
Abstract
Approximately two thirds of veterans with posttraumatic stress disorder (PTSD) remain with the disorder following treatment. Pinpointing the per-symptom effectiveness of treatments in real-world clinical settings can highlight relevant domains for treatment augmentation and development. Baseline and posttreatment assessments of PTSD and depression were performed in 709 veterans with PTSD. PTSD remission was 39.4%. Treatment was least effective for intrusion symptoms and had no effect on flashbacks or on poor recall of traumatic features. Of veterans who remitted, 72.8% still met diagnostic criteria for at least one cluster. Poor clinical effectiveness was noted for depression; only 4.1% of the patients remitted following treatment. Treatments for veterans with PTSD show limited overall effectiveness in real-world settings. Enhancing treatment response may require enhancing provider fidelity and patient compliance with extant treatments or the development of new treatments that specifically target the symptoms of PTSD that do not respond well to extant treatments.
Posttraumatic stress disorder (PTSD) is a common, chronic, and disabling condition in veteran and military populations (Forbes et al., 2019). Four decades of research established therapies that show clinically meaningful improvements in patients with PTSD (Bryant, 2019). However, nonresponse rates have been high, particularly in military and veteran populations, and around two thirds of treated veterans retain a PTSD diagnosis after receiving treatment (Forbes et al., 2010). First-line treatments such as cognitive behavior therapy (CBT) show only marginally superior results compared with active control conditions (Steenkamp et al., 2015) and demonstrate low tolerability and high dropout rates (Hembree et al., 2003; Imel et al., 2013). Furthermore, only a few large studies have documented treatment-response rates in real-world clinical settings, potentially pointing to an efficacy–effectiveness gap (Hengartner, 2018; Howard et al., 1996; Nathan et al., 2000), which can produce higher remission rates in randomized controlled efficacy trials than in real-world effectiveness studies. Thus, major challenges confront attempts to improve treatment by either enhancing provider fidelity, patient compliance, and augmentation of extant treatments or developing new treatments that target the symptoms of PTSD that do not respond well to extant treatments. One organizing path for targeting these challenges involves a careful delineation of treatment-response features in veterans with PTSD, which is the primary focus of the current investigation.
PTSD efficacy data reveal an intriguing anomaly. PTSD involves additive combinations of symptom clusters: intrusion, avoidance, hyperarousal, and, in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013), also negative changes in mood or thoughts. The symptoms of some of the PTSD clusters can be more effectively treated, for example, avoidance in the context of anxiety disorders (Hoffman & Mathew, 2008; Springer et al., 2018) or anhedonia in the context of major depression (Mann, 2005; Trivedi et al., 2006). However, overall PTSD remission rates remain much lower than those achieved in other disorders applying similar treatments. Here, we study veterans treated for PTSD in the Israel Defense Forces (IDF) Unit for Treatment of Combat-Related PTSD (UTC-PTSD), a real-world outpatient clinic specializing in combat-related PTSD. We asked the following questions:
What is the overall and per symptom-cluster (intrusion, avoidance, hyperarousal) remission rates in veterans treated for PTSD?
What is the remission rate of each of the specific symptoms of PTSD, according to the fourth edition, text revision of the DSM (DSM-IV-TR; American Psychiatric Association, 2000)?
Given that there are various ways to achieve remission from PTSD, what is the prevalence of the different ways by which patients achieve remission? And what is the proportion of patients who remain clinically symptomatic in certain symptom clusters despite being remitted from PTSD according to DSM-IV-TR?
What is the remission rate and treatment-response levels for depression symptoms in veterans treated for PTSD?
Does treatment type (trauma-focused CBT, psychodynamic psychotherapy, pharmacotherapy) affect PTSD remission rates?
Method
Participants
Between 2006 and 2014, 1,795 male veterans approached the UTC-PTSD (see description below); of these, 990 reported combat/war-related trauma or traumas that met with DSM-IV-TR Criterion A and met DSM-IV-TR criteria for PTSD (American Psychiatric Association, 2000; see below). Treatment-response data are reported for the 709 patients (mean age = 36.83 years, range = 21–80; mean age at trauma = 24.1 years, range = 18–58) who also completed one of the treatment protocols offered in the clinic (trauma-focused CBT, psychodynamic psychotherapy, or pharmacotherapy). Patients included in the analyses did not differ from the 281 patients who were not on baseline PTSD, t(988) = 0.306, p = .76, and depression severity, t(988) = 1.308, p = .76 (for measures, see below). Of the 281 veterans not included in the analyses, 34 declined treatment, and 247 dropped out and did not provide follow-up data. All participants were honorably discharged from military service.
Excluded were 805 veterans who (a) did not meet DSM-IV-TR criteria for PTSD diagnosis, (b) had active or past psychosis or current severe substance use disorder, (c) had concrete suicidal plans and were taken to a psychiatric emergency room for immediate intervention, and (d) were receiving psychotherapy or pharmacotherapy elsewhere. The study was approved by the IDF Medical Corps Ethics Committee.
The IDF UTC-PTSD
The UTC-PTSD is an in-house IDF professional clinic providing specialized psychological and psychiatric response to veterans in distress as a result of participation in combat or military activity. The diagnostic and treatment services are provided free of charge and without a need for official recognition by entities such as the Veteran Affairs Office or the Department of Defense. Service provision is not restricted by the time elapsed since trauma, and veterans from all of Israel’s wars are accepted.
Diagnostics
Veterans who approach the UTC-PTSD are invited to a formal clinical assessment conducted by clinicians with 12 or more years of formal experience in PTSD diagnosis in veterans. Semistructured diagnostic interviews based on DSM-IV-TR criteria were administered as part of the routine admission process, and PTSD and depression were specifically diagnosed using the Clinician-Administered PTSD Scale (CAPS; Blake et al., 1995) and the Montgomery–Åsberg Depression Rating Scale (MADRS; Montgomery & Åsberg, 1979), respectively. Each patient’s assessment record was presented in a staff meeting in which decisions on diagnoses and recommendations for ensuing treatment were made (Levi, 2017; Levi et al., 2016). This diagnostic procedure was repeated 1 week following end of treatment to assess its impact on symptoms and diagnoses.
CAPS
A clinical diagnosis of PTSD was established using the CAPS, a 17-item structured interview based on DSM-IV-TR criteria. The F1/I2 item rule (Blake et al., 1995) was applied such that a symptom was considered endorsed if its reported frequency was greater than 1 and its reported intensity was greater than 2. In accordance with DSM-IV-TR, a PTSD diagnosis necessitated endorsement of at least one intrusion symptom, three avoidance symptoms, and two hyperarousal symptoms. The same rules were applied to the specific symptom clusters (intrusion, hyperarousal, and avoidance) to determine their clinical endorsement. The CAPS has excellent reliability, convergent and discriminant validity, diagnostic utility, and sensitivity to clinical change in military veterans and other populations (Weathers et al., 2001). Cronbach’s α in the current sample was .91.
MADRS
A diagnosis of major depressive disorder was established using the MADRS, a 10-item clinician-administrated scale that assesses the core depressive symptoms according to the fourth edition of the DSM (DSM-IV; American Psychiatric Association, 1994). A score of 0 to 6 is considered to indicate no symptoms, a score of 7 to 19 indicates mild depression, a score of 20 to 34 indicates moderate depression, and a score greater than 34 represents severe depression. The MADRS has high interrater reliability, convergent validity, and rates of sensitivity to change comparable with other measures of depression (Khan et al., 2002; Williams & Kobak, 2008). Cronbach’s α in the current sample was .90.
Treatment assignment
In the current sample, 27% (n = 191) of patients received trauma-focused CBT, 42% (n = 299) received psychodynamic psychotherapy, and 31% (n = 219) received pharmacotherapy. Assignment to treatment type was determined according to clinical considerations (see Levi, 2017; Levi et al., 2016) and patients’ preferences. Specifically, each patient was informed about the possible treatments available at the UTC-PTSD and was offered the specific treatment protocol the intake team had deemed most appropriate for the person given the information gathered during the diagnostic process. Patients then either agreed to the recommended treatment (94%) or requested an alternative available treatment.
Treatments
The UTC-PTSD offers three types of treatment: trauma-focused CBT, psychodynamic psychotherapy, and pharmacotherapy. Group treatments were not concurrently offered. Each treatment is delivered by a team of specialists (clinical psychologists, clinical social workers, and psychiatrists) with extensive training, specialization, and experience in combat-related PTSD. These are briefly described below. For a more elaborate description and protocols overview of the trauma-focused CBT and the psychodynamic psychotherapy offered by the UTC-PTSD, see Levi et al. (2016) and the Supplemental Material available online. Weekly supervision sessions were held to monitor treatment progress.
The trauma-focused CBT protocol consisted of 20 weekly sessions of trauma-focused intervention and reflected a combination of elements from prolonged exposure (PE) therapy (Foa et al., 2005) and cognitive processing therapy (CPT; Resick & Schnicke, 1992), following five stages: (a) psycho-education on the impact of trauma, emphatic clarification of patient’s distress, and determination of treatment goals; (b) narrative reconstruction of the traumatic event; (c) identification of “stuck thinking” and the associations between such thoughts and distress (at this stage, the therapist and the patient try to identify and challenge overgeneralizations of trauma-based reactions); (d) in vivo exposure to environments and situations that elicit posttraumatic symptoms; and (e) termination and summary. At this concluding stage, therapist and patient discuss what has been achieved in therapy and review the tools the patient had acquired during the process.
The psychodynamic psychotherapy protocol applied at the UTC-PTSD lasts 1 year and constitutes three broad stages: (a) establishment of a therapeutic alliance, (b) exploration of unconscious conflicts arising from the effect of the trauma (this involves addressing the therapist–patient relationship while focusing on unresolved conflicted feelings linked to significant figures of the patient’s past and analysis of how such feelings may protect the patient’s awareness from threatening thoughts, feelings, and impulses), and (c) termination and summary, working through the sense of loss that is inherent in any trauma but particularly the loss of the therapy and therapist from the patient’s routine life. These losses are linked to trauma-related losses and to previous endings in the patient’s life. This stage also includes a review of therapy-related achievements and a discussion of what remains to be explored before treatment ends. The goal of therapy is to help patients master their inner experiences and regain integrity in their life. Psychodynamic psychotherapy as delivered at the UTC-PTSD is designed to advance patients’ understanding of how their trauma had affected their personality. Subjective experiences since the trauma are examined while also touching on relationships with significant figures from their past and how those relationships affected the assimilation of the traumatic event in the present. Interpersonal problems that had developed since the traumatic event are also discussed either directly or through the lens of the patient–therapist relationship.
Pharmacotherapy typically started with selective serotonin-reuptake inhibitors (SSRIs) followed by serotonin–norepinephrine-reuptake inhibitors (SNRIs) in the presence of inadequate response or poor medication tolerance. SSRI/SNRIs were started at the low end of their therapeutic range and titrated up gradually until response was achieved. For example, sertraline was started at 25 mg/day, and if no clinical response was seen after 3 weeks, the doses were increased in 50 mg/day increments, with 2 to 4 weeks between dosage increases, up to 250 mg/day. Therapy started with 12 weeks of acute treatment that was continued at least 6 months to reduce risk for symptom relapse. When first-line SSRI/SNRIs therapies were deemed ineffective, benzodiazepines would be sometimes used. Antidepressant treatments were sometimes augmented by atypical antipsychotics or α-adrenergic-receptor blockers to assist in reducing irritability, nightmares, and sleep difficulties.
Data analysis
To gauge overall remission rates from PTSD, we computed the percentage of patients who no longer met DSM-IV-TR diagnostic criteria for PTSD at posttreatment. Likewise, we computed the percentage of patients no longer meeting the diagnostic criteria for each of the specific symptom clusters (intrusion, avoidance, hyperarousal) at treatment end. We applied McNemar’s tests to compare remission rates between symptom clusters and applied Bonferroni-corrected αs to account for multiple comparisons. To gauge per-symptom remission rates, we computed the percentage of patients who no longer endorsed each of the 17 specific symptoms listed for PTSD in DSM-IV-TR at treatment end. We further applied McNemar’s tests to compare between pretreatment and posttreatment symptom-endorsement rates, again applying Bonferroni-corrected αs to account for multiple comparisons. In addition, we estimated dimensional overall and per-cluster symptom relief and the relative magnitude of symptom relief between clusters (intrusion, avoidance, hyperarousal) by calculating mean reductions in symptom severity from baseline to posttreatment on a scale ranging 0 to 4, which reflects the CAPS item-scores range. To test reductions in severity per symptom from pretreatment to posttreatment, we conducted paired-sample t tests on the sum of the frequency and severity of each symptom item from the CAPS (scale range = 0–8). Bonferroni-corrected paired samples t test and Cohen’s d effect sizes are reported.
To further clarify remission patterns (i.e., what symptom-cluster combinations were no longer meeting DSM-IV-TR criteria for PTSD; American Psychiatric Association, 2000), we calculated the percentage of the remitted patients who remitted via each of seven possible ways (i.e., by no longer meeting criteria for all three clusters; intrusion = B, avoidance = C, hyperarousal = D). That is, patients might meet criteria only for intrusion and avoidance, only for intrusion and hyperarousal, only for avoidance and hyperarousal, only for intrusion, only for avoidance, or only for hyperarousal. We also provide the percentage of patients who remained symptomatic in at least one cluster out of veterans who remitted and estimated the prevalence of negative treatment response by calculating the percentage of patients whose symptom severity on the CAPS increased by 15 points or more relative to their pretreatment symptom severity (Blake et al., 2000).
To gauge depression remission rates, we computed the percentage of patients who no longer met DSM-IV diagnostic criteria for major depressive disorder at end of treatment. We also contrasted pretreatment and posttreatment MADRS total scores to evaluate pretreatment to posttreatment changes in depression severity.
Finally, to probe differences in remission rates between treatment types, separate analyses of variance were conducted with overall, intrusion, avoidance, and hyperarousal remission rates as the dependent variables and treatment type (trauma-focused CBT, psychodynamic psychotherapy, pharmacotherapy) as a between-subjects factor. Significant interaction effects were followed with post hoc Bonferroni-corrected contrasts. Partial η2 effect sizes are reported.
Results
What were the overall and per symptom-cluster remission rates?
Figure 1 depicts the overall and per-symptom-cluster remission rates (left) and reductions in mean symptom severity from pretreatment to posttreatment (right). Overall, remission rate was 39.4%, and 39% of patients experienced a reduction of 15 points or more in total CAPS score from pretreatment to posttreatment. Intrusion, avoidance, and hyperarousal symptoms remitted in 15.8%, 31.7%, and 22.7% of patients, respectively. The remission rate observed for the intrusion cluster was significantly lower than those observed for the avoidance and hyperarousal clusters, and the hyperarousal cluster had a lower remission rate than the avoidance cluster, all ps < .01.
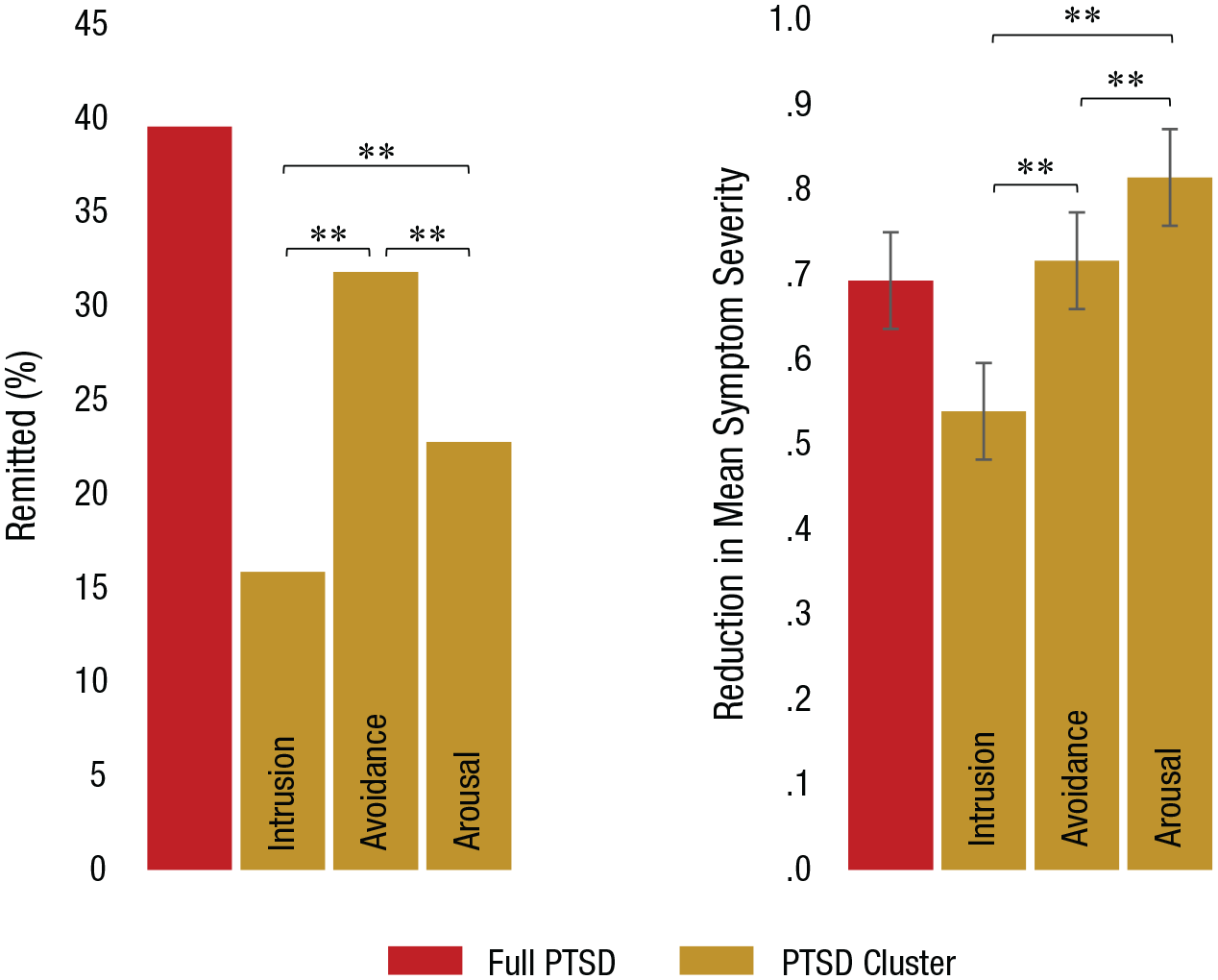
The graph on the left shows remission rates for overall posttraumatic stress disorder (PTSD) and for each symptom cluster. The graph on the right shows dimensional reduction in mean symptom severity on the Clinician-Administered PTSD (CAPS) Scale (range = 0 to 4; Blake et al., 1995). Asterisks indicate significant differences between clusters (**p < .01, Bonferroni corrected) as measured by McNemar’s test or within-subjects contrast.
The dimensional analyses indicated a reduction in overall symptom severity, t(708) = 22.94, p = .0001, d = 0.86, and significant reductions for each of the symptom clusters—intrusion: t(708) = 15.48, p = .0001, d = 0.58; avoidance: t(708) = 20.11, p = .0001, d = 0.75; hyperarousal: t(708) = 24.83, p = .0001, d = 0.93. A lower reduction in symptom severity was noted for the intrusion cluster relative to both the avoidance cluster, t = −6.09, p = .0001, d = −0.23, and the hyperarousal clusters, t(708) = −9.02, p = .0001, d = −0.34. A lower reduction was noted for the avoidance cluster relative to the hyperarousal cluster, t(708) = −3.85, p = .001, d = −0.13.
Overall, 6.2% of patients showed negative treatment response, indexed by an increase of 15 points or more on the CAPS relative to pretreatment symptom severity.
What were the remission rates and dimensional severity relief of each specific symptom?
Figure 2a depicts symptom-endorsement rates at pretreatment and posttreatment and remission rates from each of the symptoms at treatment end. Modest but significant reductions were observed following treatment in all but two symptoms. Remission rates in symptoms that significantly improved following treatment ranged between 37.5% for feeling of detachment or estrangement from others and 12.2% for physiological reactivity on exposure to internal or external cues that symbolize or resemble an aspect of the traumatic event). No change at all was noted following treatment for the inability to recall an important aspect of the trauma, and increased endorsement was noted for acting or feeling as if the traumatic event(s) were recurring (i.e., flashbacks).
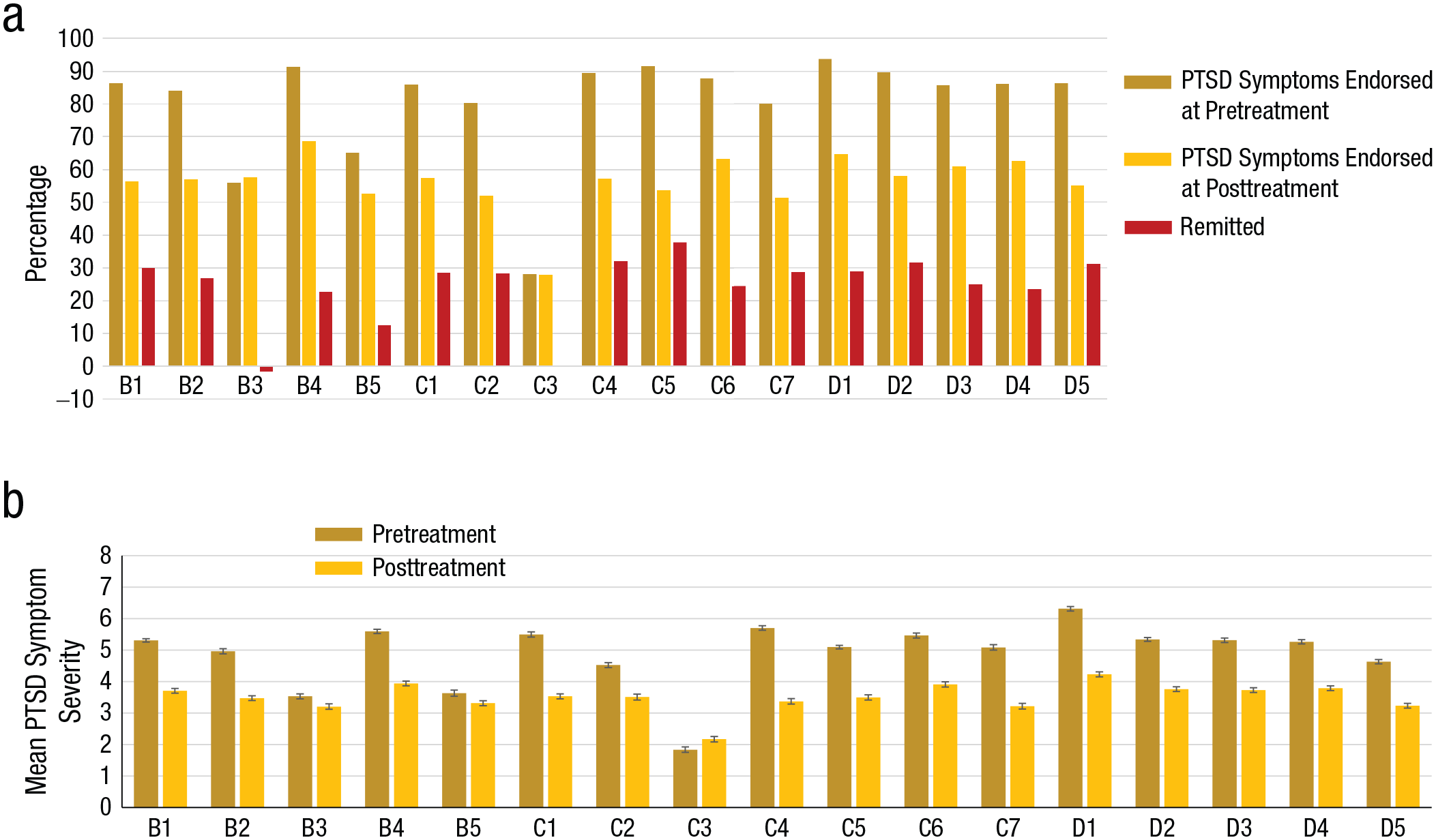
Treatment results. The graph in (a) shows the percentage of posttraumatic stress disorder (PTSD) symptom-endorsement rates at pretreatment and posttreatment and percentage of PTSD remission following treatment, separately for each symptom. The graph in (b) shows per-symptom severity (sum of frequency and severity subscales per item, range = 0–8) at pretreatment and posttreatment. Intrusion: B1 = intrusive memories; B2 = nightmares; B3 = flashbacks; B4 = emotionally upset by trauma reminders; B5 = physical reactions to trauma reminders. Avoidance: C1 = avoid thoughts or feelings associated with the trauma; C2 = avoid activities, places, people associated with the trauma; C3 = difficulty remembering aspects of the trauma; C4 = less interested in activities previously enjoyed; C5 = distant from people; C6 = emotionally numb; C7 = foreshortened future. Hyperarousal: D1 = sleep problems; D2 = irritable or angry; D3 = difficulty concentrating; D4 = alert or watchful; D5 = startle. All pretreatment/posttreatment contrasts were significant (p < . 05, Bonferroni corrected) except for B3, B5, and C3.
Figure 2b depicts symptom severity at pretreatment and at posttreatment. Reductions were observed following treatment in all but three symptoms, t(708)s = 14.22 to 21.91, ps = .0001, ds = 0.34 to 0.82. No change was noted following treatment for the symptoms acting or feeling as if the traumatic event(s) were recurring (i.e., flashbacks), physical reactions to trauma reminders, and inability to recall an important aspect of the trauma.
How did veteran patients with PTSD achieve remission?
At the symptom-clusters level, there were seven different ways to no longer meet criteria for DSM-IV-TR PTSD diagnosis: A patient can no longer meet criteria for any one of the three symptom clusters or any combination of two clusters. Figure 3 provides the percentage breakdown for each of these remission options across the total sample.
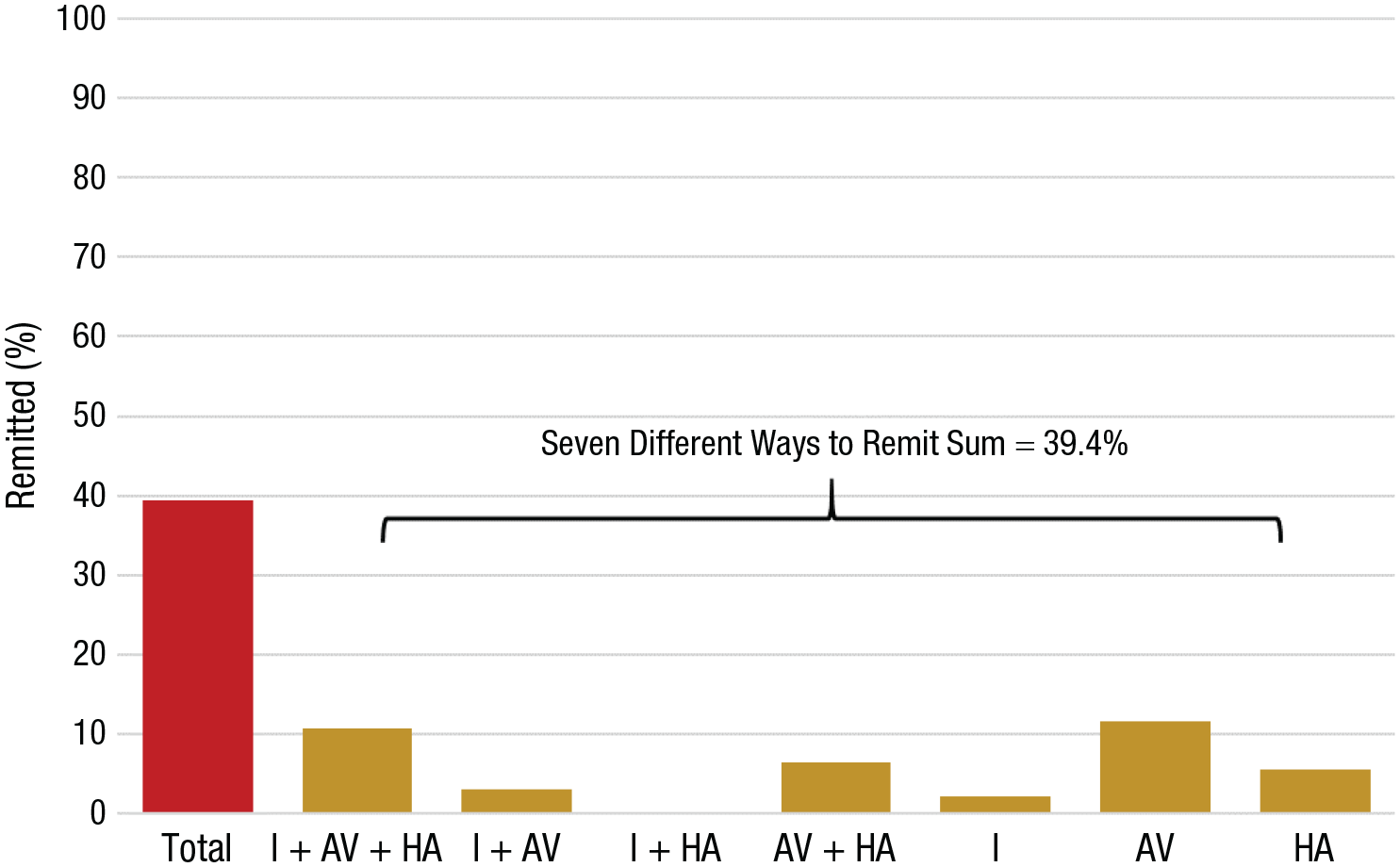
Different ways to remit from posttraumatic stress disorder (PTSD). The percentage of remissions is provided for all PTSD and for symptom cluster or combinations of symptom clusters. I = intrusion; AV = avoidance; HA = hyperarousal.
Of the 39.4% of patients who remitted at treatment end, 27.2% remitted from all three symptom clusters (intrusion, avoidance, and hyperarousal), 7.6% from intrusion and avoidance, 16.5% from avoidance and hyperarousal, 5.3% from intrusion only, 29.4% from avoidance only, and 14% from hyperarousal only. None of the patients remitted via the intrusion and hyperarousal option. Note that 72.8% of veterans who remitted continued to meet diagnostic criteria for at least one of the symptom clusters.
What were the remission rates of depression in veterans treated for PTSD?
Figure 4 depicts depression rates at pretreatment and at posttreatment for the full sample. Overall, 98.3% of the patients were diagnosed with comorbid major depressive disorder at baseline. A very modest, statistically significant reduction to 94.2% diagnosed was observed following treatment (4.1% remitted). This observation is mirrored by a statistically significant reduction in mean depression severity from pretreatment to posttreatment, t(708) = 12.82, p = .0001, d = 0.48; mean scores remained within the moderate depression severity range at posttreatment.
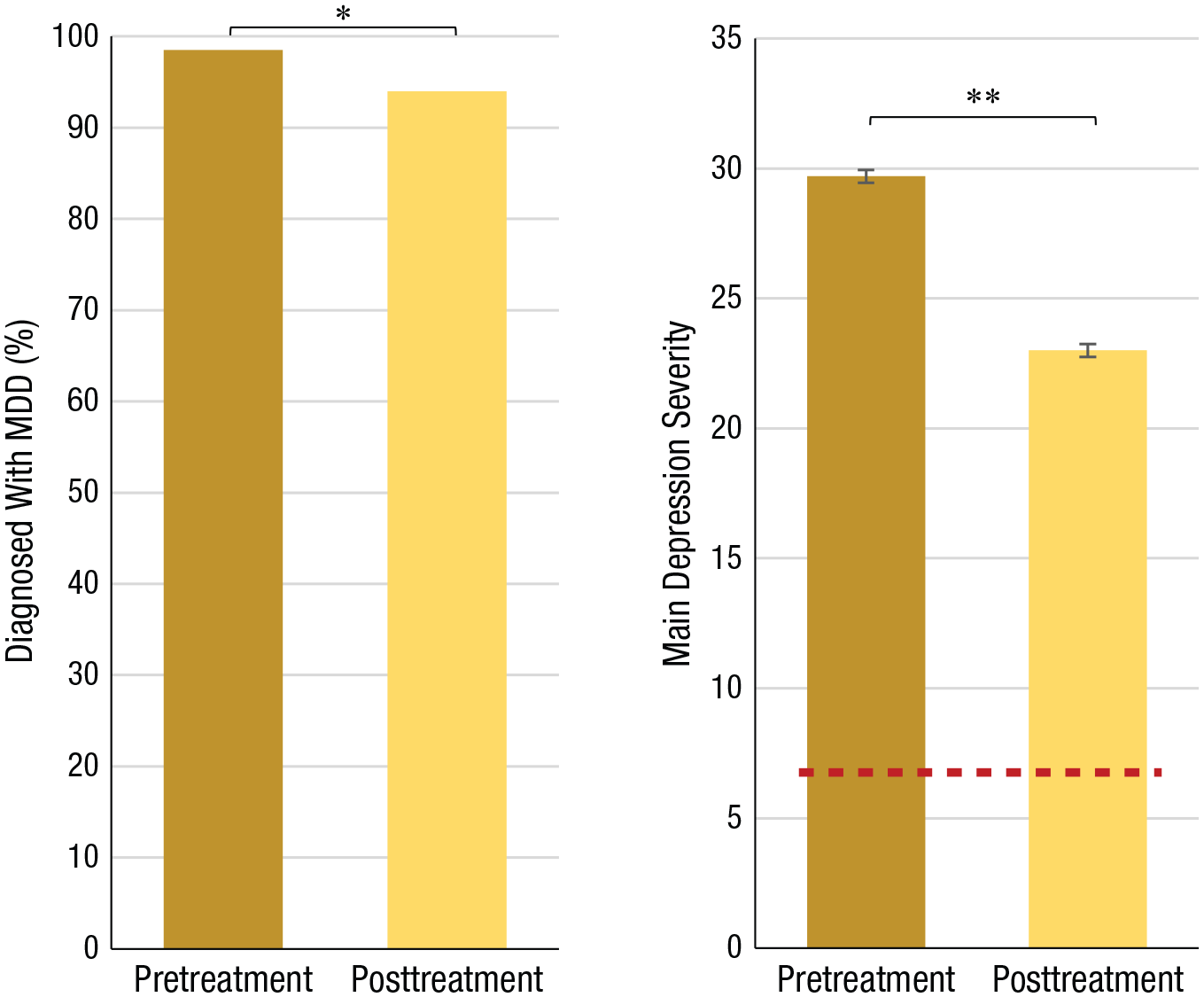
Pretreatment and posttreatment percentages of major depressive disorder (MDD) diagnosis (left) and levels of depression severity (right). Scores between 20 and 34 on the Montgomery–Åsberg Depression Rating Scale (MADRS; Montgomery & Åsberg, 1979) indicate moderate depression. A score less than 7 (dashed red line) indicates no depression. Asterisks indicate significant differences between pretreatment and posttreatment (*p < .05. **p < .01).
Treatment type and remission rates
Overall remission rates did not differ between the three treatment types (trauma-focused CBT remission = 40.8%; psychodynamic psychotherapy remission = 42.1%; pharmacotherapy remission = 34.2%), F(706) = 1.77, p = .17, η p 2 = .005. Furthermore, remission rates did not differ between treatment types for the avoidance symptom subcluster, F(706) = 0.47, p = .62, η p 2 = .001. Remission rates did differ between treatment types for the intrusion symptom subcluster, F(706) = 5.55, p = .004, η p 2 = .015, and the hyperarousal symptom subcluster, F(706) = 7.87, p = .0001, η p 2 = .022. For the intrusion subcluster, higher remission rates were noted for trauma-focused CBT (21.0%) relative to pharmacotherapy (10.0%), p = .003. Remission rates did not differ between trauma-focused CBT and psychodynamic psychotherapy (16.0%) or between psychodynamic psychotherapy and pharmacotherapy, all ps > .10. For the hyperarousal subcluster, higher remission rates were noted for both trauma-focused CBT (24.6%; p = .024) and psychodynamic psychotherapy (28.1%; p = .0001) relative to pharmacotherapy (13.7.0%). Remission rates in hyperarousal did not differ between trauma-focused CBT and psychodynamic psychotherapy, p > .10.
Discussion
The results of the current study corroborate results from previous studies in veterans, which typically note remission of PTSD following treatment in about one third of the patients (Forbes et al., 2010). Moreover, in the current study, 72.8% of the patients who did not meet criteria for PTSD following treatment still manifested significant symptoms in at least one PTSD symptom cluster; only 10.7% remitted from all three clusters. Intrusion symptoms responded most poorly to treatment, and two mnemonic symptoms—flashbacks and inability to recall an important aspect of the trauma—showed no response at all. Poor clinical effectiveness was also noted for the intrusion-related symptom of physical reactions to trauma reminders and for depression.
These results raise questions regarding differential treatment response in PTSD compared with mood and anxiety disorders. Note that CBT and SSRI pharmacotherapy produce stronger effects on the same set of mood and anxiety symptoms in anxiety disorders (~50% remission; Hoffman & Mathew, 2008; Springer et al., 2018) and major depressive disorder (20%–40% remission; Mann, 2005; Thimm & Antonsen, 2014; Trivedi et al., 2006) than these treatments produce on such symptoms in PTSD (CBT ≈ 25% remission in the current sample; SSRI pharmacotherapy ≈ 4% remission in the current sample). One explanation for this difference may reflect an instance of the often documented efficacy–effectiveness gap (Hengartner, 2018; Howard et al., 1996; Nathan et al., 2000), which can produce higher remission rates in randomized controlled efficacy trials than in real-world effectiveness studies. However, this explanation cannot fully account for such differences because effectiveness trials have found higher remission rates for mood and anxiety symptoms in patients with anxiety disorders or major depressive disorder than in patients with PTSD.
Alternatively, weak treatment effects may reflect unique clinical features in which posttraumatic mood-related and anxiety-related symptoms occur in the context of memory-based symptoms that do not occur in mood or anxiety disorders (Bar-Haim et al., 2021; Bourne et al., 2013; Brewin, 2015; Ehlers et al., 2004). Memory intrusion and reexperiencing of the trauma occur only in PTSD and not in anxiety disorders or depression. If these symptoms are not successfully treated, other features of the disorder also may persist. The current data reveal minimal relief from symptoms of intrusive traumatic reexperiencing (only 15.8% of patients remitted from this symptom cluster). Flashbacks arguably represent the most severe intrusive-reexperiencing symptom, and these were not affected by any treatment in the current sample. If mnemonic features represent a core aspect of PTSD that is poorly targeted by current treatments, treatment development for PTSD should perhaps focus more closely on the intrusive-reexperiencing symptoms, their mechanistic failure in PTSD, and their impact on additional symptoms. New treatments with more refined focus may be needed to achieve breakthroughs in efficacy and effectiveness. It also appears that current PTSD pharmacotherapy protocols are suboptimal for the treatment of comorbid major depression, which therefore highlights the need for alternative treatment strategies for PTSD patients with comorbid depression.
The results of the current study should be considered in light of several limitations. First, military service in Israel is mandatory and therefore also shapes the organized treatment response of the nation to veterans with combat-related PTSD. Generalization of the current effectiveness findings to veteran patients from professional militaries and their specific context of PTSD treatment awaits further research.
Second, as is usually the case in real-world clinical settings, patients were not randomly assigned to treatment type. Here we focus on the general effectiveness of PTSD treatment in the UTC-PTSD, the most comprehensive and established war-related PTSD clinic in Israel. Great caution must be applied when interpreting the exploratory comparative analyses of the three treatment types offered by the UTC-PTSD. This tentative analysis suggests no differences in overall remission rates or in remission from the avoidance symptom cluster. These results are in line with randomized controlled trials (RCTs) that typically have not found differences between active PTSD treatments (e.g., Markowitz et al., 2015; Rauch et al., 2019). An advantage for trauma-focused CBT over pharmacotherapy was noted for the hyperarousal and intrusion clusters and for psychodynamic psychotherapy over pharmacotherapy for the hyperarousal cluster. Note, however, that effectiveness data from trials in which patients are randomly assigned to different treatments are critical to shed further light on these specific treatment-effectiveness results.
Third, the trauma-focused CBT protocol applied by the UTC-PTSD does not adhere to the typically researched CBT protocols for PTSD and offers a combination of elements from PE and CPT with a longer treatment course than either of these specialized protocols alone. It is possible that despite being more comprehensive and extensive than PE or CPT, this hybrid treatment is in fact not as effective as either of these treatments alone. It is also possible that treatment adherence, by both providers and patients, was not as optimal as could potentially be achieved in some academic clinical trial settings, thereby reducing effectiveness. Note, however, that despite these potential caveats, remission rates for trauma-focused CBT in the current sample were similar to those reported in more strictly monitored RCTs of PE and CPT.
Fourth, longer treatment protocols might lead to higher dropout (e.g., Foa et al., 2018). With a focus on treatment completers, we do not address the dropout issue in PTSD treatment in the current report.
Fifth, the data reported here were collected before the new symptom clustering of PTSD in DSM-5 (American Psychiatric Association, 2013) was published or implemented in the UTC-PTSD. It may be useful to repeat the current analyses with data from patients who were diagnosed before and after treatment using this more recent classification.
Sixth, future studies may wish to examine clinical improvement in additional manners such as response rates, clinically meaningful changes rates, or reliable change rates. Finally, factors that may serve as mediators or moderators of treatment outcome, such as cultural background, racial/ethnicity identification, and measures of income or socioeconomic status, were not collected.
In conclusion, treatments for veterans with PTSD as delivered at the UTC-PTSD show limited overall effectiveness and particularly poor outcomes for the intrusive-traumatic-reexperiencing domain and for depression when comorbid with PTSD. It appears that current PTSD treatment efficacy/effectiveness has reached a ceiling (Bryant, 2019) and that enhancing treatment response would require either improving provider’s fidelity and adherence to extant protocoled treatments in real-world settings and modifying and enhancing such treatments or, alternatively, developing new treatments specifically targeting the unique symptoms of PTSD that do not seem to respond well to extant treatments. It further appears that a focus of treatment development on dysfunctional memory processes, those processes that cause recurrent, involuntary, vivid, unwanted, and intrusive recollection of traumatic events, may serve to bring a breakthrough in treatment efficacy (Bar-Haim et al., 2021; Monfils & Holmes, 2018).
Supplemental Material
sj-pdf-1-cpx-10.1177_21677026211051314 – Supplemental material for A Sobering Look at Treatment Effectiveness of Military-Related Posttraumatic Stress Disorder
Supplemental material, sj-pdf-1-cpx-10.1177_21677026211051314 for A Sobering Look at Treatment Effectiveness of Military-Related Posttraumatic Stress Disorder by Ofir Levi, Ariel Ben Yehuda, Daniel S. Pine and Yair Bar-Haim in Clinical Psychological Science
Footnotes
Transparency
Action Editor: Pim Cuijpers
Editor: Jennifer L. Tackett
Author Contributions
O. Levi and Y. Bar-Haim developed the study concept. All of the authors contributed to the study design. Testing and data collection were performed by O. Levi, and Y. Bar-Haim performed the data analysis and interpretation with contributions from A. Ben Yehuda and D. S. Pine. O. Levi and Y. Bar-Haim drafted the manuscript, and A. Ben Yehuda and D. S. Pine provided critical revisions. All of the authors approved the final manuscript for submission.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.