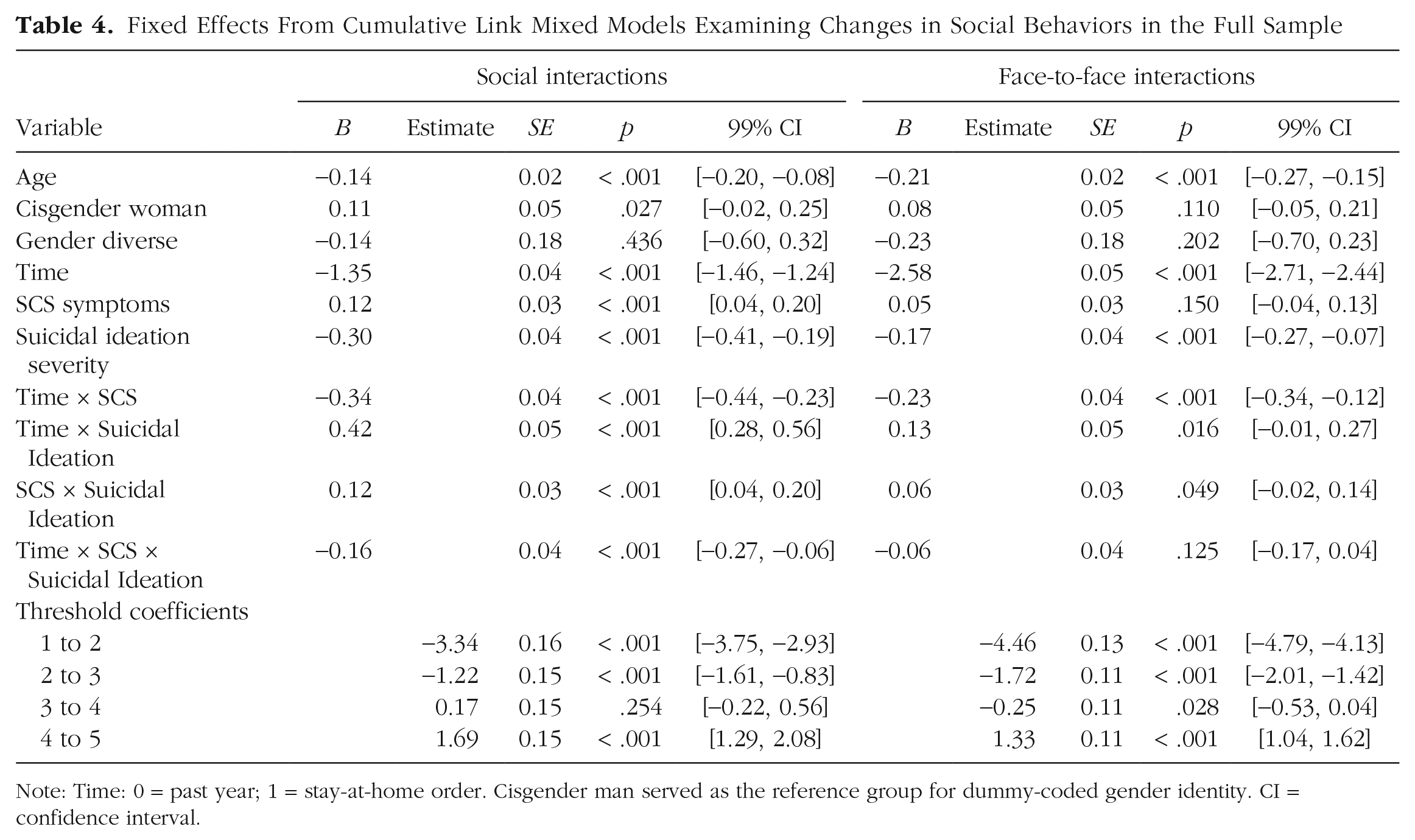
Note: Time: 0 = past year; 1 = stay-at-home order. Cisgender man served as the reference group for dummy-coded gender identity. CI = confidence interval.
Random Effects From Cumulative Link Mixed Models Examining Changes in Social Behaviors in the Full Sample
Fixed Effects From Cumulative Link Mixed Models Examining Changes in Health-Related Cognitions in the Full Sample
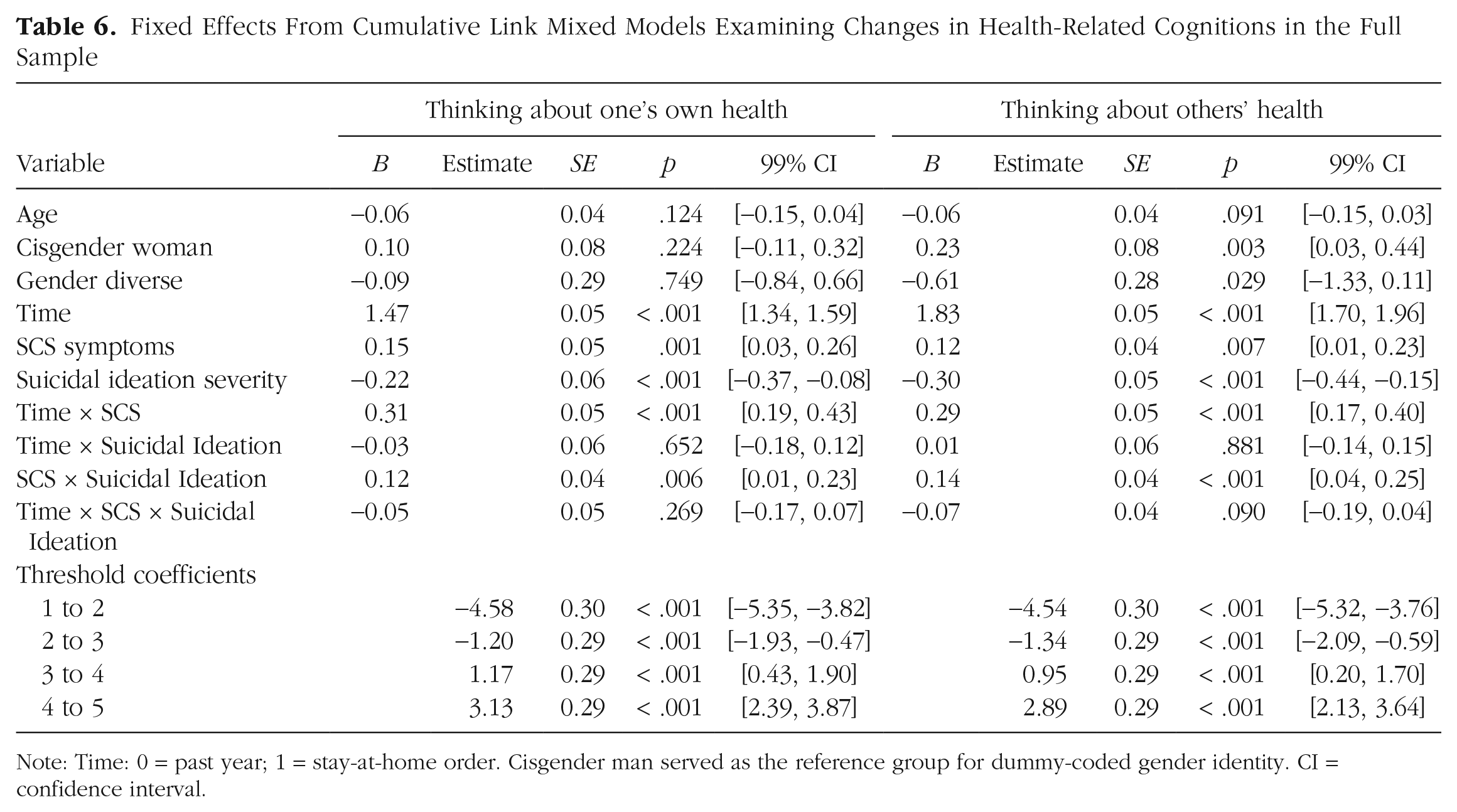
Note: Time: 0 = past year; 1 = stay-at-home order. Cisgender man served as the reference group for dummy-coded gender identity. CI = confidence interval.
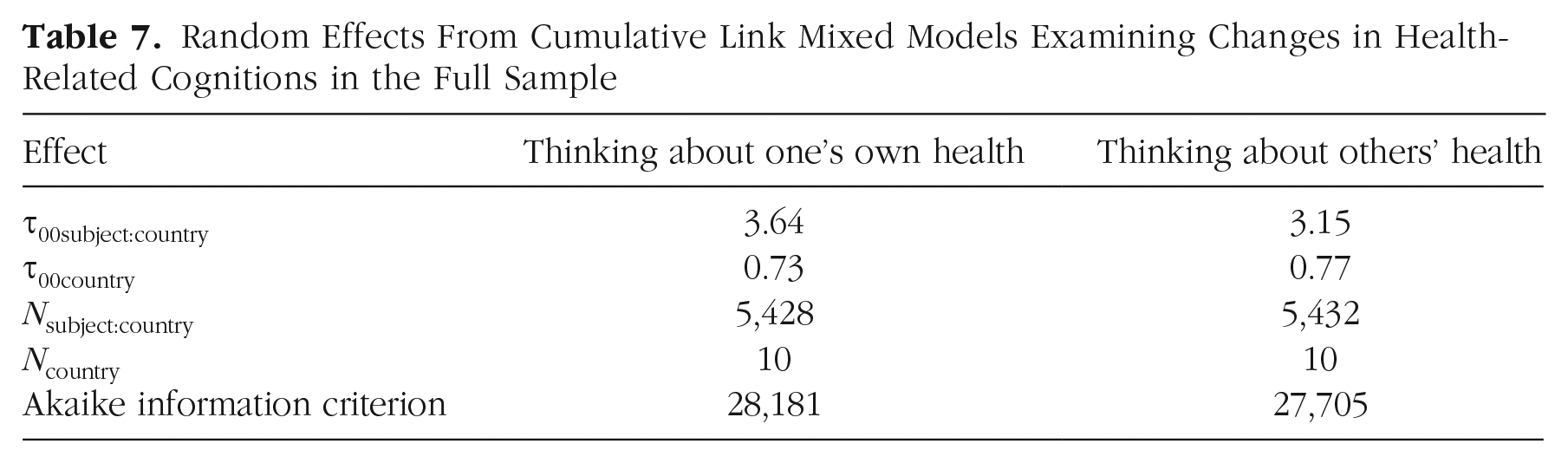
Random Effects From Cumulative Link Mixed Models Examining Changes in Health-Related Cognitions in the Full Sample
Fixed Effects From Cumulative Link Mixed Models Examining Changes in Other Cognitions in the Full Sample
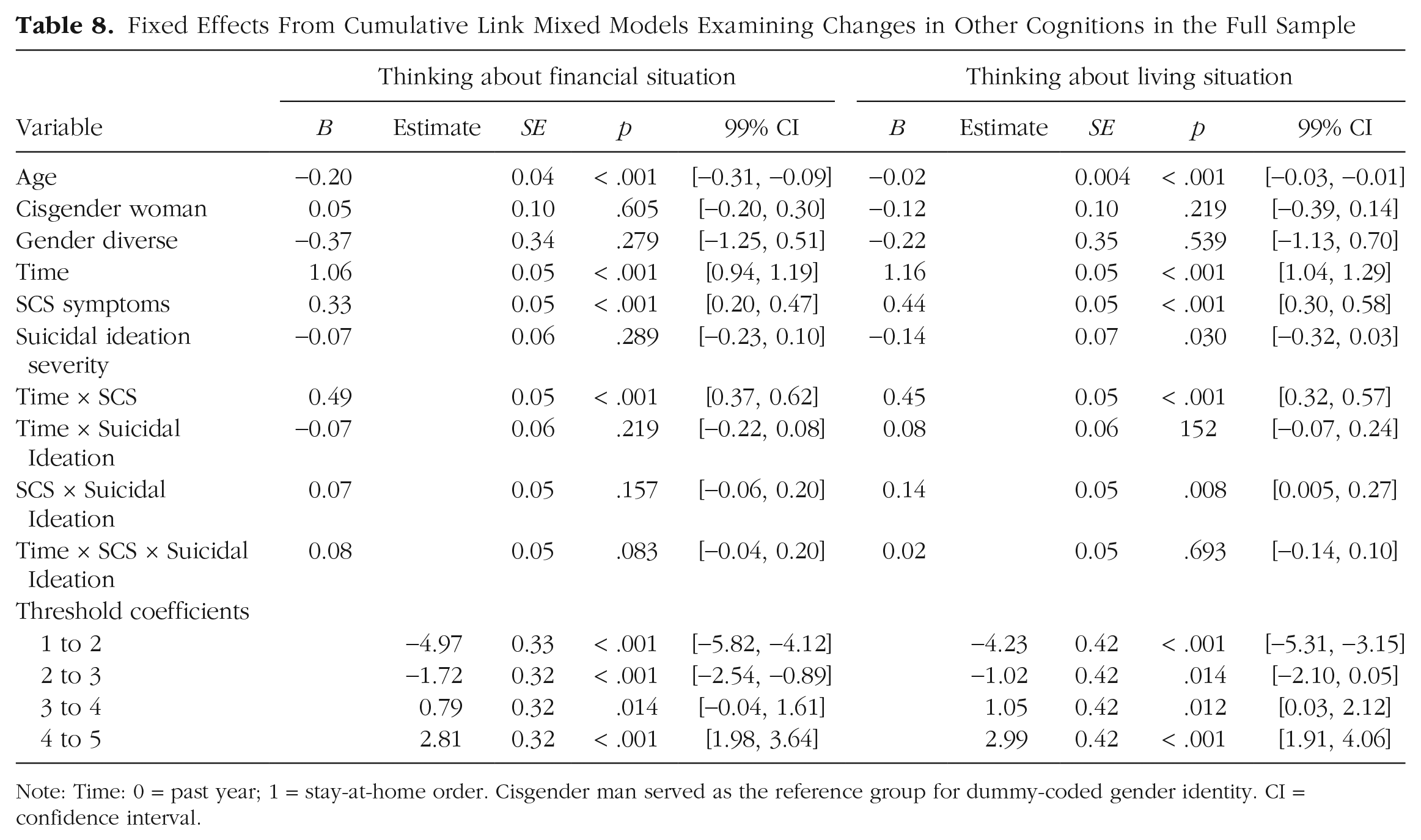
Note: Time: 0 = past year; 1 = stay-at-home order. Cisgender man served as the reference group for dummy-coded gender identity. CI = confidence interval.
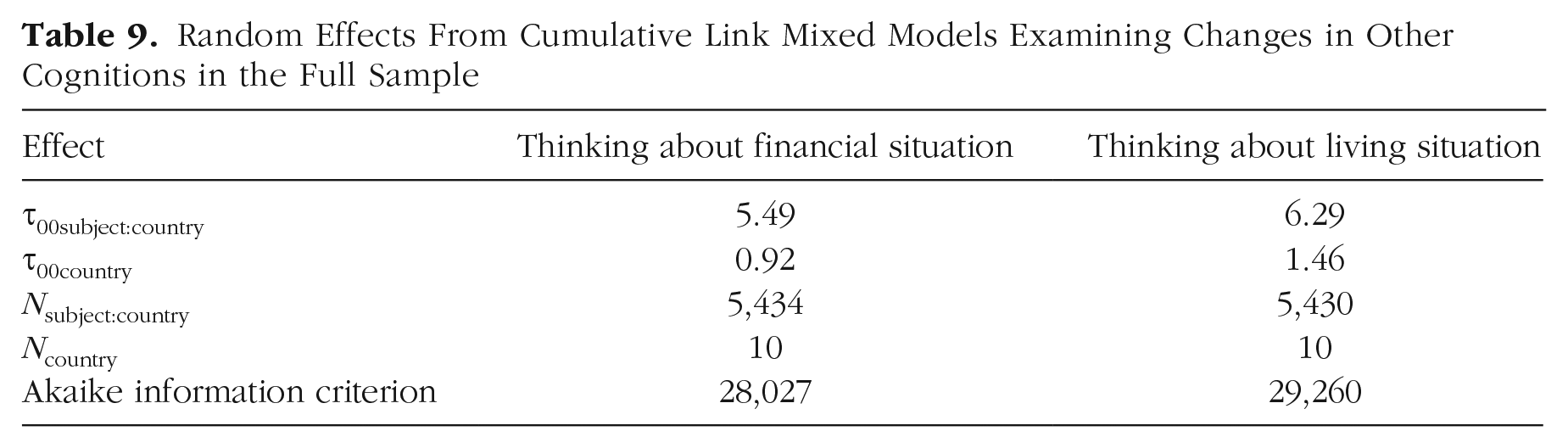
Random Effects From Cumulative Link Mixed Models Examining Changes in Other Cognitions in the Full Sample
Outdoor behaviors
Going outside
There were significant main effects of time and SCS but no main effect for suicidal ideation and no interaction effects between time, SCS, and suicidal ideation in predicting time spent going outside in the full sample (Nagelkerke R2 = .21). Specifically, there was a significant decrease in time spent going outside following the implementation of stay-at-home orders, and individuals with more severe SCS symptoms spent less time on average going outside across both time points than did those with less severe SCS symptoms.
Within individual countries, the main effect of time on time spent going outside was significant in all seven countries; specifically, there were decreases in going outside cross-nationally after the implementation of stay-at-home orders. Additionally, there was a significant interaction between time and SCS in predicting going outside in both Germany and the United States. In these countries, the decrease in time spent going outside was steeper among individuals with more severe SCS symptoms.
Engaging in outdoor activities
In the full sample (Nagelkerke R2 = .19), there were significant main effects for time and suicidal ideation, as well as significant interactions between time and suicidal ideation and between SCS and suicidal ideation, in predicting time spent engaging in outdoor activities. Time spent engaging in outdoor activities decreased among all participants following the implementation of stay-at-home orders, and those with more severe suicidal ideation symptoms spent less time on average engaging in outdoor activities across both time points than did those with less severe suicidal ideation. Moreover, simple-slopes analyses indicated that these effects were synergistic: Participants with high levels of both SCS and suicidal ideation symptoms spent less time engaging in outdoor activities than did those without high levels of both symptoms, and the decrease in time spent going outside was steeper among individuals with more severe suicidal ideation.
Significant main effects for time were found in all countries, whereas main effects for SCS were found in Russia, and main effects for suicidal ideation were found in South Korea and the United States. The interaction effect between SCS and suicidal ideation was found only within the United States. However, there were additional interaction effects between time and SCS in Germany and the United States; specifically, the decrease in time spent engaging in outdoor activities after the implementation of stay-at-home orders was steeper among individuals with more severe SCS symptoms. Finally, the three-way interaction between time, SCS, and suicidal ideation was significant only in South Korea.
Social behaviors
Social interactions
There was a significant Time × SCS × Suicidal Ideation interaction in predicting time spent engaging in social interactions in the full sample (see Fig. S1 in the Supplemental Material; Nagelkerke R2 = .17). Decomposition of this interaction effect indicated that there were steeper decreases in time spent engaging in social interactions following the implementation of stay-at-home orders among participants with more severe SCS symptoms, but this effect was attenuated as levels of suicidal ideation severity increased. In other words, changes in time spent engaging in social interactions were strongest among participants with high levels of SCS symptoms and low levels of suicidal ideation, and changes were weakest among those with low levels of SCS symptoms and high levels of suicidal ideation. All two-way interactions and main effects were also significant in this model.
Across individual countries, this three-way interaction was not maintained; however, there was a significant interaction between time and SCS in predicting time spent engaging in social interactions in Poland, Turkey, and the United States, as well as main effects of time in all countries. In Poland and the United States, changes in time spent engaging in social interactions following the implementation of stay-at-home orders decreased most steeply among participants with more severe SCS symptoms.
Face-to-face interactions
In the full sample (Nagelkerke R2 = .36), there were significant main effects for time and suicidal ideation, as well as an interaction effect between time and SCS, in predicting time spent in face-to-face interactions. Specifically, individuals with more severe suicidal ideation spent less time in face-to-face interactions across time points, and time spent in face-to-face interactions decreased after the implementation of stay-at-home orders. Furthermore, this decrease in time spent in face-to-face interactions was steeper among individuals with more severe SCS symptoms.
Within individual countries, the main effect of time was significant across all seven countries, with significant decreases in time spent in face-to-face interactions after the implementation of stay-at-home orders, but the main effect of suicidal ideation was significant only in Germany and the United States. Moreover, the interaction effect between time and SCS, with steeper decreases over time among individuals with more severe SCS symptoms, was statistically significant only in the United States.
Health-related cognitions
Thinking about one’s own health
There were significant main effects of time, SCS, and suicidal ideation, as well as significant interactions between time and SCS and between SCS and suicidal ideation, in predicting time spent thinking about one’s own health in the full sample (Nagelkerke R2 = .15). In particular, time spent thinking about one’s health increased after the implementation of stay-at-home orders, and increases were steeper among individuals with more severe SCS symptoms. Additionally, suicidal ideation severity was negatively associated with time spent thinking about one’s health across time points, but this effect was weaker among individuals with more severe SCS symptoms.
The Time × SCS interaction effect was significant in Poland and the United States, whereas the SCS × Suicidal Ideation interaction effect was significant only in Russia. The main effect for time was observed in all countries. There was also a main effect observed for SCS symptoms in Germany and South Korea; specifically, SCS symptoms were positively associated with time spent thinking about one’s health in both countries.
Thinking about other people’s health
There were significant main effects of time, SCS, and suicidal ideation, as well as significant interactions between time and SCS and between SCS and suicidal ideation, in predicting time spent thinking about the health of loved ones in the full sample (Nagelkerke R2 = .20). Namely, the amount of time spent thinking about others’ health increased after the implementation of stay-at-home orders, and increases were steeper among individuals with more severe SCS symptoms. Additionally, suicidal ideation severity was negatively associated with time spent thinking about others’ health across time points, but this effect was weaker among individuals with more severe SCS symptoms. SCS severity was positively associated with time spent thinking about others’ health.
The Time × SCS interaction was found in Poland and the United States, and the SCS × Suicidal Ideation interaction was found in Russia and Turkey. Main effects of time were also replicated across all countries, and main effects of suicidal ideation were found in Russia.
Other cognitions
Thinking about one’s financial situation
In the full sample (Nagelkerke R2 = .13), there was a significant interaction between time and SCS, as well as significant main effects for time and SCS, in predicting time spent thinking about one’s financial situation. Specifically, increases in time spent thinking about one’s financial situation occurred in the full sample after the implementation of stay-at-home orders but were strongest among individuals with more severe SCS symptoms. Likewise, individuals with more severe SCS symptoms also spent more time thinking about their financial situations across both time points.
Within individual countries, the Time × SCS interaction was significant in Germany, Russia, and the United States; however, there was additionally a three-way interaction between time, SCS, and suicidal ideation in predicting time spent thinking about one’s financial situation in Poland and South Korea. In both countries, increases in time spent thinking about one’s financial situation following the implementation of stay-at-home orders were stronger among participants with more severe SCS symptoms and were strengthened slightly at high levels of suicidal ideation among individuals with high levels of SCS symptoms. There was additionally a main effect of time in all countries except India, in which there were no significant main or interaction effects.
Thinking about one’s living situation
There was a significant interaction effect between time and SCS, as well as significant main effects for time and SCS, in predicting time spent thinking about one’s living situation in the full sample (Nagelkerke R2 = .21). Increases in time spent thinking about one’s living situation following the implementation of stay-at-home orders occurred across all participants, on average, but were strongest among those with more severe SCS symptoms. Moreover, individuals with more severe SCS tended to spend more time thinking about their living situations across time points.
Significant Time × SCS interaction effects were found in Germany and the United States, whereas main effects for time were found in all countries, and main effects for SCS were found in Germany, South Korea, and the United States. There were no other significant main or interaction effects in India, Poland, Russia, or Turkey.
Discussion
Our aims in this study were twofold. First, we wanted to examine changes in individuals’ self-reported typical patterns of cognitions and behaviors from the time period preceding the pandemic to the time period following the implementation of pandemic-related restrictions and stay-at-home orders. Second, we wanted to determine whether these changes differed in magnitude across individuals with varying SCS symptom severity and suicidal ideation. Table 10 shows the statistically significant effects. Across samples collected from 10 participating countries, results first indicated that there were significant changes in each daily behavior and cognition after the implementation of pandemic-related stay-at-home orders and restrictions. Specifically, in the full sample, participants spent significantly less time engaging in outdoors and social activities, whereas they spent significantly more time worrying about their health, the health of their loved ones, their finances, and their living situations; however, these effects were found inconsistently across individual countries. Participants with more severe suicidal ideation also tended to engage in less frequent behaviors (i.e., outdoor and social activities) and have more frequent cognitions (i.e., thoughts about health) than those with less severe ideation across both time points. Furthermore, for many of these behaviors and cognitions, individuals who reported more severe SCS symptoms reported significantly greater changes in these behaviors and cognitions, on average, than did those who reported less severe SCS symptoms. Overall, these findings have several implications regarding the impact of stressful circumstances and disruptions to daily routines among adults with varying degrees of psychological distress and suicide risk.
Summary of Statistically Significant Fixed Effects in the Full Sample
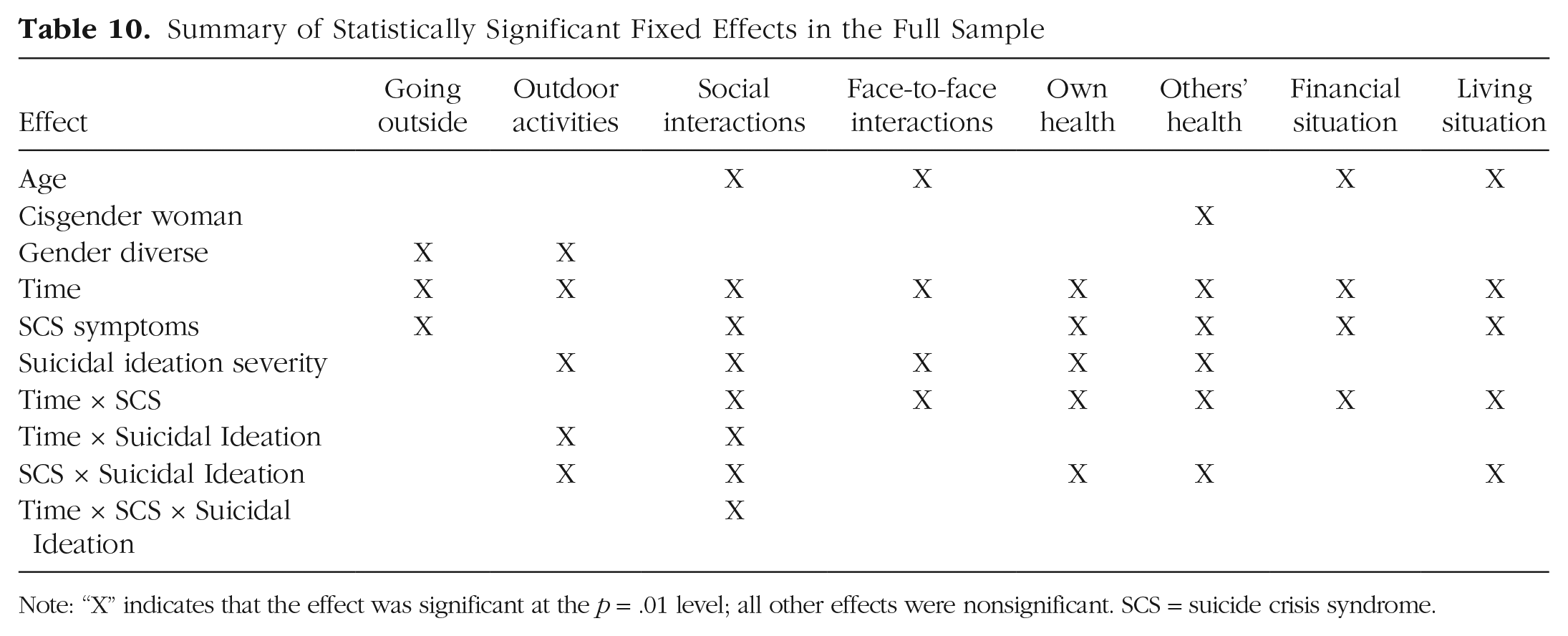
Note: “X” indicates that the effect was significant at the p = .01 level; all other effects were nonsignificant. SCS = suicide crisis syndrome.
First, the severity of recent suicidal ideation was associated with more frequent cognitions and worries, both before and during the pandemic. However, there were minimal interactions between suicidal ideation and time (except for outdoor and social activities), indicating that the severity of suicidal ideation did not consistently exacerbate the frequency of these cognitions in the context of the pandemic. The significant interaction effects were consistent with those reported in a recently published study suggesting that the presence and severity of suicidal ideation is associated with less adherence to public health guidelines within the context of the pandemic (Gainza Perez et al., 2022). On the other hand, suicidal ideation, by definition, is a cognitively laden construct and has been linked to difficulties in cognitive functioning across populations. For instance, in a sample of psychiatric patients with depression, executive functioning was poorer in those with suicidal ideation than in those without suicidal ideation (Marzuk et al., 2005). Likewise, a study of U.S. veterans highlighted links between suicidal ideation severity and attention, memory, and overall cognition (Ryan et al., 2020), and a study of young adults demonstrated relationships between suicidal ideation severity and everyday memory retrieval and encoding (Chu et al., 2016), independent of depression symptoms. Given the links between cognitive fixations—including rumination (Rogers & Joiner, 2017), cognitive constriction (Shneidman, 1996), and other cognitive vulnerabilities (Abramson et al., 1998)—and suicidal ideation, it is possible that individuals with suicidal ideation were already experiencing heightened levels of worries. Specifically, the interplay between ongoing and suicidal ideation may not have exacerbated worries about health-, finance-, and living-situation-related concerns beyond what was already present during the pandemic.
On the other hand, individuals with more severe SCS symptoms had greater changes in their social activities and behaviors, as well as thoughts regarding health, finances, and living situations. Unlike suicidal ideation, which is primarily cognitive in nature, SCS symptoms span several affective, cognitive, physiological, and behavioral domains (Schuck et al., 2019). Several of these symptoms may have had a unique influence on some individuals’ experiences. For instance, social withdrawal in itself was a behavior encouraged by the lockdowns and restrictions; although implemented to encourage individuals to maintain safe distances from others to prevent the transmission of COVID-19, these disruptions to routine may have inadvertently exacerbated preexisting SCS symptoms and/or resulted in newfound desires to withdraw from others. The emphasis placed on citizens to stay at home may have also had similar influences on feelings of entrapment based on the physical entrapment encouraged by local ordinances. Accordingly, key behavioral changes in conjunction with public safety measures may have had larger influences on SCS symptoms than on suicidal ideation itself.
Second, differences in, and the replicability of, effects across countries are worth considering within the context of differences in pandemic-related restrictions, quarantines, and overall responses. Across the vast majority of behaviors and cognitions, significant interaction effects occurred most often in South Korea, the United States, Germany, and Poland. This suggests that not only did going outdoors, engaging in outdoor and social activities, and pandemic-related worries change drastically during the pandemic, but also individuals who reported more severe SCS symptoms during the present study exhibited the greatest changes in these symptoms. Consistent with previous research, this result indicated a high-behavioral-response pattern, in which preventive behavioral measures, including avoidance of public transportation and crowded places, were actively practiced by the general public (Lee & You, 2020). In comparison with several other countries, policies implemented by the South Korean government, for instance, consistently remained at a moderate level of stringency during the months in which our data collection occurred (Hale et al., 2021). Specifically, instead of nationwide lockdowns, the South Korean government implemented brief and strict social distancing policies that targeted high-risk clusters and locations, effectively lowering population mobility in high-density areas (Dighe et al., 2020).
Similar patterns in both outdoor and social activities, with significant interaction effects, were found in Germany, Poland, and the United States. Poland attempted to lift lockdown policies and gradually reopen its economies through the summer of 2020 (International Monetary Fund, 2021), although increased restrictions were reintroduced in response to the second wave of the pandemic in the fall of 2020. Likewise, Germany responded with a wide range of policies that fluctuated throughout the duration of the pandemic, with oscillating attempts to reopen and reconstrain the economy between late April and July (International Monetary Fund, 2021). In preparation for the emerging second wave of infection, the German government introduced tightened restricting measurements targeting regional areas with high near-term infection rate, accompanied by mild nationwide lockdown during the second half of 2020. Changes in behavioral mobility corresponded with government responses, as nationwide reductions of both recreational and business travels, as well as the use of public transportation, prompted the general decrease in mobility across the country (Anke et al., 2021). Finally, in the United States, trends in diminished outdoor and social behaviors were consistent with the stringent government responses toward the pandemic, at least in certain regions of the country. Indeed, previous studies conducted in the United States also discovered that the perceived risks of engaging in outdoors activities were significantly lower than the perceived risks of social gathering and indoor activities with a large crowd in older adults (Erchick et al., 2022) and families with preexisting conditions (Landry et al., 2021). Similarly, transportation data gathered from three major cities in the United States further suggested the contextual preference of behavioral responsiveness, in which pedestrian counts and transportation decreased significantly in urban areas and residential streets, whereas physical activities increased along outdoor and recreational trails during lockdown (Doubleday et al., 2021). In each of these countries, individuals whose routines were disrupted to a greater extent may have had increased SCS symptoms.
Interestingly, it is notable that minimal interaction effects were found in India or Turkey. Both countries were reported to have implemented stage-wise reopening measures prior to the beginning of the survey to support economic activities, which remained consistent during the time frame of data collection (International Monetary Fund, 2021). Moreover, in India, much of data collection took place when the prevalence of COVID-19 was relatively low. Despite regional containment measures, domestic traveling and off-line working were allowed in both countries. On-campus learning and the full reopening of entertainment and retail venues in Turkey, as well as restrictions lifting on public transportation, events, and gatherings in India, possibly contributed to the minimum changes in both cognitions and daily behaviors when compared with the other countries, which uniformly experienced tightened restrictions in response to the second wave of infections during our time of data collection. It is also possible that effect sizes were smaller in these countries, so the power to detect these effects, given our corrections to our familywise error rate, was limited. Future studies should explore these relationships regionally with larger and more representative samples.
Finally, it is worth commenting on the potential directionality of these associations: Did the severity of preexisting SCS or suicidal ideation exacerbate changes in behaviors and cognitions in response to pandemic-related disruptions and stressors, or did pandemic-related disruptions and stressors lead to increases in psychological distress and suicide-related symptoms? Although we have primarily hypothesized that disruptions to daily routines may have exacerbated mental health symptoms, it is also possible that individuals who were already experiencing SCS symptoms at the onset of the pandemic may have been disproportionately impacted by the drastic shifts in daily routines that were caused by mass quarantines and restrictions. Unfortunately, given the cross-sectional nature of the present study, in which changes in behaviors and cognitions were assessed retrospectively and SCS symptoms and suicidal ideation were assessed at a single time point, the temporal nature of these relationships cannot be determined. However, previous research has shown that both pathways are plausible. Individuals with poor mental health may have a heightened vulnerability to negative life events and stressors, including those prompted by the pandemic (Brooks et al., 2020). In particular, individuals with preexisting symptoms of SCS experience feelings of entrapment, ruminative thinking, hyperarousal, and social withdrawal (Galynker, 2017), all of which may have been intensified by the pandemic and subsequently placed them at greater risk for significant changes in cognitive and behavioral patterns. As noted previously, elevated levels of entrapment and social withdrawal may have increased feelings of confinement and isolation and discouraged social interactions during the pandemic (Brooks et al., 2020). Hyperarousal, which includes a sense of hypervigilance as defined by SCS, may have increased levels of pandemic-related anxiety among individuals with SCS and amplified their health concerns (Schuck et al., 2019). Similarly, ruminative thinking may further encourage excessive worries about health and financial situations, as well as general fear regarding COVID-19. Thus, it is possible that the presence of SCS and/or suicidal ideation may have exacerbated behavioral and cognitive changes during the pandemic.
On the other hand, it has also been shown that quarantines and stay-at-home orders in response to the pandemic may elicit a range of psychological symptoms, including anxiety, posttraumatic stress, loneliness, and depression (Brooks et al., 2020). Pandemic-related stressors, such as financial strains and health concerns, have also been linked to elevated feelings of fear, worrisome thoughts, and emotional distress (Myers, 2000; Satici et al., 2022). In addition to negative psychological responses, it has also been shown that individuals may experience behavioral changes, such as more time spent at home and increased social isolation, following the implementation of lockdowns (S. Zhu et al., 2020). These mental health symptoms and behavioral patterns may also serve as risk factors for the development of suicidal ideation and/or SCS symptoms. Thus, it is equally plausible that pandemic-related disruptions may aggravate mental health symptoms and increase the risk for suicidal thoughts and behaviors. Longitudinal studies are needed to elucidate these associations further.
Limitations and future directions
As with any other study, the present study had several limitations that should be considered when interpreting these findings. First and foremost, as discussed previously, this study’s cross-sectional design, which relied on retrospective recall of pandemic-related changes in behaviors and cognitions and concurrent reports of suicidal ideation and SCS symptoms, limited our ability to understand the temporal nature of these relationships. This is of particular importance given the documented impacts of retrospective recall biases attributable to depressed mood (Clark & Teasdale, 1982; Kihlstrom et al., 2000), as well as suicidal ideation itself (see Chu et al., 2016), states of pain (Eich et al., 1985), and other cognitive heuristics (Bradburn et al., 1987) that may have been present during assessments. Longitudinal assessment of suicidal ideation and SCS symptoms, as well as repeated assessment of behaviors and cognitions during the pandemic, would have been preferable in understanding the trajectories of these changes and symptoms over time. Likewise, we did not collect information regarding days of quarantine or any proxies for lockdowns experienced by participants, which may have been a confounding variable impacting our results.
Third, convenience sampling was used across countries, and recruitment strategies differed by country. This limited the representativeness and comparability of the samples cross-nationally, as well as the potential generalizability of these findings. Similarly, participants in many countries self-identified as female and were highly educated; replication and extension of these findings in more diverse samples cross-culturally, cross-nationally, and of varying socioeconomic statuses is needed to understand the extent to which these findings may be generalizable to underrepresented groups. Additionally, race/ethnicity information was not collected in India or Turkey. Fifth, it is possible that some participants may have concealed relevant mental health symptoms; in particular, previous research has indicated that a significant proportion of individuals choose not to disclose suicidal ideation when it is present, especially in cultures in which suicide is more stigmatized (Drum et al., 2009; Eskin et al., 2015).
Sixth, although forward and back translations of the study battery were conducted, alongside consensus meetings to resolve disagreements, the resultant translations were not pilot tested in a monolingual sample prior to the onset of data collection. Seventh, although cutoff scores for SCS were established in a U.S. patient sample (Bloch-Elkouby et al., 2021), these cutoff scores may not be optimal cross-nationally. Thus, future research should examine the psychometric properties, validation, and predictive utility of the SCI-2—and SCS more broadly—across different countries and cultures to better understand its specific presentations worldwide. Finally, the data analyzed in this study were not missing completely at random, suggesting that there may have been biases associated with the patterns of missing data when using listwise deletion. Attenuating this limitation somewhat, sensitivity analyses using multiple imputation resulted in nearly identical estimates and statistical significance tests in our primary analyses, which used listwise deletion. However, we could not calculate estimated marginal means and slopes for multiple-imputation analyses because of computational challenges and demands associated with combining cumulative link mixed models and multiply imputed data—leading to our decision to retain listwise-deletion estimates in this study. This decision should be taken into account when interpreting our findings.
Conclusion
Despite these limitations, the present study provided evidence that changes in behaviors and cognitions in response to disruptions to daily routines and significant stressors, such as the COVID-19 pandemic, may be associated with increased risk of suicide-related symptoms, including suicidal ideation and SCS. Future research should examine the temporality (and potential bidirectional associations) of these effects, as well as replicate and extend these findings in more diverse samples to better understand the pernicious relationship between routine disruption and suicide risk.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026221148732 – Supplemental material for Changes in Daily Behaviors and Cognitions During the COVID-19 Pandemic: Associations With Suicide Crisis Syndrome and Suicidal Ideation
Supplemental material, sj-docx-1-cpx-10.1177_21677026221148732 for Changes in Daily Behaviors and Cognitions During the COVID-19 Pandemic: Associations With Suicide Crisis Syndrome and Suicidal Ideation by Megan L. Rogers, Erjia Cao, Jenelle A. Richards, Alexis Mitelman, Shira Barzilay, Yarden Blum, Ksenia Chistopolskaya, Elif Çinka, Manuela Dudeck, M. Ishrat Husain, Fatma Kantas Yilmaz, Oskar Kuśmirek, Jhoanne M. Luiz, Vikas Menon, Evgeni L. Nikolaev, Barbara Pilecka, Larissa Titze, Samira S. Valvassori, Sungeun You and Igor Galynker in Clinical Psychological Science
Footnotes
Acknowledgements
Site principal investigators and staff are listed in alphabetical order in the byline and made equal contributions to this article. We thank Gizem Akülker, Rabia Bilici, and Basşak Ünübol for assisting with data collection in Turkey.
Transparency
Action Editor: Kelsie T. Forbush
Editor: Jennifer L. Tackett
Author Contributions
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.