
Abstract
It has been known for decades that mental-health disparities exist among minoritized groups, including race, ethnicity, sexual identities, gender identity and expression, ability, and others. Theories and frameworks that incorporate stressors unique to the experiences of minoritized groups, such as the biopsychosocial model of racism and minority-stress model, offer testable mechanisms that may help explain, in part, mental-health disparities. However, research addressing mechanisms of these disparities is still scarce and is not well represented in top clinical psychology journals. In this review, we critically examine the extent to which top-tier clinical psychology journals publish work examining mechanisms of mental-health disparities among minoritized populations. We found that very few studies that address mechanisms of mental-health disparities have been published in top clinical psychology journals. We examine potential reasons for this and discuss recommendations for future research.
Although few clinical psychological scientists would deny the importance of researching mechanisms of mental-health disparities, there is a notable absence of this type of work in some of our field’s premier journal outlets. In January 2020, we began our work on this article to invite our psychology colleagues to improve the ways in which our field’s research represents and addresses the needs and experiences of minoritized populations. This desire was largely fueled by our shared, frequent experiences of reviewing manuscripts that claim to examine mental-health disparities, only to find they simply repeat what we already know—rates of mental-health problems tend to be higher in minoritized groups relative to comparison groups (often White), with no mention of causes. Little did we know that in a few short months, we would all be living through COVID-19, with its disproportionate impact on minoritized (e.g., Black, Latinx, disabled) communities, and a summer that laid bare the long-standing impact of systemic racism and historical inequities, both manifestations of the unique and additional stressors experienced by minoritized people. Those discussions between friends and the visible impact of these health crises led us to take a critical and systematic look at how well our field’s top journals, critical outlets for scientific work, represent research examining mechanisms of mental-health disparities.
On the heels of the deaths of George Floyd, Tony McDade, Breonna Taylor, and many others, there have been renewed calls to action to dismantle systems of oppression that have marginalized people on the bases of race, sexual identity or orientation, gender identity, ability status, and other identities. Note that these calls to action are not new, and it would be a mistake to assume that they are simply because there is more public attention to them. Instead, what is newer is the forward-facing, widespread, and publicly accessible nature of these calls, many taking place on social media, which have permeated various industries, including media, higher education, medicine, and even the broader field of psychology (Brown, 2020; Roberts et al., 2020). We contend that a similar call to action is needed in clinical psychology specifically. We situate the present article and its focus on mental health among minoritized peoples across social identities within this larger movement of public accountability for the ways in which fields and actors within them either perpetuate or disrupt systems of oppression. Failing to name these systems and mechanisms of harm that disproportionately affect minoritized groups is one way that a field can reinforce and perpetuate inequity. Thus, the overarching purpose of this review is to critically examine the extent to which top-tier clinical psychology journals publish work examining mechanisms of health disparities among minoritized populations. As we describe in depth below, the top journals in our field carry prestige and undeniable “lift” to articles published within them. Thus, they are a power structure within our field that can either directly address or contribute to systemic discrimination.
Words have power. Thus, we have carefully chosen our terminology throughout this article. Instead of using the term minority, we predominantly use the term minoritized to refer to people whose racial, ethnic, sexual identity or orientation, gender identity, or other social-identity membership has been marginalized in society. We attempt to be as specific as possible when appropriate and broad enough in other places. We have selected these terms to move our field beyond language that problematizes the person rather than the language and sociopolitical context in which they exist. Despite this, our best efforts still probably fail to fully capture the inherent diversity of identities possible among our fellow humans. Furthermore, given the fluidity and evolving nature of language, we recognize that the terminology used in this text is a product of the current time.
Clinical Psychology Has Not Always Gotten It Right
Innovations emanating from clinical psychology are plentiful, and work derived from the field has had considerable positive impact on the lives of many people (e.g., cognitive behavioral therapy [CBT], dialectical behavior therapy). In charging the field to embrace diversity, equity, and inclusion more publicly, scholars within it must also recognize the ways in which clinical psychology has, at times, operated to the detriment of minoritized populations. The history of intelligence (IQ) tests provides one such example: IQ tests were used to support and uphold the beliefs of eugenicists whose movement was predicated on the false notion of White Anglo-Saxons’ race-based superiority (Washington et al., 2016). Throughout the early 20th century and continuing into the 1970s, IQ scores provided a basis for the forced sterilization of thousands of people, and most of these victims were people of color and people living in poverty. In the classroom, IQ tests have been used to disproportionately track Black students into special education courses and away from gifted programs (Washington et al., 2016). Contemporarily, the field continues to struggle with how to address the disproportionate diagnosis rate of schizophrenia among Black people. Using structured clinical interviews instead of unstructured interviews may marginally attenuate this disparity, but questions remain about whether diagnostic criteria itself is insensitive to the lived experiences of Black people (Olbert et al., 2018).
To give another contemporary example, Black youths remain more likely to be diagnosed with conduct disorder compared with their White peers (e.g., Baglivio et al., 2017). The misuse of clinical psychology’s tools has not harmed only marginalized races. Although the American Psychiatric Association categorized “homosexuality” as a mental disorder until 1973 and maintained references to same-sex attraction in the Diagnostic and Statistical Manual of Mental Disorders until 1987, clinical psychologists largely adhered to this conceptualization. By accepting and applying pathologizing labels to people who are not heterosexual and/or cisgender (i.e., lesbian, gay, bisexual, queer/questioning, transgender, and nonbinary people), clinical psychologists have also been complicit in the historical marginalization of these groups (Silverstein, 2009).
Highlighting the field’s role in past harms is not intended to shame its current members or to minimize attempts made to repair those problems. Instead, these examples should serve to remind clinical psychologists that our work does not stay within the academy. In attempting to understand the causes and correlates of mental illness and psychological adjustment, we do public work, and it is ahistorical to assert that such work can be divorced from its sociopolitical context. Given that the fruits of clinical psychology enter the public domain, we contend that psychologists should be intentional in how such work is conducted and disseminated, especially as it relates to those who have been underrepresented and/or marginalized.
Clinical Psychology Must Acknowledge and Respond to Mental-Health Disparities
Disparities in health status and in health care for marginalized groups are well documented (Bonvicini, 2017; Braveman & Barclay, 2009; DuBois, 2003; Fredriksen-Goldsen et al., 2014; Kawachi et al., 2005). In intervening on these disparities in the domain of mental health, it is critically important to recognize that the nature of disparities varies between and within marginalized groups. Although marginalized racial and ethnic groups tend to endorse lower overall rates of mental disorders than Whites (Breslau et al., 2006), such broad statements obscure the harms faced by these marginalized groups. Note that there are mental-health conditions, such as posttraumatic stress disorder and alcohol use disorder (Vaeth et al., 2017), for which rates are elevated among specific marginalized racial and ethnic groups (Alegría et al., 2013; Gone & Trimble, 2012), including schizophrenia and conduct disorder, as mentioned above. Even when rates of diagnosed mental illness are lower for marginalized racial and ethnic groups, there is evidence that these groups may experience a higher symptom burden along with a more severe and persistent course of mental disorder than their White counterparts (Breslau et al., 2006; Williams et al., 2007).
Similar nuances exist in the mental-health disparities present among individuals with minoritized sexual identities as well as transgender and gender-nonconforming (TGNC) populations. Data demonstrate the elevated risks for depression, anxiety, and suicide among individuals with minoritized sexual identities relative to heterosexual individuals, albeit the pattern varies by specific sexual orientation and gender (Plöderl & Tremblay, 2015; S. T. Russell & Fish, 2016). For example, a recent meta-analysis highlighted the often amplified mental-health burden faced by bisexual women relative to lesbian and gay individuals, and relative to bisexual men (Ross et al., 2018). Furthermore, a growing literature focuses on the distinct mental-health experiences of TGNC people compared with cisgender people within and beyond the lesbian, gay, bisexual, queer/questioning, intersex, asexual (LGBQIA+) community (Valentine & Shipherd, 2018). At a structural level, members of minoritized groups are less likely to have access to mental-health treatment, and when provided treatment, they may receive worse quality care than nonminoritized groups (McGuire & Miranda, 2008; Plöderl & Tremblay, 2015; Valentine & Shipherd, 2018). Note that mental-health disparities may be compounded when multiple minoritized identities are examined in tandem (Cyrus, 2017).
Clinical psychology largely has ignored and has not prioritized research on mechanisms that explain mental-health disparities. Some people may argue that clinical psychology as a discipline is primarily interested in individual differences and that structural issues are beyond the scope of the field. However, clinical psychology’s lack of focus on sociopolitical factors does not mean that they are not critical to understanding mental-health disparities between minoritized and nonminoritized groups of people. Buchanan and Wiklund (2020) made the point that clinical psychology has abdicated responsibility for external, sociopolitical factors in mental health to other allied disciplines (e.g., counseling psychology and social work). Consistent with their argument, we similarly suggest that understanding any one individual’s mental health requires acknowledging the context in which the individual exists. Other areas in clinical psychology, such as developmental psychopathology, acknowledge and embrace the transactional nature between the environment and individual behavior. Following from this, if the environment is systematically constructed to value one identity (e.g., cisgender, heterosexual, White) over another, then unique stressors faced by the minoritized individual are essential variables in the equation of their mental health.
Existing Models of Mental-Health Disparities
Psychological models that address mechanisms of health disparities among minoritized groups have existed for years. These frameworks emphasize the unique and excessive stress experienced by individuals with minoritized status or position. Slavin and colleagues (1991) developed the multicultural stress model, which adapted Folkman and Lazarus’s (1984) seminal transactional model of stress and coping by incorporating the role of culture in every aspect of the stress process, including one’s evaluation of stressors, appraisals, coping behaviors, and health outcomes. Likewise, Clark and colleagues (1999) presented the biopsychosocial model of racism, which posited that differential exposure to racism and race-based stressors and differential access to coping responses not only explain the disparities in health outcomes experienced by Black people but also account for intragroup variation in health outcomes within Black people as a racialized group. In this model, the authors distinguished between chronic and acute sources of racism and presented moderators (e.g., perceived control) and mediators (e.g., racism-specific coping) of the relationship between racism and health outcomes.
Criticizing social scientists’ “disproportionate interest in the underlying attitudes and forms of racism, and comparatively less attention paid to the experience of racism among those who are its targets,” Harrell (2000, p. 42) noted that racism should not be reduced “simply to an experience of stress” (p. 54) and presented a multidimensional conceptualization of racism-related stress that incorporates internal (e.g., racism-related coping styles) and external (e.g., social support) mediators of the effects of racism on health outcomes. Drawing on prior work and extending the social stress frameworks to people identifying as lesbian, gay, or bisexual (LGB), Meyer (2003) presented a comprehensive model that suggests that mental-health disparities among LGB individuals result from a confluence of (a) minoritized status and identity, (b) general stressors common to all individuals, (c) specific distal stressors (e.g., discrimination/violence), and (d) proximal stressors (e.g., expectations of rejection, internalized homophobia) unique to the minoritized individual. The paths between minoritized status/identity and stress can be further moderated by social support, available coping resources, and prominence and valence of minoritized identity (Meyer, 2003). Hendricks and Testa (2012) recently expanded Meyer’s model to focus on the additional stressors experienced by TGNC people (e.g., medical care discrimination, inability to access legal documents, nonaffirmation). Note that each of the stress models described herein depicts (a) an external stress event unique to minoritized individuals (e.g., discrimination) situated within a larger sociopolitical landscape and (b) an internal appraisal process (e.g., internalized homophobia) that are hypothesized to function as mechanisms of disparities. We refer to these external events and internal processes as key stress mechanisms for minoritized individuals throughout the remainder of this article.
Stress models that incorporate unique stressors faced by minoritized individuals offer compelling explanations for why a group of individuals exposed to systemic marginalization suffers from higher rates of mental-health disorders compared with a group that benefits from such oppressive systems. Indeed, these models offer testable, mechanistic explanations for the core imbalances that drive mental-health disparities. As others have noted (Marks et al., 2020), historically, research examining disparities between minoritized and nonminoritized groups failed to clearly recognize systematic oppression and properly contextualize a group’s unique stressors. Without this important grounding, explorations of mental-health differences between minoritized and nonminoritized groups have the potential to problematize a person’s status as a minoritized individual itself rather than the sociocultural or sociopolitical context in which it is situated. Indeed, this practice has resulted in many policies, models, and conclusions regarding racial and other minoritized identity disparities that adopt a deficit model (Helms et al., 2005). Although research has progressed since then in some areas (for an excellent review of risk and resilience of minoritized youths, see Marks et al., 2020), we contend that clinical psychology has clear areas for improvement in the area of mental-health-disparities research in some of our most important scientific outlets. Clinical psychology is not alone in this struggle. Indeed, a recent review of the developmental, cognitive, and social psychology literatures showed major gaps in inclusion of empirical studies examining racial disparities (see Roberts et al., 2020).
The Present Review
Overarching goals
Our main goals were to (a) examine how well represented empirical articles testing stress mechanisms of mental-health disparities unique to minoritized groups are in our field’s top journals and (b) evaluate the relative strength of these existing articles in these outlets. We included empirical studies that either (a) discussed or cited leading frameworks of stress for minoritized groups, such as the multicultural stress model (Slavin et al., 1991), the biopsychosocial model of racism (Clark et al., 1999), the multidimensional conceptualization of racism-related stress (Harrell, 2000), the minority-stress model (Meyer, 2003), or the gender-minority-stress model (Hendricks & Testa, 2012), or (b) examined a mechanism (i.e., mediator or moderator) of mental-health disparities. We elected to focus on top-tier clinical psychology journals for two main reasons. First, top journals are ranked as such because of the overall impact factor (IF) and expected reach of published articles. Limitations of the IF metric notwithstanding, the IF remains one of the leading metrics for authors to assess overall influence of articles in the field. Thus, there is an undeniable lift for articles associated with being published in a top-tier clinical psychology journal. Second, although there are important and more focused specialty journals, we argue that the work of understanding mechanisms of mental-health disparities is relevant to every aspect of clinical psychological science and for all who engage in research on mental health. Thus, the top clinical journals can and should represent the entire spectrum of work on mental-health disparities in our field.
Examining a proxy of systemic bias
Any examination of which manuscripts get published in any journal must include a discussion of systemic bias. Systemic bias toward scholars from underrepresented groups and work on topics deemed “niche” is likely to affect what ultimately gets published and where. For example, data demonstrate that R01 applications from African American/Black scientists are less likely to be discussed by study sections at the National Institutes of Health and that when they are discussed, they receive poorer impact scores than applications from White scientists (Hoppe et al., 2019). One possible source of this bias is that African American/Black scientists initiate investigations in topics at the community or population level that are less successful in peer review than applications focused on more mechanistic evaluations, despite evidence that reviewers’ impact rankings do not accurately predict which applications go on to make substantial impacts in the field (Hoppe et al., 2019). For the present review, the number of editorial board members who are minoritized individuals and/or conduct research in this area of journals may be one proxy of this systematic bias.
We considered attempting to code the perceived minoritized identities of the board members, but we decided not to take this approach because this would introduce our own biases into the process. Because we could not confirm individual identities without reaching out to each board member, we sought to examine the extent to which the editorial boards of the journals included in this review are made up of individuals whose primary or secondary research focuses on mental-health disparities in minoritized groups. We acknowledge that this may not be a perfect representation of the diversity within editorial boards, but we contend that board members that appreciate the nuances of work involved in mental-health disparities will be better equipped to assess and prioritize meritorious work. We also focused on current, not historical, composition of the editorial boards because the focus of a given reviewer’s program of research seemed to be the best proxy for how editorial boards may be currently influencing what gets published. 1
The next section describes our methods for identifying studies. Then, we describe the number of studies for each journal and describe the samples, outcomes, and methods in the Results section. We additionally present information about the editorial board composition in the Results section. In the Discussion section, we seek to answer the following questions:
To what extent are top journals in clinical psychology publishing articles examining stressors unique to minoritized individuals as mechanisms of mental-health disparities?
To what extent do extant published articles integrate and test models of stress that incorporate stressors unique to minoritized individuals?
Among the existing studies, what are some common pitfalls that future research can address?
What influence might editorial boards and the larger field have as gatekeepers of what gets published in top journals?
Finally, we offer specific suggestions for future research.
Method
Identification of top clinical psychology journals
To identify journals for this review, we consulted the Journal Citations Report as part of Clarivate’s Web of Science (Web of Science, 2020). We included the five journals with the highest IFs in the “Psychology, Clinical” category (as of 2019) that focused on empirical articles. This resulted in the following journals: Journal of Abnormal Psychology (IF = 6.484), Psychological Medicine (IF = 5.813), Clinical Psychological Science (IF = 5.415), Depression and Anxiety (IF = 4.702), and Journal of Consulting and Clinical Psychology (IF = 4.632).
Identification of potential articles for inclusion
We used three approaches to identify potentially eligible articles within each journal up to the time of writing this manuscript, December 2020. First, we separately searched terms including “multicultural stress,” “biopsychosocial model of racism,” “minority stress,” 2 and “multidimensional conceptualization of racism related stress” in quotes. This returned articles that mentioned these terms anywhere in the article. Second, we entered these seminal articles individually into Google Scholar and searched for articles that cited these articles in addition to the two articles that extended Meyer’s (2003) minority-stress model to TGNC people (Hendricks & Testa, 2012; Testa et al., 2015), that were also in our five target journals. Third, we expanded our search terms to capture other articles discussing minoritized identities and included, in quotes, “sexual minority,” “sexual identity,” “homophobia,” “heterosexism,” “gender minority,” “gender identity,” “transphobia,” “racial minority,” “racial identity,” “racism,” “disability identity,” and “ableism.”
For the first and second search methods, all empirical articles were eligible for inclusion. 3 For the remaining terms, we included empirical articles if (a) they were not duplicates from the initial or other search terms and (b) they went beyond simply reporting differences between groups (i.e., rates of diagnoses differing between White and Black participants) by including a potential mechanism that explained the differences. Here, we considered a “mechanism” to include any potential mediator or moderator of the association between the minoritized status and outcome under investigation. Articles were not included or excluded according to the outcome under investigation.
Composition of editorial board
As a proxy for how editorial board members may serve as gatekeepers and influence what types of work get published, the focus of each current (as of December 2020) editorial board member’s apparent research program was reviewed by trained research assistants. Using university websites, lab websites, publication records, curriculum vitas (as available), or stated focus of the editorial board member’s program of research, we coded whether the board member had an explicit or easily discernable (i.e., publication record focused on minoritized individuals’ mental health) minoritized individual focus or subfocus (yes/no) in their program of research.
Results
As shown in Table 1, 61 empirical articles were included in the present article. Initially, 45 articles were included from our first two search methods. An additional 16 articles were included in the review from the added search terms after removing duplicates and excluding (a) studies that lacked focus on mechanisms of disparities (e.g., reported only differences in rates) and (b) review articles. The majority (N = 37; 60.66%) of studies came from a single journal (Journal of Consulting and Clinical Psychology). Twelve studies (19.67%) from Psychological Medicine, eight studies (13.11%) from Journal of Abnormal Psychology, and two articles (3.28%) each from Clinical Psychological Science and Depression and Anxiety were included in the present review. Encouragingly, as is evidenced in Figure 1, rates of publication on mechanisms of mental-health disparities have increased over the past 17 years. More than half of articles (65%) have been published since 2015, and the highest total number was published in 2020 (N = 11).
Studies Included in the Present Review

Note: TGNC = transgender and/or gender nonconforming; LGB = lesbian, gay, or bisexual; NSSI = nonsuicidal self-injury; CBT = cognitive behavioral therapy; PTSD = posttraumatic stress disorder.
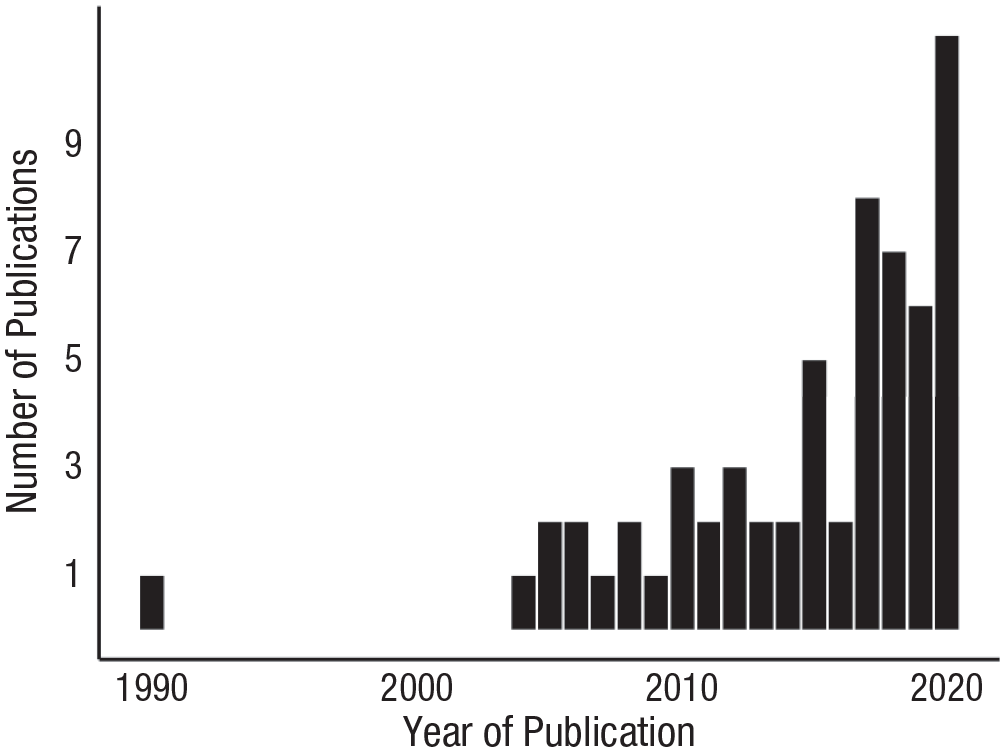
Number of publications per year in the top five clinical psychology journals that incorporated and/or test models of disparities for minoritized individuals.
Twenty-three (37.70%) were longitudinal, and 38 (62.30%) were cross-sectional. Most studies examined groups with minoritized sexual identities and/or TGNC individuals (N = 49; 80.33%). Other groups included hearing impaired (N = 1), immigrants (N = 1), and racial and/or ethnic minoritized groups (N = 7). A handful of studies included participants with minoritized sexual identities and/or TGNC identities and who were part of a racial minoritized group (N = 3). Psychological disorders or symptoms (e.g., major depressive disorder, generalized anxiety disorder, eating disorders, depression severity, anxiety severity) were the primary outcome in 39 (63.93%) of the included studies. Four studies focused primarily on self-injurious thoughts and behaviors, and five studies focused on substance use. Four studies focused on psychological well-being. Finally, one study each focused on treatment retention, treatment outcomes, rejection-sensitivity, risky sexual behavior, affect, relationship quality, body image, HIV risk, and neural correlates.
Regarding testing of stress mechanisms unique to minoritized individuals, 37 (83.78%) studies assessed a stress-related variable unique to minoritized individuals as a potential predictor, mediator, or moderator. Six studies did not measure a stress-related variable unique to minoritized individuals. Thirty (49.18%) and 27 (44.26%) studies measured a stress variable unique to minoritized individuals falling into the external stress event and internal stress process categories, respectively. Only 16 studies (26.23%) examined both an external stress event and internal stress process in their models. Main findings related to stress mechanisms unique to minoritized individuals are summarized in Table 1. Most articles included in this review cited Meyer’s minority-stress model. Far fewer studies (N = 4) cited the other models preceding Meyer’s that articulated stress processes unique to minoritized groups.
For the five included journals, the total number of current editorial board members was 453; only 30 individuals (6.62%) appeared to have a primary or secondary focus on mental-health disparities in minoritized populations. Forty-seven individuals served on multiple boards. Thus, the number of unique board members across these journals was 400, and 29 (7.25%) appeared to have a primary or secondary focus on mental-health disparities. Note that only one editor-in-chief or equivalent had a primary or secondary focus on mental-health disparities. Note that this journal (Journal of Consulting and Clinical Psychology) also had the highest number of studies included in the present review. Journal of Consulting and Clinical Psychology additionally had the highest proportion of individuals on the editorial board with a primary or secondary focus on mental-health disparities in minoritized groups (16.13% of editorial board). The other journals ranged from approximately 3% to 6%. At the associate/deputy-editor level, only five out of 94 (5.32%) had a stated or obvious secondary focus on racial and ethnic minoritized individuals.
Discussion
To what extent are top journals in clinical psychological science publishing articles examining mechanisms of mental-health disparities?
Overall, very few articles have been published that discuss, integrate, and examine stress frameworks that include stressors unique to minoritized individuals. Studies included in this review almost exclusively focused on samples with minoritized sexual identities and/or TGNC individuals and cited Meyer’s minority-stress model, which has been cited more than 9,000 times in the literature (as of March 1, 2021). Note that Meyer admitted his model pulled largely from prior scholars examining the effects of racism and sociopolitical factors contributing to mental-health disparities among people of color (Meyer, 2003). Yet very few studies in the present review focus on these earlier models or on racial and/or ethnic minoritized individuals’ experiences at all. Even after expanding our terms in a focused attempt to include more studies examining mechanisms of mental-health disparities in racial minoritized samples, we came up with alarmingly few studies. This is surprising because these race- and culture-based models are themselves well cited; Clark and colleagues’ (1999) biopsychosocial model of racism has been cited more than 3,000 times (as of March 1, 2021). This raises an important question: Why are these articles not present in our top clinical psychology journals?
This lack of representation in top clinical psychology journals likely reflects the confluence of factors from researchers, editorial boards, and peer reviewers. Indeed, if researchers do not view top clinical psychology journals as receptive outlets or outlets in which their work will receive the necessary expertise to critically evaluate it, they may pass to other journals. Indeed, Clark et al.’s (1999) model and Harrell’s (2000) model have been cited 69 and 55 times in Cultural Diversity & Ethnic Minority Psychology, respectively (as of March 1, 2021). If editorial boards are predominantly made up of individuals who do not have expertise in mental-health disparities, they may desk reject or fail to appropriately evaluate the articles scientific merit (see below for more on editorial boards). Relatedly, peer reviewers without adequate expertise in mental-health-disparities research may fail to appreciate certain aspects of a study that are strengths (e.g., a strong manuscript combining both qualitative and quantitative components) or may unfairly apply the same measuring rod for manuscripts in which mental-health disparities are ignored.
In short, top clinical psychology journals do not appear to be the primary outlets for critical and necessary work on mental-health disparities among minoritized groups. This is concerning given that mental-health disparities are the rule rather than the exception in the United States and other major developed countries. We are encouraged that it appears that the number of published studies on mechanisms of mental-health disparities among minoritized individuals are increasing over time in these top journals. Despite this recent growth, two key conclusions stand out: (a) Articles addressing mechanisms of mental-health disparities are not well represented in leading clinical psychology journals, and (b) because of this lack of attention, stakeholders must look elsewhere for expertise and guidance on factors driving mental-health disparities.
To what extent do articles integrate and test minority-stress frameworks?
The articles included in the present review varied in the degree to which the tested stress models incorporated incorporate stressors unique to minoritized or minority groups as well as in the degree to which these frameworks guided the conceptualization of the study, selection of measures, analysis, and interpretation of findings.
Recall that across all models, stress processes unique to minoritized groups were generally categorized as falling into either an external stress event (e.g., discrimination) or an internal stress process (e.g., internalized homophobia or racism). Some studies included in this review did not assess any type of stressor unique to minoritized groups (Balsam et al., 2005; Beard et al., 2017; Breslau et al., 2006; Butler et al., 2019; A. Y. Choi et al., 2020; K. W. Choi et al., 2017; Cochran et al., 2007; Cochran & Mays, 2009; Flentje et al., 2015; Keefe et al., 2018; Keo-Meier et al., 2015; Müller et al., 2018; Oginni et al., 2019; Pantalone et al., 2010; Rimes et al., 2019; Spittlehouse et al., 2020; Zietsch et al., 2012). For example, Oginni and colleagues (2019) examined self-esteem and depressive symptoms as mediators of the link between sexual identity and suicidal ideation or self-harm. This study used Meyer’s model to motivate study hypotheses and interpret results, but they did not measure key mechanisms of the framework. Relatedly, Keefe et al. (2018) included race as a moderator of treatment dropout between a prolonged exposure group and cognitive processing group and found that being a racial minoritized individual was associated with greater dropout in prolonged exposure relative to cognitive processing therapy. They mentioned stressors unique to minoritized individuals in the discussion as possibly accounting for this difference, but they did not include any of the proposed stress variables or expand on how stressors unique to minoritized individuals may help account for this. Discussion of stress mechanisms unique to minoritized groups that may be at play is an improvement over studies that simply report differences between minoritized and nonminoritized groups. However, at this stage, it is well established that there are mental-health disparities, and it is highly unlikely that these are biologically driven. Thus, the burden is on researchers to more carefully design their studies to answer these mechanistic questions.
Many studies that did aim to specifically test stress models with stressors unique to minoritized individuals examined some components but not comprehensively. For example, several studies assessed only the external stressors (Boehmer et al., 2012; Frisell et al., 2010; Frost, 2020; Gevonden et al., 2014, 2015; Livingston et al., 2017; Pachankis, Williams, et al., 2020; Post et al.,2021; Rhew Isaac et al., 2017; Rodriguez-Seijas et al., 2019; S. T. Russell & Fish, 2016; Whitton et al., 2018; Zapolski et al., 2016). These external stressors were described as objective stressors, such as discrimination and violence (Meyer, 2003). 4 For example, Whitton and colleagues (2018) measured frequency of lesbian, gay, bisexual, and transgender (LGBT) victimization experiences and found that being in a relationship reduced the negative association between victimization and psychological distress. Livingston et al. (2017) used an ecological momentary assessment (EMA) design with assessments six times a day and found that discrimination experiences were associated with increased nicotine and substance use within the same measurement window and discrimination two measurement periods earlier. These collective studies generally found that external stressor components of stressors unique to minoritized individuals help explain, in part, linkages between minoritized status and negative outcomes.
Another set of studies examined only internal stress processes (Budge et al., 2013; Fox et al., 2020; Johnson et al., 2008; Millar et al., 2016; Pachankis & Goldfried, 2010; Pachankis, Cochran, & Mays, 2015; Pachankis et al., 2008, 2011; Pachankis, McConocha, et al., 2020; Schrimshaw et al., 2013). Internal stress processes are more person centered and related to self-identity (Meyer, 2003). In relationship to individuals with minoritized sexual identities and/or TGNC individuals, internal stress processes can manifest in one’s interaction with the external environment and shape a person’s internal experience through expectations of rejections, which leads to concealing one’s identity because of fear of harm or internalizing homophobia (Meyer, 2003). Recently, Pachankis, McConocha, et al. (2020) examined an evidence-based, cognitive-behavioral treatment for women with minoritized sexual identities. This study employed careful screening of each facet of internal stress processes outlined by Meyer, including concealment, internalizing homonegativity, and expectations of rejection for sexual identity or orientation. They found small effects of treatment on reductions in internal stress processes. Fox et al. (2020) investigated mental health among adolescents with minoritized sexual identities and TGNC adolescents and children and assessed expectations of rejection, gender identity acceptance, and disclosure of identity to friends. They did not report assessing these similar internal factors in the youths with minoritized sexual identities. Note that this group examined the interaction of race and ethnicity on these internal stress factors and found that Black and Latinx TGNC youths were about half as likely to have disclosed their gender identity, but Black TGNC minoritized youths expected less rejection from family because of their gender identity (Fox et al., 2020). These two studies show strong assessment of internal stress factors suggested by stress models that include stressors unique to minoritized groups.
Finally, several studies assessed both the external stress events and internal stress processes (Feinstein et al., 2012, 2017, 2018, 2019; Karlsen et al., 2005; Kimmel & Mahalik, 2006; Lehavot & Simoni, 2011; Pachankis & Bränström, 2018; Pachankis, Hatzenbuehler, et al., 2015; Sarno et al., 2020; Smith et al., 2020; Testa et al., 2017; Timmins et al., 2018; Vincent et al., 2017). A few of these studies evidenced strong assessment of both external and internal factors (e.g., Pachankis, Hatzenbuehler, et al., 2015; Sarno et al., 2020; Testa et al., 2017; Timmins et al., 2018), whereas others used single items to capture each factor (e.g., Karlsen et al., 2005; Kimmel & Mahalik, 2006). These studies allow for examining independent and interactive effects of both external and internal factors. However, we note that no studies examined interactions between external and internal factors.
Across all studies, a few key features distinguished methodologically strong articles. Studies that account for both general stressors and/or distress in addition to unique stressors for minoritized individuals allow for conclusions about distinct processes for minoritized samples (e.g., Dyar et al., 2020; Feinstein et al., 2018; Livingston et al., 2017). The use of longitudinal designs, particularly those with EMA (Feinstein et al., 2017; Gevonden et al., 2015; Livingston et al., 2017), are critical in testing these stress mechanisms. Furthermore, longitudinal designs allow for expanding tests of these stress models by examining additional processes that are affected by stressors unique to minoritized individuals and increase subsequent risk for psychopathology. For example, Smith and colleagues (2020) found that higher rates of victimization, microaggressions, and internalized homophobia predict greater rumination; in turn, greater rumination predicted higher depression. This identifies additional targets for intervention (in the prior example, rumination) for individuals exposed to stressors unique to minoritized groups. Finally, studies that address intersectionality can capture stressors uniquely faced by identifying as a member of multiple minoritized groups (e.g., Jackson et al., 2020; Rodriguez-Seijas et al., 2019; Whitton et al., 2018).
The fact that the included studies even mention stress models that incorporate stressors unique to minoritized individuals and examine sources of potential mechanisms is a substantial improvement over the vast number of studies that note only disparities among minoritized and nonminoritized groups. Therefore, each of the included studies can be seen as an important and necessary contribution to the literature on mental-health disparities. However, these studies also share some common pitfalls that we review next. These pitfalls are noted in the spirit of advancing research in this area.
Among the existing studies, what are some common pitfalls that future research can address?
Despite variations in the specific constructs assessed and populations included, several issues frequently arose across the set of articles that weaken their ability to test mechanisms of mental-health disparities but offer important directions for future work. In highlighting these issues, we hope that future researchers proactively take them into consideration when conducting research with minoritized populations. Critically, this is not just for researchers who focus efforts on mental-health disparities; we encourage any author or research group who enrolls more than nonminoritized populations (i.e., White, straight, cisgender people) to carefully consider these pitfalls when designing studies and choosing whether to evaluate differences among minoritized groups in their samples.
Pitfall 1: lacking specificity of constructs
To accurately capture the ways in which experiences associated with minoritized status affect mental health, psychologists must assess them with specificity. Whereas the majority of measures of experiences unique to minoritized individuals (e.g., discrimination, expectations of rejection) in the studies explicitly named the cause (e.g., discrimination on the basis of race, expectations of rejection because of sexual identity or orientation), several did not (e.g., Frisell et al., 2010; Post et al., 2021). For example, Frost (2020) examined routine discrimination among a sample of migrants in the United Kingdom using the Everyday Discrimination Scale (Williams et al., 1997) but excluded Stage 2 of the measure, which requires participants to attribute the reasons for their unfair treatment. Note that conclusions drawn from the article focus on the role of migrant status as the source of minoritized stress, although the sample includes a sizable percentage of people who may experience unique stress because of other social-identity categories (e.g., 31.5% racial minoritized individuals, 10.6% individuals with minoritized sexual identities). It is likely that the discrimination that these participants endorsed was due, in part, to their migrant status. However, it is also plausible that their race, sexual identity or orientation, or a different marker of social identity was the driving force behind their discrimination.
Gevonden et al. (2015) asked about discrimination in a sample that included hearing-impaired individuals, but it was not clear that the discrimination assessed was due to being hearing impaired. Furthermore, this group did not actually report results of discrimination as a mediator or moderator of minoritized status and outcomes. Likewise, a study by Boehmer and colleagues (2012) included a measure of discrimination in a sample of women breast cancer survivors of varying sexual identities, but the reason for the perception of discrimination was not clear despite questions about various potential reasons why (e.g., sexual identity or orientation, cancer status). Other studies assessed bullying, but the cause of this bullying was not explicitly asked (e.g., K. W. Choi et al., 2017; Gevonden et al., 2014; Post et al., 2021). Unfortunately, without calibrating the measures used in a study to the specific experiences under investigation, conclusions about the nature of the emergent relationships and future targets of intervention are compromised.
Pitfall 2: failure to account for universal experiences
In addition to assessing stressors unique to minoritized individuals with specificity, psychologists must also account for related constructs whose omission could challenge inferences about the influence of stress unique to minoritized individuals. Beyond the unfairness of experiencing stressors because of a social identity, one of the particularly insidious aspects of stress unique to minoritized individuals is that it occurs on top of the general stress that we are all open to, regardless of minoritized status (Meyer, 2003). Across the studies reviewed, researchers inconsistently included measures of universal stressors that could contextualize their findings about stress unique to minoritized individuals. Dyar and colleagues (2020) noted that relatively few studies in the broader stress literature are capable of parsing the effects of stress unique to minoritized identity from general stress. However, when such measures were incorporated into the studies reviewed here, they often reinforced the robust relationships between stressors unique to minoritized groups and psychological outcomes above and beyond the role of general stressors (Dyar et al., 2020; Feinstein et al., 2018, 2019).
Researchers do not have to include universally applicable processes (e.g., emotion dysregulation, general stressors) in their work solely to demonstrate the validity of stressors unique to minoritized individuals. Indeed, incorporating these universal mechanisms can also highlight additional targets of intervention that, although not unique to minoritized groups, are still pertinent to study. For example, in several of their efficacy trials, Pachankis et al. (2015) and Pachankis, McConocha, et al. (2020) complemented their examination of stressors with “universal risk processes” (e.g., rumination, emotion dysregulation), which provided them the opportunity to explore general and minoritized individual specific, CBT-relevant mediators of change in mental-health problems. Given that stressors unique to minoritized individuals confer extra burdens to bear and added challenges to navigate, psychologists should conceptualize them as such in their work and include them as a set of stressors to be modeled in conjunction with universal stressors.
Pitfall 3: methodological limitations
Although cross-sectional studies are often a necessary first step in any given area of literature, they are inherently limited in terms of the conclusions that can be drawn. This is particularly true for studies assessing stressors unique to minoritized individuals. Some strong longitudinal designs stand out in the present article, including those that use EMA to examine stressors unique to minoritized individuals, everyday stressors, and outcomes in real time (e.g., Livingston et al., 2017). These types of studies will allow for more precision in understanding how both external and internal stress factors affect outcomes for minoritized individuals. Note that both external events and internal stress processes are directly and inextricably linked to the sociopolitical context in which a minoritized individual exists. Thus, although longitudinal design will help us understand how stressors and outcomes interact in space and time, they will not provide us with a panacea treatment to target a specific group of people without widespread sociopolitical change toward justice.
Without assessing any stressors unique to minoritized individuals, one cross-sectional study concluded that stress mechanisms unique to minoritized individuals may not be a supported reason for mental-health disparities because genetic factors and shared family environments largely accounted for associations with increased depression (Zietsch et al., 2012). Frisell et al. (2010) similarly concluded that genetic factors are likely more strongly associated with risk for psychiatric disorders than are stressors unique to minoritized individuals. Note that this study used a single item assessing whether any discrimination had occurred. In comparison, Timmins and colleagues (2018) assessed stressors unique to minoritized individuals and found that environmental factors specific to the twin with a minoritized sexual identity (e.g., self-stigma) explained, in part, greater rumination than the heterosexual twin. Note that all three studies were cross-sectional. Although twin designs have inherent strengths in the ability to assess genetic and environmental contributions, it is difficult to quantify the effects of stressors unique to minoritized individuals perpetrated to one twin and not the other. In other words, if one twin is victimized because of their sexual identity, it is highly unlikely that this will not also, in some way, affect the other twin. Therefore, it is improbable that these designs are “pure” tests of minority stress for individuals with minoritized sexual identities.
In addition, we must acknowledge that researchers who identify as part of minoritized groups and conduct research in this area face numerous structural barriers to conducting this research. Factors affecting the researchers include lower funding rates for grant applications and additional service burdens within departments. The research itself faces barriers to participation, including populations who may not have time available to participate, resources to access participation, or reason to trust in research studies. These factors likely limit the scope and resources available to conduct methodologically rigorous work in this area. Addressing these factors should not fall solely on the researcher but also the systems supporting these researchers (e.g., academic departments).
Pitfall 4: failure to incorporate intersectional lens
Throughout this article, we have discussed members of minoritized groups, largely separated by identity (e.g., racial and/or ethnic minoritized groups or groups with minoritized sexual identities and/or TGNC groups), and there has been passing mention of individuals who embody multiple marginalized identities. Unfortunately, this approach is consistent with much of the way in which minoritized populations are studied in the psychological science literature. In our review, only a small proportion of articles focused on the experiences of people living at the intersection of multiple minoritized identities, and all were recent contributions (Frost, 2020; Jackson et al., 2020; Rodriguez-Seijas et al., 2019; Vincent et al., 2017). These inquiries are critical because the lived experiences of people who are multiply marginalized are distinct from those of people who are members of a single minoritized group. For example, individuals with both minoritized sexual and racial identities likely experience their race in the context of their sexual identity, and their sexual identity will likely be racialized as well. Indeed, prior work has found that Black individuals with minoritized sexual identities and/or TGNC identities report experiencing racism from within the LGBTQIA+ community and homophobia from within the Black community. Failure to capture these stressors (both racialized sexual identity related and sexual identity and/or TGNC-filtered race related) would miss the mark in understanding potential contributors to these individuals’ mental health.
In the present-day literature, the term intersectionality has been used to understand the unique oppression faced by individuals occupying multiple oppressed identities. This term, coined by legal, feminist, and critical-race scholar Kimberle Crenshaw (1989), which has roots reaching much further back, was originally created to articulate the particular legal challenges faced by Black women in the workplace but has been applied to other multiply oppressed groups. Note that this framework posits that the experiences of multiply marginalized people are not additive but are interlocking and mutually constructive (Crenshaw, 1991). Thus, they should be examined concurrently. Capturing this notion particularly well, Jackson et al. (2020) anchored their measures of negative and positive identity experiences to “being both Black and LGBQ” rather than assessing race and sexual orientation identity separately. Furthermore, these authors’ inclusion of a measure of identity conflict provides a more robust view of another representation of stress that may be unique to members of multiply minoritized groups—the challenge to ameliorate potential conflict between minority identities.
Our review of the few studies that focused on people with multiple minoritized identities highlighted the importance of the study design in understanding stressors unique to minoritized identities and mental health among these individuals. Both Vincent and colleagues (2017) and Jackson and colleagues (2020) recruited samples that exclusively comprised Black individuals with minoritized sexual identities, although their different approaches yielded nuanced differences in interpretation. Although findings from the former may be understood as the experiences related to having a minoritized sexual identity within a racial minority group, as mentioned above, the latter may be understood as the experiences of people who are jointly sexually and racially minoritized. Arguably, findings from both studies are racialized given the all-Black samples, but the framing of the first may provide subtle messaging that the experiences of racially and sexually minoritized status can be separated. Other studies relied on samples that included people with a single minoritized identity, no minoritized identity, and multiple minoritized identities (Fox et al., 2020; Rodriguez-Seijas et al., 2019). These studies were able to provide information about differences between groups but were less able to contextualize their findings, sometimes yielding results that were difficult to interpret. For example, Rodriguez-Seijas and colleagues (2019) found that White individuals with minoritized sexual identities in their sample reported greater race/ethnicity-related discrimination than White heterosexuals. This small but statistically significant effect may be an artifact of measurement but highlights the need to strongly consider the constructs incorporated in these inquiries along with the overall study design.
Note that our discussion here assumes that the authors of these studies specifically reported all the possible minoritized identities of the participants; however, it is possible and likely that some participants belong to multiple minoritized identities that were either not assessed, not reported, or not viewed as minoritized by the authors. Examples that are possible but not exhaustive include womanhood, poverty, refugee status, disability, and others that may also interact with more commonly reported and investigated race, ethnicity, sexual orientation, and gender identity.
Other concerns
Although this issue was not widespread among the included studies, it is concerning that at least three articles miscategorized childhood maltreatment as a stress mechanisms unique to minoritized individuals either overtly or inadvertently (Gevonden et al., 2014; Post et al., 2021; Zietsch et al., 2012). Gevonden and colleagues (2014) explicitly named childhood maltreatment as a stress mechanism unique to minoritized individuals, whereas Post et al. (2021) set up their theoretical argument for studying child maltreatment with Meyer’s minority-stress model. Zietsch et al. (2012) explored “the effect of adverse childhood experiences and other variables thought to be associated with sexual orientation” (p. 526) as potential factors explaining differences in rates of depression among twins discordant for sexual orientation. Although studies have demonstrated that rates of child maltreatment are more frequently reported among individuals with minoritized sexual identities (Friedman et al., 2011), it does not logically follow that this should be considered a stress experience unique to minoritized individuals. Indeed, the implication here is that something about child maltreatment among individuals with minoritized sexual identities is uniquely associated with poor outcomes when in reality, child maltreatment increases risks for poor mental-health outcomes in general (Green et al., 2010; McLaughlin et al., 2010). Child maltreatment may be one factor that increases risk for poor outcomes among individuals with minoritized sexual identities, but it is not a stressor unique to minoritized individuals as conceptualized by stress models included in this review.
What influence might editorial boards and the larger field have as gatekeepers of what gets published in top journals?
Rigorous research that is focused specifically on minoritized populations frequently are designated as niche and relegated to specialty journals. Note that it is our (L. M. Adams, A. B. Miller) opinion that specialty journals (e.g., Journal of Black Psychology, Psychology of Sexual Orientation and Gender Diversity) are critically important to advance research in their respective areas. At the same time, it is difficult to argue against the importance of the lift received by articles published in top-tier journals within clinical psychology. We contend that articles addressing mental-health disparities and rigorously testing stress frameworks that incorporate stressors unique to minoritized individuals are critical to our most highly cited journals.
One factor that is perhaps easier to comment on is the makeup of editorial boards. Specifically, both identity as a scholar from a minoritized group and a focus on research in this area likely influence what gets published in the journal. As we outlined above, we focused on the board members’ program of research as a proxy of representation, although we acknowledge that this approach is inherently limited. In the current top five journals in clinical psychology (as of 2020), fewer than 7% of individuals on the collective editorial boards are researchers who have a stated primary or secondary focus on health disparities in minoritized populations. Even more concerning, the initial gatekeepers (editors, action/associate editors) are even less likely to focus on mental-health disparities in their own programs of research. The importance of the editorial board’s composition should be underscored. It is likely that the systemic racism and biases, even those that are implicit, ever present in society likely also operate within editorial board members and editors. The degree to which these biases influence publication of stress mechanism work for minoritized groups is an open question worthy of investigation. Nevertheless, efforts to diversify editorial boards should begin immediately. Note that it is possible that individual editorial board members are well connected with other colleagues who focus more specifically on mental-health disparities work. Theoretically, they could enlist these colleagues’ help in finding reviewers equipped to provide a rigorous and fair review.
However, we contend that increased representation on the board will likely result in two concrete changes: (a) More researchers conducting studies on mental-health disparities in minoritized populations will submit their manuscripts to these top five journals, and (b) the quality of peer reviewers (and subsequently published studies) will improve. For example, Journal of Consulting and Clinical Psychology has an editor who has a stated focus on the full spectrum of gender and sexuality. Note that this editor-in-chief’s journal had the highest ratio of editorial board members who focused on health disparities among minoritized groups, and this journal also had the highest number of studies that met inclusion criteria for the present article. Although this could be a coincidence, it is equally plausible that having an editor and editorial board members who focus on minoritized groups in some capacity has a direct influence on the number of studies addressing disparities being published. The net benefit of increased representation on the boards should result in critical studies addressing mechanisms of mental-health disparities in our top journals in the field.
Recommendations
We believe that it is critical for studies addressing mental-health disparities to incorporate frameworks that have been offered in other areas of research to guide study design and selection. In addition, journals have an important responsibility in this arena as well. In this section, we expand on specific recommendations.
We encourage editors, board members, reviewers, and authors to consult the excellent recommendations offered recently by Roberts et al. (2020). Many of these same recommendations apply here. In brief, Roberts et al. offered specific steps to increase diversity and representation of racially minoritized individuals on editorial boards, as lead authors, and in research samples. Here, we offer some additional recommendations specific to improving research on mental-health disparities across multiple minoritized populations.
Make editorial boards more diverse
Consistent with Roberts et al. (2020), we strongly recommend that journals take immediate action to diversify editorial boards. We did not specifically examine the demographics of individual editorial board members. However, we did examine the apparent focus of individual editorial board members’ research programs. Not surprisingly, most of the editorial board members do not have a primary or even secondary focus on mental-health disparities. It bears repeating that the journal with the largest proportion of editorial board members focusing on mental-health disparities also contributed the largest number of studies to the present review. Thus, we recommend that in addition to increasing diversity in terms of demographics, journals should seek to increase the number of individuals with research programs on mental-health disparities.
Note that simply diversifying editorial boards does not address the myriad systemic factors that shape access to funding and resources necessary to conduct mechanistic and longitudinal research on mental-health disparities. We view the charge to make editorial boards more diverse as an actionable first step that editors can begin to change immediately. Larger and more complex problems such as funding disparities will take additional changes to resolve. However, note that by serving on an editorial board, a minority individual could become more likely to be asked to serve on a grant funding review agency, thereby indirectly addressing systemic biases in funding.
Assess mechanisms driving mental-health disparities
We strongly encourage authors to assess mechanisms likely underlying the apparent differences between two groups. Minoritized identity is a proxy for other factors driving the disparities. There is nothing inherently causal about the color of someone’s skin or someone’s sexual orientation in terms of mental-health difficulties. Rather, it is the sociopolitical context in which someone exists that drive endless and complex transactions between the individual and the environment. The downstream effects of this are the mental-health disparities we see in our studies and clinics. Measuring demographics in one’s sample is a great start; however, researchers must do the work to understand mechanisms driving the differences in their samples. Simply reporting these differences is no longer sufficient. It is up to journals to prioritize publishing mechanistic studies, which is our next point.
Prioritize publishing studies that address mechanisms of mental-health disparities
Journals must take a strong stance to prioritize work that publishes mechanisms of mental-health disparities. This includes requiring authors to go beyond simply reporting differences in rates of disorders and even common underlying mechanisms of psychopathology, such as emotion dysregulation. A study reporting emotion-dysregulation differences between individuals with minoritized sexual identities and heterosexual individuals and subsequent psychopathology is interesting, but what are the individual and sociopolitical factors likely driving differences in the emotion regulation?
Note that individual-level mediators are probably only one small driver of mental-health disparities. Note that even among the handful of studies included in this review, not all measured an individual-level mediator (i.e., discrimination, internalized homophobia). As Neblett (2019) offered in his recent article on racism and racial mental-health disparities, we must move beyond focusing on individual mechanisms alone to assessing institutional, cultural, and structural/systemic racism. We believe this applies to other minoritized groups as well.
We note that there absolutely is high-quality work on mechanisms of mental-health disparities being conducted in the field, not just within journals within psychology (e.g., Cultural Diversity and Ethnic Minority Psychology, Journal of Black Psychology) but also in complementary fields (e.g., sociology, African American studies, counseling psychology). These are critically important outlets that have published some of the most important studies in this area. At the same time, we note that our field operates under a token economy that places higher value on what is viewed as more “prestigious” (code for higher IF) outlets. We assert that work addressing mechanisms of mental-health disparities deserves full and equal consideration in top journals as well as what is often referred to in coded language as specialty journals.
Reassess and adjust the measuring rod of what counts as a rigorous study
Prioritizing research on mechanisms of mental-health disparities will require adjusting or reimagining the measuring rod of what “counts” as rigorous science. Note that we specifically do not mean “lowering the bar.” We have outlined, in this article, examples of methodologically strong studies that still have room for improvement. Rather, we encourage editorial boards to consider that rigorous studies on mental-health disparities may not look like other studies published in the journal not considering mental-health disparities. For example, it may not be possible to have a sample size of several hundred or thousand, depending on the group under investigation. It may not make sense to have a comparison group when the question is about the strength of the association between internalized homophobia, experiences of discrimination, and psychopathology symptoms.
Historical context also may affect the amount and quality of work in a given area. For example, Black people were not admitted to psychology graduate programs in substantial numbers until the late 1970s and early 1980s, and research focused on racial and ethnic minoritized groups was largely deficit focused in the absence of a collective of racially diverse scholars in the field (for an excellent review of the development of African American psychology, see Holliday, 2009). It was not until 1985 that the National Institute of Mental Health began funding work focused on racial and ethnic minoritized groups in each of its divisions and not until 2016 that the National Institutes of Health formally designated sexual and gender minoritized identities as a health disparity population. Given that funding is often a barrier to support large-scale, “traditionally rigorous” research, funding priorities, in part, shape the nature of work being done.
Relatedly, the apparent strength of any given methodology is likely tied to the degree to which investigators who do this type of research are faced with environmental challenges. For example, a researcher investigating mental-health disparities may not be able to obtain large grants to fund their research if it does not fit with the current priority areas of funding sources. Pressure from departments and colleagues to focus on less niche research may influence a researcher’s choices in designing studies. Furthermore, it can be more challenging to engage and retain minoritized groups in research. These factors combine to create additional barriers for researchers interested in investigating mental-health disparities among minoritized groups. Top journals in our field can help mitigate these barriers by prioritizing and elevating traditionally overlooked studies.
Adopt an intersectional lens
An additional recommendation following from the discussion above is that researchers should aim to expand beyond viewing and studying people as though they represent only a single minoritized identity. To date, most of the research focused on minoritized groups has used a single-issue framework (e.g., race or sexual identity and/or TGNC). Like calls for interventions to be tailored to address questions of statistical moderation—such as “For whom?” and “Under which circumstances?”—we and others contend that it is well past time for psychologists to examine how the experiences of minoritized individuals vary and are uniquely constructed in conjunction with other minoritized identities (e.g., disability status).
Note that it takes intentional work to design a study that fully addresses the experiences of multiply minoritized people, and this work must be done in the development phase of the study, not during data analysis. Furthermore, epistemological, conceptual, and practical questions about how well our current statistical methods for quantitative data analysis can appropriately handle research that is truly grounded in an intersectional framework remain (Cole, 2009; Else-Quest & Hyde, 2016a; Richman & Zucker, 2019). Nonetheless, in our work to serve the broader community in all of its diversity, our science must also reflect this. Echoing Buchanan and Wiklund (2020), clinical psychology must adopt an intersectional lens or be left behind other fields that will address this critical need. Specific guidelines on how researchers can adopt an intersectional lens in their work vary, although all recommendations are grounded in the idea that there must be an explicit emphasis on power dynamics and the social-structural context when exploring the lives of minoritized people. Else-Quest and Hyde (2016a, 2016b) provided practical tips for employing an intersectional analytic approach through statistical techniques such as moderated-mediation and person-centered analyses. In their response to these tips, Bowleg and Bauer (2016) provided several additional recommendations, including that researchers (a) measure and incorporate structural elements (e.g., education public funding, neighborhood violence, wealth inequity) into their design to link individuals’ experiences to broader contexts; (b) use other sampling and recruitment techniques (e.g., respondent driven) to address the structural barriers to accessing populations who are not as readily accessible, making their experiences “empirically invisible”; and (c) consider using mixed methods approaches in their work given that the methodologies typically used in our field may not be ones that work well for research with minoritized communities.
Limitations
The present review offers a critical evaluation of the degree to which articles addressing mechanisms of mental-health disparities among minoritized groups, such as stressors unique to minoritized individuals, are represented in top clinical psychology journals. In addition, we note strengths and limitations of extant studies with recommendations for future work. However, some limitations are worth noting for the present review. First, although we expanded our initial search terms, we did not use an exhaustive list. Instead, we offer an initial, focused examination. Future reviews could expand terms to potentially yield a larger set of studies and supplement our conclusions. Second, we did not conduct a meta-analysis, which could provide useful information regarding the magnitude of effects specified by these frameworks. Although several features of the research we reviewed may complicate such an endeavor (e.g., inconsistent inclusion of stressors, varying populations of interest), future work could consider such a significant contribution to the literature. Third, articles in our review, and thus much of our discussion, focused predominantly on individuals with minoritized sexual identities and/or TGNC individuals and on racial and ethnic minoritized individuals. This highlights the need for work focused on other minoritized communities (e.g., people with disabilities) to be better represented in top clinical psychology journals as well. Relatedly, we used the terms individuals with minoritized sexual identities and TGNC, which encompass numerous identities and subgroups. We note that the large majority of these studies focused on gay men. Thus, even within minoritized identities, there is room for more work. Finally, it is possible that our screening of the editorial board members’ research foci did not fully capture the degree to which they engage in work focused on mental-health disparities. Even so, it is worth considering that the absence of a clear, explicit emphasis of such work among editorial board members may still act as a barrier to research focused on mental-health disparities being perceived as favorable to these outlets. We also were unable to confirm individual board members’ identity, and thus, we may not have fully captured the representation of individuals from minoritized groups.
Concluding remarks
We hope that we provided a compelling call to action for our psychology colleagues to prioritize conducting, publishing, and elevating research that addresses mechanisms of mental-health disparities among minoritized groups. We specifically hope that this article can be useful to nonminoritized researchers to identify places they can strengthen their own programs of research and assess stressors unique to minoritized groups. This work cannot and should not fall solely to members of each respective community (e.g., Black researchers investigating Black mental-health disparities). Regardless of how involved the work is—start somewhere. Our strongest conclusion from this review is that it is no longer sufficient to include minoritized status in the absence of understanding the sociocultural and sociopolitical context in which the individual exists. Race, sexual orientation, gender identity, and other “demographic” variables rarely explain the differences observed. Rather, they are proxies of much larger and more complex individual and sociopolitical factors. Our current historical context demands that we address these factors in our top journals.
Footnotes
Acknowledgements
We are grateful to Adrienne Bonar, Christian Fary, Nathan Hacker, and Kinjal Patel, who served as research assistants on this project. At the time of writing, one author self-identified as a cisgender, heterosexual Black woman and one author self-identified as a cisgender, gay White man.
Transparency
Action Editor: Erin B. Tone
Editor: Kenneth J. Sher
Author Contributions
Both authors contributed equally to this article from conceptualization, reviewed articles, and prepared the manuscript for publication. Both authors approved the final manuscript for submission.