
Abstract
Clinical high risk for psychosis (CHR) is a transdiagnostic risk state. However, it is unclear how risk states such as CHR fit within broad transdiagnostic models such as the Hierarchical Taxonomy of Psychopathology (HiTOP). In this study, a hierarchical dimensional symptom structure was defined by unfolding factor analysis of self-report data from 3,460 young adults (mean age = 20.3 years). A subsample (n = 436) completed clinical interviews, 85 of whom met CHR criteria. Regression models examined relationships between symptom dimensions, CHR status, and clinician-rated symptoms. CHR status was best explained by a reality-distortion dimension, with contributions from internalizing dimensions. Positive and negative attenuated psychotic symptoms were best explained by multiple psychotic and nonpsychotic symptom dimensions, including reality distortion, distress, fear, detachment, and mania. Attenuated psychotic symptoms are a complex presenting problem warranting comprehensive assessment. HiTOP can provide both diagnostic precision and broad transdiagnostic coverage, making it a valuable resource for use with at-risk individuals.
Keywords
Tens of millions of people worldwide—0.5% to 1% of the global population—live with schizophrenia, a serious mental illness characterized by positive symptoms (e.g., delusions, hallucinations, paranoia) and negative symptoms (e.g., loss of motivation, blunted emotional expression, social withdrawal; American Psychiatric Association, 2013). Schizophrenia and related psychotic disorders tend to manifest in young adulthood and cause chronic and severe functional impairment. In fact, schizophrenia’s global disease burden is the third largest of any mental illness in terms of years lived with disability (behind only major depressive disorder and anxiety disorders; Vos et al., 2015). Because of their early incidence and chronic course, psychotic disorders are prime targets for early identification and intervention. Psychotic disorders are often preceded by a prodromal stage marked by subclinical or attenuated psychotic symptoms. Early identification strategies largely focus on detecting these attenuated symptoms (e.g., perplexed mood, suspiciousness, transient or unformed perceptual abnormalities) in youths who do not currently have a diagnosable psychotic disorder (Fusar-Poli et al., 2013). Youths meet criteria for a clinical high risk (CHR) for psychosis syndrome if they exhibit attenuated psychotic symptoms; brief, intermittent frank psychotic symptoms; and/or genetic risk and functional decline (Fusar-Poli et al., 2016; Miller et al., 1999; Yung et al., 2005). 1 A determination of CHR status is primarily based on attenuated positive symptoms of psychosis, although attenuated negative symptoms are also commonly observed in CHR (Strauss et al., 2020). Individuals meeting CHR criteria have greatly elevated risk for psychotic disorders, and roughly 25% develop a psychotic disorder within 2 years of identification (Fusar-Poli et al., 2013).
The CHR syndrome is a heterogeneous and transdiagnostic group. This syndrome confers risk for various psychotic diagnoses (e.g., schizophrenia, delusional disorder, mood disorder with psychotic features), indicating that it reflects risk for a broad psychosis spectrum rather than a specific psychotic disorder. Moreover, most individuals meeting CHR criteria also meet criteria for at least one nonpsychotic psychiatric diagnosis—typically mood, anxiety, or substance use disorders (Addington et al., 2017; Albert et al., 2018; Fusar-Poli et al., 2014; Lim et al., 2015; Salokangas et al., 2012), although personality disorders are also common (Boldrini et al., 2019). Finally, individuals who meet CHR criteria but do not go on to develop psychotic disorders (“nonconverters”) experience high rates of nonpsychotic disorders causing cognitive and functional impairment (Addington et al., 2017). Psychosis risk—operationalized by the CHR syndrome—is evidently heterogeneous and transdiagnostic. It is therefore important to have accurate and efficient models for understanding the co-occurrence of psychotic and nonpsychotic symptoms in this at-risk population.
There are two broad approaches to integrating disparate psychiatric symptoms. One approach is represented by the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013) and its predecessors, in which symptoms have been clustered into psychiatric disorders using a mixture of research, clinical observation, and expert consensus. Note that DSM disorders have tended to evolve independently of one another, which has led to disorders co-occurring and sharing overlapping symptoms. Within DSM disorders, it is also often the case the symptoms are heterogeneous and individuals with the same disorder have dissimilar clinical presentations (e.g., representing subgroups). This is certainly the case in schizophrenia, which has long been recognized as a heterogeneous disorder with many possible presentations (Andreasen, 1993).
Increasingly, researchers have used more quantitatively driven approaches, in which co-occurring symptoms are thought to reflect underlying psychopathology dimensions that cut across DSM disorders. Because transdiagnostic assessment typically measures psychiatric symptoms quantitatively, latent dimensions can be defined at various levels of analysis—from broad psychopathology spectra (e.g., psychosis) to specific symptom clusters (e.g., paranoia). Increasingly, momentum is building toward organizing these latent dimensional constructs in the Hierarchical Taxonomy of Psychopathology (HiTOP; Kotov et al., 2017, 2021). HiTOP proposes a nested hierarchy of transdiagnostic symptom factors, with comorbidity explained by variation in higher-order psychopathology dimensions (e.g., internalizing) that manifest across multiple lower-order dimensions (e.g., social anxiety and panic-like symptoms; Kotov et al., 2021).
In CHR samples, comorbid symptoms have traditionally been modeled through DSM categorical diagnoses (e.g., Addington et al., 2017; Fusar-Poli et al., 2014). More recently, clinical-staging studies have suggested that transdiagnostic factors play important roles in psychosis risk (Addington et al., 2019; McGorry et al., 2018). We recently conducted a small pilot study to investigate symptoms in a CHR sample through quantitative transdiagnostic factors (Cowan & Mittal, 2021). That study identified several transdiagnostic dimensions cutting across symptom categories and showed that depression and hypomania were relevant for multiple dimensions. However, that study was a case-control study of 71 CHR and 73 healthy comparison youths, which constrained analyses to a simple latent variable model (exploratory factor analysis of scale means). The CHR syndrome is rare in the general population, and CHR sample sizes tend to be relatively small as a result (Addington et al., 2008). However, psychosis occurs on a continuum with normative experience (DeRosse & Karlsgodt, 2015; Johns & van Os, 2001; Nelson et al., 2013). When this is the case, large population-based structural studies can address some limitations of traditional case-control studies (Kotov et al., 2022; Preacher et al., 2005). Specifically, if a CHR sample is drawn from a large, representative reference group of demographically matched youths, more complex hierarchical structures can be defined by item-level analyses in the reference group and then applied in the CHR sample.
As evidence accumulates for transdiagnostic models of psychosis risk, there are considerable advantages to analyzing CHR-symptom data from a transdiagnostic and hierarchical perspective. First, a hierarchical transdiagnostic approach allows new evidence from hard-to-reach CHR samples to be integrated into the larger picture of psychiatric comorbidity. Second, this approach can determine which transdiagnostic dimensions at which levels of analysis are most important for understanding psychosis risk. A hierarchical, transdiagnostic model of CHR symptoms can then guide research or clinical decision-making, for example in how broadly versus specifically to assess various symptoms. Third, this approach can determine whether nonpsychotic symptoms directly contribute to psychosis risk. For instance, outcomes in the CHR syndrome (e.g., conversion to a psychotic disorder) might relate only to psychotic symptom dimensions (and not nonpsychotic symptom dimensions). This would imply that nonpsychotic symptoms—although important for individuals’ functioning and well being—are co-occurring problems unrelated to psychosis risk. By contrast, if outcomes relate to psychotic and nonpsychotic dimensions, this would suggest that nonpsychotic symptoms directly contribute to psychosis risk.
In the current study, we examined the transdiagnostic phenotypic profile of CHR symptoms in a hierarchical-dimensional framework. A hierarchical-dimensional structure was established using self-report measures of psychotic and nonpsychotic symptoms in a large sample of community youths (N = 3,460). Nonpsychotic symptoms included various categories that have been shown to be relevant for psychosis risk, including internalizing (Fusar-Poli et al., 2014), mania (Correll et al., 2007), dissociation (Gibson et al., 2019; Williams et al., 2018), and substance use (Addington et al., 2017). Relationships were then examined between symptom dimensions and key psychosis risk variables (CHR status, attenuated positive symptoms, and attenuated negative symptoms) assessed in clinical interviews with a subset of participants (n = 436; 85 of whom met CHR criteria). These data-driven analyses addressed three research questions. First, what is the best level of specificity in the dimensional hierarchy to explain each psychosis risk variable? Second, at that level of specificity, which symptom dimensions relate to each psychosis risk variable? Third, do nonpsychotic symptom dimensions directly contribute to psychosis risk variables, indicated by incremental variance explained above and beyond the effect of psychotic symptom dimensions? We hypothesized that more fine-grained levels of the symptom hierarchy would explain more variance in interview-rated psychosis-risk variables and that both psychotic and nonpsychotic symptom dimensions would relate to attenuated psychotic symptoms.
Transparency and Openness
Preregistration
This study’s analyses were not preregistered and are clearly labeled as exploratory.
Data, materials, code, and online resources
Study data are uploaded periodically to a publicly accessible data repository, following the data-sharing plan approved by all study sites’ institutional review boards, to which all participants consented. Data can be accessed at https://nda.nih.gov/edit_collection.html?id=2783. Study materials are commonly used and include easily accessed questionnaires and clinical interviews. Study analysis code is available online and can be accessed at https://github.com/hrcowan/HiTOP-MAP.
Reporting
We report how we determined our sample size, all data exclusions, all manipulations, and all measures in the study.
Ethical approval
The study protocol was approved by institutional review boards at all study sites. Participants gave written informed consent, including consent to the data-sharing plan included in the protocol. The study was carried out in accordance with the World Medical Association Declaration of Helsinki, as amended in 2013. The study protocol was made publicly available before data collection (Ellman et al., 2020).
Method
Participants
The reference sample comprised 3,460 community youths who took part in the Multi-Site Assessment of Psychosis-Risk Study (for full study details, see Ellman et al., 2020). Participants were recruited from several large metropolitan areas in the eastern and midwestern United States. Eligibility requirements were age 16 to 30, English proficiency to complete online questionnaires, and normal or corrected-normal vision. Participants were not excluded on any clinical or demographic characteristics. All participants completed an online questionnaire battery including demographic variables and measures of psychotic-like experiences, depression, anxiety, mania, dissociation, and substance use. A subsample of 439 individuals drawn from the reference sample attended an in-person clinical interview (see Fig. 1). Three of these participants were excluded (see below), leaving an effective interview sample size of 436. Demographic characteristics of the reference sample and interview subsample are shown in Table 1. Sample size was determined by estimating population prevalence of CHR using pilot data and prior population estimates (van Os et al., 2009) to obtain sufficient participants meeting CHR criteria for all planned analyses (for full details, see Ellman et al., 2020).
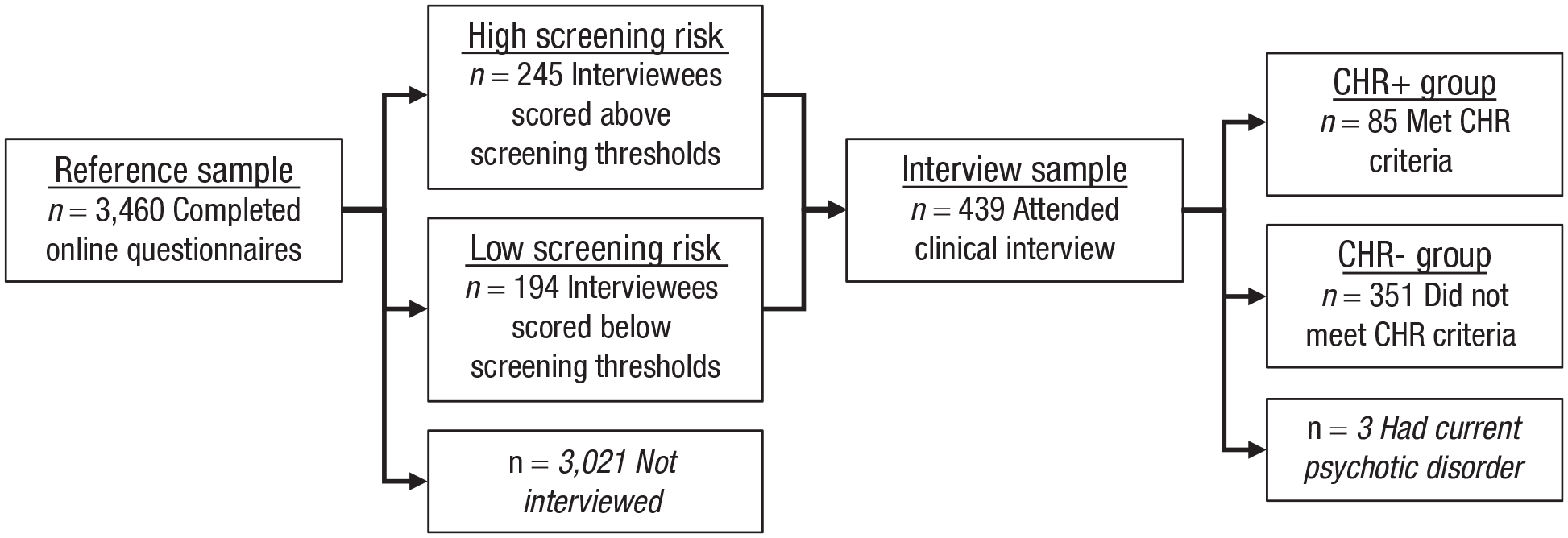
Study flowchart. See Table 1 for participant characteristics in the reference sample and interview sample.
Participant Characteristics
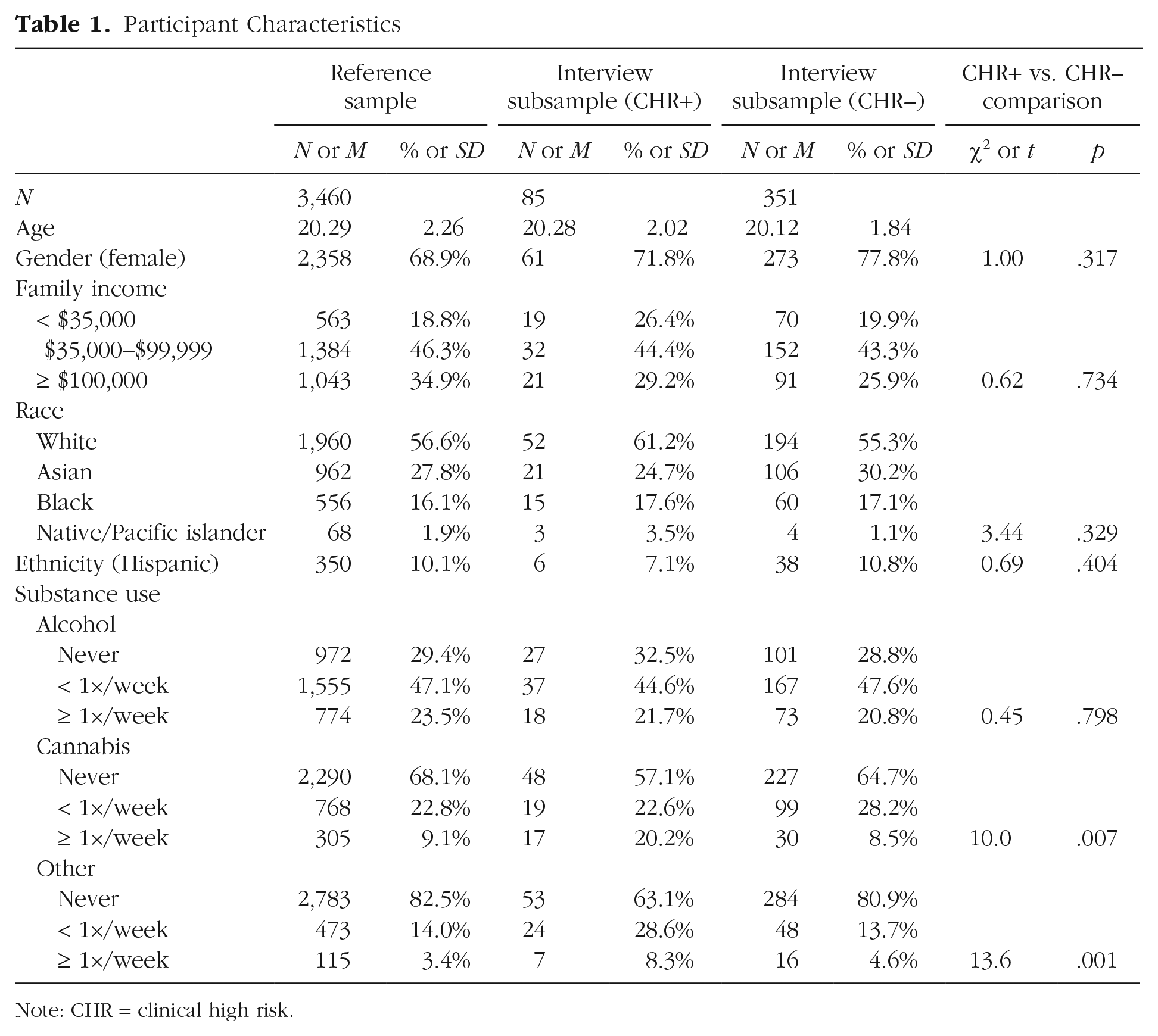
Note: CHR = clinical high risk.
Procedures
As shown in Figure 1, participants in the reference sample completed online questionnaires assessing multiple forms of psychotic and nonpsychotic psychopathology. An interview subsample was then drawn from the reference sample. The sampling strategy was designed to produce a fully dimensional sample enriched for psychosis risk. All individuals who scored above established screening thresholds on two measures of psychotic-like experiences were invited to participate in interviews (high screening risk, n = 245). Thresholds were eight or more items on the Prodromal Questionnaire (PQ; Loewy et al., 2005) rated as “distressing” (Gibson et al., 2014; Loewy et al., 2005, 2007) or two or more PRIME screen items rated as “somewhat” or “definitely” agree (Kline et al., 2012). See “Measures” below for details of these questionnaires. To obtain a fully dimensional interview subsample, randomly selected individuals scoring below screening thresholds were also invited to participate in interviews (low screening risk, n = 194). Clinical interviews assessed CHR status and positive and negative attenuated psychosis symptoms (see “Measures” below). Individuals who met criteria for a current psychotic disorder at the time of the interview (n = 3) were excluded from analysis of interview data, leaving an effective interview sample size of 436 participants.
Measures
All participants completed questionnaires, including measures of psychotic-like experiences, depression, anxiety, mania, dissociation, and substance use. Psychotic-like experiences were assessed by the PQ (Loewy et al., 2005), the PRIME screen (Kline et al., 2012), and the PROD screen (Heinimaa et al., 2003), three commonly used measures of psychosis risk. Depression was assessed by a shortened 14-item version of the Center for Epidemiological Studies-Depression Scale (Kohout et al., 1993), a measure of depression severity in the past week. Anxiety was assessed by a seven-item version of the State-Trait Anxiety Inventory—Trait Form (Bieling et al., 1998) that removes items overlapping with depression and the Social Phobia Scale (Mattick & Clarke, 1998), a 20-item measure of social anxiety. Mania was assessed by the General Behavior Inventory—Patient Version (Youngstrom et al., 2008), a 10-item measure of hypomanic or manic elevations in mood or behavior over the past year. Dissociation was assessed by an abbreviated 14-item version of the Dissociative Experiences Scale (DES; Bernstein & Putnam, 1986), with some items removed to decrease participant burden (primarily items related to rare dissociative identity disorder symptoms). Substance use was assessed by the Drug Use Frequency scale (O’Farrell et al., 2003), a measure of substance use frequency in the past 3 months.
Participants in the interview subsample completed two structured clinical interviews following the questionnaire administration. CHR status and positive-symptom severity were assessed by the Structured Interview for Psychosis-Risk Syndromes (SIPS; Miller et al., 1999), a clinician-rated interview that measures the severity of positive, negative, disorganized, and general symptoms and classifies participants who currently meet CHR syndrome criteria. CHR criteria are based on the presence of attenuated positive symptoms, brief intermittent psychotic symptoms, and/or genetic risk and recent functional decline.
Negative-symptom severity was assessed by the Prodromal Inventory of Negative Symptoms (PINS; Pelletier-Baldelli et al., 2017; Strauss et al., 2020). The PINS is a clinician-rated interview designed to assess negative symptoms in the CHR syndrome, including anhedonia, avolition, and asociality across social, role, and recreation domains, as well as blunted affect and alogia.
Data analysis
A series of exploratory factor analyses (EFAs) were performed on the items in the nine self-report scales (see “Measures” above) using an unfolding or “bass-ackwards” method (Goldberg, 2006). We computed a series of EFAs with 1, 2, . . ., k factors, where k was the largest number of factors for which (a) parallel analysis showed eigenvalues larger than those generated from random data and (b) all factors were identified with at least two items (i.e., at least two items loaded ≥ .30 on the factor). EFAs used minimum residual factoring and varimax rotation, producing orthogonal factors in each factor model. Orthogonal rotation is typical in unfolding analyses (e.g., Kim & Eaton, 2015) because it produces interpretable cross-level correlations between latent variables (Goldberg, 2006). The number of participants (N = 3,460) gave an adequate 17.0:1 subject:item ratio. These factor models represent increasingly complex data-driven dimensional transdiagnostic models that should theoretically approximate higher to lower levels of the HiTOP transdiagnostic hierarchy as the number of factors increases (superspectra → spectra → subfactors; Kotov et al., 2021). Regression-based factor scores were saved for all factors in all factor models. Pearson correlations between factor scores were examined to approximate relationships between factors at adjacent levels of the factor hierarchy. Missing data were infrequent (missing data < 6% for all items). Missing data were handled by pairwise deletion (factor analysis) and median imputation (regression-based factor scores). Simulations have shown that various methods of handling missing data perform similarly when sample size is large (n > 1,000) and when missing data rates are low (≈5%; Enders & Bandalos, 2001; Nassiri et al., 2018), as was the case in the current study.
To examine the placement of clinical variables in the dimensional symptom hierarchy, we calculated regression models with factor scores entered as independent variables and clinical variables (CHR status, positive symptoms, or negative symptoms) entered as dependent variables. Clinical variables were entered as means of symptom items. Continuous variables (positive and negative symptoms) were analyzed through linear regression. The categorical variable of CHR status was analyzed through logistic regression. For each clinical variable, a separate regression model was calculated for each level of the factor hierarchy (3 clinical variables × 10 factor levels = 30 total-regression models). To determine which factor level provided the best fit for each clinical variable, overall fit statistics were compared for regression models at various factor levels (adjusted R2 for linear regression models and McFadden R2 for logistic regression models), and improvements in model fit from one level to the next were examined through likelihood ratio tests. Best fit was defined as the most complex factor level that achieved a statistically significant improvement in model fit. We examined standardized regression coefficients in the best-fitting regression model to determine which symptom dimensions had independent associations with the clinical variable of interest. Finally, we also calculated linear regression models for CHR status (dummy coded as 0 = absent, 1 = present) to facilitate direct comparisons of adjusted R2 and coefficients between CHR status and positive/negative symptoms (these appear in Fig. S1 in the Supplemental Material available online).
Whereas an empirical approach to deriving symptom scores (e.g., EFA of symptom items) may be more precise, in research and clinical practice, the SIPS and PINS are commonly analyzed and interpreted as means or total scores. To be consistent with prior research and clinical practice in this area, in the present study, we analyzed scale means rather than latent variables for interview-rated symptoms.
Results
Preliminary analyses
Demographic variables for the reference sample and the interview subsample are shown in Table 1. Chi-squared tests and t tests found no significant differences in demographic variables between participants who met CHR criteria at the diagnostic interview (n = 85) and participants who did not (n = 351). As shown in Table 1, participants meeting CHR criteria were more likely to use cannabis and other nonalcohol substances (e.g., cocaine, hallucinogens).
Descriptive statistics for full-scale symptom scores are shown in Table S1 in the Supplemental Material. All symptoms were elevated in participants meeting CHR criteria (all ps < .019). Following conventional effect-size magnitudes (small: Cohen’s d < .50; medium: d = .50–.80, large: d > .80), effect sizes ranged from small (depression, drug use frequency, negative symptoms) to medium (state-trait anxiety, social anxiety, dissociation, mania, PROD screen) to large (PQ, PRIME screen, SIPS positive symptoms). Descriptive statistics by screening risk (high vs. low) and CHR status are shown in Table S2 in the Supplemental Material. High screening risk CHR– participants scored higher than low screening risk CHR– participants on all symptom measures. By contrast, CHR+ participants scored higher than high screening risk CHR– participants only on the PQ, PRIME, and SIPS positive but not on any other symptom measures.
Bivariate correlations between symptoms are shown in Table S3 in the Supplemental Material. All correlations were significant at p < .05 after false discovery rate correction except for several correlations between drug use frequency and other scales (PRIME screen, DES, and SIPS attenuated positive symptoms). The mean correlation between study variables was r = .360, suggesting a meaningful amount of shared variance.
Hierarchical symptom dimensions
Figure 2 shows the hierarchical-factor structure of the items in the self-report scales, with lines indicating Pearson correlations across factor levels. For models with one through 10 factors, parallel analysis indicated eigenvalues greater than chance, and all factors had at least two items loading .30 or higher. New factors introduced in the 11- and 12-factor solutions did not have two items loading .30 and higher; therefore, the hierarchical factor analysis was conducted for one through 10 factors. See Table 2 for the highest-loading items on each factor in the 10-factor solution; for the full item names of the highest-loading items at all levels of the factor hierarchy, see Tables S4.1 through S4.10 in the Supplemental Material; and for the item loadings of all items in the 10-factor solution, see Table S5 in the Supplemental Material.
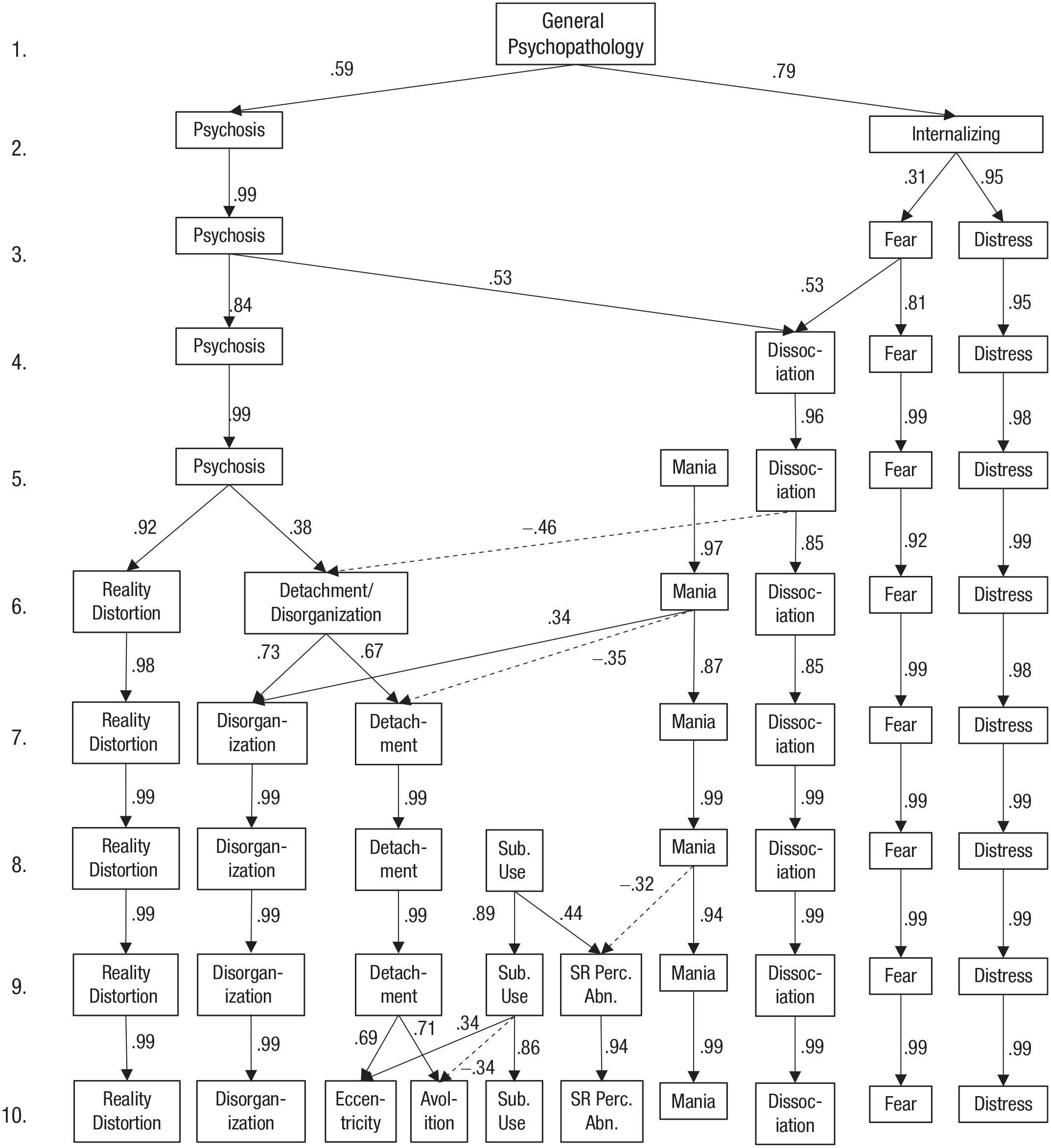
Hierarchy of self-reported symptom dimensions in the reference sample of 3,460 community young adults (mean age = 20.3 years). Factor analysis was performed for each number of factors (1–10) using varimax rotation. Arrows indicate cross-level correlations (Pearson correlations between estimated factor scores). Correlations r ≤ .30 are omitted for clarity. Sub. Use. = Substance use; SR Perc. Abn. = substance-related perceptual abnormalities.
Highest-Loading Items on Each Factor in the 10-Factor Solution: Abridged Item Names and Factor Loadings
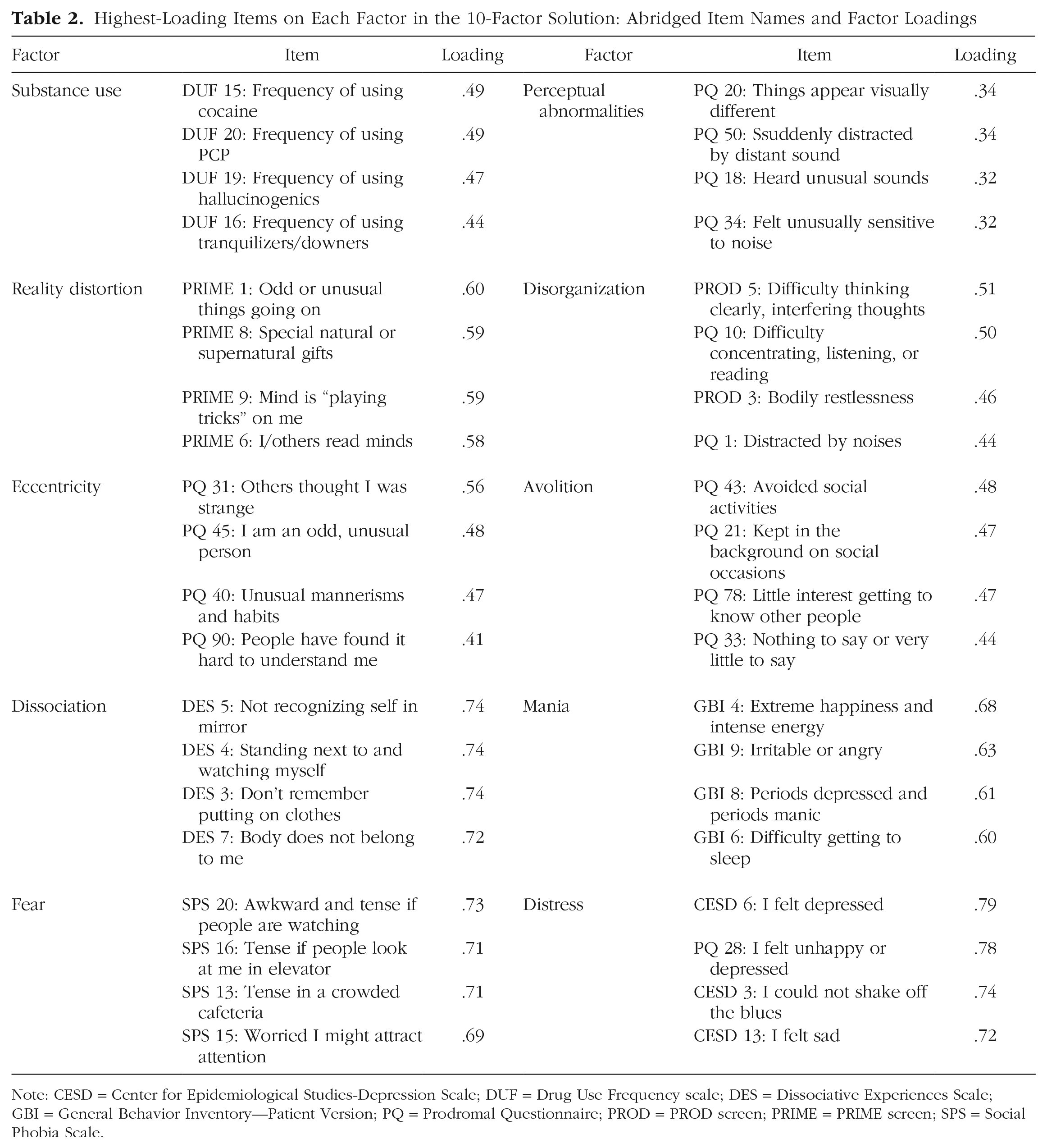
Note: CESD = Center for Epidemiological Studies-Depression Scale; DUF = Drug Use Frequency scale; DES = Dissociative Experiences Scale; GBI = General Behavior Inventory—Patient Version; PQ = Prodromal Questionnaire; PROD = PROD screen; PRIME = PRIME screen; SPS = Social Phobia Scale.
At Level 1, a single general-psychopathology dimension serves as a baseline for comparison. At Level 2, psychosis and internalizing dimensions split apart. From Levels 3 through 5, the structure of nonpsychotic symptoms differentiates into separate dimensions for dissociation, mania, fear, and distress, whereas psychosis remains a single dimension. Note that at Level 4, the new dissociation factor contains variance from both psychosis and fearful internalizing. From Levels 6 through 10, psychosis splits into progressively finer-grained dimensions, with substance use appearing at Level 8 and a substance-related perceptual-abnormalities factor appearing at Level 9.
Associations with psychosis risk variables
Figure 3a shows model fit for models with clinical variables (CHR status, positive- and negative-attenuated psychosis symptoms) entered as dependent variables and symptom dimensions for progressively more complex levels of the factor hierarchy (Factor Levels 1–10) entered as independent variables. 2 For all three clinical variables, model fit improved at more complex levels of the factor hierarchy. Overall model fit was best for positive symptoms (best-fitting model adjusted R2 = .405), followed by CHR status (best-fitting model McFadden R2 = .248) and then negative symptoms (best-fitting model adjusted R2 = .173). Overall F tests were significant in all regression models (p < .001).
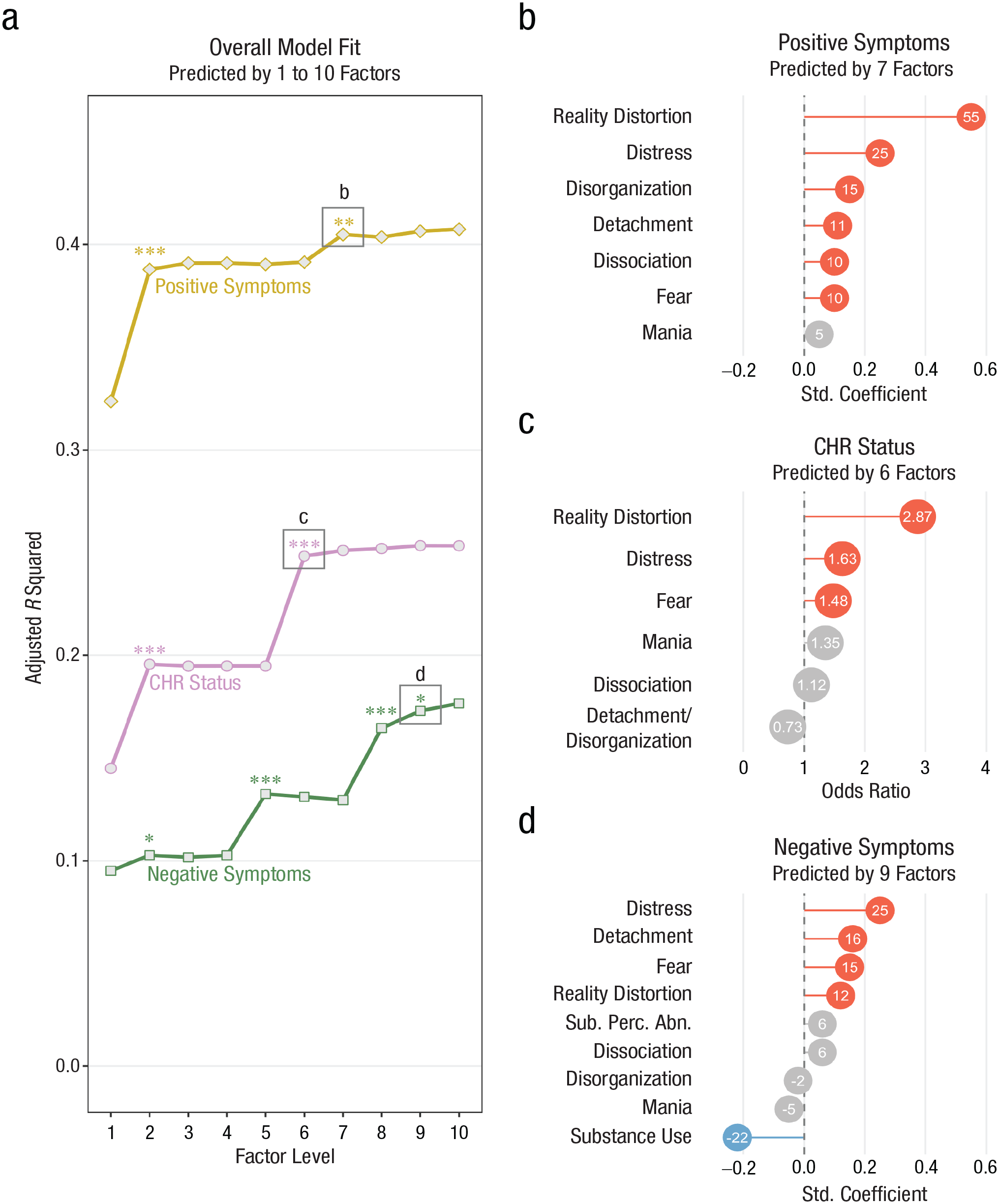
Associations between hierarchical transdiagnostic factors (see Fig. 2) and interview-rated psychosis risk variables (n = 436). (a) Overall fit of regression models with each psychosis risk variable entered as the dependent variable (clinical high risk [CHR] status, positive symptoms, and negative symptoms) at each level of the factor hierarchy. Note that model fit is expressed as adjusted R2 for linear regression models (positive and negative symptoms) and as McFadden R2 for logistic regression models (CHR status). All models were significant with p < .001 in all overall F tests. Significant improvements in model fit (F tests of residual sums of squares) are shown as *p < .05, **p < .01, ***p < .001. (b–d) Standardized regression coefficients or odds ratios from the most complex regression models that achieved a significant increase in model fit. Red indicates a positive coefficient (p < .05), blue indicates a negative coefficient (p < .05), and gray indicates a nonsignificant coefficient (p ≥ .05). Decimal points are omitted from linear regression coefficients for clarity. Sub. perc. abn. = substance-related perceptual abnormalities.
CHR status
As shown in Figure 3a, model fit for CHR status significantly improved when internalizing split from psychosis (moving from Level 1 to Level 2 in the factor hierarchy) and then improved again when psychosis split into separate dimensions for reality distortion and detachment/disorganization (Level 6). There were no further improvements in model fit at more complex levels of the hierarchy.
Odds ratios (ORs) from the best-fitting model for CHR status (Level 6) are shown in Figure 3c. CHR status was primarily associated with reality distortion (OR = 2.87, p < .001) and somewhat associated with distress (OR = 1.63, p = .006) and fear (OR = 1.48, p = .030). CHR status was not associated with mania, dissociation, or detachment/disorganization.
Attenuated positive symptoms
As shown in Figure 3a, model fit for attenuated positive symptoms significantly improved when internalizing split from psychosis at factor Level 2 and when disorganization split from detachment at Level 7.
Standardized regression coefficients from the best-fitting model for positive symptoms (Level 7) are shown in Figure 3b. Positive symptoms were most associated with reality distortion (β = 0.554, p < .001), followed by distress (β = 0.251, p < .001), disorganization (β = 0.149, p < .001), detachment (β = 0.108, p = .005), dissociation (β = 0.105, p = .006), and fear (β = 0.104, p = .007. The only factors unrelated to positive symptoms were mania and substance use.
Note that model fit predicting positive symptoms improved marginally from Level 8 to Level 9 when a substance-related perceptual abnormalities factor emerged, ∆ sum of squares = .039, F(1, 414) = 3.02, p = .083. Given this marginal improvement and the theoretical relevance of perceptual abnormalities in characterizing attenuated positive symptoms, we also examined the nine-factor model for positive symptoms. As shown in Figure S2 in the Supplemental Material, results largely resembled the seven-factor model with the addition of a significant coefficient for substance-related perceptual abnormalities (β = 0.151, p < .001) and a nonsignificant coefficient for substance use (β = 0.032, p = .406).
Attenuated negative symptoms
As shown in Figure 3d, model fit for attenuated negative symptoms significantly improved when internalizing split from psychosis at factor Level 2, when mania appeared at Level 5, when substance use appeared at Level 8, and when substance-related perceptual abnormalities split from substance use at Level 9. Note that some improvements in model fit were driven by negative coefficients from mania and substance use. The improvement in model fit at Level 5 coincided with a negative coefficient for mania (β = −0.128, p = .006), whereas the improvement in model fit at Level 8 coincided with a negative coefficient for substance use (β = −0.186, p < .001). Note that the coefficient for mania is no longer significant in the nine-factor model shown in Figure 3d. This coefficient decreased in magnitude and became nonsignificant at lower levels of the factor hierarchy as psychotic symptom clusters absorbed some of the variance in the mania dimension (as shown in Fig. 2).
Standardized regression coefficients from the best-fitting model for negative symptoms (Level 9) are shown in Figure 3d. Negative symptoms were most associated with distress (β = 0.249, p < .001), followed by detachment (β = 0.163, p < .001), fear (β = 0.145, p = .001), and reality distortion (β = 0.115, p = .011). Negative symptoms were inversely associated with substance use (β = −0.224, p < .001) and were not associated with substance-related perceptual abnormalities, dissociation, disorganization, or mania.
Discussion
Consistent with previous findings (Cowan & Mittal, 2021), this new sample of CHR youths reported broad psychopathology across every measured symptom category. A hierarchical unfolding factor analysis modeled this complex comorbidity picture by defining data-driven symptom dimensions at multiple levels of analysis. Ten progressively finer-grained factors unfolded in the data, from general psychopathological distress to specific symptom clusters for various kinds of psychotic and nonpsychotic psychopathology. This analysis revealed complex relationships between different kinds of symptoms in a large sample of community youths—showing, for example, that dissociation, mania, and substance use each related to different aspects of psychosis. Moreover, the symptom dimensions provided the framework for a transdiagnostic phenotypic profile of CHR symptoms that supplied important insights into characterizing attenuated psychotic symptoms, differentiating attenuated psychotic symptoms from mood symptoms, integrating psychosis risk symptom data into current theoretical models of psychopathology, improving the efficiency of psychosis risk assessment, and enhancing step-based care for individuals meeting CHR criteria.
A transdiagnostic perspective on attenuated positive symptoms and CHR status
Clinician-rated attenuated positive symptoms were related to all psychotic and internalizing dimensions in the seven-factor model. Note that distressed internalizing accounted for the second-most variance after reality distortion, implicating distress as a factor directly affecting attenuated positive psychotic symptoms. Transdiagnostic dimensions also provided a new perspective on attenuated negative symptoms, which are consistently shown to predict transition to psychosis in CHR samples (Alderman et al., 2015; Cowan & Mittal, 2021; Metzler et al., 2016; Oliver et al., 2020; Piskulic et al., 2012). Negative symptoms were most related to internalizing dimensions (distress and fear), psychotic dimensions (detachment and reality distortion), and the absence of substance use. Substance use may have been less likely to co-occur with negative symptoms because of the social context of substance use. Youths’ substance use primarily occurs in groups of socially motivated peers (Dumas et al., 2020; Kuntsche et al., 2005). Youths experiencing significant negative symptoms would be less likely to participate in these social-group contexts, possibly resulting in less access and/or less social motivation to use substances.
Internalizing and negative symptoms are not easily distinguishable in the early clinical stages of risk for serious mental illness (Addington et al., 2019; Azar et al., 2018; Cowan et al., 2019; Cowan & Mittal, 2021). This study identified distinct self-reported symptom factors for distressed internalizing and detachment, providing an inroad into differentiating these symptoms in CHR samples (although, see “Measurement Approach” below for a discussion of potential limits on self-report of negative symptoms). Note that these findings suggest that differential diagnosis of internalizing symptoms versus negative symptoms can be improved using the explanatory power of symptoms that are unlikely to co-occur with attenuated negative symptoms (i.e., mania and substance use). If individuals experiencing mania or substance use are less likely to experience negative symptoms, then it is more likely that any affective or volitional disturbances in these individuals would be better explained by internalizing symptoms rather than negative symptoms. Speculatively, this argument suggests that it may be possible to identify transdiagnostic risk profiles within the CHR syndrome. Individuals presenting with positive symptoms, hypomania, and/or substance use may be at risk for affective or stress-reactive psychosis (Myin-Germeys & van Os, 2007), whereas individuals presenting with positive and negative symptoms may be at risk for anhedonic or deficit-syndrome psychosis (Kirkpatrick & Buchanan, 1990).
Regarding CHR status, comorbidity patterns were not obvious when symptoms were modeled as questionnaire mean scores (see Tables S1 and S2 in the Supplemental Material). CHR+ participants scored higher than CHR– participants on all symptom measures. When screening risk was taken into account, CHR+ participants scored higher than high screening risk CHR– participants on only a few measures tapping positive symptoms (PQ, PRIME, and SIPS positive). However, when symptoms were modeled through latent transdiagnostic dimensions, clear and specific associations emerged between CHR status and internalizing symptoms.
In the prevailing structured clinical interviews for detecting psychosis risk syndromes (Miller et al., 1999; Yung et al., 2005), CHR status is largely determined by the presence of positive symptoms. Genetic, neuropsychological, social, and environmental evidence support a fully dimensional model of psychosis in which a single psychosis continuum spans the entire general population, with severity of psychotic-like experiences differentiating normative experience from attenuated psychotic symptoms and clinical psychotic symptoms (Cowan & Mittal, 2020; DeRosse & Karlsgodt, 2015; Johns & van Os, 2001; Nelson et al., 2013). A determination of CHR status is, in a sense, a decision about where a given individual falls in the population distribution of positive psychotic-like experiences. In other words, CHR status can be seen as a dichotomization of a continuous variable. Dichotomous variables tend to be less precise and less statistically powerful than continuous variables, which may explain the weaker observed effects for CHR status in the present study.
Given the current diagnostic criteria for CHR status, which do not include attenuated negative symptoms, attenuated positive symptom severity is probably the best dimensional indicator of CHR symptoms. The current study showed that attenuated positive symptom severity was a transdiagnostic factor linked to various psychotic and nonpsychotic self-reported symptom dimensions. If future diagnostic criteria for CHR status were to include negative symptoms, then an appropriately weighted composite of standardized positive and negative symptom severity would be a more appropriate choice for a dimensional indicator of CHR symptoms.
Insights for transdiagnostic models
The symptom dimensions identified in this study provide further information on the placement of dissociation, mania, substance use, perceptual abnormalities, and disorganization in HiTOP.
Dissociation
Although transdiagnostic evidence on dissociative symptoms is limited (Kotov et al., 2021), these symptoms have been linked to internalizing, externalizing, and psychosis (Ellickson-Larew et al., 2020). In HiTOP, dissociation has been provisionally grouped with the thought-disorder subfactor of psychosis pending further structural evidence (Kotov et al., 2020). In the present study, dissociation bridged fearful internalizing and psychosis factors, providing further evidence for dissociation’s relevance across HiTOP superspectra. Furthermore, dissociation related to positive symptoms but not negative symptoms, indicated by two pieces of evidence. First, dissociation positively correlated with the higher-order psychosis factor and negatively correlated with the lower-order detachment/disorganization factor. Second, dissociation had a small independent relationship with interview-rated positive symptoms (Fig. 2b). These findings are consistent with prior empirical work (Longden et al., 2020) and reinforce dissociation’s links to the HiTOP thought-disorder subfactor (Kotov et al., 2020). In sum, the current findings support dissociation’s placement as a transdiagnostic factor associated with multiple psychopathology spectra while also reinforcing dissociation’s links to positive psychotic symptoms within the psychosis spectrum.
Mania
Mania is another dimension whose placement in transdiagnostic models is not yet settled. Mania has been linked to both the internalizing and psychosis spectra, and several placements have been proposed relative to these two spectra. Mania may fit within internalizing or psychosis, blend elements of both, or form its own independent dimension (Kotov et al., 2020, 2021). Building on known relationships between mania and psychosis, we found in our previous study in a smaller CHR sample that hypomania linked to more positive symptoms but less negative symptoms (Cowan & Mittal, 2021). Because the hierarchical model in the current study was defined using a community sample, the mania dimension likely captures hypomania more than true manic symptoms. This mania dimension appeared as an independent factor in the unfolding factor analysis, not splitting off from psychosis or internalizing. It also had a positive cross-level correlation with disorganization and negative cross-level correlations with detachment and substance-related perceptual abnormalities. Mania’s negative association with detachment is noteworthy because mania was also associated with lower levels of attenuated negative symptoms in the clinical interview (see “Attenuated Negative Symptoms” above). In sum, in the current study, hypomania appeared to be an independent dimension that co-occurred with higher levels of disorganization and lower levels of detachment.
Substance use and perceptual abnormalities
A substance-related perceptual abnormalities factor appeared with a cross-level correlation with substance use and items cross-loading from reality distortion. The substances with highest loadings on the substance use factor included PCP and hallucinogens (see Table 2), whose active effects include perceptual abnormalities. The substance-related perceptual abnormalities factor had highest loading items from the PQ, which asks participants not to include experiences while using alcohol or substances (Loewy et al., 2005). However, many participants may not read and follow survey instructions (Oppenheimer et al., 2009; Ramsey et al., 2016), and some participants in the current study likely included perceptual abnormalities experienced while intoxicated. Nevertheless, substance-related perceptual abnormalities also had an independent positive relationship with interview-rated attenuated positive symptoms (β = 0.151, p < .001) in the nine-factor positive-symptoms model (see Fig. S2 in the Supplemental Material). SIPS interviewers are trained not to rate perceptual abnormalities experienced while intoxicated, so there may in fact be an empirical association between substance-related perceptual abnormalities and overall attenuated positive symptoms. Future studies that can fully disambiguate perceptual abnormalities experienced while using versus not using substances would be valuable to explore this relationship in more detail.
In addition, there were other potential links between substance use and CHR symptoms. Individuals meeting CHR criteria were more likely to use nonalcohol substances (although note that the majority—57% for cannabis and 63% for other substances—reported never using these substances). This is in line with research showing high rates of substance use in CHR samples and suggesting substance use as a risk factor for conversion to a psychotic disorder (Addington et al., 2014). Externalizing psychopathology more broadly—which includes disordered substance use (Kotov et al., 2021)—also appears to be a risk factor for future psychotic disorders (Gin et al., 2021). Despite the elevated levels of substance use observed in the current study’s CHR sample, substance use was associated with lower levels of interview-rated negative symptoms and also differentiated lower-order detachment symptoms (eccentricity vs. avolition). Speculatively, this pattern of evidence suggests that substance use may differentiate two subgroups within the CHR syndrome: one subgroup with higher levels of substance use, more perceptual abnormalities, more eccentricity, and a less severe negative-symptom profile and another subgroup with lower levels of substance use, fewer perceptual abnormalities, and a more severe negative-symptom profile marked by asociality and avolition. In future studies, subgroup analyses within CHR samples could explore this possibility.
Disorganization
The factor we labeled Disorganization included items tapping into distractibility and inattention. We chose to label this factor Disorganization rather than “inattention” to recognize its placement in relation to the broad psychosis factor and the detachment factor. However, this factor was only a minor contributor to clinician-rated psychosis risk variables, relating to attenuated positive symptoms (β = 0.149, p < .001) but not CHR status or attenuated negative symptoms. Further research is warranted on the potential for self-report scales to detect subclinical disorganization symptoms.
Practical and theoretical implications
Practically, a transdiagnostic model of psychosis risk can potentially save time and effort by making assessment more efficient in two ways. First, rather than independently assessing for each categorical diagnosis, a researcher or clinician can assess a single dimension that captures the overlapping features of these diagnoses. For instance, the current study showed that the distress dimension related to both positive and negative symptoms. Various DSM-5 (American Psychiatric Association, 2013) diagnoses are consistent with a high loading on distress, including major depressive disorder, persistent depressive disorder, generalized anxiety disorder, posttraumatic stress disorder, insomnia disorder, borderline personality disorder, and probably bipolar disorder (Kotov et al., 2021). Rather than assessing all DSM-5 categorical diagnoses, researchers may be able to focus on a handful of dimensions. Second, clinicians and researchers can take advantage of the hierarchical nature of HiTOP to gain further efficiency. In some contexts, a fine-grained assessment of externalizing subdimensions may be important, but in other cases, simply assessing general externalizing symptoms might be sufficient.
The current study builds on these general advantages of HiTOP through identifying dimensions specifically relevant to psychosis risk. In particular, the HiTOP subfactors of reality distortion, detachment, distress, fear, and mania captured the most relevant symptom variance in the present study. These symptom dimensions come from both internalizing and psychosis superspectra, suggesting that a broad assessment of psychopathology dimensions can inform case conceptualization. For example, the same positive-symptom scores on the SIPS may be interpreted differently if they are accompanied by associated features of mania and substance use in one case versus distress and detachment in another. In practice, CHR individuals are typically identified when attenuated positive symptoms become concerning to the individual or the individual’s family members. Given the current study’s findings, attenuated positive symptoms can be conceptualized as transdiagnostic expressions of interactions between multiple latent psychopathology dimensions. Practically, attenuated positive symptoms are therefore a complex presenting problem warranting comprehensive transdiagnostic assessment (e.g., using the HiTOP-DAT digital tool; Jonas et al., 2021). With a comprehensive assessment, an individualized phenotypic-symptom profile can guide case conceptualization and treatment. Future research defining subtypes of CHR symptom presentation based on co-occurring psychopathology dimensions would be highly useful in this respect.
Theoretically, a hierarchical transdiagnostic model of psychosis risk also allows results from hard-to-reach CHR samples to be integrated into the HiTOP framework, leveraging the growing body of knowledge on transdiagnostic psychopathology (e.g., Kotov et al., 2020, 2021) to deepen the understanding of psychosis risk states. The current study was cross-sectional and does not provide any evidence on longitudinal changes in symptoms. Hierarchical approaches, however, may allow for more precise modeling of symptom expression in different clinical stages. Early stages of incipient psychopathology are characterized by relatively nonspecific indicators of psychological distress, which can include psychotic-like experiences as well as other symptoms (Addington et al., 2019; McGorry et al., 2018). In later clinical stages, symptoms crystalize into primary disorders. This hypothesis is difficult to test in the DSM framework because all diagnoses are defined at the same level of specificity. By contrast, from a hierarchical-transdiagnostic perspective, an individual’s symptom profile might initially show disturbances in broad dimensions in earlier stages that crystalize into more specific symptom clusters in later stages. One study found that dimensional measures of psychopathology are already elevated at age 7 in the children of adults with schizophrenia or bipolar disorder (Ellersgaard et al., 2018), highlighting the potential of dimensional approaches to inform clinical-staging models. The HiTOP model therefore may facilitate more rigorous tests of clinical-staging models of the development of mental illness through longitudinal studies or cross-sectional studies of individuals in different clinical stages.
The current results also support step-based treatment suggested by clinical-staging models (Hartmann et al., 2021; McGorry et al., 2018; Scott et al., 2013). Transdiagnostic treatments, such as the unified protocol for transdiagnostic treatment of emotional disorders (Barlow et al., 2010), likewise may be most effective for broad symptom dimensions, whereas specialized treatments, such as cognitive-behavioral therapy for psychosis risk (van der Gaag et al., 2013), may be most effective for specific symptom dimensions.
Measurement approach
In the current study, symptoms were measured on a variety of timescales ranging from past week to past year. The timescale instructions matched those commonly used for each measure to keep findings as consistent as possible with how these measures are used in research and clinical practice. Note that keeping the original timescales of the three psychosis screeners preserved the validity of their established screening cutoffs. However, differing timescales could introduce an additional source of variance. It is currently unknown on what timescales state-symptom measures begin to approximate trait measures (DeYoung et al., 2022). Whereas state and trait measures often show differing results in schizophrenia (e.g., in state vs. trait anhedonia; Cowan et al., 2020; Dickinson et al., 2018; Strauss & Gold, 2012), past-week measures already capture considerably more trait-like variance than true state measures (DeYoung et al., 2022). For instance, past-week and entire-lifetime measures of depression in schizophrenia correlate with r > .60 (Chiappelli et al., 2014). Although there would still have been some value in harmonizing the time frames of assessment to improve the current study’s measurement precision (e.g., changing all instructions to “past month” to match the clinician-rated variables), this approach would have come with the downside of making results less compatible with prior research using the same measures.
Symptoms were also assessed by different modalities in the reference sample (self-report) and the interview subsample (clinician-rated interviews). By examining outcomes assessed in a different modality, the current study minimizes common method variance that could inflate estimated relationships between symptom dimensions and clinician-rated outcomes (Podsakoff et al., 2003). Clinician-rated outcomes were also rated on an intermediate timescale (past month), which would be expected to relate similarly to shorter (e.g., past week) and longer (e.g., past year) self-report timescales. At the same time, there may be important nuances to the use of self-report and clinician-rated assessments in the current study. Note that self-report items tapping anhedonic or blunted affect aspects of negative symptoms (e.g., PQ 89: “I have felt uninterested in the things I used to enjoy”; PQ 82: “I have left like . . . I was no longer able to feel sadness, or . . . I could not feel happy”) loaded onto the Distress factor rather than the Detachment factor or its subfactors (see Table S5 in the Supplemental Material). These items correspond to those forming a “dissociative/depressive” factor in a recent EFA of PQ negative-symptom items (Pierce et al., 2021). In that study, the dissociative/depressive factor correlated strongly (r ≥ .62) with depression and anxiety.
These converging findings could reflect issues with measuring negative symptoms—that is, that available self-report measures identify some negative-symptom factors (e.g., asociality) more cleanly than others (e.g., anhedonia, blunted affect). Alternatively, these findings could indicate that distressed internalizing and anhedonia/blunted affect cannot be distinguished in samples of community youths, perhaps because of phenotypic overlap between distress and negative symptoms in the early clinical stages of developing psychopathology. Future research including more targeted measures of negative symptoms (e.g., Self-Evaluation of Negative Symptoms scale) could shed light on these issues. Likewise, insight or symptom severity may also affect young people’s ability to accurately report on their own symptoms. Future research could explore this possibility by including measures of cognitive or clinical insight.
Strengths and limitations
This study’s strengths included its large sample size in the reference group, which allowed for a complex data-driven hierarchy of symptom dimensions without sacrificing statistical power; its high-resolution assessment of psychotic-like experiences; and its validation of self-reported symptom dimensions by clinical interviews. The study also had some limitations. Participants were recruited from large metropolitan areas in the central and eastern United States, leaving the possibility that results would not generalize to youths recruited in different contexts. Mitigating this concern, SIPS positive-symptom scores for CHR participants in this study (mean total score = 9.68, SD = 3.30) were typical of SIPS scores for CHR samples recruited across many contexts in 38 studies worldwide (median total score = 9.9, interquartile range = 9.0–11.6; Woods et al., 2019). Another potential limitation concerns sample size in the CHR+ subgroup. Although the overall study leveraged structural findings from a large reference group, future studies with larger CHR sample sizes would be required to examine hierarchical symptom dimensions within a pure CHR sample. Externalizing symptoms were also underrepresented in the symptom questionnaires, with coverage limited to substance use. It is unclear, for example, whether the link between substance use and lower negative symptoms reflects a unique effect for substance use or a shared effect for externalizing symptoms more broadly. Likewise, there were potential confounds with perceptual abnormalities experienced while intoxicated (see “Substance Use and Perceptual Abnormalities” above). This study also did not assess cognitive deficits, which have been shown to relate to detachment and disorganization symptom dimensions in psychotic disorders (Kotov et al., 2020). Further research linking cognitive deficits to hierarchical symptom dimensions in CHR would be valuable. Finally, this study was cross-sectional rather than longitudinal, which did not allow analyses of participants in distinct clinical stages or participants who went on to develop psychotic disorders.
Conclusion
Psychosis risk symptoms were revealed to be transdiagnostic constructs when mapped onto hierarchical symptom dimensions. These data allow new evidence from CHR samples to be integrated into the larger picture of psychiatric comorbidity. Continued research can build on these results to explore the relative contribution of various symptom dimensions to psychosis risk, identify subgroups in psychosis risk samples with different phenotypic symptom profiles, and implement transdiagnostic assessment and treatment strategies for individuals at risk for psychosis.
Supplemental Material
sj-docx-1-cpx-10.1177_21677026221146178 – Supplemental material for Mapping Psychosis Risk States Onto the Hierarchical Taxonomy of Psychopathology Using Hierarchical Symptom Dimensions
Supplemental material, sj-docx-1-cpx-10.1177_21677026221146178 for Mapping Psychosis Risk States Onto the Hierarchical Taxonomy of Psychopathology Using Hierarchical Symptom Dimensions by Henry R. Cowan, Trevor F. Williams, Jason Schiffman, Lauren M. Ellman and Vijay A. Mittal in Clinical Psychological Science
Footnotes
Transparency
Action Editor: Vina Goghari
Editor: Jennifer L. Tackett
Author Contributions
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.