
Abstract
We examined longitudinal associations of resting heart rate (RHR) and general intelligence (IQ) with two psychopathology models (correlated factors and general factor model). RHR and IQ were measured during conscription (mean age = 18.23 years; N = 899,398 Swedish males). A correlated factors model of register-based outcomes (including 10 psychiatric diagnoses, criminal convictions, and prescription of anxiolytic medications; mean age at follow-up = 43.09 years) identified internalizing, externalizing, and psychotic dimensions; the general factor model additionally identified a general dimension. All correlated factors were inversely associated with IQ; however, the general factor model showed that several of these associations were attributable to general variance rather than specific variance. In both psychopathology models, RHR weakly but significantly predicted higher internalizing but lower externalizing problems. Intelligence might be a transdiagnostic risk factor for any form of psychopathology, and the internalizing and externalizing spectra might be differentiated by psychobiological processes related to sensitivity to punishment.
In recent years, it has been hypothesized that a general factor and several specific factors influence mental health problems (Caspi & Moffitt, 2018; Lahey, Krueger, Rathouz, Waldman, & Zald, 2017). Although this model is useful because it can account for comorbidity among mental health problems, it is still unclear what the general and specific factors actually measure (Bonifay, Lane, & Reise, 2017; Caspi & Moffitt, 2018; Snyder & Hankin, 2017; van Bork, Epskamp, Rhemtulla, Borsboom, & van der Maas, 2017; Widiger & Oltmanns, 2017). There is growing evidence, however, that the general factor of psychopathology is associated with lower intelligence and greater negative emotionality, impulsivity, and atypical thinking (Carver, Johnson, & Timpano, 2017; Caspi & Moffitt, 2018; Lahey et al., 2017; Tackett et al., 2013). Much less is known about the nature of the specific latent factors of psychopathology identified in general factor models. For example, it is unclear what psychobiological processes are associated with specific internalizing problems, such as depression and anxiety, independently of general distress and impairment.
The first of three goals of this study was to test the prediction that individual differences in intelligence is one of the transdiagnostic factors that nonspecifically increases risk for any form of psychopathology (Caspi & Moffitt, 2018; Lahey et al., 2017). In a study of more than 1 million Swedish men who completed an intelligence test during conscription at age 18, scoring 1 SD below the mean increased the risk of later psychotic, internalizing, and substance misuse diagnoses by 50% or more (Gale, Batty, Tynelius, Deary, & Rasmussen, 2010). Several cross-sectional studies and one prospective study that followed participants from childhood to adulthood (range of Ns = 415–2,450) have since demonstrated that a substantial proportion of these associations can be attributed to a general factor of psychopathology as measured by clinical or parental interviews (Caspi et al., 2014; Castellanos-Ryan et al., 2016; Grotzinger, Cheung, Patterson, Harden, & Tucker-Drob, 2019; Huang-Pollock, Shapiro, Galloway-Long, & Weigard, 2017; Lahey et al., 2015; Nigg et al., 2017). However, it remains uncertain whether general intelligence (IQ) in emerging adulthood predicts general psychopathology in middle adulthood when based on psychopathology severe enough to warrant clinical diagnoses. Furthermore, these studies have reached different conclusions regarding the associations between IQ and the specific factors of psychopathology, perhaps because of sampling variation attributable to relatively small sample sizes.
The second goal of this study was to examine associations between resting heart rate (RHR) and the general and specific factors of psychopathology. RHR is a well-studied Research Domain Criteria (RDoC) marker of individual differences in the neural fear circuitry system (Alvares, Quintana, Hickie, & Guastella, 2016; Cuthbert & Insel, 2013; Palma & Benarroch, 2014). Earlier studies have reported that RHR is elevated in patients with major depression, generalized anxiety disorder, and psychotic disorders (Clamor et al., 2014; Kemp et al., 2014). In contrast, adolescents and adults displaying antisocial behavior have lower RHR (Lorber, 2004; Ortiz & Raine, 2004). We (Latvala et al., 2016) replicated these findings by showing that higher RHR, measured in more than 1 million 18-year-old Swedish men during the mandatory military conscription evaluation, was associated with subsequent higher risk of being diagnosed with obsessive compulsive disorder, schizophrenia, and anxiety disorders but lower risk of substance use disorders and criminal convictions. One speculation is that the internalizing spectrum might partly reflect an elevated sensitivity toward threats and punishment and that the externalizing spectrum might partly reflect insensitivity to threats and punishment (cf. Raine, 2015).
Our third goal was to further the construct validity of the general and specific factors by comparing the findings with those based on a correlated factors model. In the former, the shared variance is funneled into a general factor, whereas in the latter, the shared variance is captured via factor correlations. In exploratory factor analysis (EFA), these are equivalent models such that a comparison between them allows for examining to what extent associations with predictors can be attributed to shared variance versus unique variance.
Method
Participants
We identified men who were born in Sweden and were conscripted for the Swedish Armed Forces between 1969 and 2010 (N = 1,840,911). Men with severe diseases, handicaps, or intellectual disability were exempt, leading to more than 95% of Swedish men having attended the conscription assessment (Mårdberg & Carlstedt, 1998). We excluded men with missing information on parents’ identity and men who had emigrated from Sweden before conscription. Furthermore, to ensure that the study design was prospective for all participants, we excluded men who suffered the adverse outcomes before conscription. After these exclusions, the study population included 1,542,707 conscripted men. For unknown reasons, RHR values between 1984 and 1993 were almost completely missing from the Conscription Register, leading to a total of 899,398 males with complete information on both RHR and IQ. The Regional Ethical Review Board of Stockholm approved the study. In accord with Swedish law, informed consent was not required because the study relied on deidentified register data.
Predictors: resting heart rate and intelligence measured at conscription
The mean age at conscription was 18.23 years. As part of the conscription evaluation, RHR was measured after 5 to 10 min of rest in the supine position with an appropriate cuff at heart level. We excluded RHR values below 35 and above 145 beats per minute (n = 172) as outliers or potential data entry errors (Latvala et al., 2016). IQ was also assessed during the conscription evaluation using the Swedish Enlistment Battery (SEB). Three different versions of the SEB were used during the study period: SEB67 during 1969 to 1979 (reliability not reported), SEB80 during 1980 to 1993 (hierarchical ω = .82), and CAT-SEB during 1994 to 2010 (hierarchical ω = .81; Carlstedt & Mårdberg, 1993; Mårdberg & Carlstedt, 1998). We standardized (M = 0, SD = 1) RHR and IQ to facilitate effect size comparisons (for unstandardized means and standard deviations, see Table S1 in the Supplemental Material available online).
Outcomes: later psychiatric disorders, crimes, and anxiolytic prescriptions
The mean age of the sample at end of follow-up (2013) was 43.09 years (range = 21–63); thus, the average follow-up time after conscription was 24.86 years (range = 3–44). We linked the males to several national registers that record contact with the mental health and judicial systems. Information about all psychiatric inpatient admissions since 1973 and outpatient diagnoses since 2001 were available from the National Patient Register until the end of 2013. To access inpatient or outpatient care, individuals must receive a referral from a primary care physician, present (and be admitted) at a psychiatric emergency clinic, or be forcibly admitted against their will. Diagnoses were assigned by the attending psychiatrist according to Swedish translations of the International Classification of Diseases (ICD 8, 9, and 10) in a nonhierarchical fashion. We included 10 psychiatric disorders (Table 1; ICD codes are available in Table S2 in the Supplemental Material). We also included violent (e.g., unlawful threats, assault, and homicide) and property (e.g., theft and burglary) criminal convictions from the Swedish Crime Register as indicators of antisocial behavior. As a measure of potentially less severe internalizing problems, we included prescription of anxiolytics (sedatives, Anatomical Therapeutic Chemical [ATC] N05C; anxiolytics, ATC N05B; and antidepressants, ATC N06A), which can be prescribed without contact with inpatient or outpatient care (i.e., they can be prescribed by primary care physicians and private mental health practitioners). All outcomes were treated as binary variables, that is, we examined only whether they had occurred. Descriptive statistics are displayed in Table S1 in the Supplemental Material.
Exploratory Factor Analysis of Outcomes
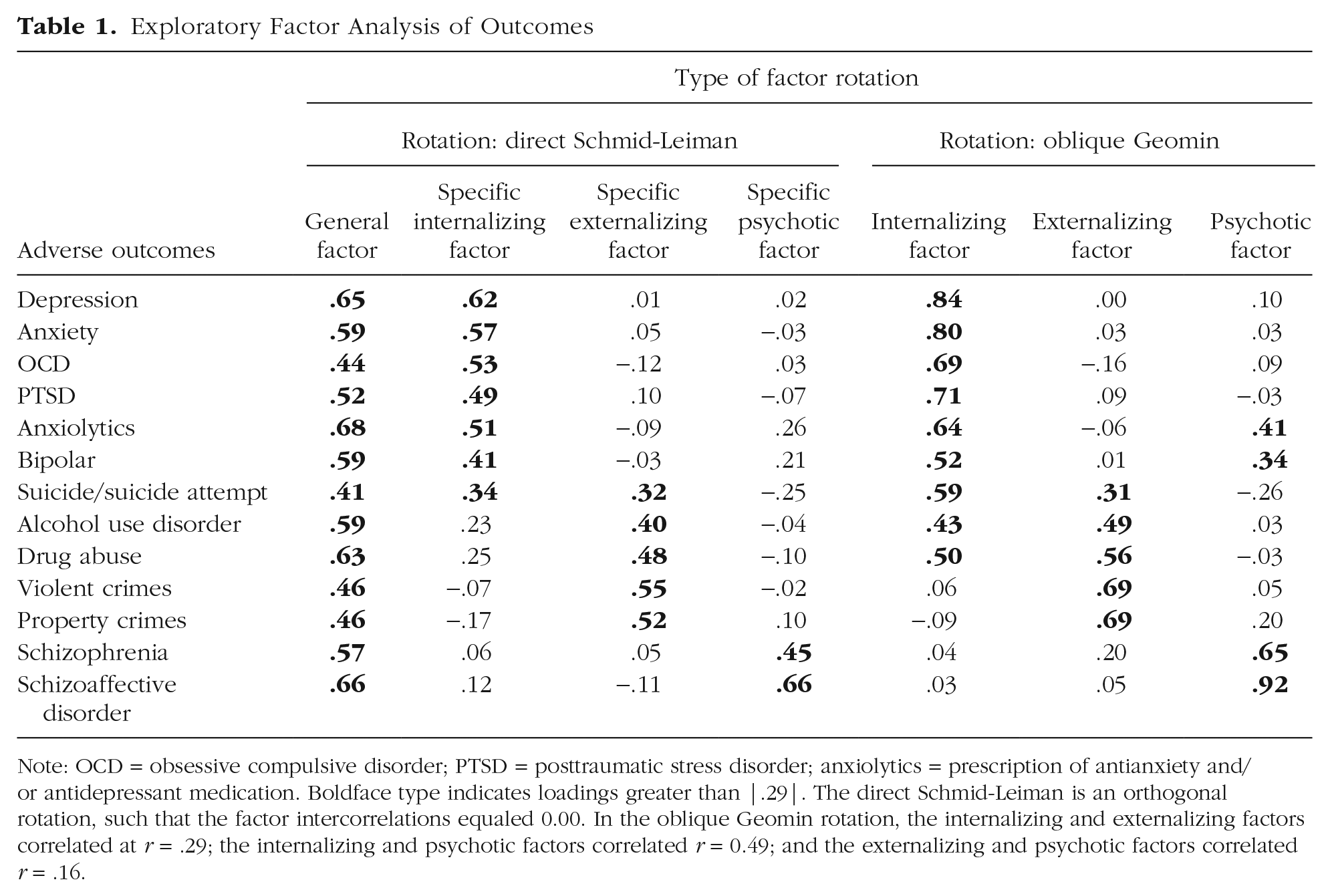
Note: OCD = obsessive compulsive disorder; PTSD = posttraumatic stress disorder; anxiolytics = prescription of antianxiety and/or antidepressant medication. Boldface type indicates loadings greater than |.29|. The direct Schmid-Leiman is an orthogonal rotation, such that the factor intercorrelations equaled 0.00. In the oblique Geomin rotation, the internalizing and externalizing factors correlated at r = .29; the internalizing and psychotic factors correlated r = 0.49; and the externalizing and psychotic factors correlated r = .16.
Covariates
We adjusted the analyses for several potential confounders, similar to our earlier studies based on the same sample (Latvala et al., 2016). To control for possible associations with body size, we adjusted for height and weight, which were measured during the conscription evaluation. We also adjusted for physical fitness, which was assessed during the conscription evaluation via an exercise test with a bicycle ergometer, generating a measure of maximal workload (expressed in watts). This measure was divided by weight to take into account body size. Family socioeconomic status in childhood was derived from the occupation of the head of the household and coded into three classes: low, medium, and high. Finally, we included year of birth to adjust for potential cohort and period effects.
Statistical analyses
First, we conducted an EFA of the 13 adverse outcomes. We used an exploratory analysis rather than confirmatory analysis because the outcomes seemed unlikely to have simple structure. That is, in contrast to paper-and-pencil instruments, which allow test developers to iteratively delete or amend interstitial factor markers until simple structure is achieved, we analyzed adverse outcomes recorded in national registers. It seemed unreasonable to assume that these outcomes would align perfectly along only a single specific dimension in the multivariate space (i.e., load at zero on all but one specific factor). We used the scree plot, which pits the number of extracted components against their explained variance, to decide how many factors to extract (Cattell, 1966).
We rotated the factor solution in two ways. First, to isolate a general factor, we rotated the solution toward one general factor and several uncorrelated specific factors using a direct Schmid-Leiman transformation (Waller, 2018). Second, we rotated the solution toward a correlated factors model using the oblique Geomin rotation. Using exploratory structural equation modeling (Asparouhov & Muthen, 2009), we then regressed each of these two rotations onto RHR, IQ, and the covariates. To examine the linearity of the associations, we divided RHR and IQ into sextiles and examined latent factor means, as well as prevalence of the 13 observed outcomes, in each sextile.
We derived the factor rotation matrices with the package GPArotation (Bernaards & Jennrich, 2005) for the R software environment (Version 3.5.1; R Core Team, 2018). All analyses were carried out in Mplus (Muthén & Muthén, 2012). We treated the binary outcomes as ordered categorical variables and used the mean- and variance-adjusted weighted least square estimator. Because we captured a large proportion of all Swedish males, some of the participants were siblings, so we might have underestimated the standard errors. Therefore, we clustered on the mother to estimate unbiased standard errors.
Sensitivity analyses
First, because the age span was wide, we divided the sample into four cohorts: men who were conscripted between 1969 and 1980, between 1980 and 1990, between 1990 and 2000, and between 2000 and 2010. We then examined the similarity of the factor structure and standardized regression coefficients (βs) across these four cohorts. Second, because we lumped together three versions of the SEB IQ test, we examined the βs separately for the three tests. Third, we reran the regressions excluding either IQ or RHR to examine whether their covariance influenced the βs. Fourth, we regressed both the latent general and specific factors, and the observed outcomes, onto the exposures simultaneously to examine the proportion of the variance in each outcome that could be attributed to indirect effects (via the latent factors) or direct effects.
Results
Exploratory factor analysis
The first five eigenvalues of the 13 outcomes were 6.91, 1.63, 1.33, 0.78, and 0.62. Consequently, we extracted three exploratory factors that fit the data well (root mean square error of approximation [RMSEA] = 0.011, 90% confidence interval [CI] = [0.011, 0.011]; confirmatory fit index, CFI = .995; Tucker-Lewis index [TLI] = .990; χ2(42) = 8,168.602, p < .001).
We rotated this solution toward a general factor model and toward a correlated factors model. Table 1 displays the factor loadings and correlations. In the general factor model, all outcomes loaded positively on the general factor (mean loading = 0.56; range = 0.41–0.68). The first specific factor captured internalizing problems (depression loading = 0.62; anxiety loading = 0.57). The second specific factor captured externalizing problems (drug abuse loading = 0.48; violent crimes loading = 0.55). The third specific factor captured psychotic problems (schizophrenia loading = 0.45; schizoaffective disorder loading = 0.66). In the correlated factors model, the factors mimicked the specific factors, albeit with stronger loadings (Table 1).
Exploratory factors regressed onto resting heart rate and intelligence
First, we regressed the general factor model onto RHR, IQ, and the covariates (RMSEA = 0.008, 90% CI = [0.007, 0.008]; CFI = .994; TLI = .993; χ2(148) = 13,063.714, p < .001). The results are displayed in Table 1. RHR had a small but significant effect on the general factor (β = −0.010, 95% CI = [−0.014, −0.006]). Furthermore, RHR significantly predicted higher specific internalizing problems (β = 0.040, 95% CI = [0.034, 0.046]) and higher specific psychotic problems (β = 0.025, 95% CI = [0.017, 0.033]) but lower specific externalizing problems (β = −0.074, 95% CI = [−0.078, −0.070]). In contrast, IQ was a significant and negative predictor of the general factor of psychopathology (β = −0.181, 95% CI = [−0.183, −0.179]). Furthermore, IQ was negatively associated with the specific externalizing factors (β = −0.221, 95% CI = [−0.225, −0.217]) and specific psychotic factors (β = −0.015, 95% CI = [−0.021, −0.009]) and positively associated with the specific internalizing factor (β = 0.054, 95% CI = [0.050, 0.058]). The associations with the four latent factors (Fig. 1) and the 13 adverse outcomes (see Table S3 in the Supplemental Material) appeared largely linear.
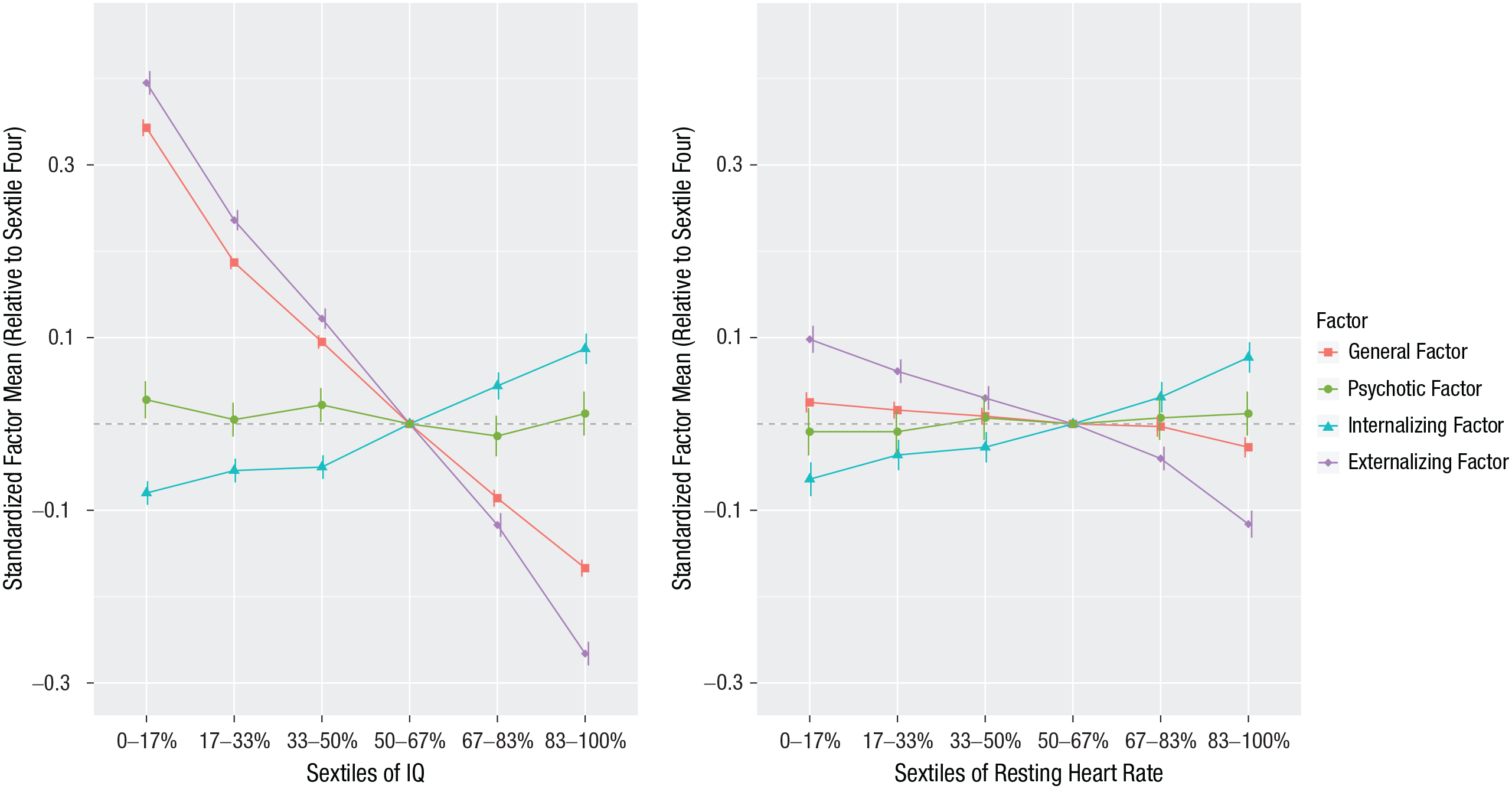
Standardized factor means by sextiles of resting heart rate and general intelligence (IQ). Displays standardized factor means by sextiles of predictors, and the fourth sextile was the reference group. Bars represent 95% confidence intervals.
Second, we regressed the correlated factors model onto RHR and IQ (Table 1). RHR significantly predicted higher internalizing problems (β = 0.017, 95% CI = [0.013, 0.022]) and higher psychotic problems (β = 0.028, 95% CI = [0.021, 0.035]) but lower externalizing problems (β = −0.075, 95% CI = [−0.079, −0.070]). IQ was negatively associated with the externalizing factor (β = −0.288, 95% CI = [−0.291, −0.284]), the psychotic factor (β = −0.087, 95% CI = [−0.092, −0.082]), and the internalizing factor (β = −0.094, 95% CI = [−0.098, −0.091]).
Because the association between RHR and the factors remained similar in the general and the correlated factors model, it implies that RHR is primarily associated with specific rather than general variance. In contrast, the correlated factors rotation appeared to mask that a substantial part of the associations between IQ and the factors could be attributed to general rather than specific variance.
Sensitivity analysis
First, both the factor structures and the βs were similar across four conscription cohorts, indicating that the results generalized across a wide age span (sensitivity analysis; see Table S4 in the Supplemental Material). Second, the βs were similar across the three versions of the SEB, supporting our lumping of the IQ tests (see Table S4 in the Supplemental Material). Third, the βs remained very similar after excluding either IQ or RHR (see Table S4 in the Supplemental Material), indicating that their covariance did not influence the results. Fourth, on average, 87% of the variance explained in each outcome could be attributed to indirect effects via the latent factor model (see Fig. S1 in the Supplemental Material). This further suggests that the exposures influenced the underlying risk toward broader forms of psychopathology rather than each of the observed outcomes independently.
Discussion
Although a general factor model is useful in that it can account for comorbidity among mental health problems, it presents interpretive challenges. We showed that lower intelligence at age 18 years was a transdiagnostic predictor for every form of psychopathology in middle adulthood via the general psychopathology factor. In contrast, RHR distinguished between internalizing and externalizing problems.
One speculation is that RHR might index an underlying psychobiological process akin to sensitivity to threat and punishment (Raine, 2015). Insensitivity to threats was central to the original conceptualization of the psychopathy construct (Cleckley, 1955). Indeed, people with psychopathic traits tend to display damped physiological arousal in response to impending punishments (Hare, 1965; Lykken, 1957), are slower to recognize faces with fearful expressions (Sylvers, Brennan, & Lilienfeld, 2011), and self-report as less suicidal, anxious, and depressed after suppression effects are isolated (Blonigen et al., 2010; Douglas et al., 2008; Hicks & Patrick, 2006). Thus, independently of general distress and impairment, a high sensitivity to threats and punishment might predispose people toward internalizing problems, whereas a low sensitivity to threats and punishment might predispose people toward externalizing problems.
In contrast to RHR, the association between IQ and psychopathology appeared to be substantially attributable to general variance, replicating past studies (Caspi et al., 2014; Castellanos-Ryan et al., 2016; Grotzinger et al., 2019; Huang-Pollock et al., 2017; Lahey et al., 2015; Nigg et al., 2017). This association could arise because lower cognitive ability increases exposure to adverse environments that in turn increase general mental health problems or because lower cognitive ability reduces the tendency to seek mental health treatment (Caspi & Moffitt, 2018). However, because the diagnoses in this study were assigned after individuals sought treatment and because the association between IQ and general psychopathology appears to emerge before the age of 6 (Caspi & Moffitt, 2018; Grotzinger et al., 2019), adverse environments or lack of treatment-seeking behavior might not account for the entire association. One speculation is that part of the association might be attributable to executive functioning, which is phenotypically and genetically associated with both general psychopathology and intelligence (Harden et al., 2020; Martel et al., 2017).
Lower IQ also predicted higher scores on the specific externalizing factor, replicating past research (Huang-Pollock et al., 2017; Nigg et al., 2017). This might represent a direct effect, perhaps mediated via education, because even after adjusting for potential family-level confounds (including genetics), low IQ and academic achievement remain associated with externalizing problems (Frisell, Pawitan, & Langstrom, 2012; Kendler et al., 2018).
Implications
The results presented herein have several implications. First, it might be useful to examine whether executive functions partly drive the associations between lower intelligence and general psychopathology and specific externalizing problems (Harden et al., 2020; Martel et al., 2017). Second, in a recent review, RHR was the only endophenotype out of 40 candidates that displayed reliable associations with molecular genetic variants (Iacono, Malone, & Vrieze, 2017). Thus, one possibility is that RHR might help shed light on the genetic architecture underlying internalizing and externalizing problems. Third, whereas the current RDoC perspective highlights the biological underpinnings of anxiety and fear (Cuthbert & Insel, 2013), it does not appear to consider the opposite extreme of fear (i.e., fearlessness) as equally maladaptive. These results imply that both extremes of the fear continuum might predispose people toward opposite types of adverse outcomes (Rojas & Widiger, 2018).
Limitations
These results should be interpreted in light of the strengths and limitations of the study. Study strengths include that we relied on a large sample of males followed up for an average of 25 years and that the outcomes were retrieved from population registers and the judicial system. Study limitations include first, that because only 95% of the men born in Sweden were mandated to participate in the conscription evaluation, it remains uncertain whether our results generalize to the remaining 5% of Swedish males who did not undergo conscription, females, and people born in other countries. Second, although we speculate that RHR might be an indicator of an underlying trait dimension, it is unknown whether the associations are driven by constant differences in RHR or by differences in response to a potentially stressful evaluation. If the latter, RHR would be predictive of only future outcomes if assessed during an equally stressful situation. Third, it is possible that when the loadings on the general factor are based on register data, they might be overestimated because of collider bias, given that people with several disorders might be more prone to end up in the mental health system (also called Berkson’s bias); however, the magnitude of the loadings on the general factor in this register-based study appeared similar to that of survey studies, in which one might expect collider bias to lead to underestimation of general factor loadings because individuals with several mental health problems might be less prone to participate in such surveys (Caspi et al., 2014; Lahey et al., 2015).
Conclusion
Lower IQ was a transdiagnostic predictor of future mental health problems via the general factor of psychopathology. In contrast, RHR was associated in opposite directions with the specific internalizing and specific externalizing factors, which suggests that these latent factors of psychopathology might partly reflect elevated sensitivity versus insensitivity toward threats and punishment, respectively.
Supplemental Material
sj-pdf-1-cpx-10.1177_2167702620961081 – Supplemental material for Associations of Resting Heart Rate and Intelligence With General and Specific Psychopathology: A Prospective Population Study of 899,398 Swedish Men
Supplemental material, sj-pdf-1-cpx-10.1177_2167702620961081 for Associations of Resting Heart Rate and Intelligence With General and Specific Psychopathology: A Prospective Population Study of 899,398 Swedish Men by Erik Pettersson, Paul Lichtenstein, Henrik Larsson, Brian M. D’Onofrio, Benjamin B. Lahey and Antti Latvala in Clinical Psychological Science
Footnotes
Transparency
Action Editor: Kenneth J. Sher
Editor: Scott O. Lilienfeld
Author Contributions
E. Pettersson, A. Latvala, P. Lichtenstein, and B. B. Lahey developed the study concept. All of the authors contributed to the study design. Data extraction was performed by E. Pettersson and A. Latvala. E. Pettersson conducted the analyses and drafted the manuscript. All of the authors provided critical revisions and approved the final manuscript for submission.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.